
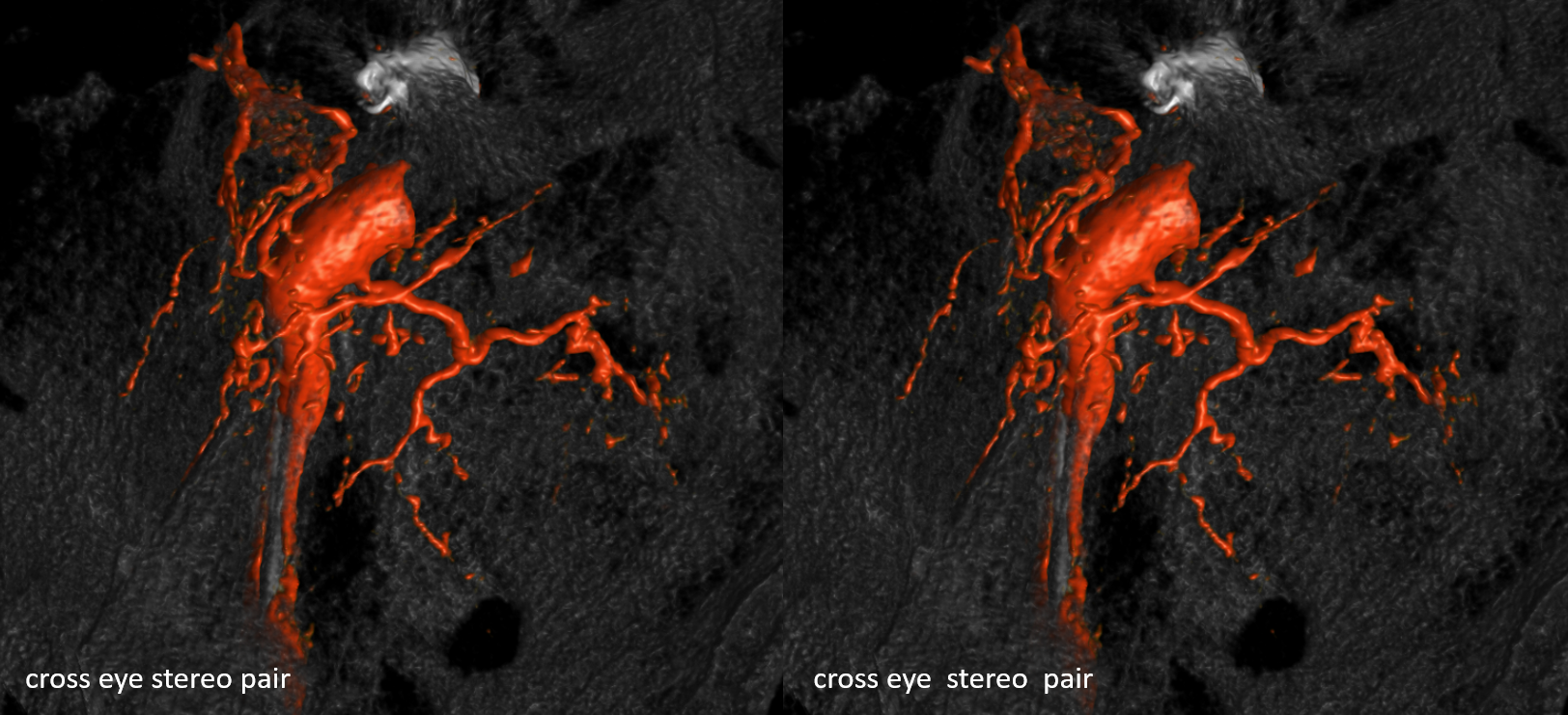
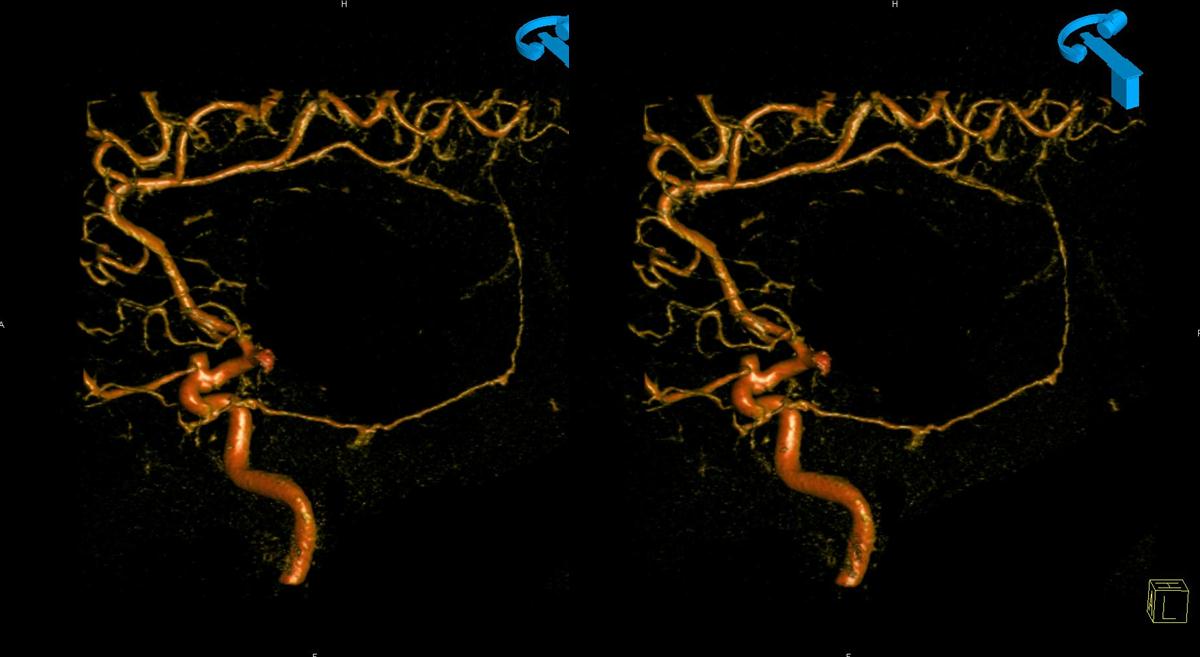
Stereo
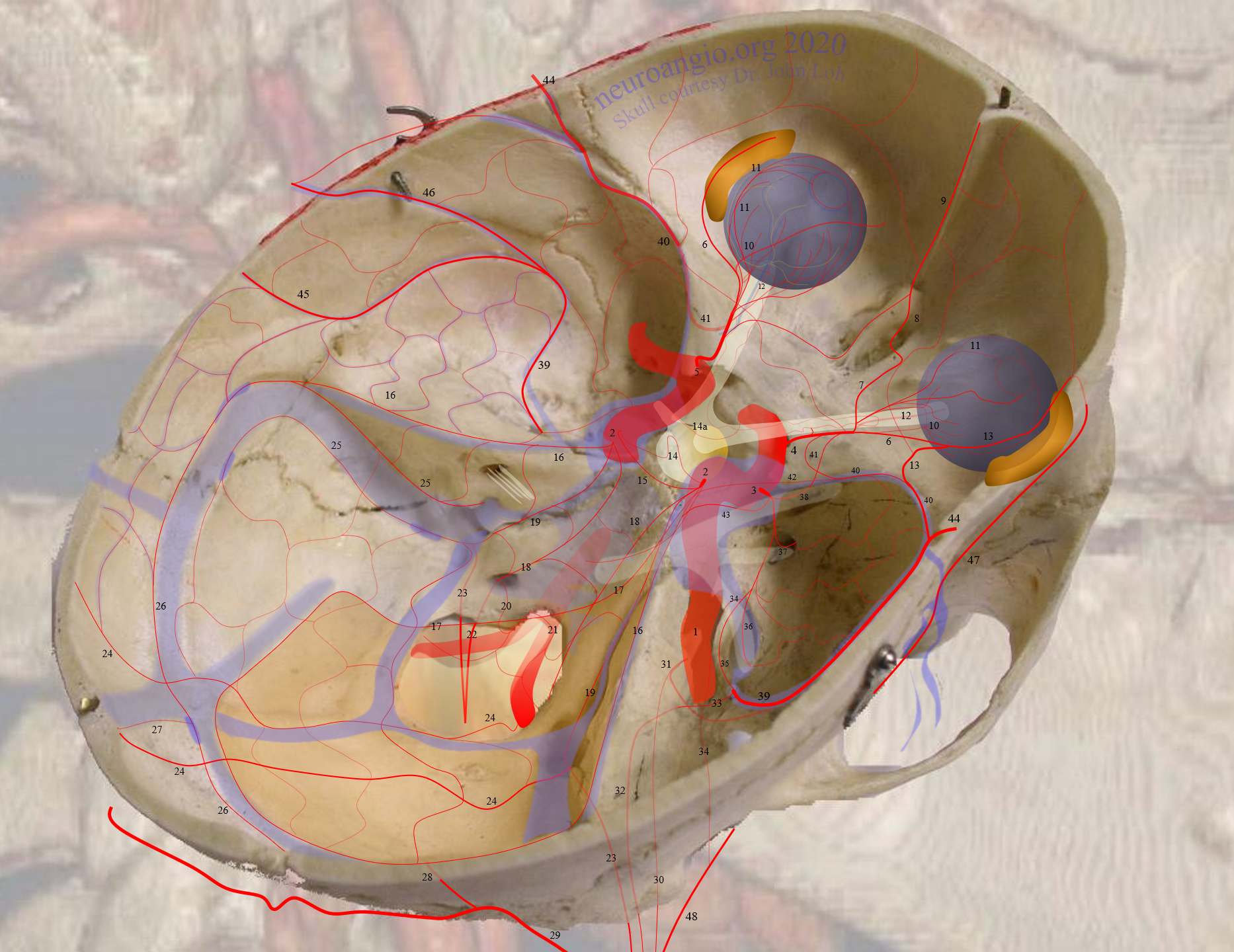
Meningohypophyseal Trunk (number 2 above) is a key region located in the posterior genu of the ICA cavernous segment. It may be a single or several trunks. MHT vessels usually supply the posterior pituitary and portions of the clivus, CN III, IV, V, and VI, tentorium cerebelli, and adjacent dura.
BALANCE / ADJACENT TERRITORIES
The MHT is in balance with the ILT, MMA, Accessory Meningeal, ophthalmic artery, hypoglossal branch of the ascending pharyngeal artery, and the superior hypophyseal arteries. Thus it is important both as an EC-IC anastomosis and cranial nerve supply area. Also see Diagrams and Drawings page.
Classic Branches:
Inferior Hypophyseal (14) — supplying posterior pituitary. In balance with contralateral homolog and, occasionally, the superior hypophyseal family
Lateral Clival Arcade (19) — anastomosing with / same aracde as ascending clival branches of the Jugular Division of the Ascending Pharyngeal Artery
Medial Clival Arcade (18) — anastomosing with / same aracde as ascending clival branches of the Hypoglossal Division of the Ascending Pharyngeal Artery
Marginal Tentorial Arcade (17) — also known as Artery of Bernasconi and Cassinari — supplying the free edge of the tentorium cerebelli
Lateral Tentorial Arcade (16) — arcade of the superior petrosal sinus, along the petrous ridge.
Deep recurrent meningeal / proximal marginal tentorial (42) — arcade in free margin between anterior and posterior clinoids. Connects the MHT with the ILT and recurrent meningeal/sphenoid ridge branches
Trigeminal — MHT/ILT to basilar/AICA anastomosis.
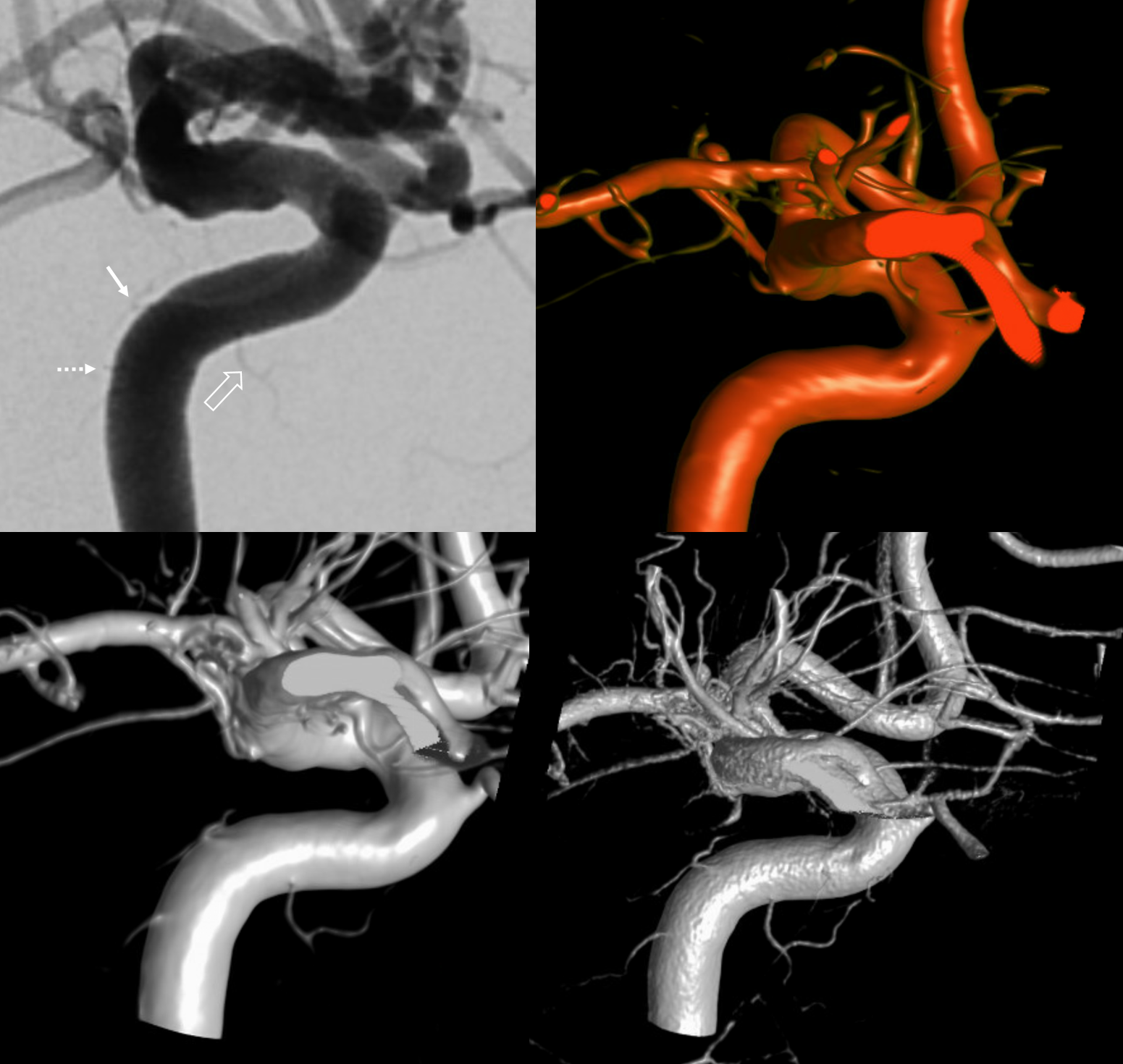
IMAGING APPEARANCE
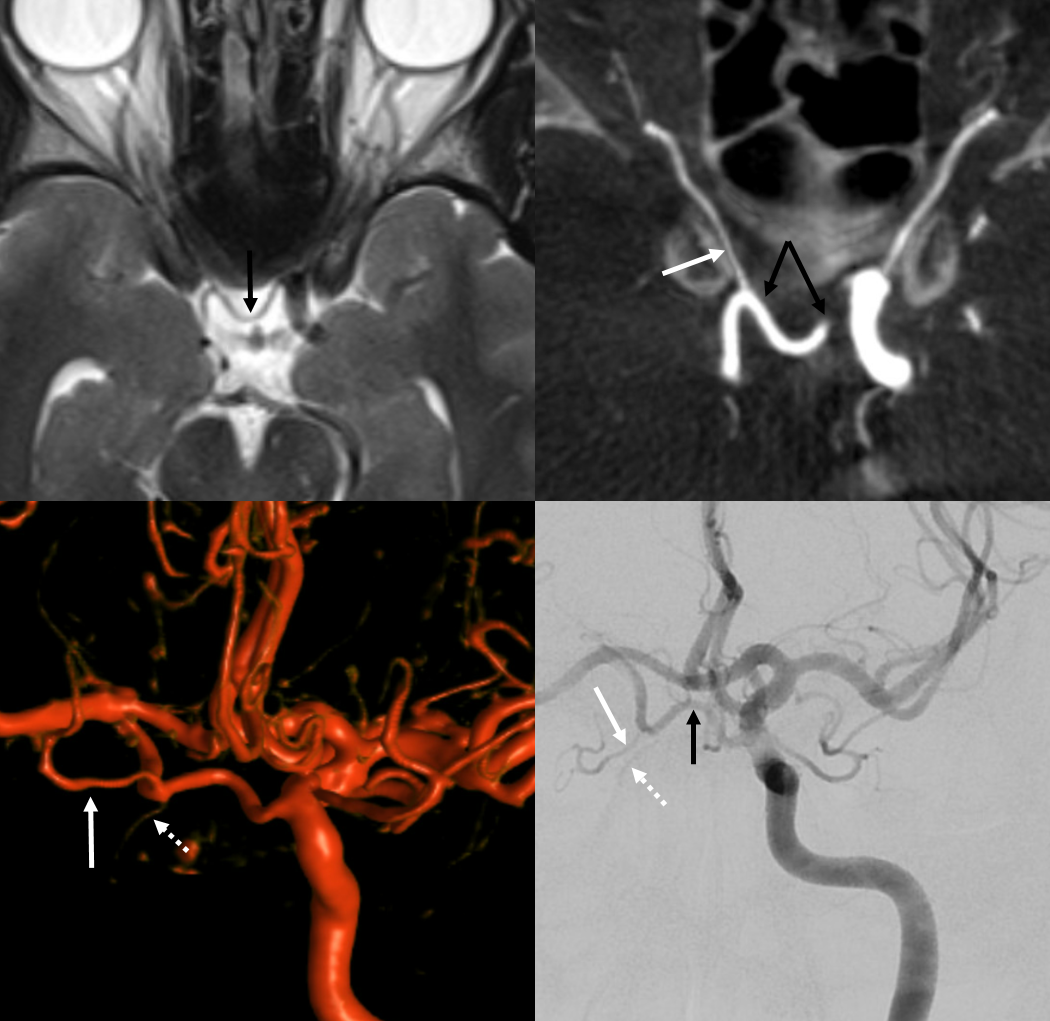
Varies substantially — the MHT is in balance with contralateral MHT, ILT, and others (see below). Generally invisible on MR or CT studies unless pathologically enlarged. 2-D angiographic appearance depends on technique, machine quality, and intrinsic size. Study of detailed anatomy and anastomoses requires Cone Beam CT.
