Any creature with a trigeminal nerve has a trigeminal artery, which has as much right to life, liberty, and pursuit of happiness as facial or hypoglossal, for example. Which is why the adage “Persistent” is a misnomer. Yes, we all call it that, but it is important to recognize that this term is a product of an earlier, incomplete understanding of vascular embryology. Although the trigeminal is usually below angiographic resolution, it nevertheless exists in everyone. It is seldom the vessel selected by development to serve as an intracranial anastomosis between the anterior and posterior circulations — even the more usual PCOM is far from constant, and subject to the important embryologic variation of the fetal disposition. The great Lasjaunias considered the PCOM to be an integral part of the anterior circulation (caudal ramus, see dedicated Neurovascular Evolution page). However, some have challenged that notion on the basis of certain internal carotid artery variations that do not seem to conform to Lasjaunias’ model, and proposed that the PCOM is in fact an anastomotic vessel, like the trigeminal. This, to me, seems to be at odds with the nature of the trigeminal artery as the vessel of the first branchial arch, which seems to have no correlate to the PCOM; I have no proof for either idea, but love to digress, as happened just now…
Getting back to the point, the trigeminal artery is an important potential conduit between the carotid and basilar arteries. It does follow the course of the trigeminal nerve. The classic anastomosis is between the basilar trunk, between the AICA and SCA, and the MHT of the ICA. In the full spectrum of possibilities, the trigeminal can arise from either the MHT or the ILT, and anywhere between the SCA and the AICA , including rare variants where it is the exclusive source of either complete or partial AICA and SCA territory supply (see below). Presence of the trigeminal artery need not imply hypoplasia of the PCOM; in fact, in most instances of angiographically resolvable trigeminal, the PCOM is present as well.
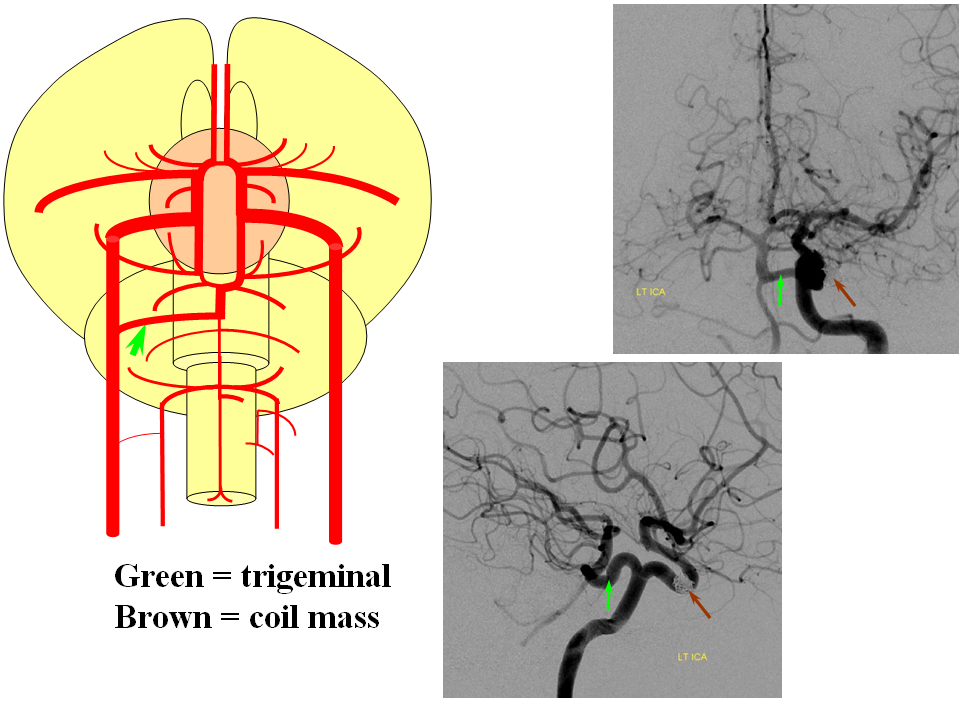
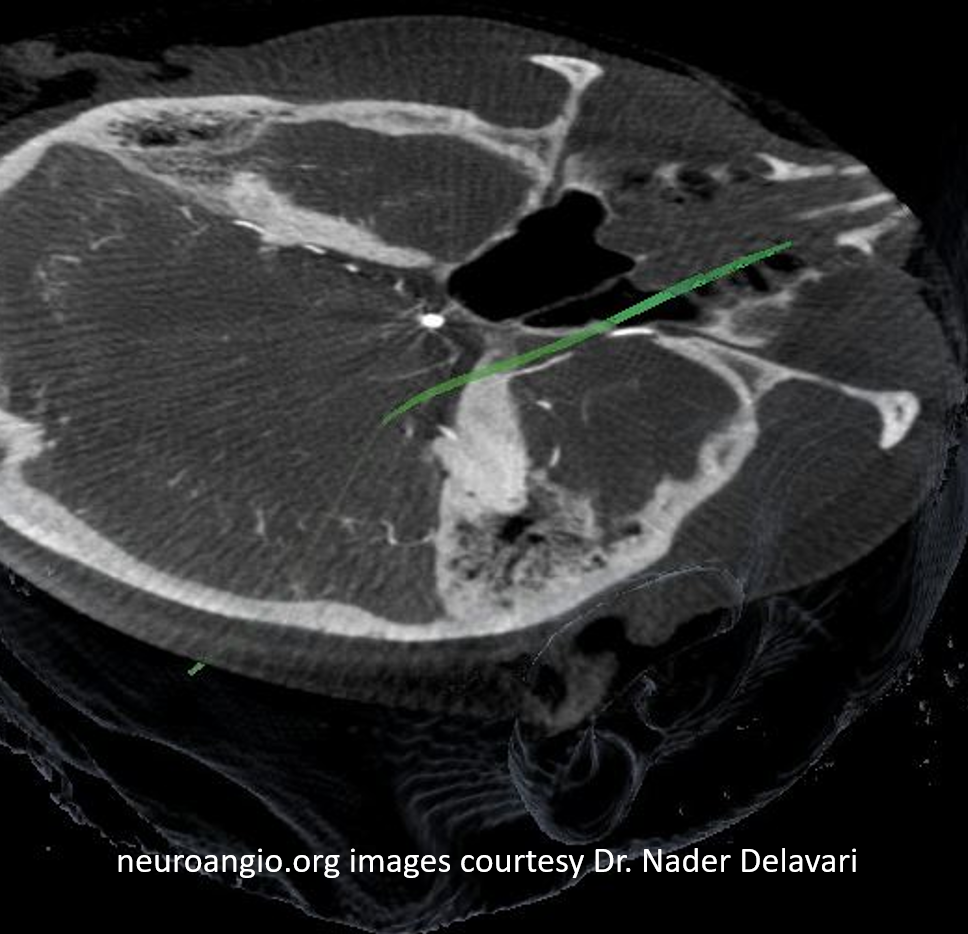
Here is an example, also found on the Neurovascular Evolution page; the “classic” trigeminal (green arrows) extends from the basilar trunk between the AICA and SCA, to the MHT, and is associated in this case with hypoplasia of the PCOM. Essentially all vascular variants are associated with a slightly increased incidence of brain aneurysms, as evidenced by the coil mass (brown arrows)
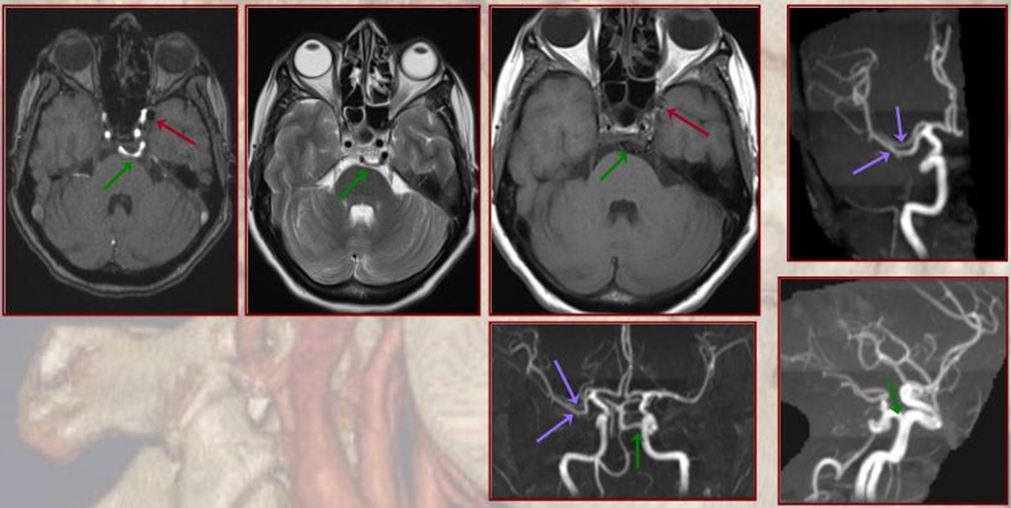
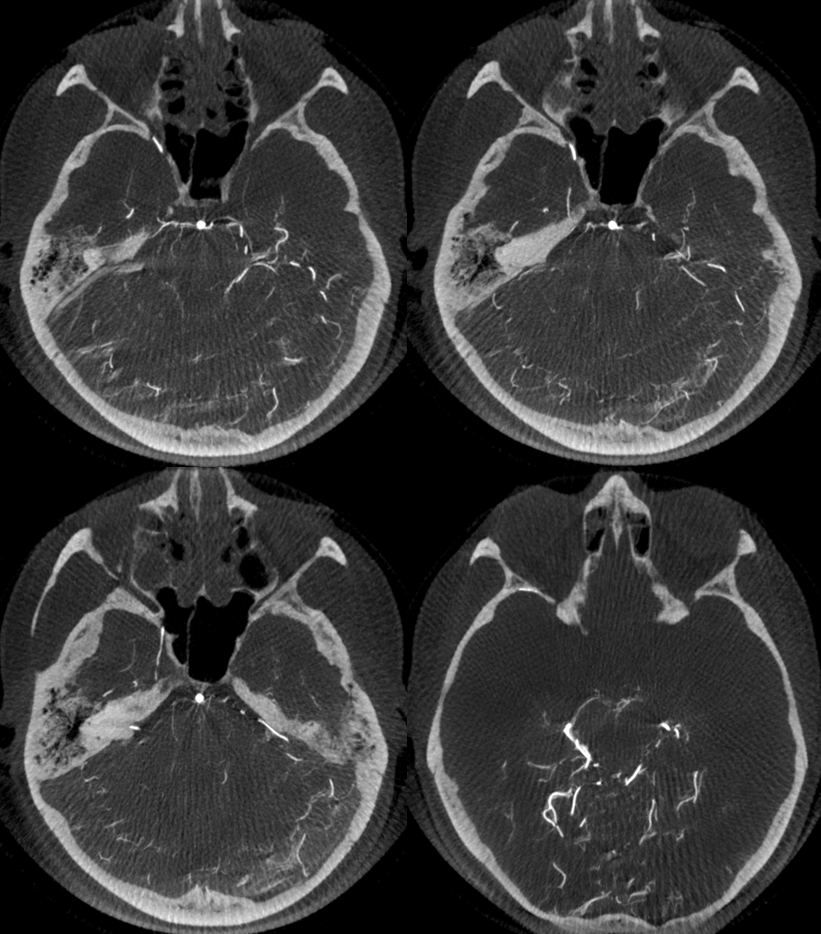
Here is a CT of the same case, showing the trigeminal as well as another variant, the accessory MCA (purple arrows), also discussed in greater detail on the Neurovascular Evolution page.
In the case below, the trigeminal artery itself is associated with a large aneurysm. Is it intradural or extradural?
