
Diploic veins are veins in the diploic space of the skull — the space between inner and outer tables. They are depicted in all kinds of atlases. However their importance in draining the brain is generally under-appreciated. Just like suboccipital / condylar veins can be as big as a jugular, so can emissary veins carry a ton of flow. They are very variable — some people have very prominent ones, others don’t. Generally, i believe that their prominence is inversely proportional to size of the superior sagittal sinus — they are the natural regional collateral — the smaller the sagittal sinus, the larger the diploic veins — roughly speaking. This is part of the overall “balance” and “spectrum” approach to anatomy we are advocating — looking at the system as a whole, the larger the AICA the smaller the PICA, the bigger the P1, the smaller the PCOM, etc.
It is important to have a healthy surgical respect for diploic veins when craniotomy is the game.
What is their importance? Sometimes, they are just a variant that leads to perhaps more bleeding from skull during surgery. Other times, however, it is a sign that traditional veins are somehow hypoplastic or compromised. The more constraint on usual veins/sinuses, the more other veins such as diploic ones have to contribute. In extreme cases they become functionally indispensable. Taking them down risks venous stroke.
Diploic veins are super easy to see on an x-ray of the skull –because there is an edge between the vein and skull itself. They look like lucent tracks running from top to bottom of skull, like tracks burrowed in wood by insects. Their location is different from expected suture lines, and they are generally wider than either suture lines or meningeal artery grooves. On angiography, they typically opacify later than venous sinuses because of the time it takes for the contrast to traverse via the emissary foramina into and through the diploic space. They are easy to differentiate from soft tissue emissary veins which run on the outside of the skull because these do not produce grooves in the skull.
What is the difference between diploic and emissary veins? Diploic ones stay in the skull. Emissary veins are “emissary” — they go through and through the skull to end up in the soft tissues. When a diploic vein exits the skull it becomes an emissary vein.
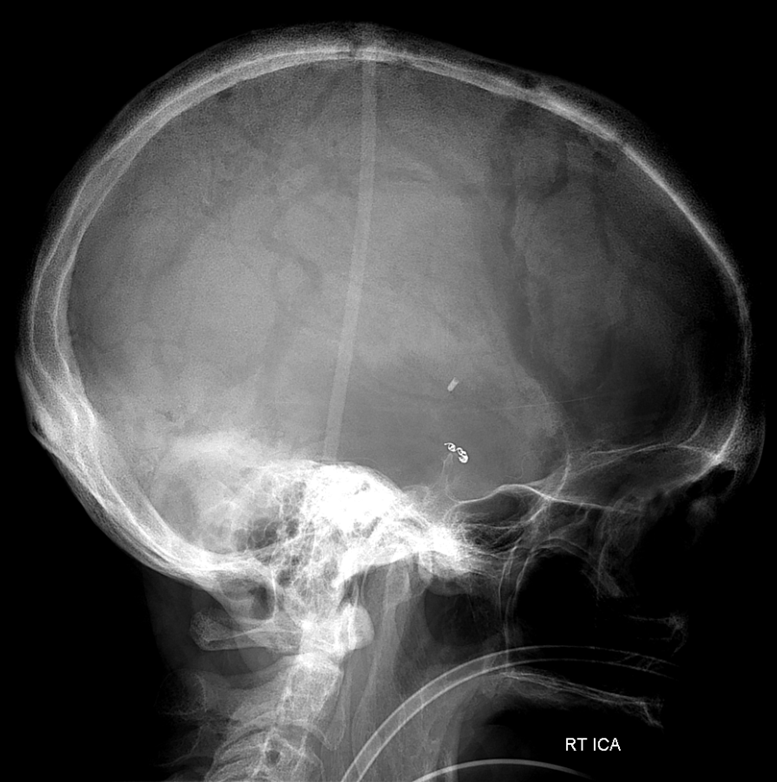
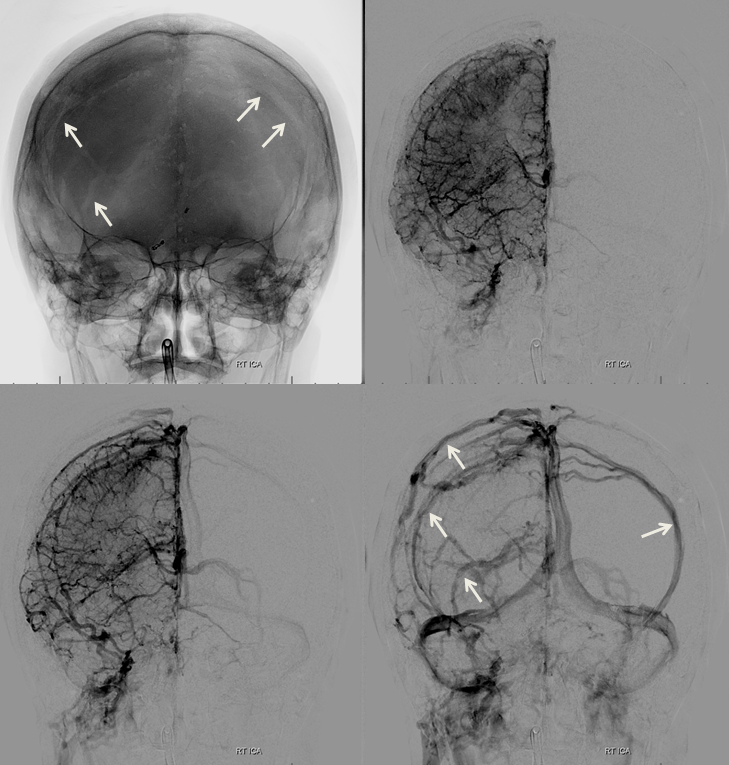
Above is a typical x-ray of diploic veins. Below is the same x-ray with arrows pointing to diploic veins
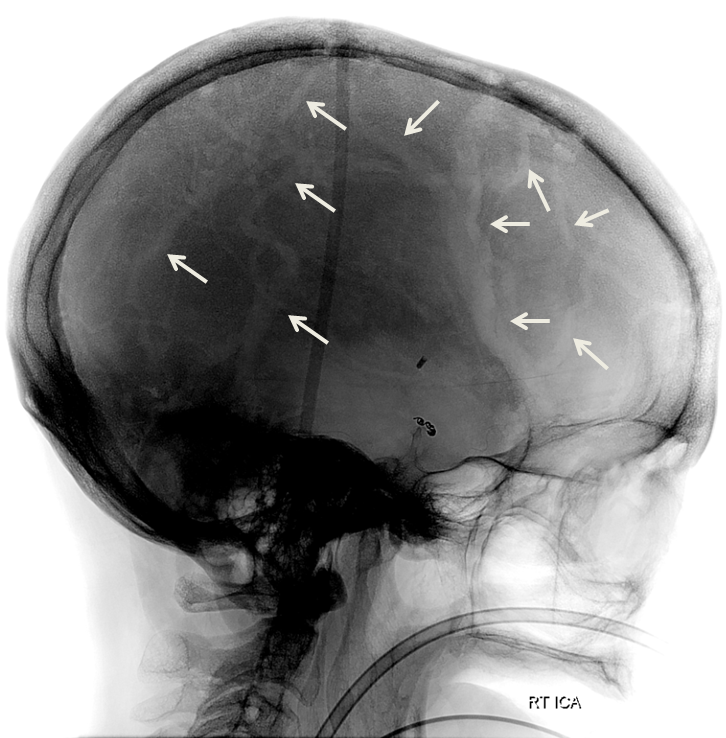
Because of some eye trick effects, they are easier to see on a black background of old-time x-rays
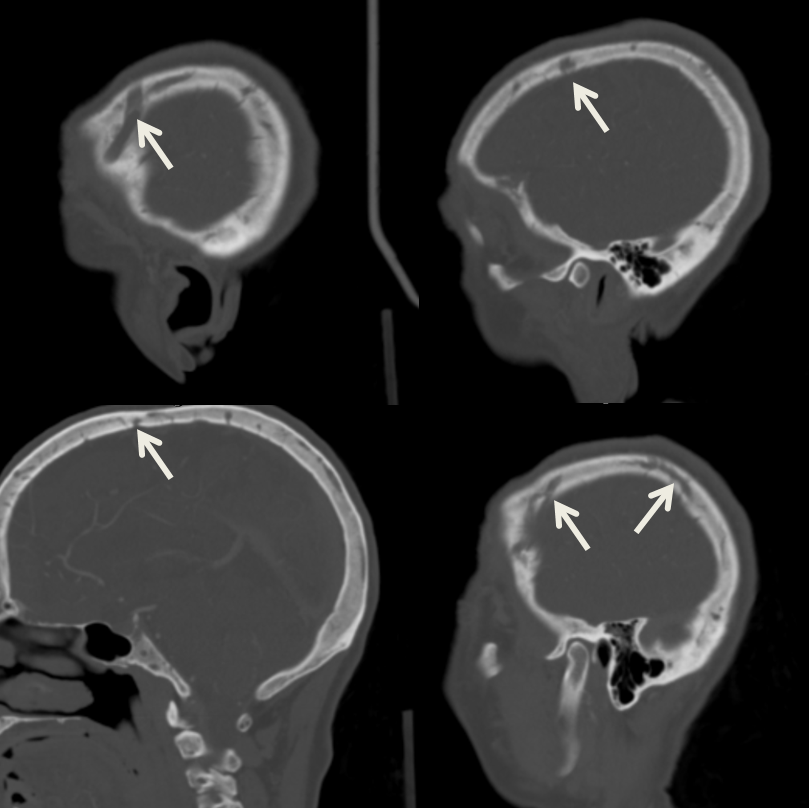
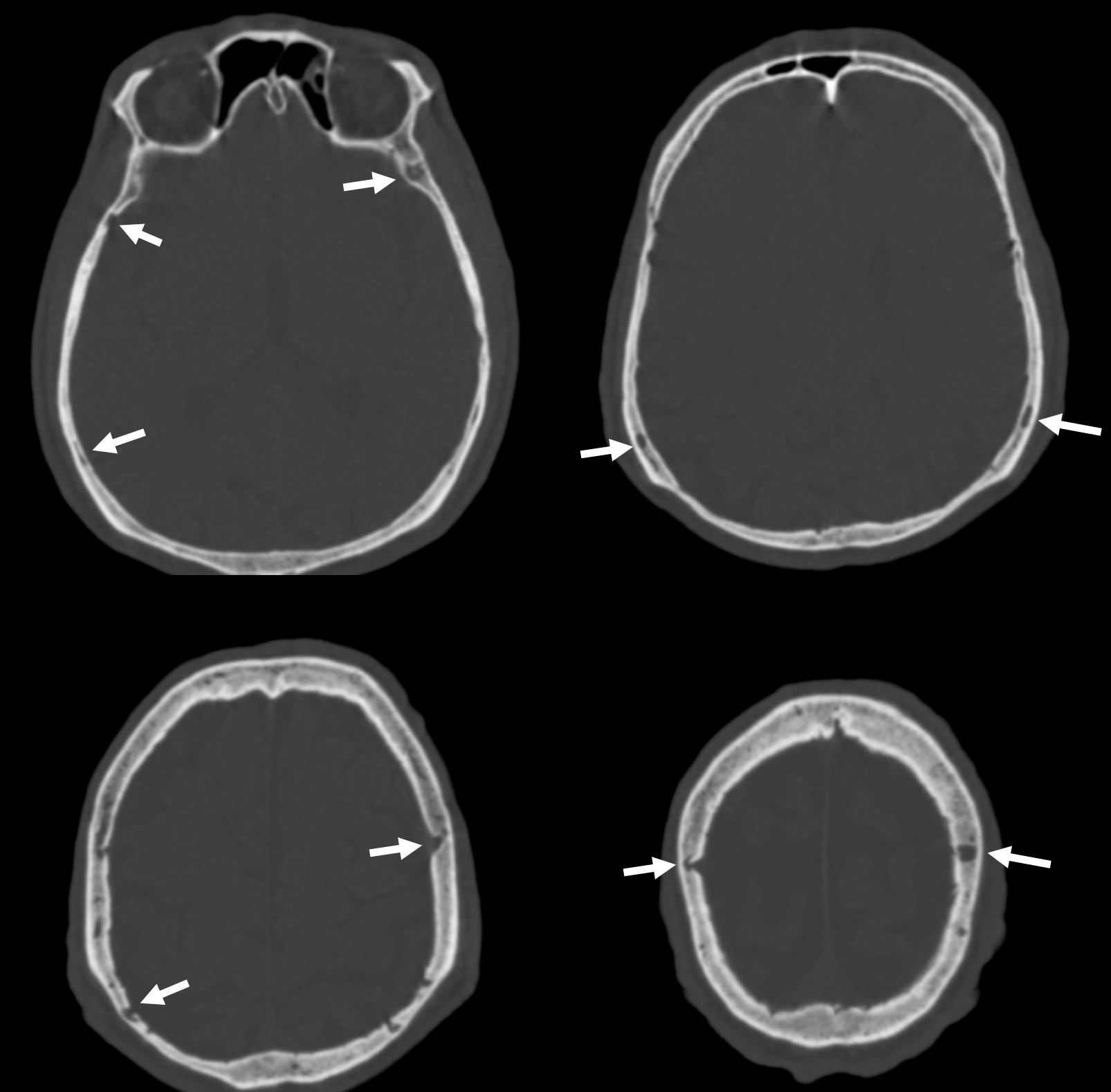
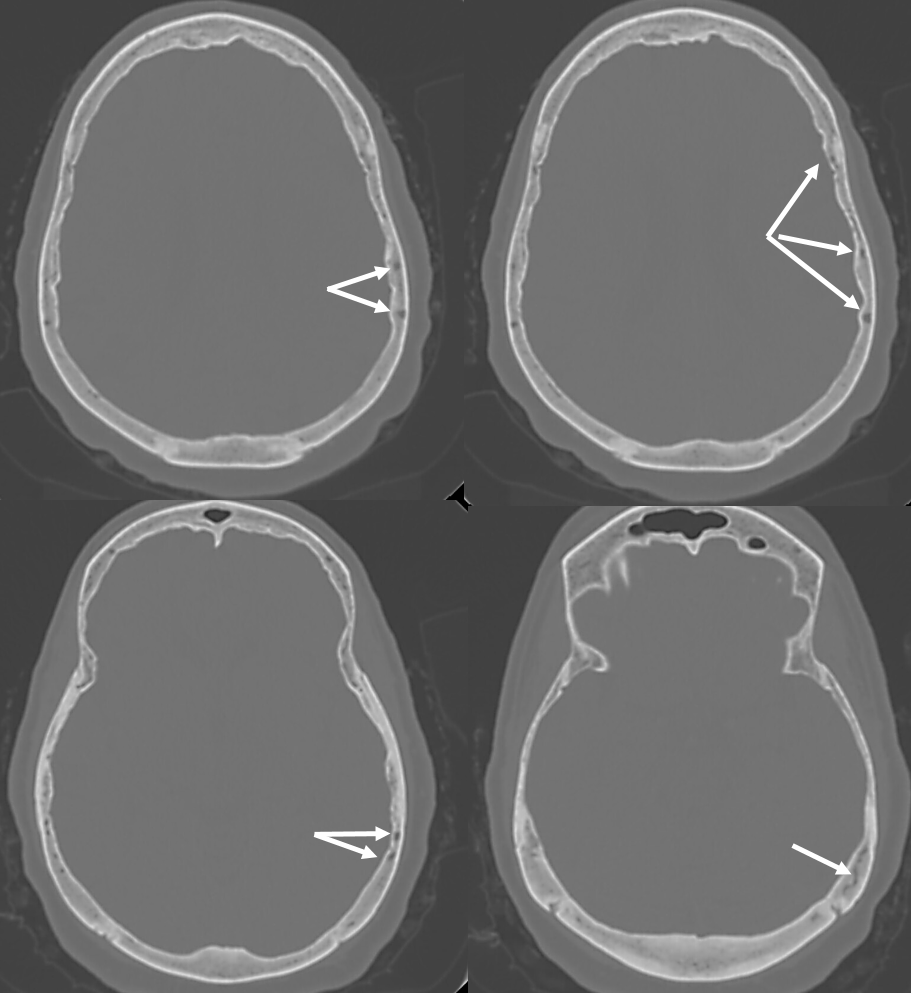
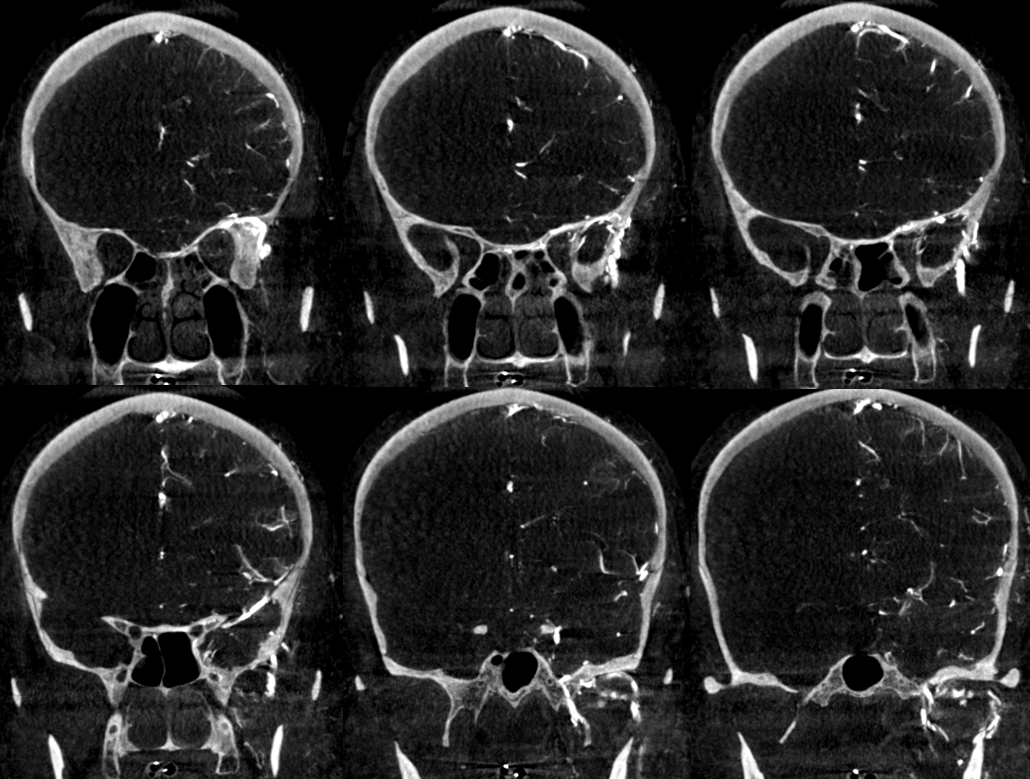
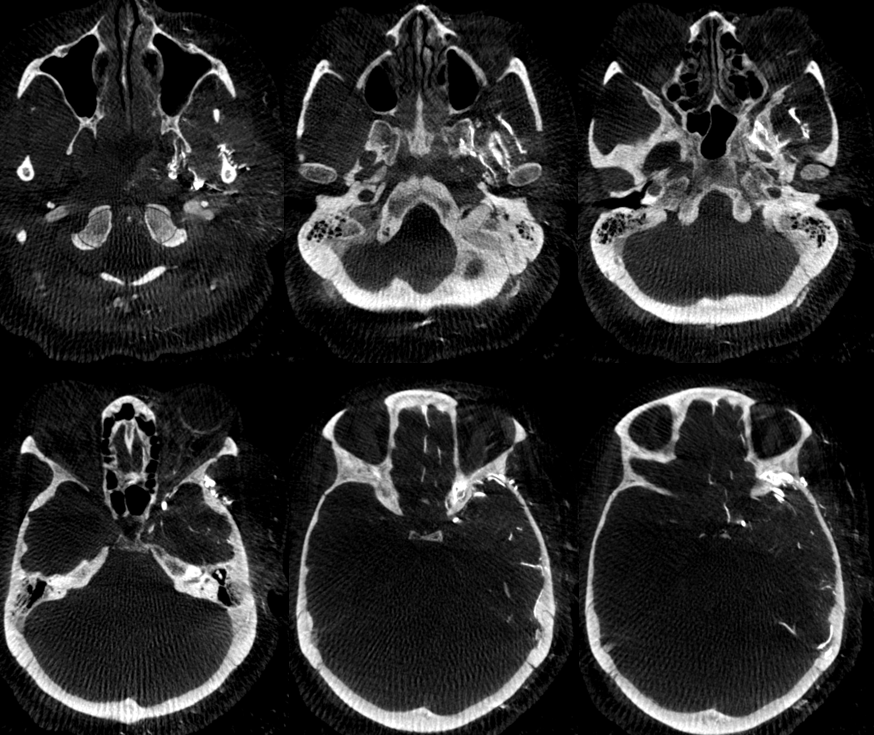
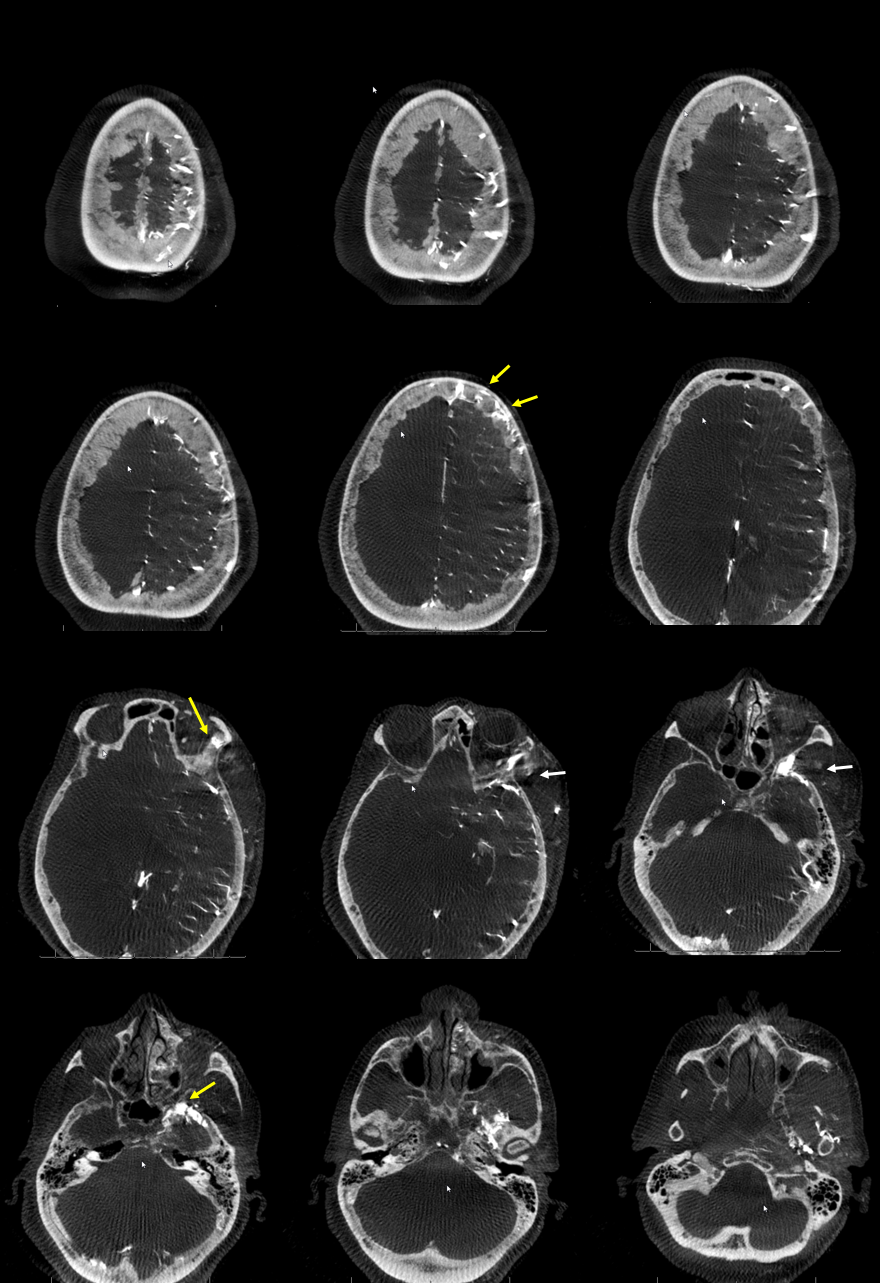
Since we don’t usually look at skull x-rays too often (and ignore all kinds of useful info on them when we do angiograms, as a rule), here is what diploic veins look like on a CT — channels in the diploic space. Not as striking as on skull lateral x-ray, however it is the same patient.