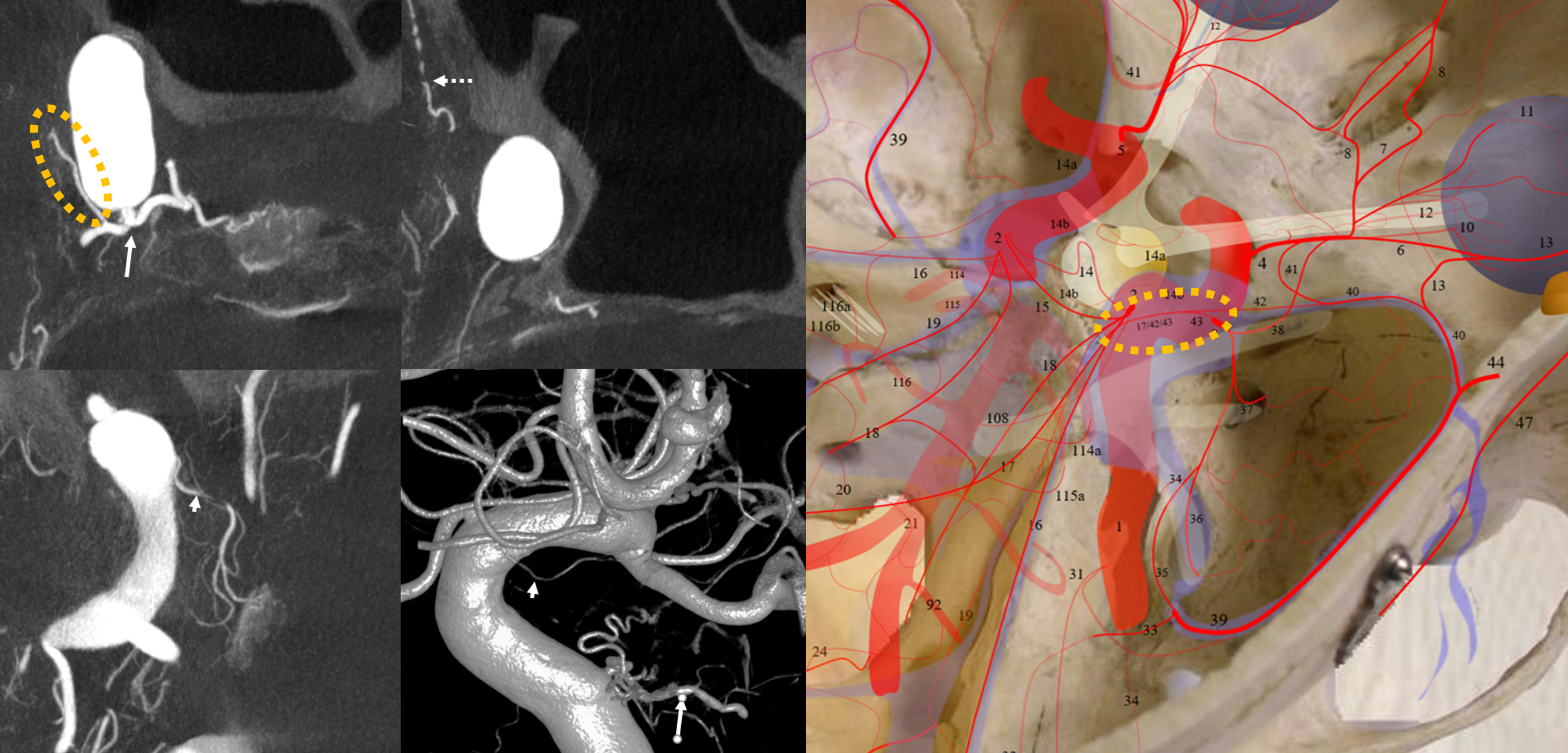
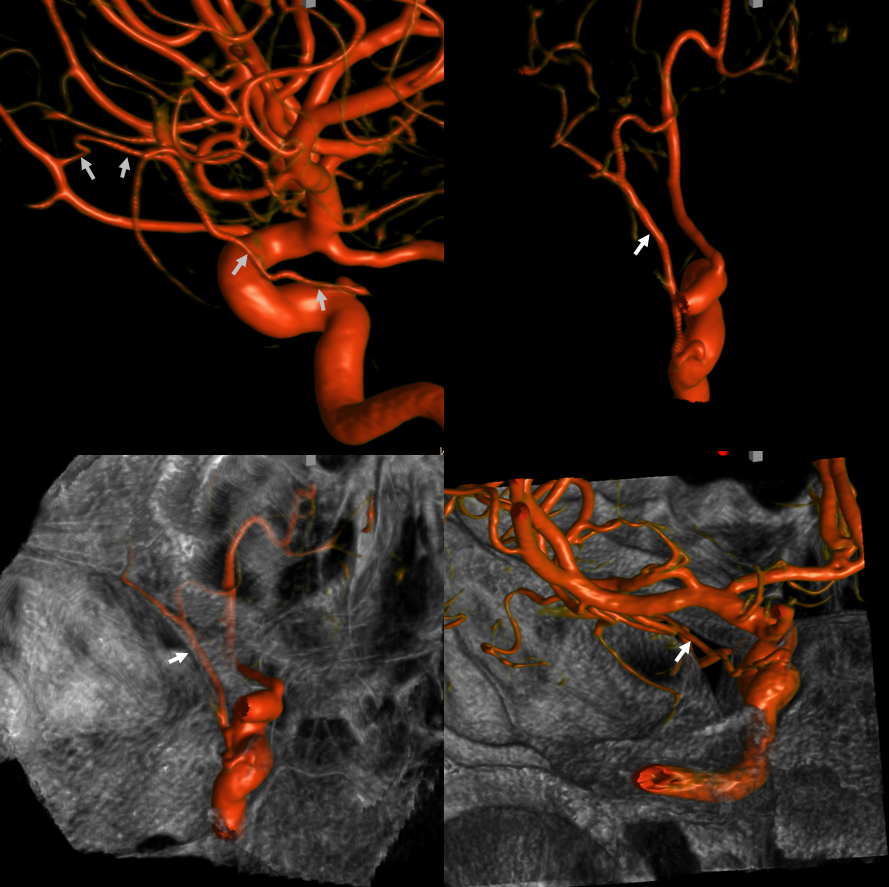
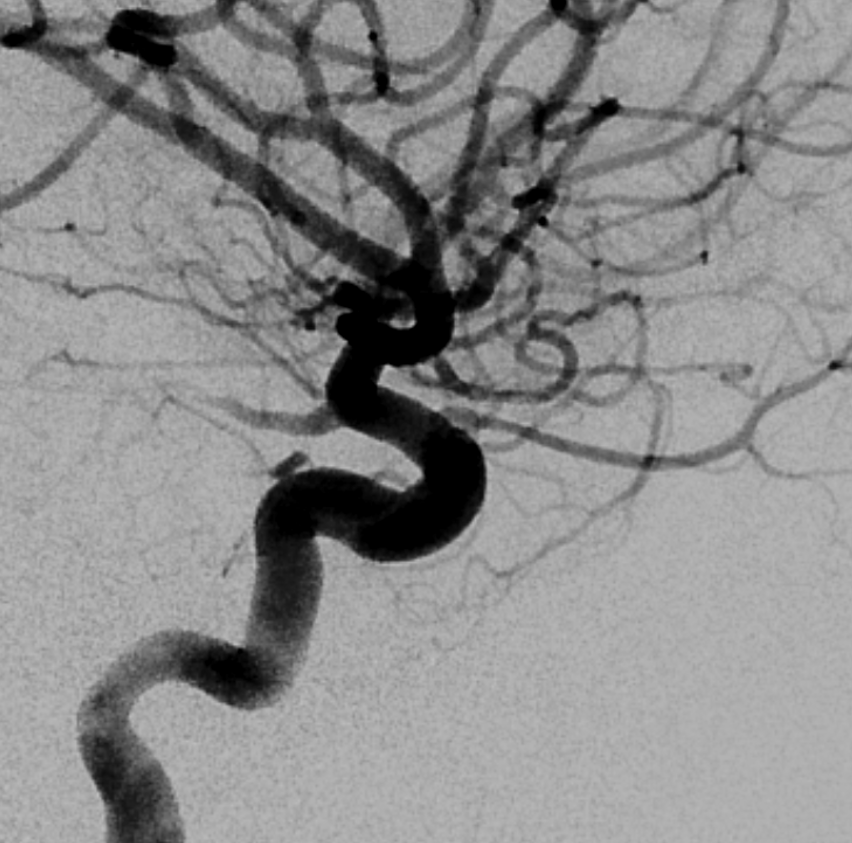
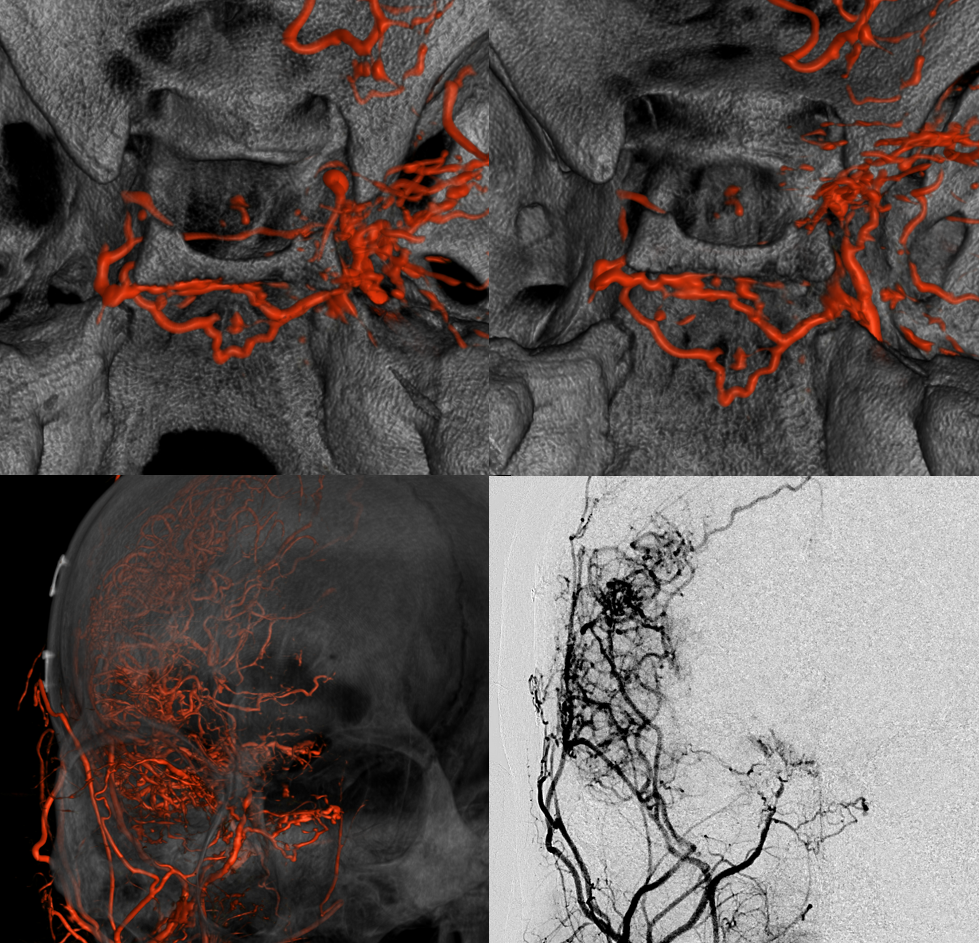
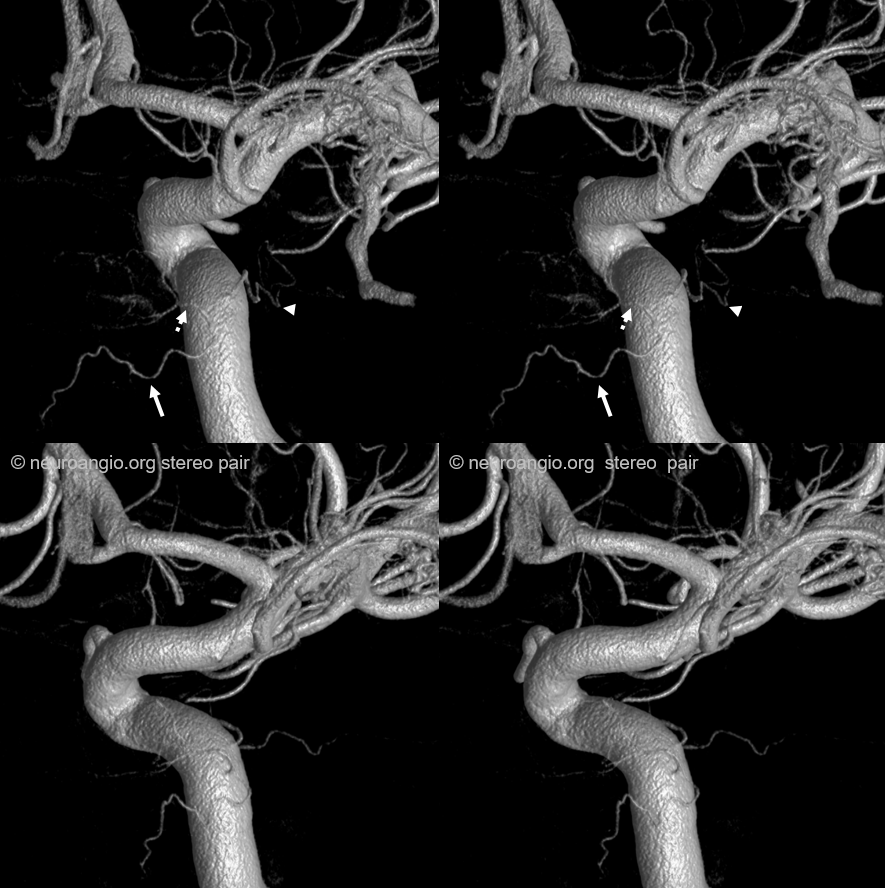
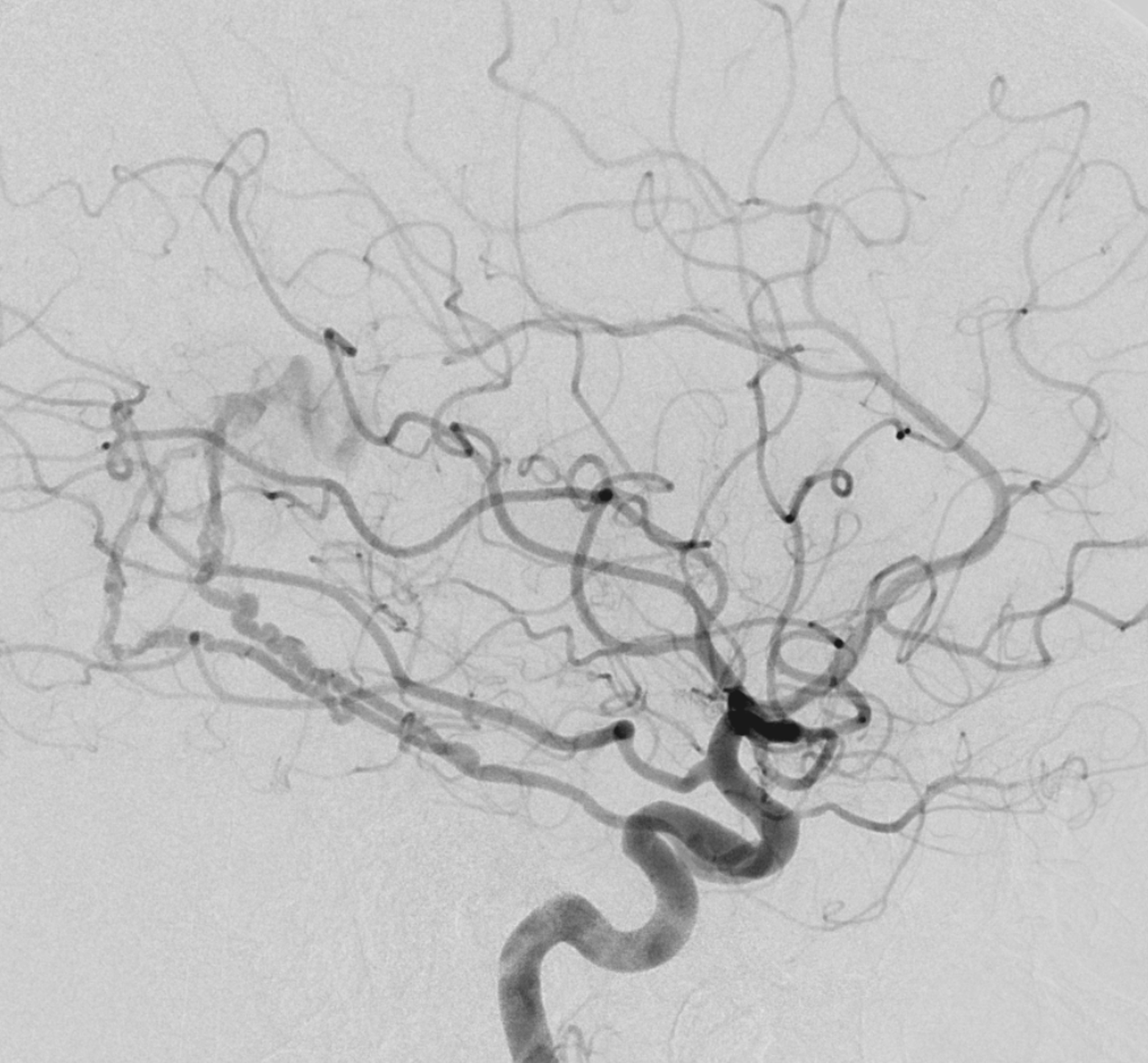
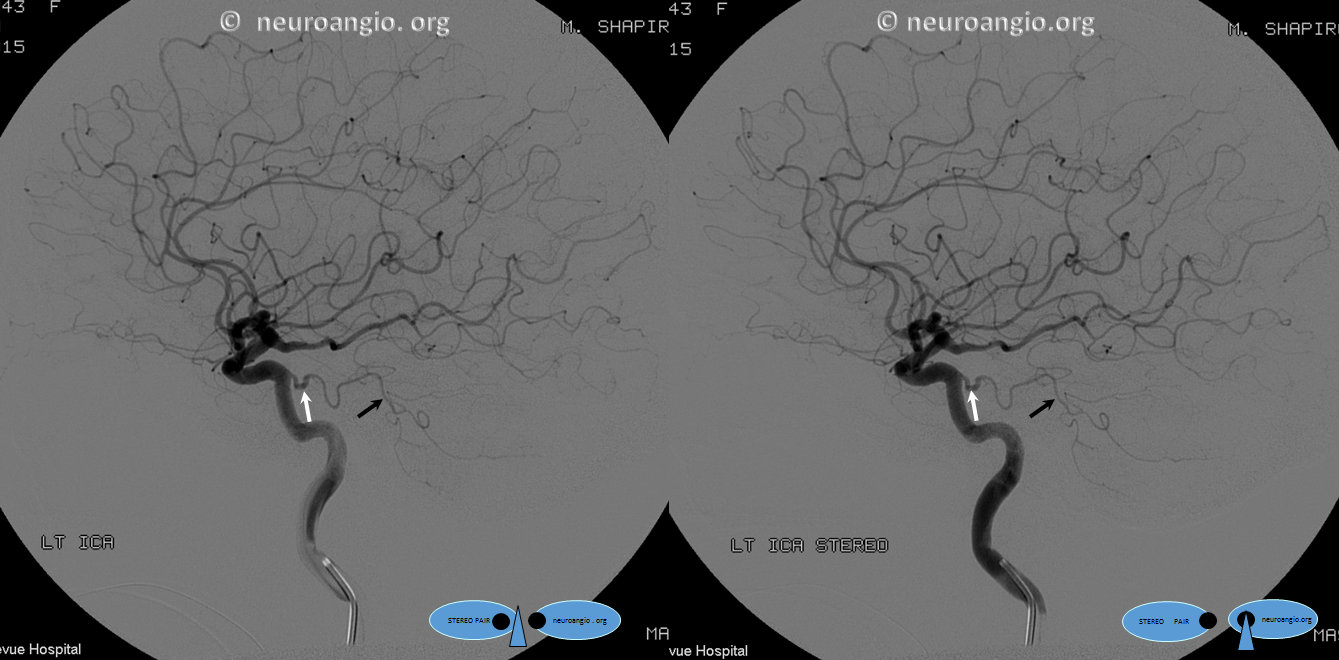
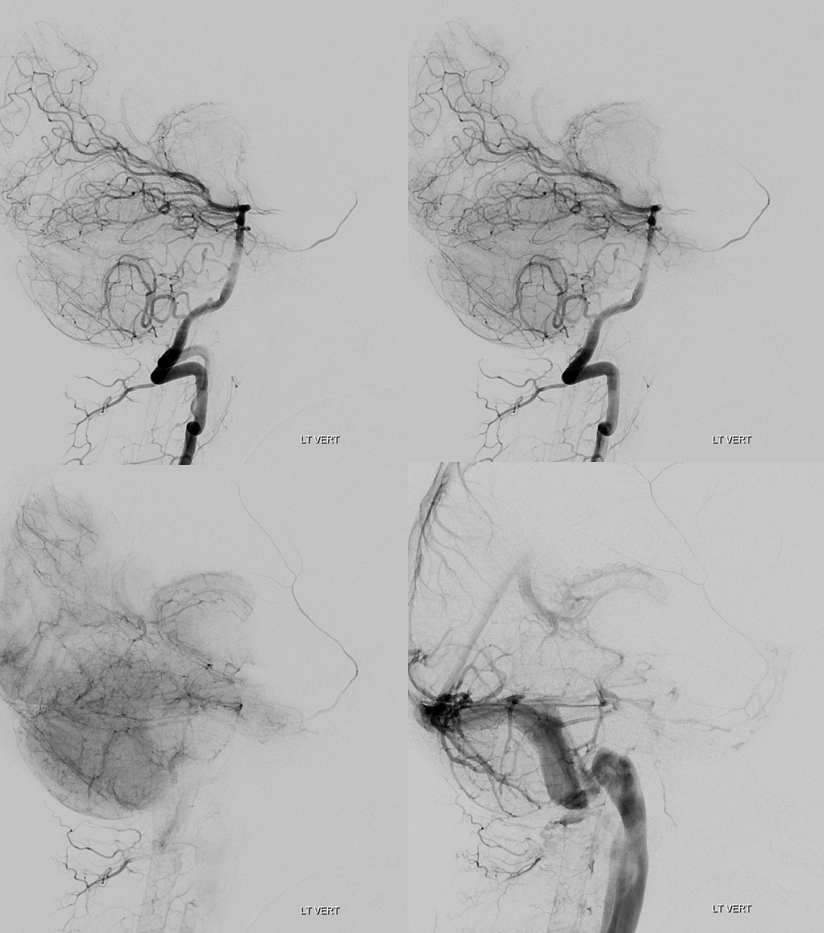
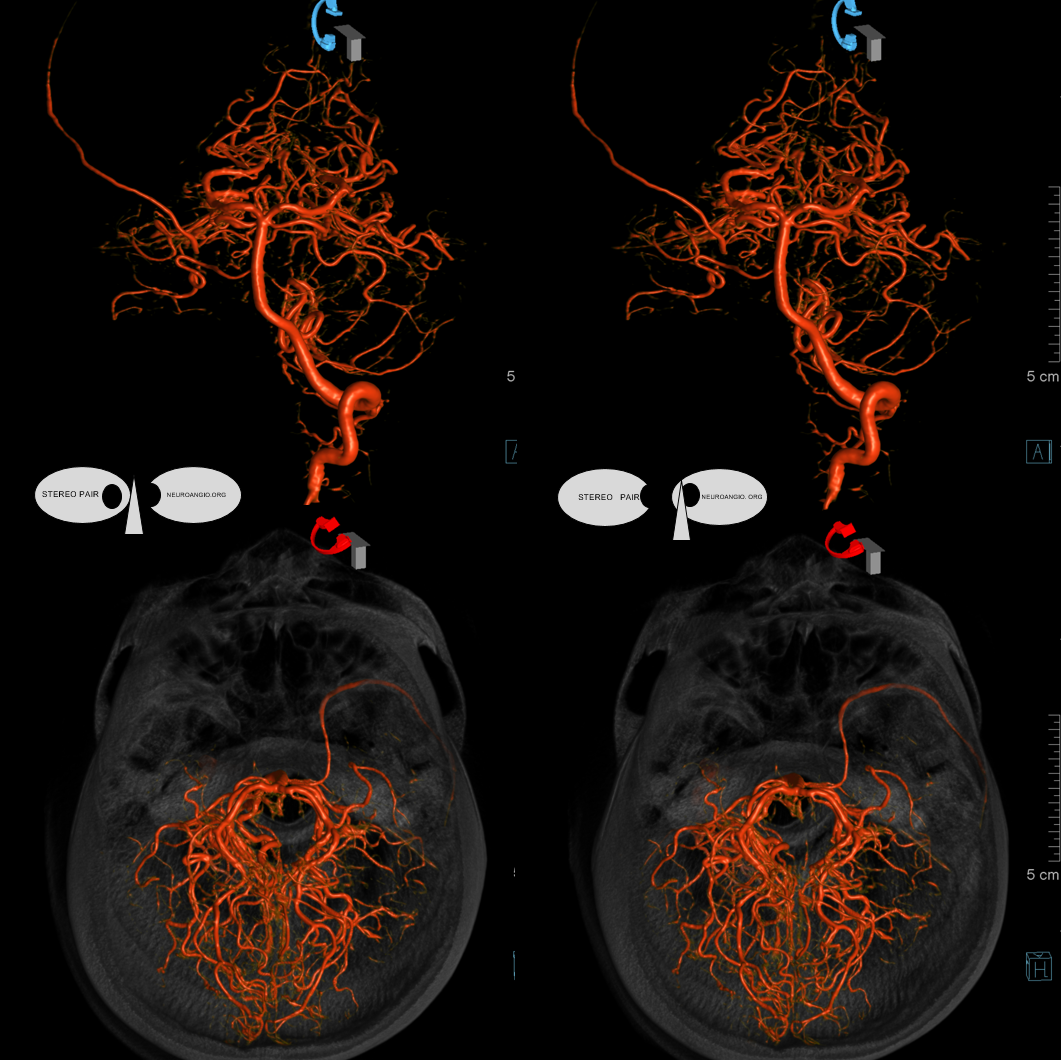
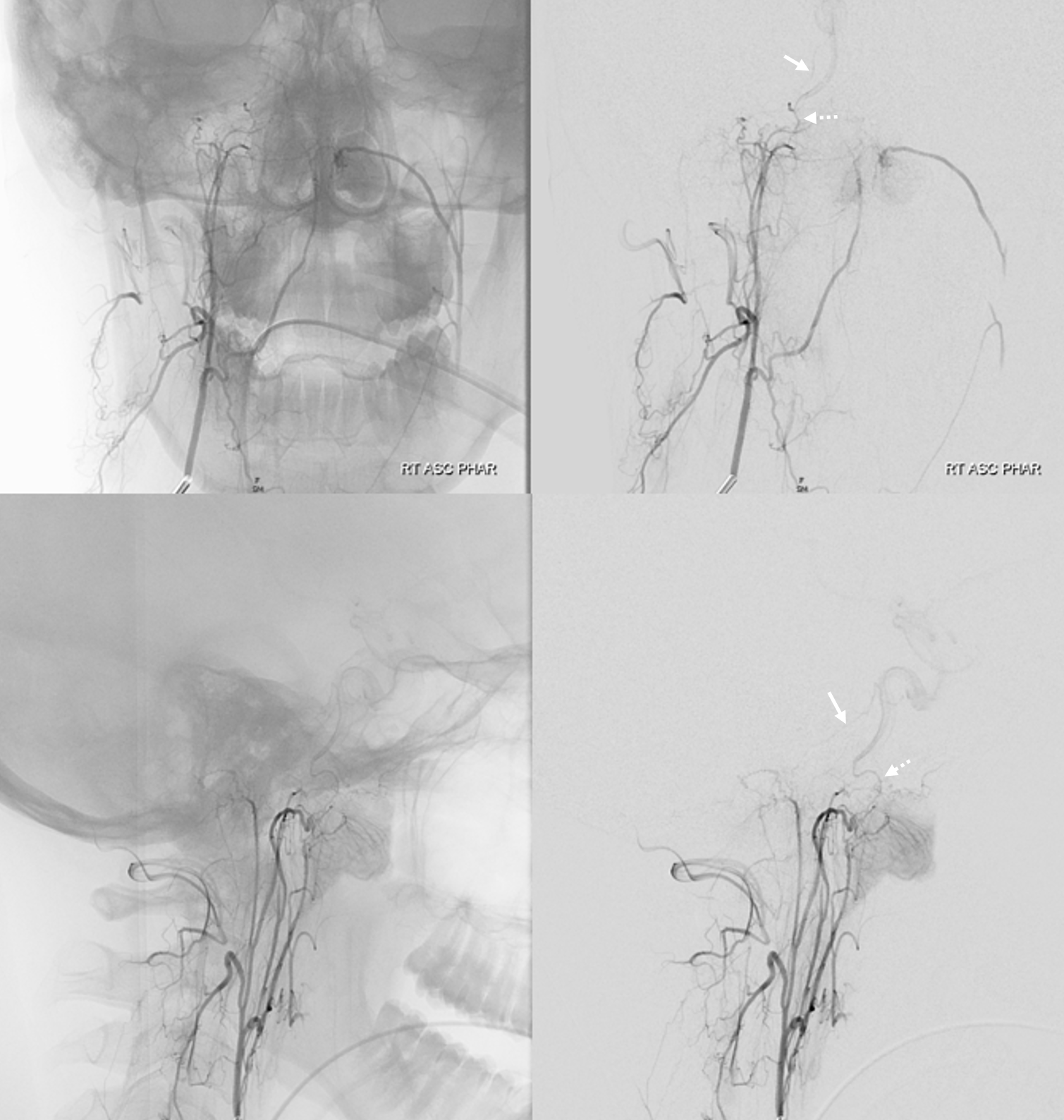
Below is the same case, imaged in 4 different ways. See for yourself. Top left — 2D-DSA. Top right — low resolution Cone Beam CT (3D-DSA), subtracted. Bottom left — low resolution Cone Beam CT (3D-DSA), UNsubtracted. Bottom right — high resolution Cone Beam CT (DYNA), unsubtracted.
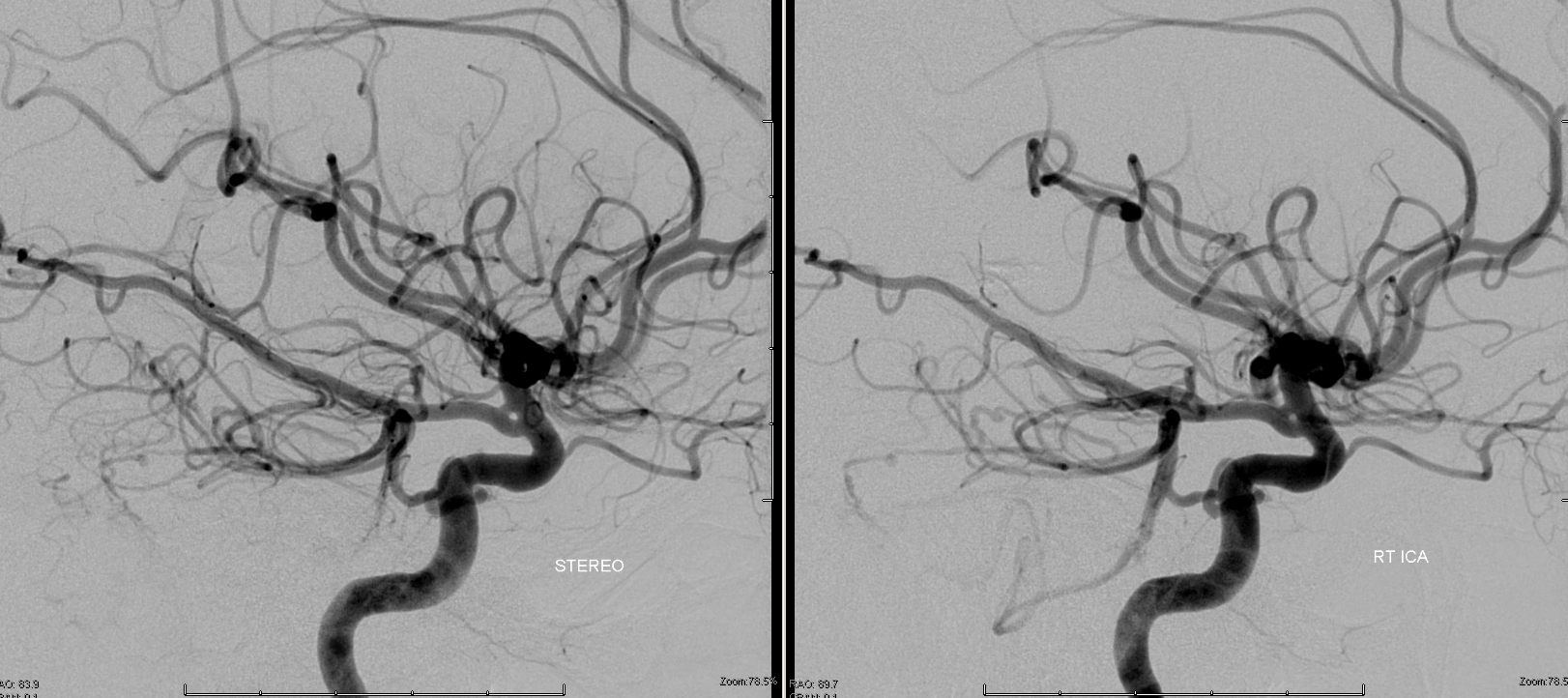
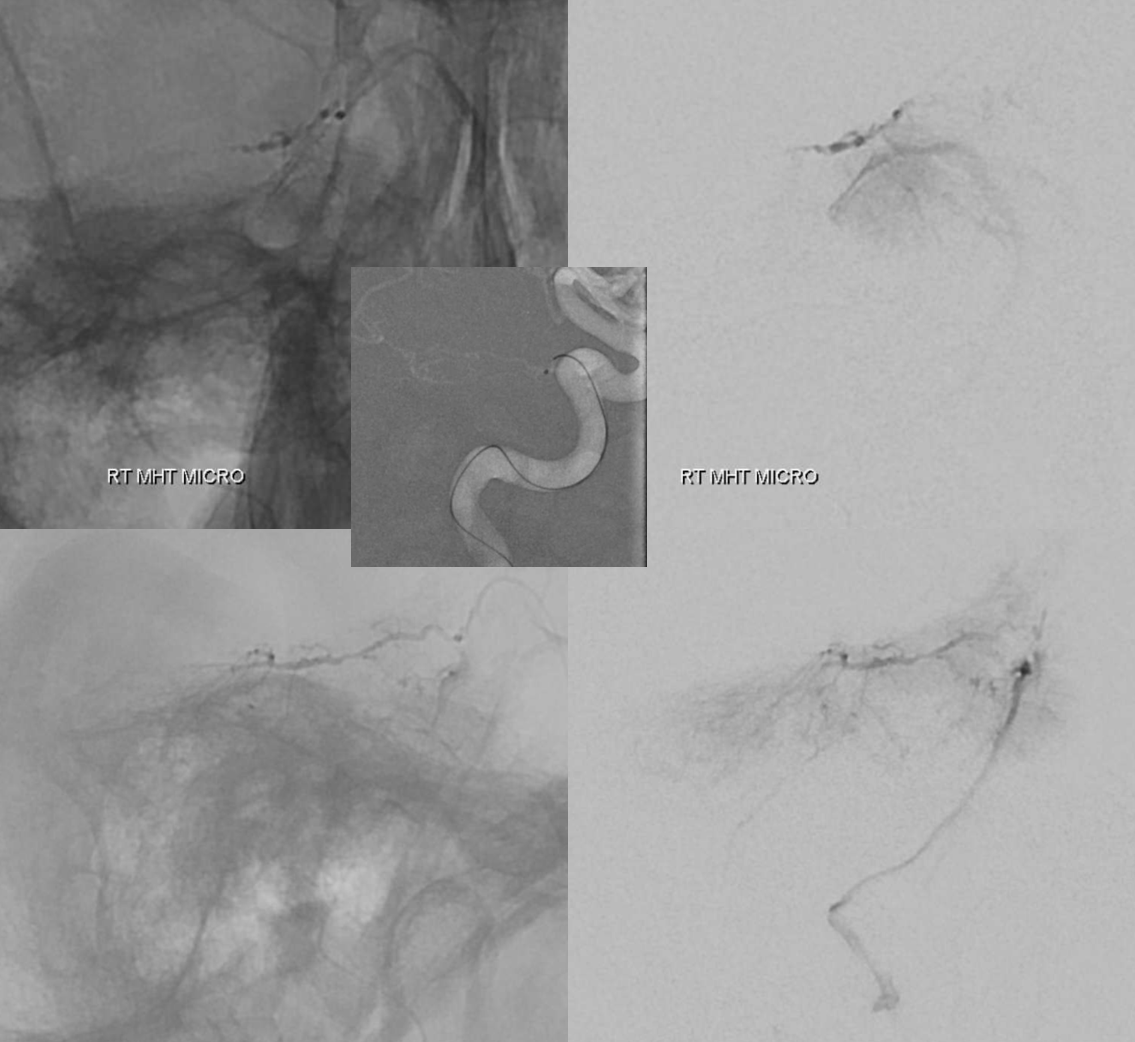
