
Number 9 below

R and V below
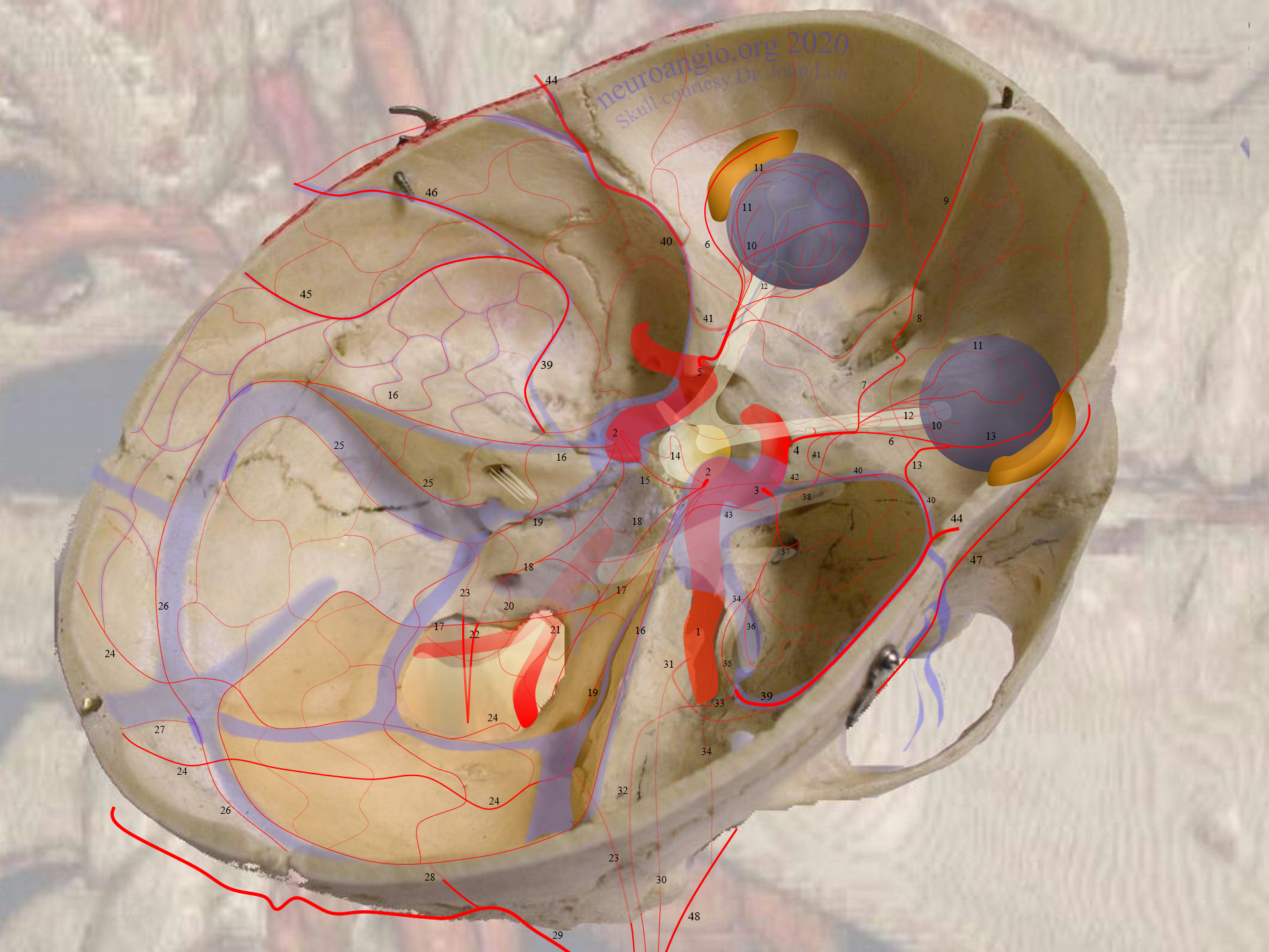
Location: Arterial network (usually one macroscopically identifiable vessel) in the dural wall of the distal superior sagittal sinus.