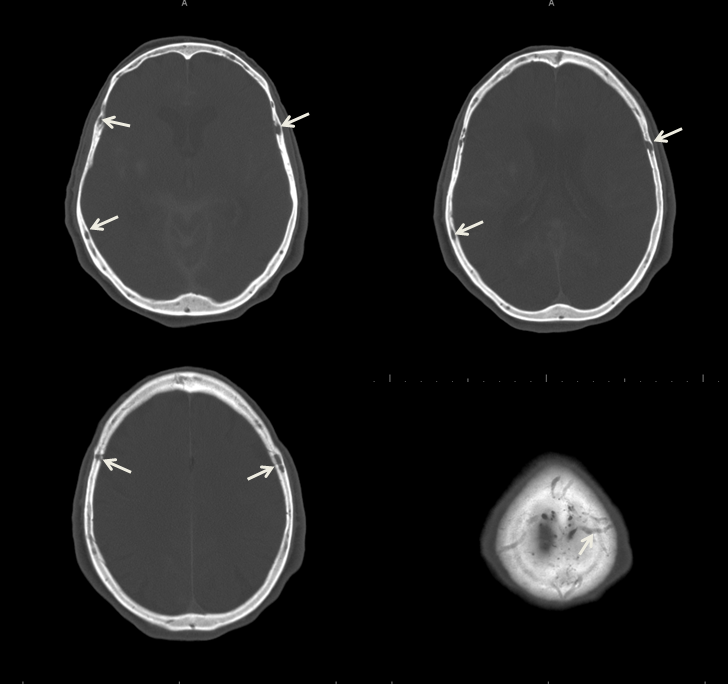
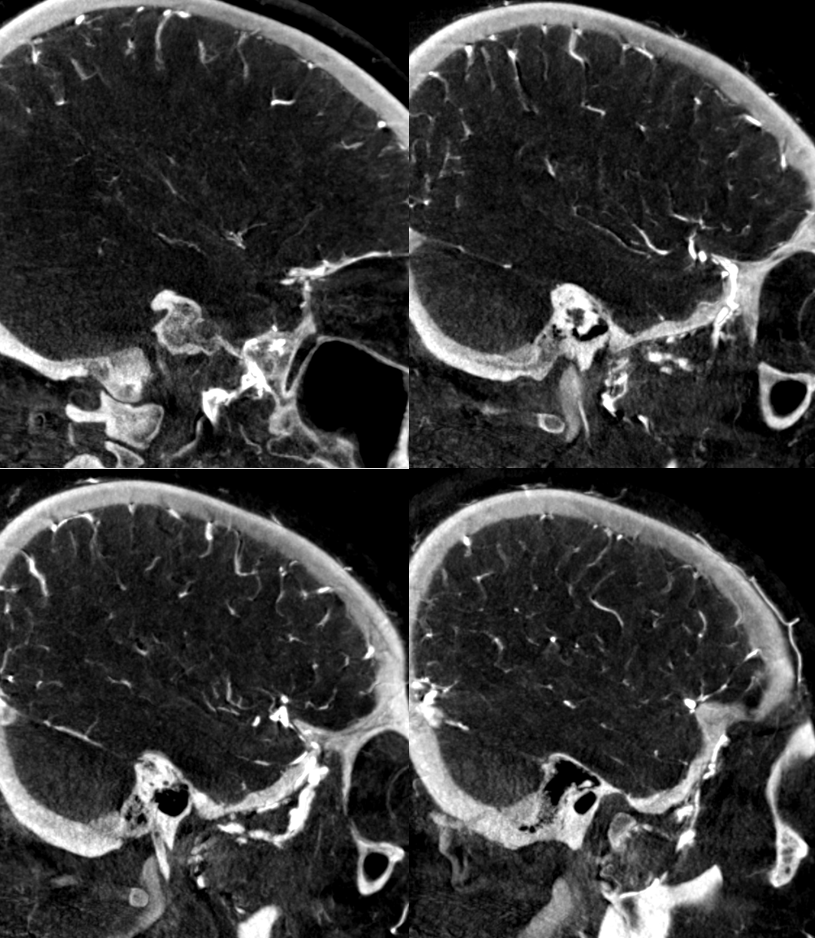
Axial views are best. Other views are not too helpful
Here is a picture from venerable Gray’s Anatomy

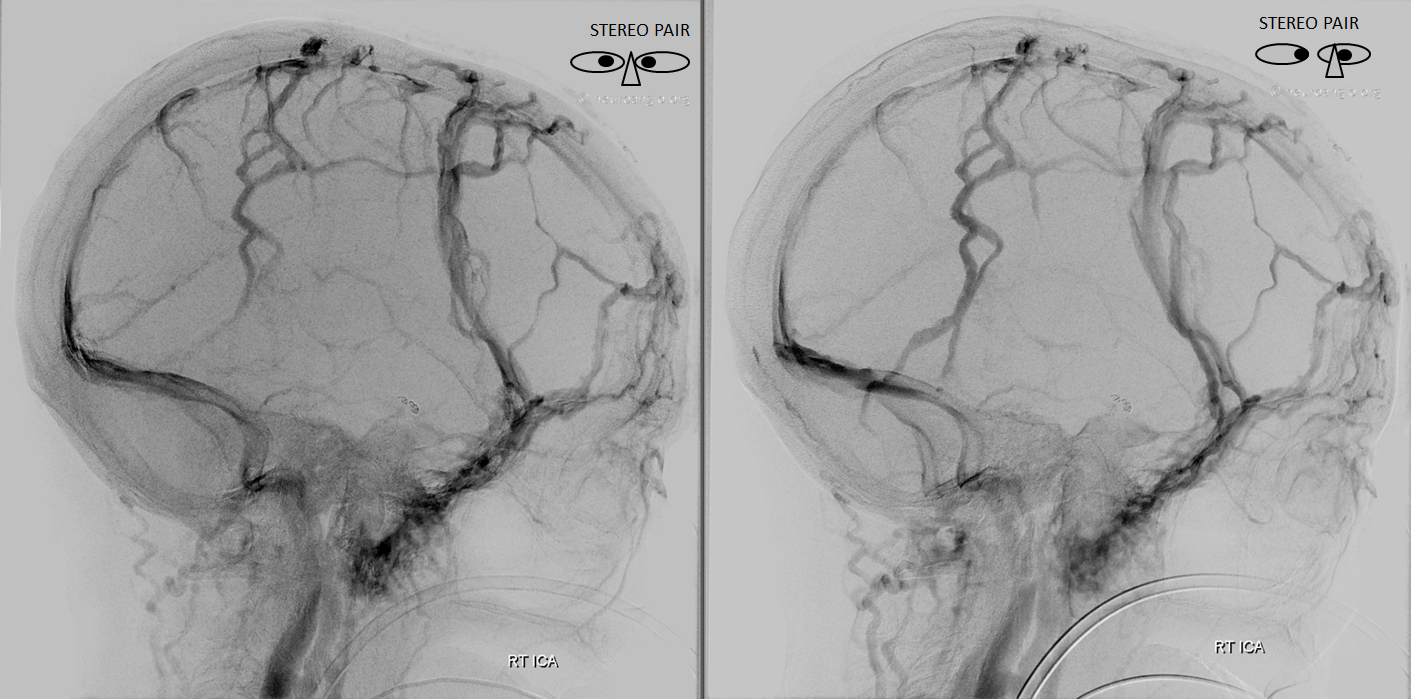
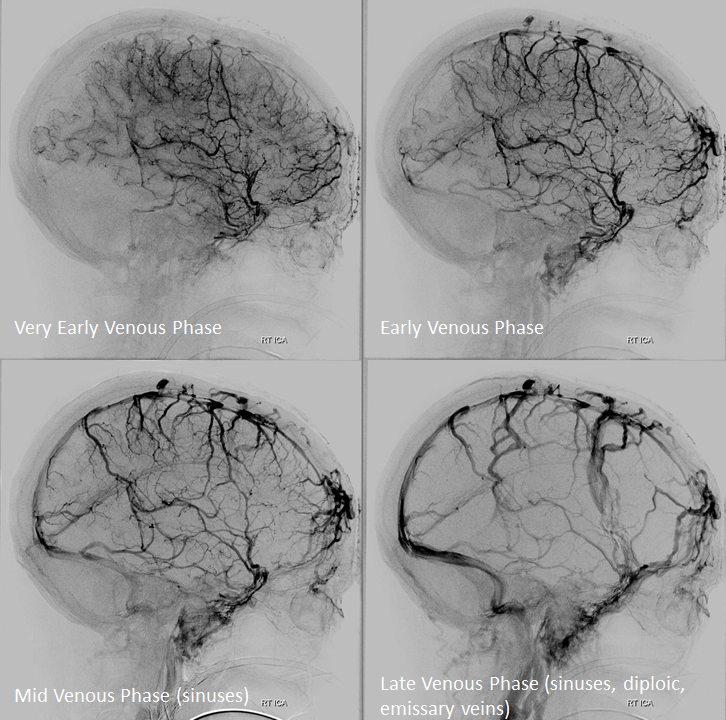
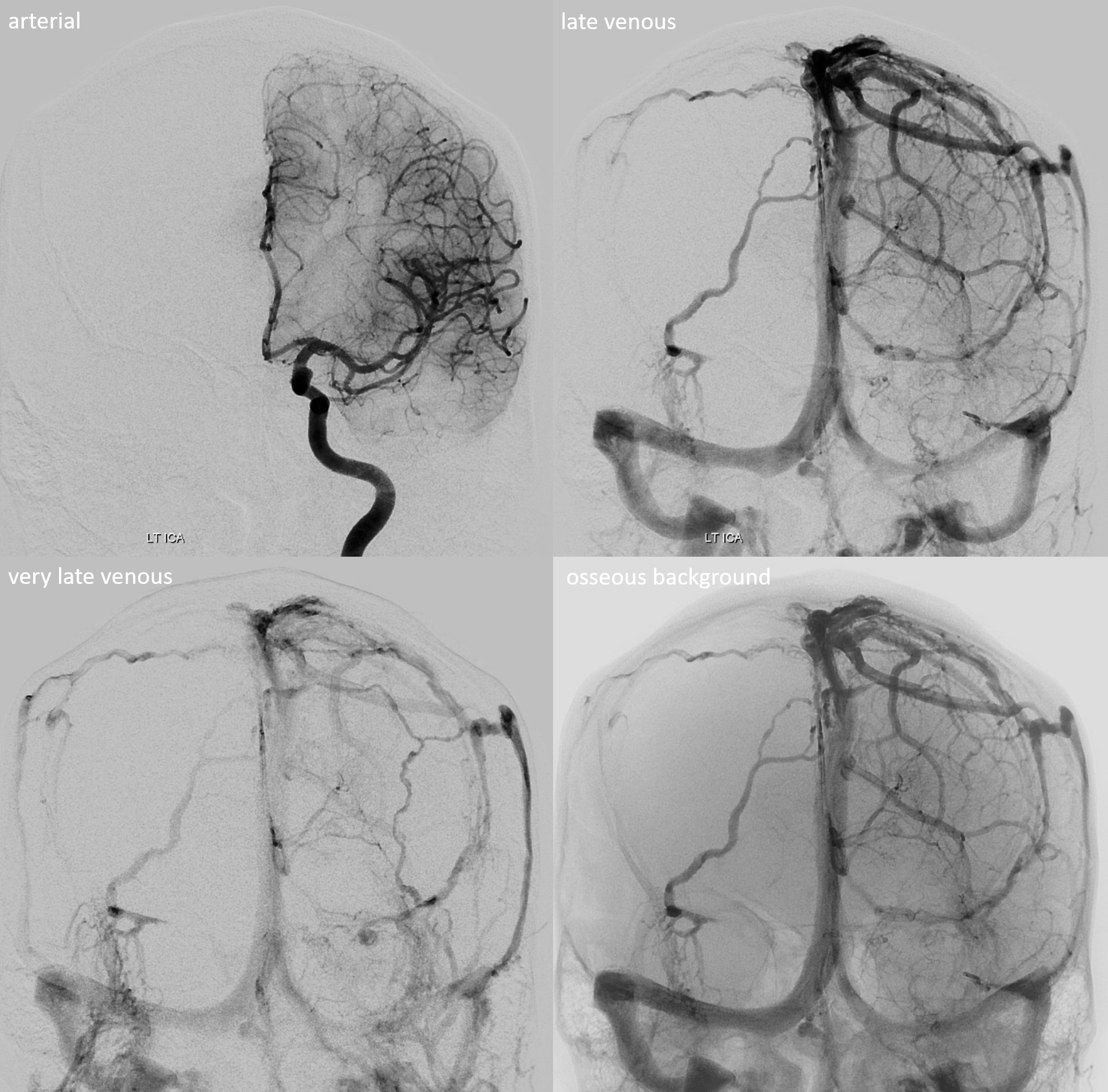
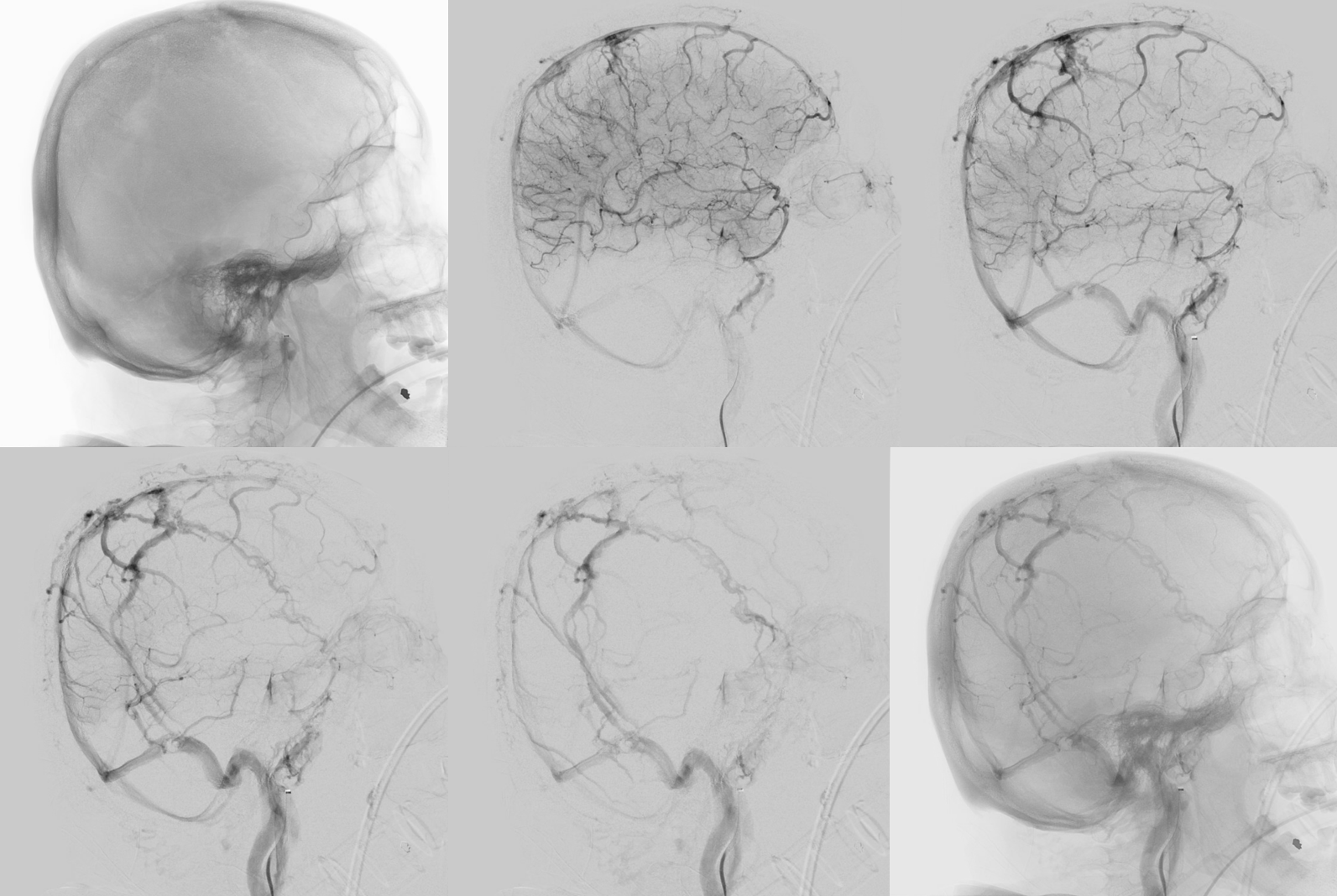
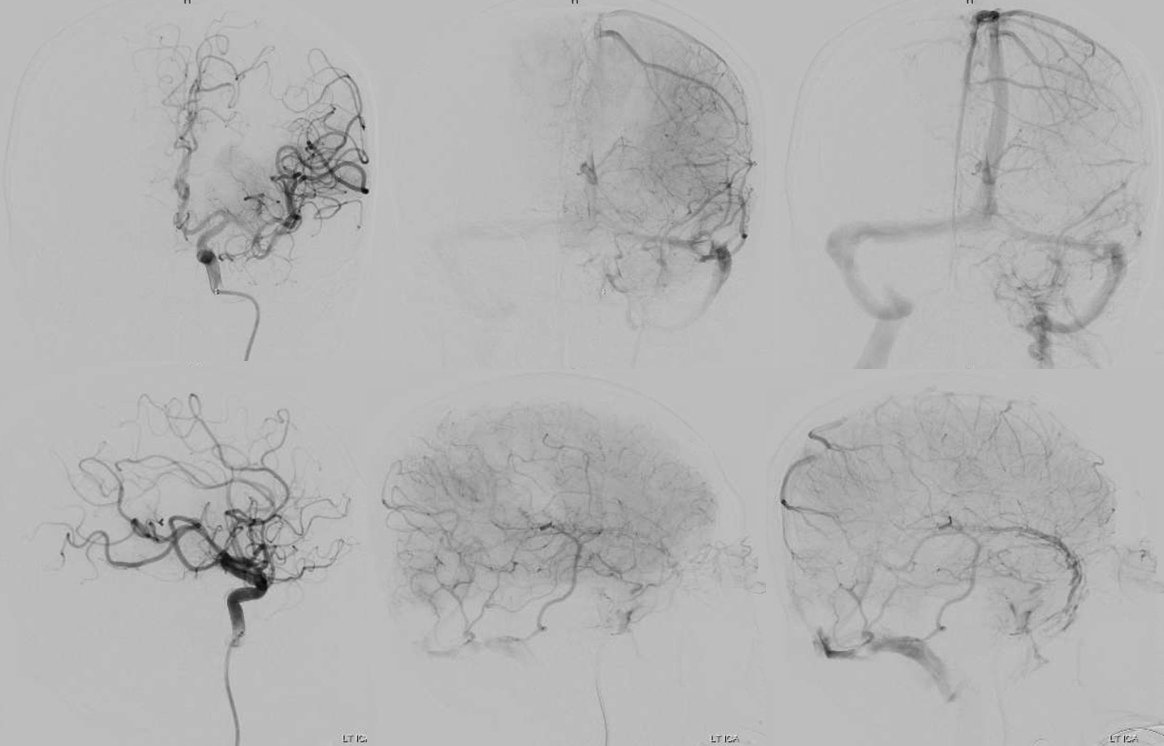
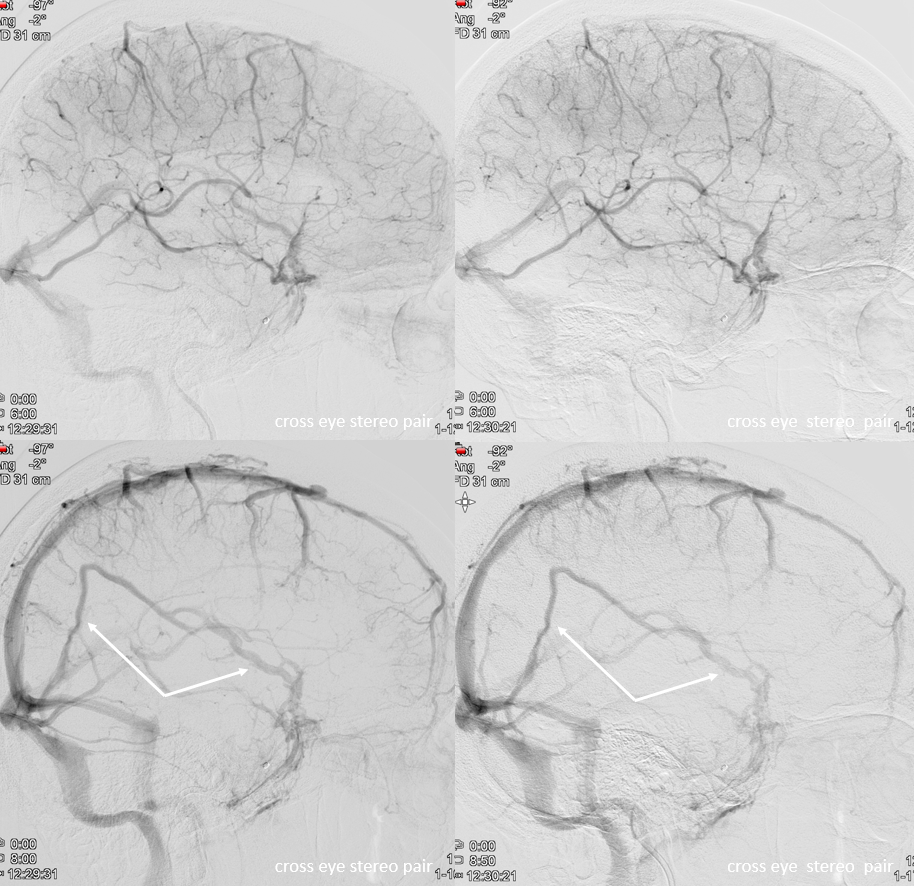
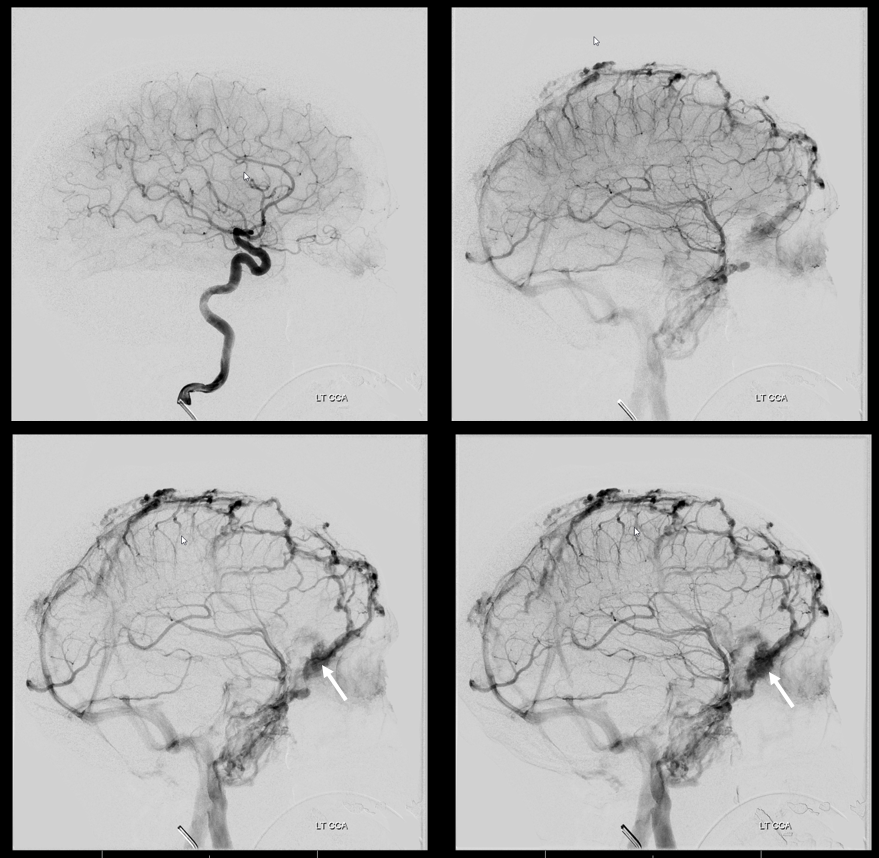
On angio, the key is to hold that pedal down into late venous phase. As you can see, these veins are most obvious in the late venous phase, after sinuses have opacified — note here