2D-DSA Classic


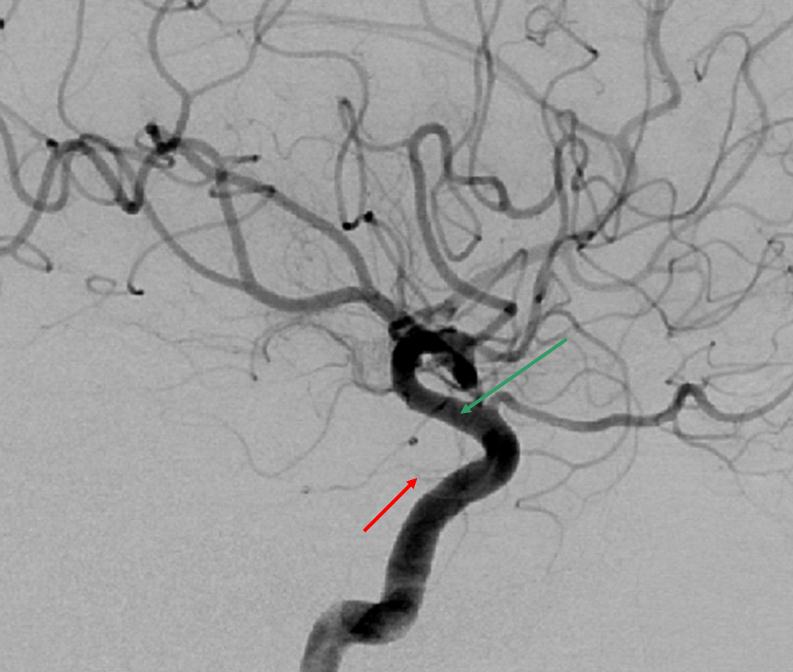
MHT-ILT Balance
Very important concept. Classic images / texts always depict both MHT and ILT in a happy equal coexistence (just like there is likely to be a perfect circle of Willis in most books). You know that’s not how the Willis circle is. The same applies to nearly every other “ideal” situation. “Normal” MHT and ILT are often in balance — the smaller the one the larger the other. Because they are also in balance with other areas (meningeal, ophthalmic, accessory meningeal systems) the situation is typically more complicated. It is important to consider the system as a whole and understand balance among different sources (functional neuroanatomy). To really appreciate this high resolution cone beam CT is required.