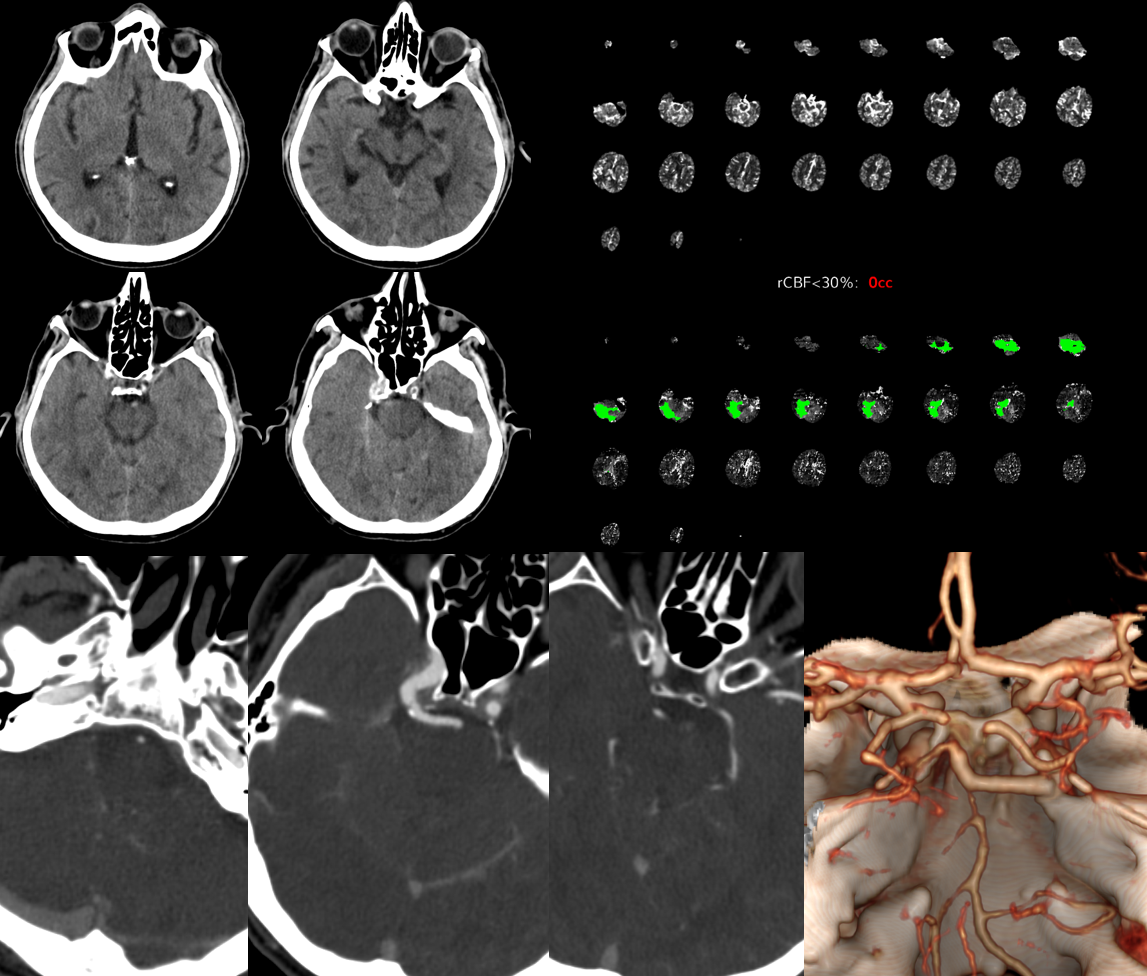
Trigeminal Stroke
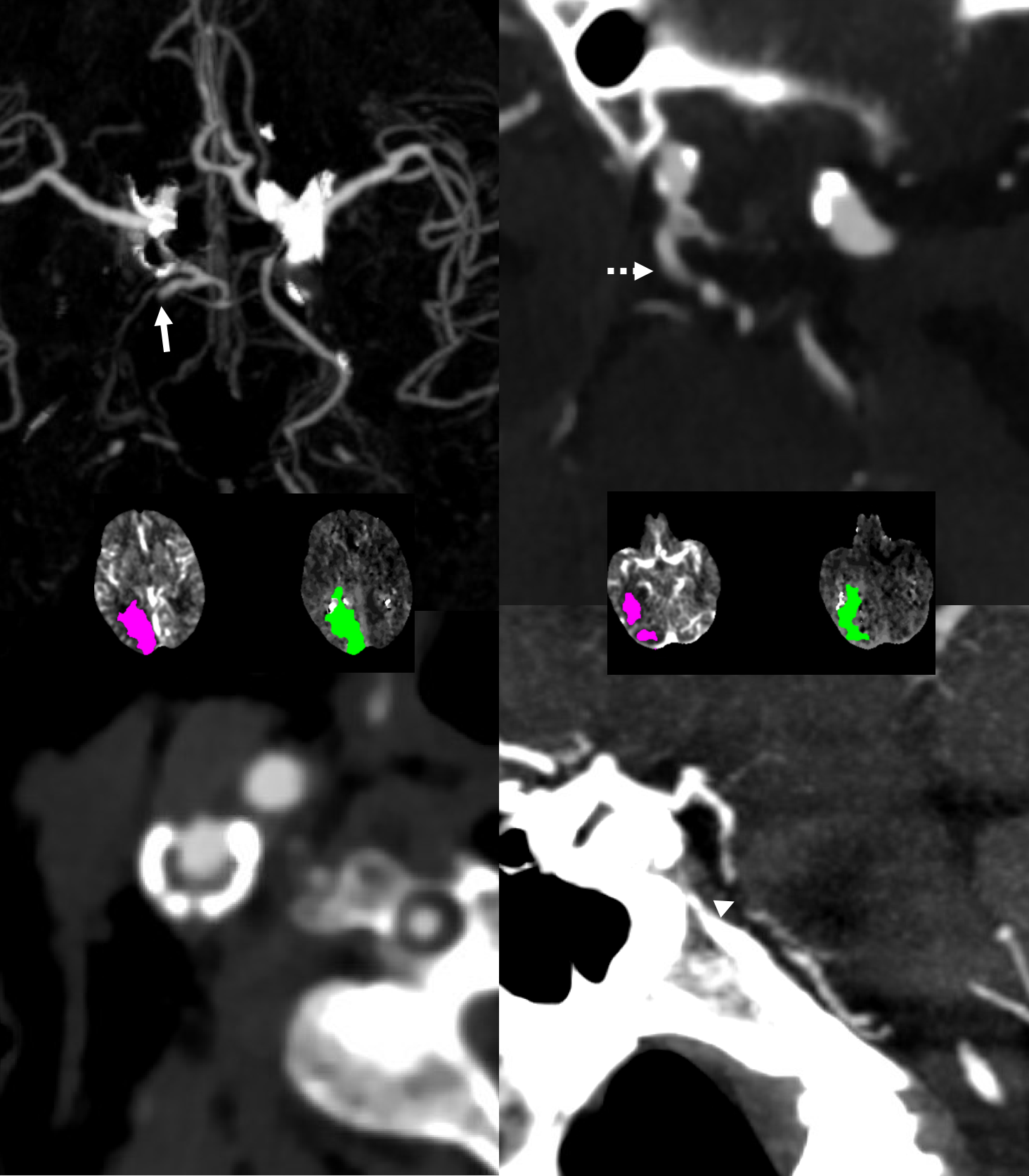
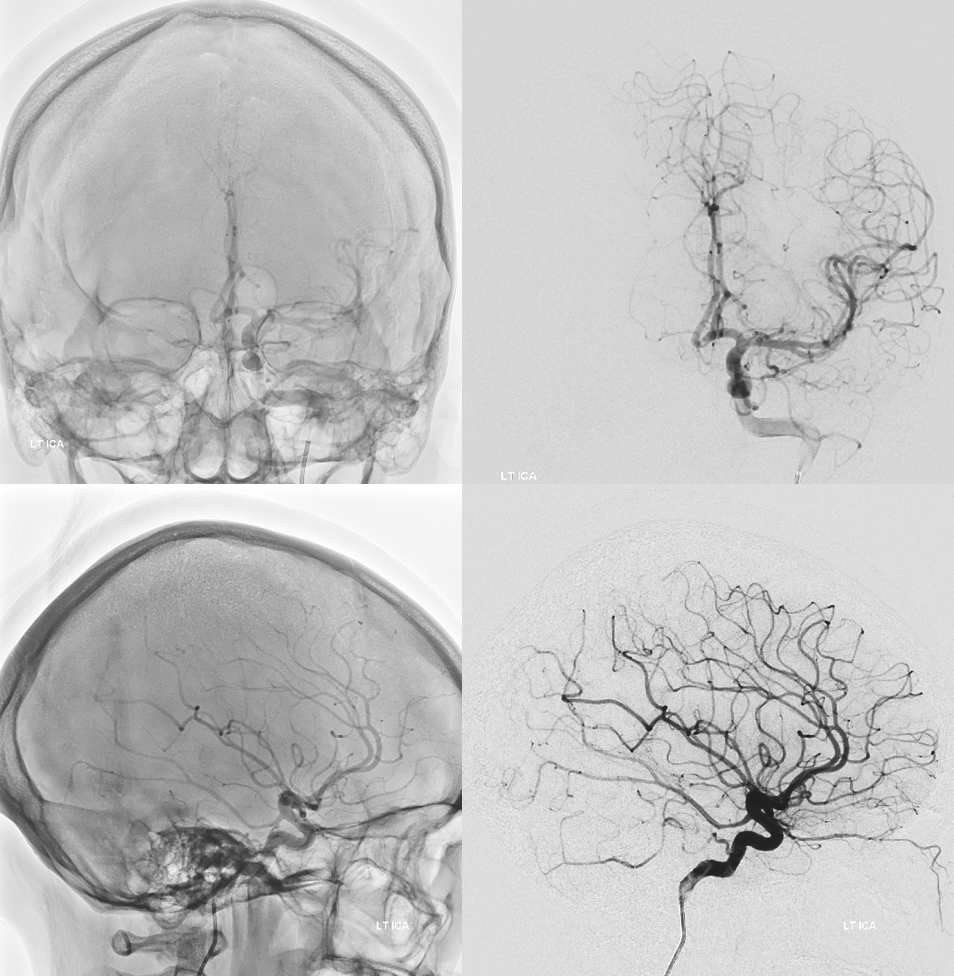
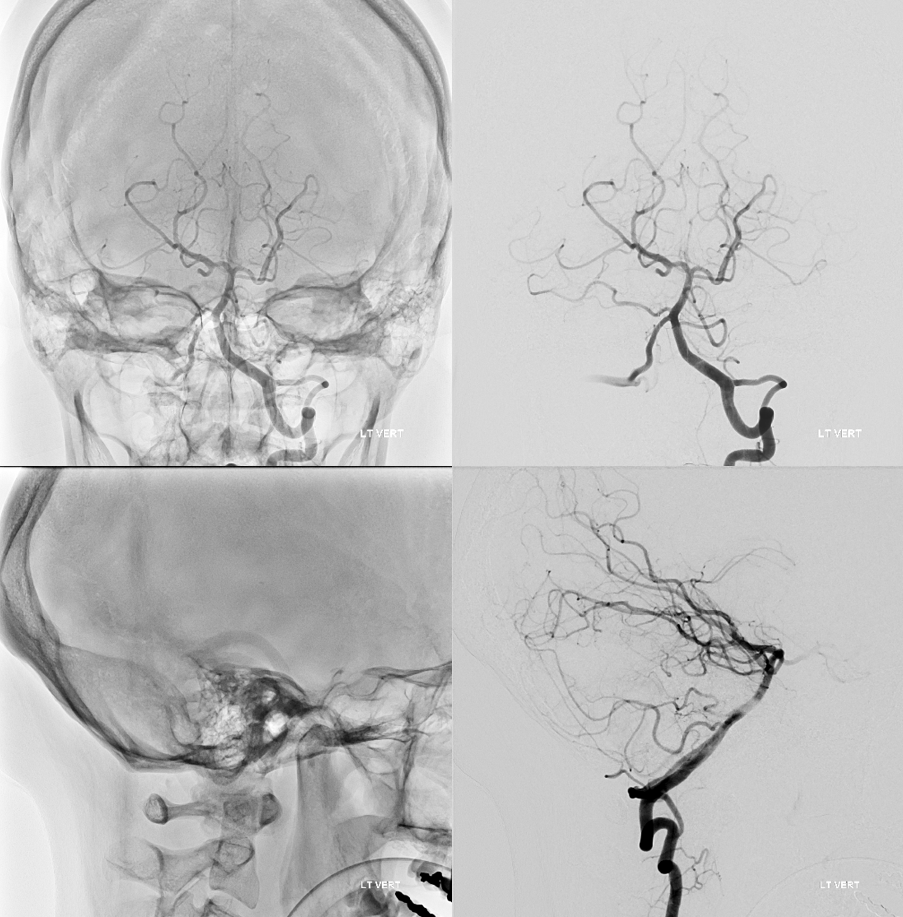
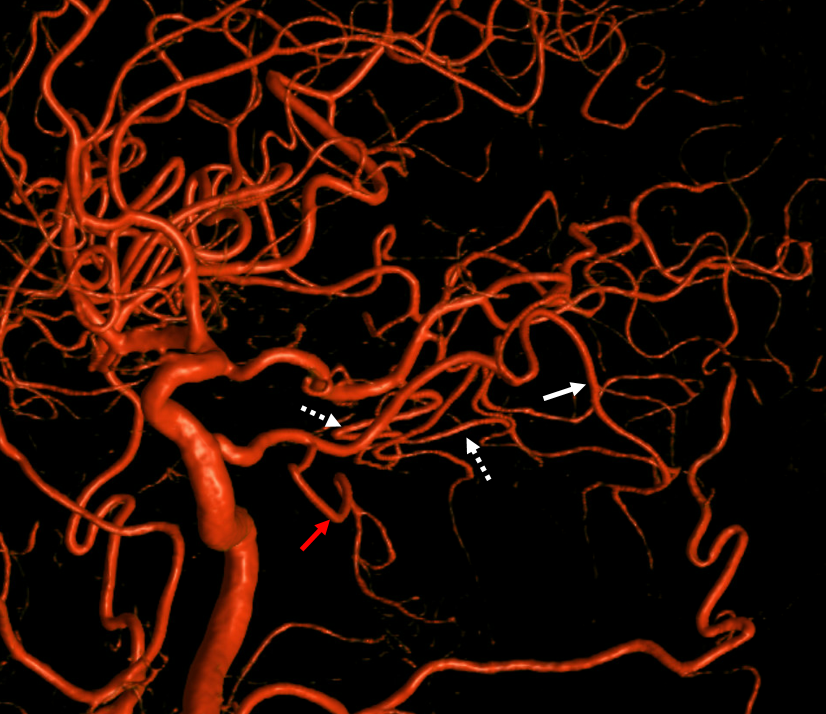
Below is a right PCA (P2) segment embolic occlusion. This is an artery to artery embolus from a diseased right cervical carotid (no arrows needed), via the trigeminal (dashed arrow), into the right P2 (arrow). The anatomy solves the riddle — left PCOM is fetal (no arrows needed), thus left P1 is hypoplastic and embolus of that size would not go there. it also could not have come from the verts because the basilar below trigeminal is hypoplastic as well (arrowhead) — in fact this was originally considered a basilar occlusion. However, clinical presentation was not consistent with that location and basilar hypoplasia below trigeminal is common. Excellent clinical correlation here.
