CHANGE IS COMING — WE ARE WELL-AWARE THAT THIS PAGE IS PRETTY DATED…
RATHER THAN MODIFY, WE ARE WORKING ON A COMPLETE REBUILDING OF THIS PAGE. STAY TUNED
Embryology: For a full discussion of this endless topic, you can consult Lasjaunias, Berenstein, and Ter Brugge. Surgical Neuroangiography, 2nd edition, 1st volume, A limited but essential understanding of the topic is provided here by way of general important knowledge. A brief discussion with some illustrations is provided here. All of these observations were advanced first and foremost by anatomical work of D. Padget in his work The development of the cranial arteries in the human embryo. Contrib Embryol 1948; 32:207 –262 and discussed in detail by Lasjaunias P, Berenstein A, Ter Brugge KG inClinical vascular anatomy and variations. Berlin, Germany: Springer,2001 : 414–424
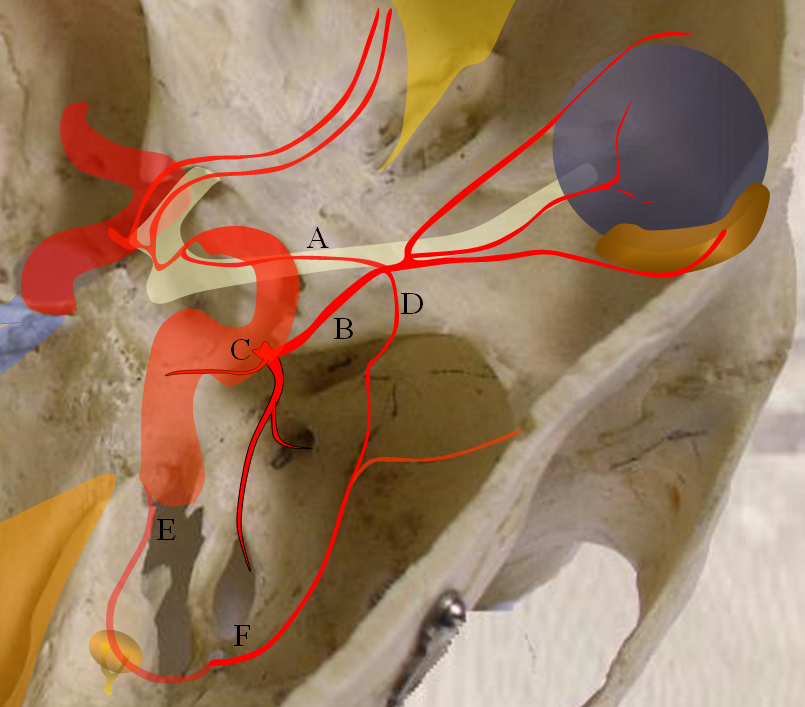
The evolution of orbital supply seems quite strange in that the adult ophthalmic does not appear to come from a known precursor vessel in its expected location. In the early embryonic life, the orbit seems to be supplied by a balance of three arteries, all of which subsequently take a step back in favor of a somewhat mysteriously appearing adult ophthalmic. These three early arteries, illustrated in Figure 1 are:
1) Dorsal ophthalmic artery — originating from the adult location of the ILT and entering the orbit via the superior orbital fissure. The role of this artery gradually diminishes. In the adult, the anteromedial branch of the ILT and the recurrent tentorial branch of the ophthalmic artery (see figure below) correspond to vestiges of the embryonic dorsal ophthalmic. Very rarely, this artery persists into adult life to maintain dominant supply of the orbit, as illustrated in a case below.
2) Ventral ophthalmic artery — this seemingly strange vessel originates from the supraclinoid carotid artery or the anterior cerebral artery (what would later become the A1 segment) and enters the orbit via the optic canal to anastomose with the dorsal ophthalmic artery. Some mammals, such as horse, maintain this disposition as the dominant solution to orbital supply. On occasion, this arrangement can persist in the human also (more common than persistence of dorsal ophthalmic). Literature reports of an unusual ophthalmic artery origin with the vessel coursing above the optic nerve in fact are describing this disposition (see example below).
3) Middle meningeal artery — technically speaking this vessel is not yet called the MMA — as in embryonic life it originates from the stapedial artery. The MMA undergoes a complex evolution of its own with eventual transfer of MMA territory from internal carotid to external carotid systems. At the embryonic point in question, however, the “MMA” supplies the orbit through its meningo-ophthalmic branch. This, too, can on occasion persist into adult life, much more commonly than either dorsal or ventral ophthalmic persistence (see cases below). From a clinical standpoint this is the MOST IMPORTANT variant. Embolization of the middle meningeal artery from a point proximal to the takeoff of the meningo-ophthalmic artery will have the same effect as embolization of the “usual” ophthalmic artery.
All of the above arrangements can be either complete or partial. For example, a “usual” origin ophthalmic artery may supply the globe (and central retinal artery) while the MMA vascularizes the lacrimal gland (in which case it is called the meningo-lacrimal variant). So, variability is the rule. From a clinical perspective, the most important vessel is the one producing the choroid blush, although any variable supply to the orbit should give one great pause prior to any kind of embolization. Intraorbital anastomoses between separate systems will exist and embolization of the central retinal artery will be a major disaster.
Getting back to embryology, it is not clear to me how the above-describes triumvirate looses out to a vessel that seemingly comes from nowhere. Some very respectable authorities (Pierce Morris, for example) believe that the adult ophthalmic artery evolves via gradual transfer of the origin of the ventral ophthalmic artery caudally along the ICA until it reaches its usual point origin at what is eventually called the ophthalmic segment. The mechanism of this is unclear and I do not think that all authorities on the subject share this view.
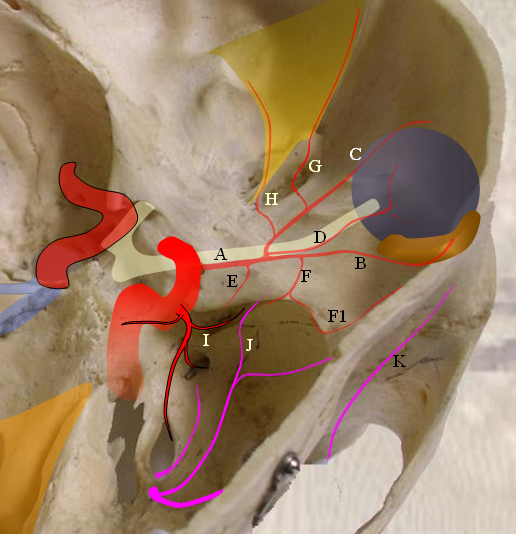
Figure 1: A — ventral ophthalmic artery, B — dorsal ophthalmic artery, C — Inferolateral Trunk, D — meningo-ophthalmic artery, E — stapedial artery, F — forerunner of the middle meninigeal artery originating from the stapedial system at this point
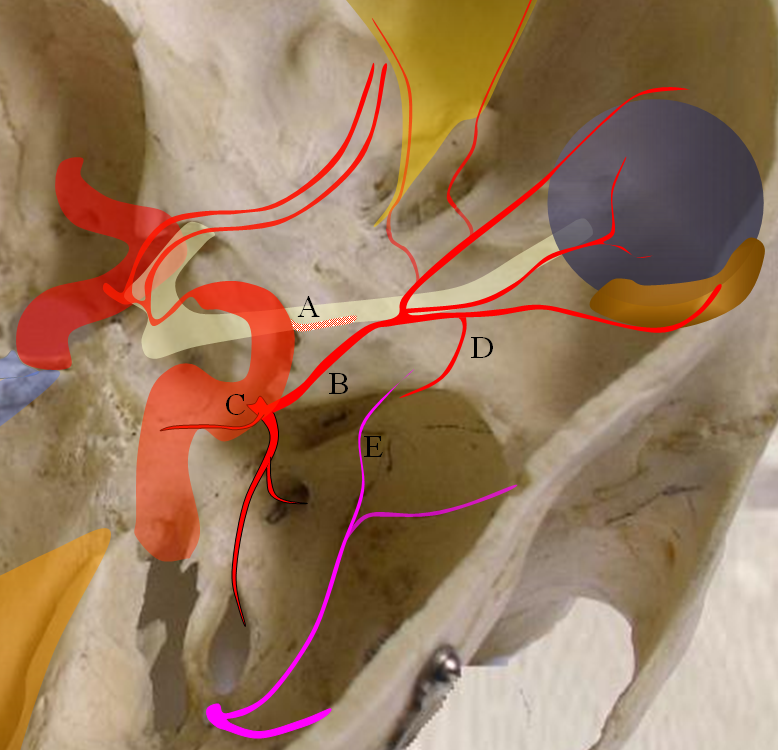
Figure 2 — persistence of dorsal ophthalmic artery. A — site of “classic” ophthalmic artery origin; B — dorsal ophthalmic artery; C — future ILT; D — recurrent meningeal branch of the ophthalmic artery; E — meningo-ophthalmic branch of the MMA
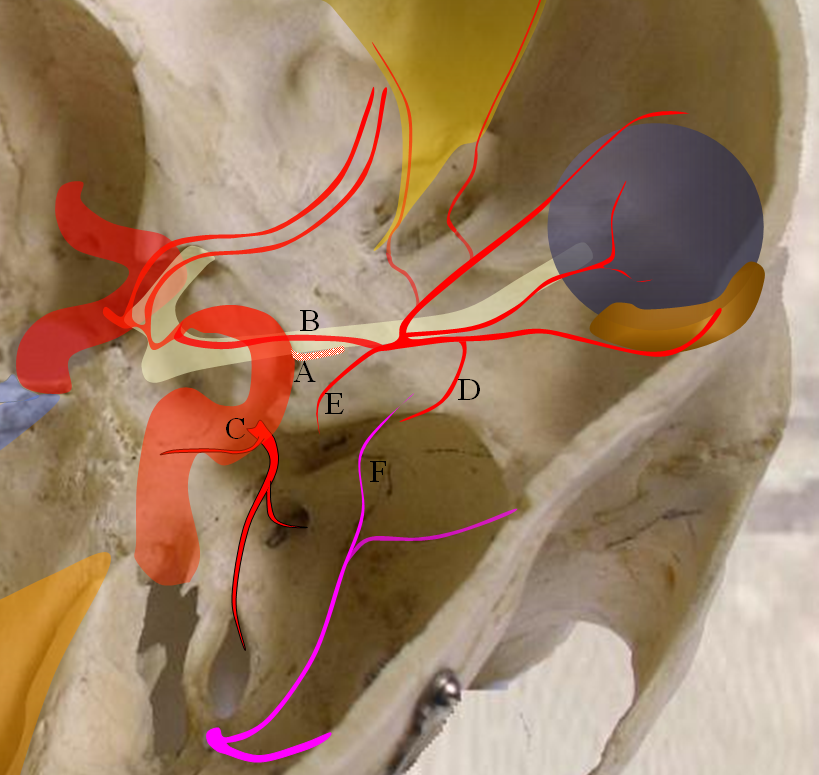
Figure 3 — persistence of ventral ophthalmic artery. A — site of “classic” ophthalmic artery origin; B — ventral ophthalmic artery; C — future ILT; D — recurrent meningeal branch of the ophthalmic artery; E — recurrent tentorial branch of the ophthalmic artery; F — MMA branches
Imaging:
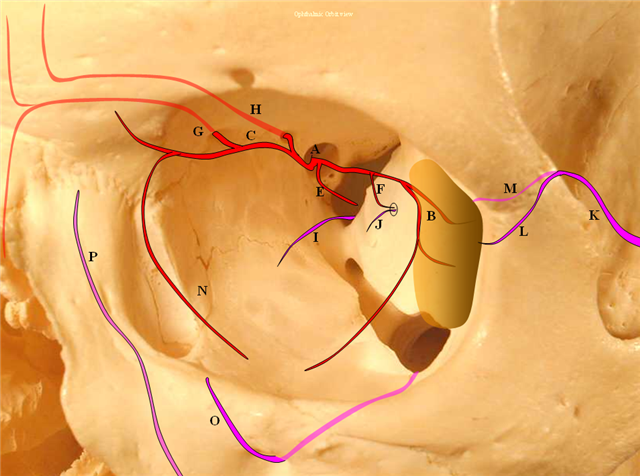
Figure 4: Pictorial visualization of the “classic” Ophthalmic Artery, intracranial view above and orbital view below.
A) Main Ophthalmic Artery
B) Lacrimal branch (actually many small branches by the time it gets to the lacrimal gland), which will collateralize with IMAX anterior deep temporal branches (K) thru transosseous (M) or muscular (L) routes. This is a very common pathway of ophthalmic / ICA reconstitution via the IMAX.
C) Medial division which gives off important anterior (G) and posterior (H) ethmoidal arteries. These enter the anterior cranial fossa thru respective foramina and supply regions of the cribriform plate and anterior falx. The anterior falcine artery can be particularly prominent especially after pterional craniotomies or other destructive processes of the middle meningeal artery. The ethmoid arteries also send branches into the nasal cavity (see below)
D) Central retinal artery: a true end-artery with NO collaterals. Occlusion results in irreversible permanent loss of vision. Aside from the central retinal artery, the other ophthalmic branches supply muscle and other orbital tissue.
E) Recurrent tentorial branch — an important collateral pathway connecting orbit to middle cranial fossa, collateralizing with anteromedial branch (I) of the ILT. Both (E) and (I) are vestiges of the primitive dorsal ophthalmic artery (see embryology)
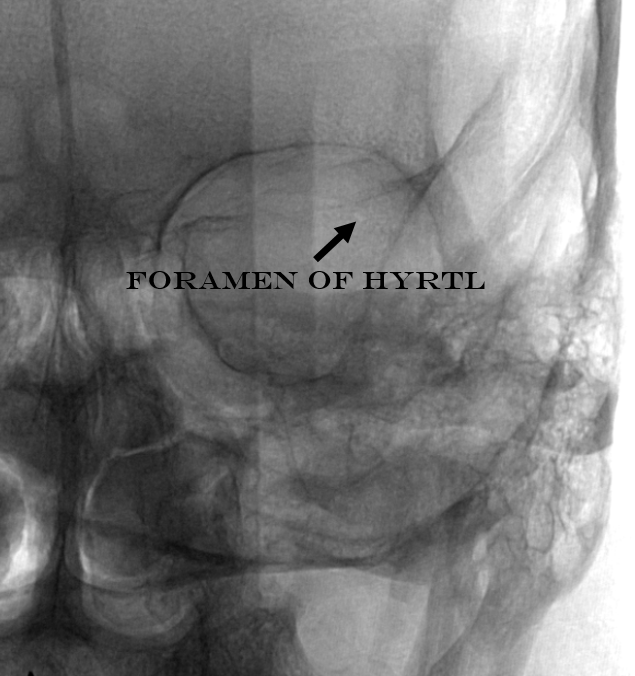
F) Recurrent meningeal branch — important branch from the lateral (lacrimal) division which can collateralize with ophthalmic branch (J) of the middle meningeal artery and is a potential MMA to ophthalmic connection, often visualized in setting of main ophthalmic or ICA occlusions. This artery tends to exit the orbit through its own foramen, which when large enough carries a name of Foramen of Hyrtl
F1) Anterior Frontal Meningeal Branch — vascularises dura of the frontal convexity, can be prominent in setting of meningiomas, etc.
N) Inferior branches supplying muscle and other tissue, which can collateralize with distal inferior orbital branch (O) of the IMAX exiting through the infraorbital foramen and angular branch (P) of the facial artery.
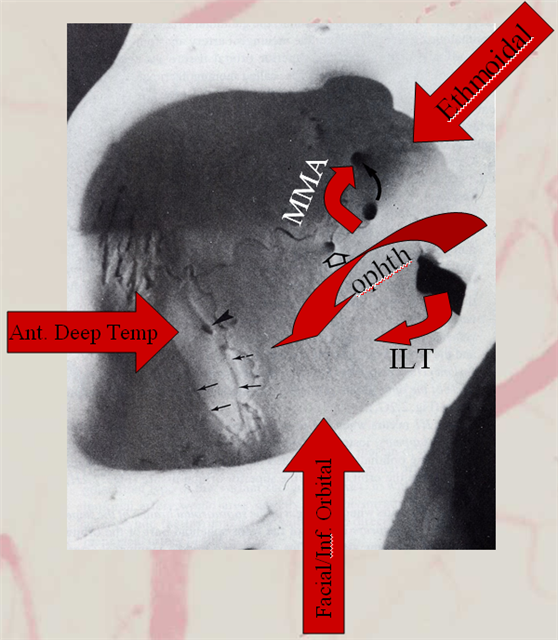
Collateral pathways into/from the orbit. Orbital photo from Lasjaunias, Berenstein, and Ter Brugge. Surgical Neuroangiography, 2nd edition, 1st volume, page 446. Bony landmarks attest to collateral potential of the orbital vasular supply. The meningolacrimal branch of the MMA enters the orbit through foramen of Hyrtl (open arrow). The MMA can enter the orbit (meningoophthalmic branch, curved arrow) The anteromedial branch of the ILT can collateralize through the superior orbital fissure. The anterior deep temporal branches can be transosseous (arrowhead) or muscular draped over the lateral orbital wall and get into the orbit that way to hook up with lacrimal branches of the ophthalmic. Angular branch of the facial artery or the infraorbital artery collateralize the orbit from below. Finally, the ethmoidal arteries, usually supplied by the ophthalmic to vascularize crista galli and anterior falx and superior nasal cavity can on occasion reverse flow and backfeed into the ophthalmic, although other collaterals are much more frequently recruited for this purpose.
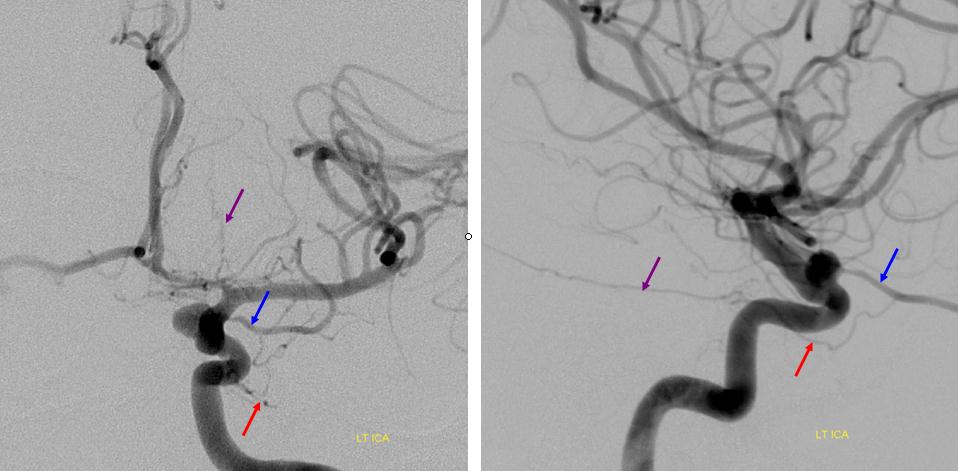
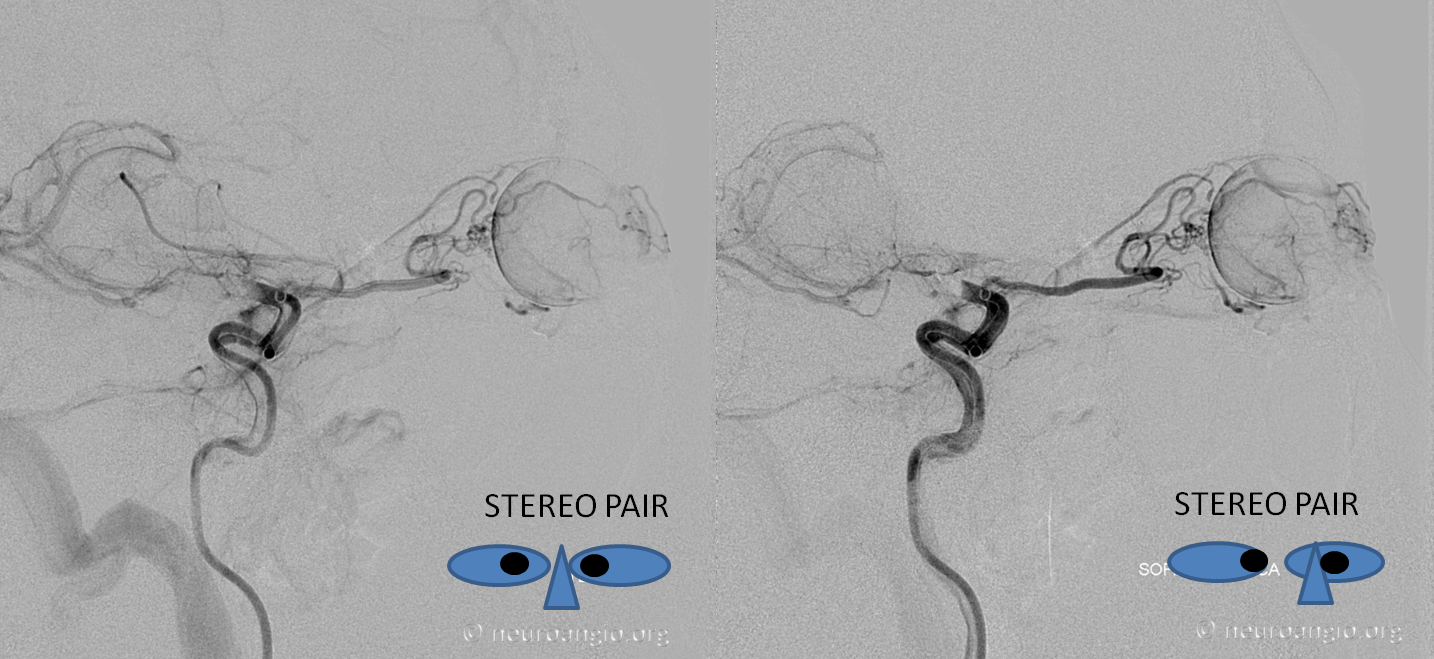
Dorsal Ophthalmic Artery — Cavernous Origin of the Ophthalmic Artery — this rare disposition corresponds to persistence of embryonic dorsal ophthalmic artery, essentially representing an ILT origin of the ophthalmic.