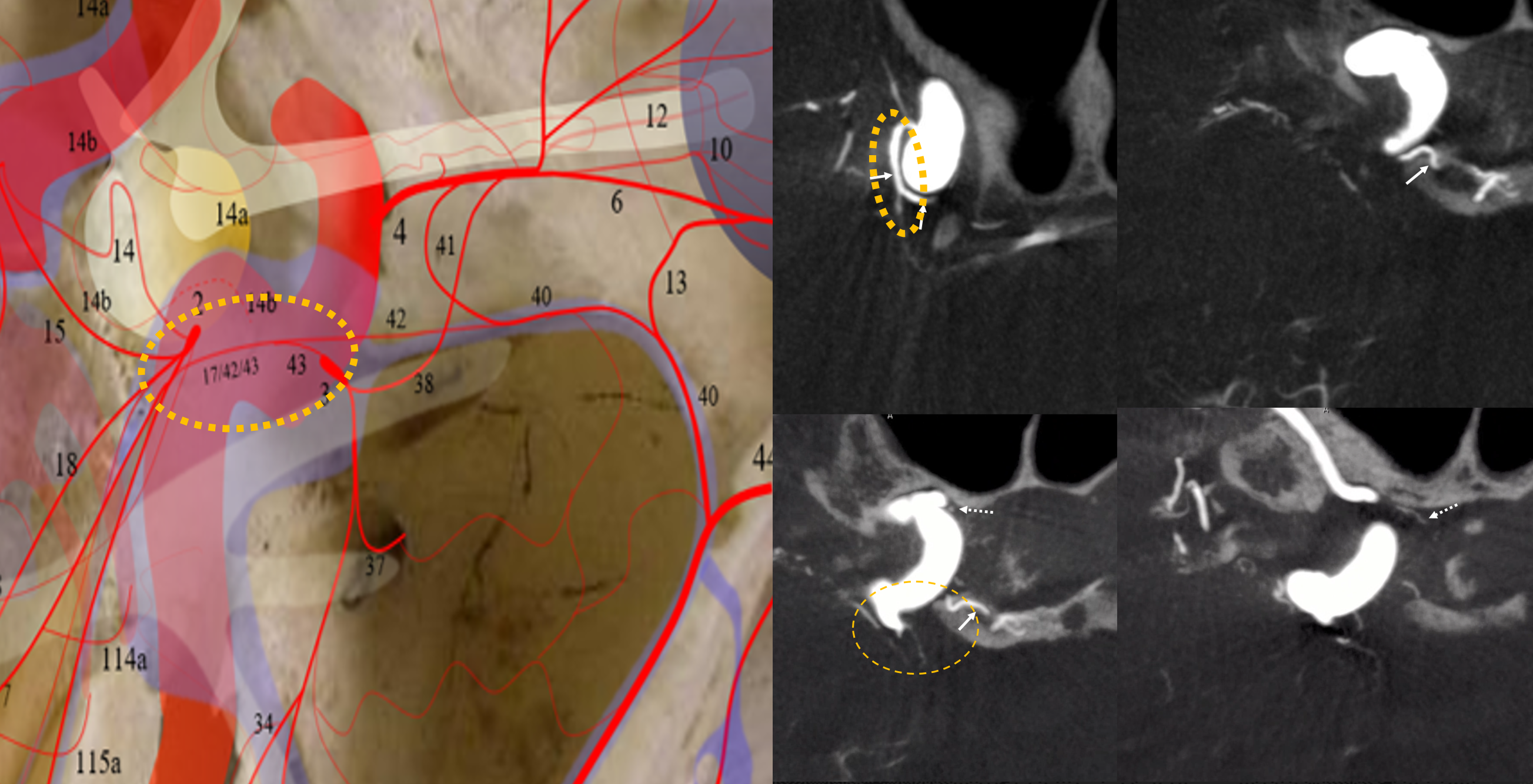
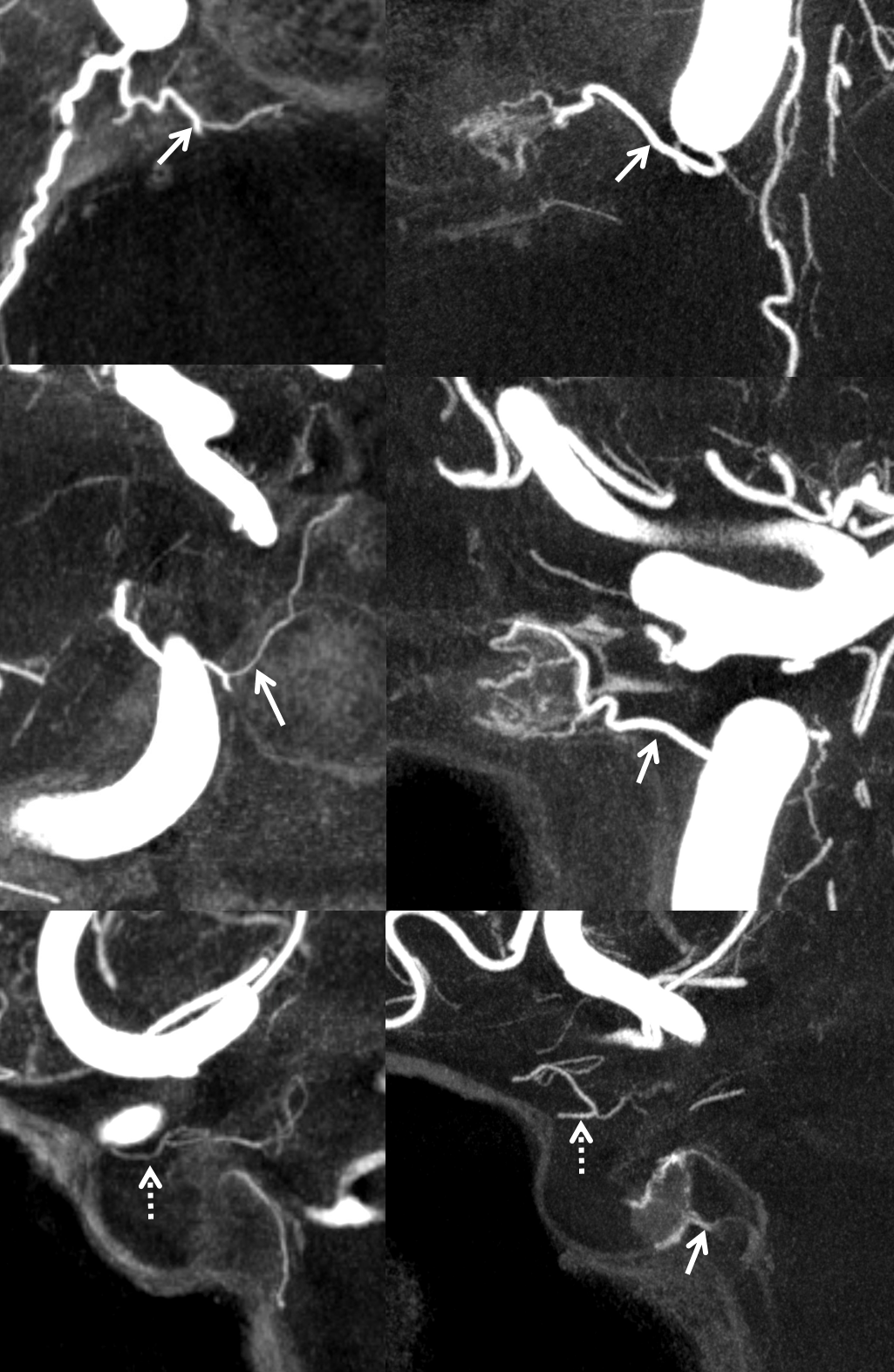
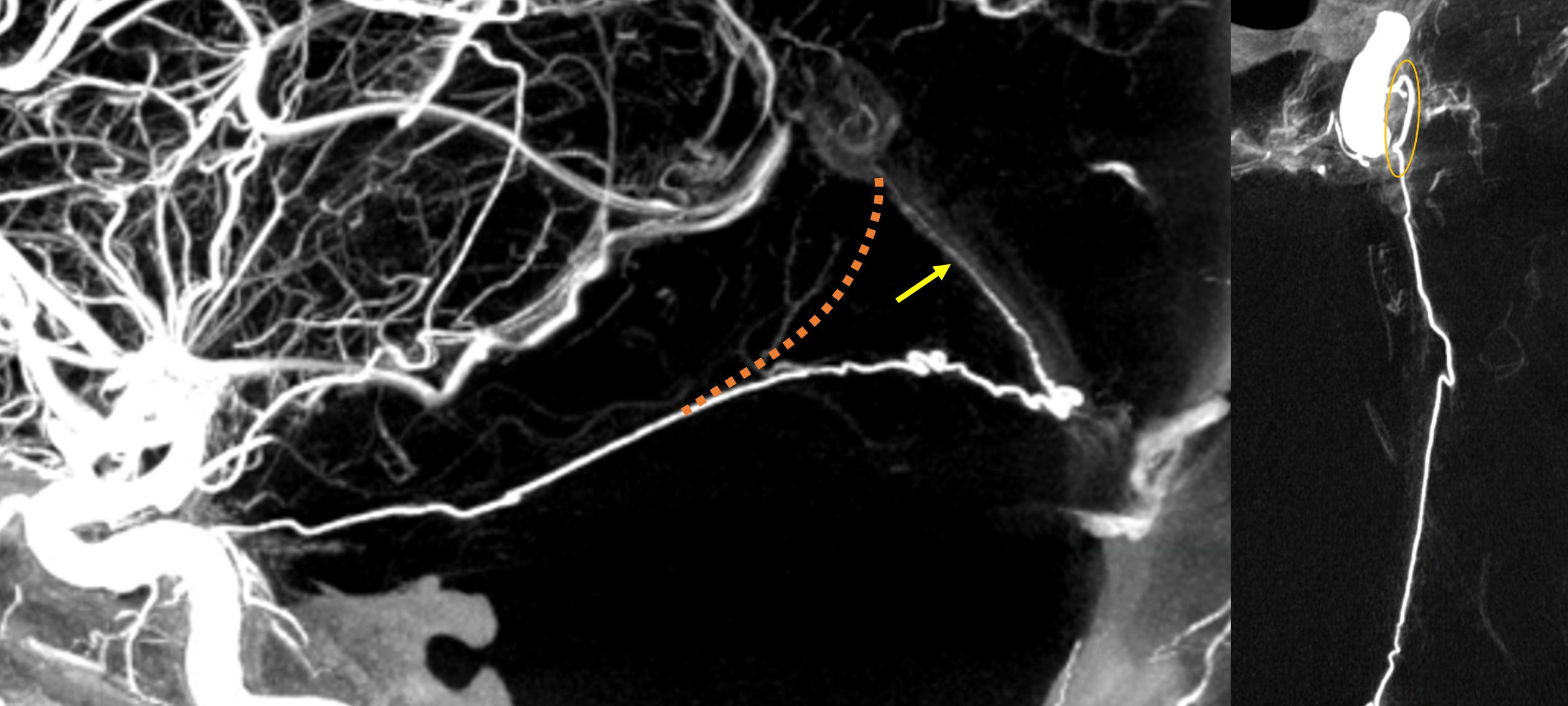
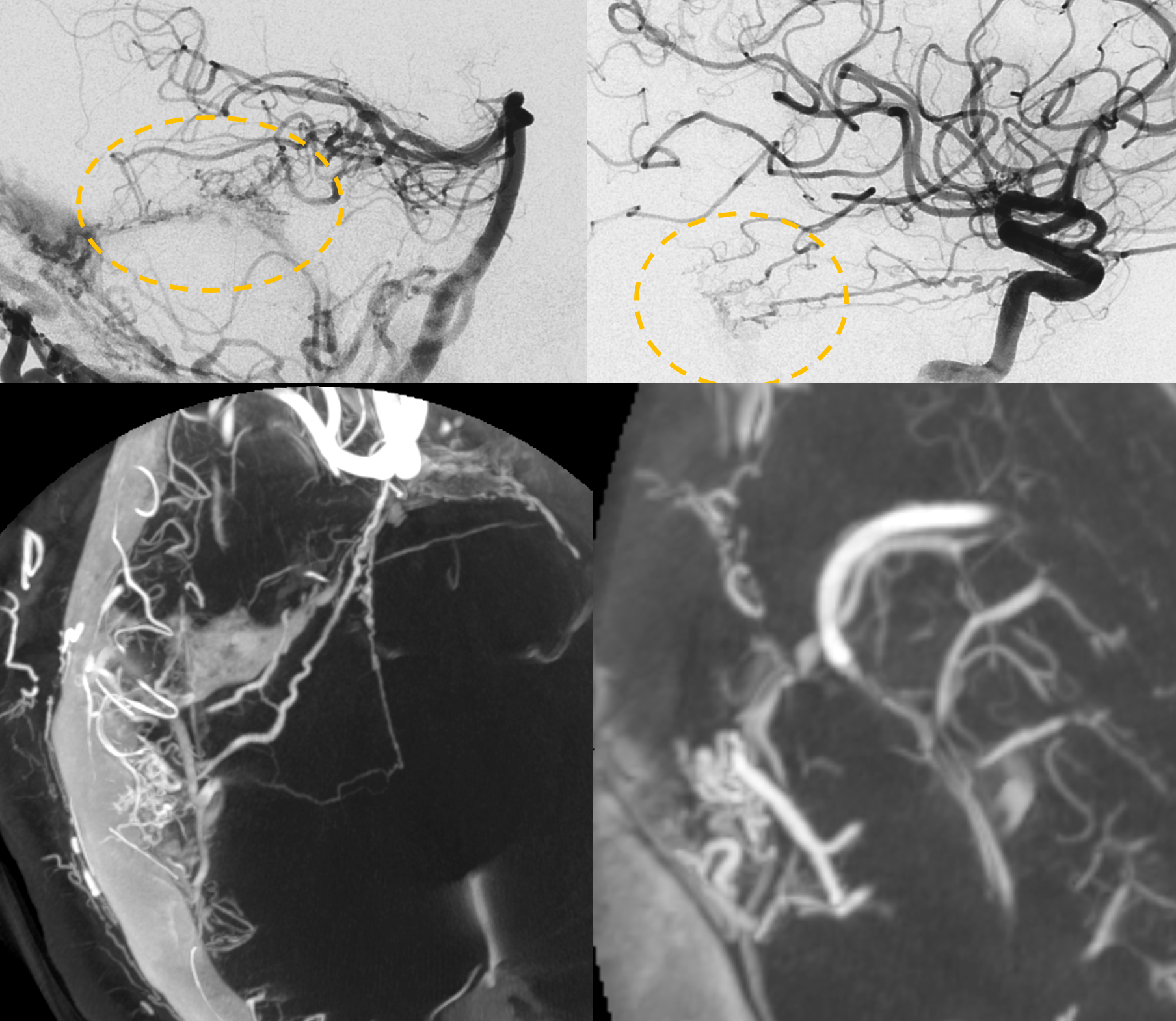
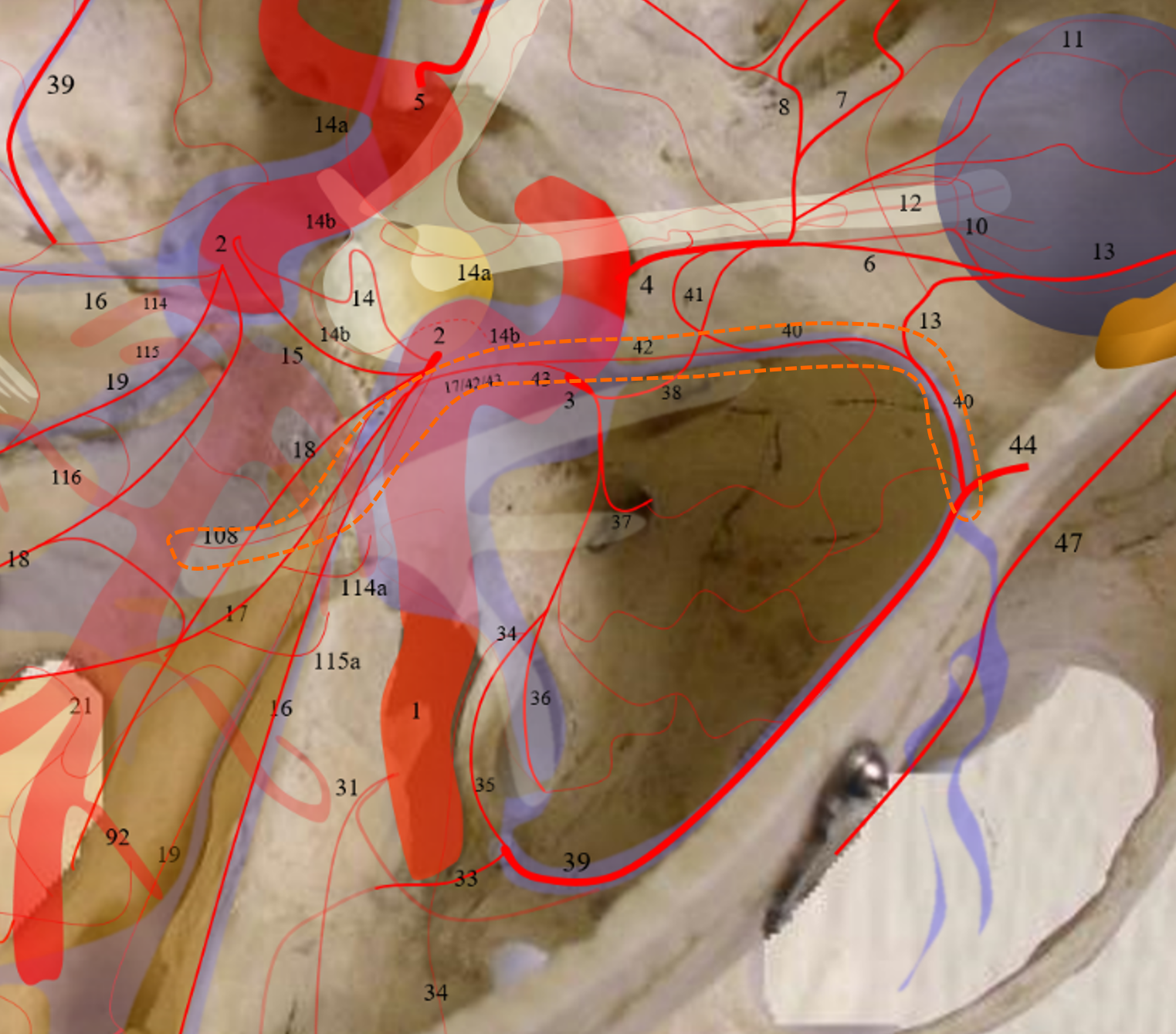
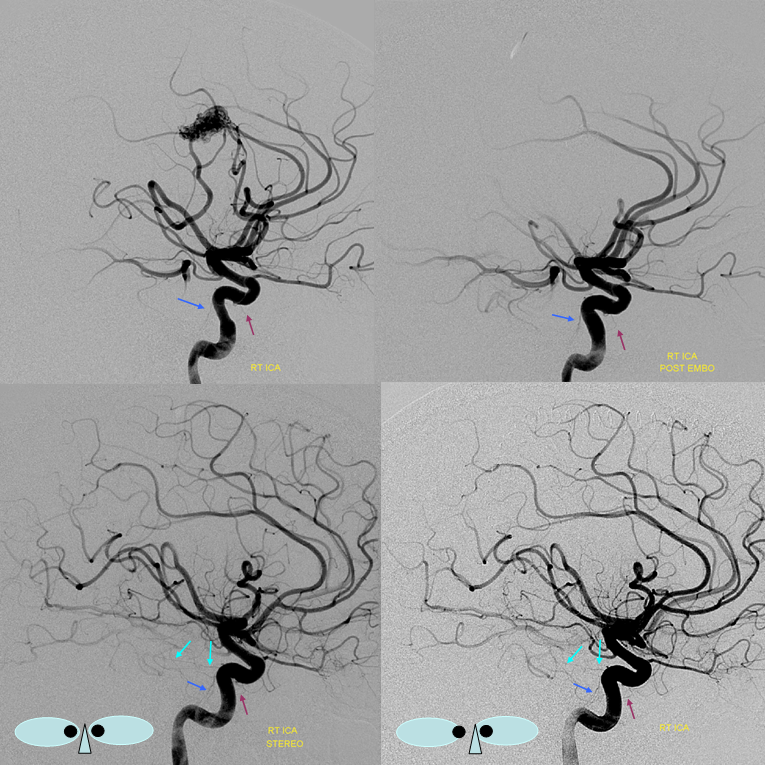
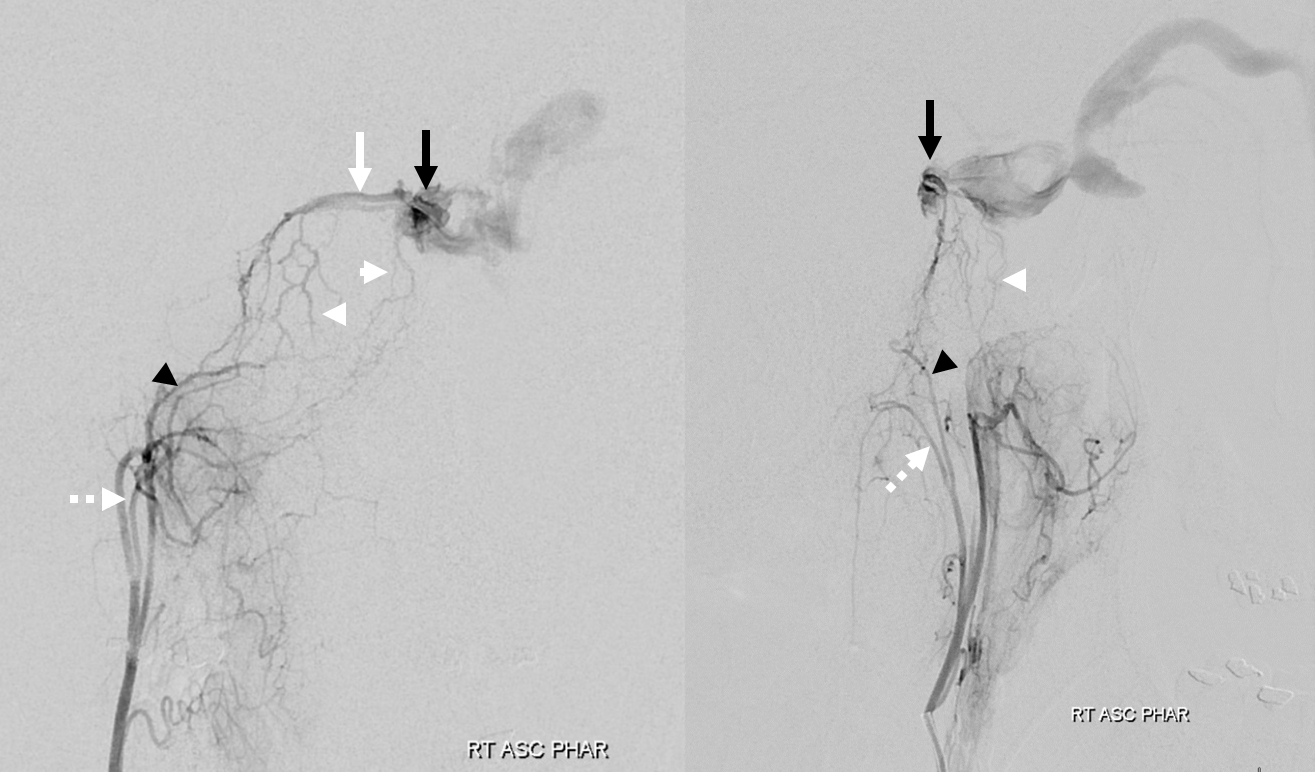
The connection between MHT and ILT is almost always via the “deep recurrent meningeal” arcade. It is very important and does not have a good name. When seen from ILT it is called the “superior branch”. When seen from the ophthalmic it is called the “deep recurrent meningeal”. Below it is labeled 17/42/43. The ILT is hypoplastic, with MHT reconstitution (dashed orange ovals). Note reconstituted anteromedial branch (dashed arrow) in the foramen rotundum. Arrowheads are on the superior hypophyseal artery.