Supply: Usually by one or both ophthalmic arteries via the anterior (less likely posterior) ethmoidal arteries. Typically one of the ophthalmics is the dominant one.
Territory: Parasagittal / high convexity dura — in proportion to supply of same by the Middle Meningeal Arteries
In balance with: Most commonly the middle meningeal arteries. Usually supplies more one side than another — and is more connected with same MMA as preferential side of supply
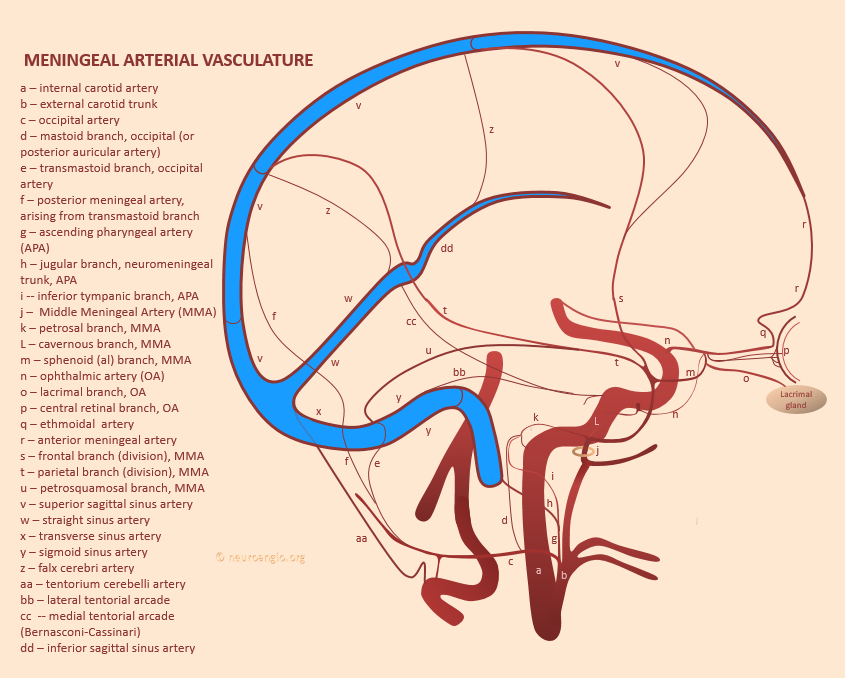
This network is part of a global network of arteries in the walls of all major sinuses. See Diagram above and “Meningeal Vessels” as well “Intrinsic Dural Arterial Vasculature” pages
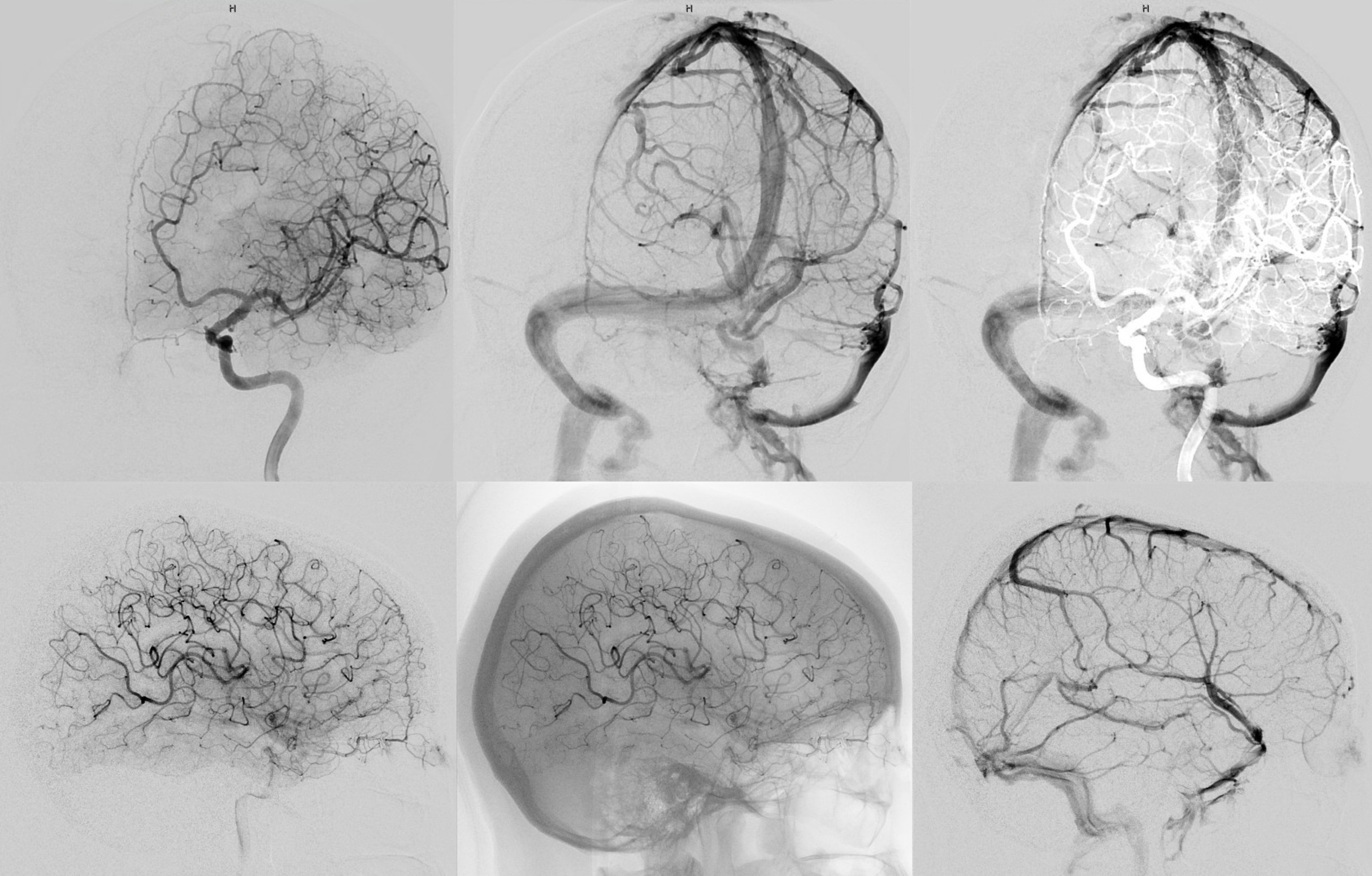
Usual look
Prominent anterior meningeal due to prior pterional craniotomy interrupting the MMA — hense its compensatory hypertrophy to supply