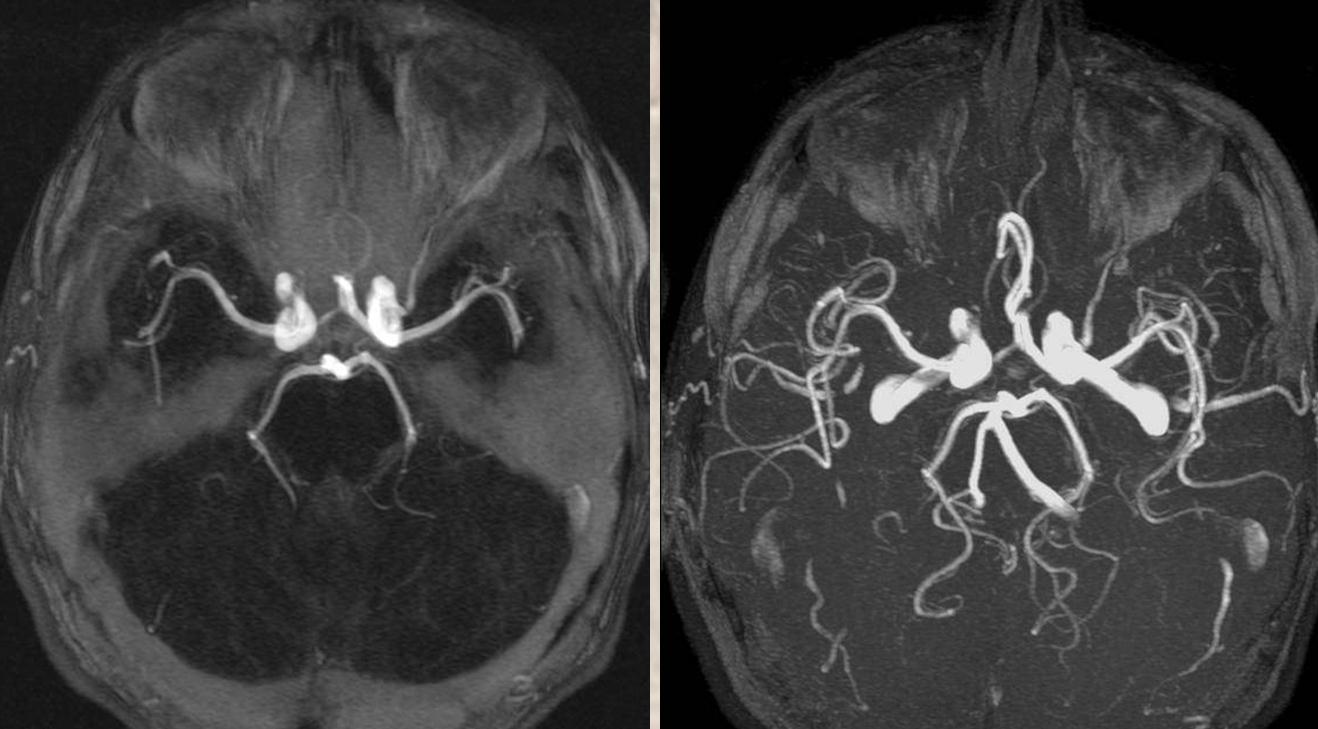
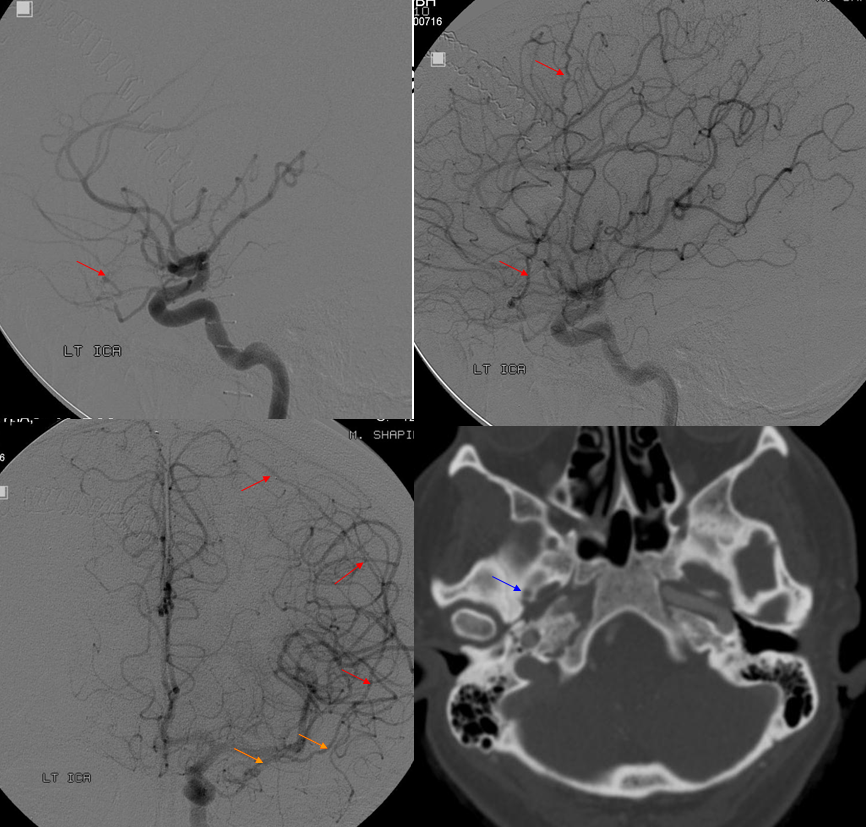
A vessel originates from the lateral cavernous portion of the left carotid artery corresponding to location of the ILT and enters the orbit (red arrows). The right ophthalmic artery origin (yellow) is normal. Average (left) and MIP (right) projections of the same case are seen below.
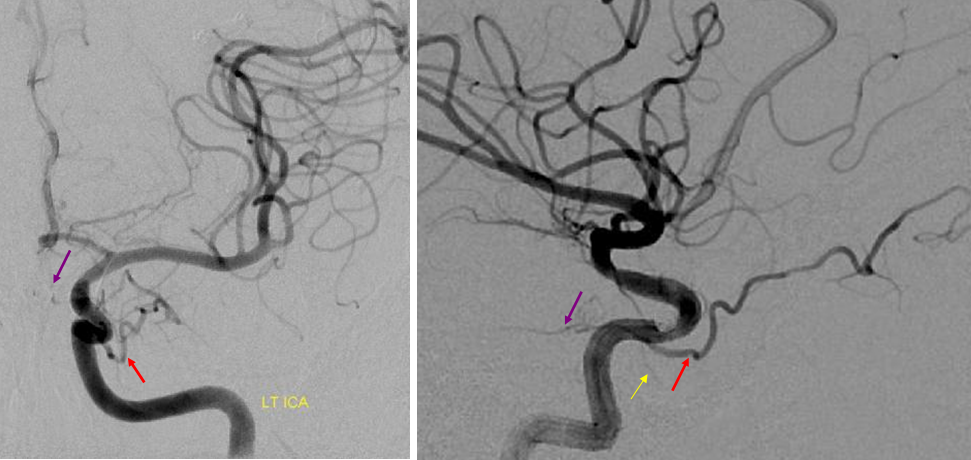
A different patient with dorsal opthalmic ILT origin
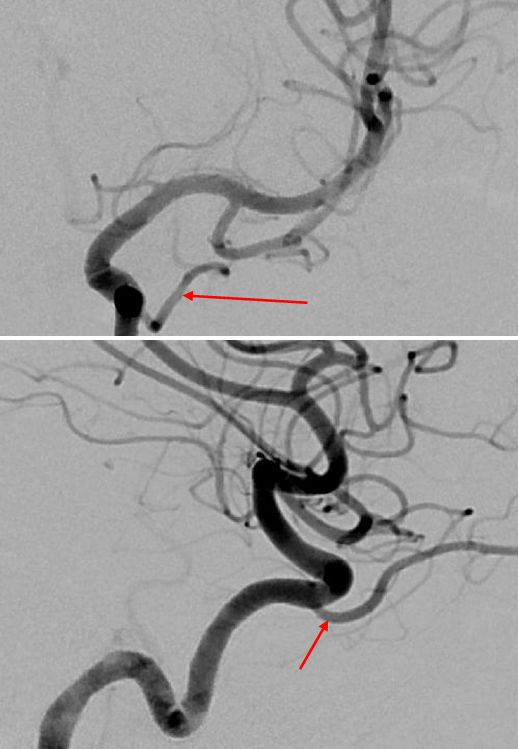
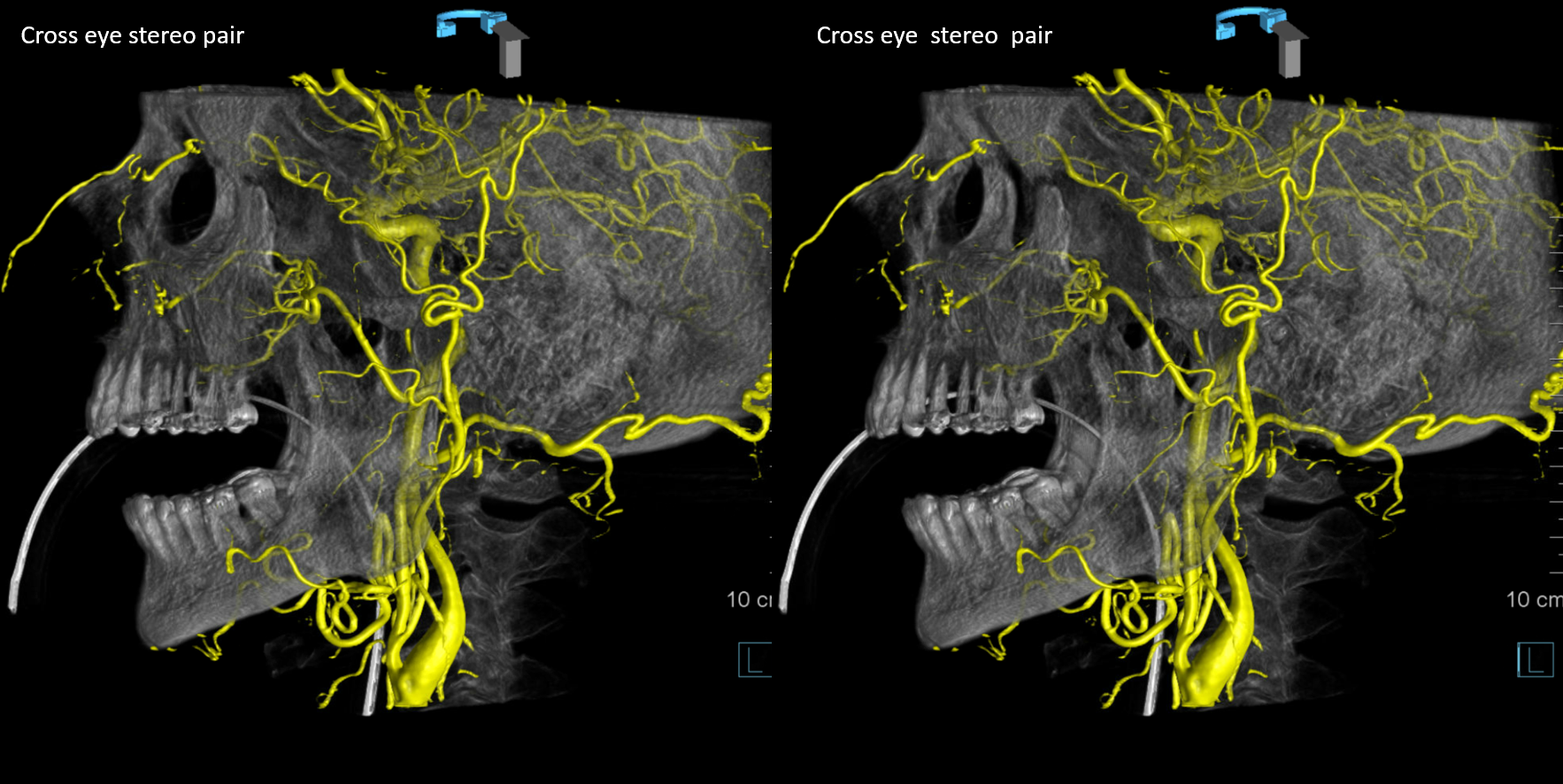
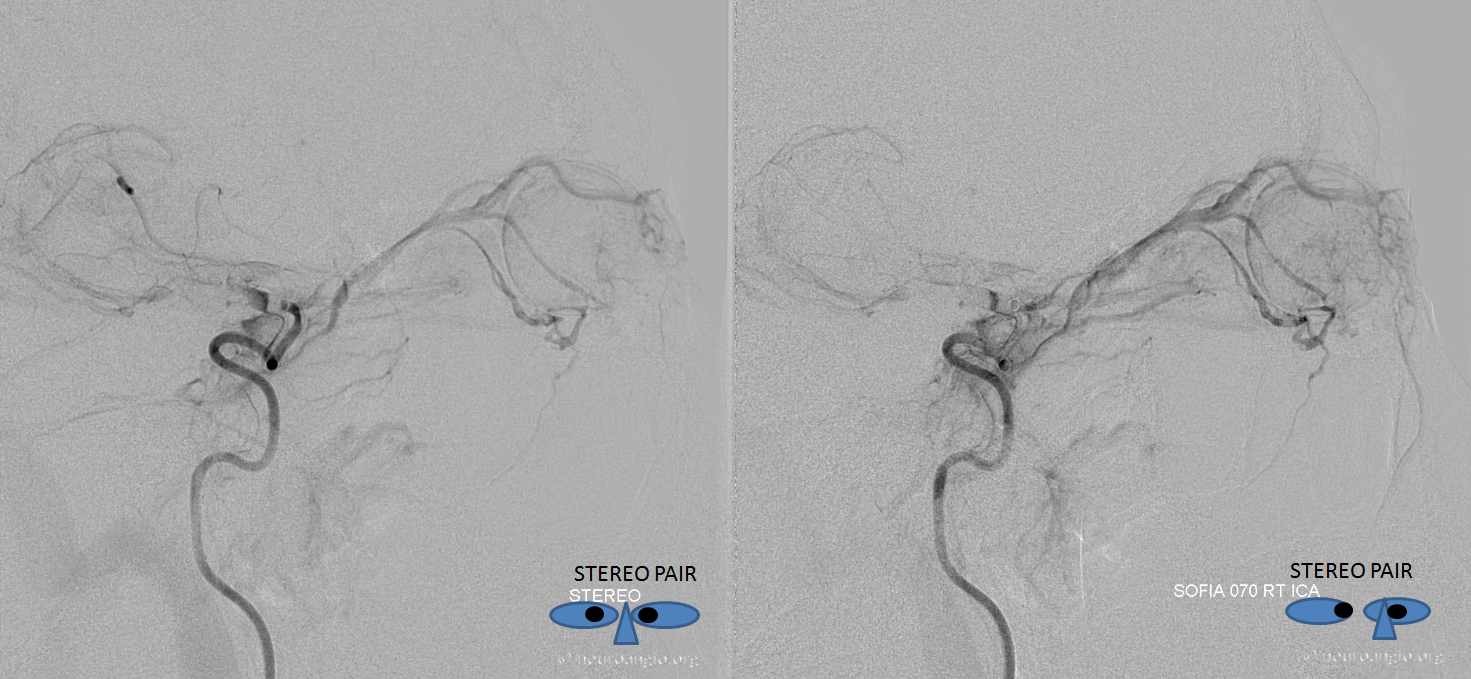
Another dorsal ophthalmic, with stereo projections
Origin of dorsal ophthalmic is labeled in red
Dorsal ophthalmic and “regular” ophthalmic arteries — can coexist as you can see. In these cases the vessels usually supply different portions of the orbit — as in this case, where the smaller “regular” ophthalmic (purple) gives off a choroidal blush (light blue) whereas the larger dorsal ophthalmic branch (red) supplies the extraoccular muscle apparatus.
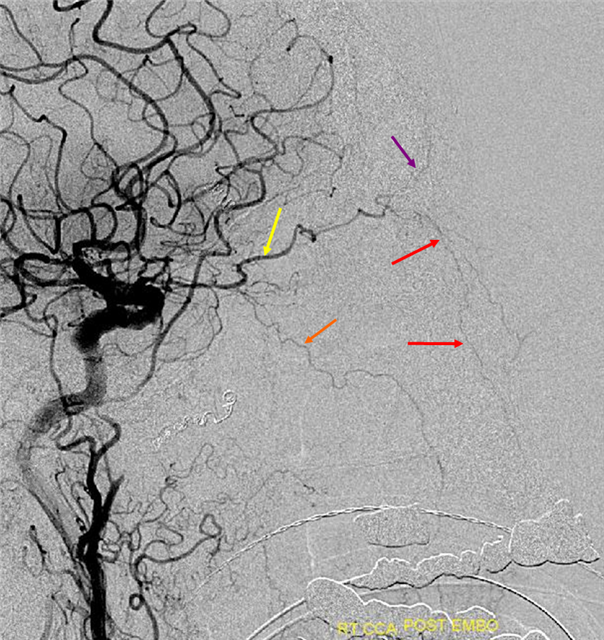
Curiously, the same patient demonstrates absence of ICA origin ophthalmic artery on the contralateral side, with a meningo-ophthalmic artery (red) disposition arising from the MMA (orange)
Acquired ophthalmic artery meningohypophyseal trunk origin from the anteromedial branch.
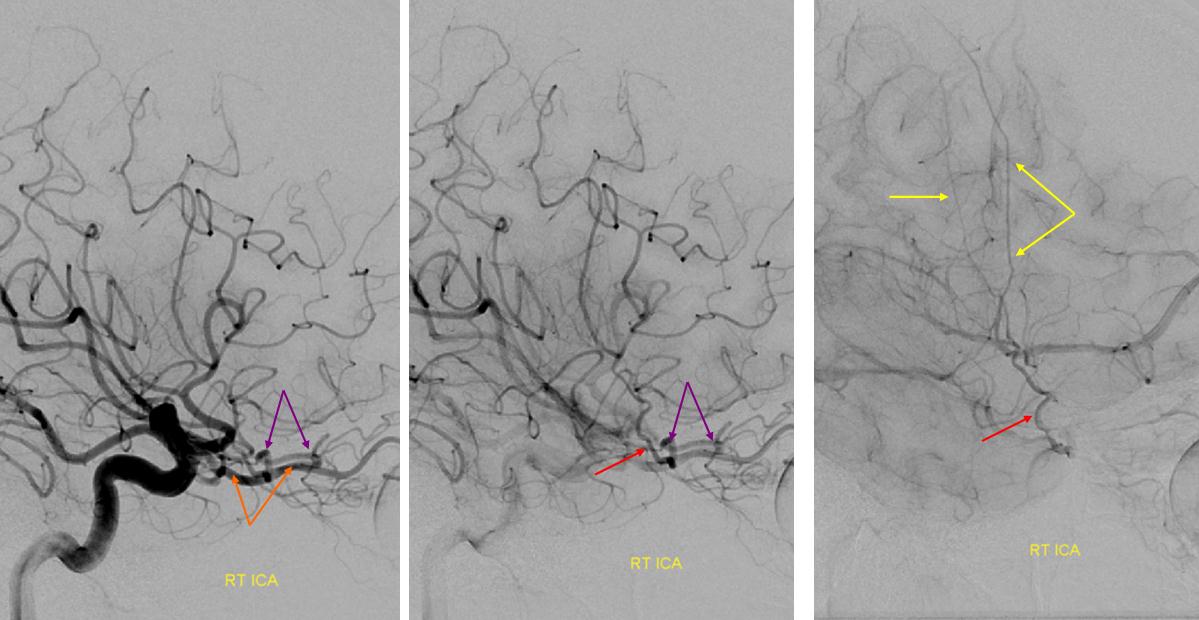
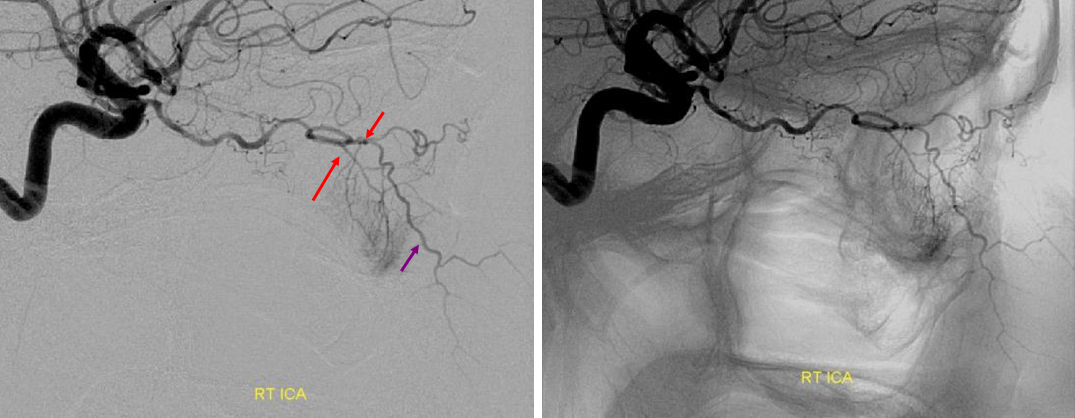
In this patient the ophthalmic artery origin was associated with an aneurysm. The upper set of images shows pre-treatment disposition with a prominent anteromedial branch (red) of the MHT collateralizing orbital supply (one can think of it as partial persistence of the dorsal ophthalmic artery). Following treatment, the aneurysm is no longer visible, and neither is the “normal” ophthalmic artery. The orbit is now being entirely supplied by the anteromedial branch of the MHT, resembling an “acquired” doral ophthalmic disposition.