Another example below
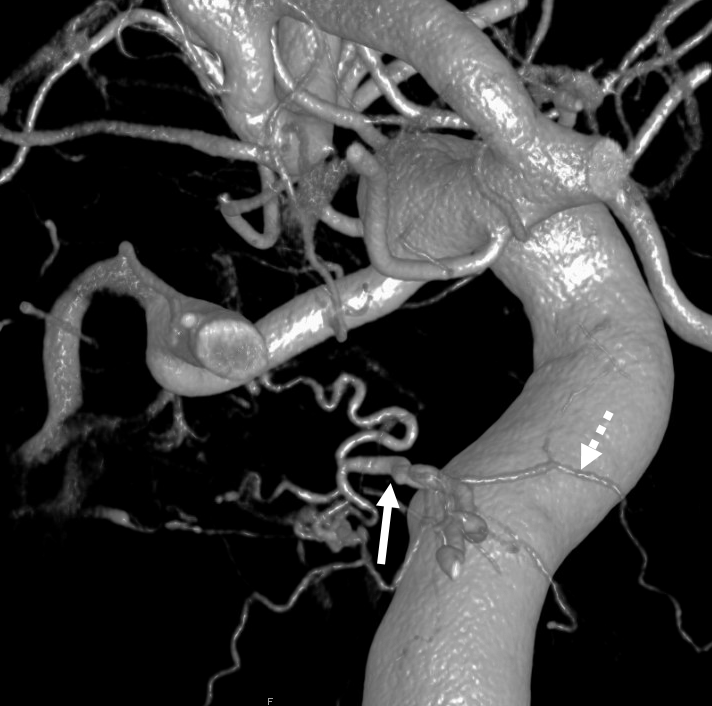
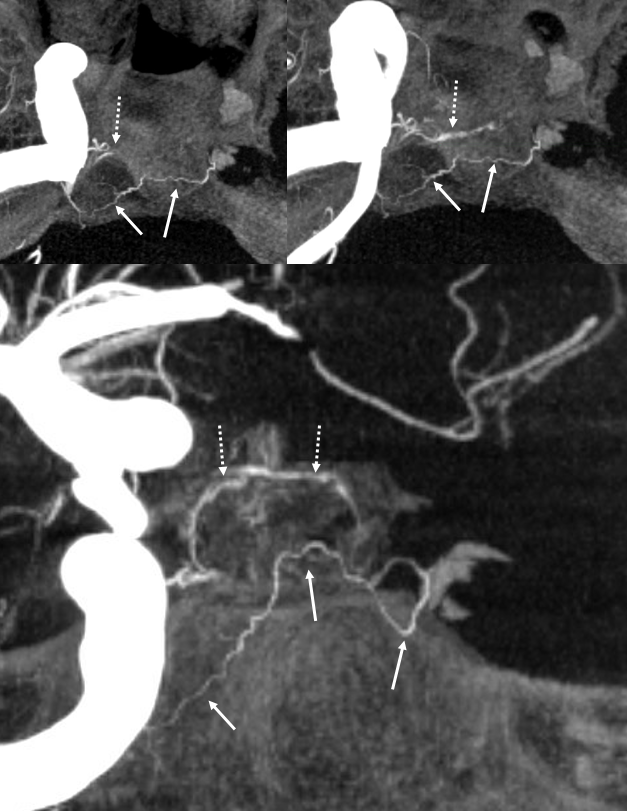
Another example
The 17/42/43 “deep recurrent meningeal” / marginal tentorial artery (arrows) reconstitutes the ILT

Yet another example — to show you this balance is very real
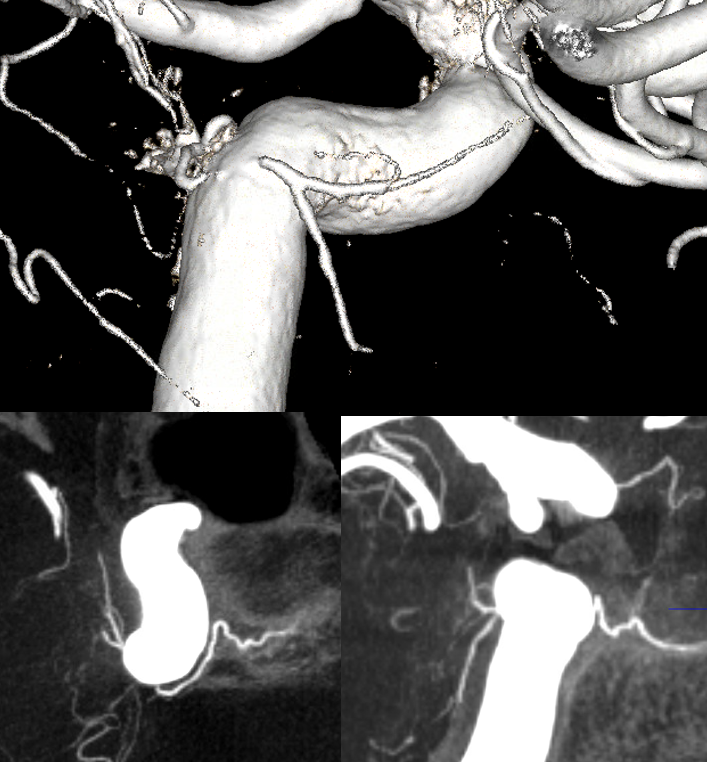
Movie of the same case
MHT — Ophthalmic Balance!
A more extreme (and therefore rare) version of balance between MHT and ILT. Remember we showed above how MHT can reconstitute ILT territory extending into foramen rotundum? The balance principle is that progressively greater takeover of one territory by another is correspondingly rarer. For example, ILT can occasionally contribute to supply of the ophthalmic via the “Dorsal Ophthalmic Artery” — the same vessel as the anteromedial branch of the ILT. So, you can now imagine that if an ILT were hypoplastic, and its territory supplied by the MHT as we saw above, it might happen that this supply could possibly extend into the orbit by the same “anteromedial branch” route. Below is an example of this
2D angio of the same case — can you recognize the connection? Not easy. We got the Cone Beam CT because MHT origin looked so weird
Dominant ILT
Of course, the reverse is also true — ILT can be dominant with a hypoplastic MHT. See ILT page for more examples. Below is one (including ILT supply of the posterior pituitary) — same 17/42/43 arcade, different direction…
MHT-MHT Balance
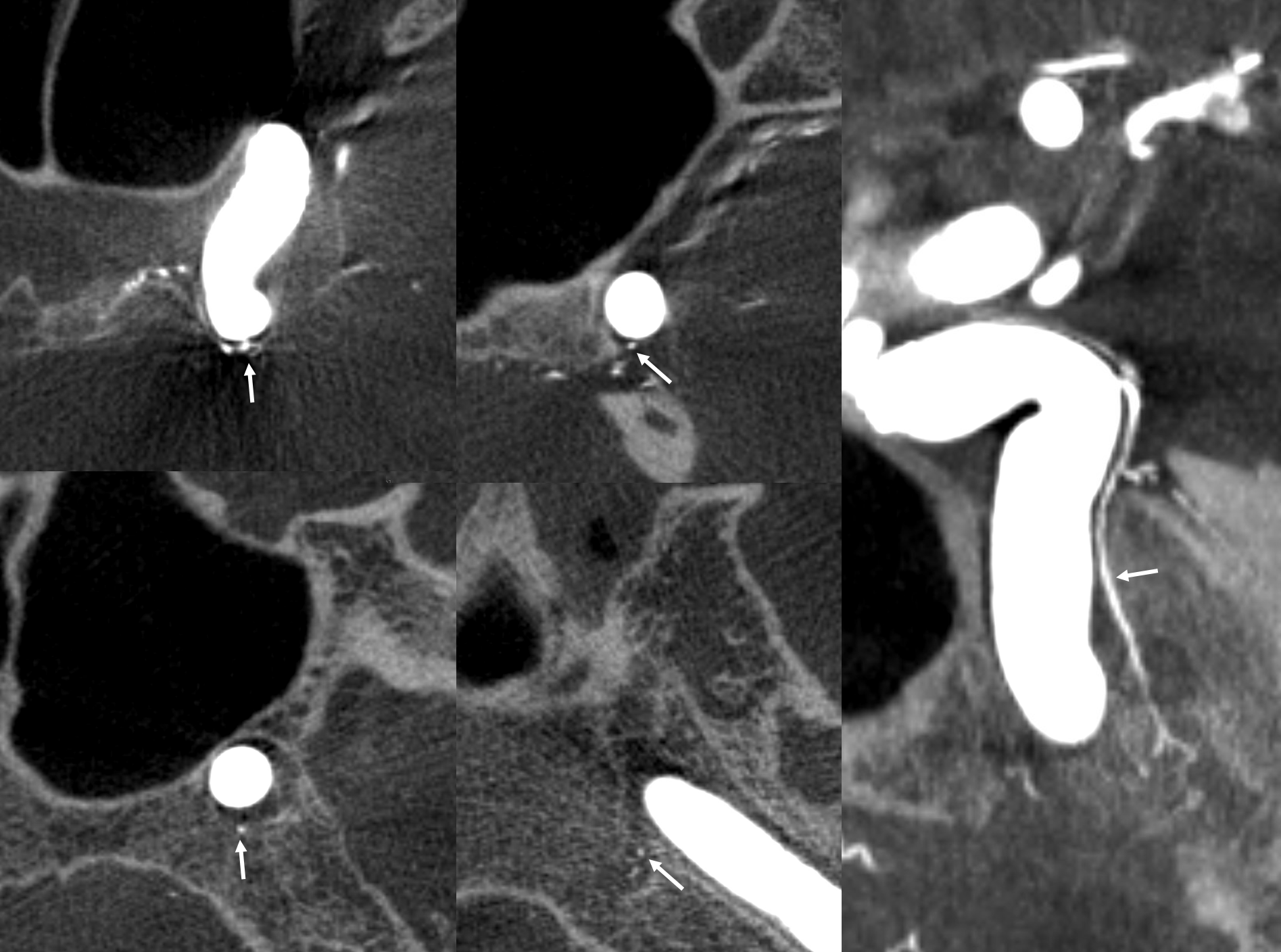
Sometimes due to developmental hypoplasia, other time because of athero, one MHT might be smaller than the other. The left-right balance mainly involves the posterior pituitary and the marginal tentorial arcade.
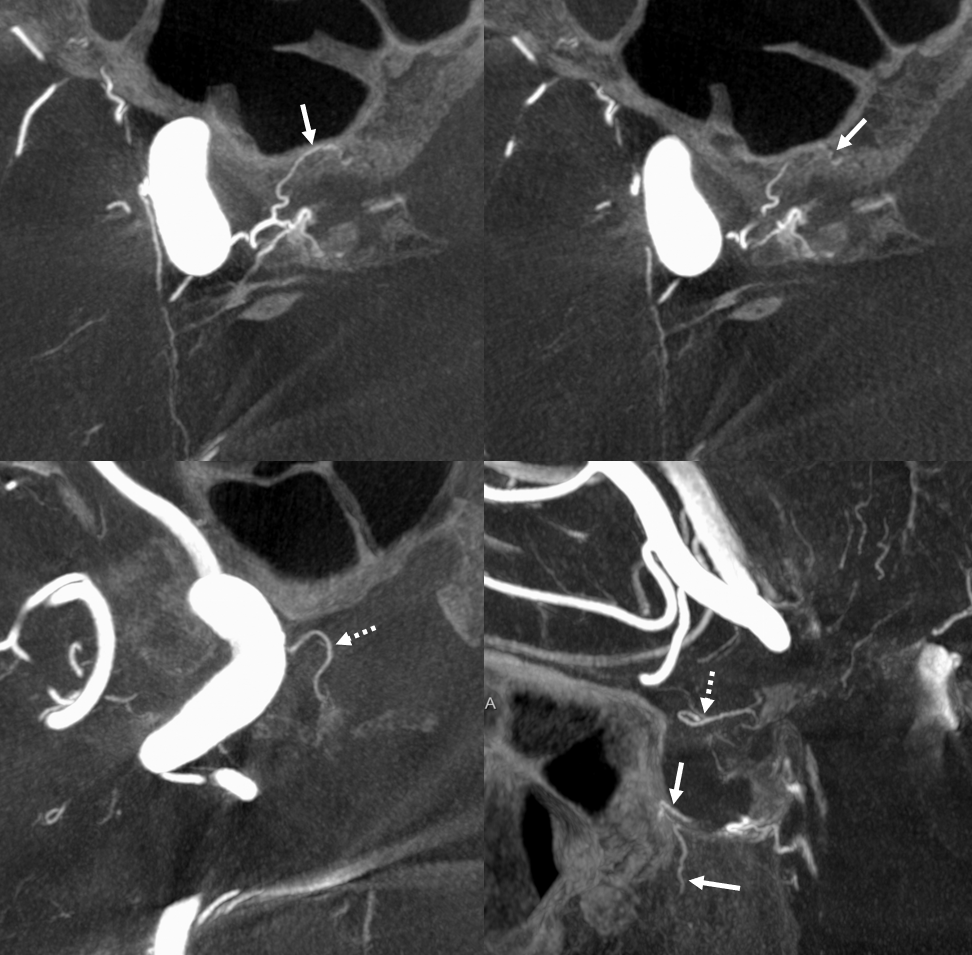
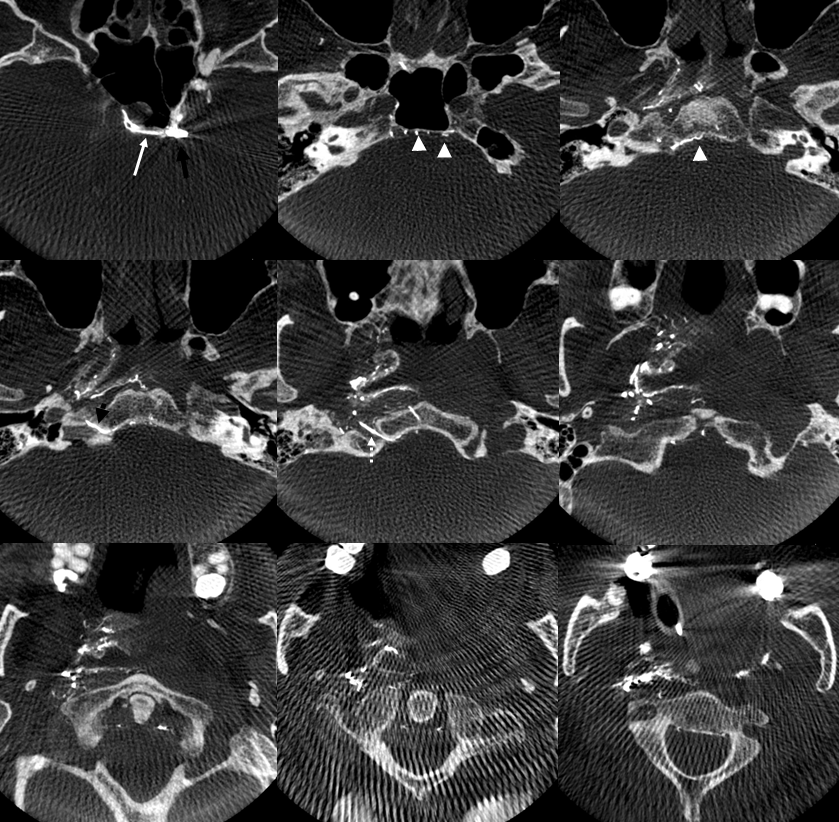
Reconstitution of left MHT occluded by atheromatous disease (see associated calcs) by right MHT — inferior hypophyseal (dashed arrows) and clival (arrows) arcades. Axials on top, coronal on bottom
Another Example of MHT-MHT balance: see dominant supply of the posterior pituitary from the LEFT (arrows). Anterior pituitary supply (dashed arrows) is bilateral
MHT-MHT Carotid Occlusion Reconstitution
Posterior Clival (medial, lateral, etc– purople) branches of left MHT (blue) converging on the right MHT (yellow) to help reconstitute cervically occluded right ICA (red). Old image
More recently — Moya Moya. Right side is worse, but left has an acute cervical carotid occlusion. The righteous right ICA donates despite its own hardship. Both posterior clinoid (15) and inferior hypophyseal intrasellar (14) anastomoses are present
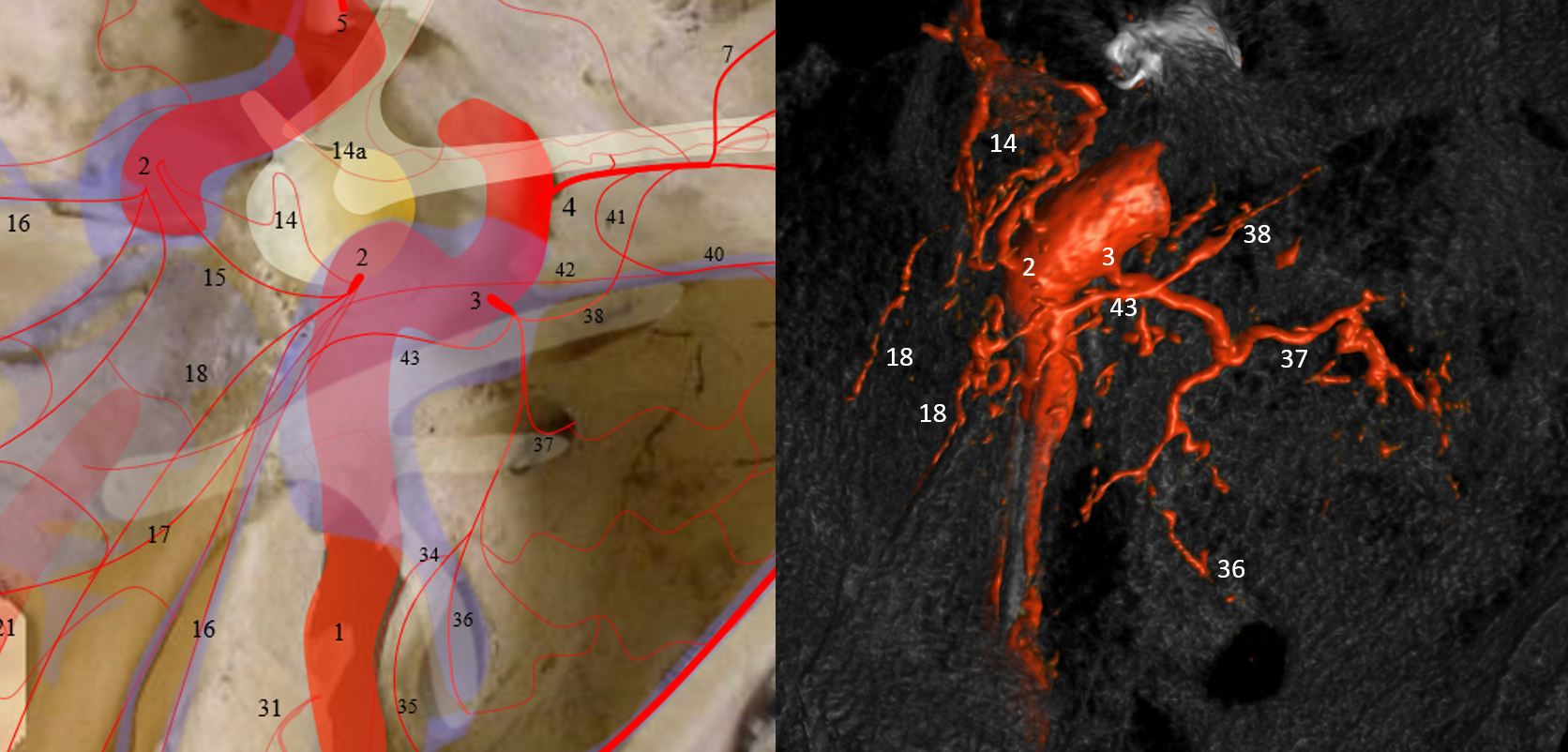
Capsular Arteries of McConnell (CaM) MHT Supply
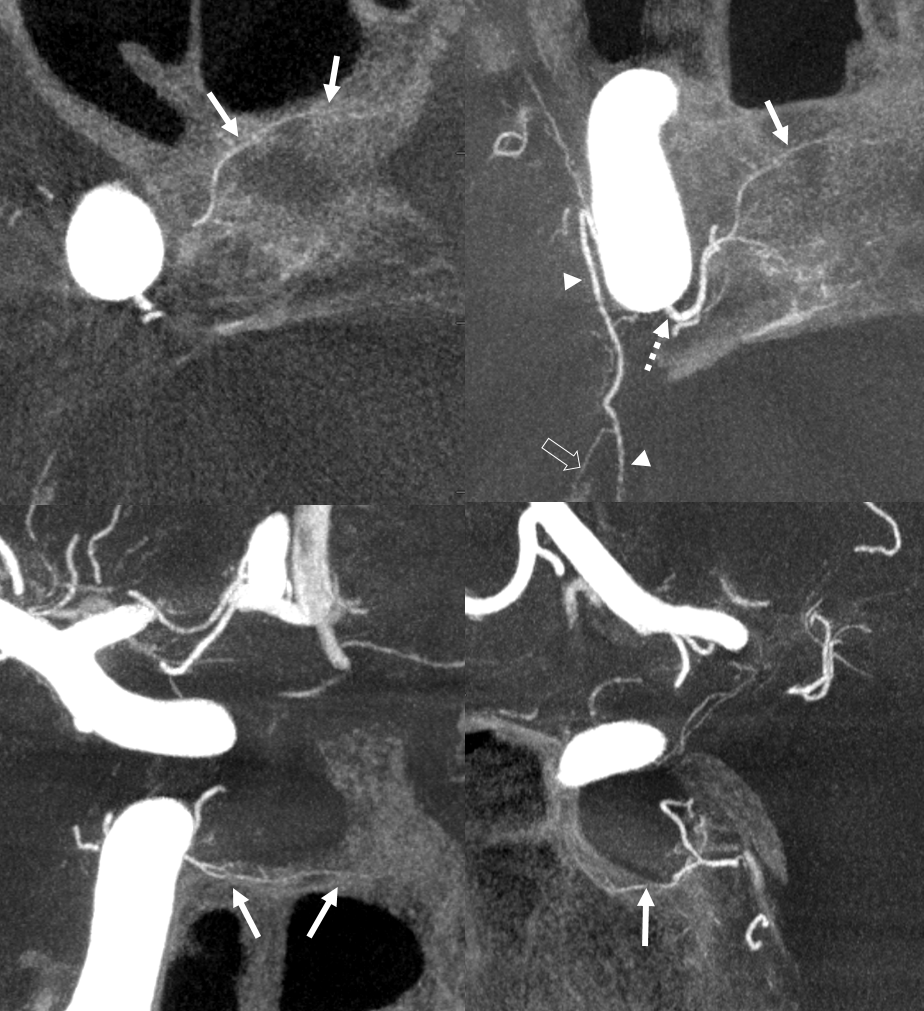
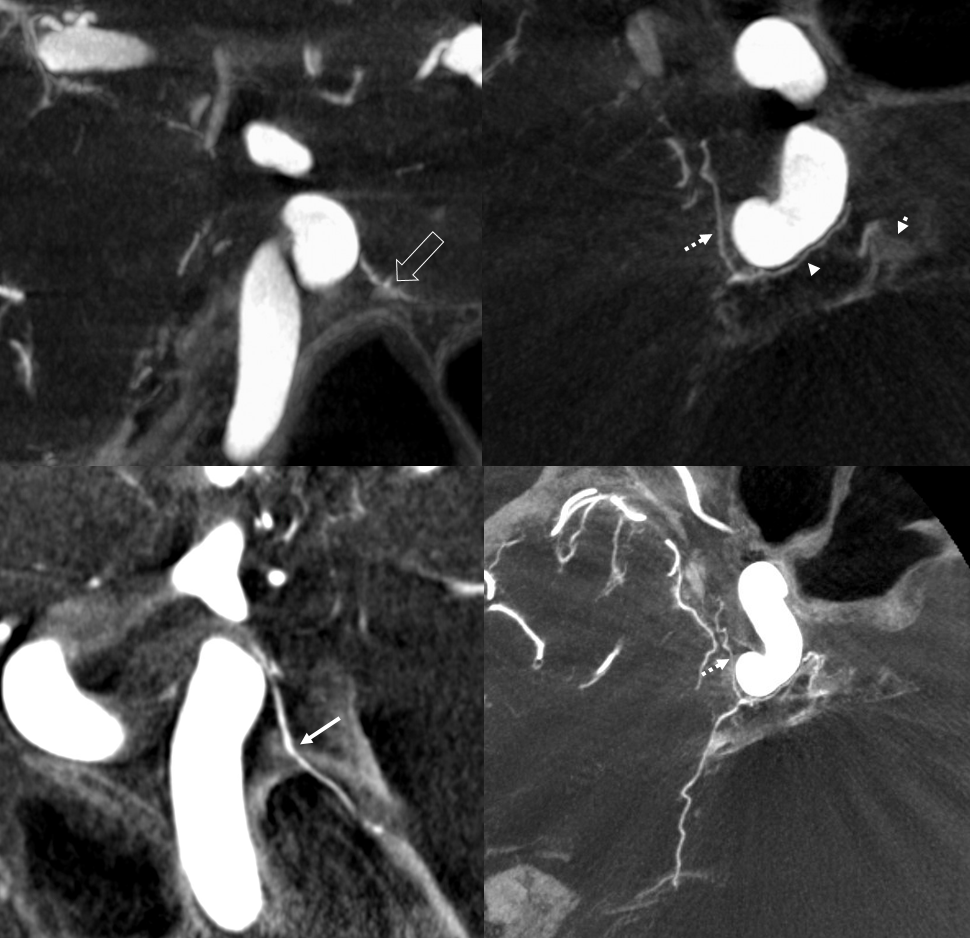
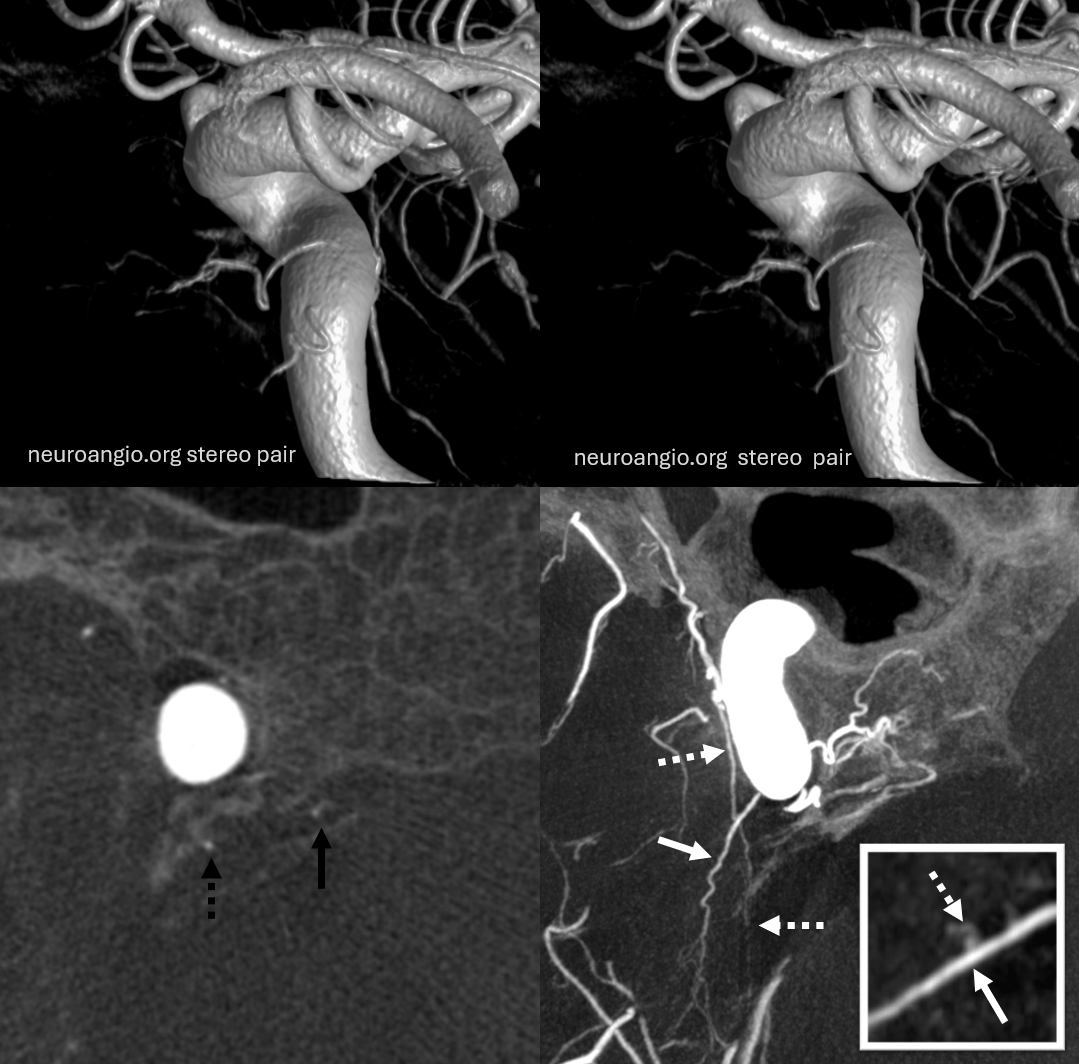
Very rare find. CaMs certainly exist — microsurgically often, and angiographically rarely. Too small to be seen even on modern DYNAs often. Usually these arise from medial wall of the horizonal cavernous carotid segment (not lateral wall, where ILT is from, and not from the MHT). Supply to the dura and bone underneath / around the sella. Not to the pituitary itself. In the case below, these arteries (arrows) happen to arise from the MHT (dashed arrow). Also note artery of the free margin of tentorium continuing as marginal tentorial arcade (arrowheads), and lateral tentorial arcade (open arrow)