the lateral convexity — BALANCE. Nte very cool motion of the clip due to brain / vessel pulsation at the moment of xray exposure.
Prominent anterior meningeal just because. No craniotomy or other pathology
Clinical Significance — Occlusive Disease
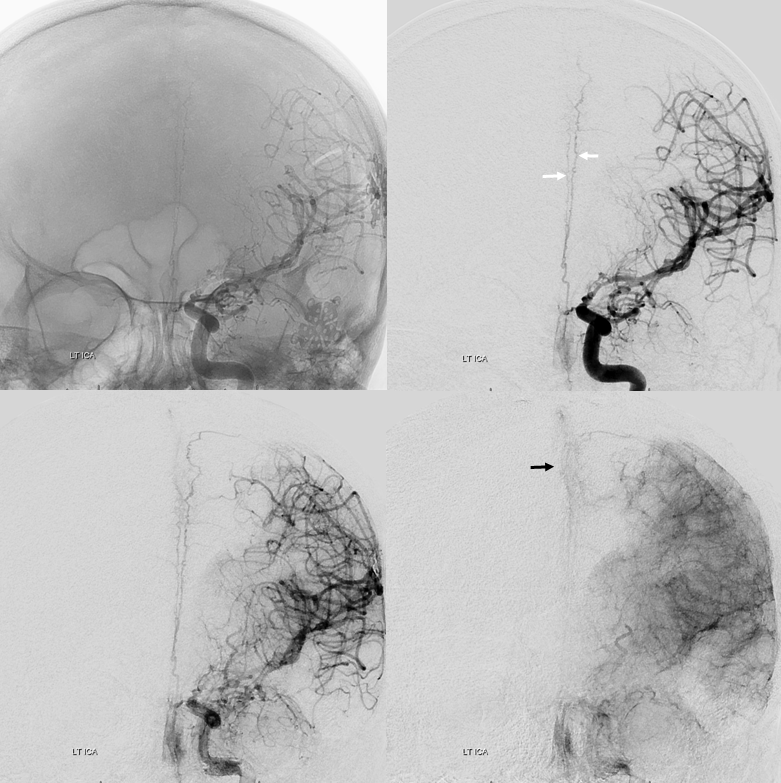
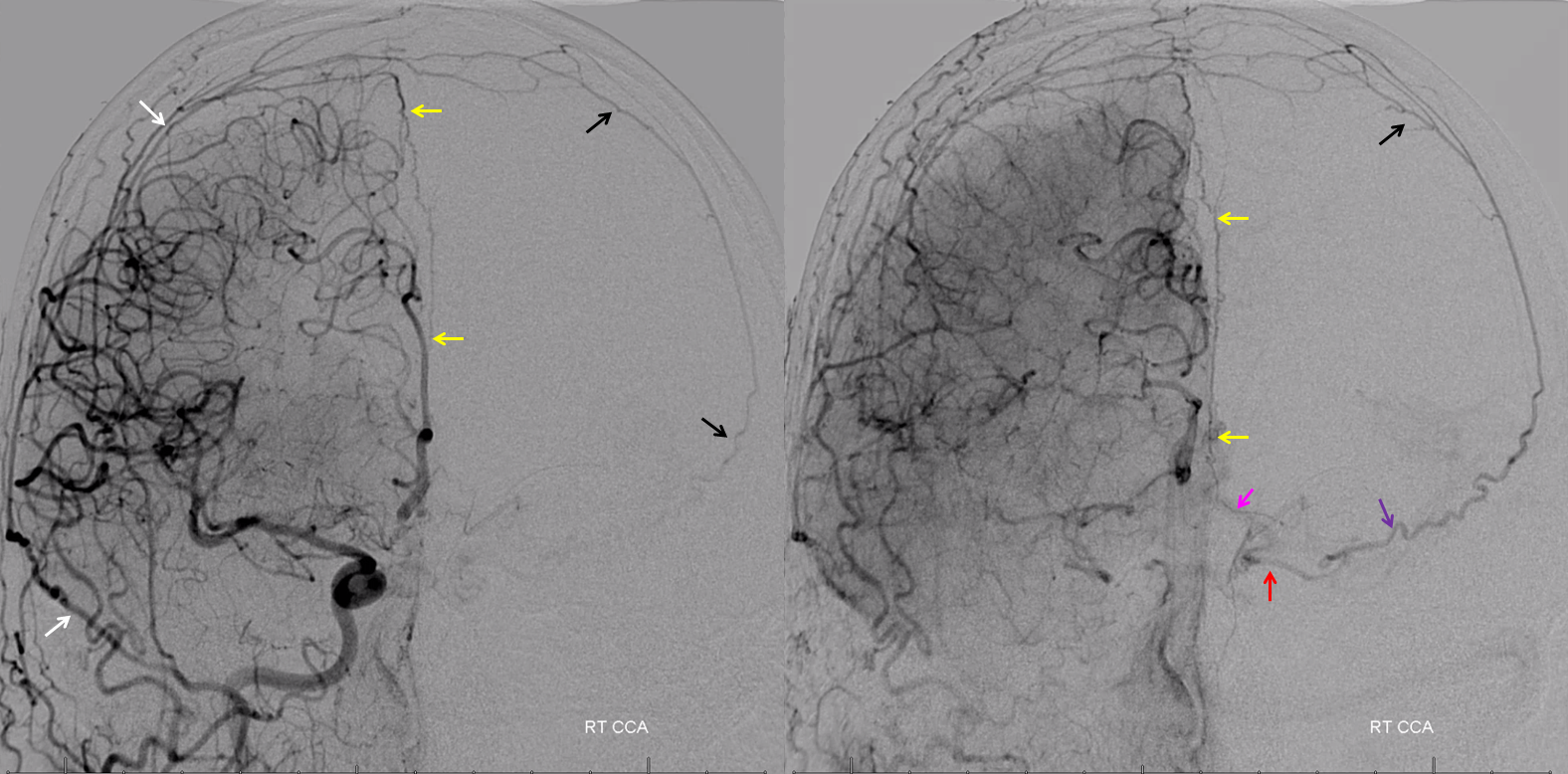
Patient with left cervical ICA dissection
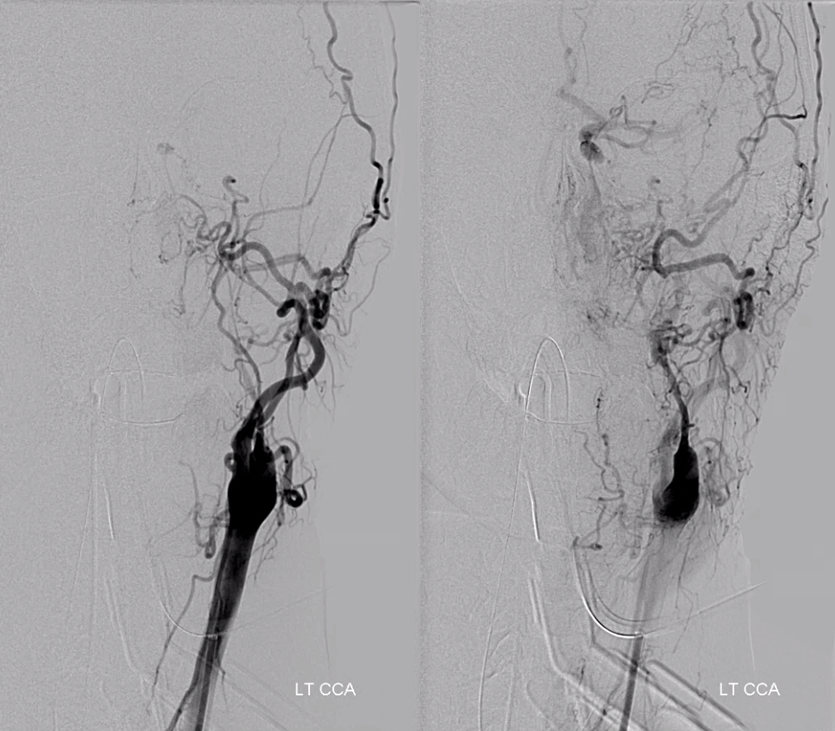