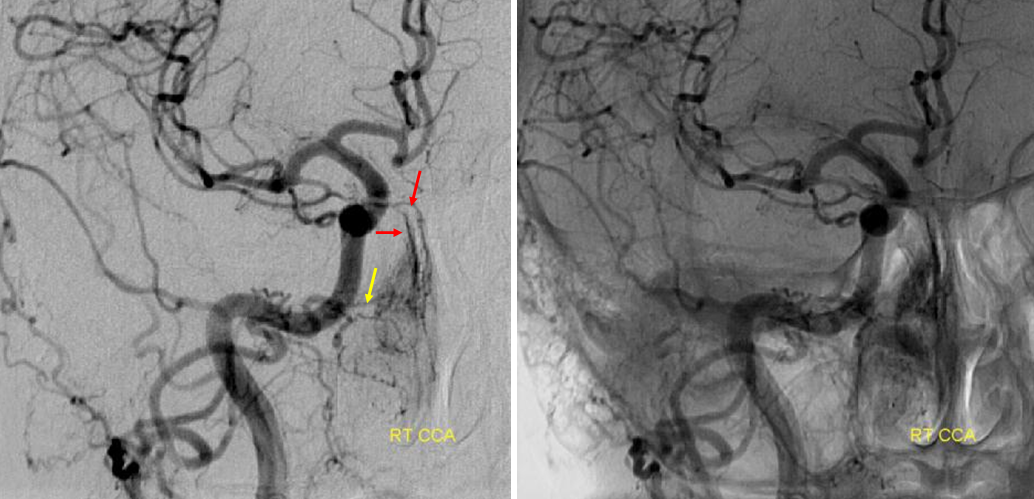
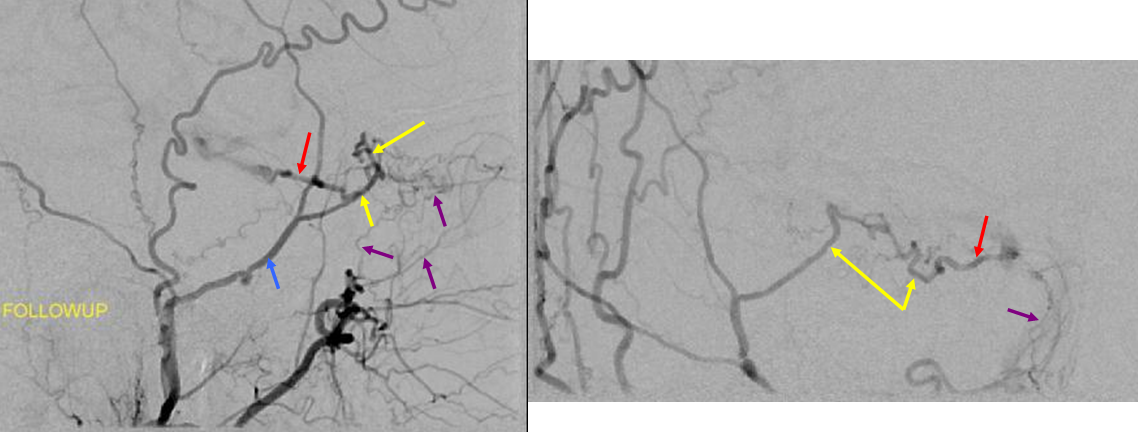
Pre-treatment AP and lateral projections demonstrating a large anteromedial branch (red) of the ILT participating in orbital supply together with the “usual” origin ophthalmic artery. The marginal tentorial branch is also prominent secondary to pterional craniotomy for attempted clipping of the aneurysm and craniotomy-related sacrifice of the ipsilateral MMA.
Post-treatment follow-up AP and lateral views of the same case. The ophthalmic artery is no longer visualized. The entire orbit is now supplied by an enlarged anterior branch of the MHT. This is a very unusual pattern of reconstition. Also notice decrease in size of the marginal tentorial branch (purple) likely due to collateralization of the left MMA territory since time of the craniotomy 6 months previously.
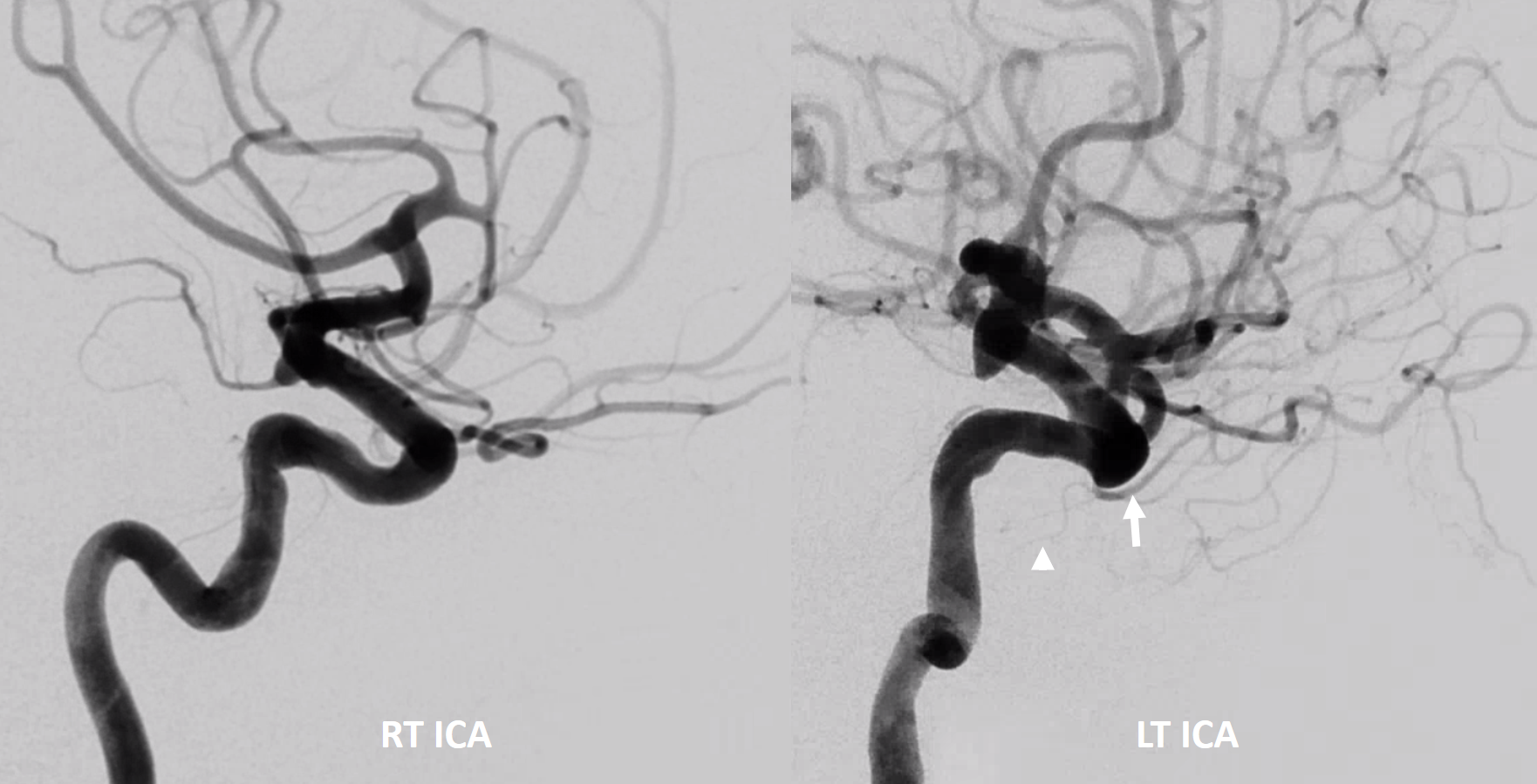
The embryology of ophthalmic artery is a debated topic. In it there is the idea of a ring that forms around the OA at the orbital apex area in early development, connecting various OA forerunners such as dorsal and ventral ophthalmic. Absence of this ring is postulated to result in dual sources of ophthalmic supply, including “regular” and Dorsal ophthalmic coexistence, as shown above. Here is a case of such co-existence on one side, while on the other a curious loop of the proximal ophthalmic is present. Some would postulate both sides to be representative of incomplete ophthalmic ring in early development.
Notice on left the ovale / MMA branch of ILT (white arrowhead) as well, together with the classic anteromedial / dorsal ophthalmic ILT branch (white arrow)
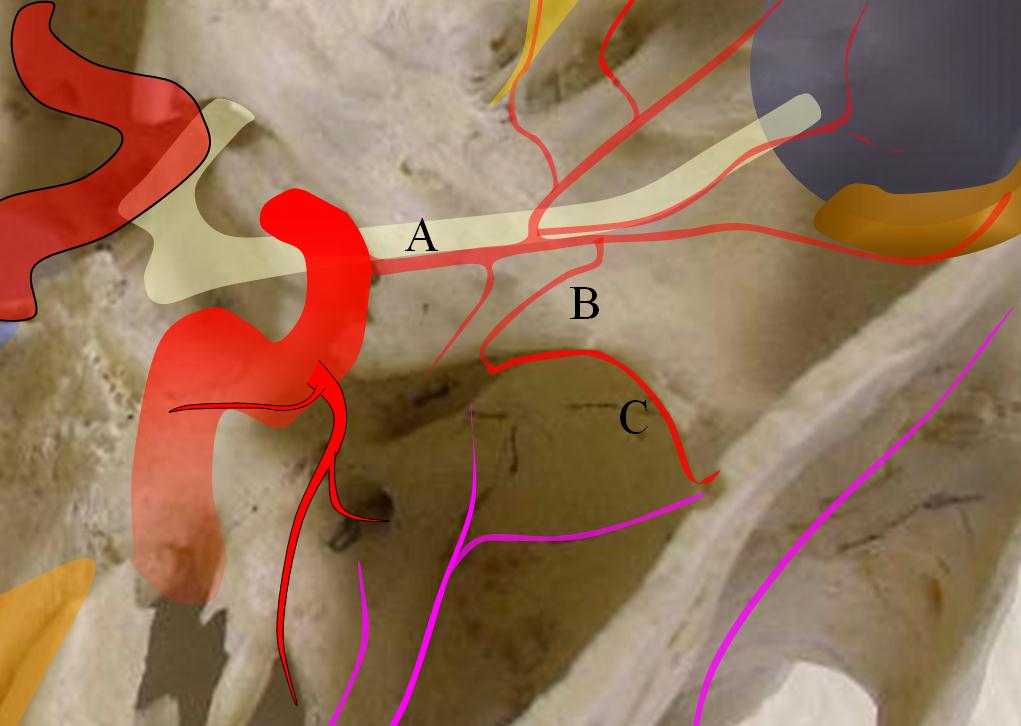
Cross-eye stereoAnaglyphLoop cross-eye stereoAnaglyphAnother example of such a ring in a different patient on DYNA CTVentral Ophthalmic ArteryThis variant is extremely rare in the human — a persistent embryonic connection between the area of the anterior communicating artery and the intraorbital ophthalmic — (A) in the diagram below:
A — ventral ophthalmic artery, B — dorsal ophthalmic artery, C — Inferolateral Trunk, D — meningo-ophthalmic artery, E — stapedial artery, F — forerunner of the middle meninigeal artery originating from the stapedial system at this pointBelow is an illustration of an incidentally found ventral ophthalmic artery (white arrows). Note opacification of the globe choroid (not labeled)
Stereo pair in frontal oblique position, demonstrating associated A1 segment fenestration (black arrows), an embryologic variant closely tied to the ventral ophthalmic artery — the infraoptic course of the A1
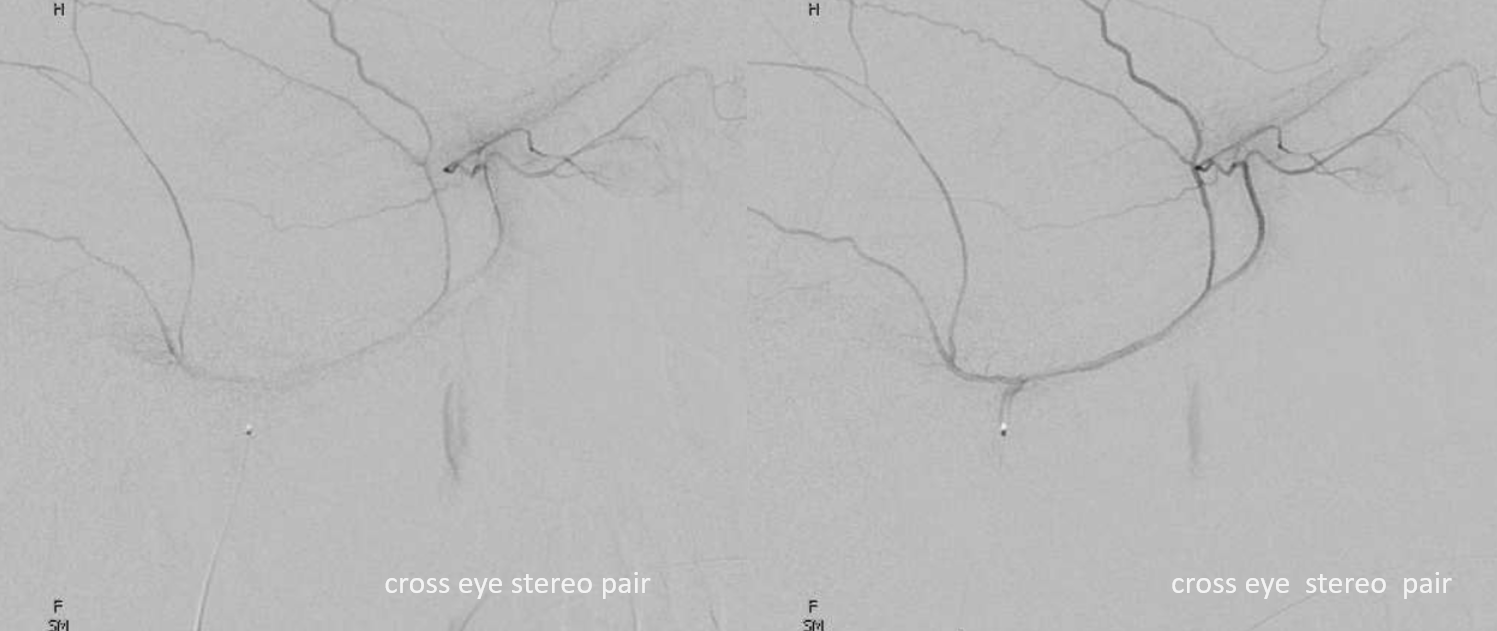
Beautiful stereo pairs
Another example of ventral ophthalmic artery (white arrows) with choroid globe blush in parenchymal phase (black arrows) in a patient with a giant, partially thrombosed ACOM aneurysm, courtesy Dr. Peter Kim Nelson.
Stereo pairs
Ventral ophthalmic remains uncovered after Pipeline aneurysm embolization
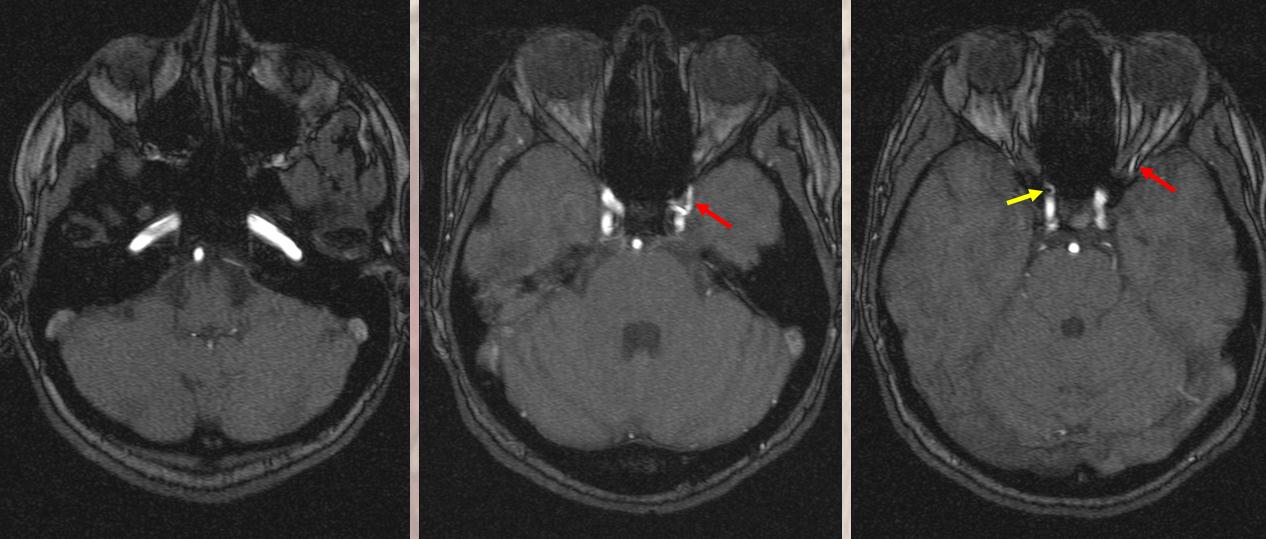
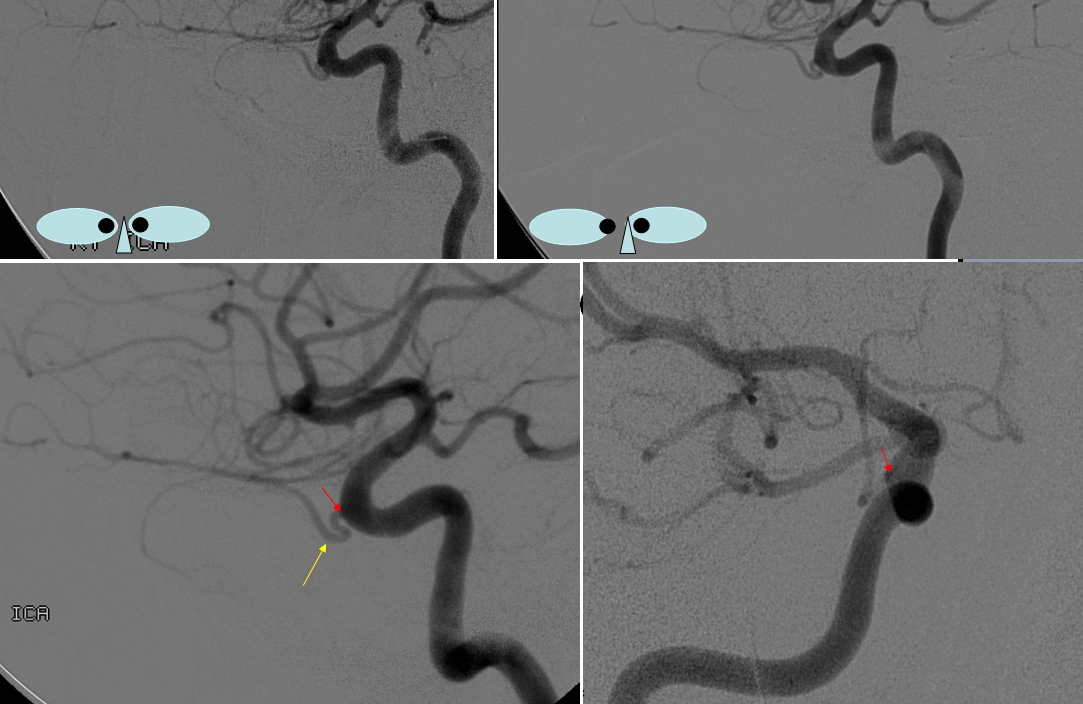
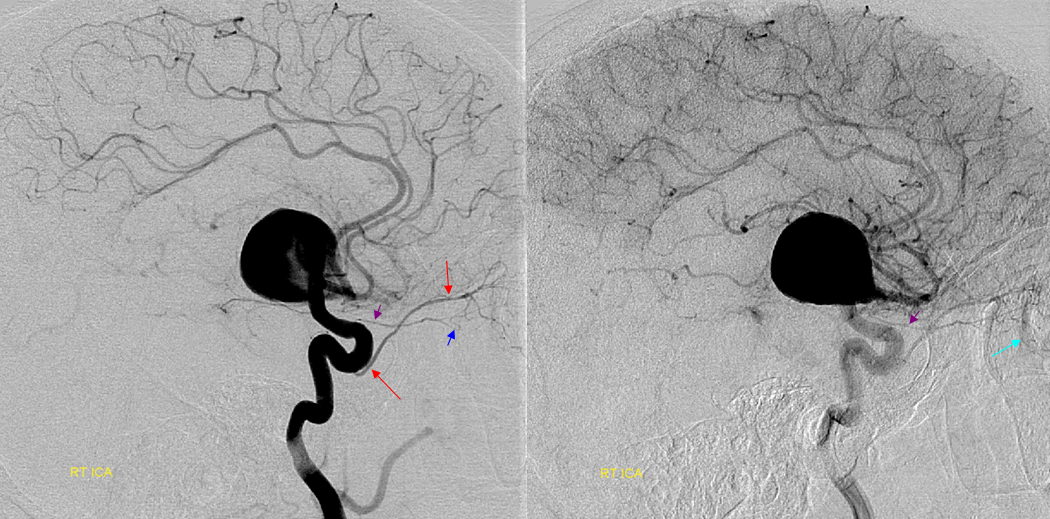
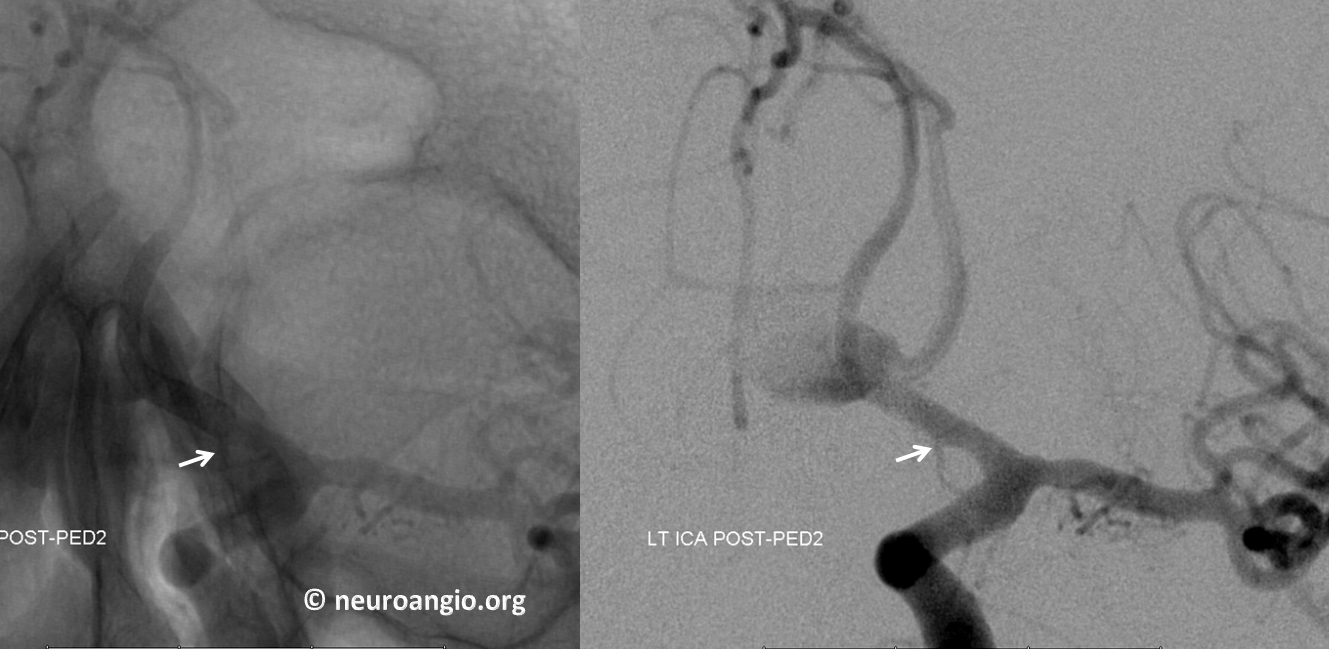
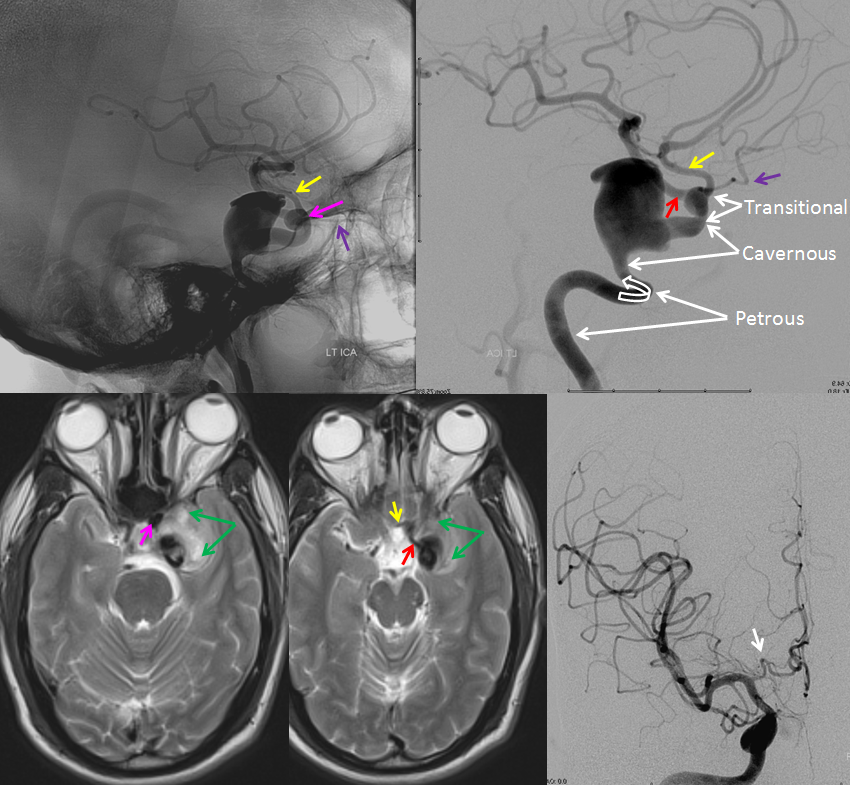
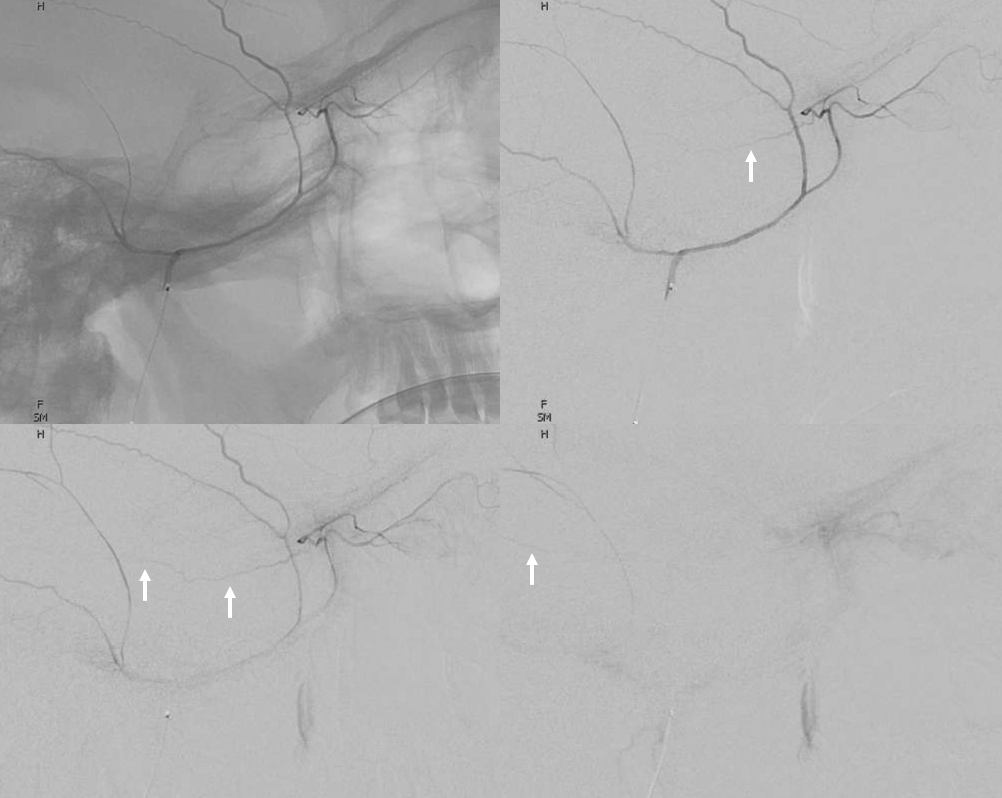
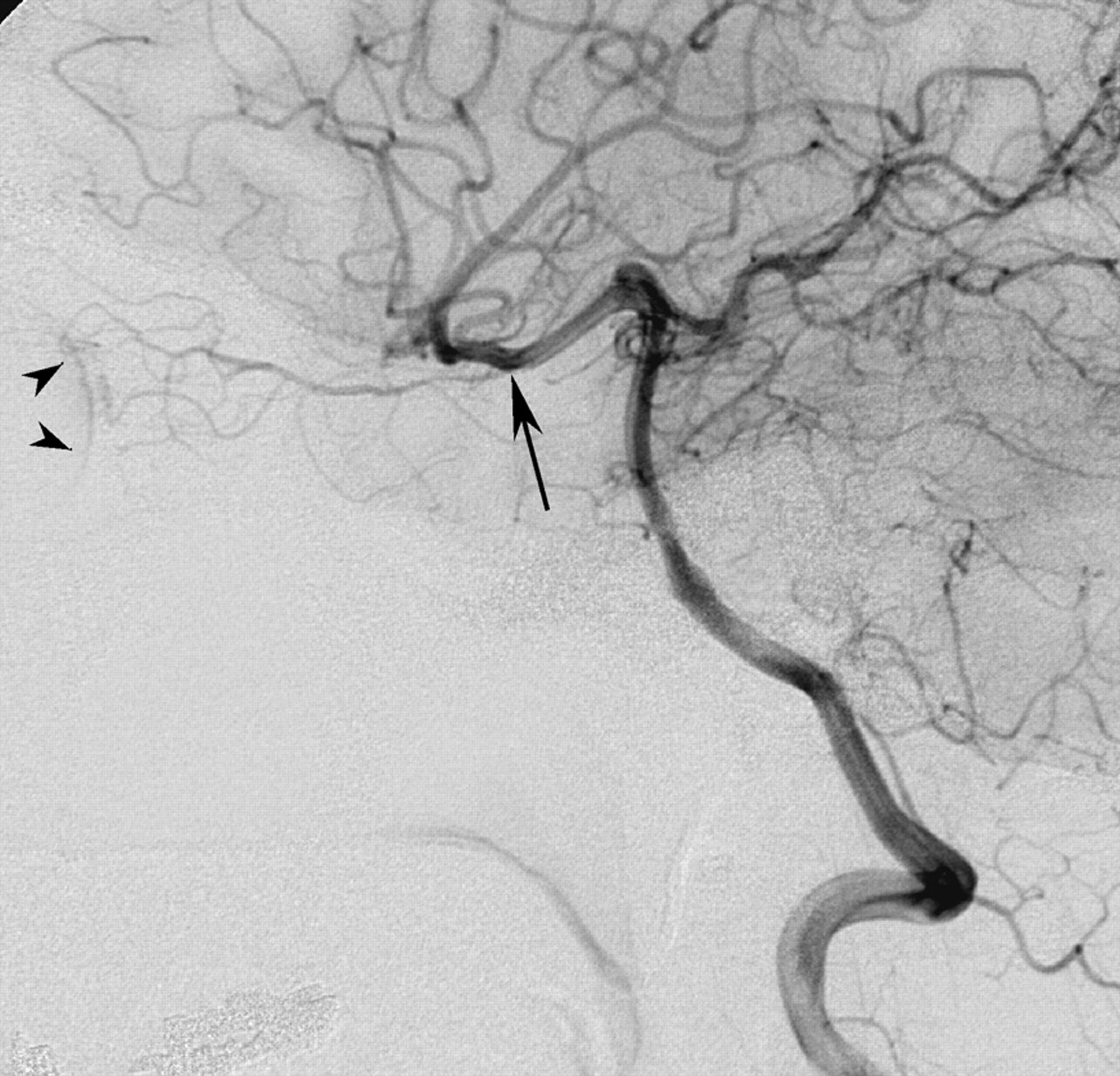
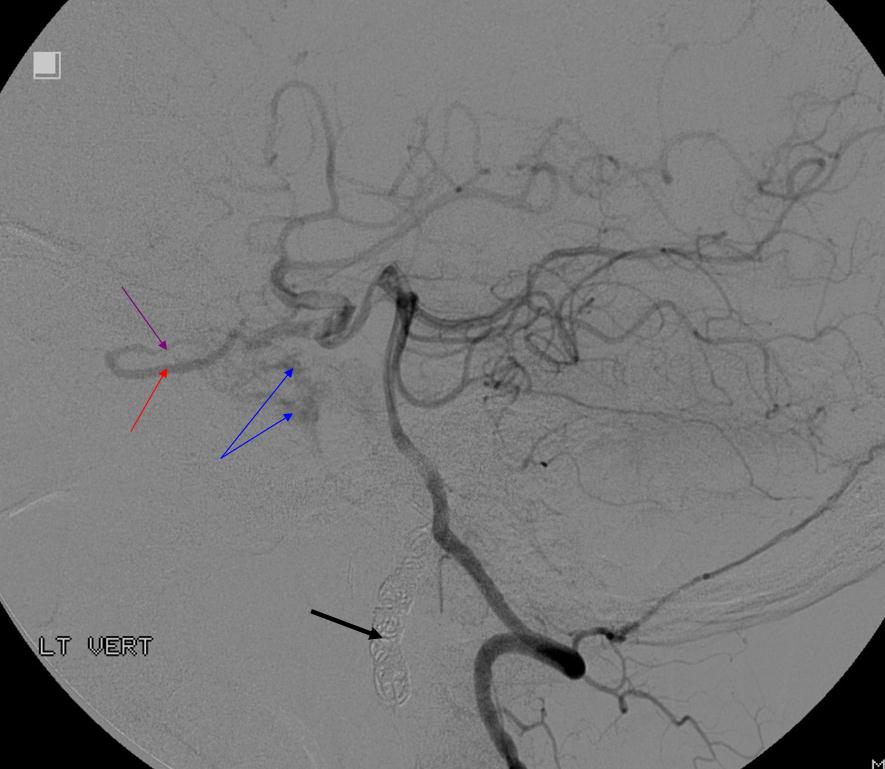
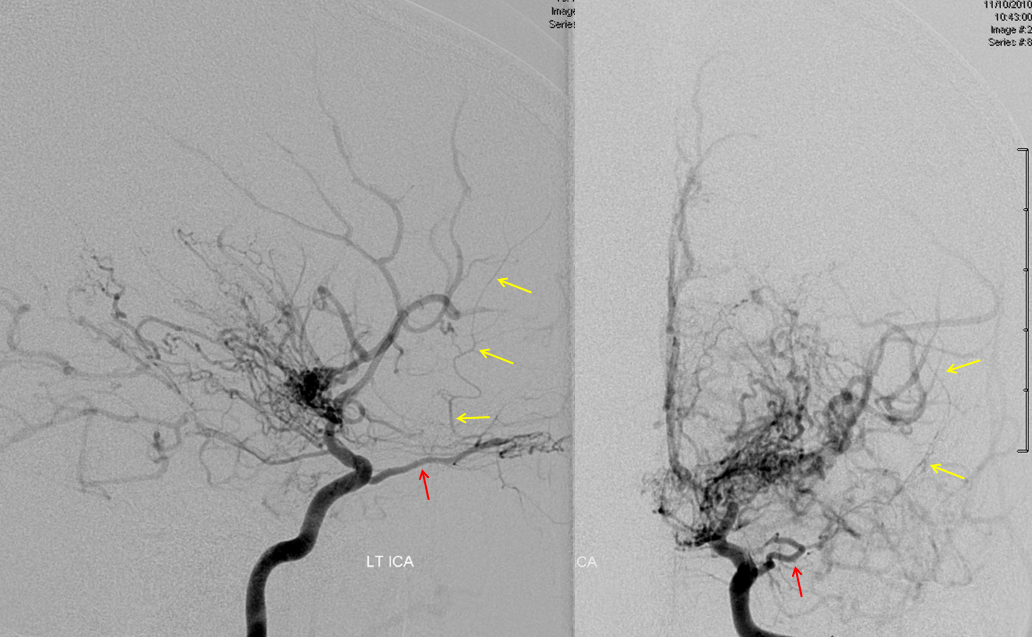