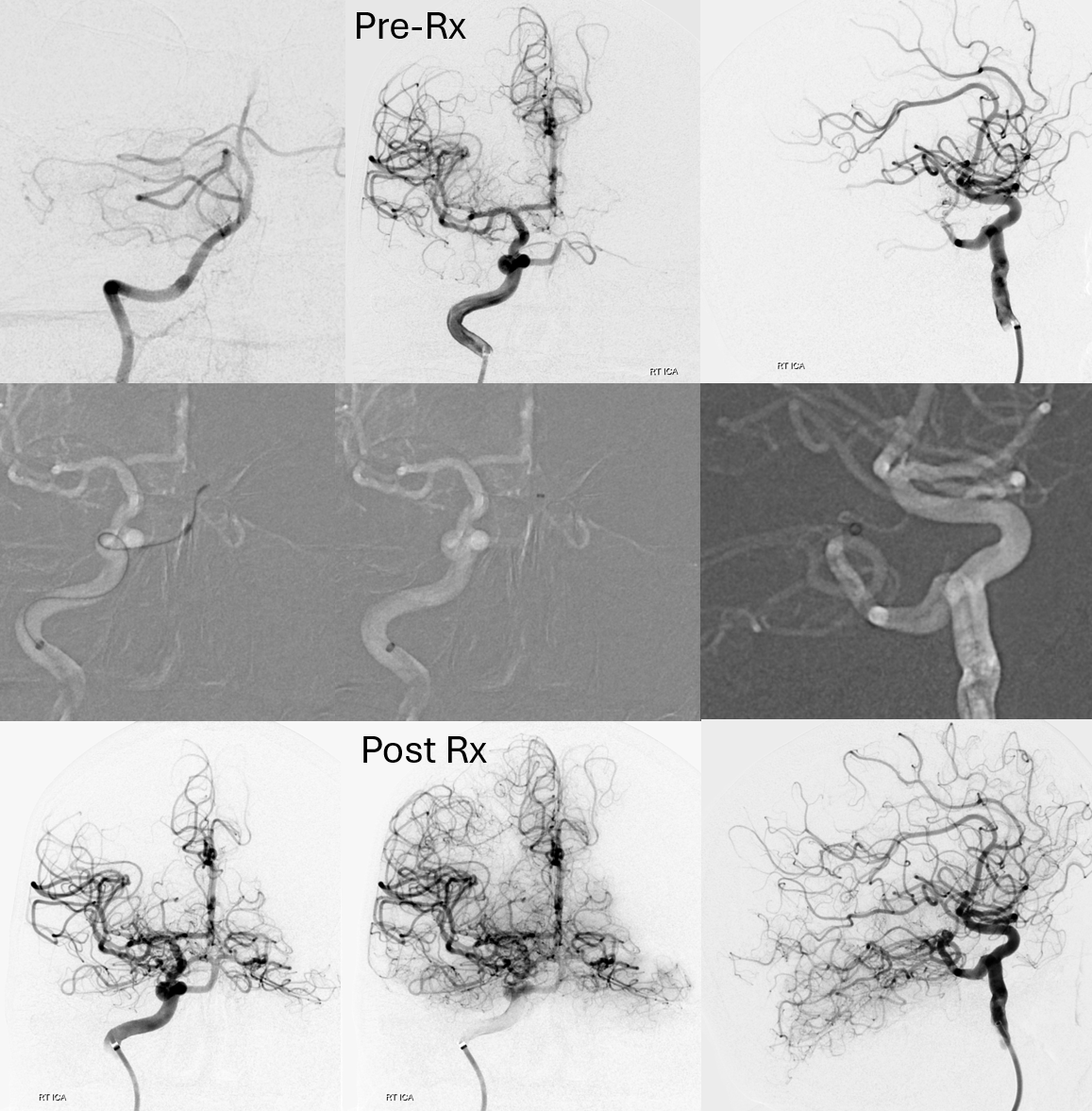
Trigeminal Artery Thrombectomy — Lest you think this is impossible — a fantastic case by Vera Sharashidze. Below are key images. Full case here as part of Case Archives.
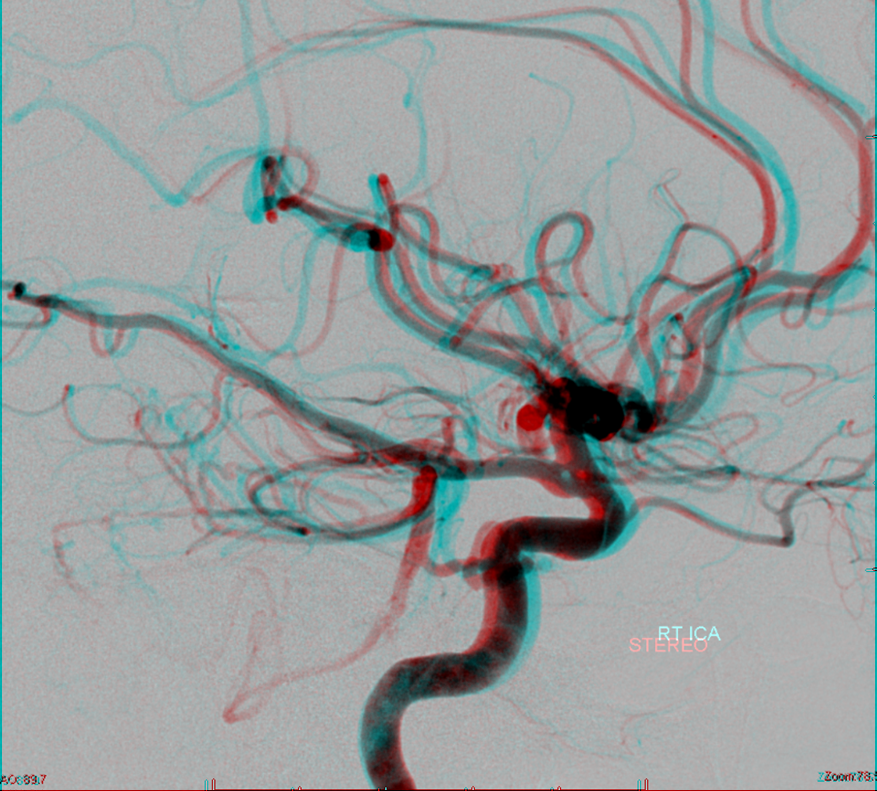
Trigeminal Artery and PCOM fenestration — not only does this person have a PCOM, but a fenestrated one — a finding that is exceedingly rare — I’ve only seen one. There is one report of it in the literature, however this report does not seem to have images. So, this one is the only fenestrated PCOM image in the world I know of — except for all the ones being hidden somewhere for no useful purpose. Therefore, if you have any, please SHARE — like they told you in childhood. Credits guaranteed. Stereoscopic image below courtesy of Dr. Nelson and Dr. Becske

Anaglyph
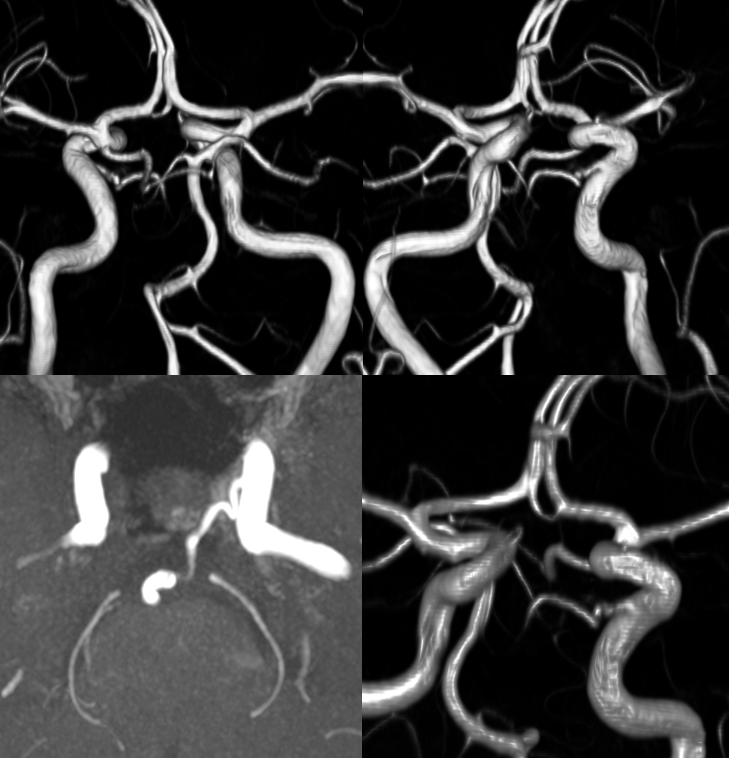
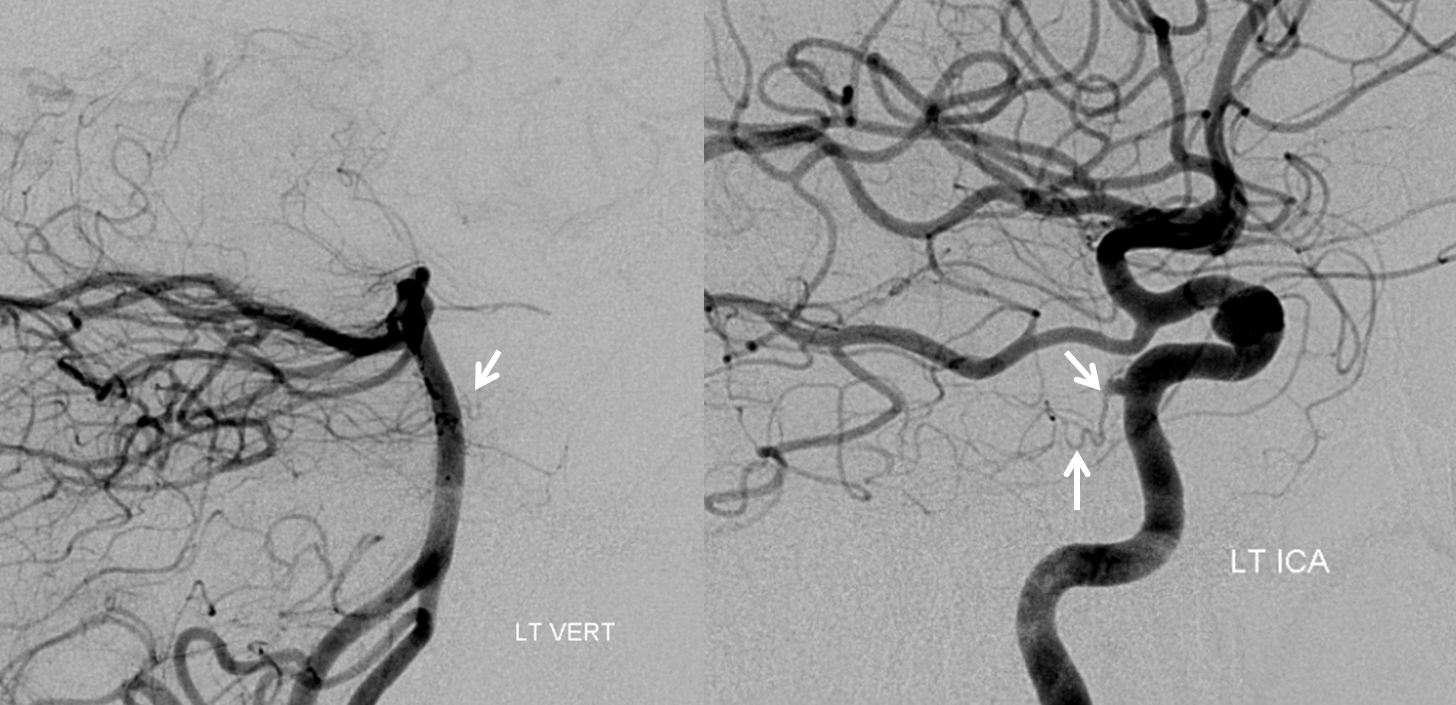
Spectrum — those “classic” cases of huge trigeminals and small PCOMs and small verts are just part of the spectrum. Just like PCOMs range from tiny to fetal, so do trigeminals. As mentioned above, everyone has a tiny trigeminal on the surface of the trigeminal nerve. Here is an infundibulum of small trigeminal artery seen from both ICA and vert
Trigeminal supply to the AICA
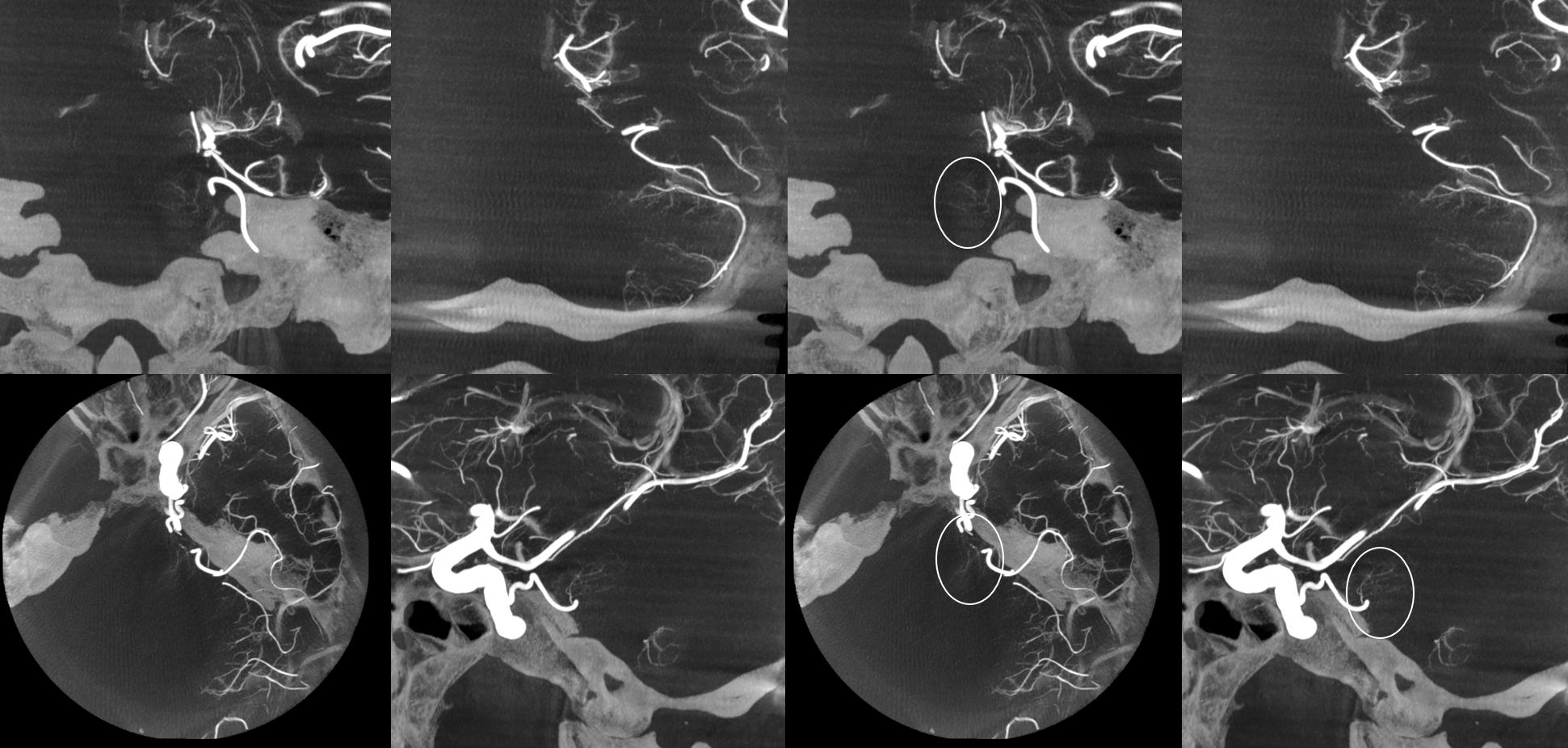
Hey, here is another myth buster. Trigeminal always connects carotid to basilar. Yes of course!! Except the half time that it does not — yes, indeed. Trigeminal artery VERY frequently supplies the AICA territory, and is not at least macroscopically connected to the basilar artery. Its is a spectrum of course like everything else — sometimes its more than AICA etc. See below. But, what we have never seen yet, is trigeminal supply of the labyrinthine artery — which we believe is the very definition of what AICA is. All of this needs Cone Beam CT to see well.