Collateral reconstitution of the left ICA is provided by right MMA (white arrows) to left MMA (meningo-ophthalmic, black arrows; sphenoidal branch -purple arrow) to ophthalmic artery (red arrow)! Notice anterior meningeal branch (yellow) reconstituting ophthalmic via the ethmoid artery (pink arrow). Case courtesy Dr. Eytan Raz
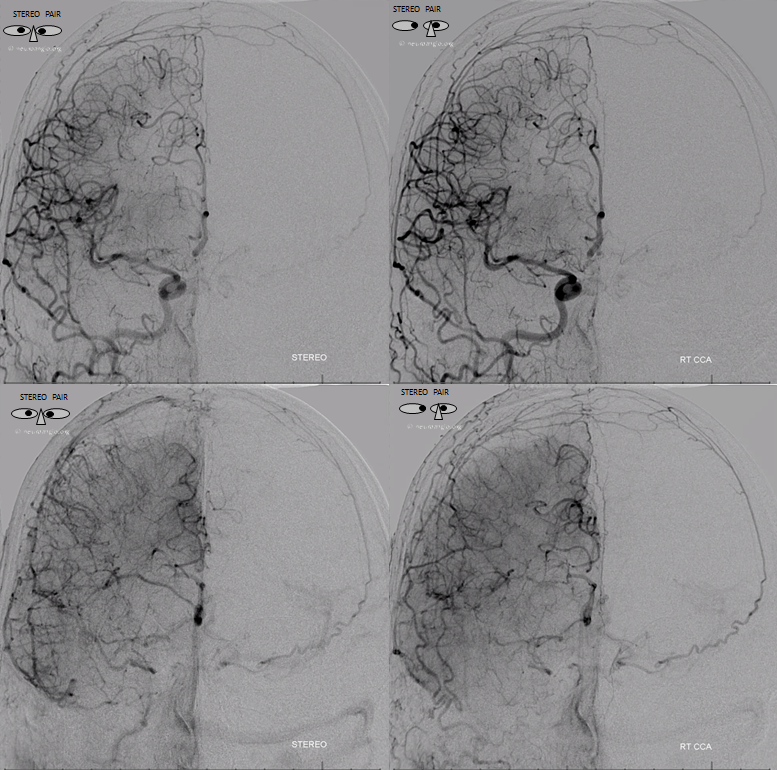
Stereos


Clinical Significance: Ethmoidal Fistulas