Same case in Volume Rendered Stereo Imaging, but different arrows… The inferior hypophyseal artery supplying the posterior pituitary is dashed arrows. The descending clival branch is arrows. The marginal tentorial is arrowheads.
Another Example — its more common than is appreciated in the literature for sure. Solid arrows — osseous supply. Dashed arrows — superior hypophyseal artery
Yet another example of McConnell supply — not as good but still… HOWEVER, note rare intraosseous course of the descending clival branch = arrow. Marginal tentorial branch (hypoplastic ILT territory reconstitution) = dashed arrow. Inferior hypophyseal and posterior pituitary = arrowheads; capsular artery of McConnell = open arrow upper left image.
For the rare exception of McConnell arteries supplying the posterior pituitary, see McConnell page here and see image below

Pituitary Gland Visualization
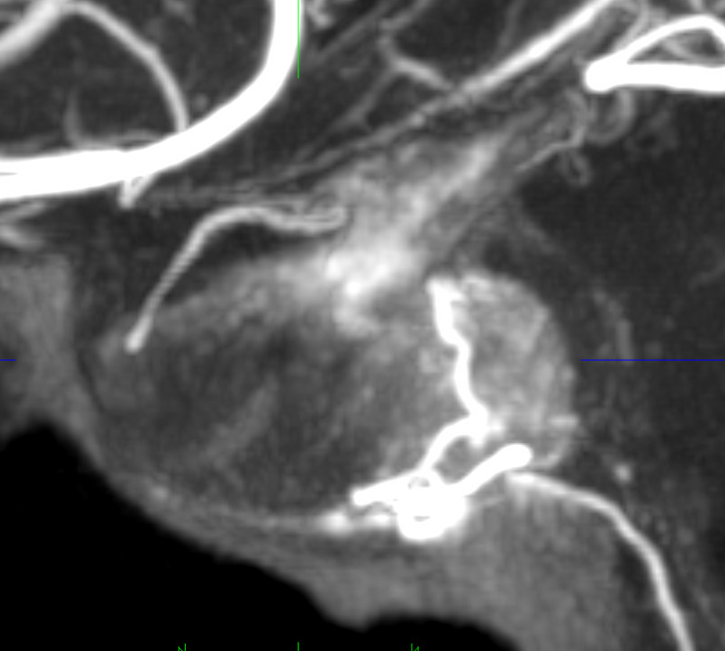
Sagittal MIP images are excellent for the pitutiary. Look at this beautiful cross-section. The posterior pituitary is supplied by the inferior hypophyseal, anterior by the superior hypophyseals going to the stalk.
Another example
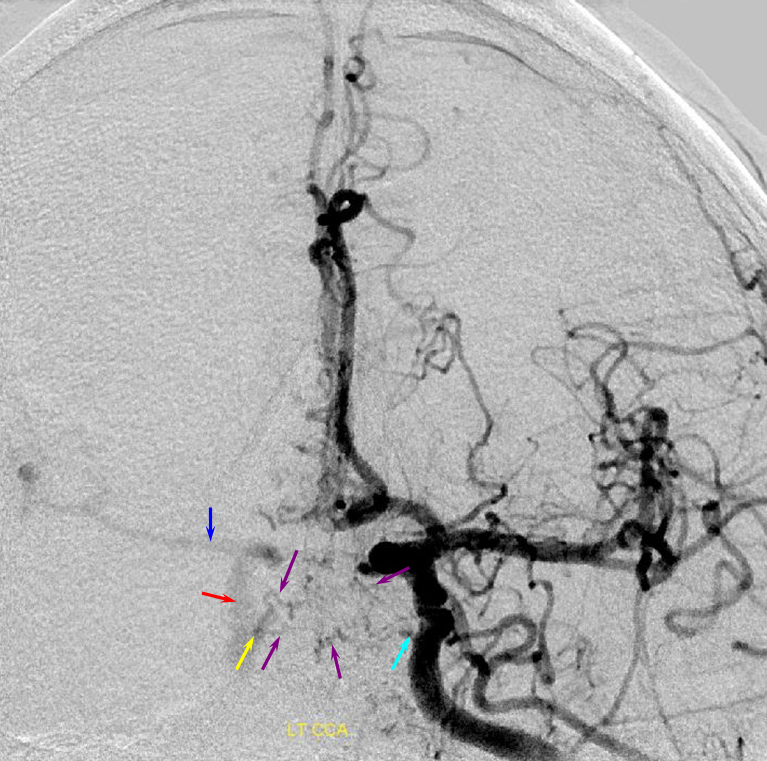
Here is a throwback to the old days — an analog 2D-DSA image
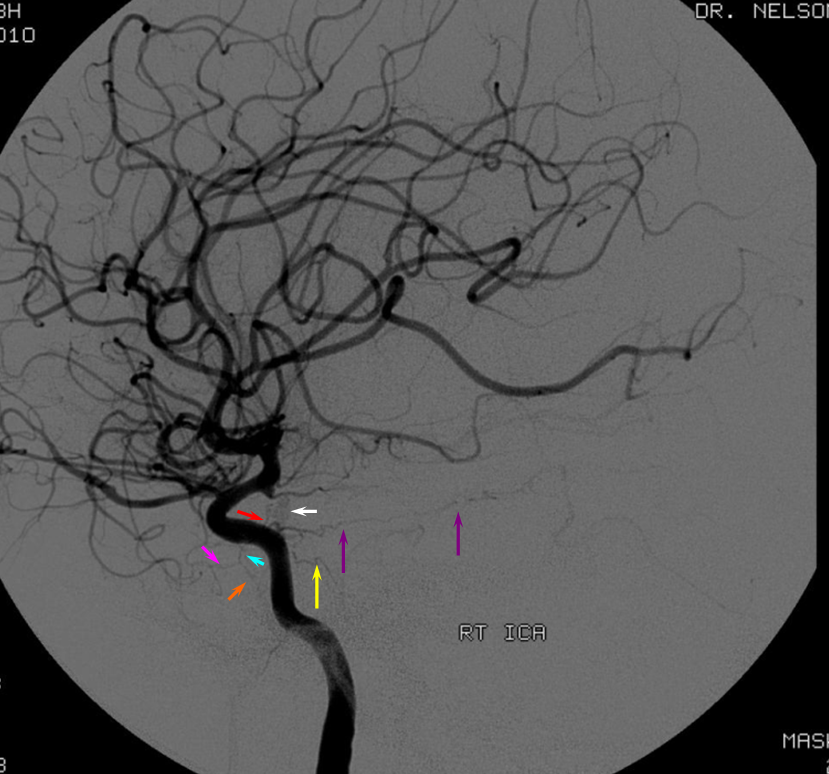
Red= inferior hypophyseal, white=pituitary blush; purple = marginal tentorial; yellow — descending clival (medial or lateral); blue = ILT; purple = anteromedial / rotundum branch; orange = ovale / spinosum branch.
Foramen Lacerum Branch
Rare. The carotid branch of the ascending pharyngeal artery is better known as the superior division pharyngeal trunk of the AP “dangerous anastomosis” with the ICA. The less common branch is the MHT origin lacerum — it courses downward along the ICA into the lacerum
Supplies the Free Margin of tentorium. Classic origin is from MHT — however in our experience it more often is supplied by the ILT — via that same connection (42). Here is a classic 2D-DSA image — note the artery continuing upward into the inferior falx. Why? You think about it.
Lateral (top) and AP (bottom) images of a patient s/p left pterional craniotomy for attempted clipping of an ophthalmic artery aneurysm. The surgery was aborted. The MMA has been sacrificed during the craniotomy. The marginal tentorial arcade is secondarily enlarged and now assumes supply of the falx cerebri (purple arrows). Notice the upward course of the marginal tentorial, following the incisura. The lateral tentorial has a more straight or downward-pointing course on the lateral following the course of the petrous apex, which can be well seen on the native images. Also notice, incidentally, the anteromedial branch of the ILT (red) which is participating in supply of the orbit. Blue — ophthalmic artery.
Circa 2010 3D-DSA of the same
More often than MHT, marginal tentorial origin is from ILT (again, via that 17/42/43 arcade — beige oval). See below. The highly developed marginal tentorial exends to the artery of the straight sinus (yellow arrow). The incisura is outlined by dashed orage line.
Falcotentorial Fistula
The marginal tentorial usually participates in supply of falcotentorial fistulas. Note its origin from the ILT, not MHT below. See also dedicated examples on the “Case Archives” page
Lateral (Basal) Tentorial Arcade
Extends along petrous ridge within the dura of the Superior Petrosal Sinus. It is truly an arcade rather than a single vessel. Usually only seen in setting of disease such as Sigmoid Sinus Dural Fistula (see Case Archives page for many examples).