Because ventral ophthalmic represents a persistent communication between the ACOM complex and the ophthalmic artery / ophthalmic segment of the ICA, it also explains the so-called “infraoptic course” of the A1. The A1 which runs underneath, rather than over the optic nerve is nothing more than a segment of persistent ventral ophthalmic artery, in this case associated with “normal” origin of the ophthalmic artery itself. Here is an example of this variant, in a patient with a giant cavernous aneurysm — another testament to aberrant development. The infraoptic A1 / ventral ophthalmic is labeled wit the yellow arrow. The ophthalmic artery arises from the same same segment as the “A1” — as should be the case if both represent a vestige of the ventral ophthalmic artery. Notice infraoptic course on T2 MRI, and developmental ectasia of the contralateral right A1 (white arrow)Stereoscopic view of 3D-DSA, from medial to lateral, demonstrating preferential lateral aneurysm expansion and ophthalmic segment anatomy, and the infraoptic ventral ophthalmic / A1 segment. There is also a well-seen mandibulovidian artery (white arrow)Lateral projection views immediately post Pipeline embolization (top), and 4 months later (bottom). Notice branches of the MHT (purple arrows) which remain open, and are now visible after the aneurysm has disappeared. The mandibulovidian artery is again marked with white arrow.The following case, courtesy of Dr. Hima Pendharkar, National Institute of Mental Health & Neuro Sciences, Bangalore, India illustrates this connection in a patient with an unusual Moya-Moya variant characterized by occlusion of the carotid artery at the supraclinoid level, just beyond the typical origin of the ophthalmic artery. As a result of this more proximal occlusion, the typical puff of smoke collaterals between the anterior choroidal, superior hypophyseal, and lenticulostriate arteries are unavailable. Instead, one sees a pathway of “typical” ophthalmic (black arrow) to “ventral ophthalmic” ( white arrows) to anterior cerebral artery. In other words, both the typical and ventral ophthalmic arteries are present in this patient, with retrograde ventral ophthalmic flow reconstituting the anterior cerebral artery territory.
DSA of the same image, right side:
The same is seen on the left side. Notice marginal tentorial artery (Bernasconi-Cassinari) reconstituting the posterior pericalossal artery territory.
The bulk of MCA territory support comes through the PCOMs:
Also note lack of effective external carotid to internal carotid autosynangioses, which i think would reasonably be expected in this case.
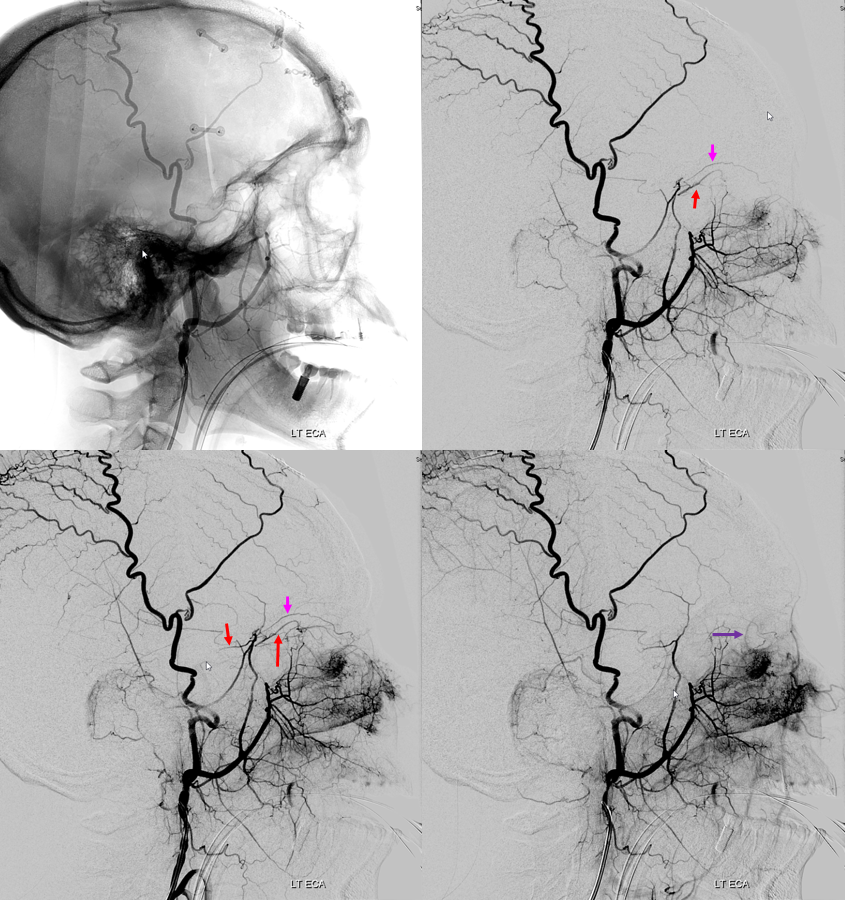
Meningo-ophthalmic Artery — an extremely important variant of the ophthalmic supply from MMA. A must-know “dangerous anastomosis”
The ophthalmic artery does not arise from the ICA. A sphenoidal branch of the MMA (B) gives rise to the meningo-ophthalmic artery (A) supplying the orbit.
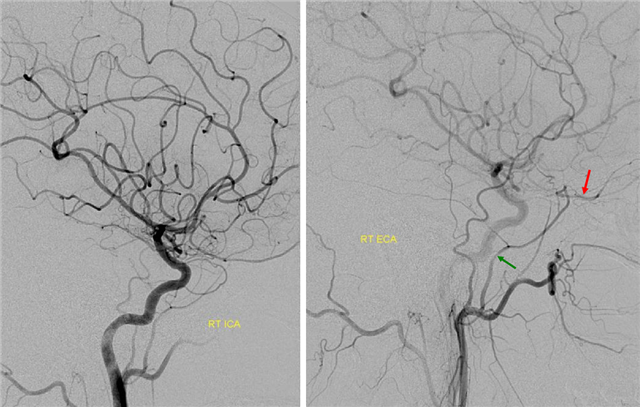
Primary ICA injection of the left with some ECA reflux demonstrates absence of “normal” ophthalmic artery origin. Primary ECA with some ICA reflux injection on the right shows the meningo-ophthalmic artery (red), a branch of the MMA (green) supplying the orbit exclusively. This is in contrast to the meningo-lacrimal variant, where said artery supplies the lacrimal (lateral) aspect of the orbit whereas a small “normal” origin ophthalmic takes care of the globe and the rest of orbital tissues. MRA of the same case is shown below.
Same case, TOF MRA: The usual origin left ophthlamic artery is faintly visible. On the right, the ophthalmic arises from the MMA. We have several other cases with MRA and angio imaging of the same variant, with less obvious correlation. One strategy for catching these is to look at ophthalmic artery origin. It is usually seen although bone and flow direction make it relatively poorly visible. Asymmetry in ophthalmic artery visualization may be normal however looking at the MMA could be worthwhile.