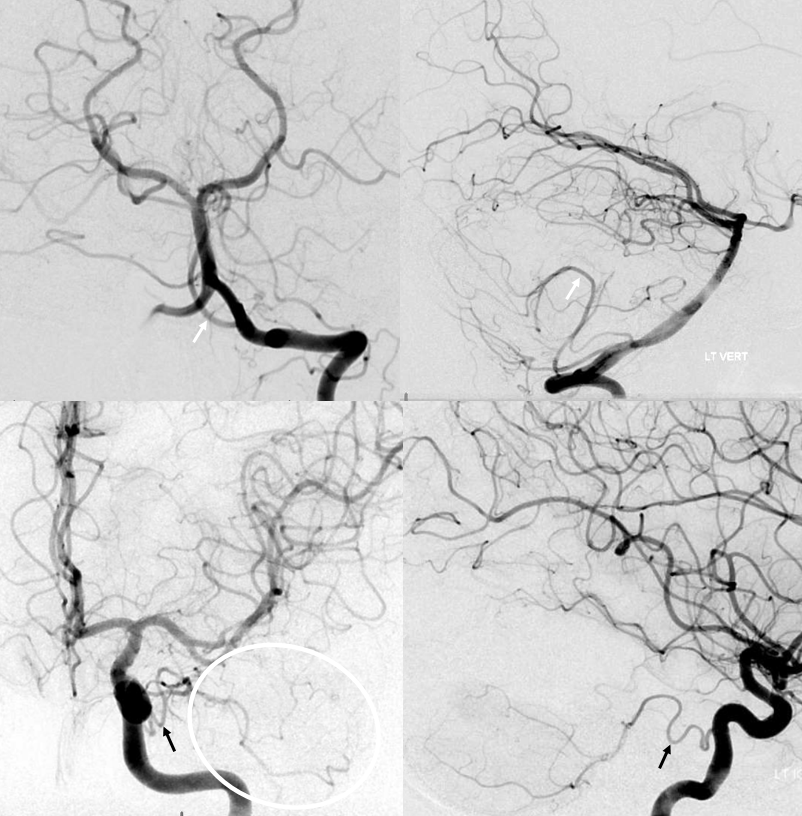
Here are 2D-DSAs
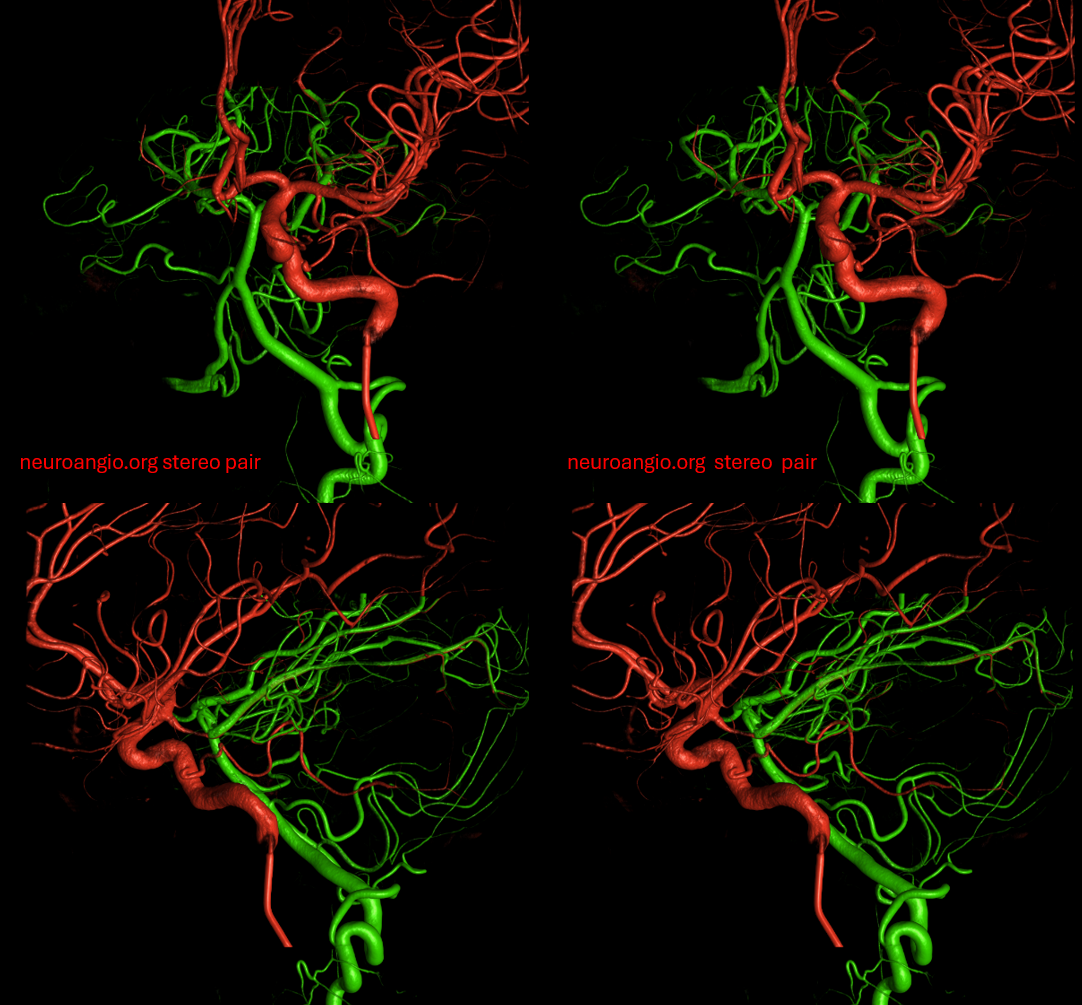
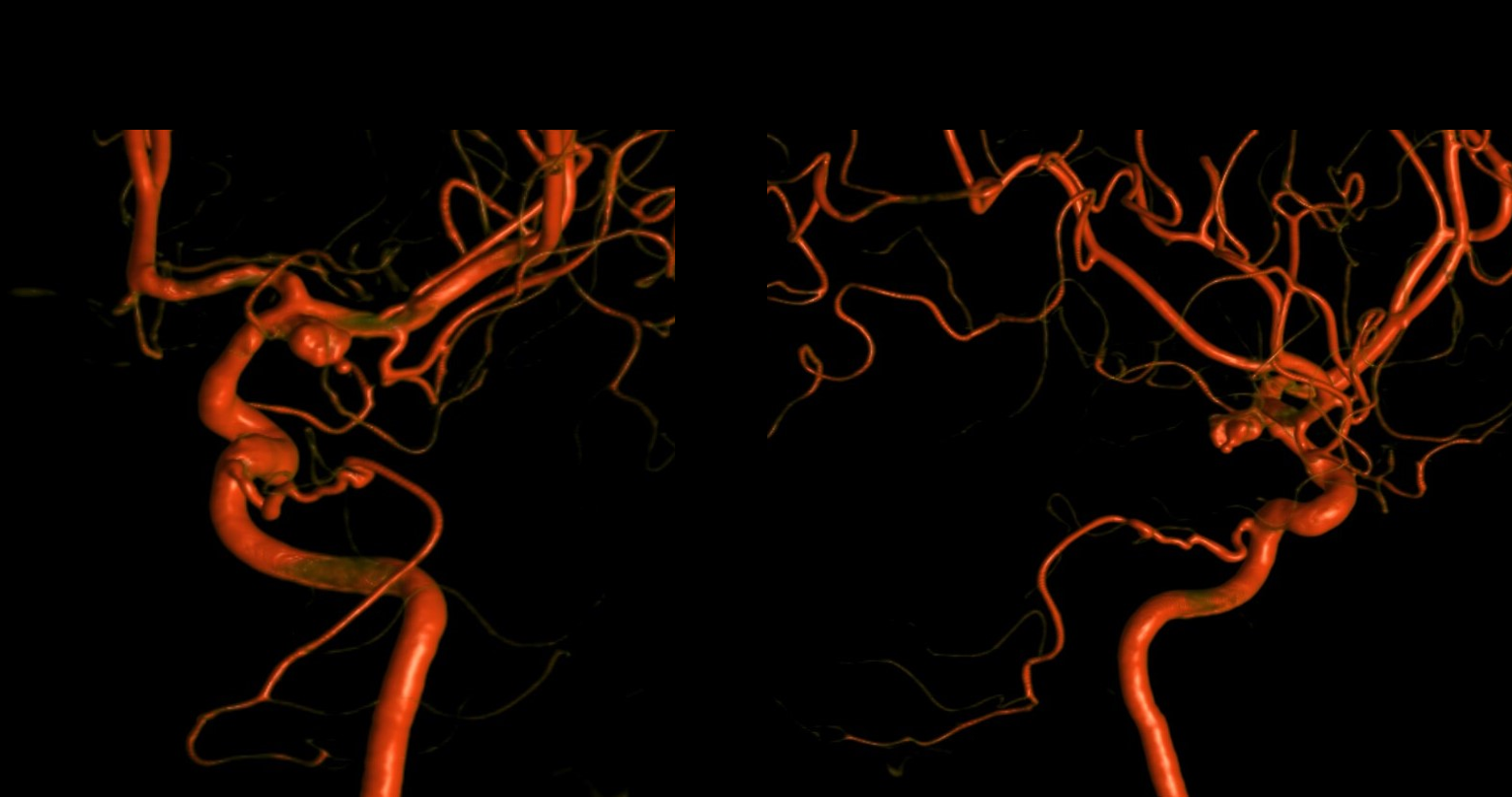
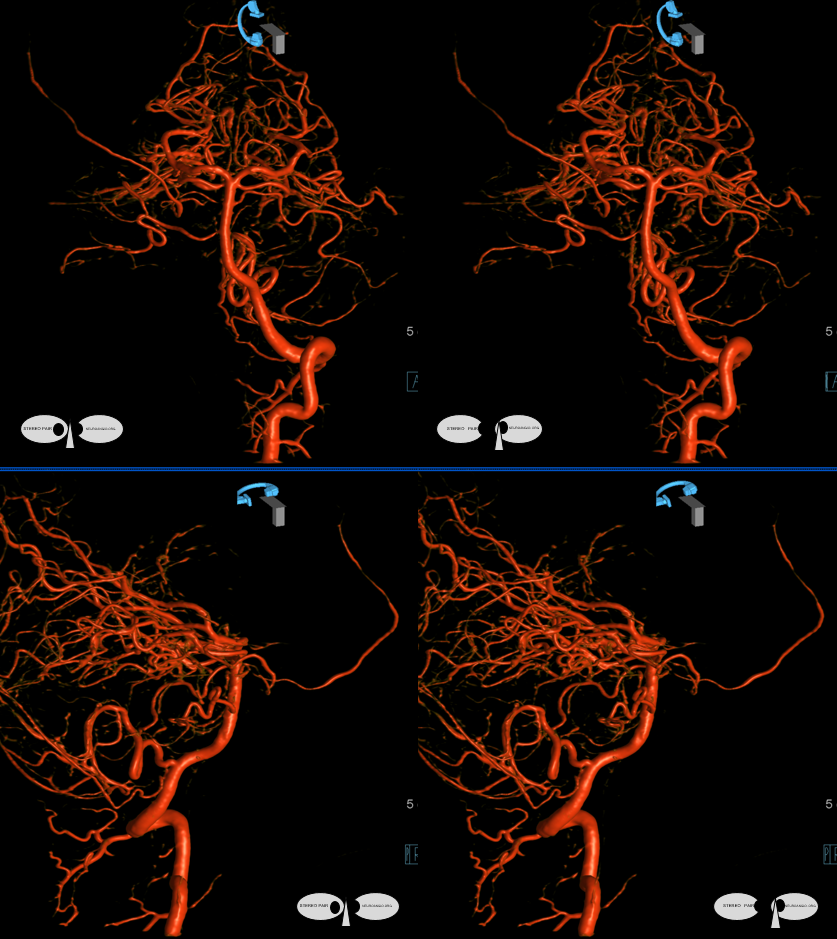
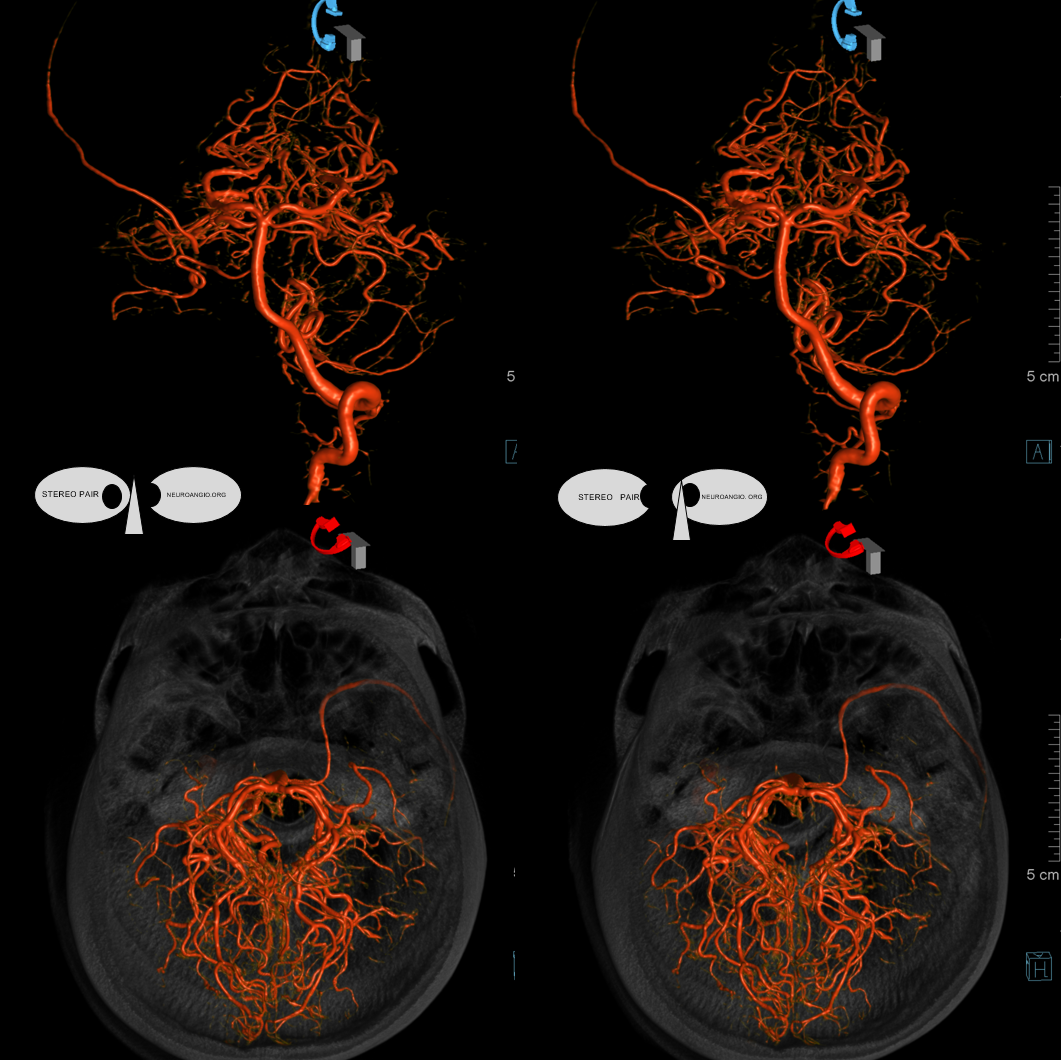
Stereo volume rendered images of Cone Beam CT fusions of the ICA and Vert — see how that works — cute but not very informative of the details
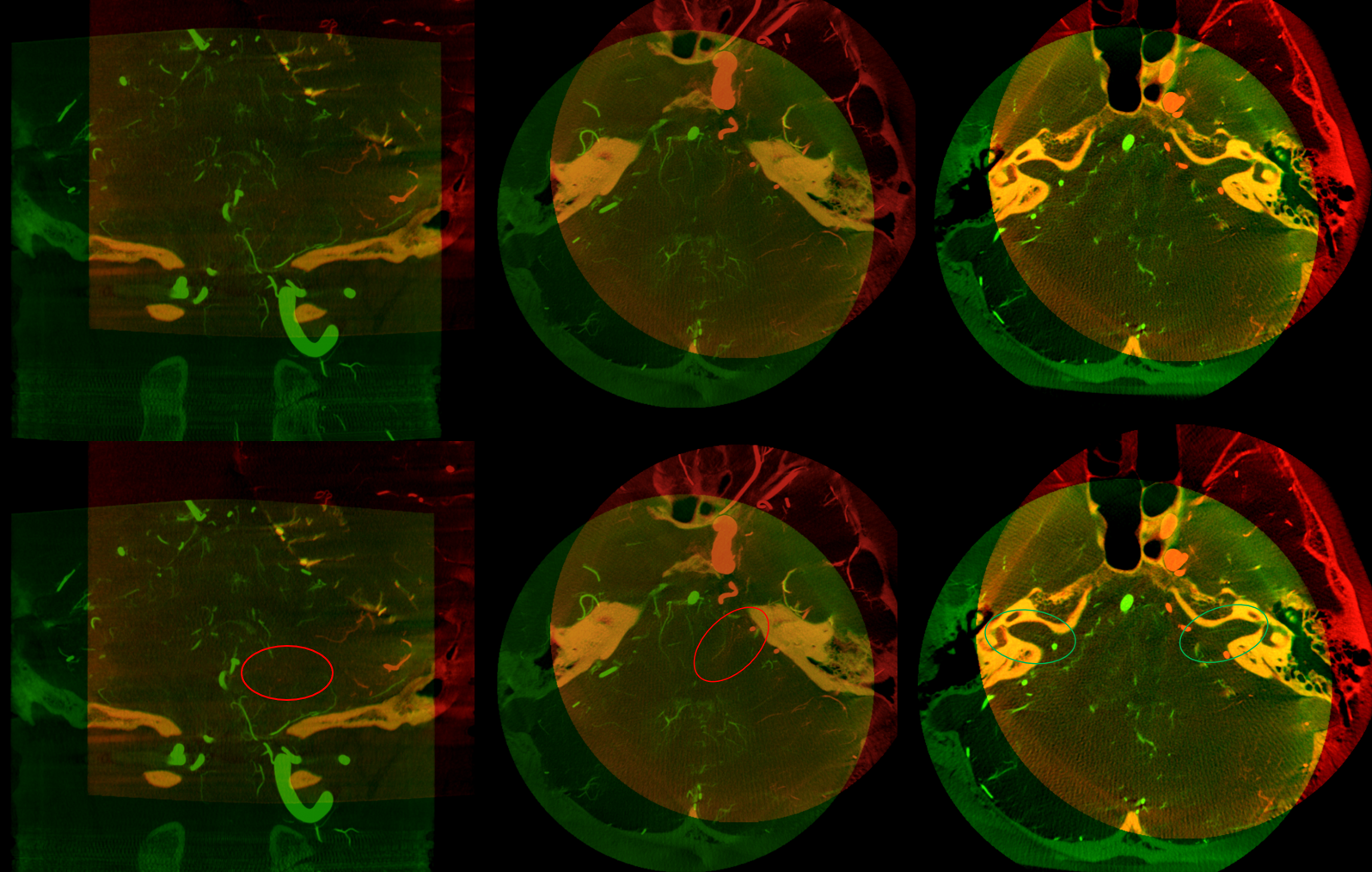
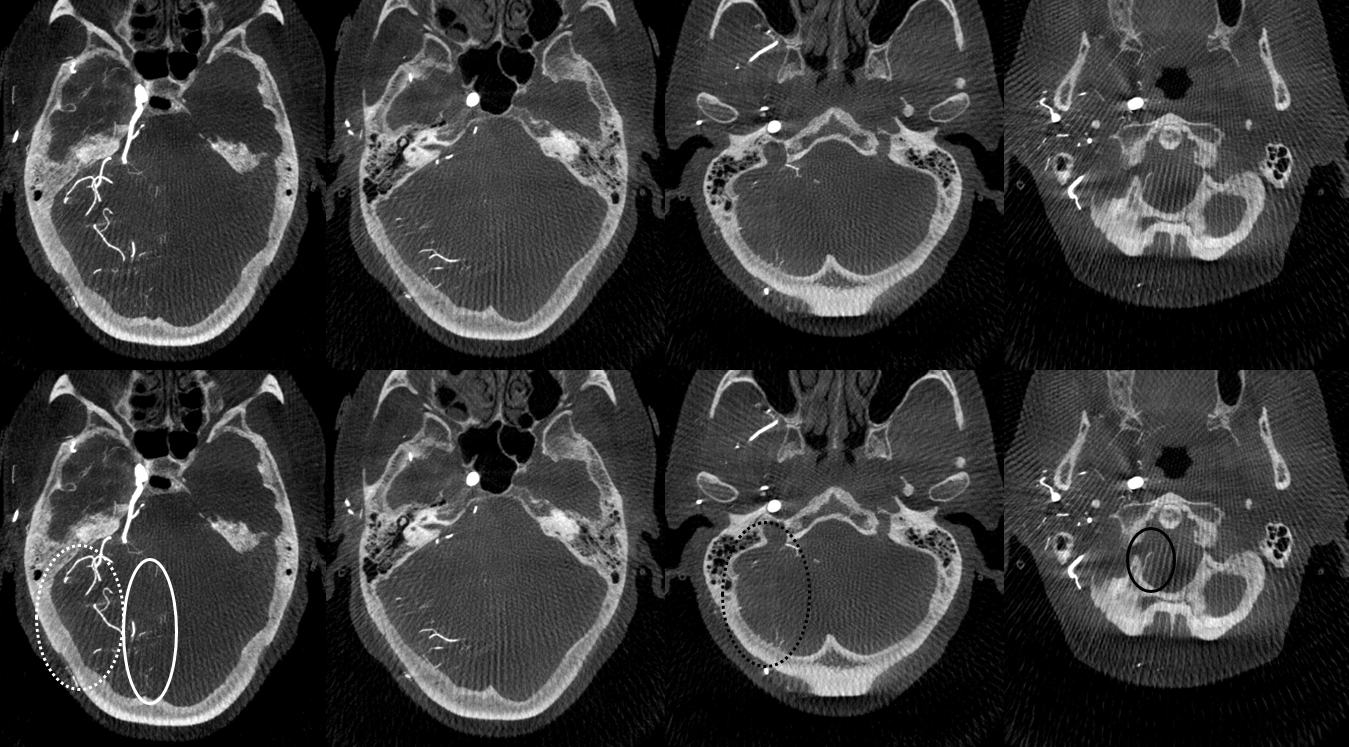
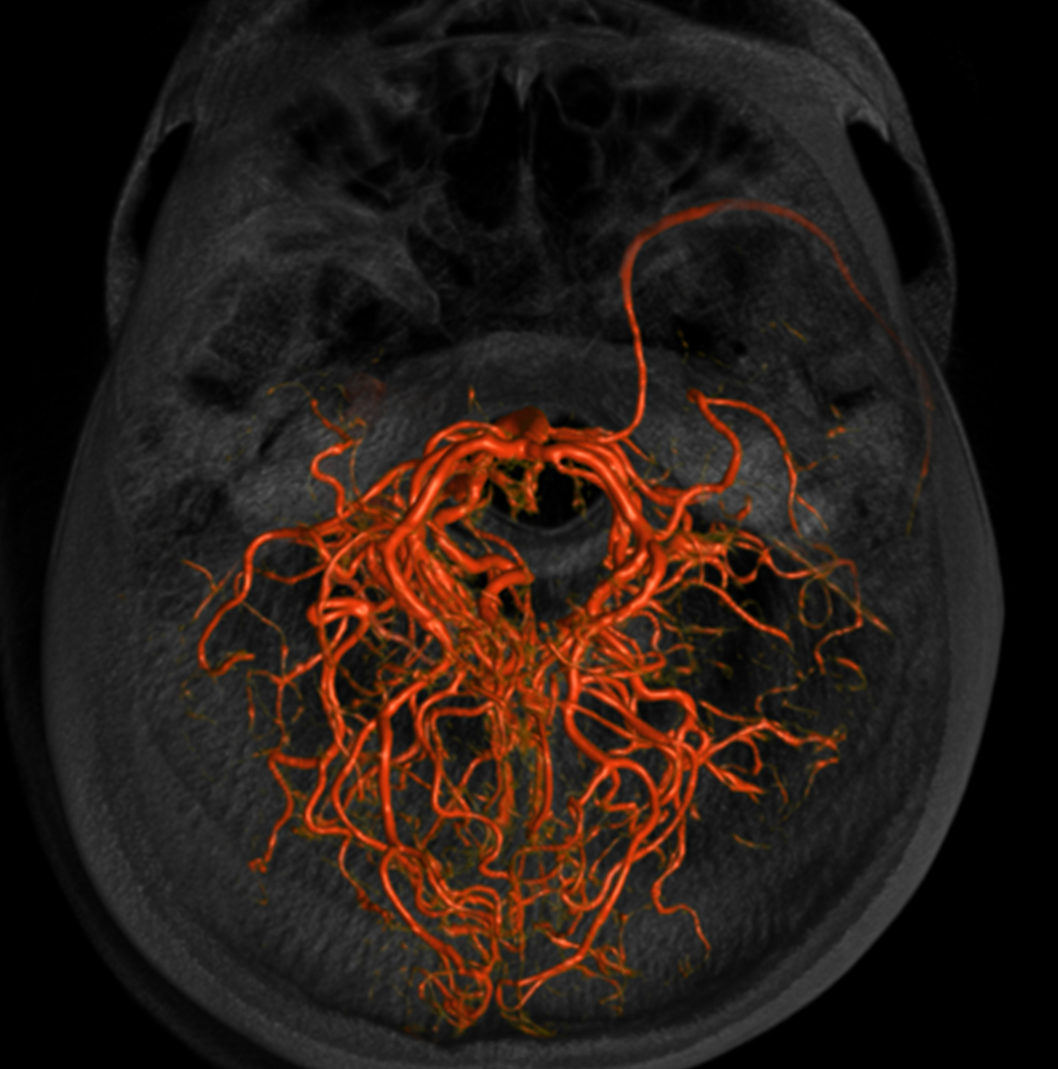
Below are the fusion MIPs — thats where the money is. Note all what’s been said — in color. Mostly supply is of lateral AICA territory. However, very importantly, there is also supply of the lateral brainstem (red ovals), but