small size of the superior sagittal sinus — as we spoke — these are large because SSS is small — balance…
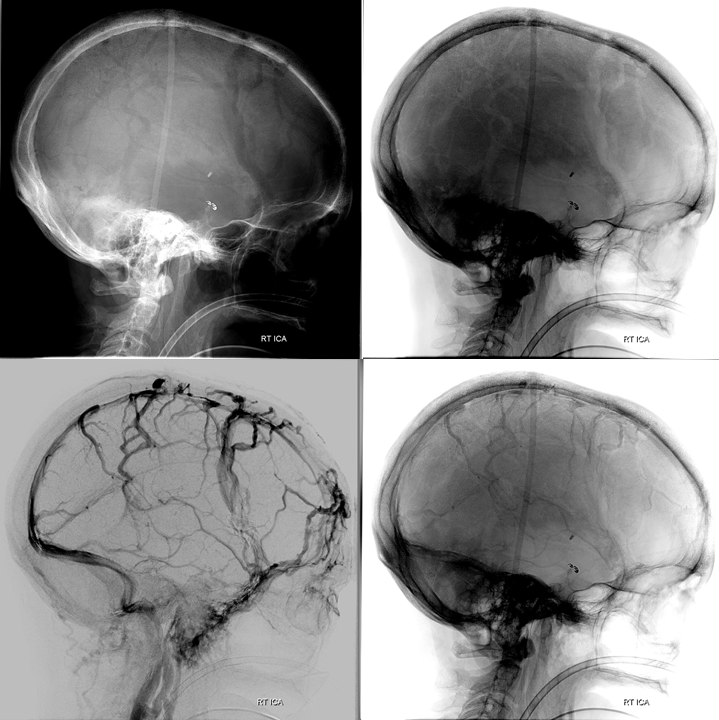
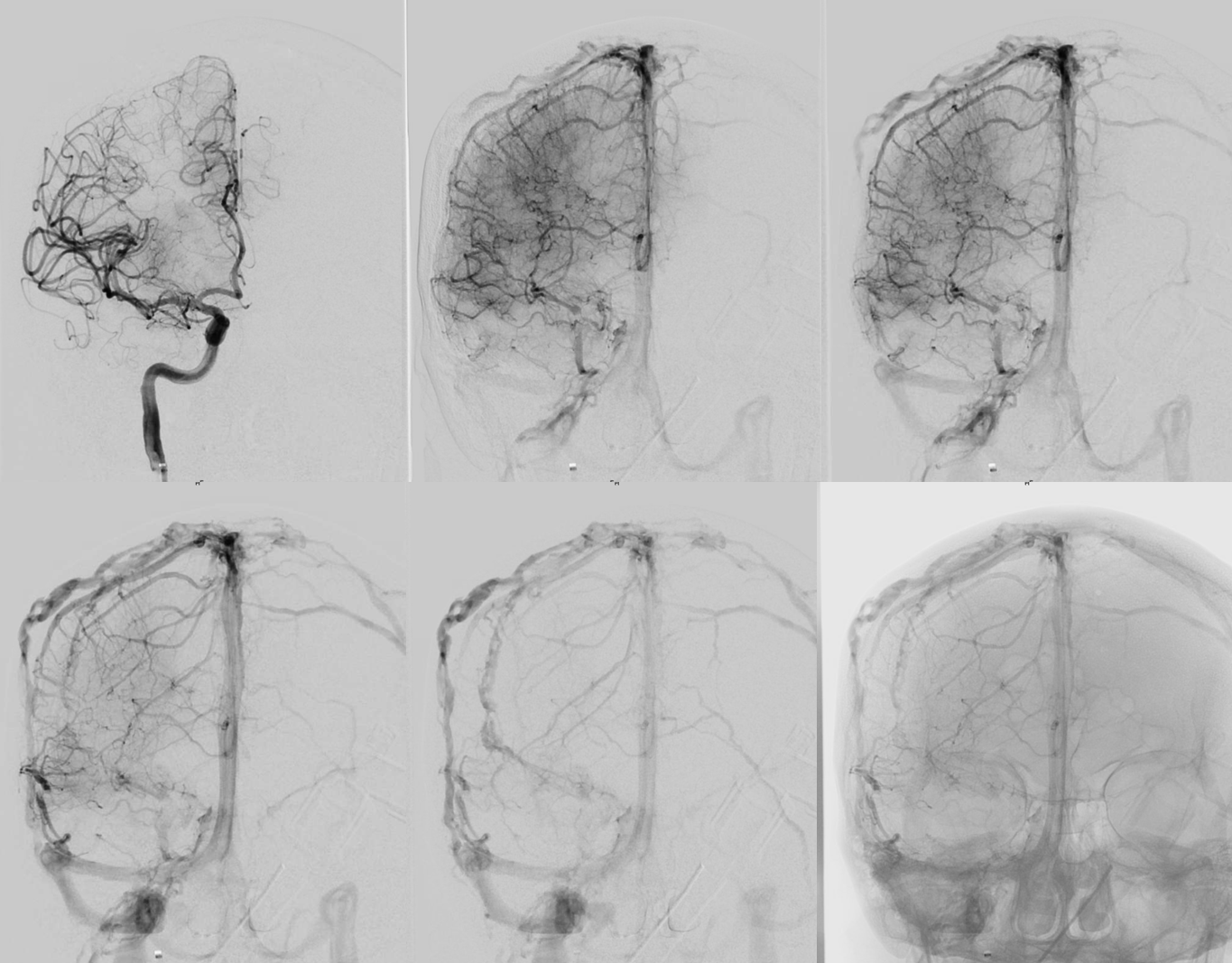
Images below show native views (black and white backgrounds, top). Lower left image shows diploic veins on a DSA. Lower right unsubtracted venous phase image shows contrast in diploic veins filling the curvilinear lucent spaces seen in the top row
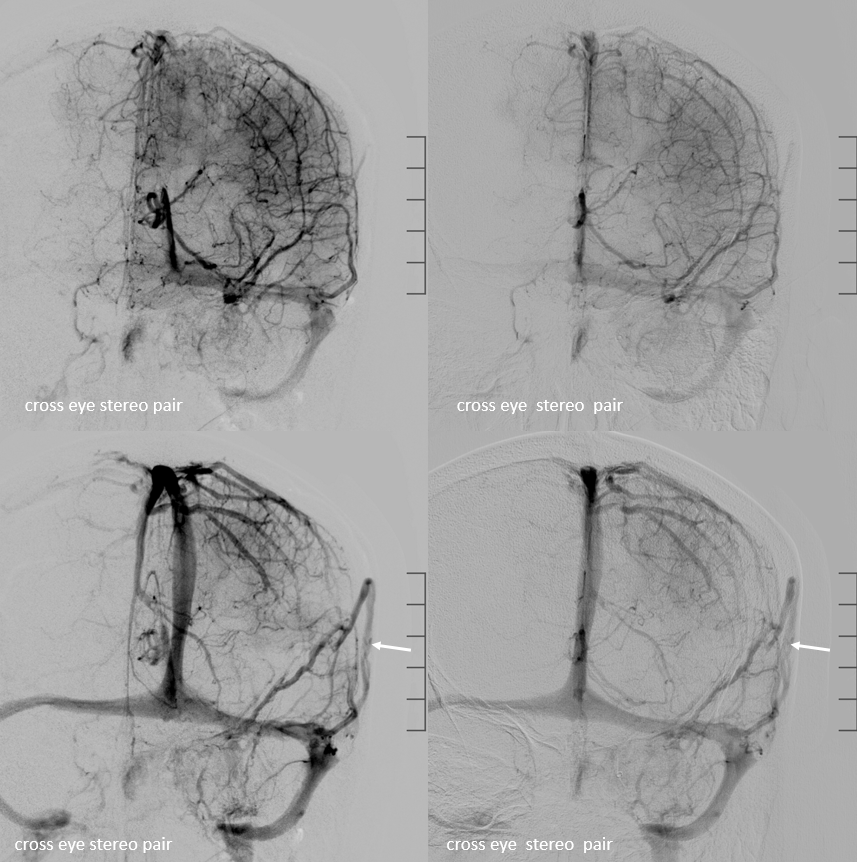
Lateral views are best. However, frontal views show these also. Skull x-ray shows lucent channels (white arrows) while lower right late venous phase angio shows diploic veins (arrows)