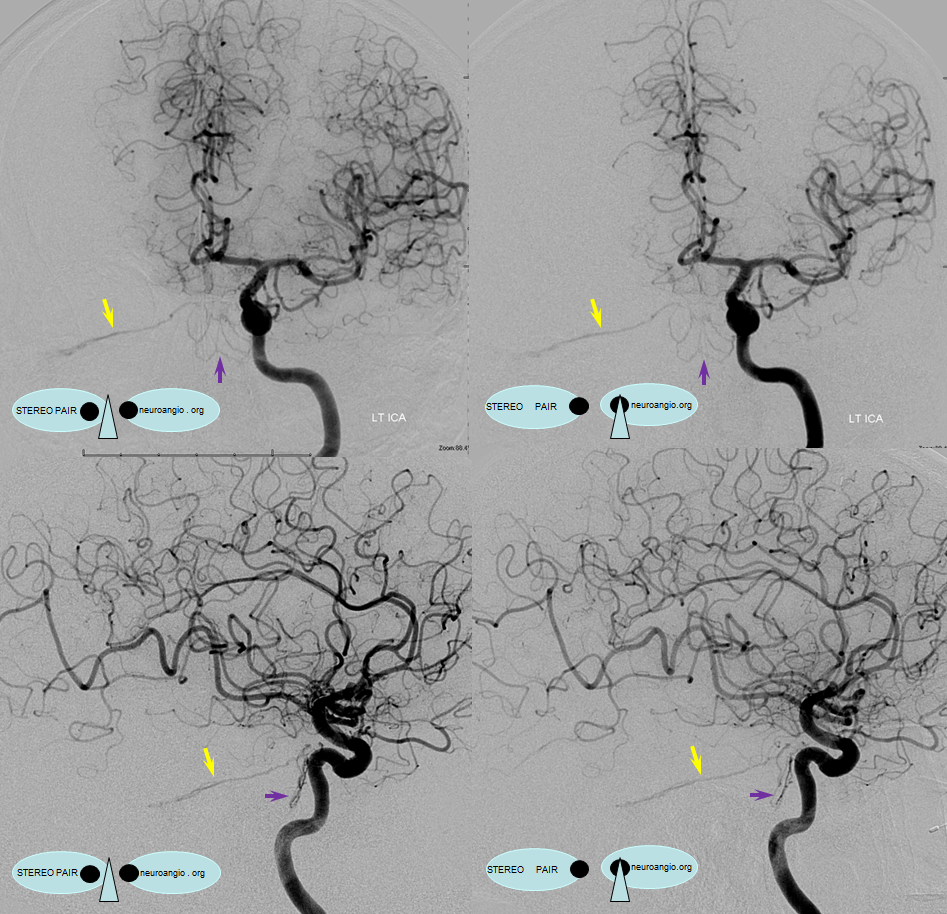
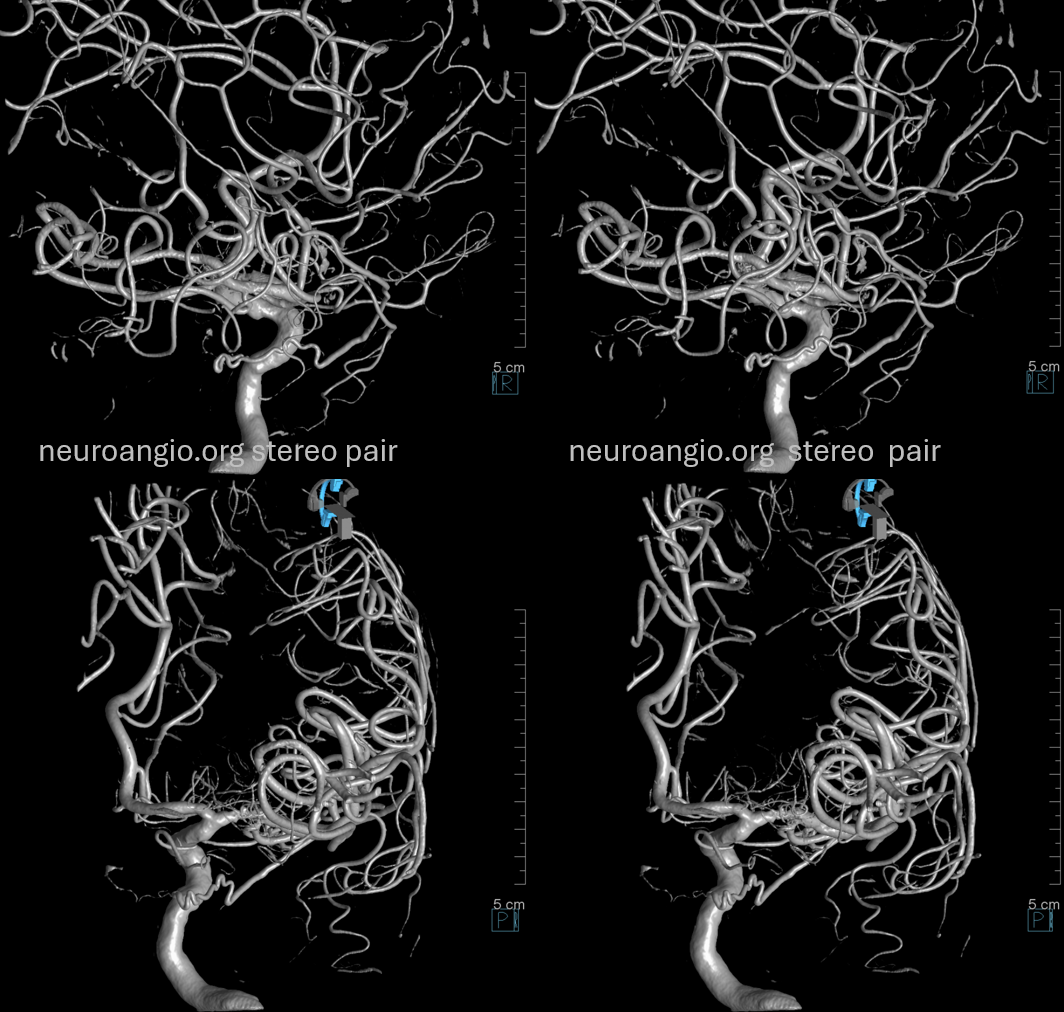
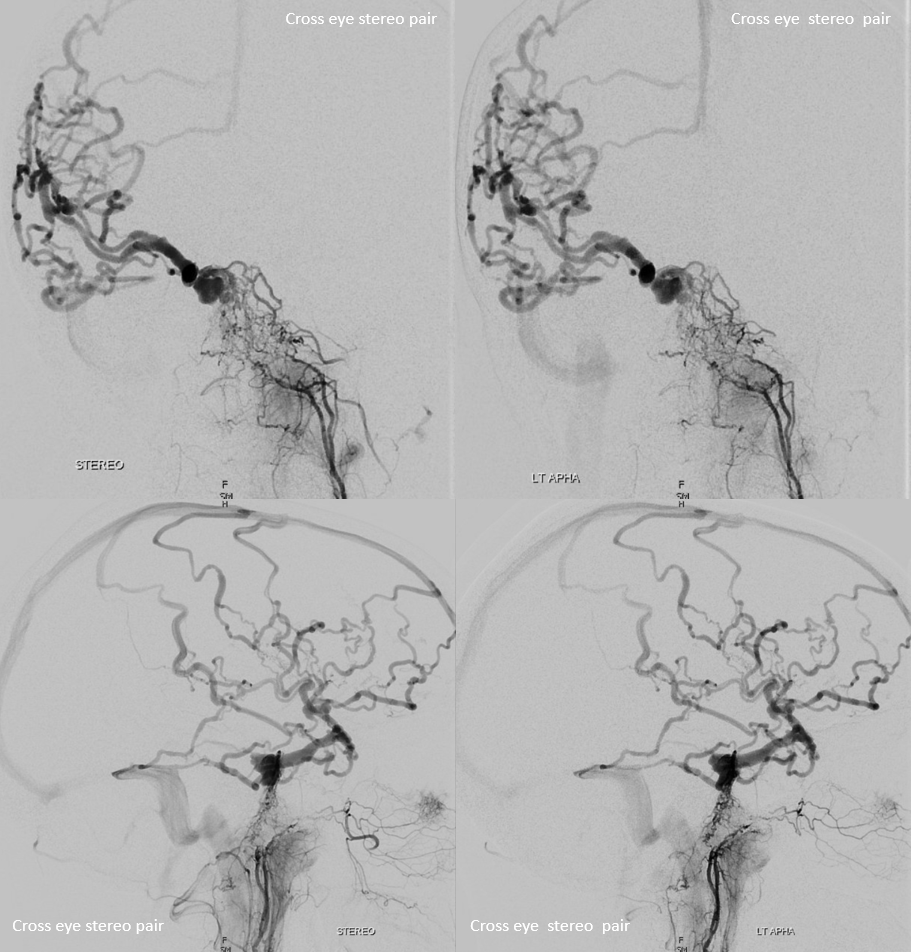
It is curious that while the marginal tentorial artery most often is connected to the ILT, the lateral tentorial arcade is pretty much always an MHT connection. They really are i believe embryologically distinct. Below is an example of this — the two actually cross… Marginal tentorial (dashed white arrows) ILT origin and basal tentorial (white arrows) in lower right image. Inset shows the point of crossing. Also notable are medial (solid black) and lateral (dashed black) clival branches and separate origins of the clival and inferior hypophyseal branches (top stereo pair). What is the very small branch at 1 o’clock relative to the carotid artery circle in the lower left image?
Below are RT ECA and RT ICA injections — yellow arrows point to the lateral tentorial arcade (supplied by MHT, MMA, occipital) in a sigmoid fistula case. Note the descending course of the arcade on lateral views — as opposed to the gently upturning lateral projection of the marginal tentorial.
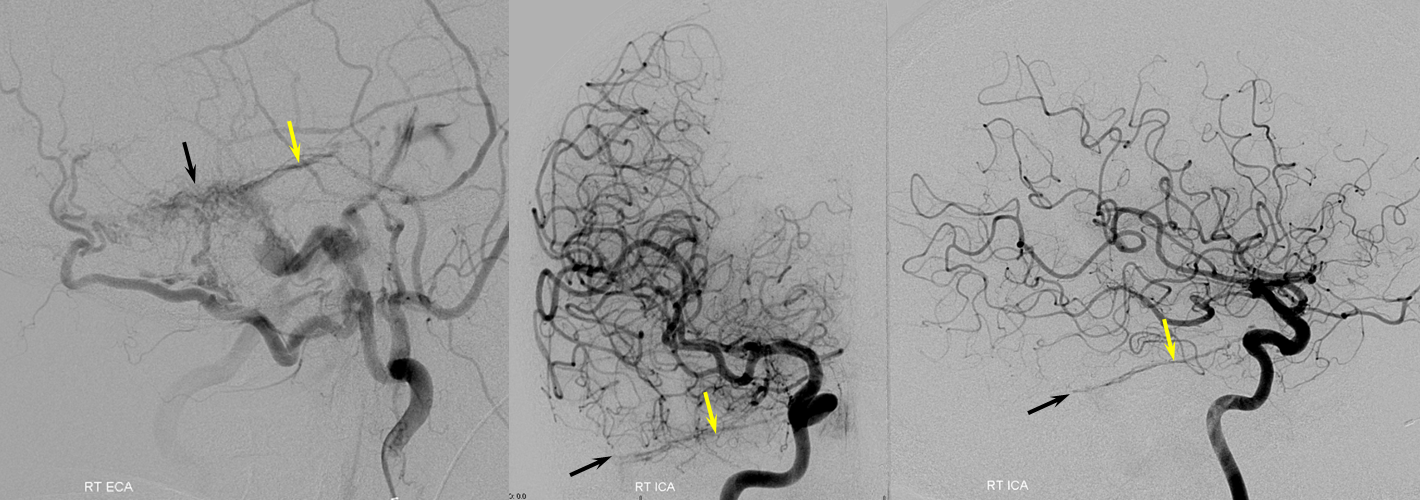
Beautiful vintage stereos of the same case. Left ICA injection shows LEFT MHT contribution to the same arcade via MHT-MHT interclival anastomoses (purple) — via descending clival branches.
Another case — lateral tentorial arcade and multiple piodural anastomoses involving the MCA and PCA in another sigmoid sinus fistula case
See dedicated “Trigeminal Artery” page for tons of examples. It is an embryonic connection between “anterior” and “posterior” circulations. The trigeminal artery classic origin is the MHT (although of course ILT can do it too, see above). Below are a few examples. Remember BALANCE — the trigeminal is in balance with the PCOM. One can have large PCOM and small trigeminal, or vice versa, etc. This one came with a rare PCOM fenestation also.
The basilar connection is not required — occasionally it will be supplying the AICA territory “only”
The one below came with an aneurysm

Finally, in regard to balance, the “basilar” origin middle meningeal artery (extremely rare) is explaned as a basilar-trigeminal-deep-recurrent-meningeal (17/42/43) – sphenoid-ridge-MMA route…
See below
MHT origin of the MMA — Via the same Sphenoid Ridge Branch 3-40-44
Stroke — the gift that keeps on giving. Note posterior/parietal MMA division usual origin and course. See MMA page for discussion of the spectrum.
Descending Clival Branches (Lateral and Medial)
Usually seen on DYNA / High Res Cone Beam CT. Occasionally on angio (see again image below — yellow arrow)
Balance again!
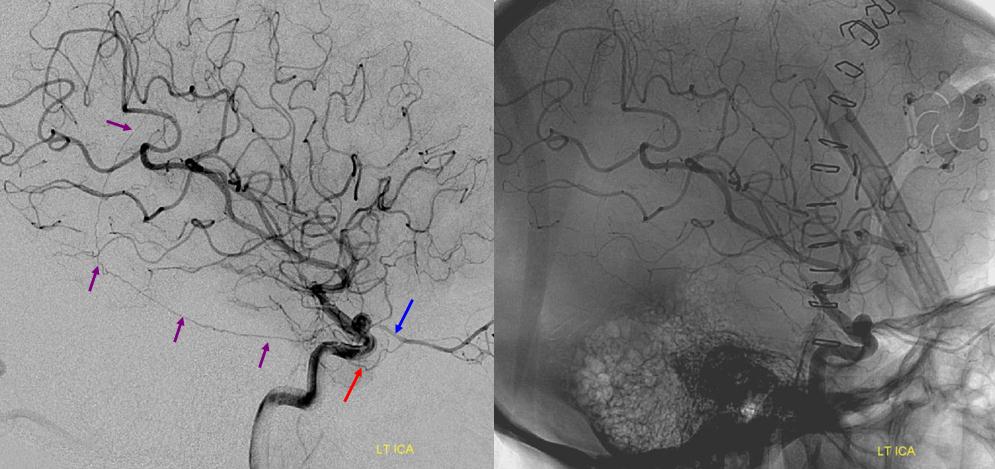
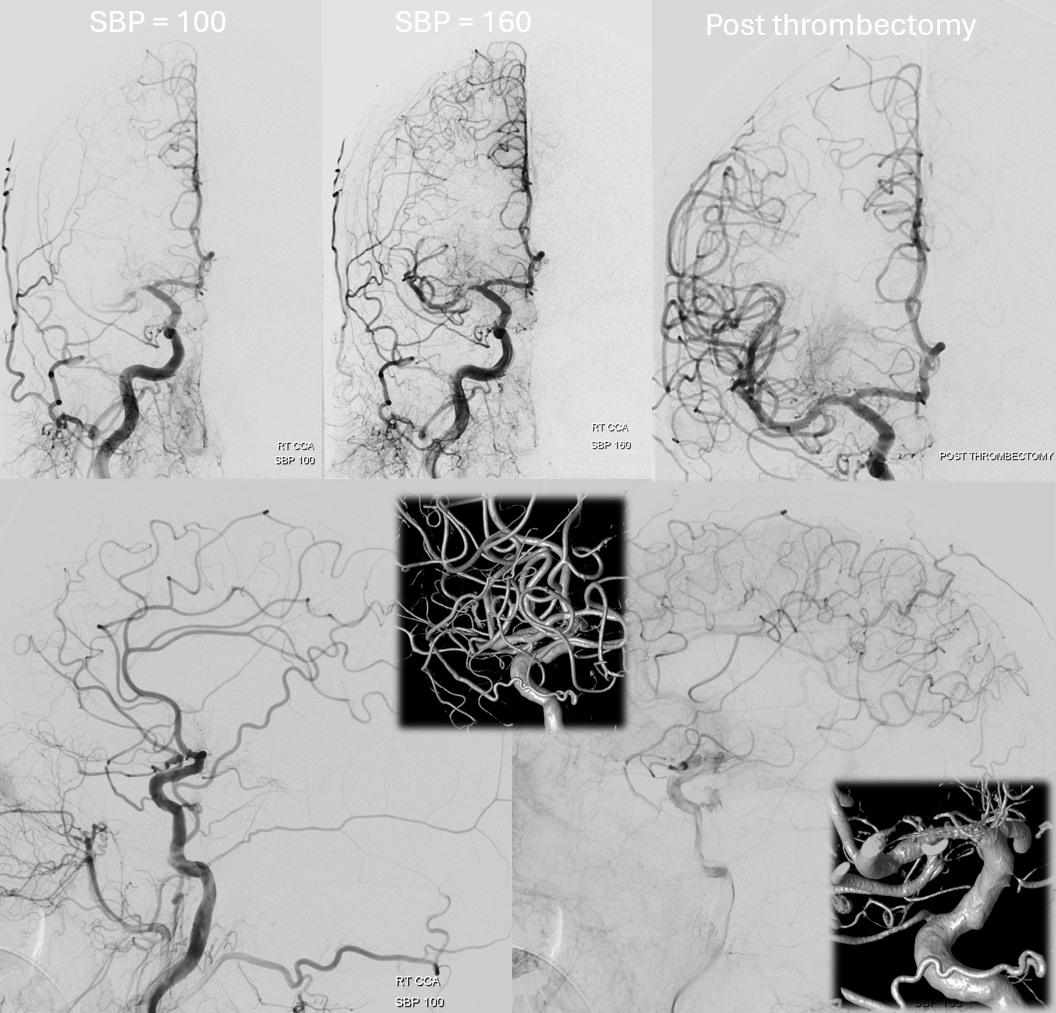
See case below. Top images demonsrate and AVM pre and post embolization. Bottom row stereo pair shows better visualization of the MHT and ILT branches following ipsilateral craniotomy for AVM resection, which involved MMA sacrifice. Blue=MHT descending clival branches; Light blue=marginal tentorial arcade; Purple = ILT
The same family of arteries is often seen from the ascending pharyngeal — contributing to supply of Cavernous Sinus Fistulas (See Case Archives Page for examples) and meningiomas. Below is a “normal” case of an ascending pharyngeal injection — showing Clival (arrows) and “carotid branch” (dashed arrows) ascending pharyngeal connections with the MHT.
Vintage images
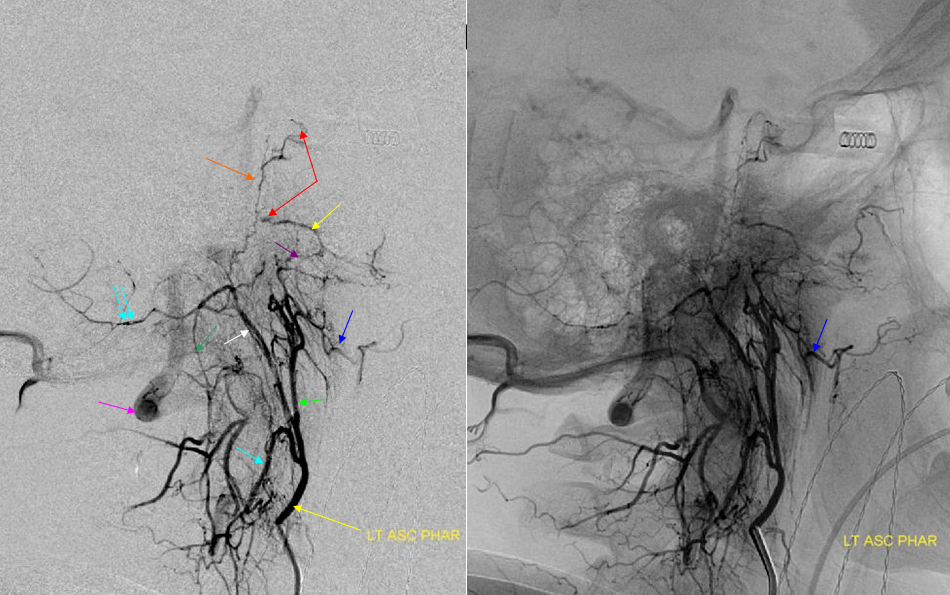
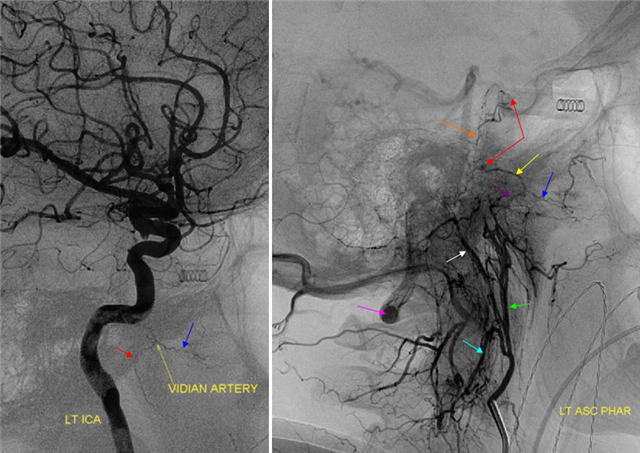
Latearal (below) views of an ascending pharyngeal injection demonstrate a number of very instructive findings. The pharyngeal trunk (green) superior branch anastomoses wtih the ascending palatine artery (blue) and the vidian artery (yellow) which opaficies petrous ICA with a small blush (red). The neuromeningeal trunk (white) hypoglossal branch shows prominent ascending clival branches wich reconstitute the proximal cavernous carotid artery a the level of the MHT with another small carotid blush (red). The descending branch (green) of the hypoglossal division opacifies various components of the odontoid arch (black arrows). A prominent musculospinal branch (blue) reconstitutes the vertebral artery (pink).