NOT of the labyrinthine (green ovals, bilaterally seen by the way). The suspicion is that lateral brainstem supply by the trigeminal artery corresponds to its natural supply of the trigeminal nerve
Seen in black and white
How about some movies of the same — very cool
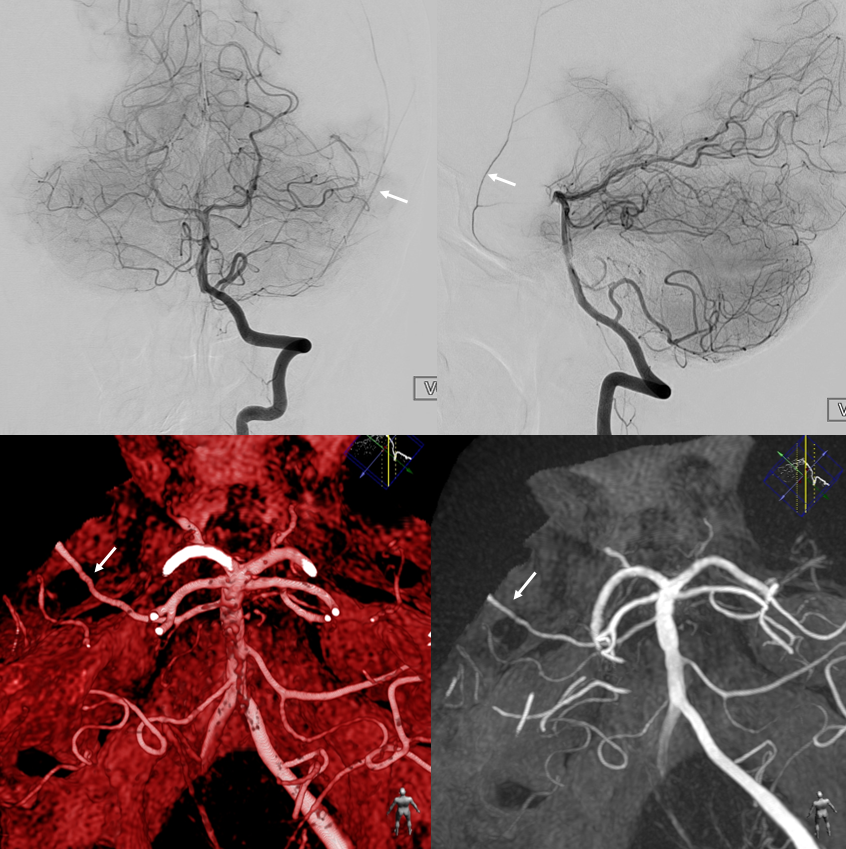
In this variant, the trigeminal artery (white arrow), supplies the lateral cerebellar territory classically belonging to the AICA In the Saltzman classification, this corresponds to Type IIIB 
Anaglyph

AP view of carotid injections showing the AICA (black arrow), with corresponding wedge-shaped void of its territory seen on the right vert injection. Notice fetal disposition of both PCOMs.