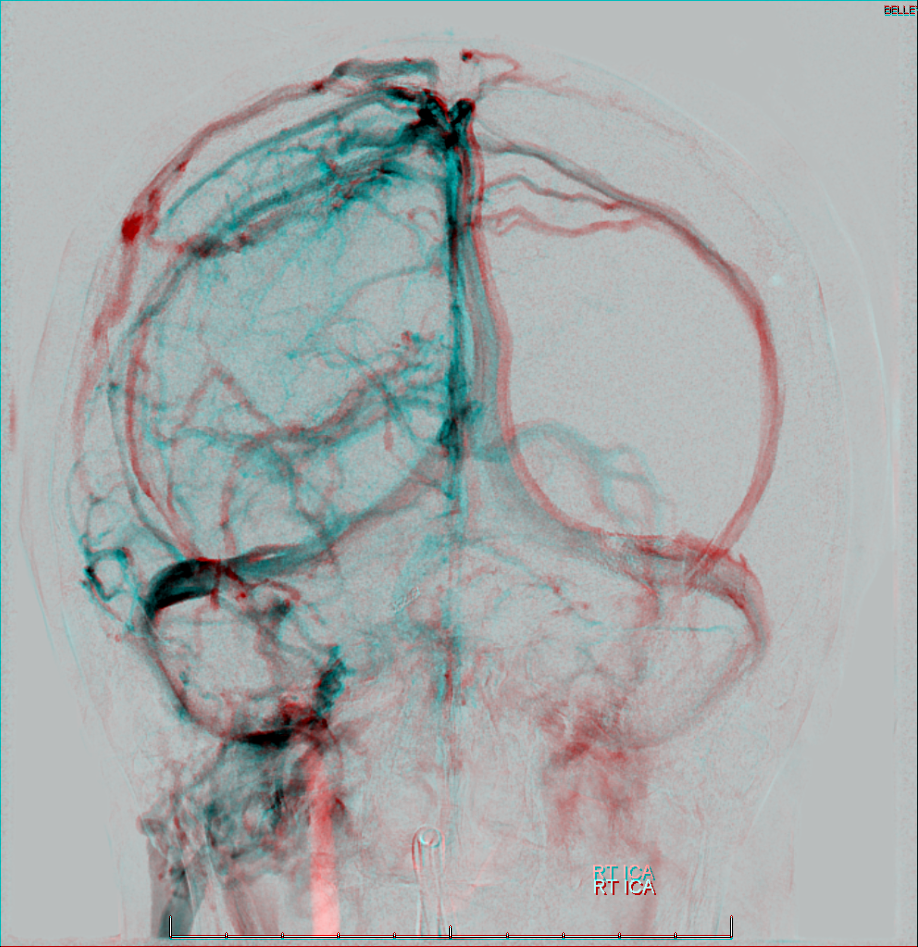
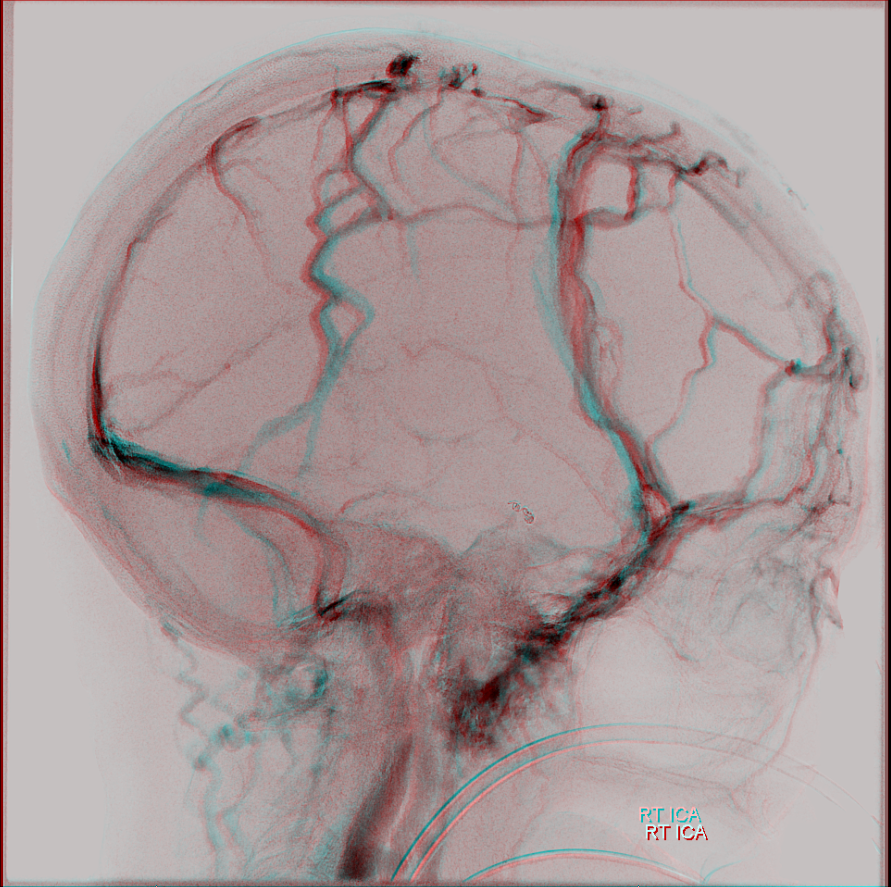
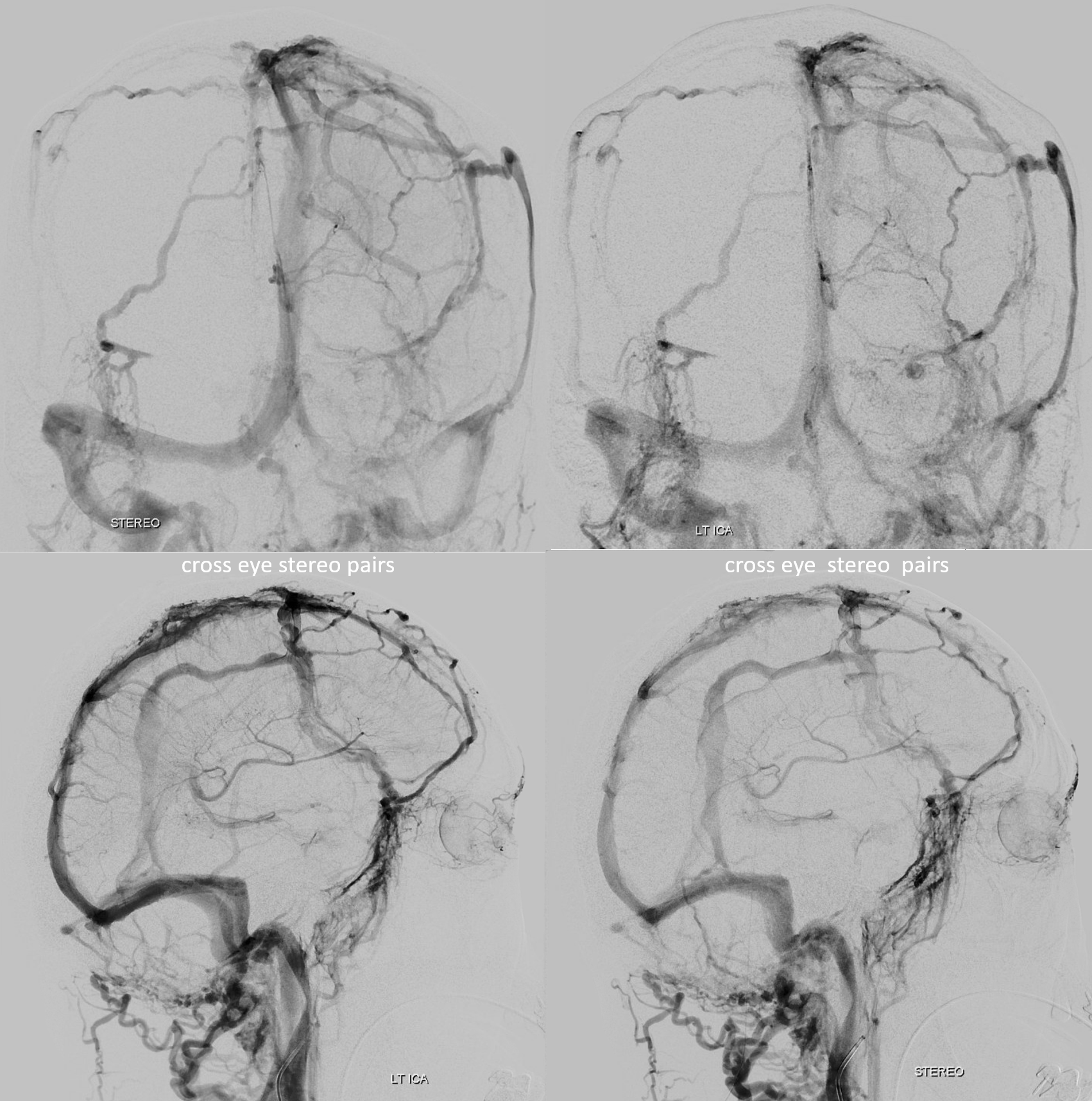
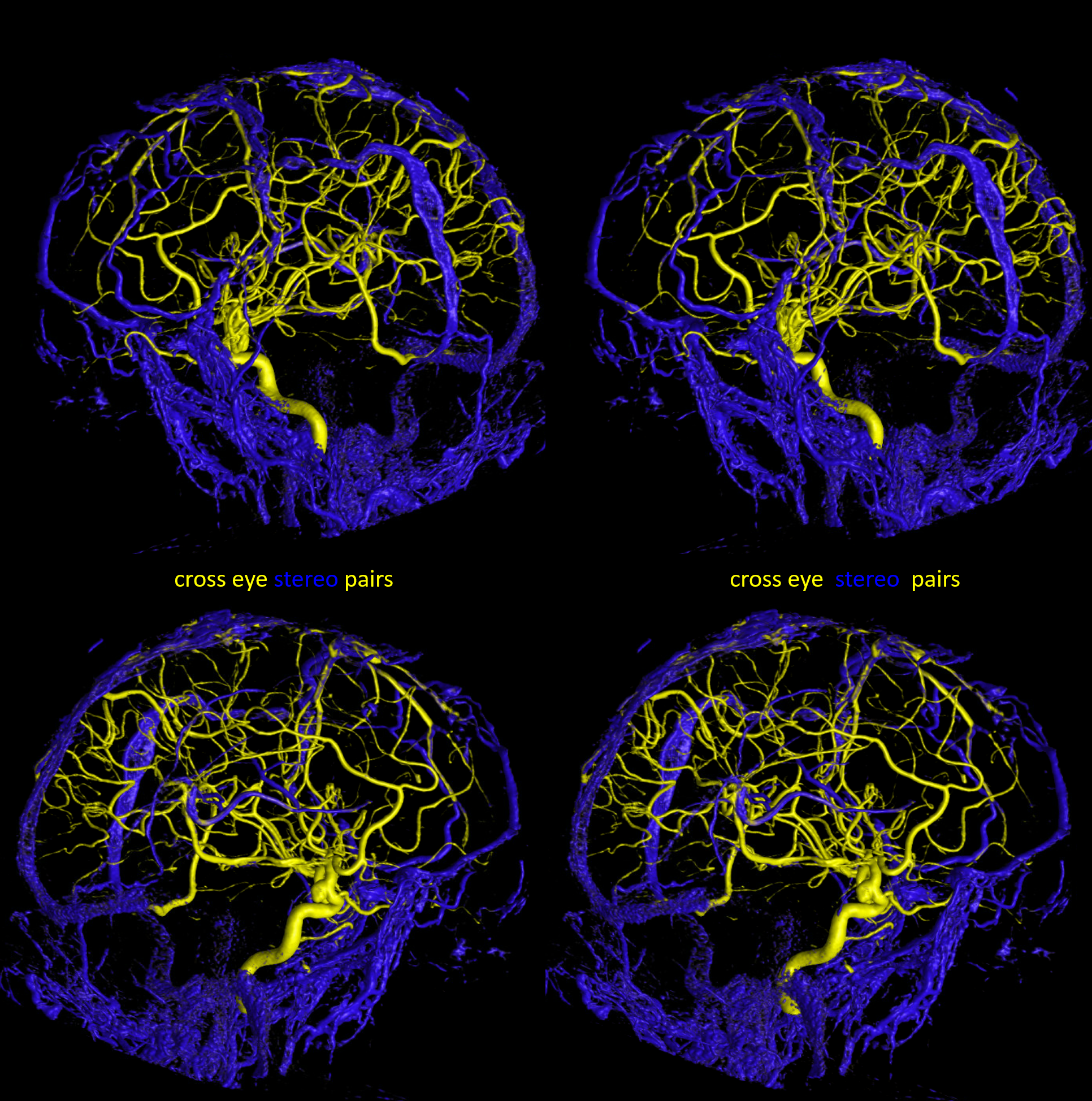
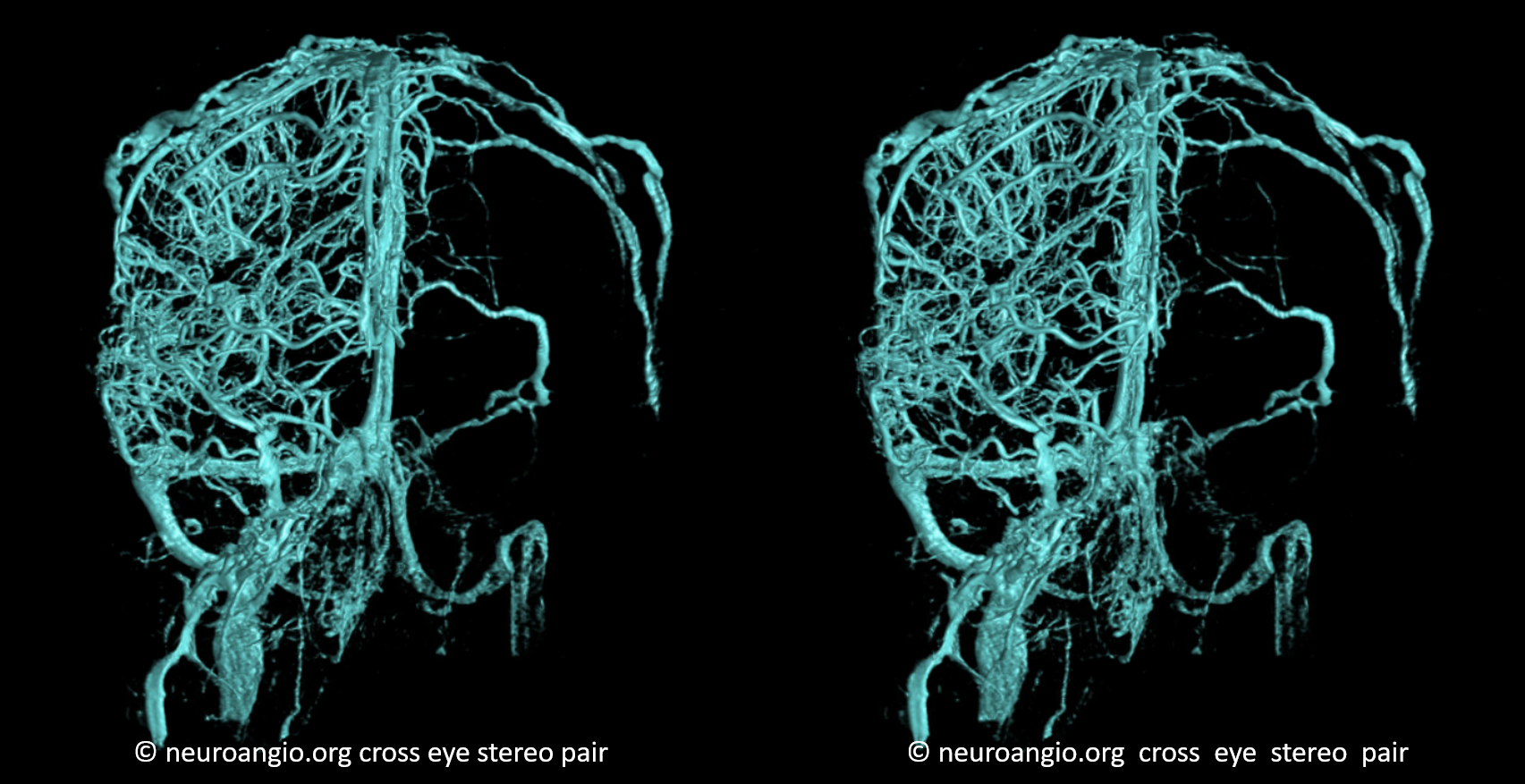
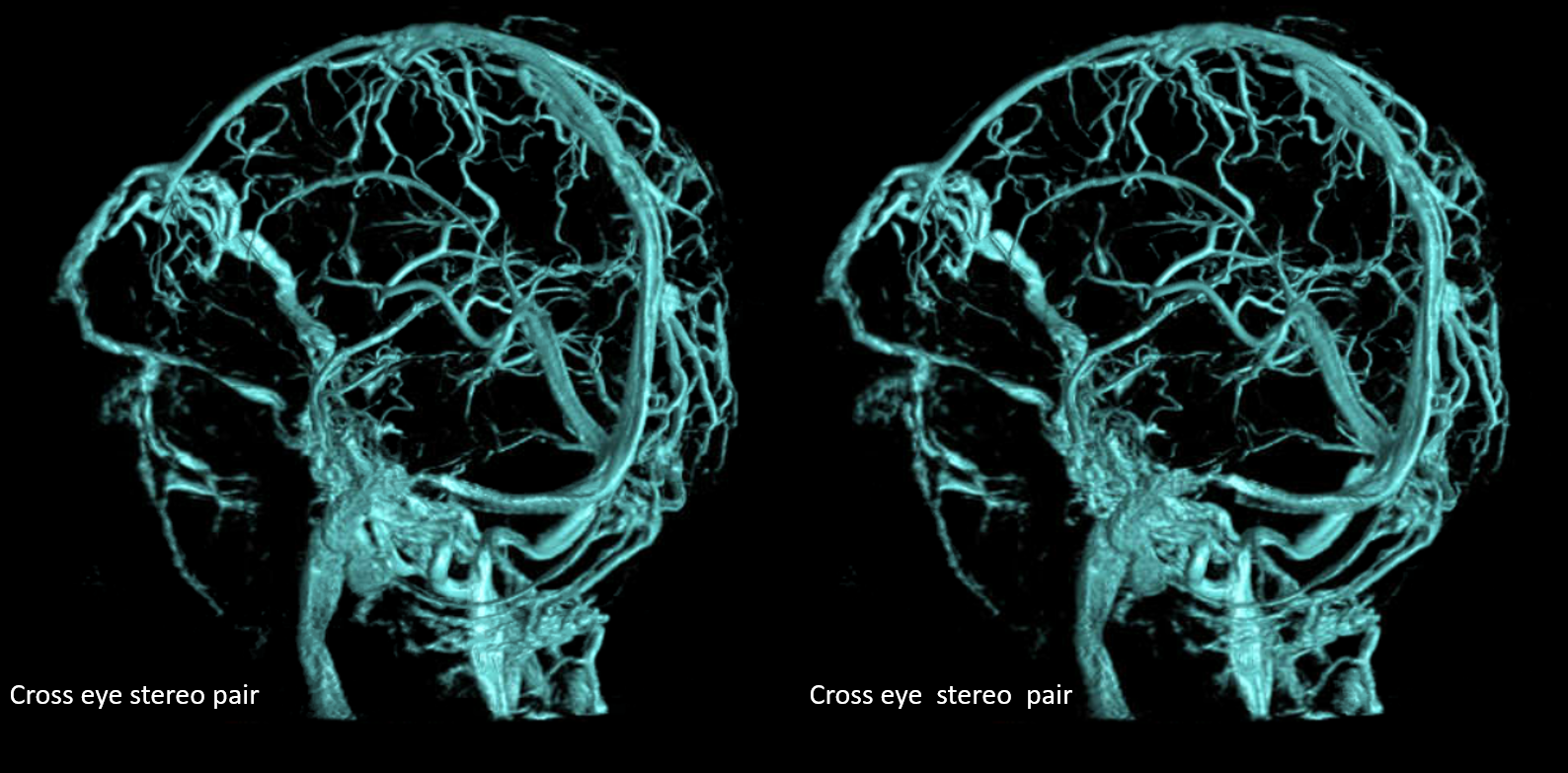
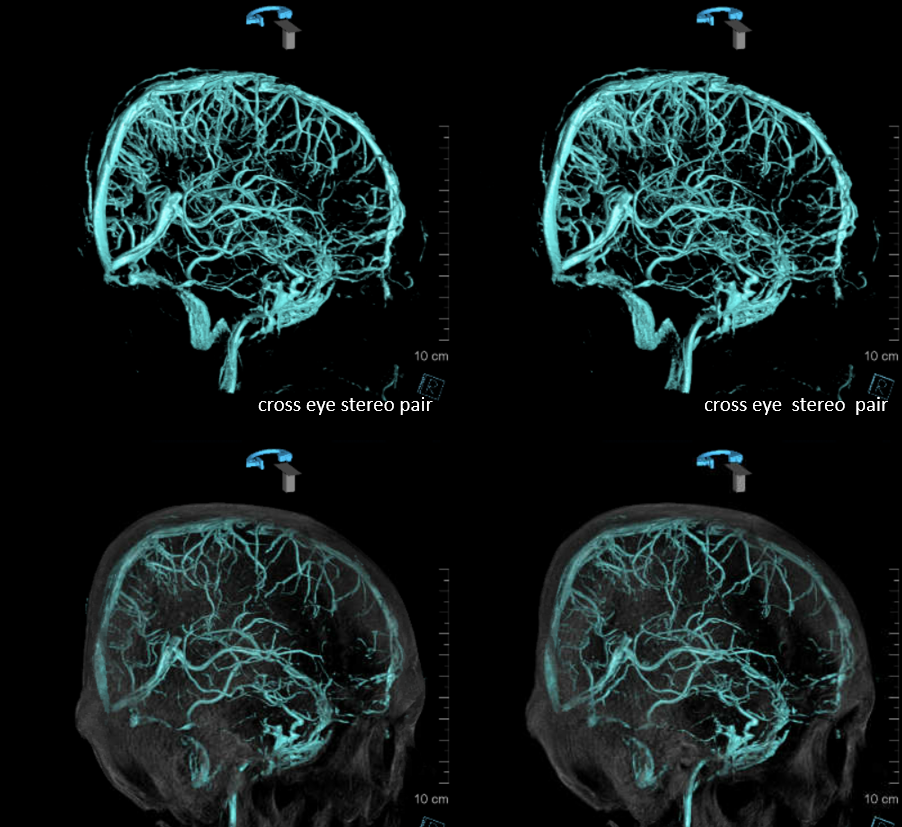
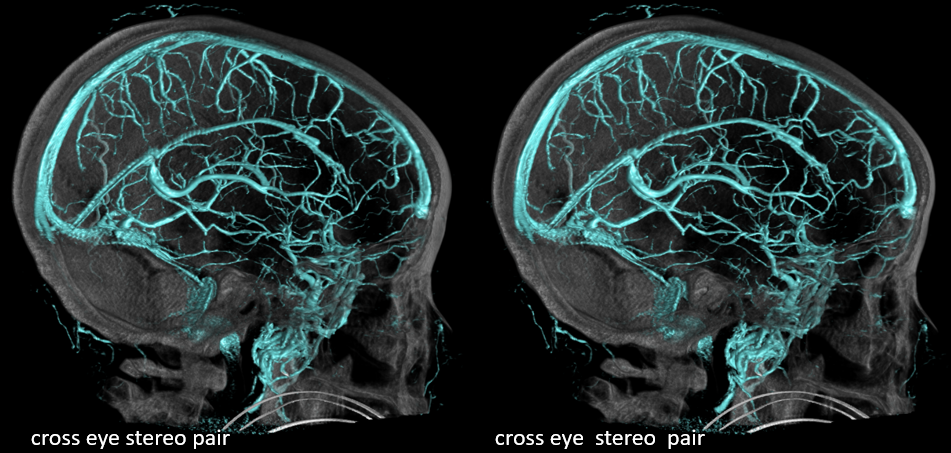
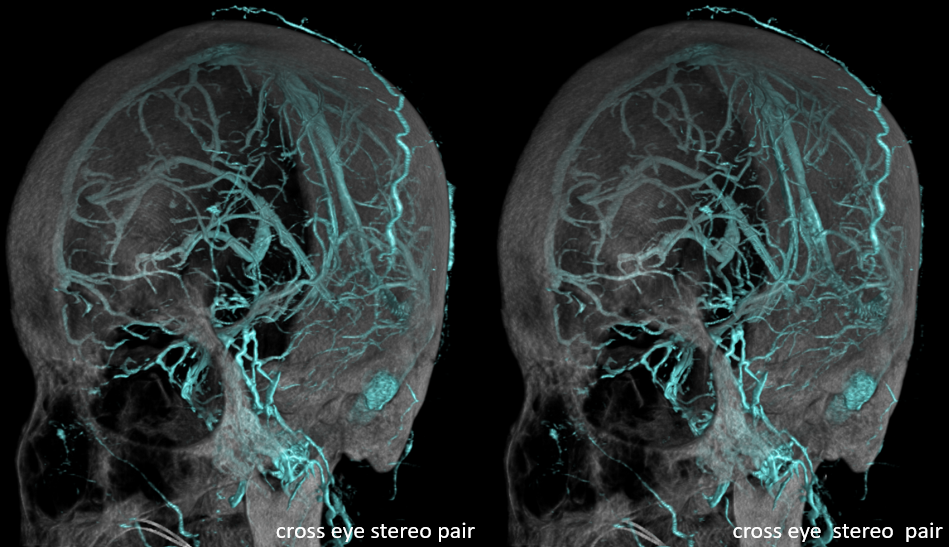
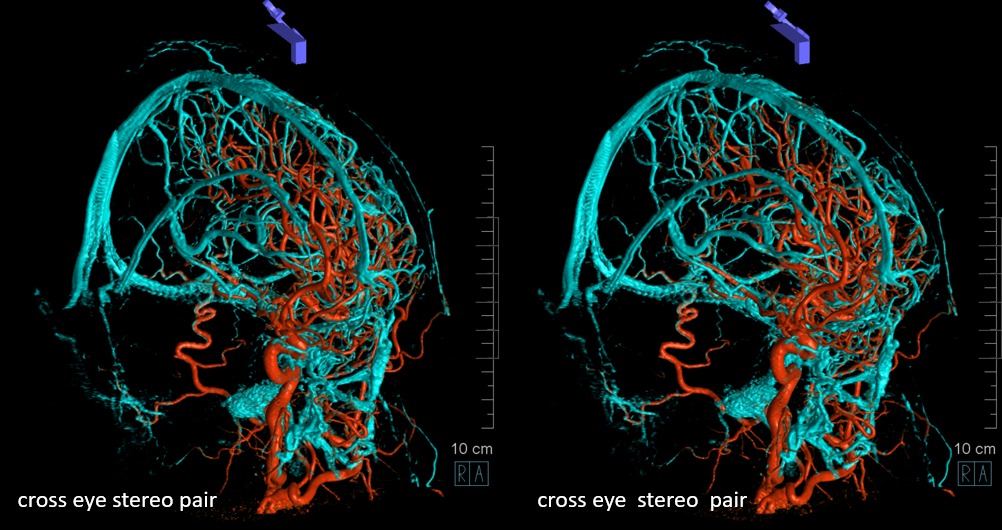
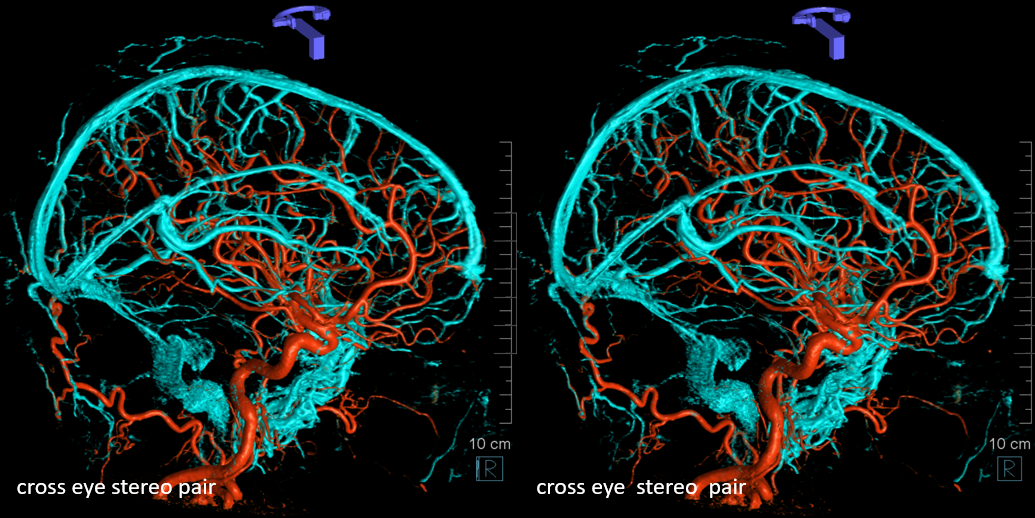
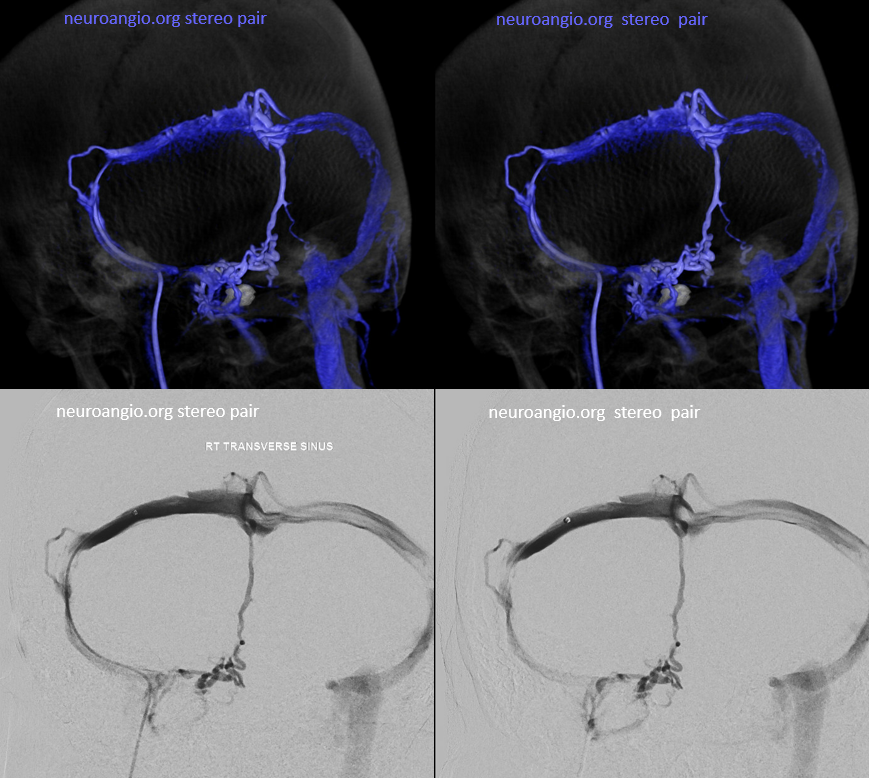
Stereo Pair of diploic veins, cross-eye view
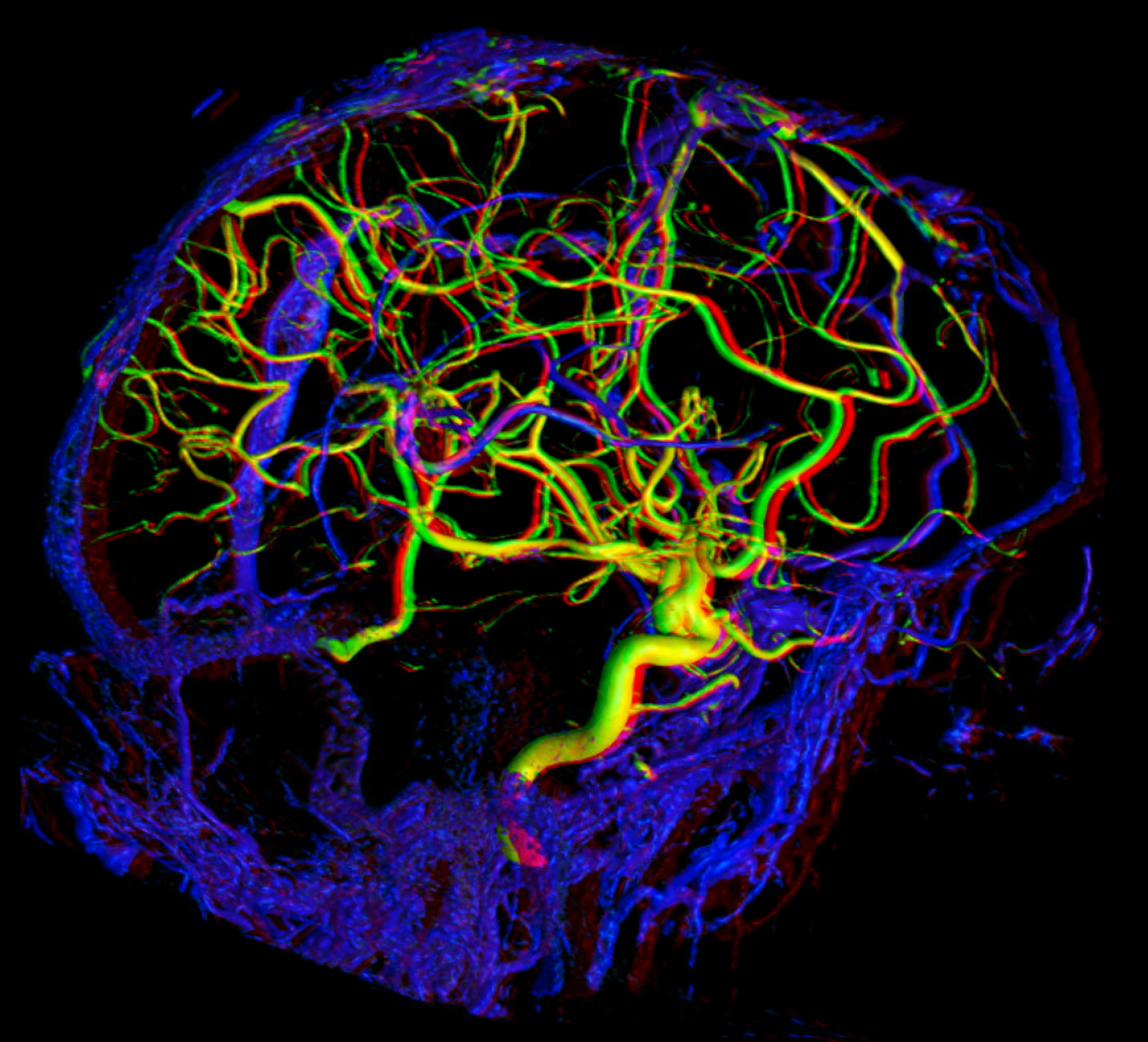
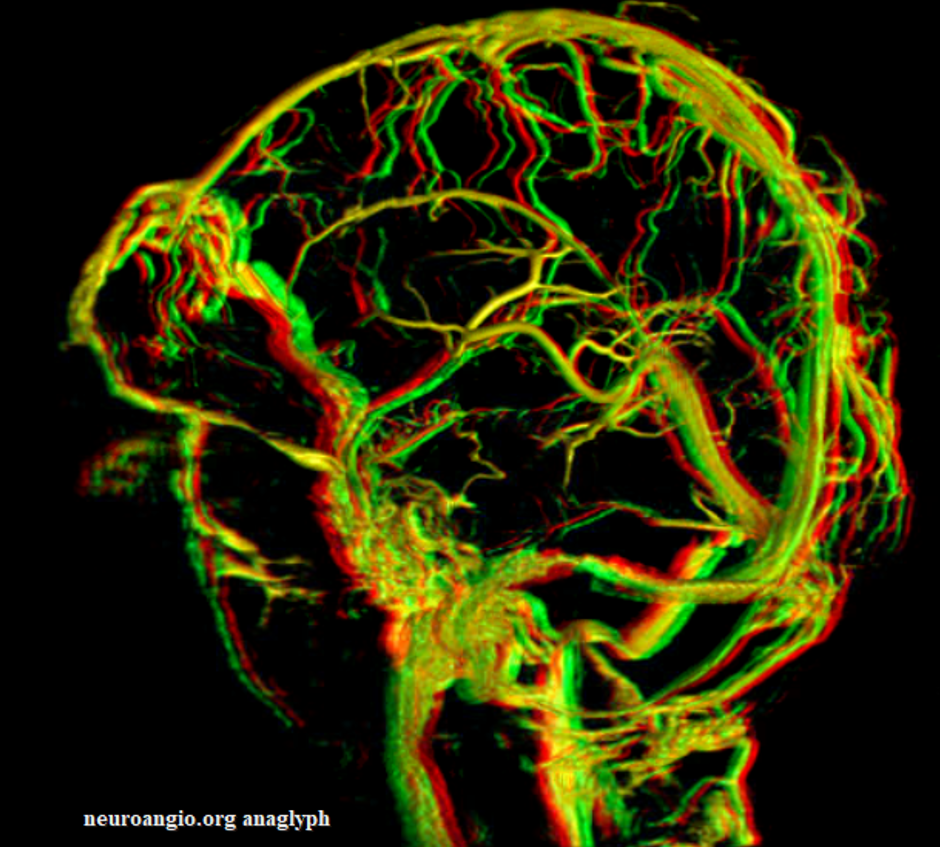
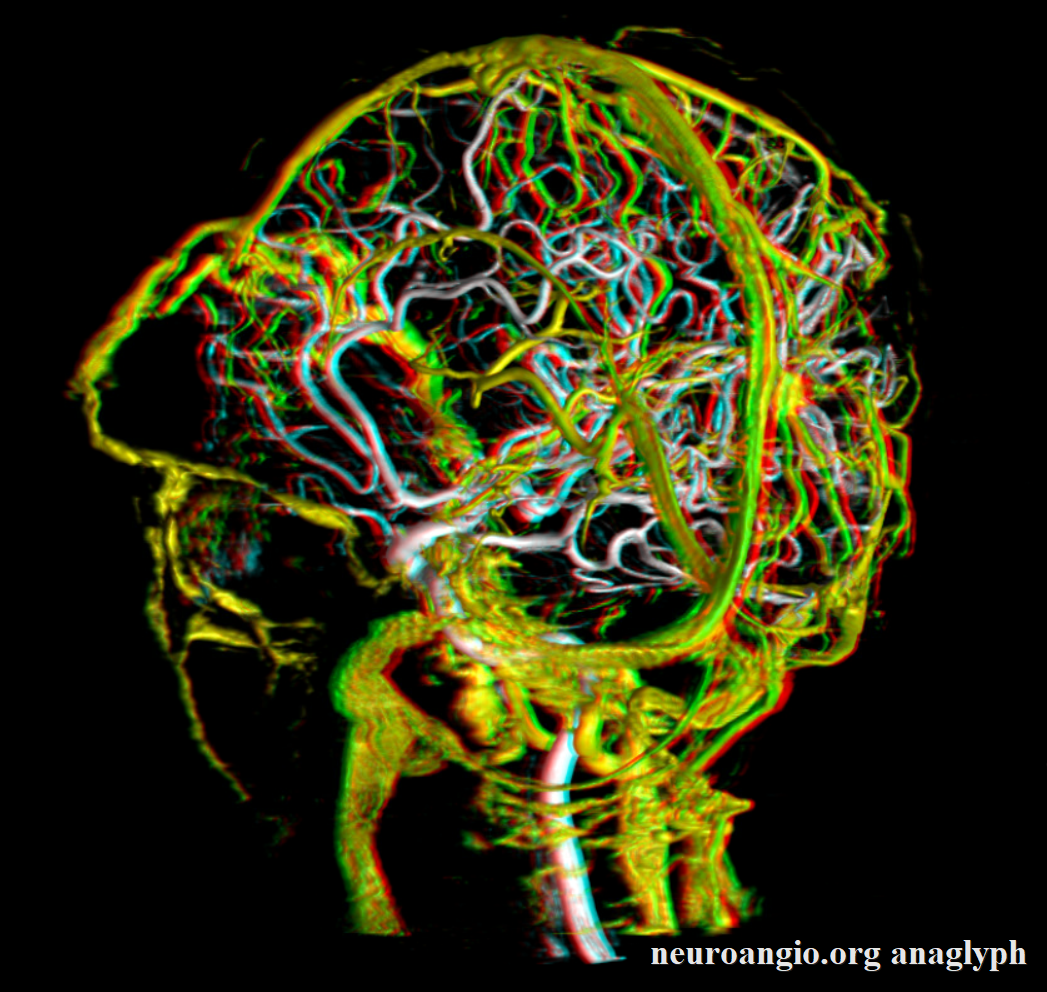