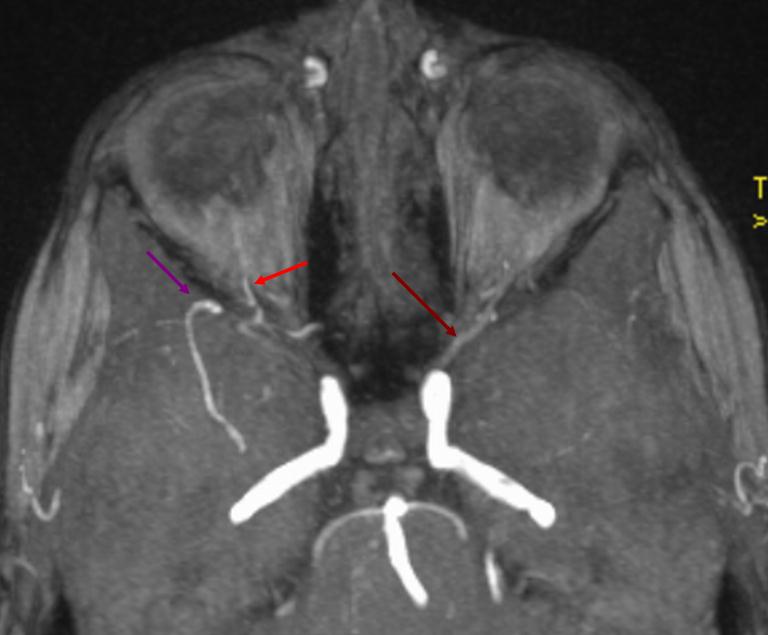
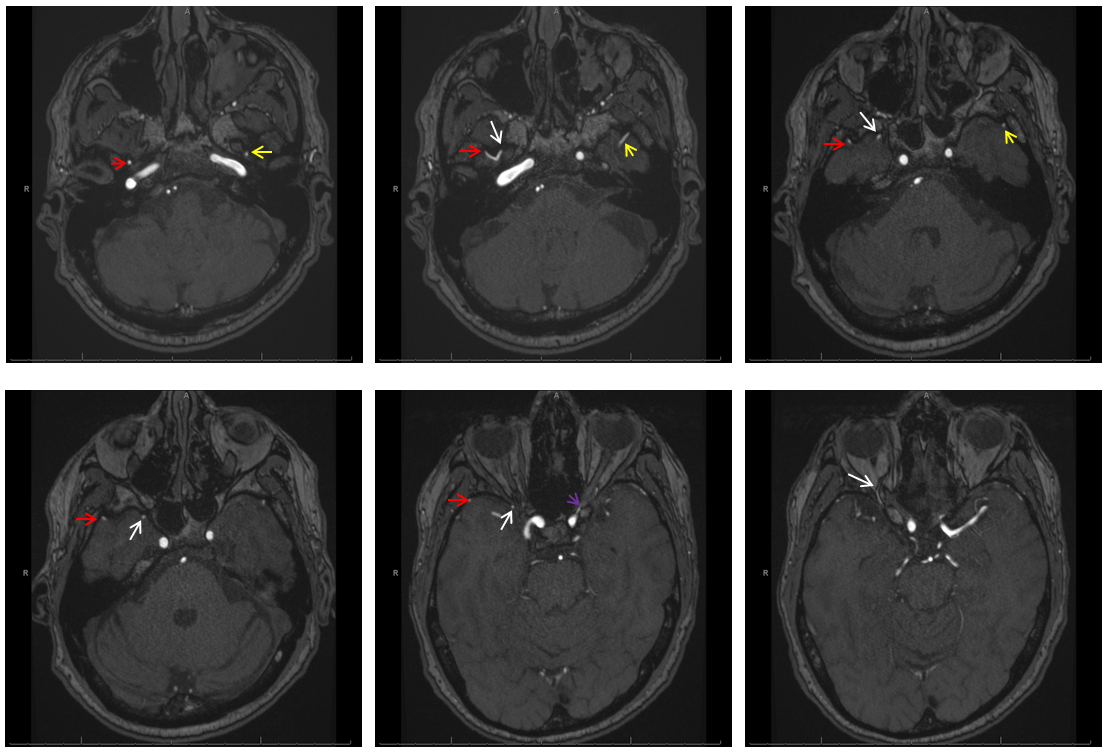
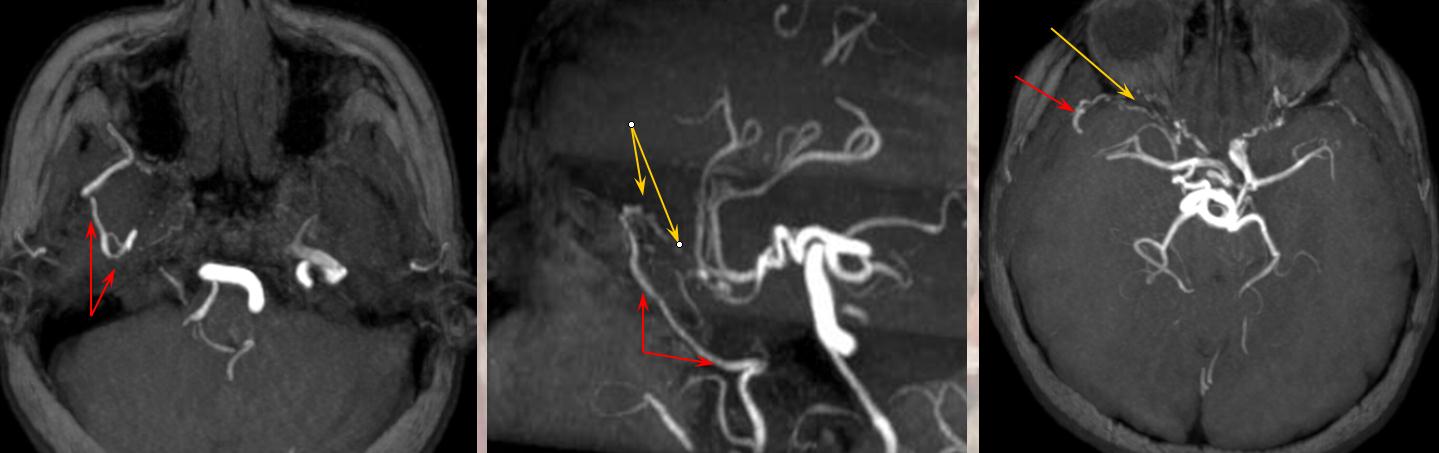
A much better MRA demonstration on a 3T magnet, otherwise normal study. A larger proximal MMA on the right (red arrow, upper right image) gives off the meningo-ophthalmic (white arrows) which can be traced into the orbit. On the left, a “standard” MMA (yellow arrows) is present, as well as normla ICA origin left ophthalmic artery (purple arrow)
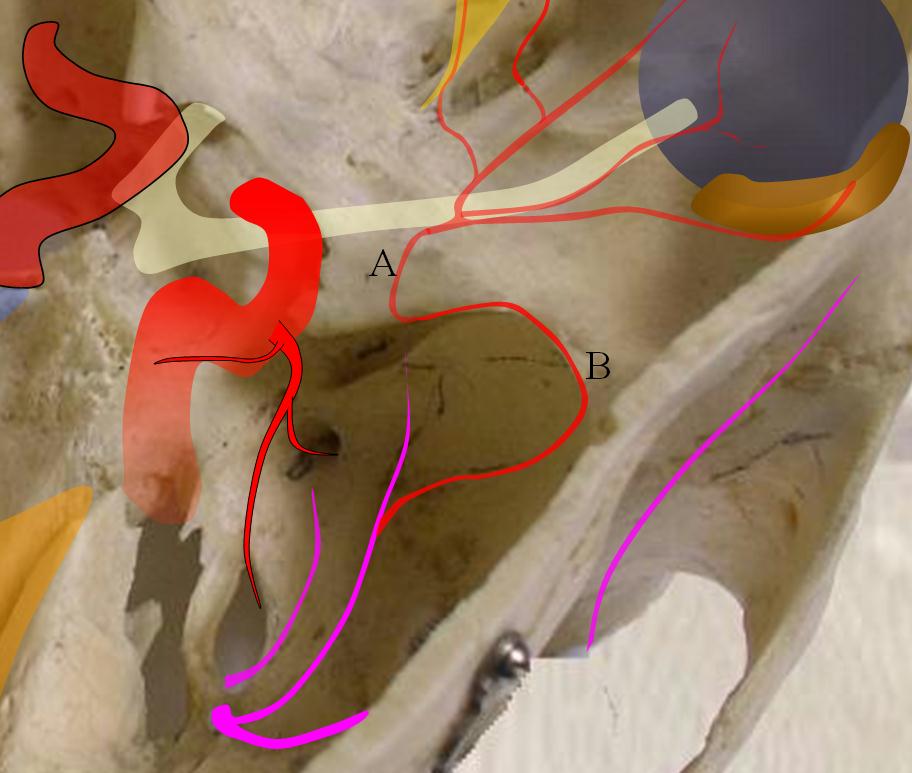
Meningo-lacrimal (meningolacrimal) variant — supply of MMA is “limited” to lacrimal gland. Usually MMA enters orbit via its own laterally placed “Foramen of Hyrtl” — in contradistinction to full meningo-ophthalmic variant when it goes thru the superior orbital fissureMeningolacrimal is white. Hyrtl foramen is blackAnother example. Angio example, with typical origin ophthalmic including choroid blush of the globeECA injection shows MMA (purple) and sphenoid branch (white) supplying via the lacrimal branch (brown) the lacrimal gland (peach). Note lateral entry of lacrimal branch into orbit (foramen of Hyrtl). A more medial branch (red) likely connects the lacrimal branch to the ophthalmic artery.
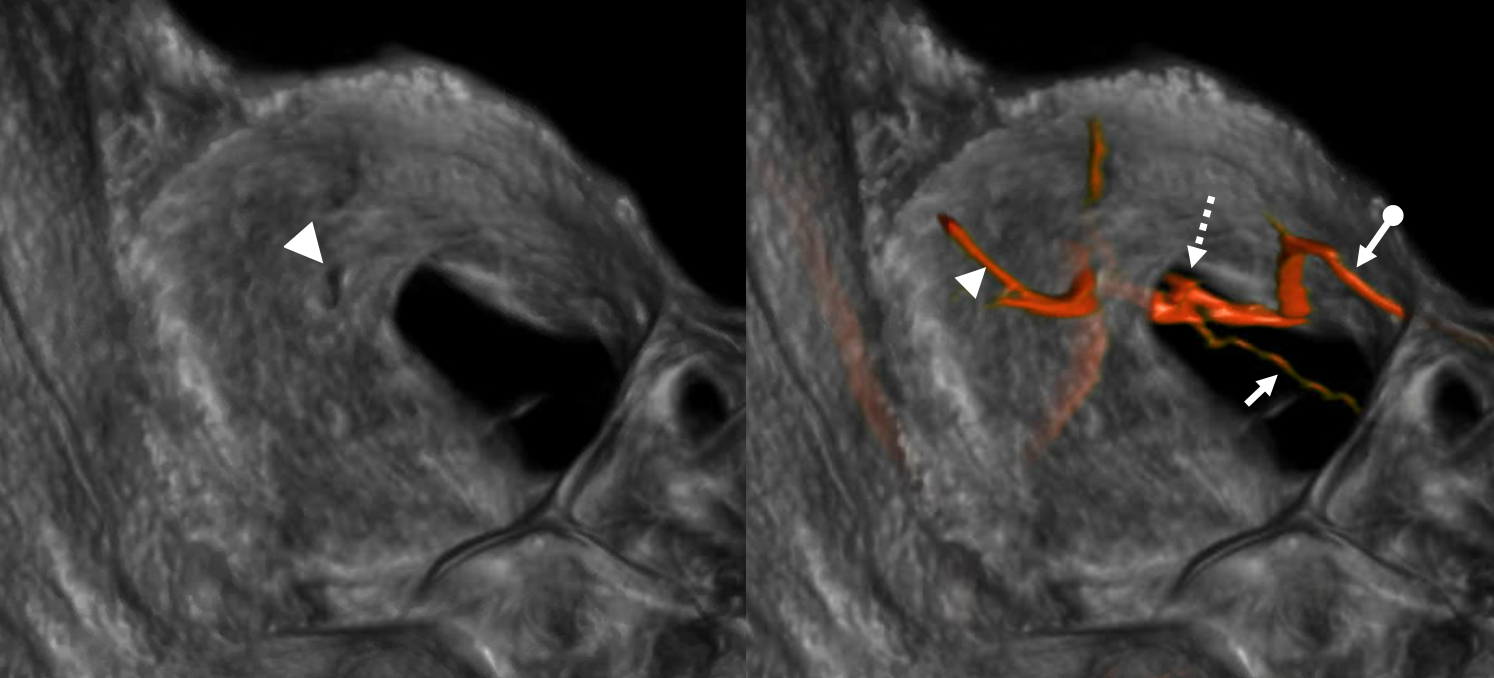
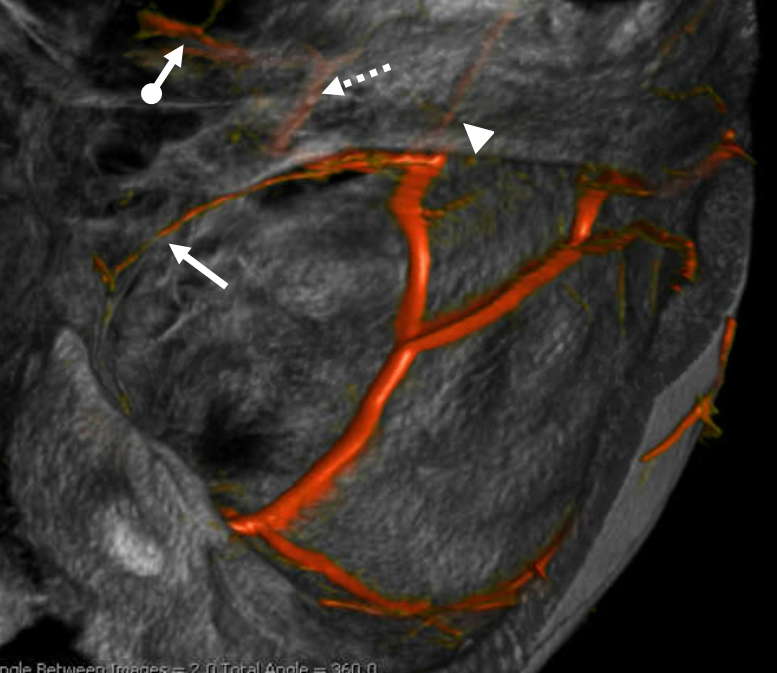
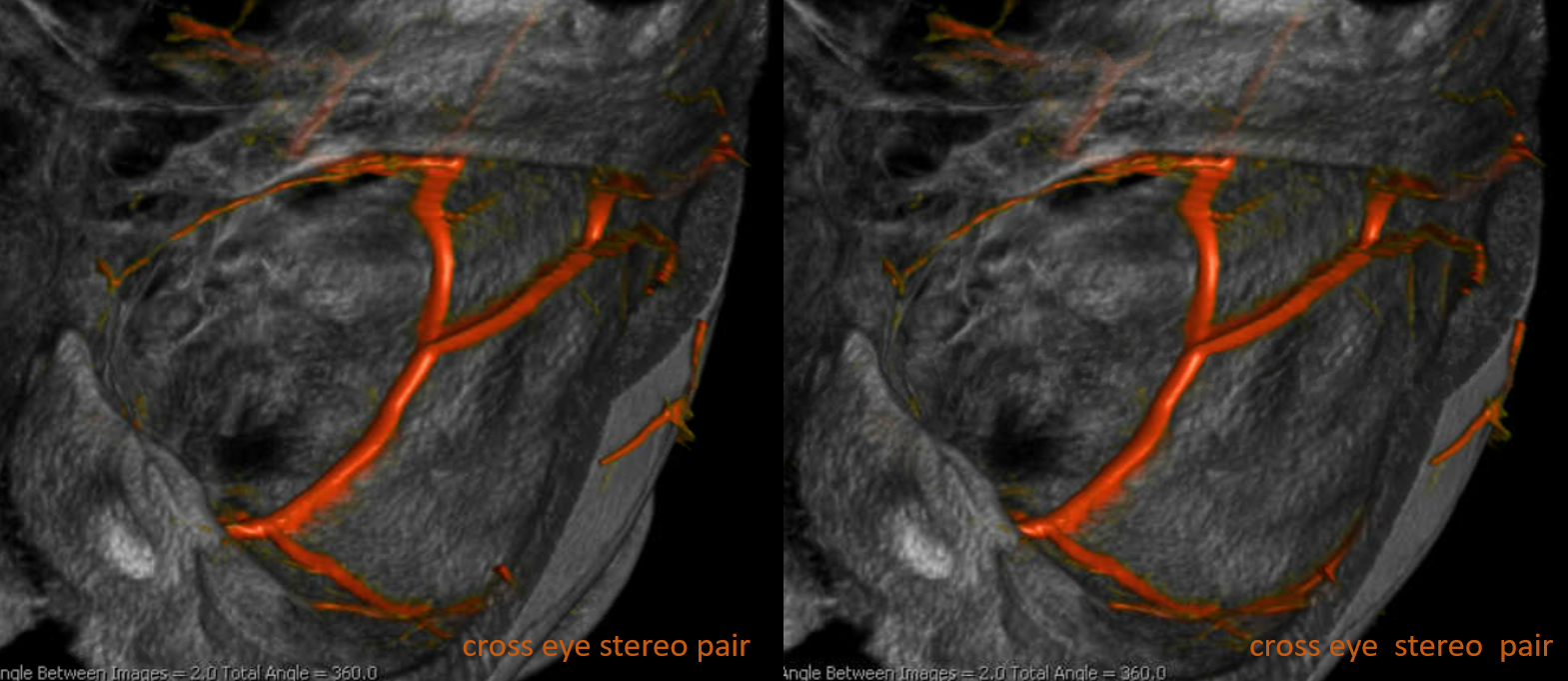
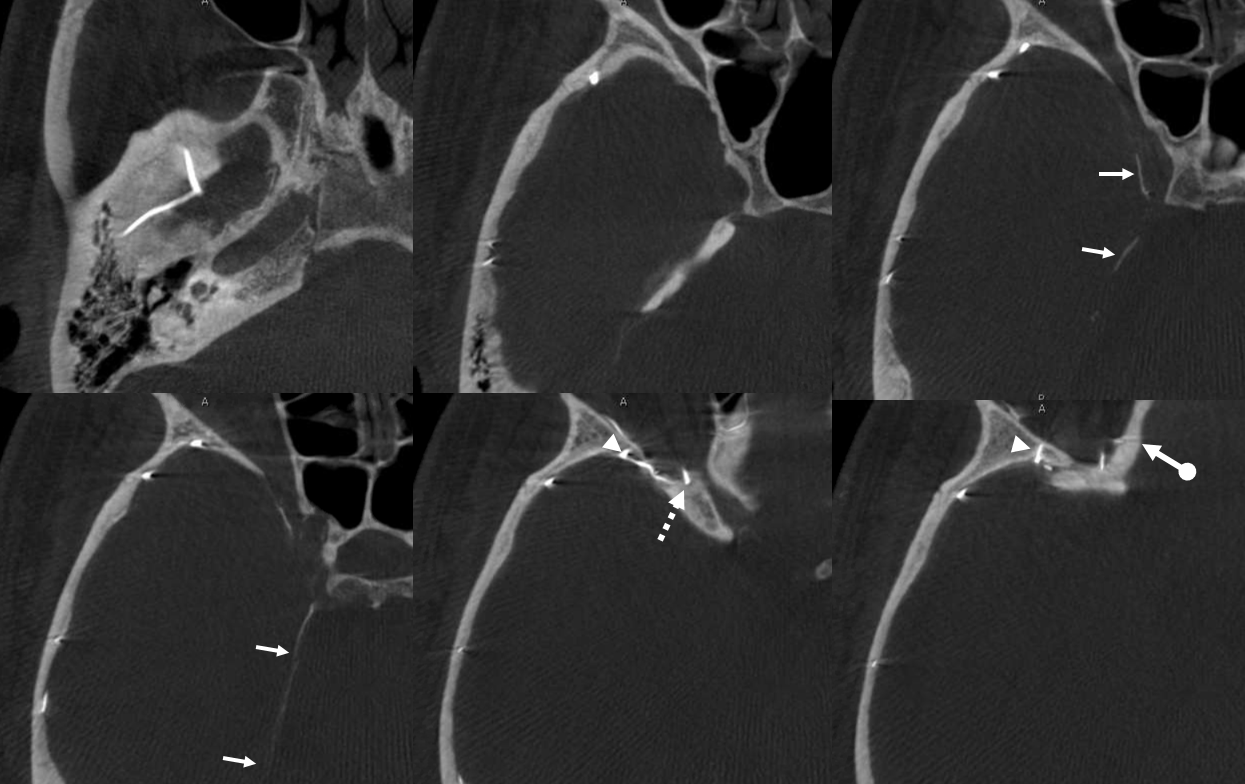
Again, there is a continuum. Bodies don’t read books. In example below, the meningeal contribution to the orbit includes both classic “meningolacrimal” artery via foramen of Hyrtl (arrowheads), and a superior orbital fissure contribution (dashed arrow) that mainly goes to the posterior ethmoidal foramen (ball arrow). Neither directly supplies the orbit. Also present is a rare but important connection to the tentorial arcade (arrow) going backwards — usually supplied by ILT.
The recurrent tentorial branch (arrows) heads far posterior to become the free margin artery (Bernasconi-Cassinari)
Movie — pause and scroll thru images
Posterior Communicating origin of the Ophthalmic Artery.
Naeini, De, Satow, and Benndorf demonstrated this unusual origin of the ophthalmic artery in a patient with ICA agenesis in AJR 2006;184:571-573 (http://www.ajronline.org/cgi/content/full/184/2/571) A very nice discussion of embryology is included there as well. How does above embryology allow for such an origin? I think the most likely possibility is not carotid agensis but aquired carotid occlusion, likely in early life, proximal to the origin of a normal disposition ophthalmic artery. The PCOM then takes over the supply of the ophthalmic artery territory. A similar disposition can be seen with iatrogenic or aquired carotid occlusions in adult life as well.
PCOM origin of the ophthalmic artery. Image from Naeini, De, Satow, and Benndorf. Unilateral Agenesis of Internal Carotid Artery with Ophthalmic Artery Arising from Posterior Communicating Artery. AJR 2006;184:571-573 http://www.ajronline.org/cgi/content/full/184/2/571. The embryologic implication of this arrangement may be that this is a result of ICA occlusion rather than agenesis. The postulate is that ICA did form, along with the ophthalmic artery, and was subsequently occluded with PCOM reconstitution of ophthalmic terrritory. This can be observed in adult as well. Below is a case of ophthalmic supply via the PCOM following ipsilateral planned ICA occlusion with coils in a case of carotid-cavernous fistula.
Adult version of ophthalmic artery (red) supply via the pcom. The ipsilateral ICA has been closed with coils (black) one week previously. Notice also a prominent recurrent meningeal artery (purple) feeding a residual cavernous carotid fistula (blue)
Recurrent Meningeal Artery — this dispositiong is complementary to the meningo-ophthalmic situation. Here, it is the ophthalmic artery that supplies territory of the middle meningeal artery through its recurrent meningeal branch (Letter F in figures above). This branch arises from the proximal ophthalmic arery and projects posteriorly through the superior orbital fissuer or through its own foramen. On occasion, it assumes supply of middle meningeal territory, via a meningeal branch of the sphenoid ridge (running along the ridge, as expected) and continuing along the inner table of the frontal bone as one or several frontal branches.
Recurrent Meningeal Artery (purple) arising from the ophthalmic artery (orange) and heading posteriorly into the middle cranial fossa. The artery assumes territory of the meningeal branch for the sphenoid ridge (red, foreshortened in lateral projection) and contiues as several branches of the frontoparietal inner table (yellow).
Recurrent Meningeal Artery (B) giving rise to the artery of sphenoid ridge (C), normally a branch of the middle or accessory meningeal artery.
Recurrent Meningeal Artery2: On head CT, aberrant MMA origin can be inferred by absence of foramen spinosum (or a much smaller foramen than contralaterally, attesting to asymmetery in MMA size.) The contralateral foramen spinosum is labeled in blue. The recurrent meningeal artery travels along the sphenoid ridge (orange arrows) and then over the convexity (red arrows)
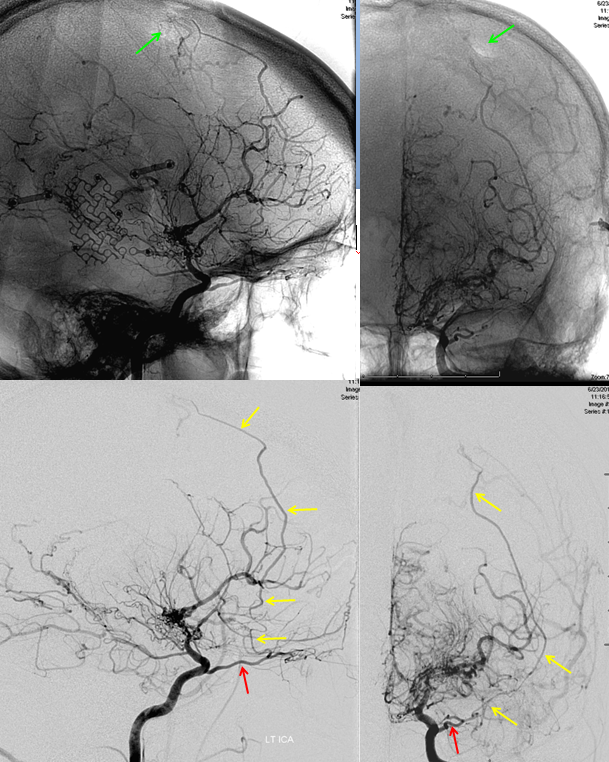
Recurrent meningeal artery in setting of Moya-Moya / synangiosis
Pre-surgical AP and lateral images, demonstrating a recurrent meningeal artery (meningeal vessels can be prominent in patients with Moya-Moya and other chronic progressive occlusive disease, reflecting autosynangiosis)
Ophthalmic – red. Recurrent Meningeal – yellow.