This variant can also be appreciated by an astute neuroradiologist on a CT angiogram

Another example of a trigeminal artery (red) supplying “classic” AICA (yellow) territory

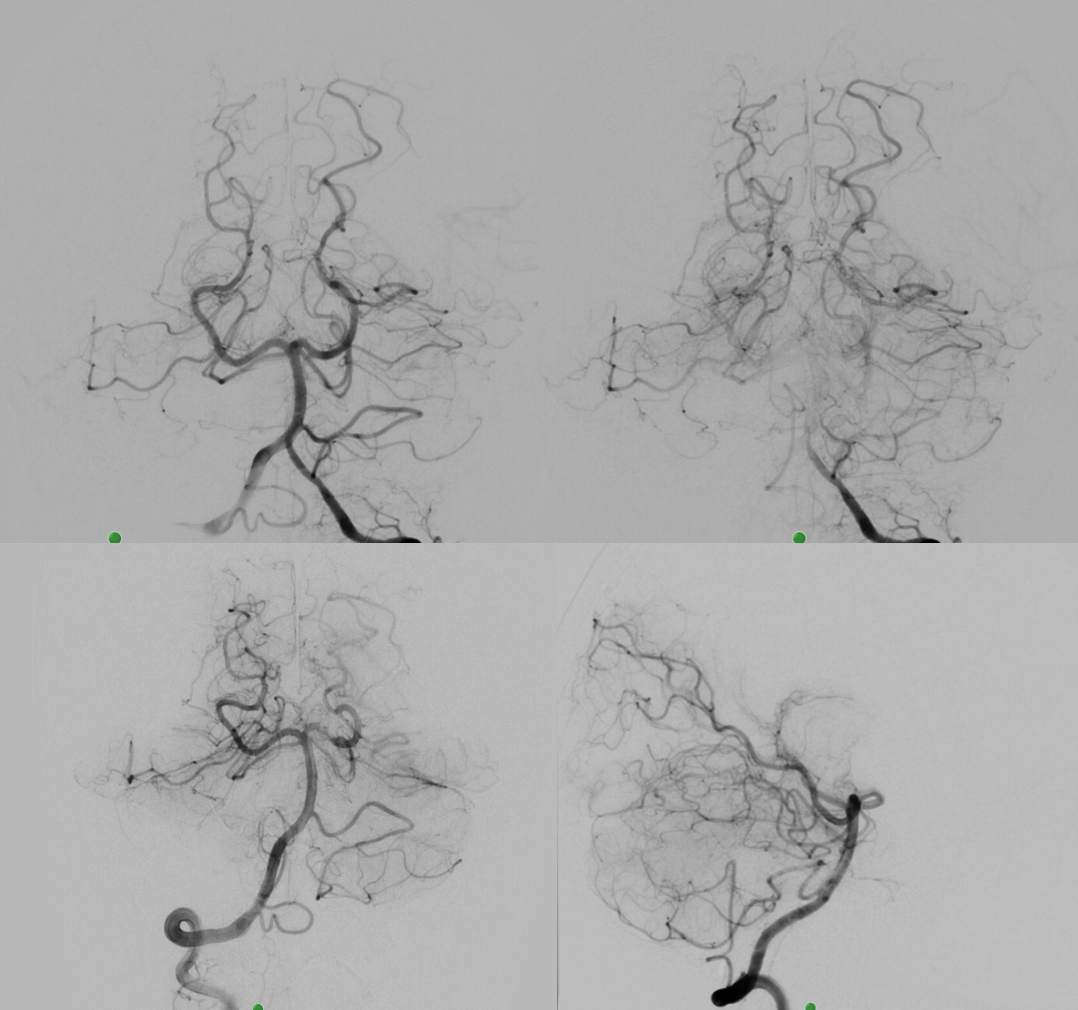
Want more? How about this — see below — the left AICA is hypoplastic. Left PICA (white arrows) supply is limited to vermis. The left SCA is small. How come? There are two possibilities — either the tissue is missing (infarcted, resected, etc), or there is yet another source of supply. The answer is Trigeminal Artery — (black arrows). It again often supplies “AICA territory”. However, insofar as there is really no such thing as “AICA territory” — it being in balance as we keep saying with SCA and PICA — the extent of trigeminal cerebellar supply is as variable as anything else. Here, it is responsible for a big chunk of it (white oval in frontal view), self-evident in lower right lateral view — taking care of both lateral and inferior right hemisphere.
Another PICA territory supply — also interestingly not involving the vermis, courtesy Dr. Tibor Becske

Trigeminal Supply of Superior Cerebellar, AICA, and lateral / hemispheric PICA
Neat. And extremely rare — i am not sure there is another example out there. I am very sure however that there are many people like that walking around, with no problems at all.
I guess that would be Saltzman IIIA+IIIB+IIIC/2. This is either very advanced algebra or a reflection on classifications in general — you decide. The important thing is to put everything together and understand what goes where