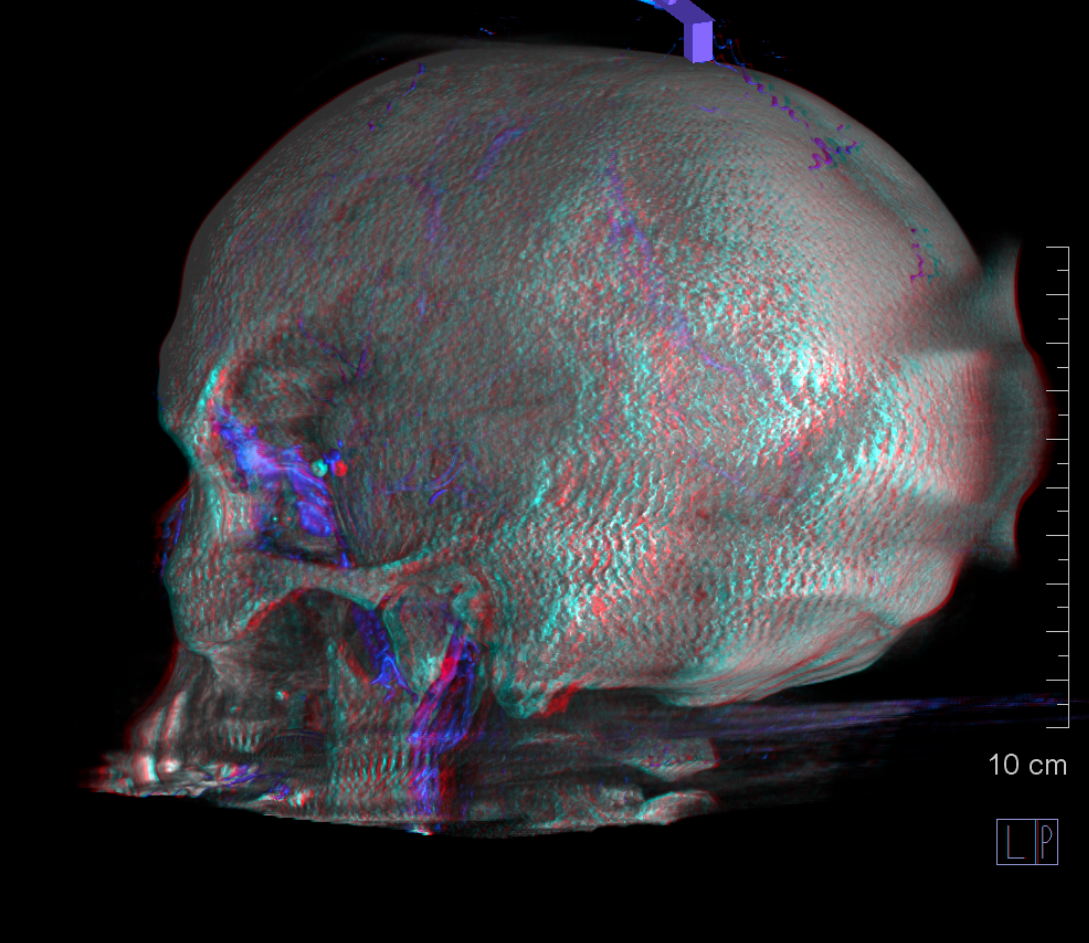
Anaglyph stereo views


MRI example — case courtesy Matthew Young
Same idea — look at small size of the SSS
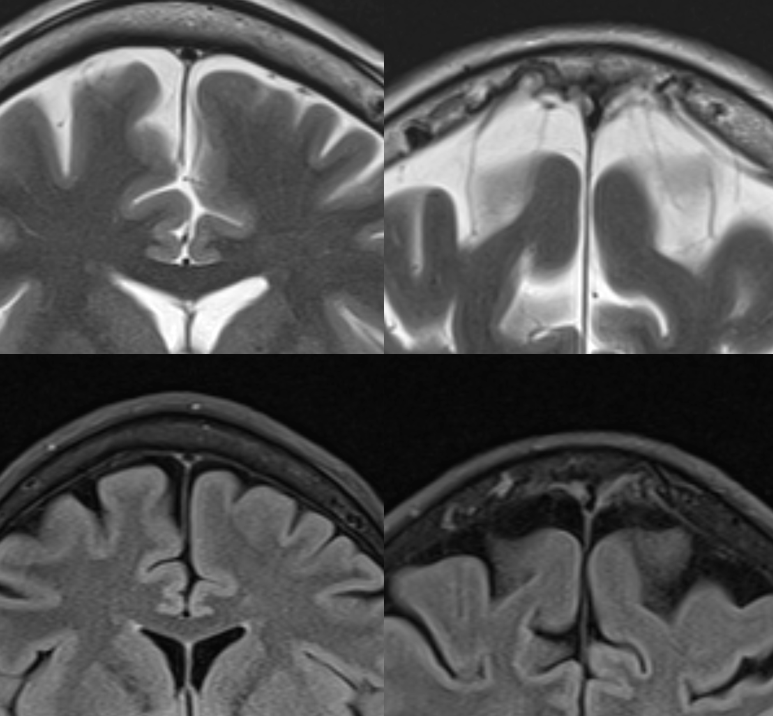
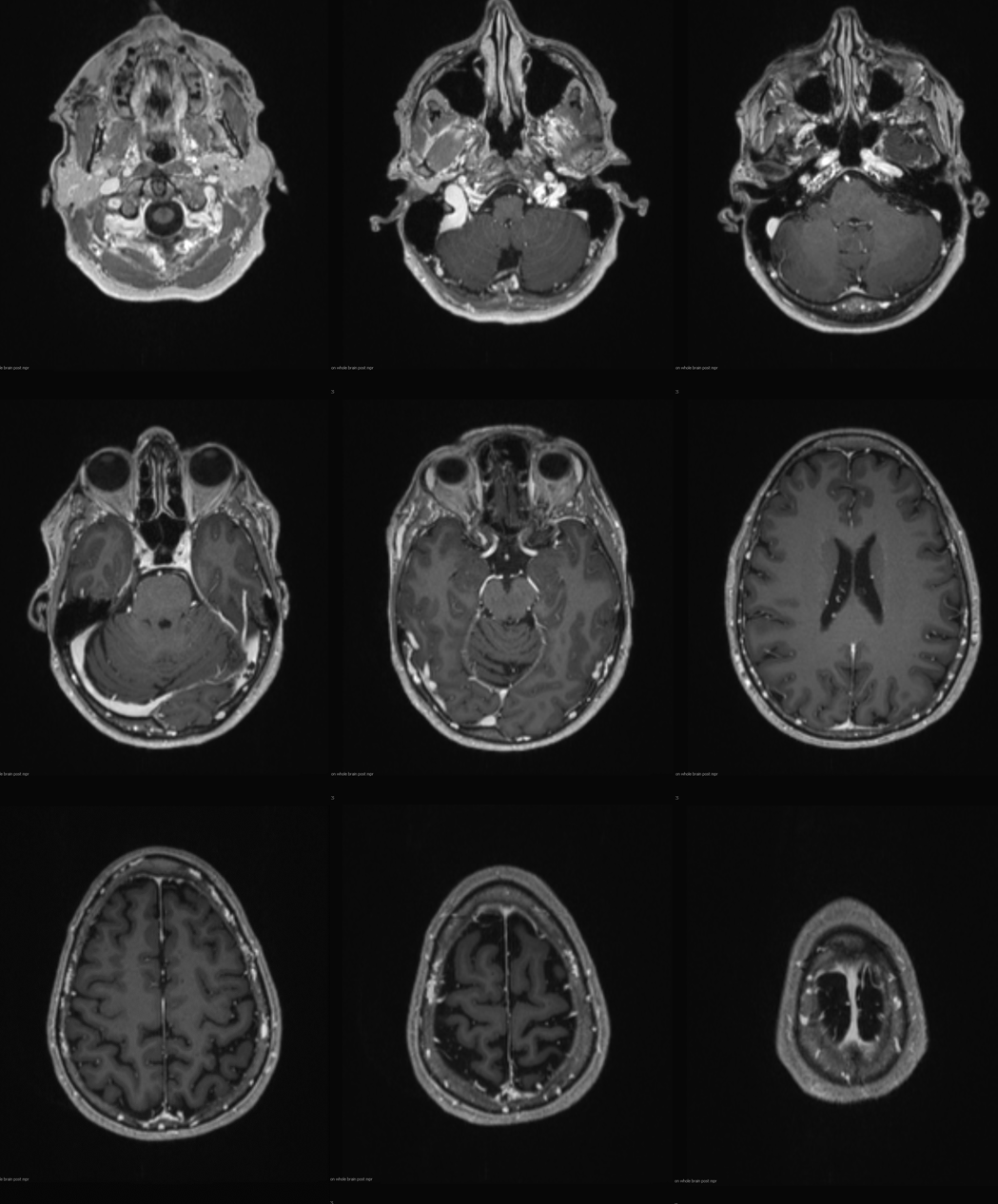
Post T1 — see all those contrast pools in the diploic space, even basiocciput — since his cavernous sinuses are hypoplastic also. Pretty neat, huh
Movie — pause to scroll thru images
Another example – same thing — big diploic veins usually means some kind of stenosis of the SSS
This is something else — nothing to do with diploic veins — but yes has something to do with venous balance… (off the topic!)