Very important point — anterior meningeal arteries often contribute, in retrograde fashion, via the MMAs, to supply of the ethmoidal fistulas. This can be used as a relatively safe transarterial access route — certainly safer than ophthlamic catheterization (now, if you are interested in that, see cases HERE and HERE)
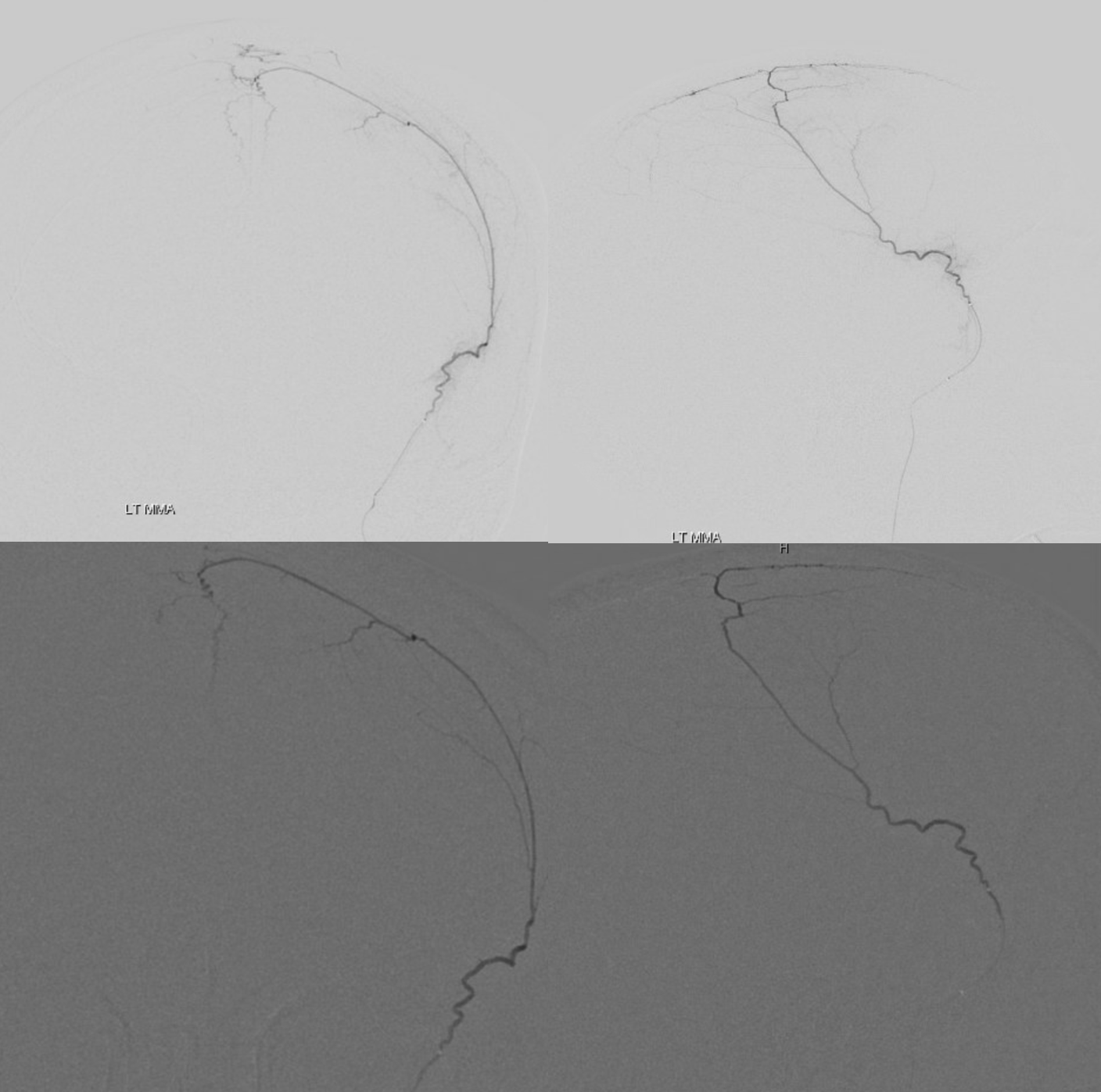
Example 1: Complete controlled embolization via MMA -anterior meningeal route. Full case HERE.