The patient underwent surgical synangiosis with craniectomy and burr holes. Post-operative imaging (obtained 6 months after surgery) demonstrates significant interval enlargement of the recurrent meningeal, which is reconstituting pial circulation at the location of the superior frontal burr hole (green arrows)
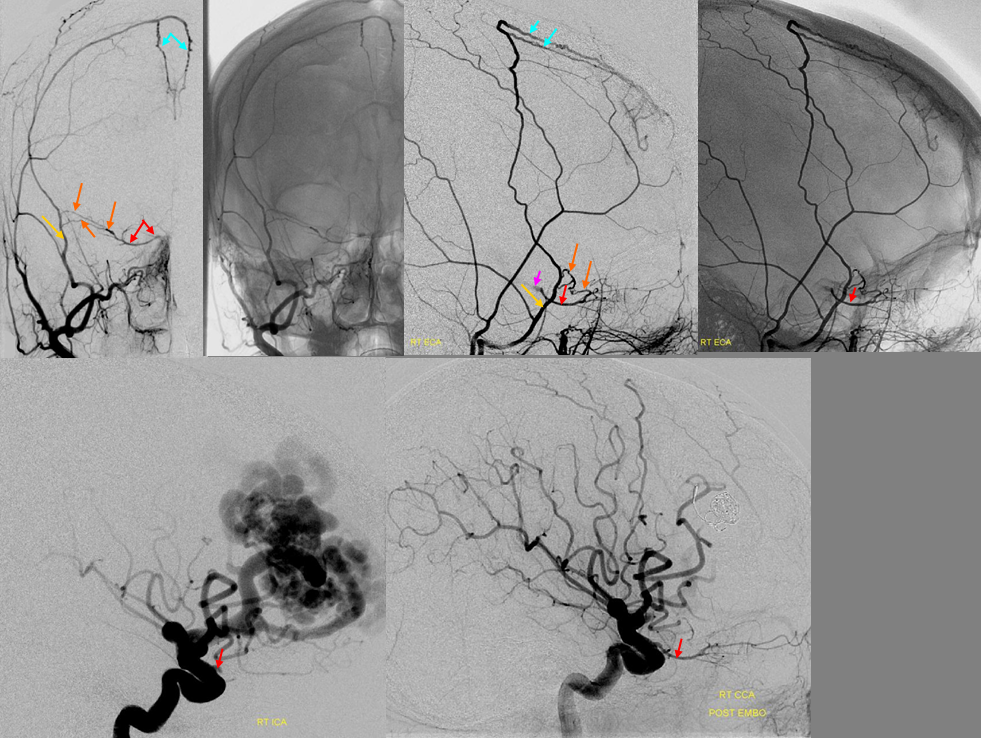
Sphenoid Branch reconstitution of the ophthalmic artery. Ophthalmic artery flow is reversed due to sump from a frontal AVM. Robust sphenoid ridge branches help fill the ophthalmic artery which is barely seen on the pre-embolization injection. Following embolization, normal anterograde flow in the ophthalmic is re-established.
Red=ophthalmic artery. Purple = ICA blush. Orange=sphenoid ridge branch of the MMA. Yellow=MMA.
Recurrent Meningeal Artery, extremely large.
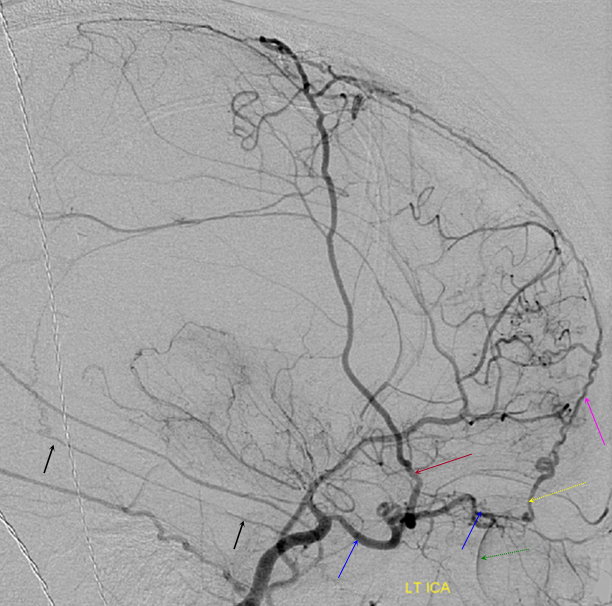
An unfortunate child extensively irradiated in his home country with subsequent development of radiation angiopathy. A moya-moya pattent is seen on this ICA injection. An absolutely enourmous recurrent meningeal artery (red) arising from a large ophthalmic (blue) supplies portions of the cerebral hemipheres thru pial collaterals. Notice ACA evidence of ventriculomegaly and a large anterior ethmoidal artery (yellow) giving rise the the artery of the falx cerebri (pink). The choroidal blush is labeled in green. Also present is a large marginal tentorial artery (Bernasconi-Cassinari) supplying the posterior falx cerebri (black)
Co-dominance — this patient has a robust connection between “normal” ophthalmic artery and MMA. Like any ICA reconstitution by ophthalmic — the connections are always there. Here is a “normal” origin ophthalmic (red), giving off ethmoid brach (pink) with choroid blush of globe in venous phase (purple)
External carotid injection, lateral views, shows sphenoid branch connection with the ophthalmic artery and is branches (same arrow colors)
Anterior Frontal Meningeal Branch, patient with NFII
Stereo injections of the left common carotid artery in an NFII patient with a large frontal falx meningioma. Notice mass effect on the anterior cerebral artery (MRI below). The anterior frontal meningeal branch (red) of the ophthalmic artery can be seen in stereo to course laterally along the convexity and not in the midline, where without stereo it may be mistaken for a posterior ethmoidal artery of the falx. The falxine artery (purple) participates in supply of the meningiomas, as expected. Notice prominent contribution from a falxine branch (orange) of the anterior cerebral artery. The anterior choroidal artery (blue) is prominent, an anatomical variant whereby the vessel retains much of its embryonic cortical territory. Notice how its origin is inseparable on these projections from the PCOM (green) leading to erroneous descriptions of “duplicated PCOM” in older literature. In fact, a duplicated PCOM is impossible. An enlarged posterior clival branch of the MHT is labeled in purple.
Supraclinoid ICA fenestration, case courtesy of Drs. Eytan Raz and Howard Riina. Some believe that the rare supraclinoid ICA fenestration is related to migration of the primitive ventral ophthalmic artery to its usual position. There is no certainty in that, in my opinion, but nevertheless this curious case can be shown here as an embryologic possibility. See Lasjaunias and Berenstein for further details. Of the 10 or so cases in the literature to date, many seem to be associated with aneurysms and about 2/3 are on the right side, as is ours. No aneurysm however.
Angio of the same patient. Notice a large recurrent meningeal artery as well.
Ethmoidal arteries — anterior falcine artery.
Prominent Anterior Falcine Artery (red arrows) originating from the ethmoid branches of the ophthalmic artery supplies the falx. This is often seen in setting of middle meningeal artery takedown/sacrifice, such as after pterional craniotomy. Notice a large run of surgical staples (blue) and various electrodes (purple) in this patient with subdural grids and other hardware of epilepsy surgery.
Ethmoidal Arteries — Nasal branches.
Common Carotid Injection, status-post epistaxis embolization. The IMAX distal to the MMA (light blue) has been closed with coils (black). Nasal mucosa is now supplied by inferior nasal branches (red) of ethmoidal artery coming off the ophthalmic (yellow). These branches cannot be embolized without catheterizing and embolizing through the ophthalmic artery and risking blindness (i say its not worth it) — surgical clipping/buzzing via a small incision near the nasal bridge is the prefered method of treatment should epistaxis recur. Usually it does not, even if these branches are present. Also notice very faint anterior falcine (purple) branche of the ethmoidal artery. The artery labeled with orange arrow is another branch vascularizing the posterior portion of the nasal septum and nasal mucosa.
Lateral Projection demonstrating unusually prominent participation of the ophthalmic thru ethmoid branches (red) of the nasal mucosa. The mucosal blush is well seen. A superficial nasal septal branch is purple
AP COMMON carotid injection of the same case with prominent ethmoidal branches (red) giving a nasal mucosal blush. Sphenopalatine septal and lateral branches (yellow) of the IMAX are visible also.
Another example, in stereo, of incidentally prominent ophthalmic dominance in supply of both nasal (ethmoidal = pink, skin dorsal nasal = white) and forehead (purple) soft tissues
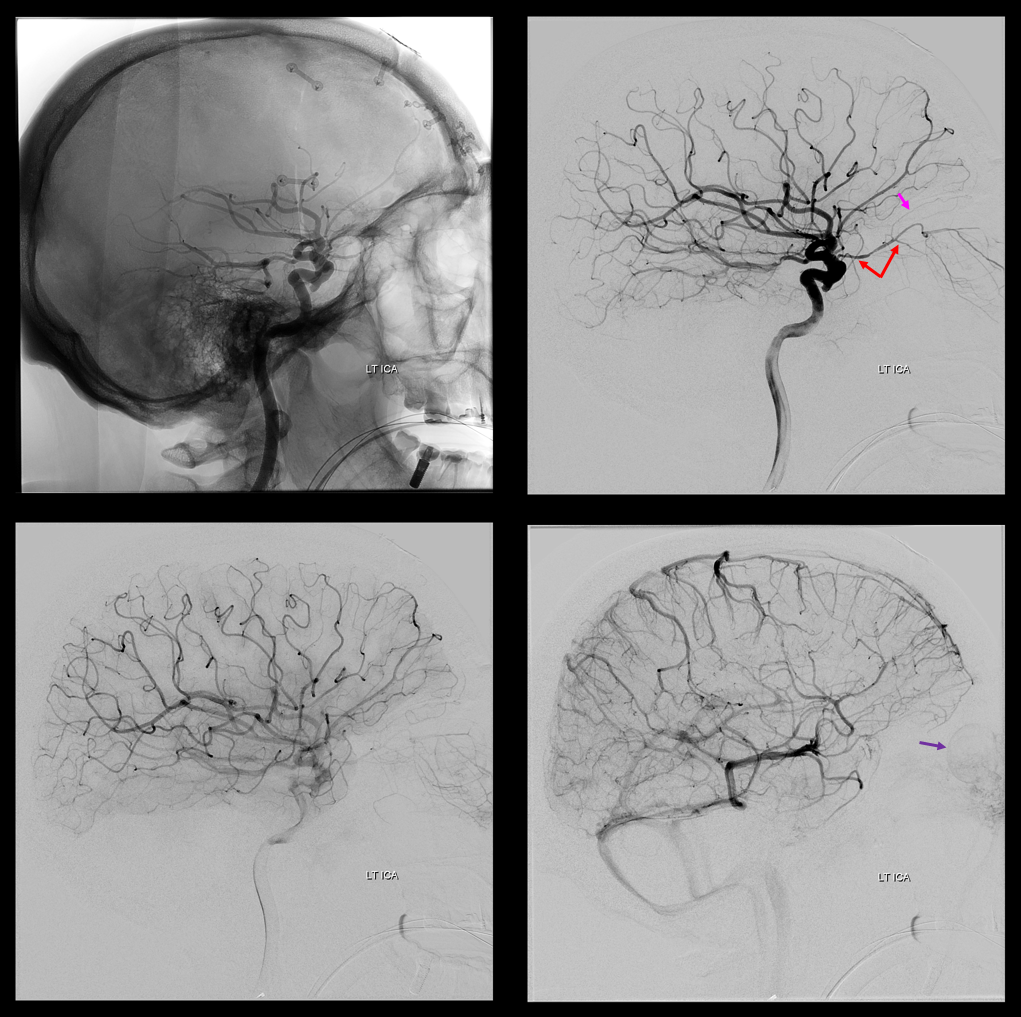
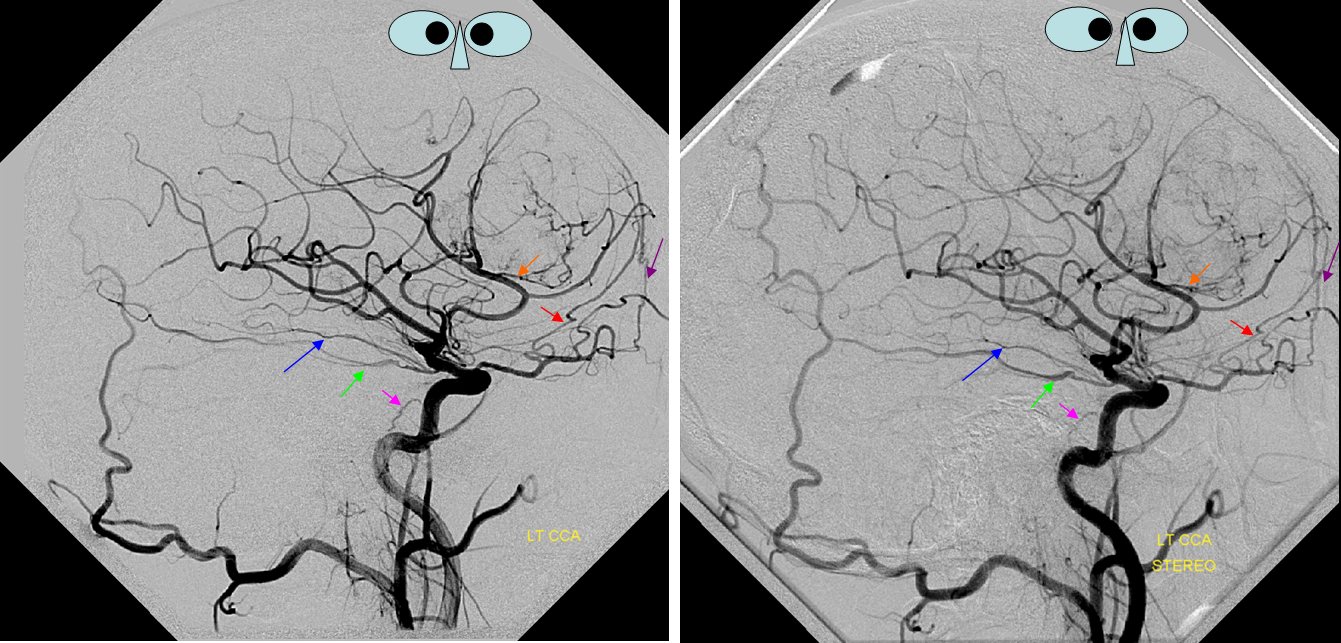
In the typical scenario of common or internal carotid injection, the intraorbital branches may not be sufficiently well seen — the bulk of contrast is consumed by the brain. The way to get detailed views is to either perform a direct intra-ophthalmic arterial injection (the few of us who do retinoblastoma chemotherapy have the world’s largest experience — AND ARE WELCOME TO CONTRIBUTE IMAGES!) or to wait for a case where the bulk of flow is directed into the ophthalmic artery, i.e. one of supraclinoid carotid occlusion. In this case of acute stroke, we had a few moments between revascularization steps to acquire a set of decent stereo images.
A stereo image of similar situation. As always there is variability everywhere. In this case the ophthalmic artery supply is limited to portions of the orbit, without supply to the lacrimal gland, and no ethmoid contribution. Notice also amazing view of the subependymal venous system.
Venous phase showing hypoplasia of the inferior ophthalmic vein
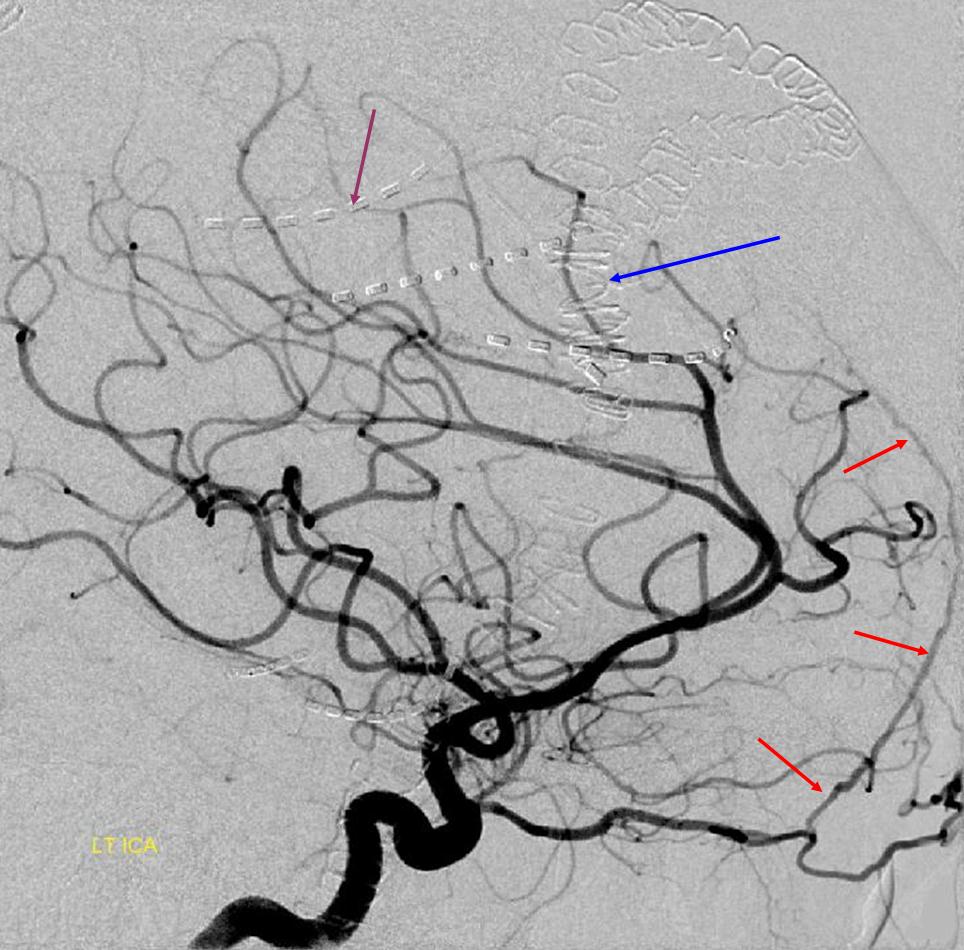
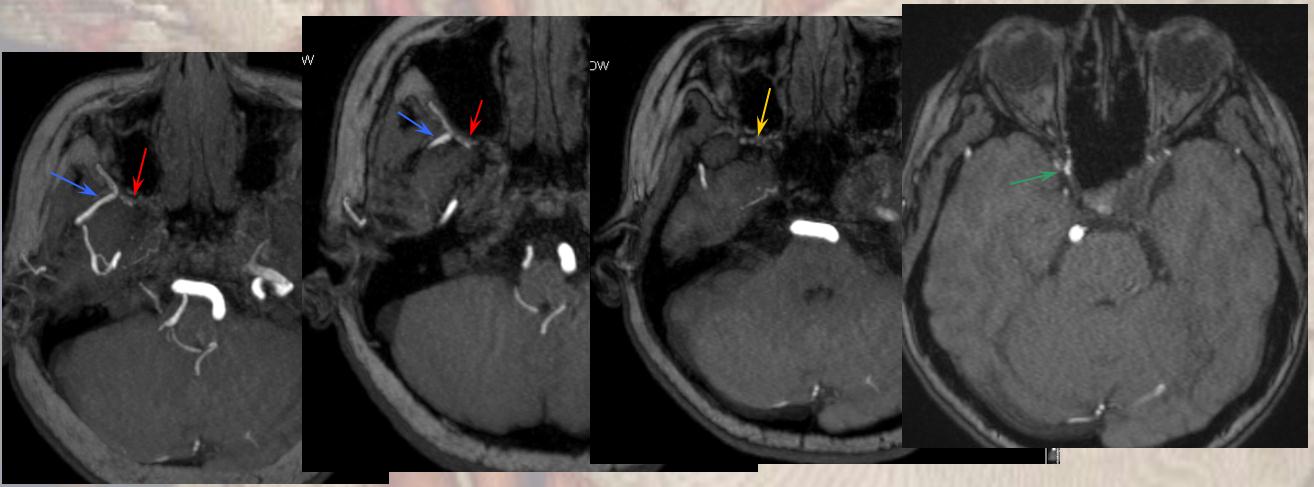
The classical intradural ophthalmic is seen here. The portion inside the bony optic canal is betwene the white arrows. You can imagine the nerve sitting on top of the artery there, like this:
In many cases, the ophthalmic artery will turn to lie superior and lateral to the nerve, at the level of the blue arrows. This turn is a vestige of the embryonic ophthalmic ring formed by the union of dorsal and ventral contributors to the intraorbital tissues. At this point, the vessel will typically give off the critical cilliary and central retinal arteries (yellow). The central retinal artery is too small to be resolved in most cases. The cilliary arteries (a.k.a. choroidal but this name is confusing for obvious reasons) will supply the choroid of the eye, which is responsible for the choroid blush. It is important to understand that seeing the choroid blush does not guarantee presence of vision — the central retinal artery may in fact be completely occluded. Vice versa is also true — one can have absent choroid blush and preserved vision — we have a lucky case like that ourselves. The critical thing to understand is that the central retinal artery is an early branch of the ophthalmic, in most cases.