back to topic
ANAGLYPHS

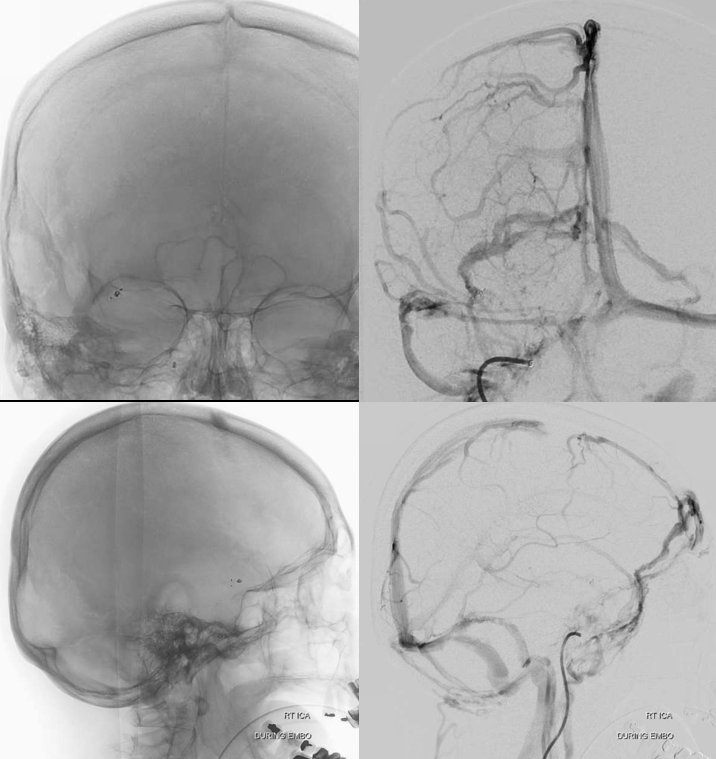
Here are some more examples (one side is marked with black arrows, one with white ones)

Again, these are diploic veins. You know they are thinning the skull because of the lucencies they produce (the actual sharp line is due to a bone-tissue interface). The below digital subtraction angiogram (middle image), in late venous phase, nicely shows the corresponding venous channels filling in the diploic venous spaces seen on the skull radiograph (above and left image). Venous phase unsubtracted view (right image) shows contrast in the vein, for those who still remain in doubt. The patient is post clipping of cerebral aneurysm (no relationship to diploic veins…). It is important to extent the acquisition into late venous phase, since these emissary veins are often opacified quite late.

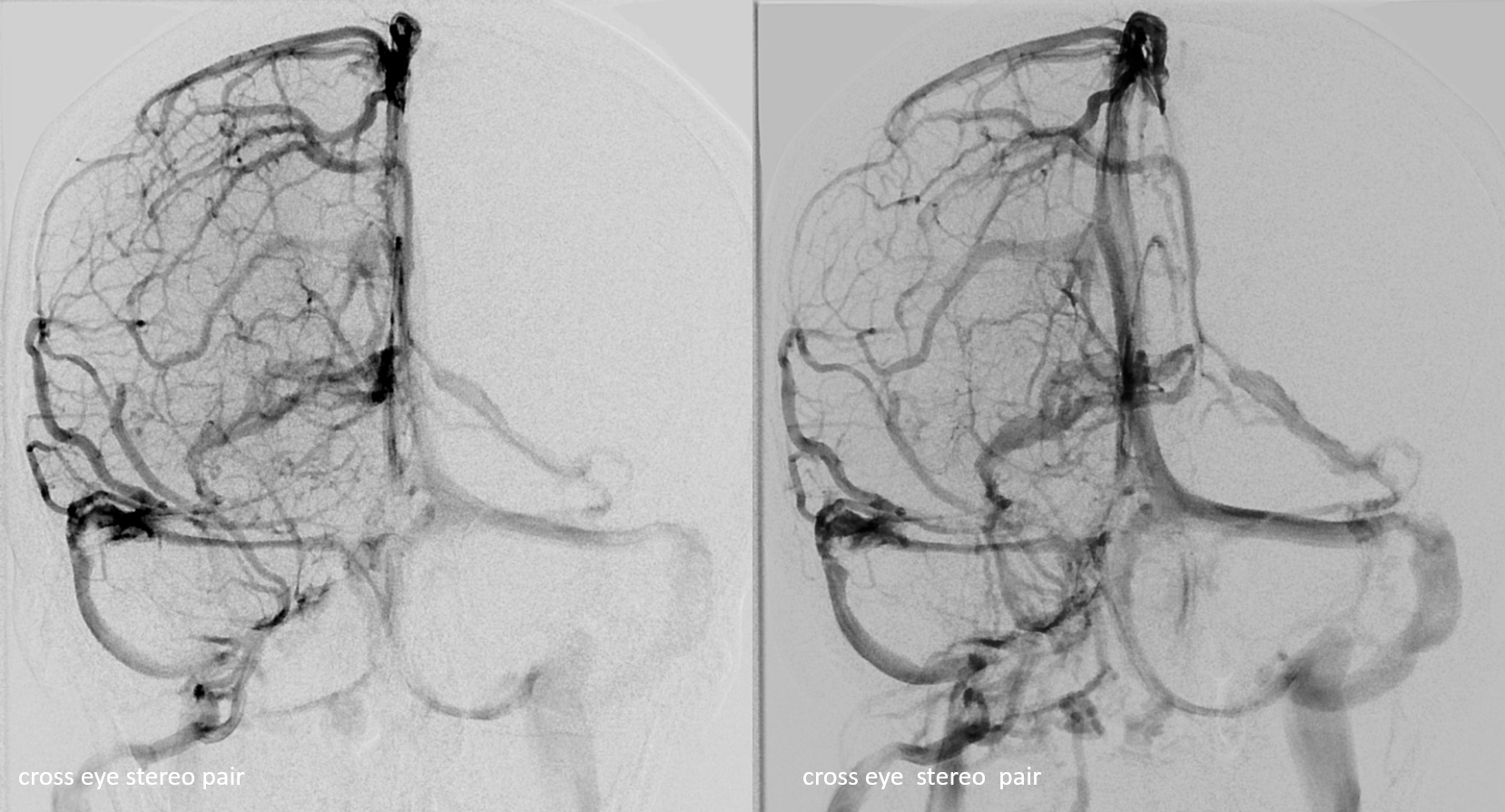
Stereo pairs of the same:

Diploic Veins as intrinsic veins of skull and dura
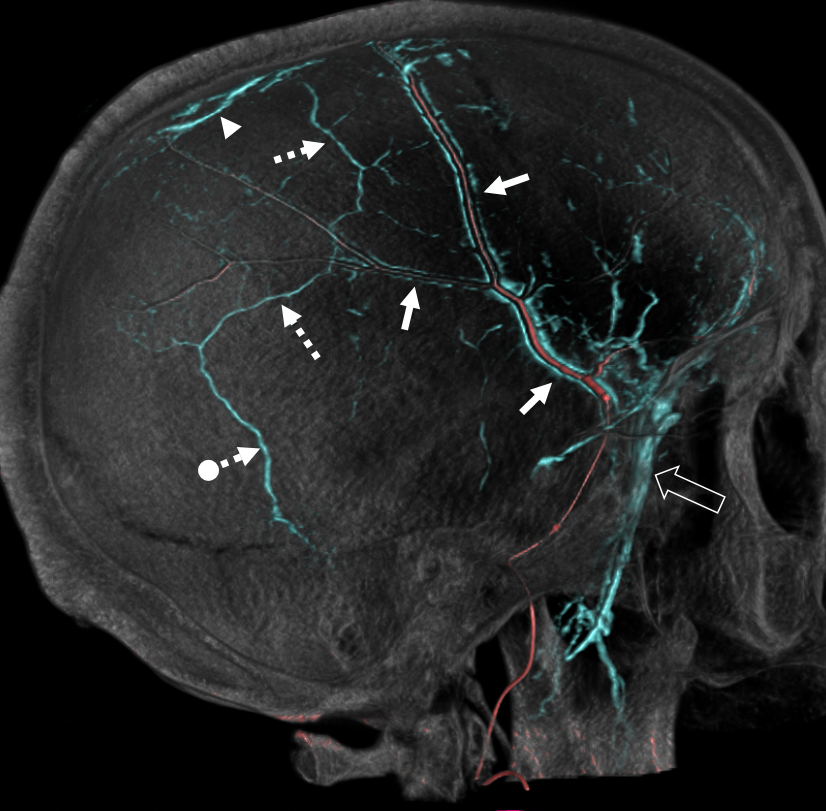
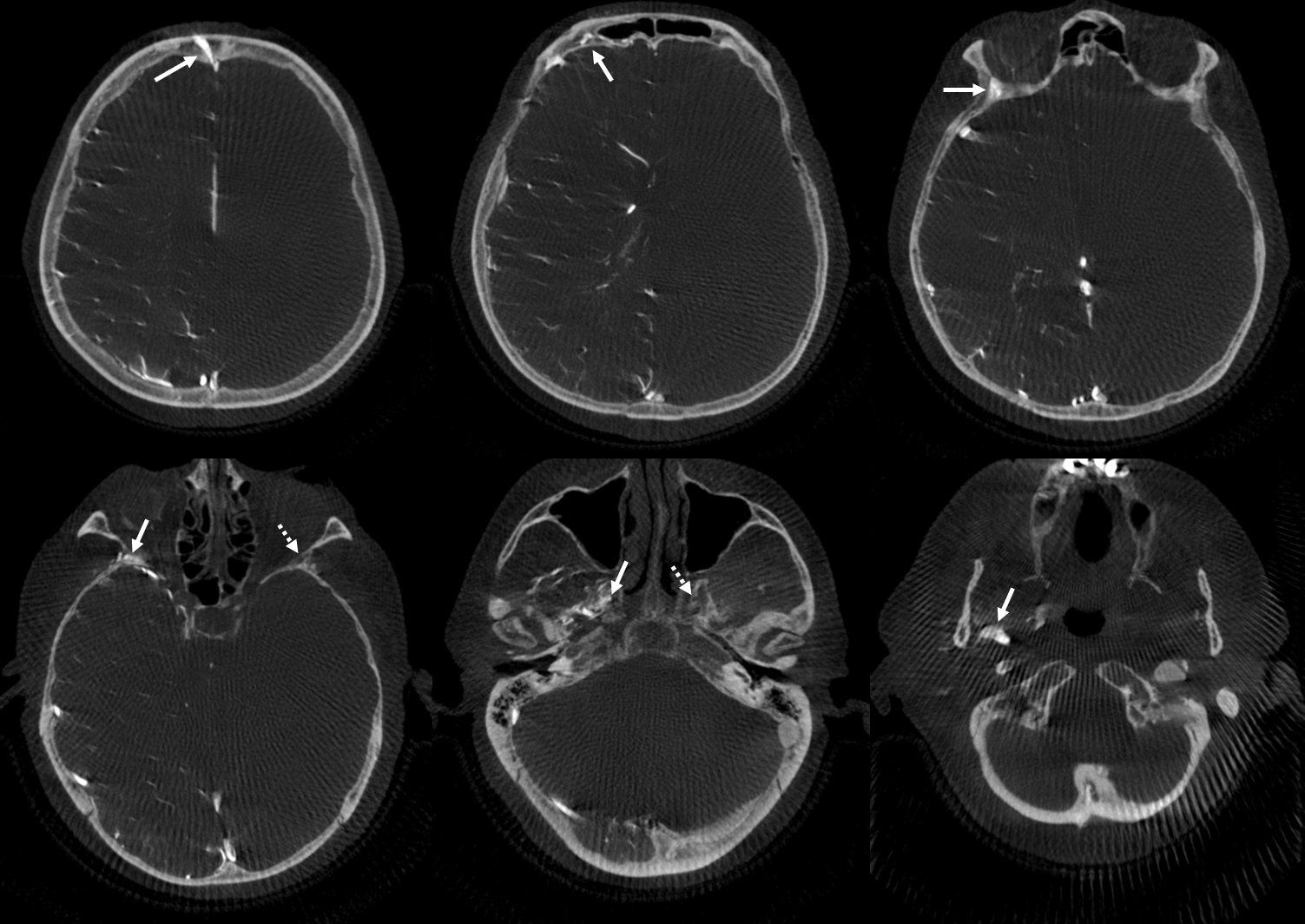
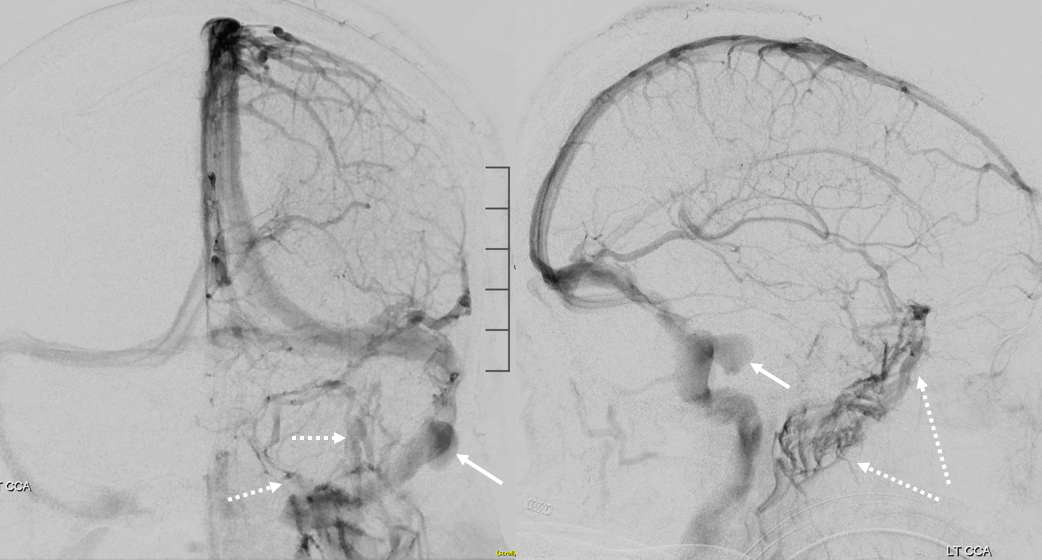
What supplies and drains skull itself? Supply is from whats next to skull — meningeal arteries and superficial vessels such as occipital and STA. How does skull drain — diploic / emissary veins. This is extensively described in our Intrinsic Dural Venous Drainage page. Differentiating skull from dural venous drainage is not easy. However a lot of dura drains into the diploic veins, just like brain does. Some examples of “triple-phase” MMA injections, showing diploic skull veins (dashed arrows) is below. See Intrinsic Dural Venous Drainage page
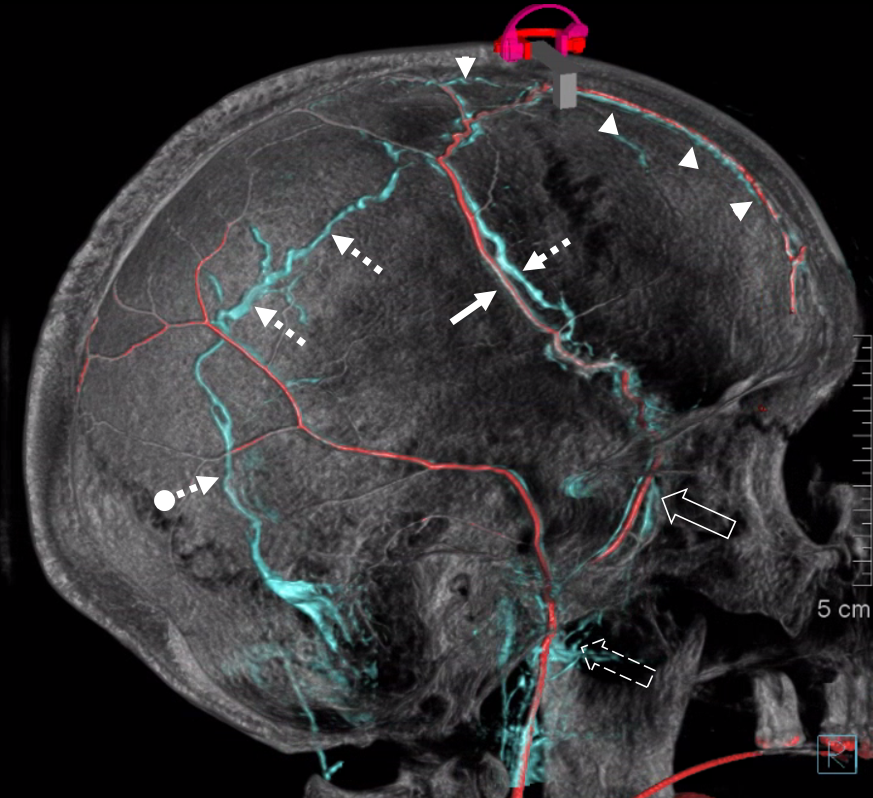
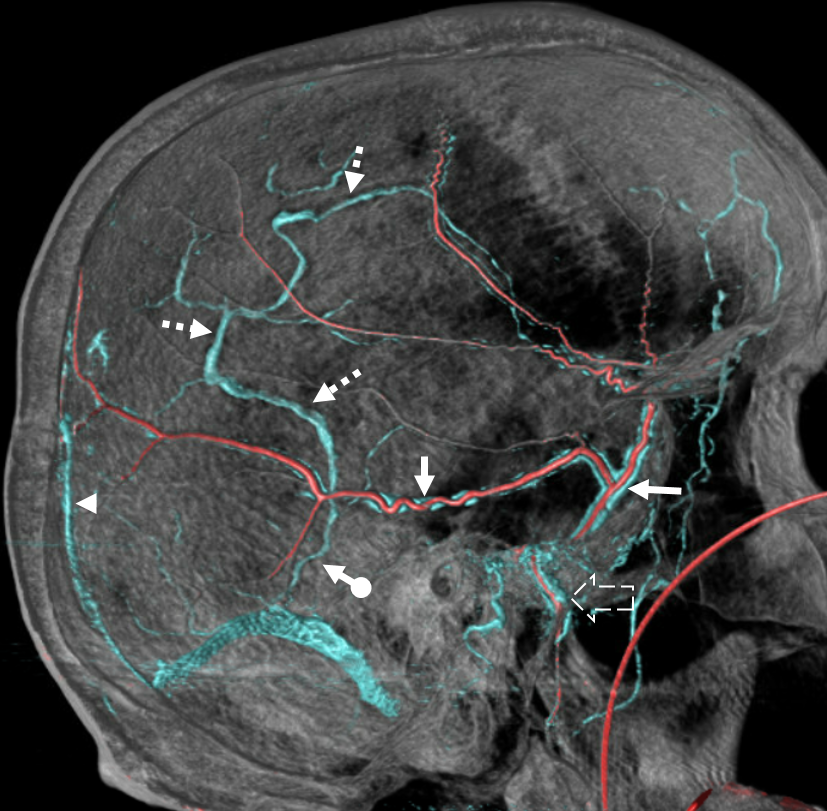
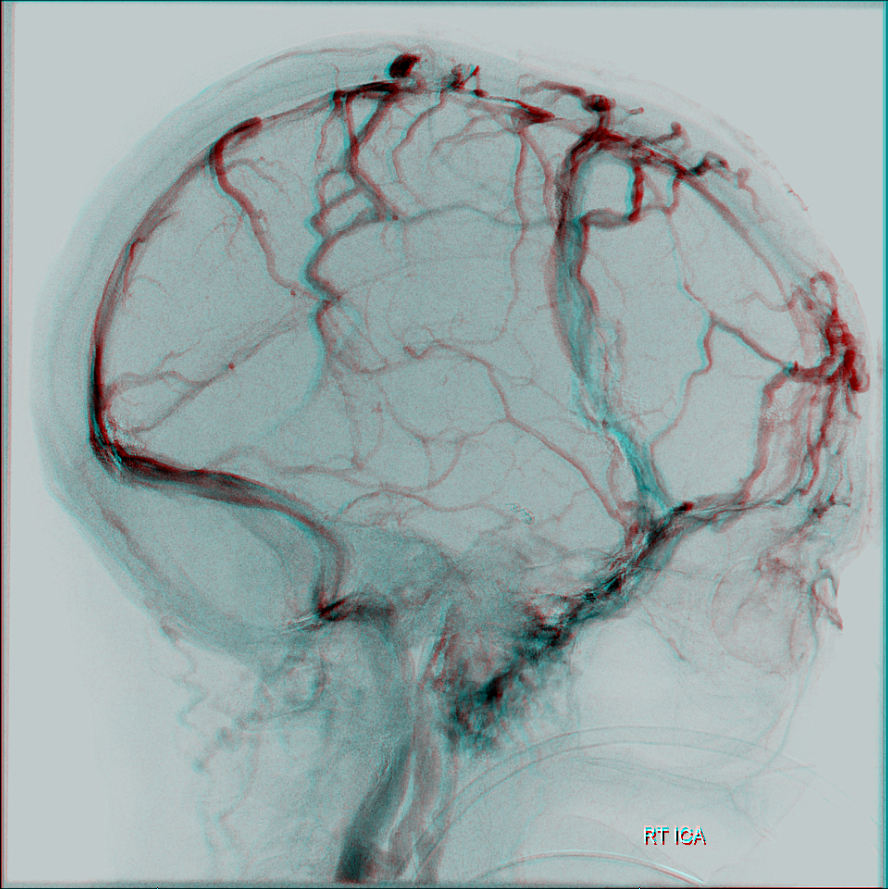
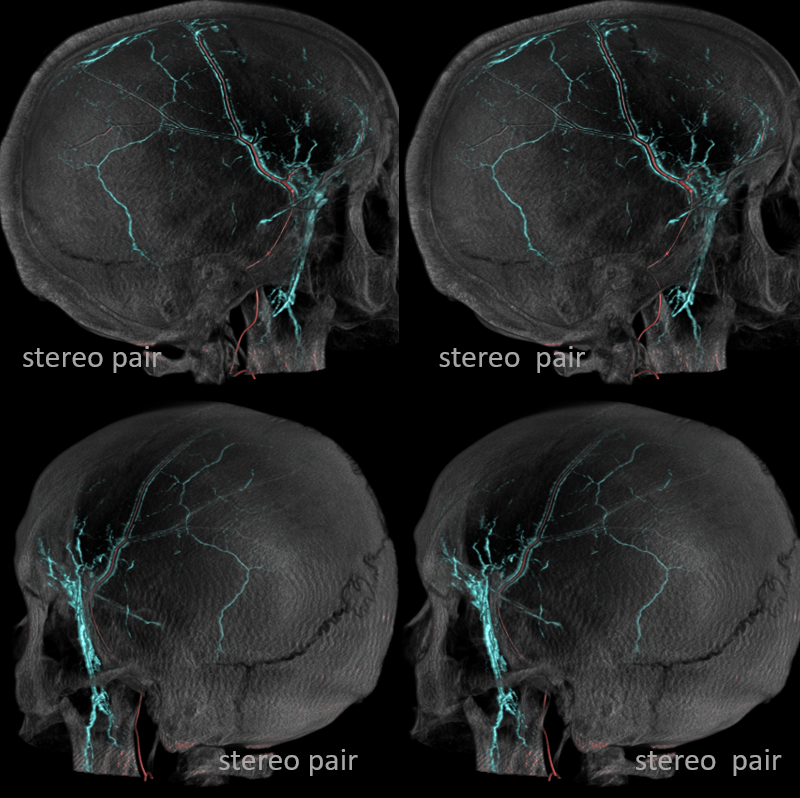
Stereos can help a lot with depth perception — especially when differentiating diploic from dural from extracranial plexus veins. Notice in bottom set the temporalis veins superficial to the skull
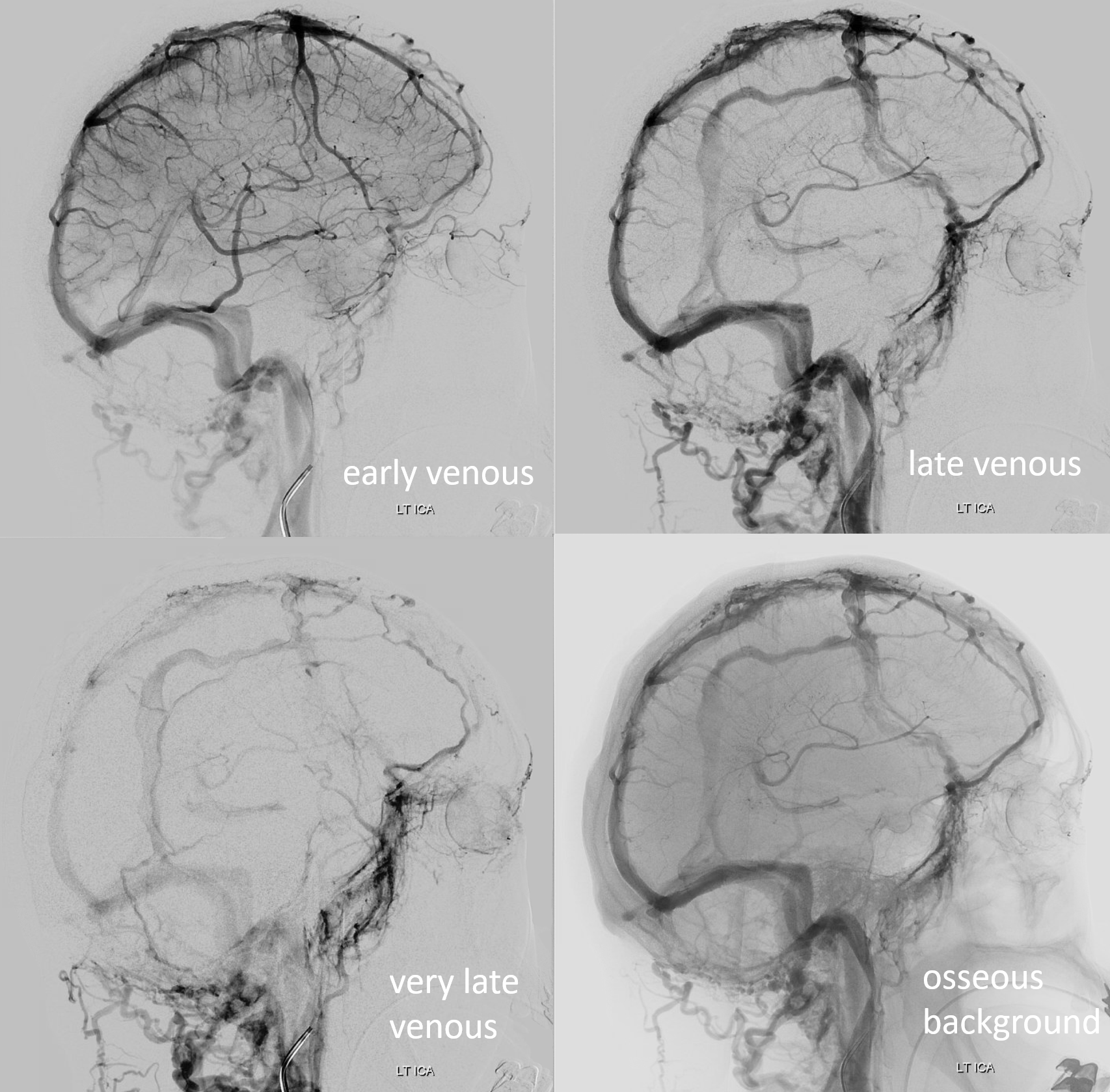