With injection of the ICA, identifying some of the same arteries
Clival Branches Dural Cavernous Sinus Fistula
Very frequent contribution and, occasionally, a transarterial embolization route. Below are stereo views of ascending pharyngeal artery injection. Full case here
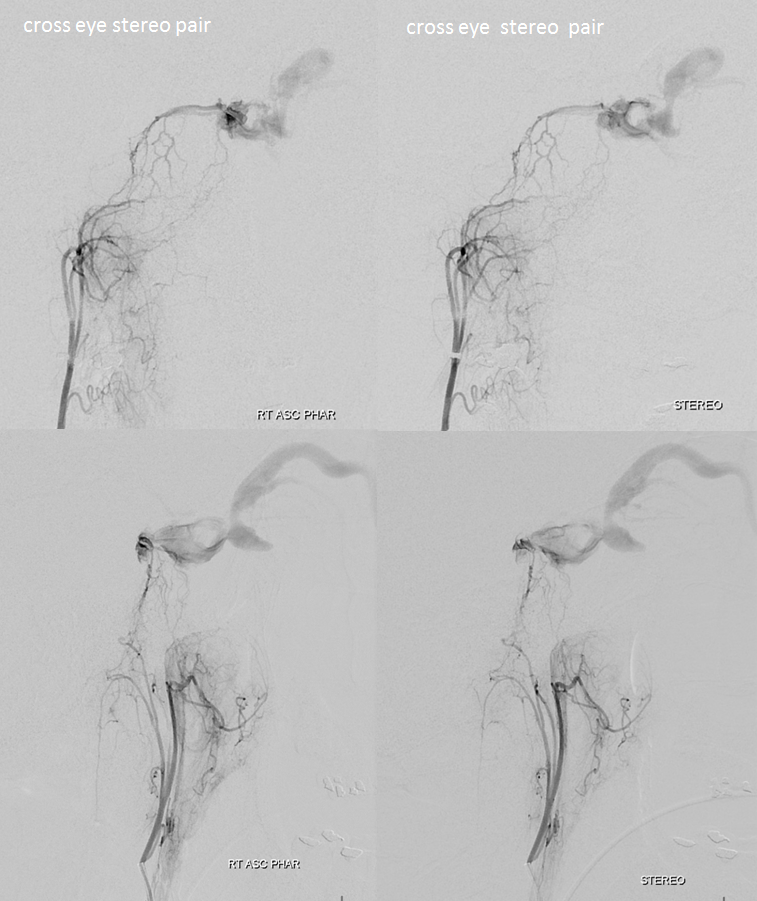
Fistula site — black arrow. Posterior clival arterial arcade — white arrow. Hypoglossal division — black arrowhead; transossesous branches of the pharyngeal division — white arrowheads; jugular division — dashed white arrows. Clival branches are not labeled — find them — 🙂
DYNA CT — same arrows
Another Example
Fantastic cavernous sinus dural fistula case here and also on www.youtube.com/neuroangio — with analysis of the case “To See a World In a Grain of Sand“. Innumerable clival arcade branches supplying a cavernous sinus fistula.
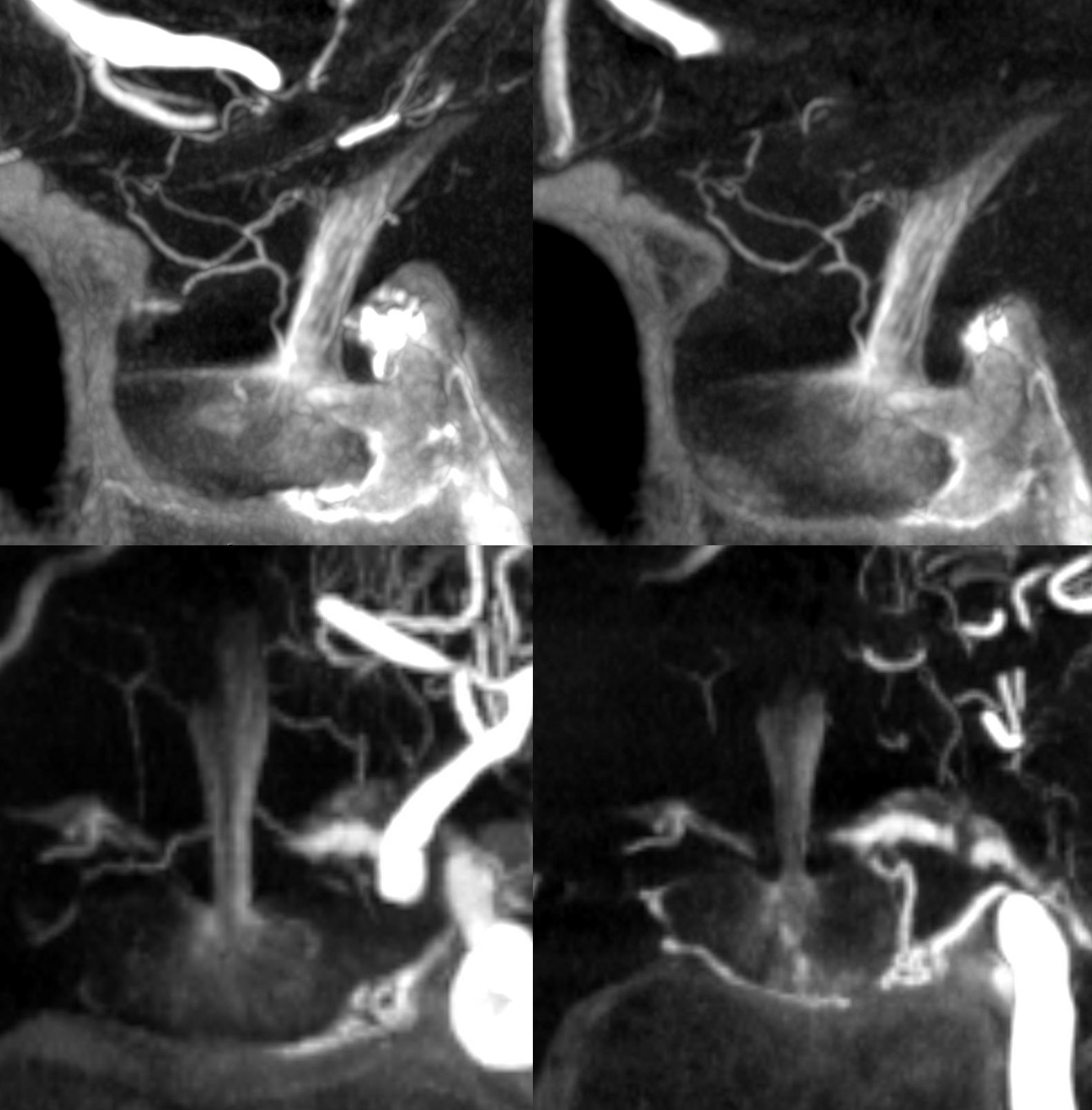
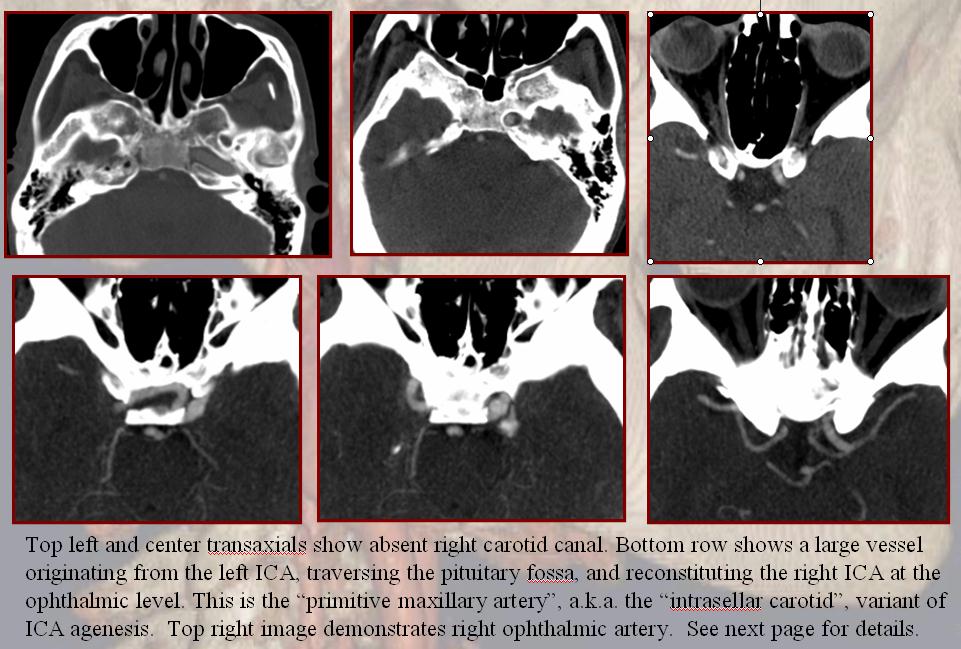
This is an embryologic concept — the MHT being a “remnant” of the primitive maxillary. The primitive maxillary is an artery which connects the right and left developing ICAs at the MHT level — basically and MHT-MHT anastomosis.
The left and right inferior hypophyseal counterparts anastomose with each other normally and supply the pituitary gland as above. In cases of carotid agenesis involving the petrous segment, the carotid artery can be reconstituted via the contralateral carotid thru this primitive maxillary anastomosis, resulting in a bizzare large vessel traversing the pituitary fossa connecting one carotid artery to the other. I believe there are a lot of unanswered questions in the embryology neck of woods here, but that’s the official theory. Here is an old CTA example
Below is one that seems clearly related to the superior hypophyseal arteries (not inferior hypophyseals) — see what I mean about the embryology questions…
PATHOLOGY — MHT INVOLVEMENT IN DISEASE
Mainly this concerns dural fistulas and meningiomas. Many examples can be found on “Case Archives” Page.
Catheterization of MHT for preoperative particle embolization of meningiomas is something we do often. It is safe and effective in our experience — but this is not to be done if one is not familiar with technique…
Cross-sectional Imaging
MHT, ILT, superior hypophyseals — none are seen on MR or CT unless enlarged by a pathologic process at this time. Below is a terrible petroclival mening
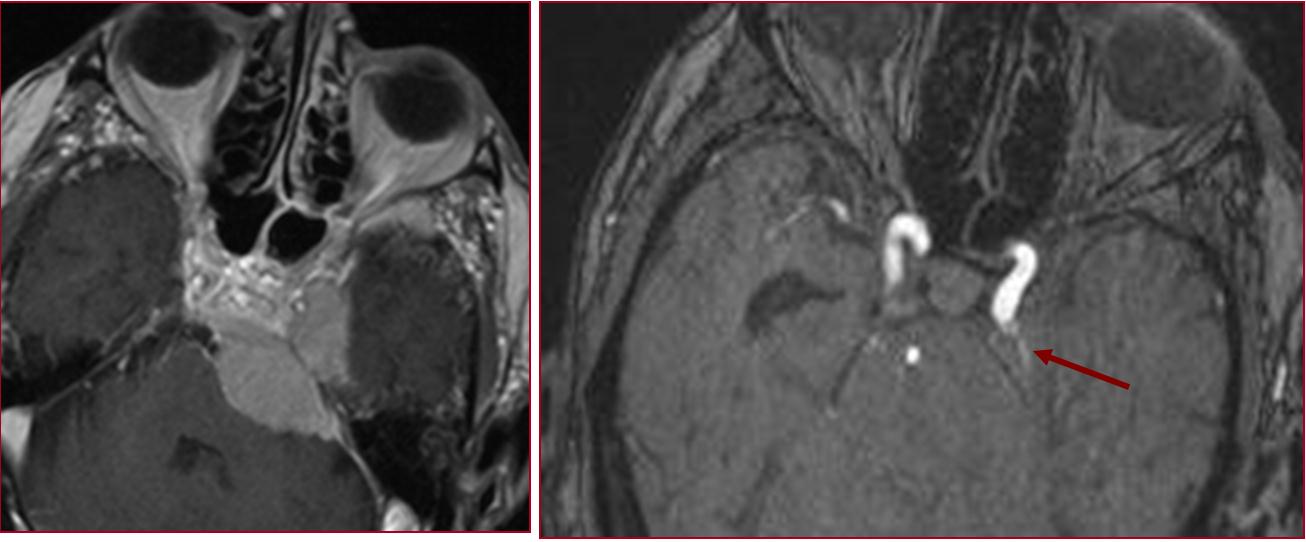
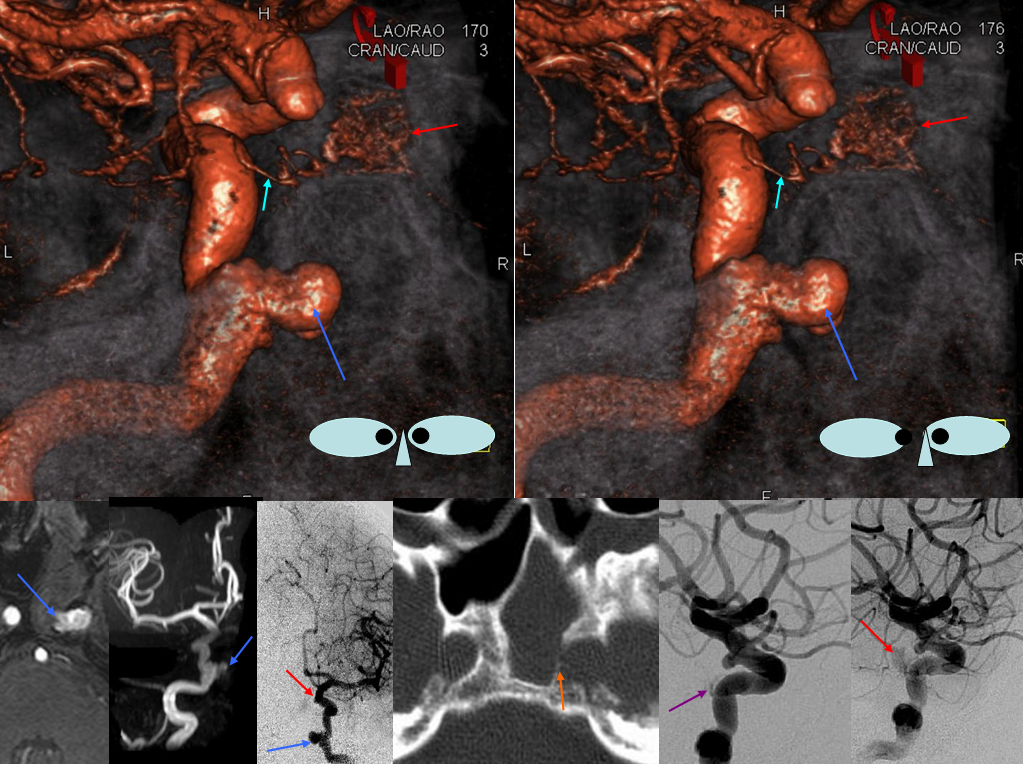
And a terrible petrous apex fistula…
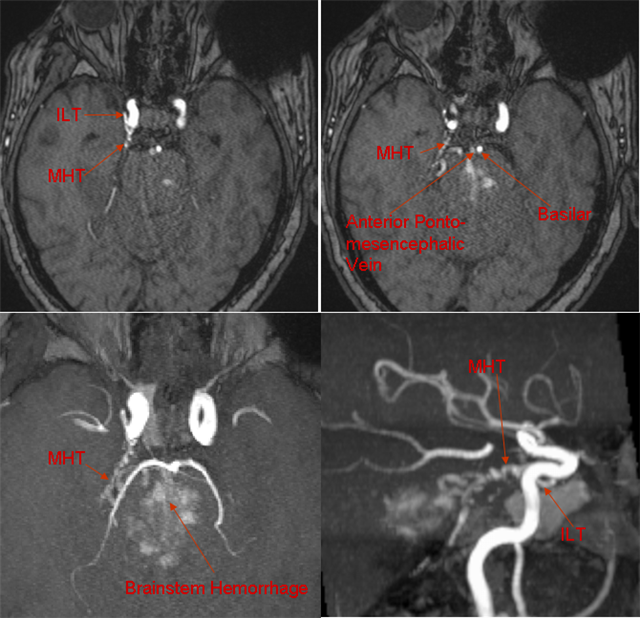
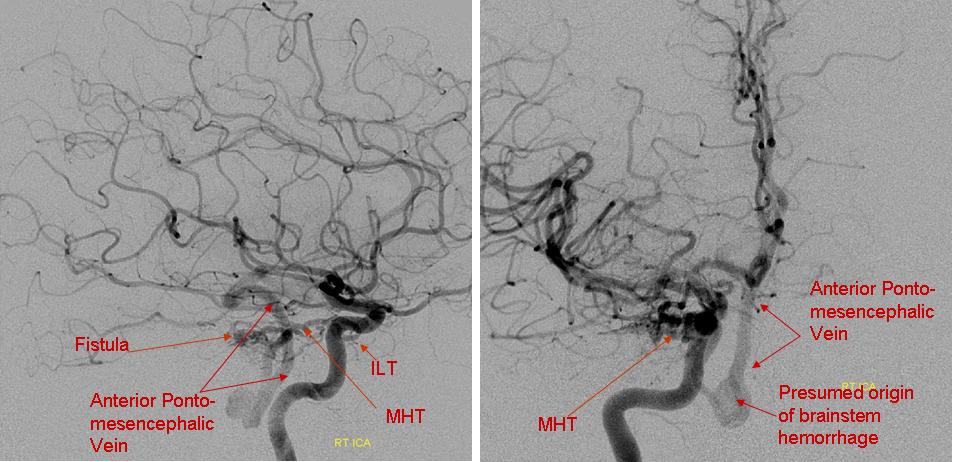
Angio below — hemorrhage into brainstem from congested anterior pontomesencephalic vein
MISCELLANEOUS
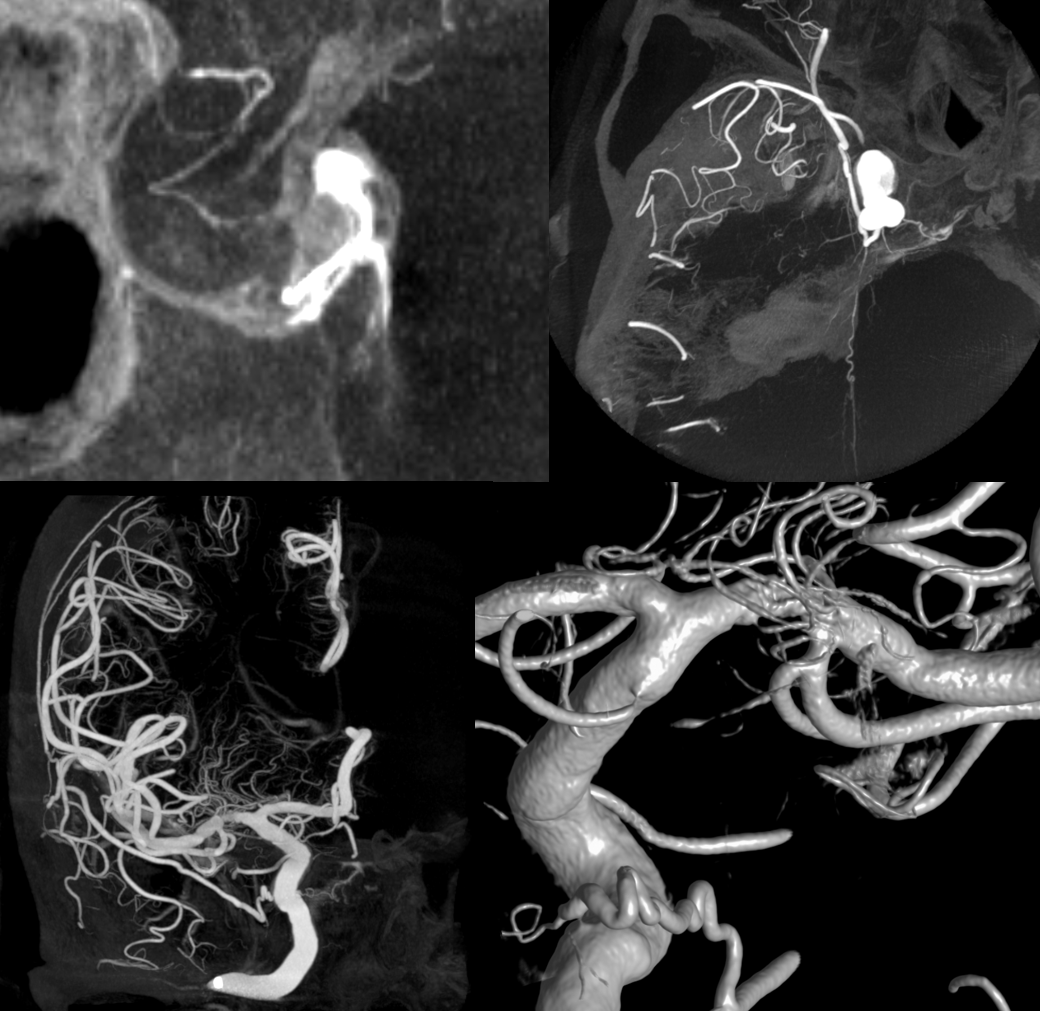
Hey, this is not a book… no limits to what we want to show here. Below is an old nice case of sphenoid sinus dehiscence (infection, malignancy) and epstaxis due to carotid pseudoaneurysm. Inferior hypophyseal (light blue); pituitary blush (red); pseudoaneurysm (blue); bony dehiscence (orange). Treated with bypass and sacrifice.
LIKE IT? Good, study more… and send good cases to neuroangio@neuroangio.org