Beyond this, one can essentially guess the name and function of the branch based on where its going. Laterally in the orbit there is the lacrimal gland and lacrimal branches (black arrows). The lacrimal blush is usually well-seen, and particularly well so in nervous/emotional patients. In this case, there are cutaneous branches going over the zygoma beyond the lacrimal gland (rightmost black arrow on the AP view — this will collateralize with the deep temporal arteries — see below). Also notable are branches to the inferior rectus (orange), superior rectus (brown), anterior meningeal branch (green). This patient has prominent supra-orbital artery (pink) which emerges from the supra-orbital foramen. That’s why the main stem of the ophthalmic artery continues in that direction in this patient. Importantly, one can see posterior ethmoid artery (red) supplying the nasal septum (light blue, see cases above). Also present are superior (purple) and inferior (light green) palpebral arteries to the eyelids. Here are the promised stereos, which make the whole thing much easier to see:
Opthalmic artery reconstitution of the ICA
The opthalmic artery represents the most common pathway of retrograde reconstitution of the ICA following a more proximal acquired occlusion. All of the above depicted ECA to ophthalmic anastomoses can participate in suppying the ophthalmic artery, which reverses flow into the ICA and reconstitutes brain parenchyma. Statistically, the most frequently recruited collateral routes are through the anterior deep temporal artery and middle meningeal artery, with less important contributions from the angular and infraorbital channelsand. Other common pathways of ICA reconstituion not involving the ophthalmic artery utilize the ILT via the IMAX (usually foramen rotundum, MMA thru its cavernous and sphenoid ridge branches, and accessory meningeal thru foramen ovale) Below are some examples:
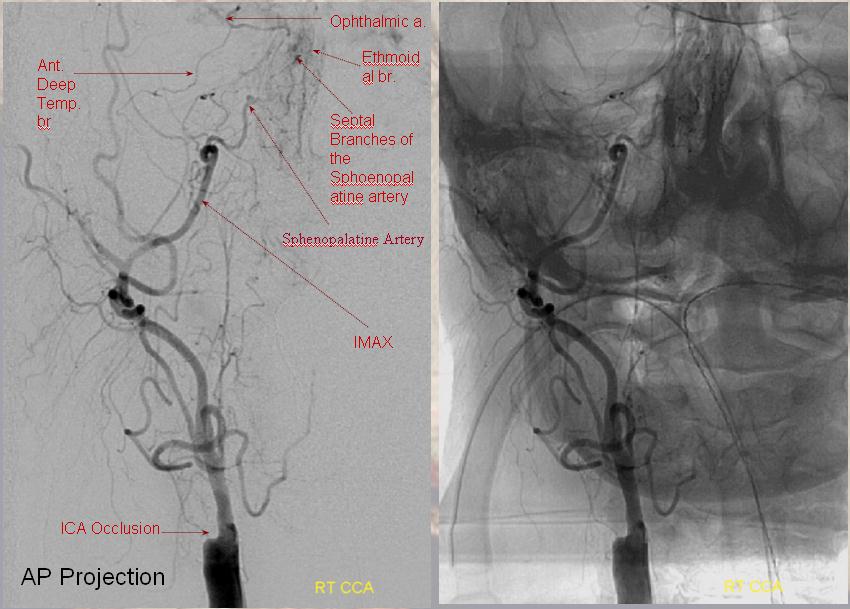
Ethmoidal and Anterior Deep Temporal Reconstitution of ICA
AP projection (above) and Lateral (below) demonstrating complete Right ICA occlusion. The ophthalmic artery retrogradely reconstitutes ICA flow through anterior deep temporal collateral to the lacrimal branches and sphenopalatine IMAX branches collateralizing with ethmoidal branches of the anterior and posterior septum (a.k.a. red and orange arrows of the case immediately above)
ICA occlusion with ILT and ophthalmic reconstitution. The sphenoidal branch (green, best seen on AP and foreshortened on the lateral) of the MMA (yellow) reconstitutes the ophthalmic artery (Blue). Cavernous branches of the MMA (red) also participate in reconstitution of the inferolateral trunk region (brown)
Lateral and AP views of another case showing robust retrograde flow in the ophthalmic artery (red) from sphenoid brach (yellow) of the MMA (blue) and from setal branches of the distal IMAX into the ethmoid branches of the ophthalmic (purple)
Noninvasive imaing of ophthalmic ICA reconstitution: Present day TOF MRA on a 1.5 T machine can be quite effective in visualizing these collaterals especially when one knows where to look for them.
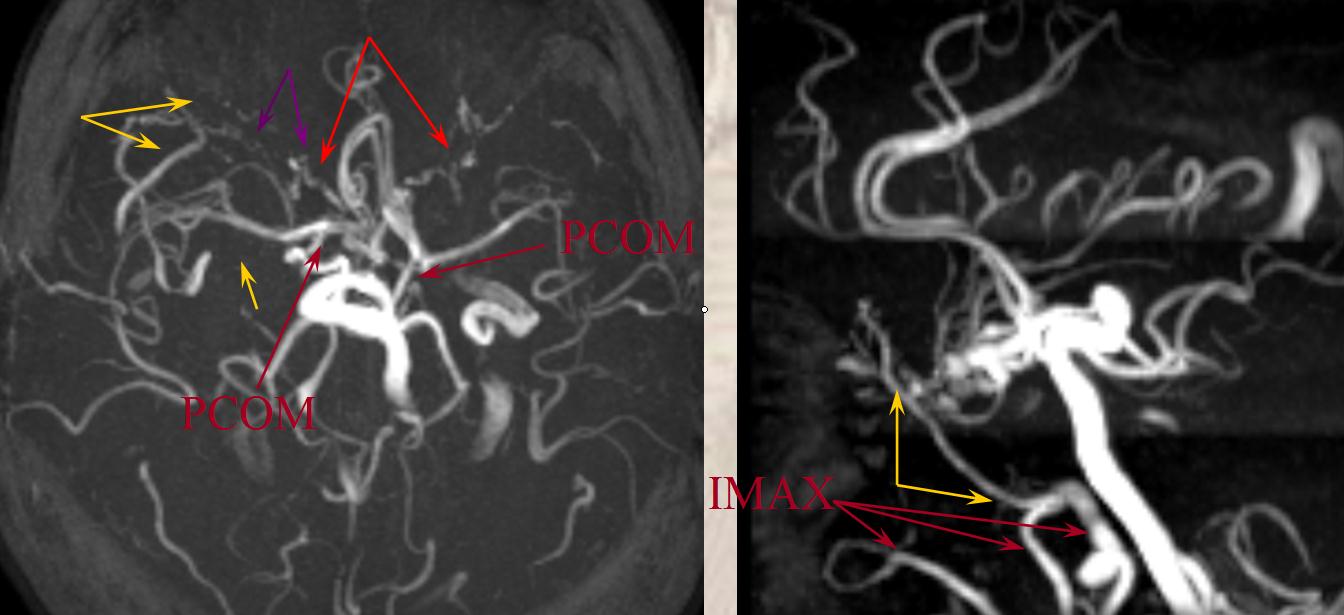
Standard projection maxiumim intensity (MIP) projection MRA images demonstrate bilateral intracranial ICA occlusions. The left vert and basilar are tortuous and prominent. Both PCOMs are large and undoubtedly help reconstitute ICA territory. Notice also the tortuosity and prominence of vessels in bilateral ophthalmic regions (red arrows), attesting to presence of robust ophthalmic ECA-ICA anastomoses. The largest of these is a markedly hypertrophied right MMA (yellow arrows)
Targeted MIP images highlight the course of the right MMA (red arrows), which reconstitutes the right carotid at the ophthalmic segment through the artery of the sphenoid ridge (yellow arrows). Other IMAX non-ophthalmic collaterals are also present.
Another likely route is from the distal internal maxillary within the prerygopalatine fossa. This IMAX (blue arrow) takes a superficial course relative to the lateral pterygoid muscle, and gives off a medially-oriented branch (red arrow) which likely connects to a faintly seen area of flow-related signal in the region of the pterygopalatine fossa (yellow arrow), and extending posteriorly towards the lateral border of the cavernous sinus (green arrow). This is most probably a foramen rotundum branch-ILT anastomosis (see ILT as well)




 Cross-eye stereo
Cross-eye stereo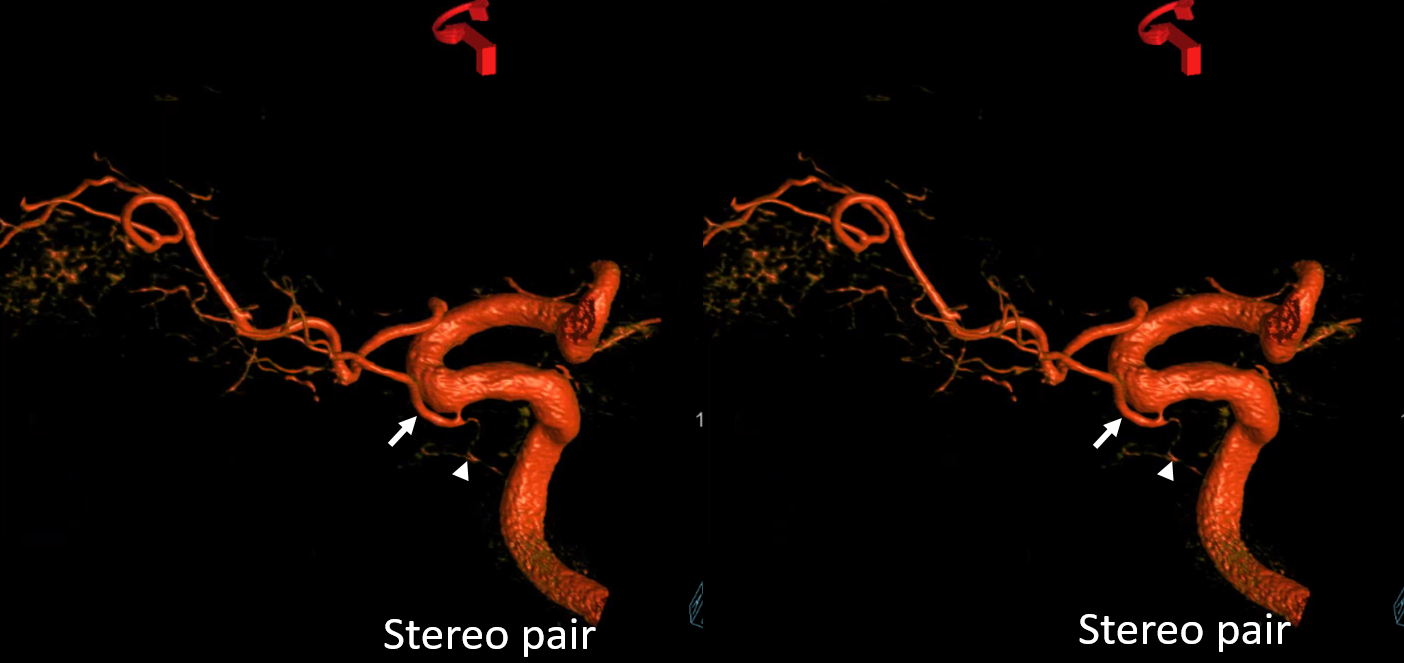 Anaglyph
Anaglyph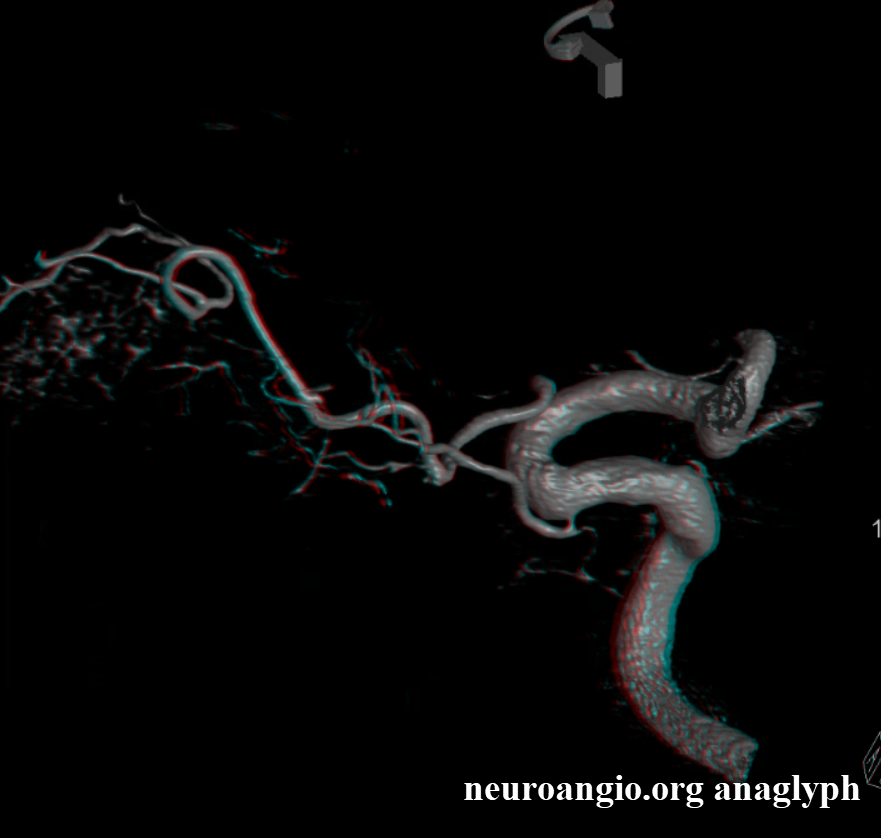 Loop cross-eye stereo
Loop cross-eye stereo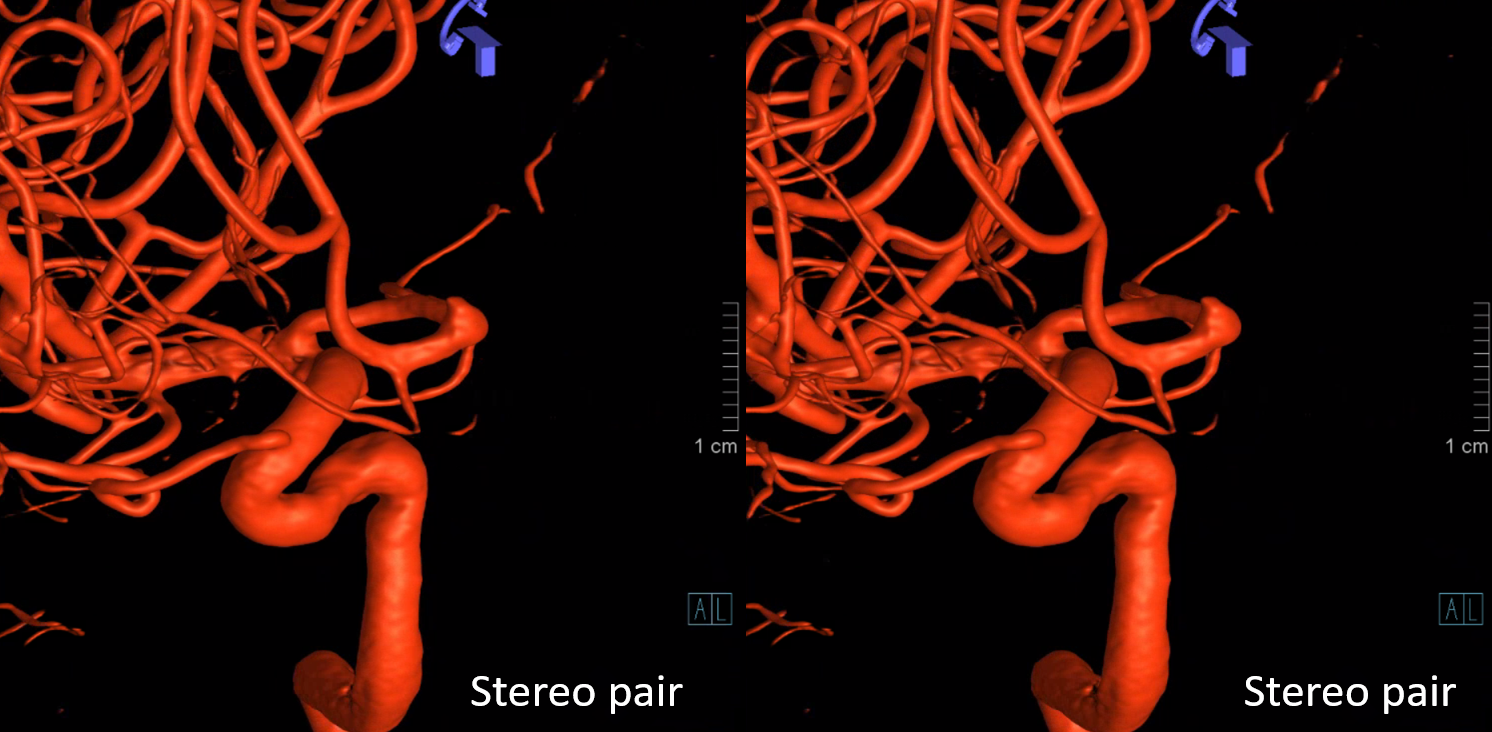 Anaglyph
Anaglyph Another example of such a ring in a different patient on DYNA CT
Another example of such a ring in a different patient on DYNA CT Ventral Ophthalmic ArteryThis variant is extremely rare in the human — a persistent embryonic connection between the area of the anterior communicating artery and the intraorbital ophthalmic — (A) in the diagram below:
Ventral Ophthalmic ArteryThis variant is extremely rare in the human — a persistent embryonic connection between the area of the anterior communicating artery and the intraorbital ophthalmic — (A) in the diagram below:
 Stereo pair in frontal oblique position, demonstrating associated A1 segment fenestration (black arrows), an embryologic variant closely tied to the ventral ophthalmic artery — the infraoptic course of the A1
Stereo pair in frontal oblique position, demonstrating associated A1 segment fenestration (black arrows), an embryologic variant closely tied to the ventral ophthalmic artery — the infraoptic course of the A1 Beautiful stereo pairs
Beautiful stereo pairs  Another example of ventral ophthalmic artery (white arrows) with choroid globe blush in parenchymal phase (black arrows) in a patient with a giant, partially thrombosed ACOM aneurysm, courtesy Dr. Peter Kim Nelson.
Another example of ventral ophthalmic artery (white arrows) with choroid globe blush in parenchymal phase (black arrows) in a patient with a giant, partially thrombosed ACOM aneurysm, courtesy Dr. Peter Kim Nelson. 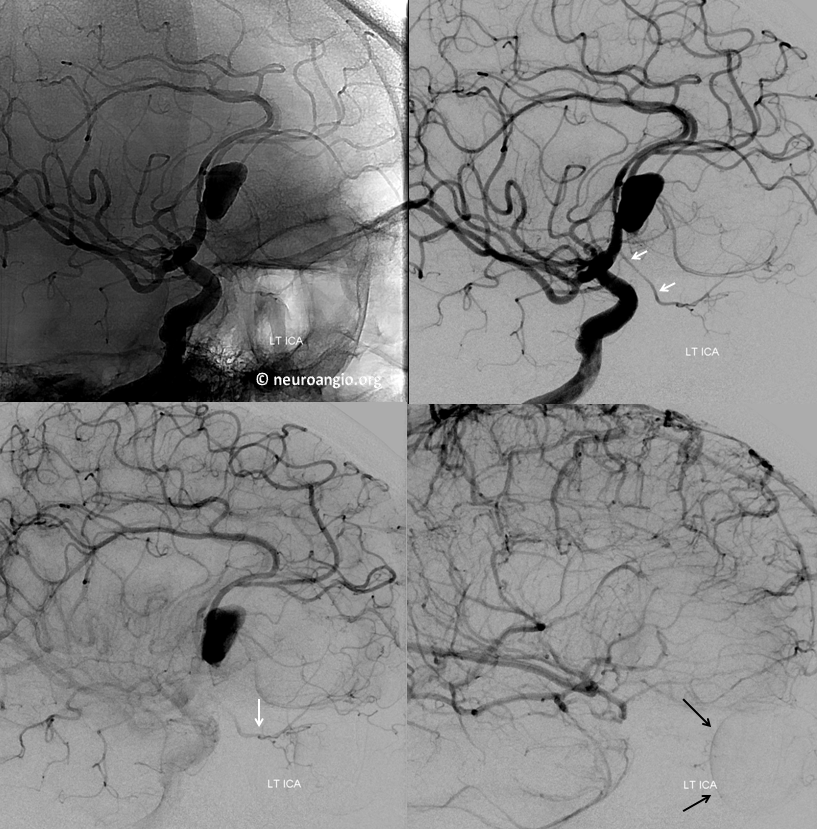 Stereo pairs
Stereo pairs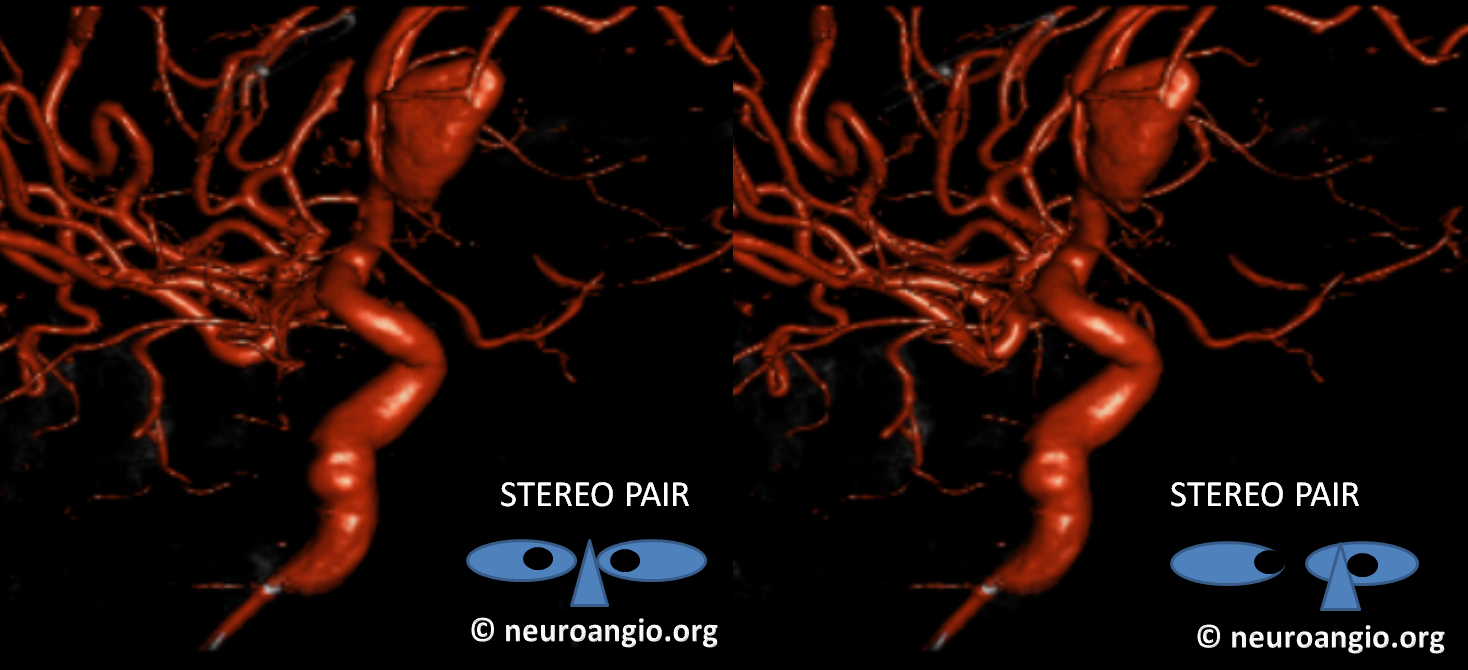
 Stereoscopic view of 3D-DSA, from medial to lateral, demonstrating preferential lateral aneurysm expansion and ophthalmic segment anatomy, and the infraoptic ventral ophthalmic / A1 segment. There is also a well-seen mandibulovidian artery (white arrow)
Stereoscopic view of 3D-DSA, from medial to lateral, demonstrating preferential lateral aneurysm expansion and ophthalmic segment anatomy, and the infraoptic ventral ophthalmic / A1 segment. There is also a well-seen mandibulovidian artery (white arrow)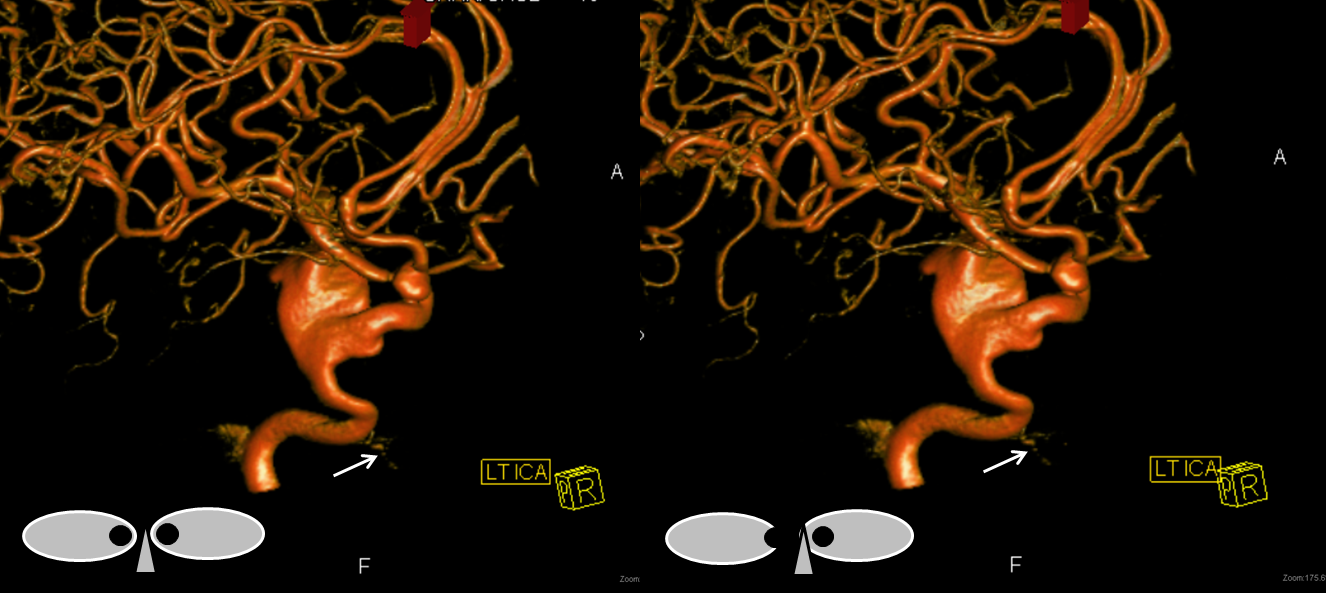 Lateral projection views immediately post Pipeline embolization (top), and 4 months later (bottom). Notice branches of the MHT (purple arrows) which remain open, and are now visible after the aneurysm has disappeared. The mandibulovidian artery is again marked with white arrow.