“Second Venous Phase”
Diploic veins drain later than venous sinuses. Keep that pedal down or you will miss them. See how they materialize more and more later on — the “second venous phase”
The linear lucencies in the skull on lateral views are going to be diploic channels — arteries or veins. The MMA ones follow expected course of that vessel. The diploic venous ones are thicker and don’t follow course of arteries
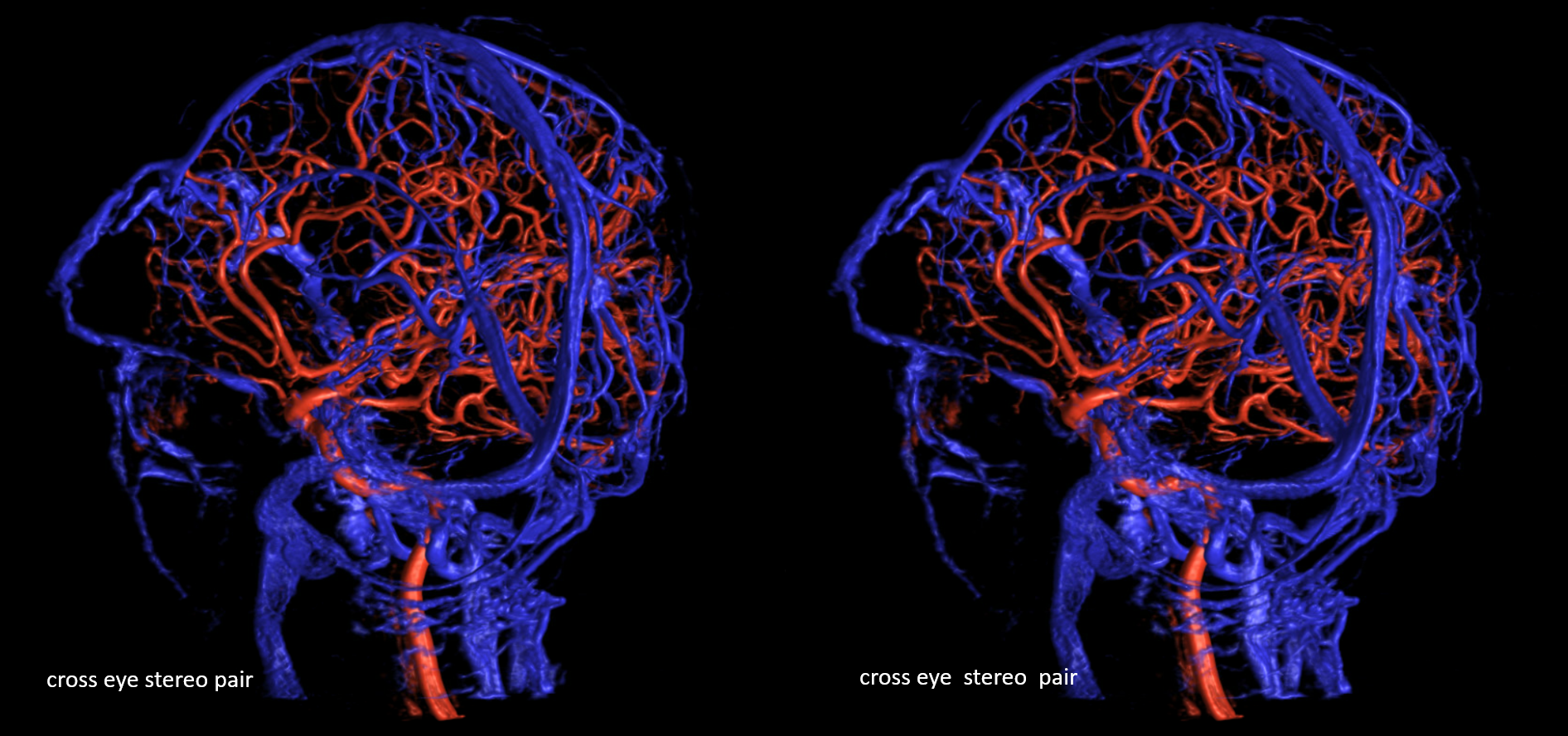
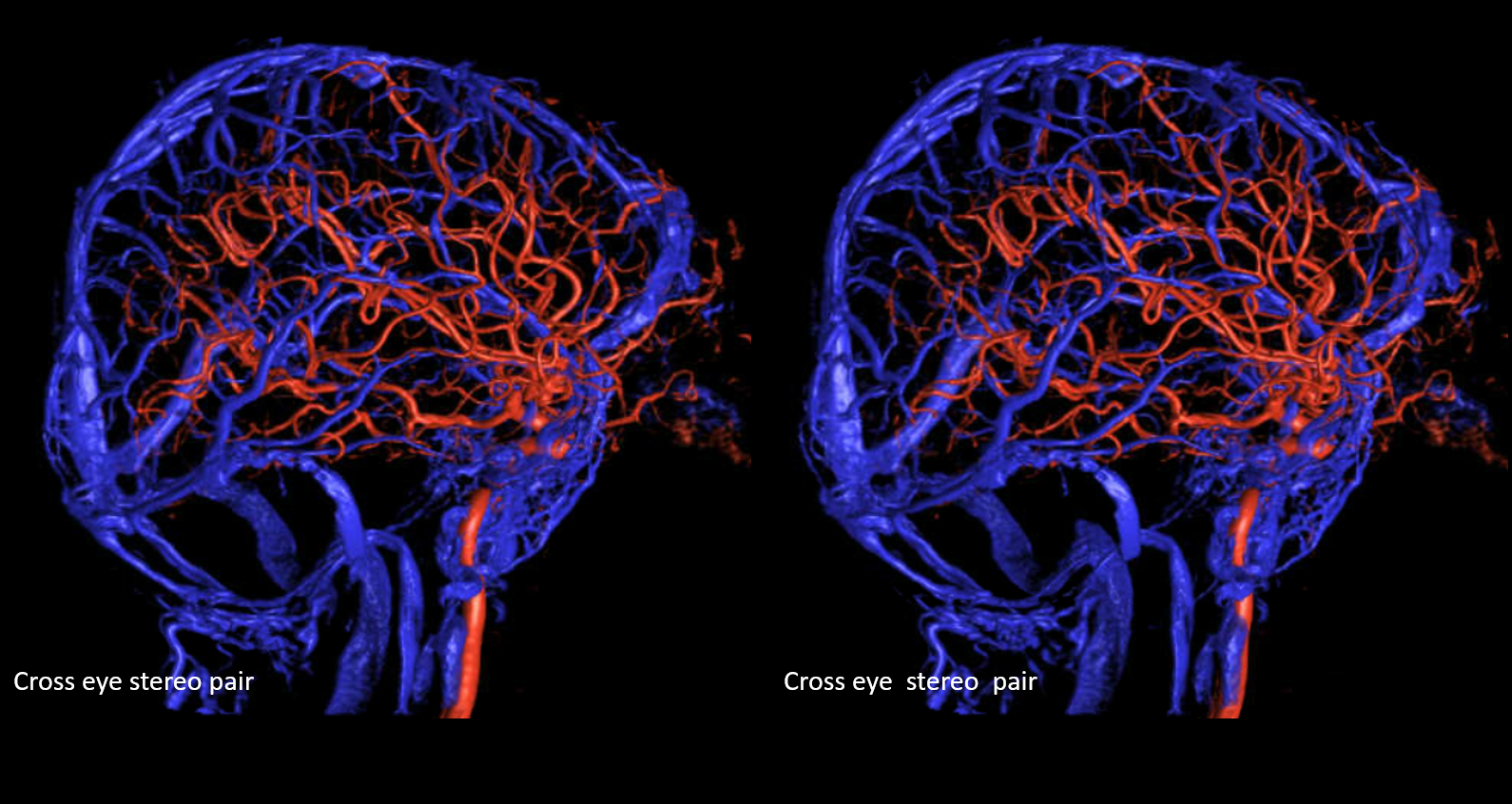
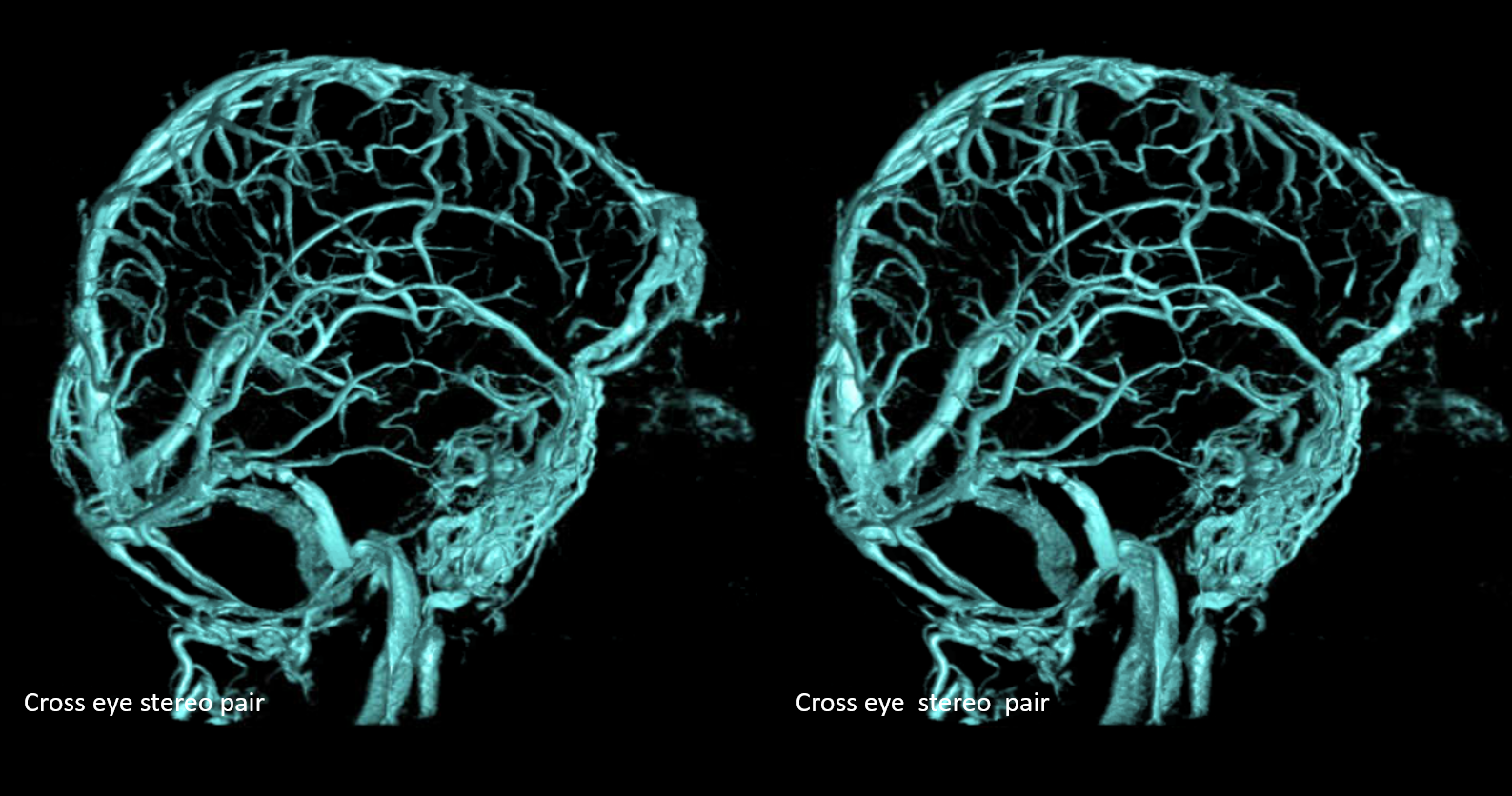
Stereo Pair Venous VR
Movies — pause to scroll thru individual images
FUNCTIONAL SIGNIFICANCE
Frontal Functional Diploic Veins Draining Large Part of Frontal Lobes
These are the ones to pay attention to and not sack during surgery, as they drain lots of frontal lobes
Source data show diploic nature — it is hard to see those lucent channels in the skull when they are so frontal on plain xray or native dsa views
Dashed arrow points to mirror image hypodensity in the diploic space for the left sided veins
Another example of Superficial Sylvian Veins (dashed arrow) draining via diploic channels (arrows) — the so-called sphenoparietal sinus is absent — toward foramen ovale (arrowhead)
All same case — also has a rare foramen cecum vein
Angio is a bit less impressive — thats why paying attention is important
Movie — stop and scroll through images
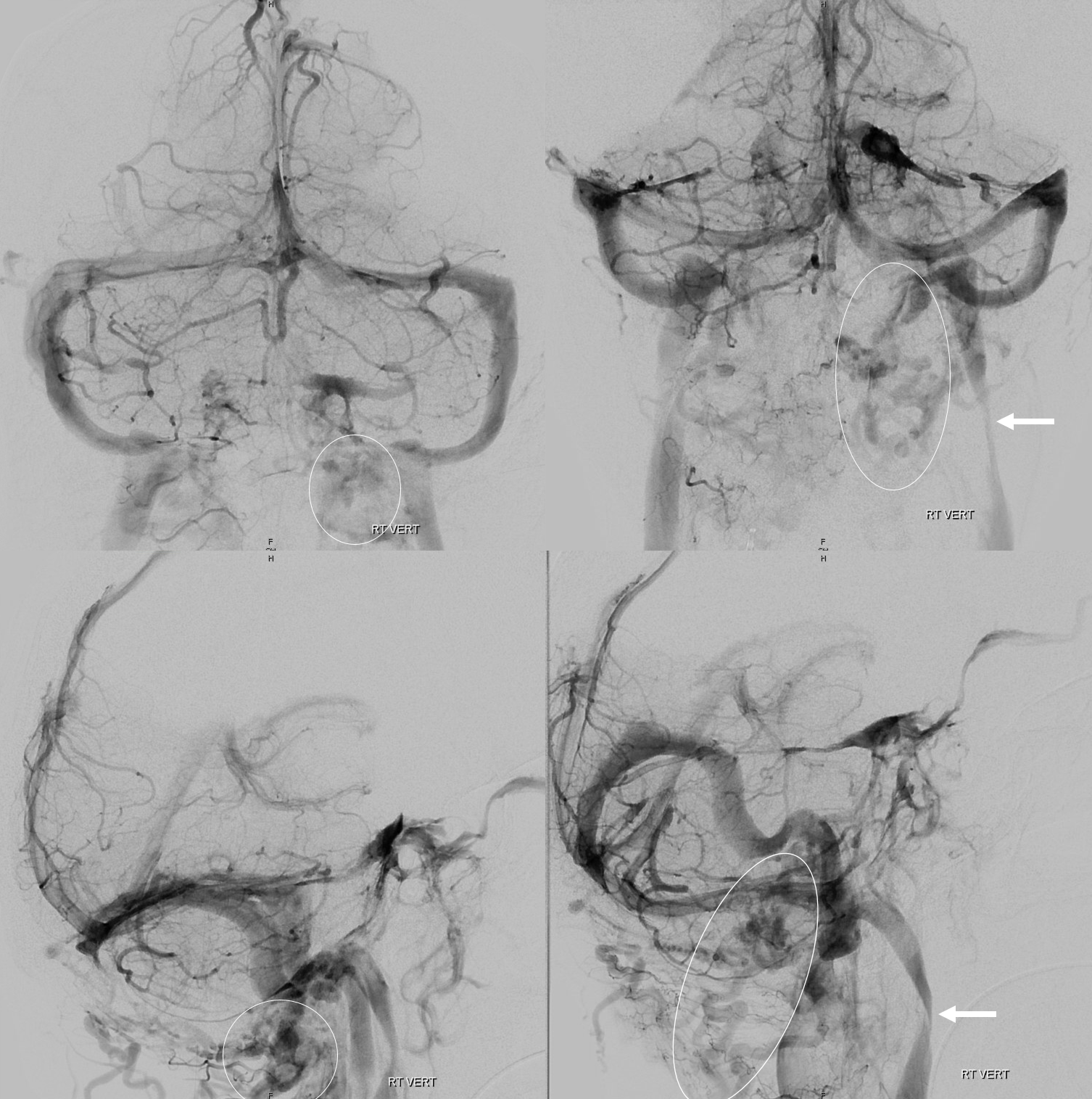
More large and unusual diploic veins – here is one draining superficial sylvian veins into all the way into the sigmoid sinus — the embryology of this as one of the primitive sinuses can be debated
Single plane stroke case — no cute flat panel images
Sphenoid wing/temporal large diploic veins draining superficial and deep sylvian veins
GIF of MMA injection shows drainage of dura and skull into prominent diploic and emissary veins
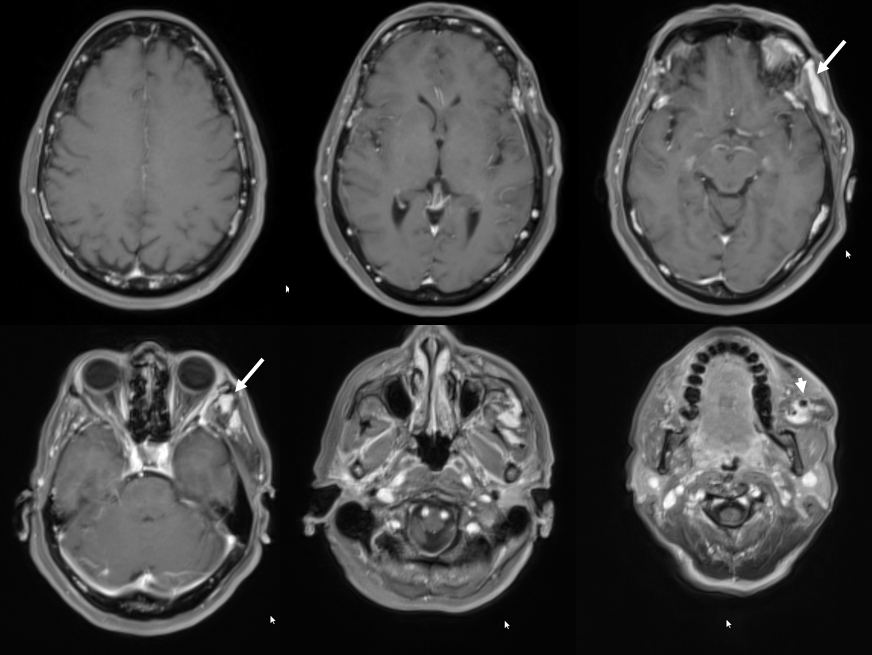
Functionally important diploic veins — facial “Venous Malformation”
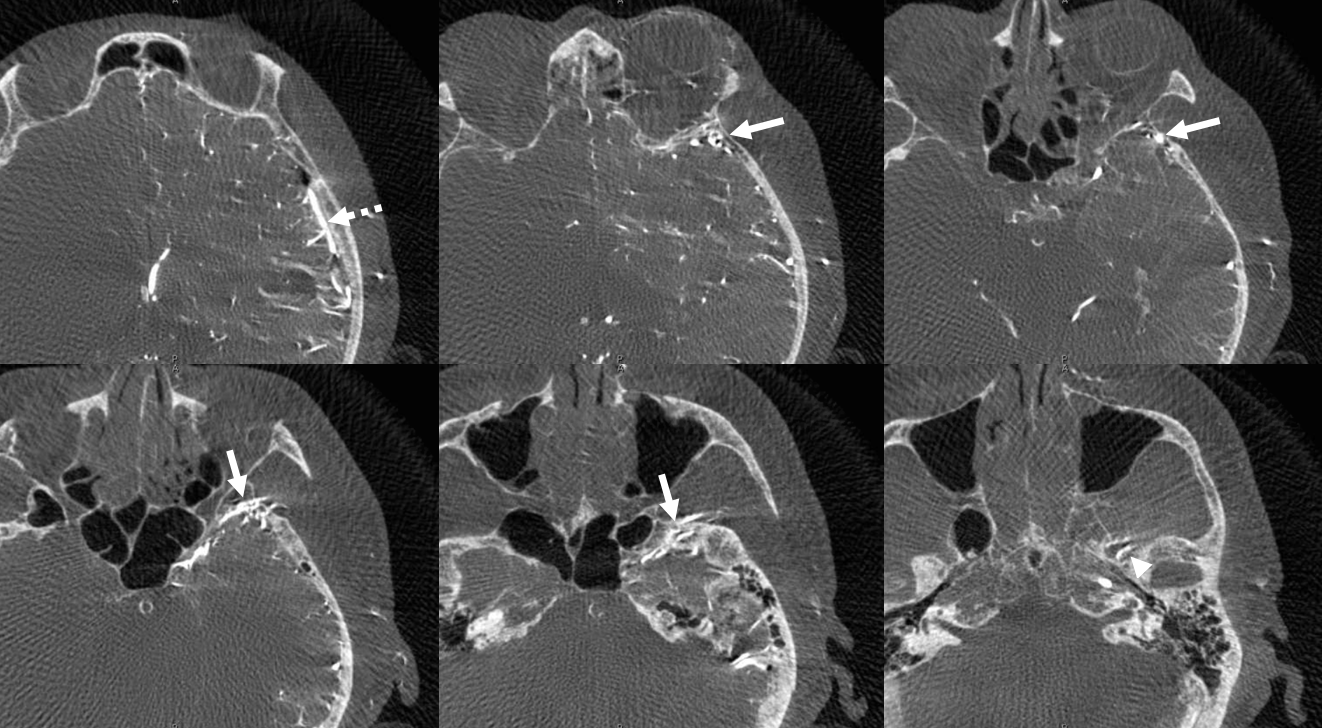
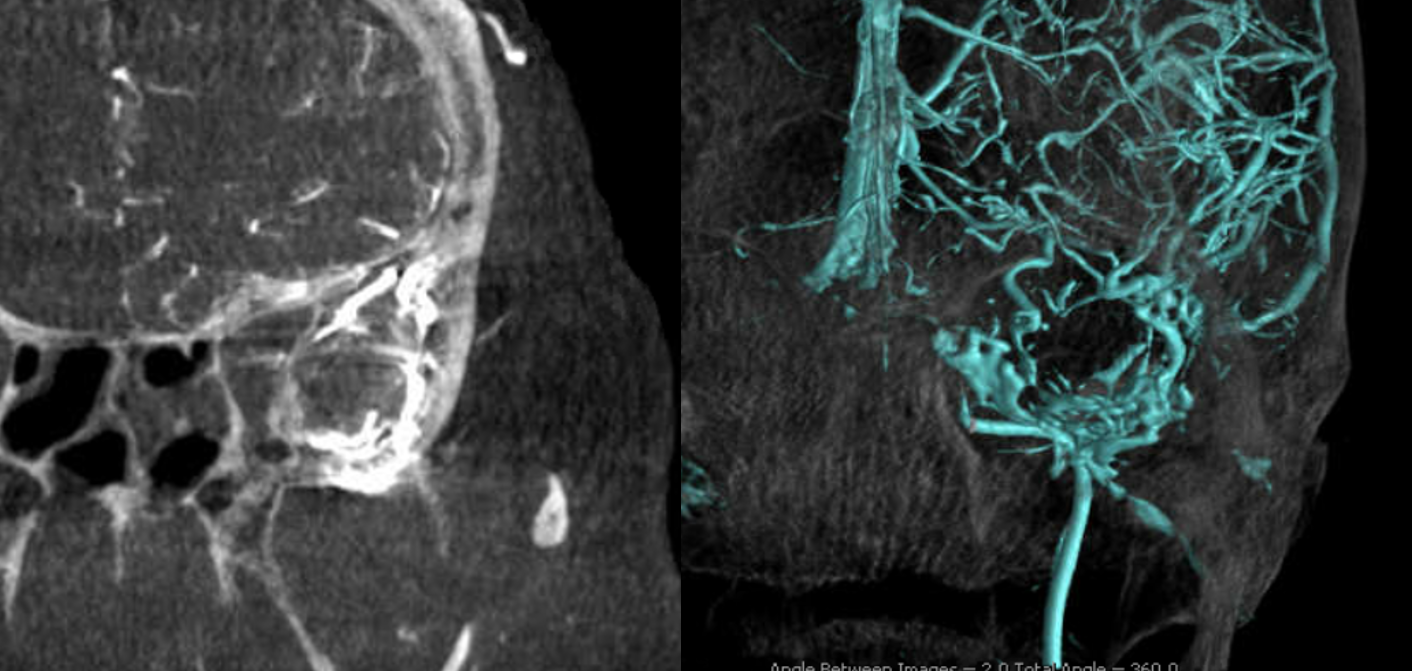