Angio shows large trigeminal with clear supply of the SCA on lateral view. Vert injection shows no right SCA. There is a diminutive branch from mid-basilar projecting laterally — that is likely the right labyrinthine artery — what is embryologically solid AICA territory. The rest is taken by the trigeminal. The right PICA is limited to vermian territory. The inferolateral hemisphere is supplied by the trigeminal as well. Dont look for arrows. You should figure it out.

DYNA VR. White arrow — vermian branch SCA; dashed white arrows — lateral hemispheric branches of SCA; red arrow — AICA. Note inferior extension towards PICA territory.
Stereos

Movie VR
MIP images. Superior vermian territory = white oval; lateral SCA territory = dashed white oval; AICA (minus the labyrinthine branch) = dashed black oval; inferior PICA/down to tonsillar branch = black oval
Movie MIP
Another example of SCA supply in the literature — link here
TRIGEMINAL NERVE AVM — Case of Eytan Raz MD PhD
What is better to show all possible supply to the trigeminal nerve (after all, we all have this nerve as far as i know, and therefore the trigeminal artery also). In this case, the AVM magnifies supply to the trigeminal nerve and we see it all
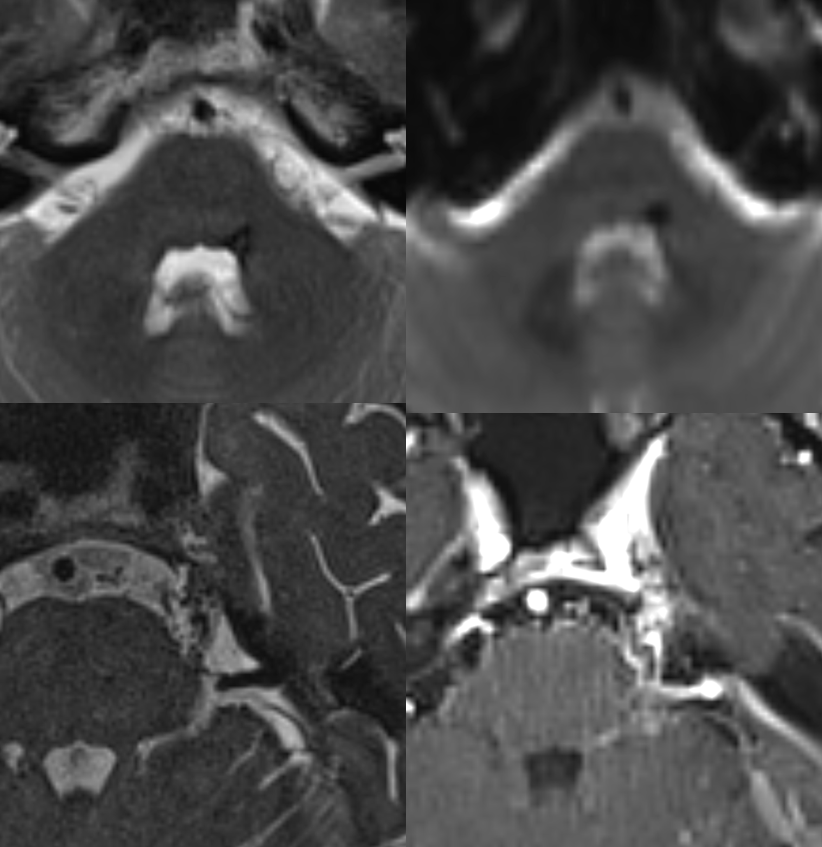
MRI
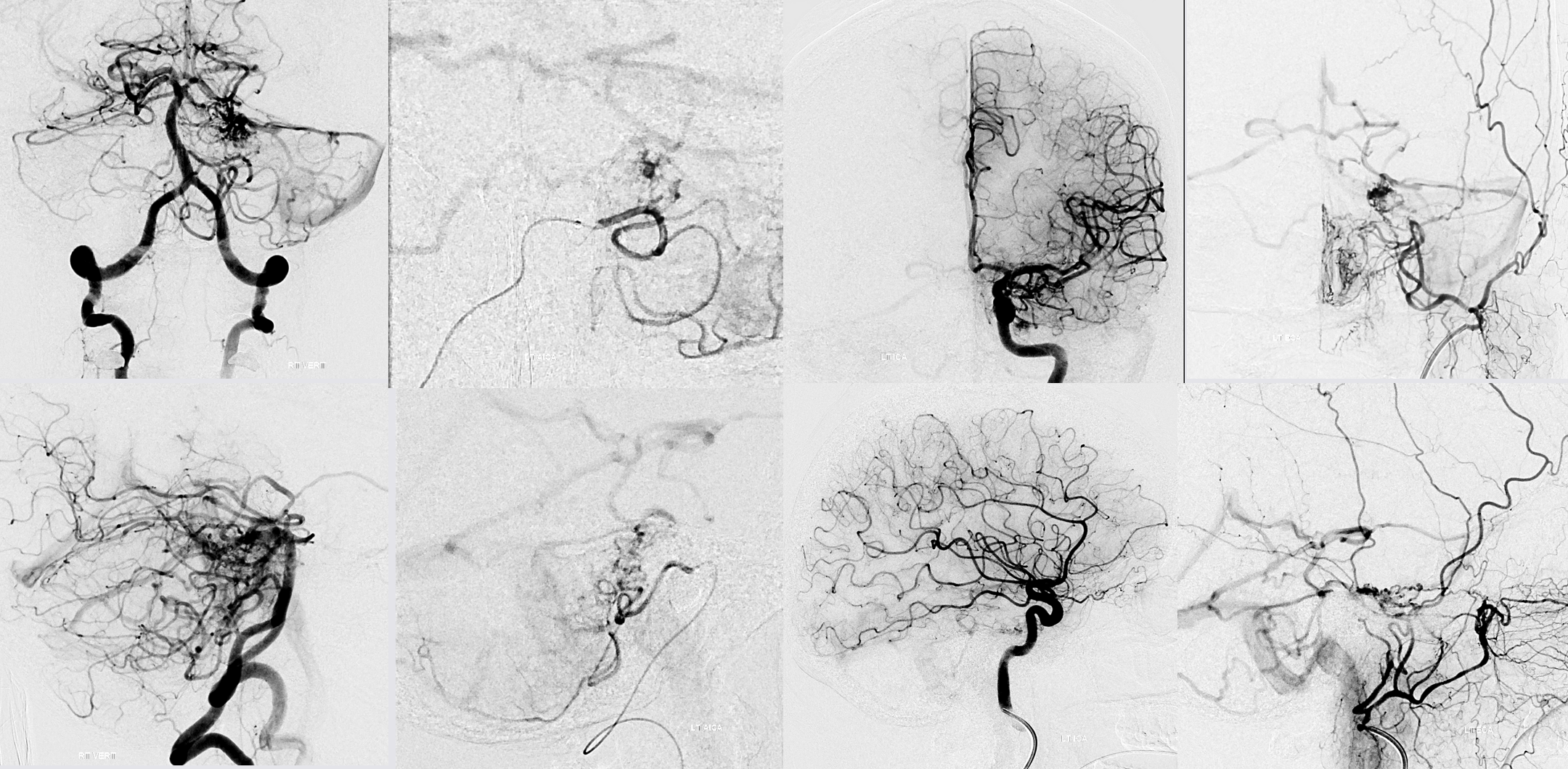
2D-DSA
MIP CBCT Vert and CCA
MIP Fusion
VR Fusion
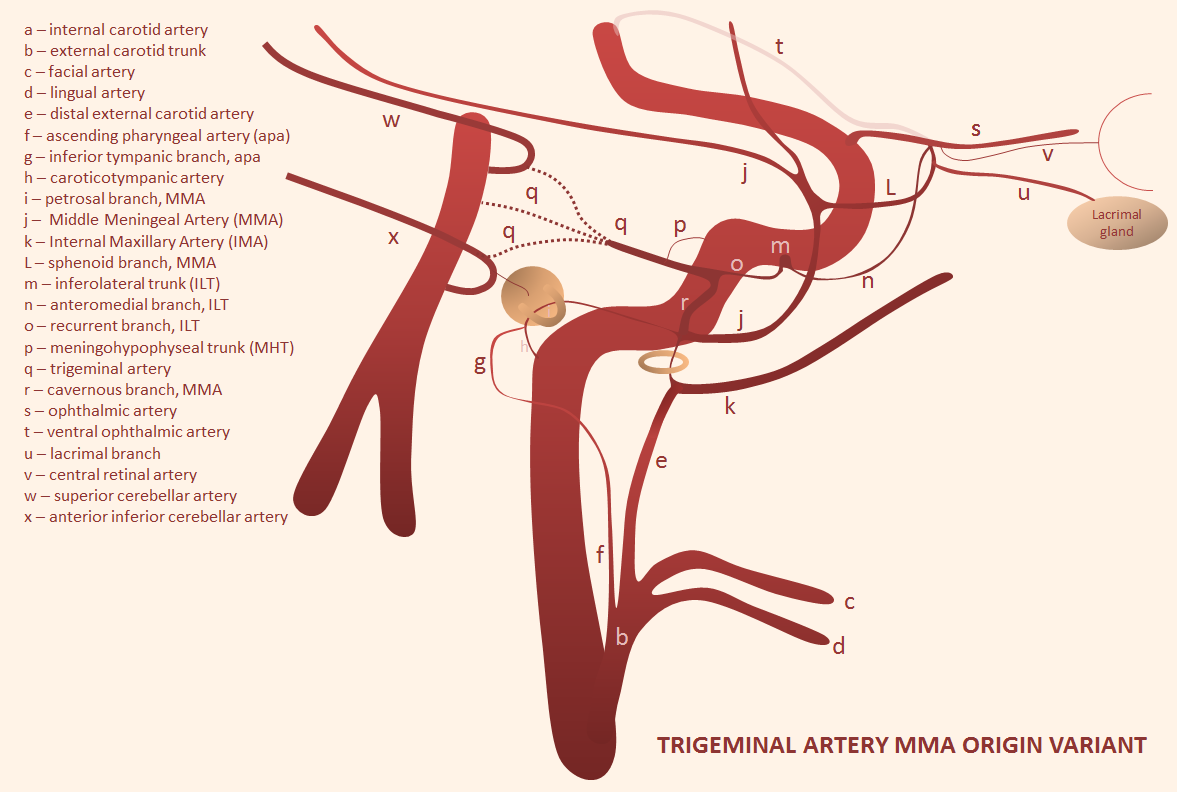