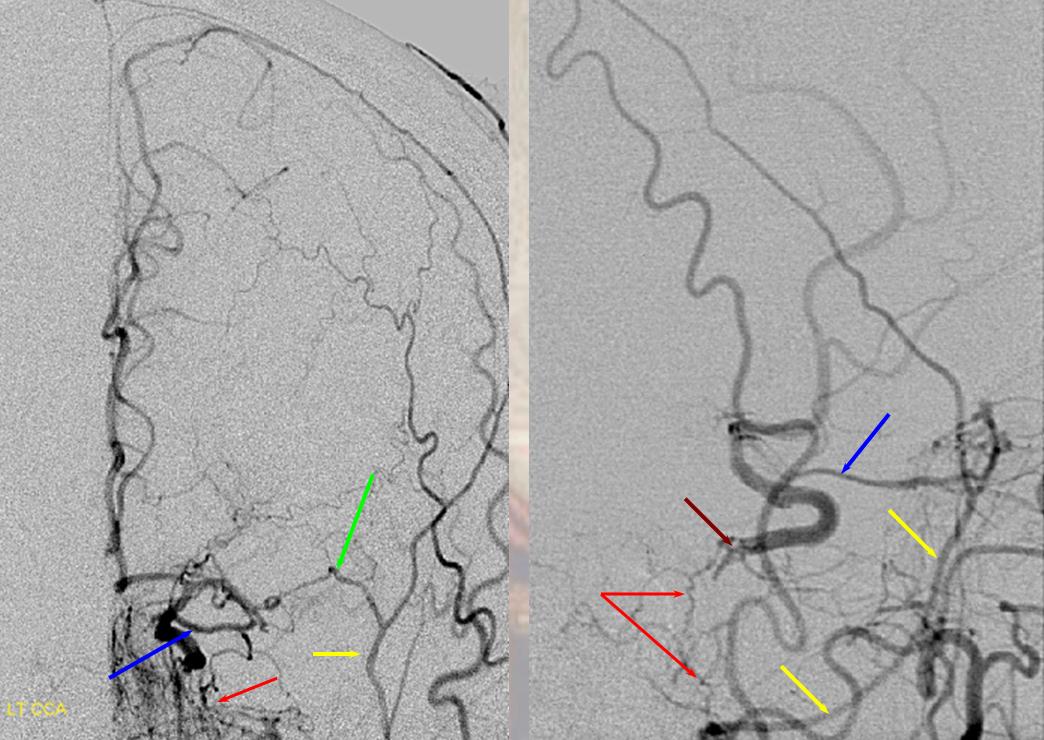
Lateral projection views immediately post Pipeline embolization (top), and 4 months later (bottom). Notice branches of the MHT (purple arrows) which remain open, and are now visible after the aneurysm has disappeared. The mandibulovidian artery is again marked with white arrow.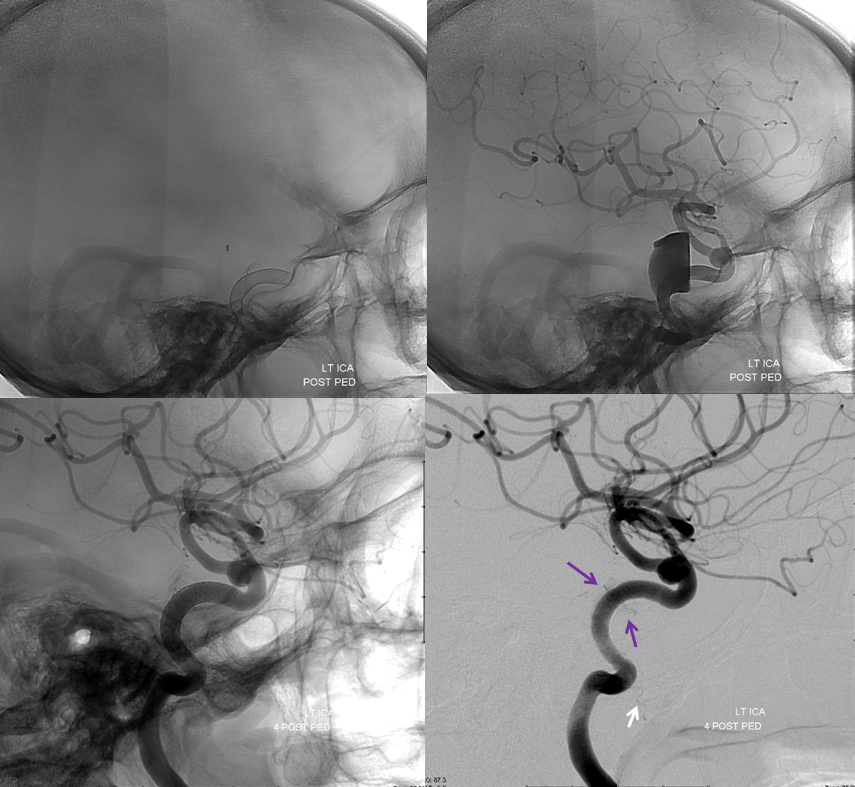 The following case, courtesy of Dr. Hima Pendharkar, National Institute of Mental Health & Neuro Sciences, Bangalore, India illustrates this connection in a patient with an unusual Moya-Moya variant characterized by occlusion of the carotid artery at the supraclinoid level, just beyond the typical origin of the ophthalmic artery. As a result of this more proximal occlusion, the typical puff of smoke collaterals between the anterior choroidal, superior hypophyseal, and lenticulostriate arteries are unavailable. Instead, one sees a pathway of “typical” ophthalmic (black arrow) to “ventral ophthalmic” ( white arrows) to anterior cerebral artery. In other words, both the typical and ventral ophthalmic arteries are present in this patient, with retrograde ventral ophthalmic flow reconstituting the anterior cerebral artery territory.
The following case, courtesy of Dr. Hima Pendharkar, National Institute of Mental Health & Neuro Sciences, Bangalore, India illustrates this connection in a patient with an unusual Moya-Moya variant characterized by occlusion of the carotid artery at the supraclinoid level, just beyond the typical origin of the ophthalmic artery. As a result of this more proximal occlusion, the typical puff of smoke collaterals between the anterior choroidal, superior hypophyseal, and lenticulostriate arteries are unavailable. Instead, one sees a pathway of “typical” ophthalmic (black arrow) to “ventral ophthalmic” ( white arrows) to anterior cerebral artery. In other words, both the typical and ventral ophthalmic arteries are present in this patient, with retrograde ventral ophthalmic flow reconstituting the anterior cerebral artery territory.




 Meningolacrimal is white. Hyrtl foramen is black
Meningolacrimal is white. Hyrtl foramen is black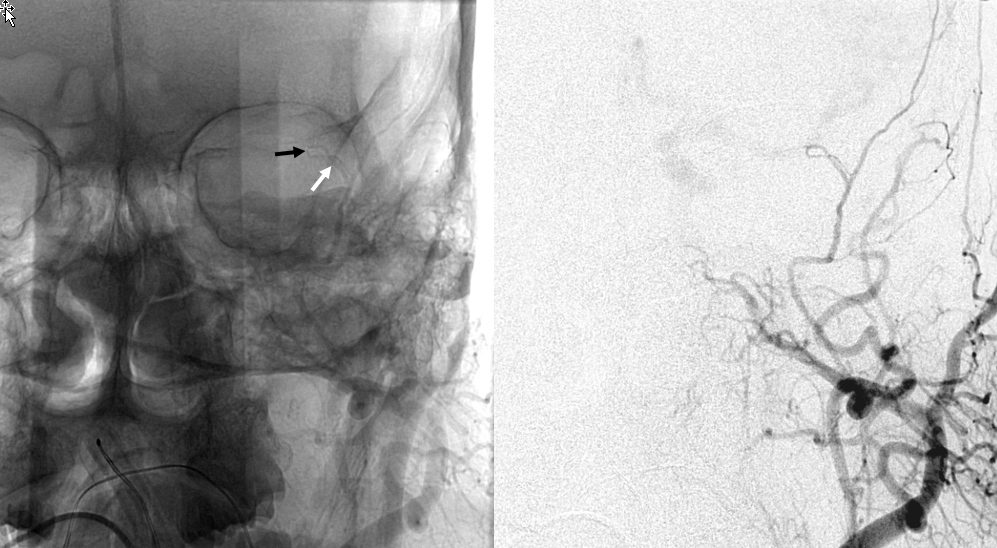 Another example. Angio example, with typical origin ophthalmic including choroid blush of the globe
Another example. Angio example, with typical origin ophthalmic including choroid blush of the globe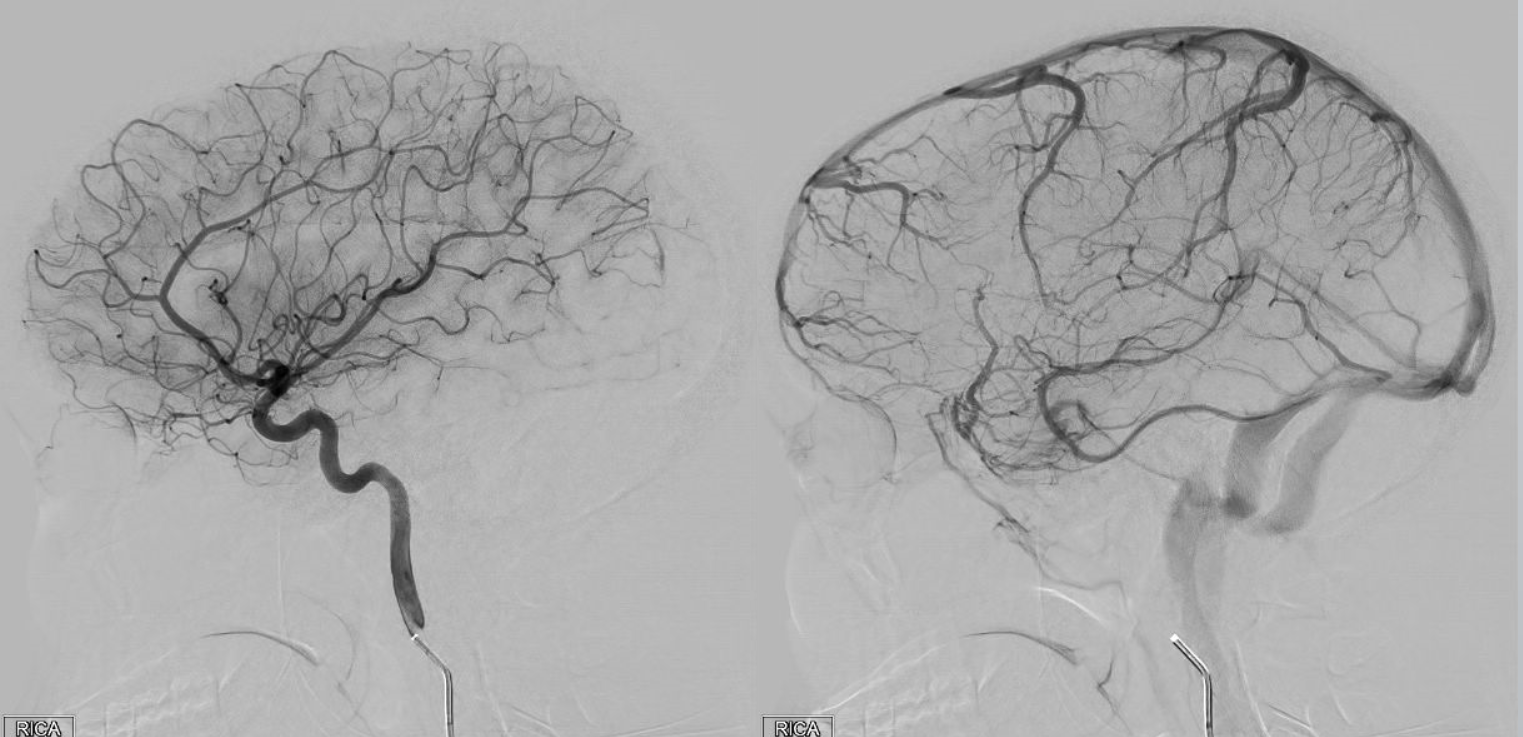 ECA injection shows MMA (purple) and sphenoid branch (white) supplying via the lacrimal branch (brown) the lacrimal gland (peach). Note lateral entry of lacrimal branch into orbit (foramen of Hyrtl). A more medial branch (red) likely connects the lacrimal branch to the ophthalmic artery.
ECA injection shows MMA (purple) and sphenoid branch (white) supplying via the lacrimal branch (brown) the lacrimal gland (peach). Note lateral entry of lacrimal branch into orbit (foramen of Hyrtl). A more medial branch (red) likely connects the lacrimal branch to the ophthalmic artery.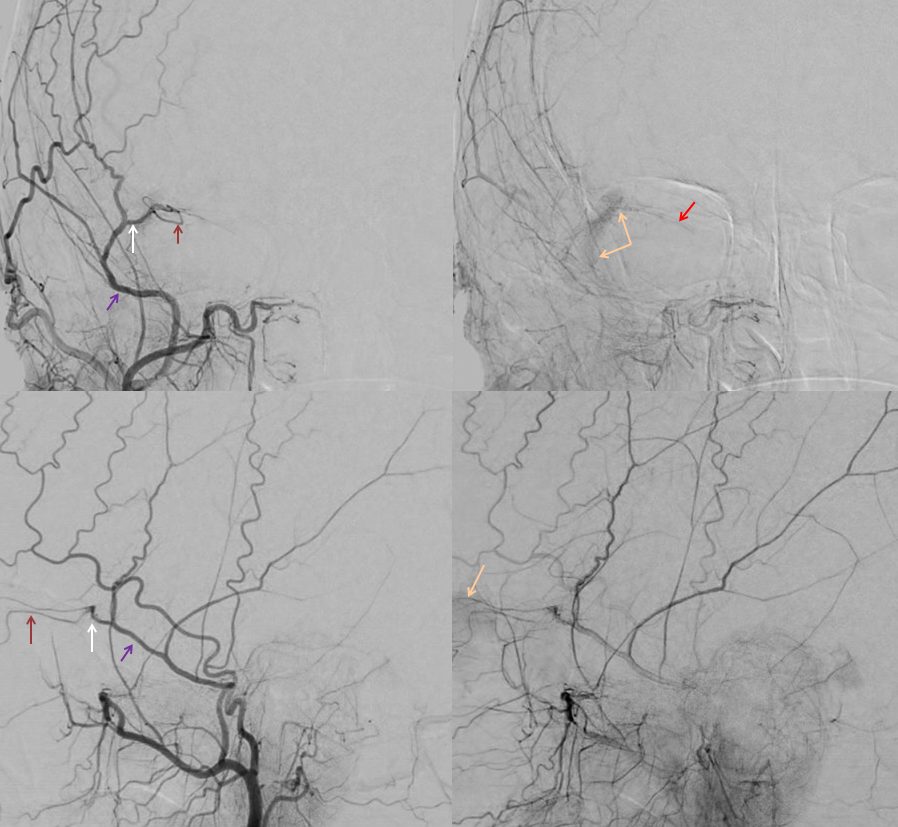

 Frontal views (white arrow – sphenoid branch, yellow arrow — lacrimal branch)
Frontal views (white arrow – sphenoid branch, yellow arrow — lacrimal branch)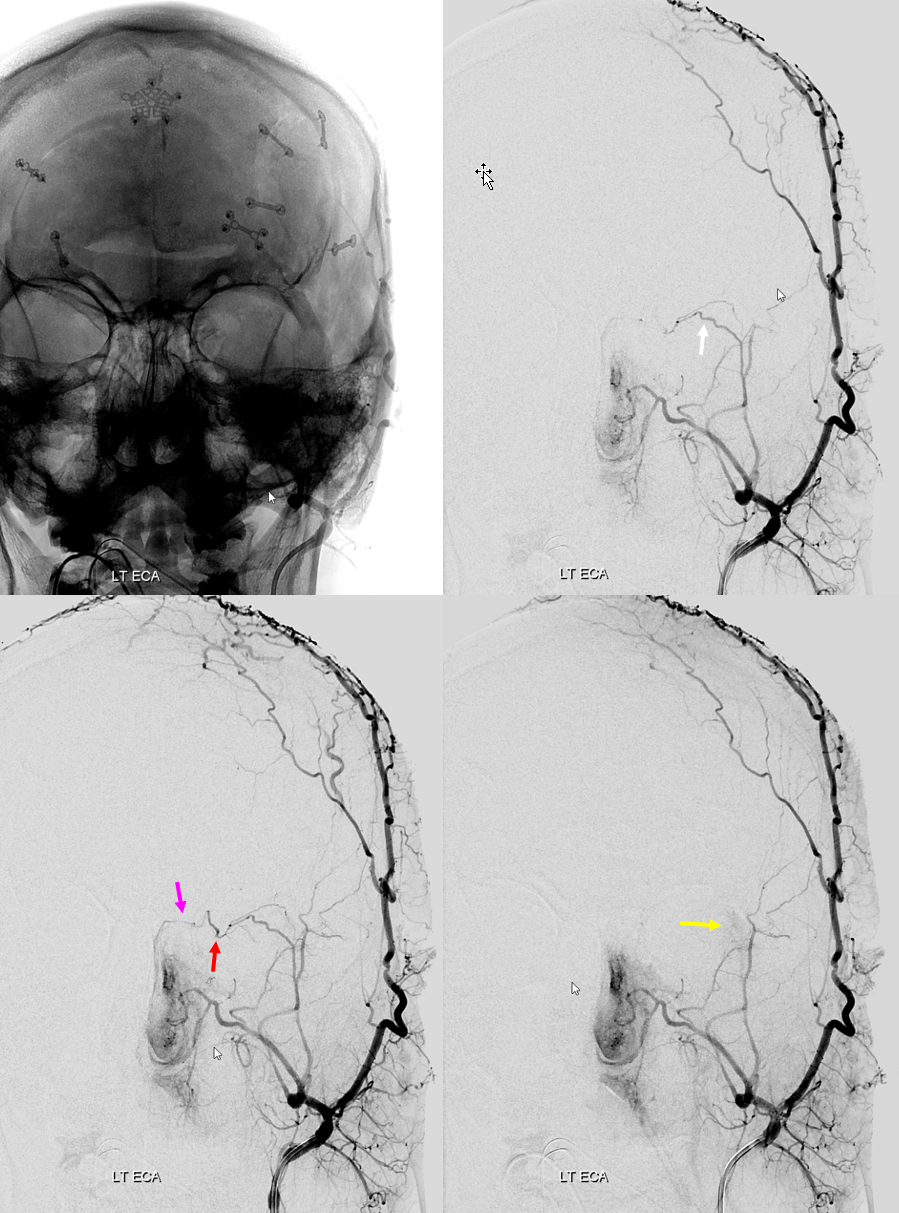









 Another likely route is from the distal internal maxillary within the prerygopalatine fossa. This IMAX (blue arrow) takes a superficial course relative to the lateral pterygoid muscle, and gives off a medially-oriented branch (red arrow) which likely connects to a faintly seen area of flow-related signal in the region of the pterygopalatine fossa (yellow arrow), and extending posteriorly towards the lateral border of the cavernous sinus (green arrow). This is most probably a foramen rotundum branch-ILT anastomosis (see ILT as well)
Another likely route is from the distal internal maxillary within the prerygopalatine fossa. This IMAX (blue arrow) takes a superficial course relative to the lateral pterygoid muscle, and gives off a medially-oriented branch (red arrow) which likely connects to a faintly seen area of flow-related signal in the region of the pterygopalatine fossa (yellow arrow), and extending posteriorly towards the lateral border of the cavernous sinus (green arrow). This is most probably a foramen rotundum branch-ILT anastomosis (see ILT as well)