Below is an example of why these veins matter. Example of how diploic veins compensate for not having the usual venous apparatus in place. Here is a patient referred for sclerotherapy of facial venous malformation. There are two parts, upper temporalis (white arrows) and cheek/buccal (white arrowhead)
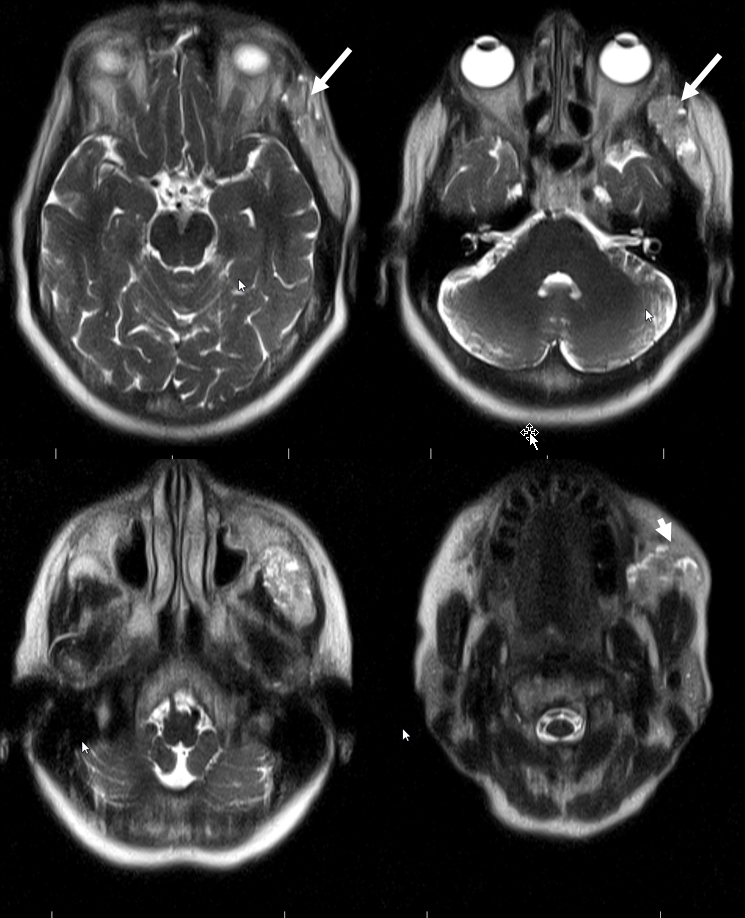
Postcontrast MRI. Same arrows. The arrowhead points at a phlebolith
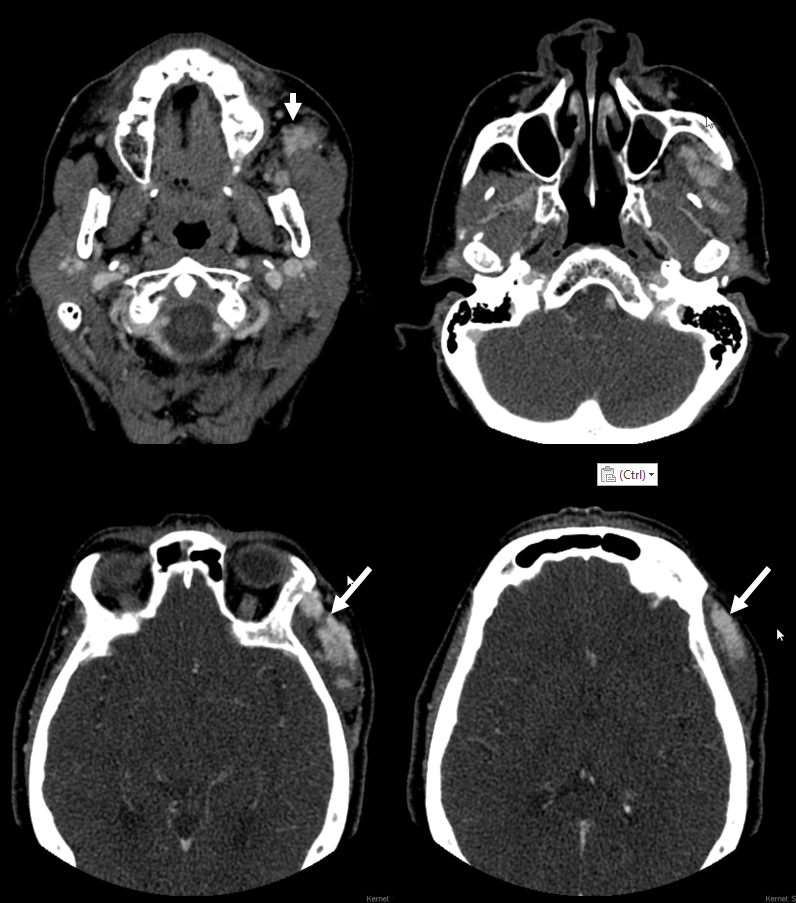
CT shows some contrast in both areas. there is a lot of heterogeneity among vascular lesions, but this much contrast in a late CTA kind of setting is a bit unusual
We, fortunately, do an angio. The right side is OK
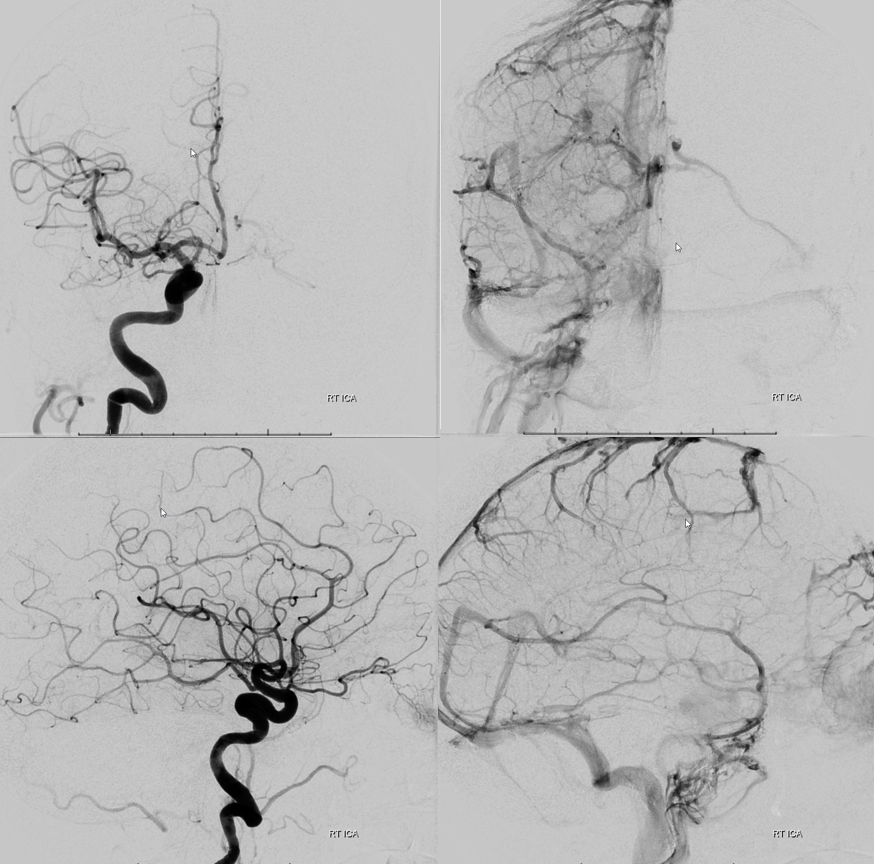
Frontal views of left side. Strange-looking images, right? Arrow points to same temporalis venous pouch as seen on MR and CT
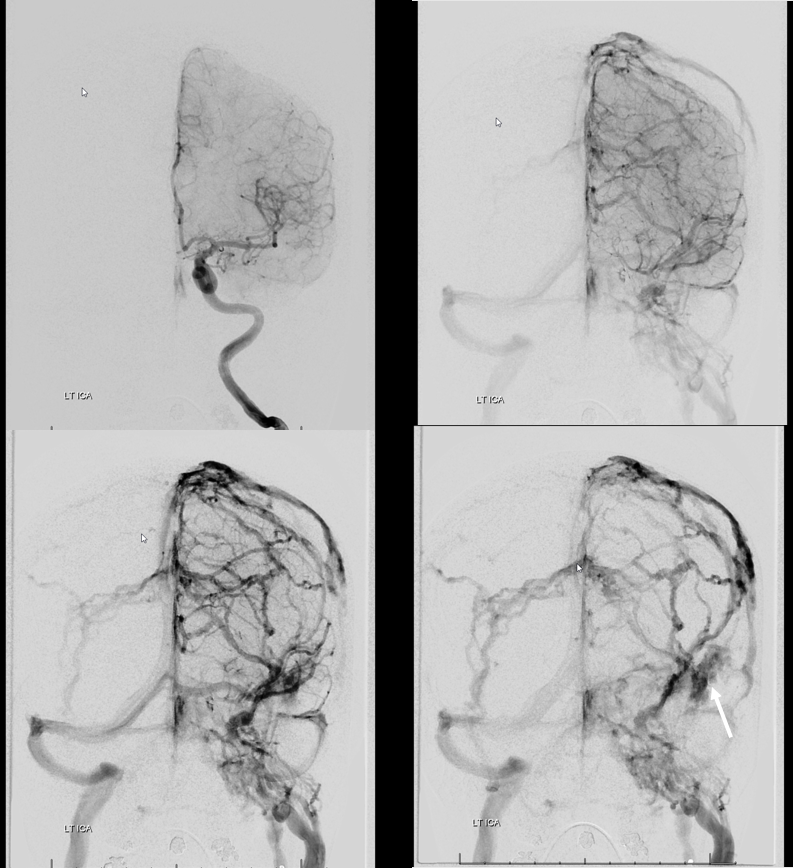

Lateral views. Arrow points to the same point as on CT and MR studies above. There is hypoplasia of the frontal portion of the superior sagittal sinus. The frontal lobe drains via multiple diploic/emissary veins into the same venous pouch in the temporalis region.
Dyna CT of the left ICA injection. Yellow arrows point to diploic venous lakes/channels which ultimately drain into the pterygopalatine fossa and into the temporalis region.
Movie of same — pause it and scroll thru individual frames
Nice anaglyph views



Movie
Conclusion is that the temporalis abnormality is not a venous vascular malformation but rather functionally necessary venous egress for left frontal lobe. Thus, sclerotherapy was only performed for the cheek region, not temporalis.
Finally, another example of a similar disposition in a patient with Chiari Malformation. Relationship is not certain, but possibly crowded posterior fossa influences development of other outflow routes.
FUNCTIONAL SIGNIFICANCE
Diploic venous channel “collateral” bypassing a long-standing venous sinus stenosis. A nice example of how important it is to sent the right channel…

See also: Venous Sinuses Page