Trigeminal artery origin of the Middle Meningeal Artery — it all makes embryologic sense — check out MMA page
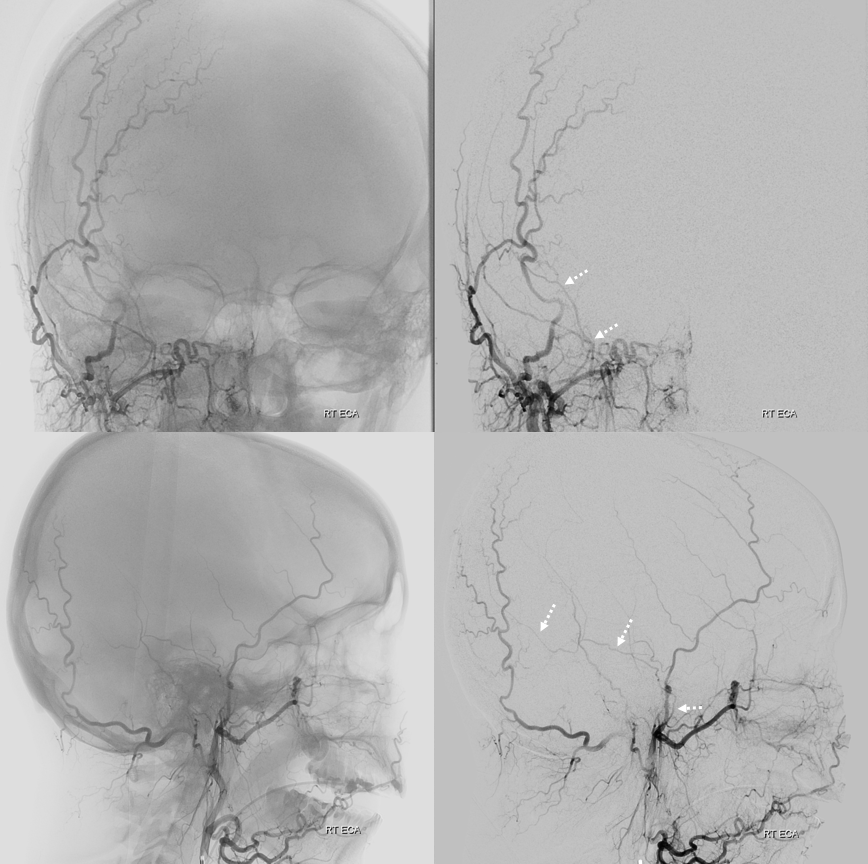
ECA with missing frontal division of MMA — petrosquamosal branch is shown by dashed arrows
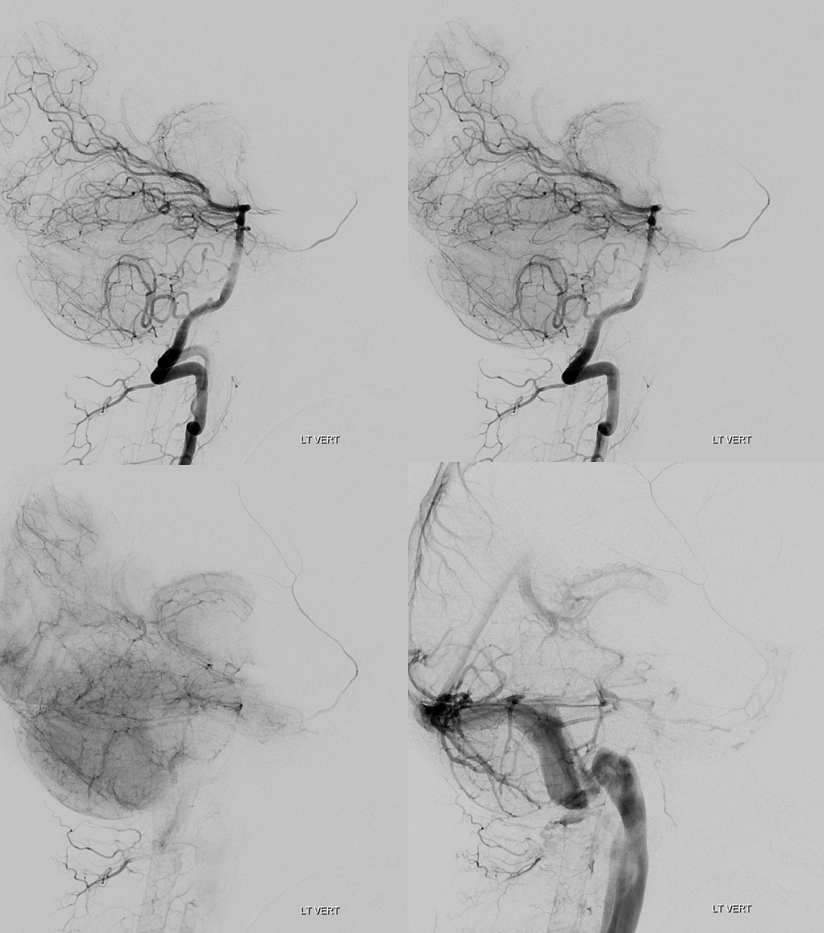
Vert

Rotational angio and 3D MIPs
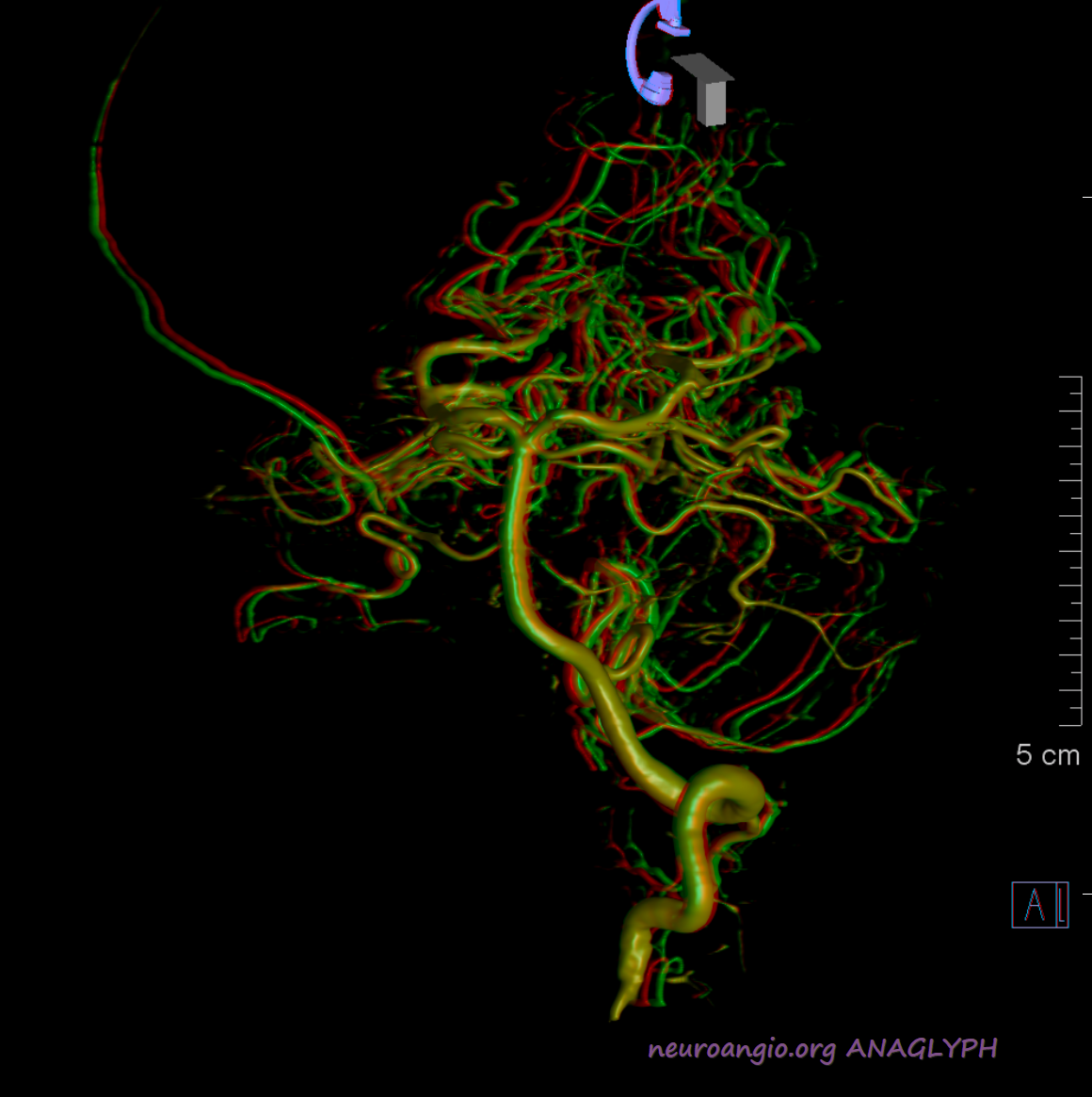
Stereo Volume Rendered images
Anaglyph stereos
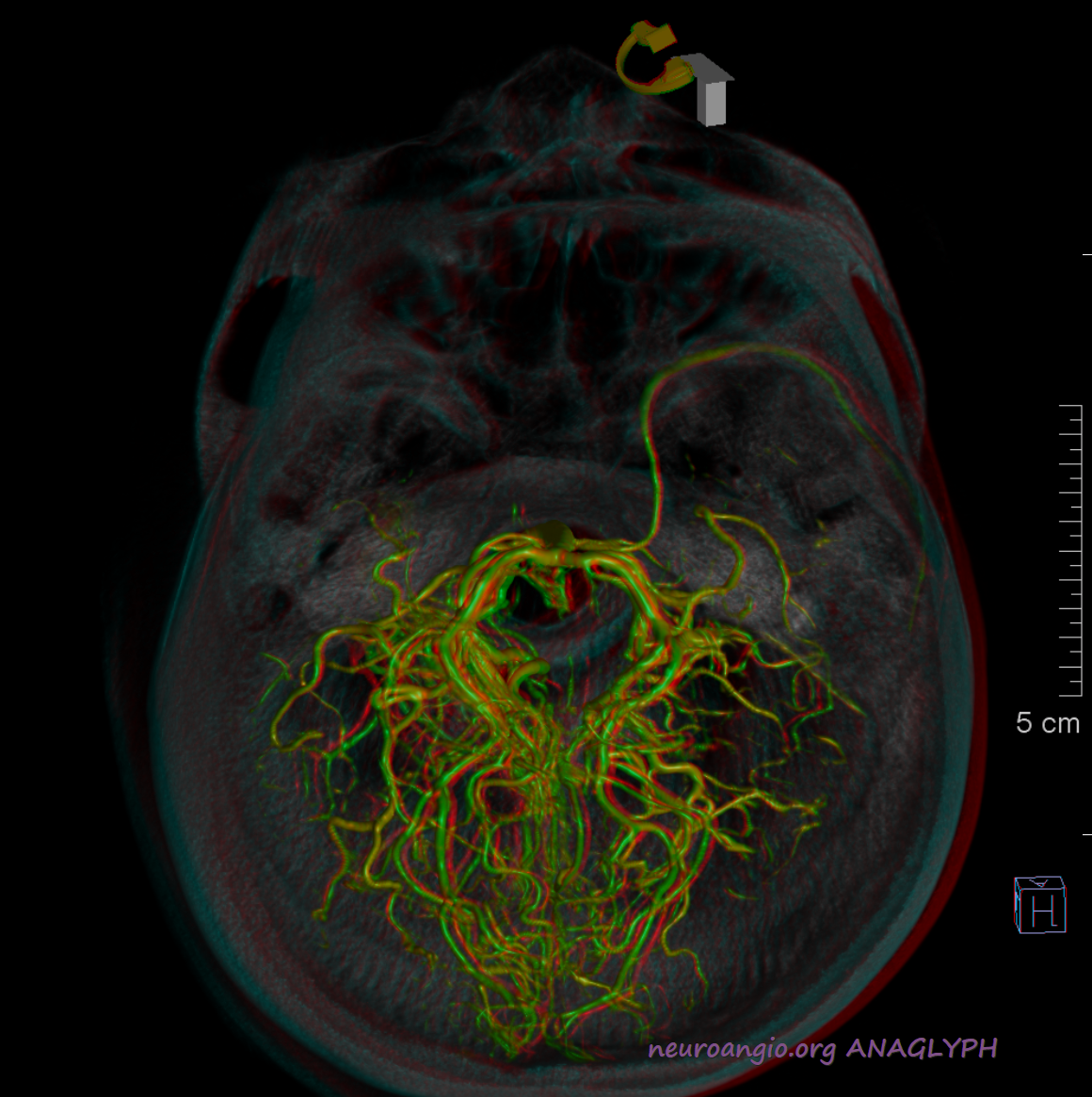
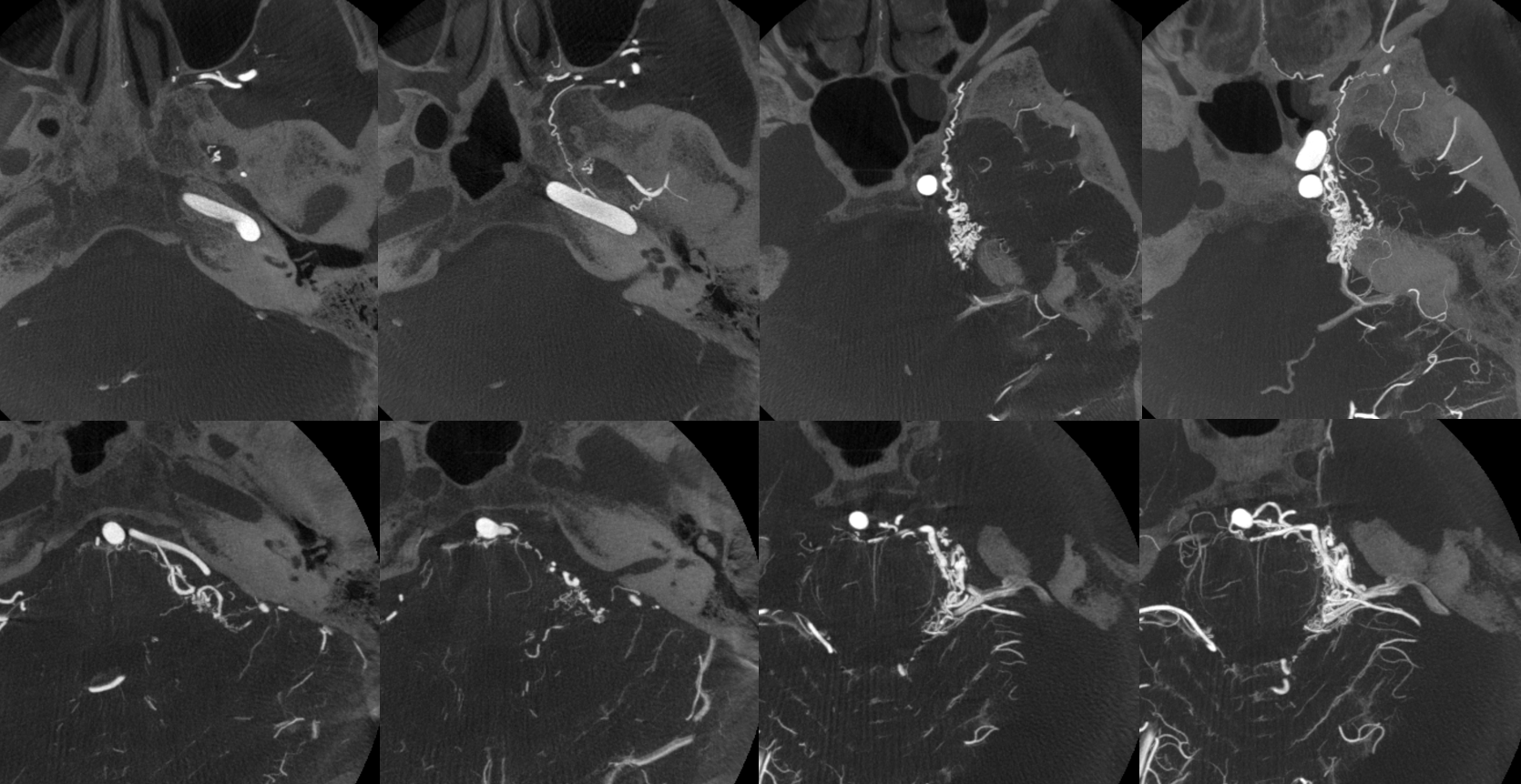
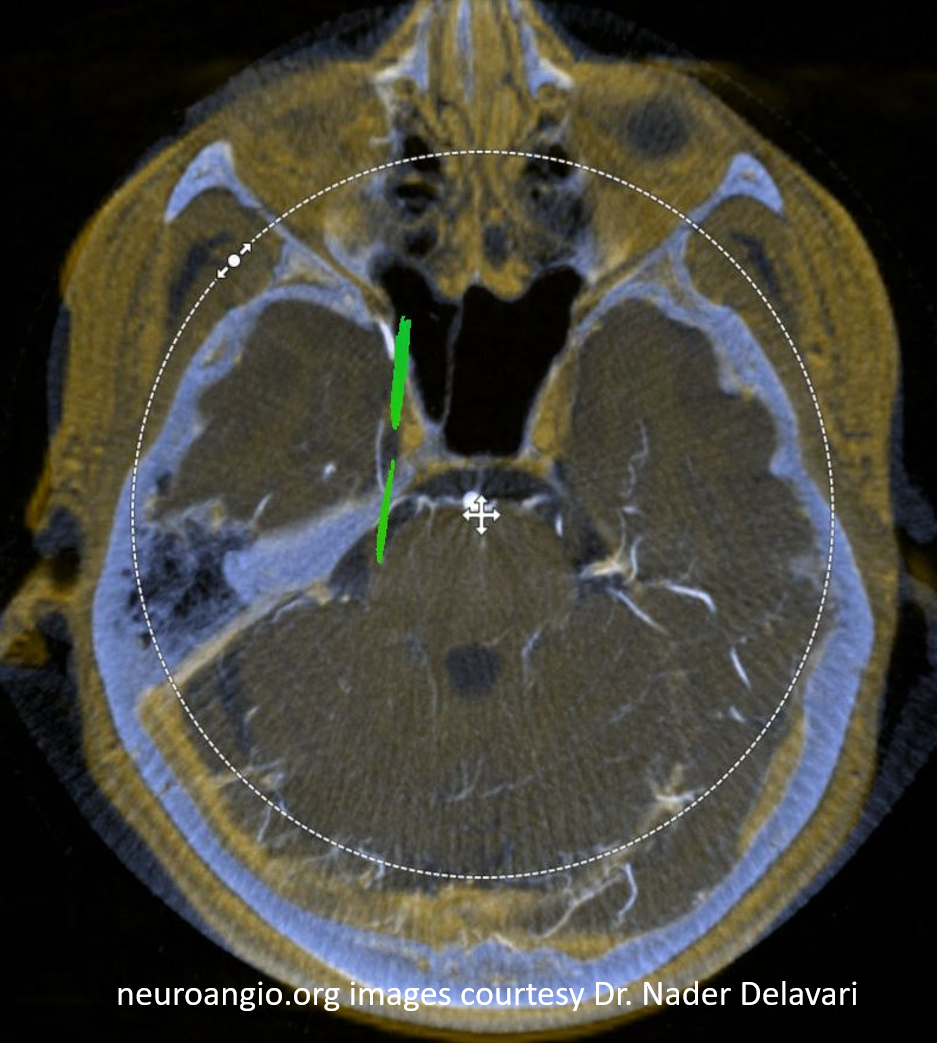
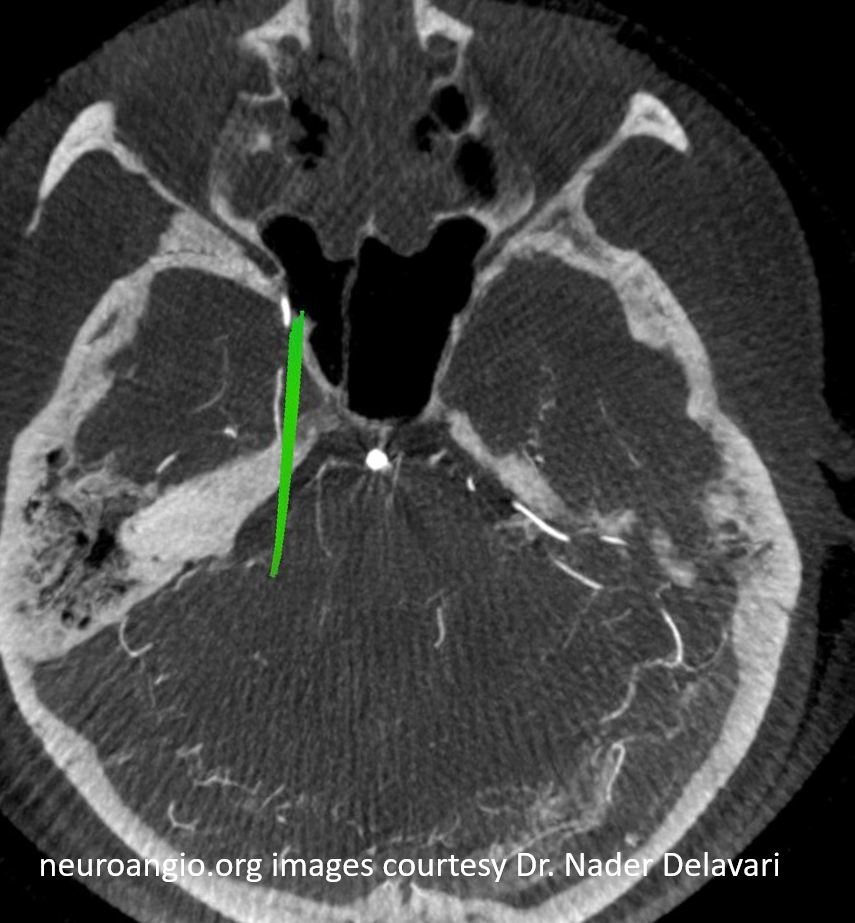
And, in case you really dont believe its the trigeminal artery, check out these co-registration images of angio (axial MIP reconstructions of rotational angio) and finally with superimposed tractography of the Vth nerve! Images courtesy Dr. Nader Delavari
Superimposed MRI and angio axials (our trigeminal artery is shown bi arrow)

Now with tractography of CN V
Another trigeminal origin MMA (arrows), courtesy Interventional Neuroradiology Department of Strasbourg University Hospital
An unusual origin of trigeminal artery from the medial horizontal cavernous carotid segment. This may be a variant of MHT origin — a super rare one at that. Another possibility is that the origin is at location of the capsular arteries of McConnell. These are usually below even angiographic resolution, and supply the dura and bone of the sella turcica. They do not classically supply the pituitary itself (nor give rise to trigeminal artery…). No catheter angiography is available.