Lateral views
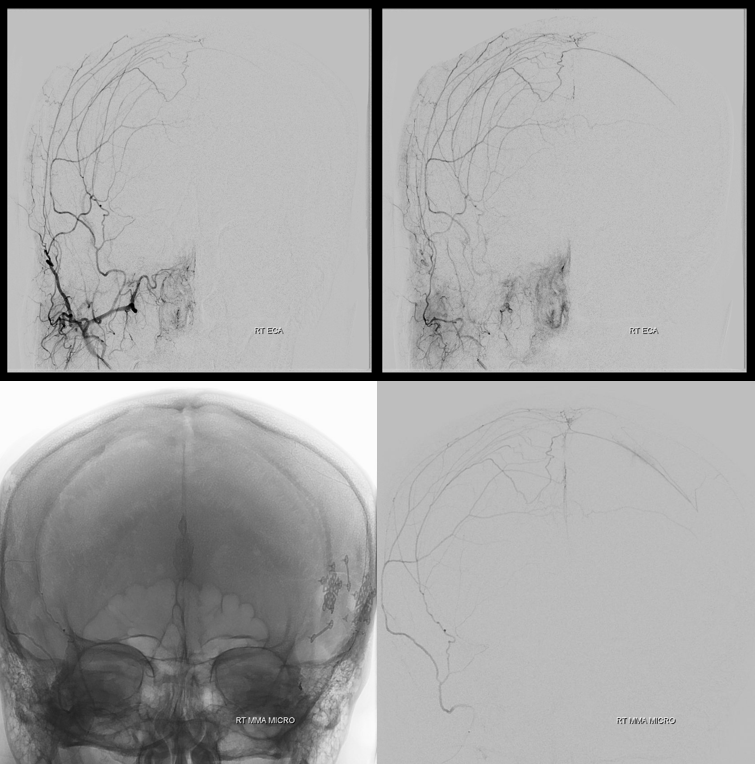
Example 2: Ethmoid Fistula supplied by Superior Sagittal Sinus Artery (white), opacified via frontal branch of MMA (black). Full case is here — treatment included
![]()
Clinical Significance — MMA Subdural Embolization
Another important clinical aspect here. The anterior meningeal artery an important source of collateral supply to the dura after MMA embolization (for subdurals), together with the contralateral MMA. When bilateral MMA embo is done, it is usually THE prinicipal reconstitution route. One of the advantages of using liquid embolics is potential to embolize the anterior meningeal via MMA convexity collaterals. This enhances the probability of success, since it reduces or eliminates an important reconstitution pathway.
Very often, this is possible with dilute nBCA, from a wedge position in an MMA convexity branch. Alghough the anterior meningeal is not often visible during test injections, glue injection will often penetrate into the accessory meningeal. Care is of course important, as it ultimately connects to the orbit. However, the route is usually long and injection can be stopped beforehand. See examples below:
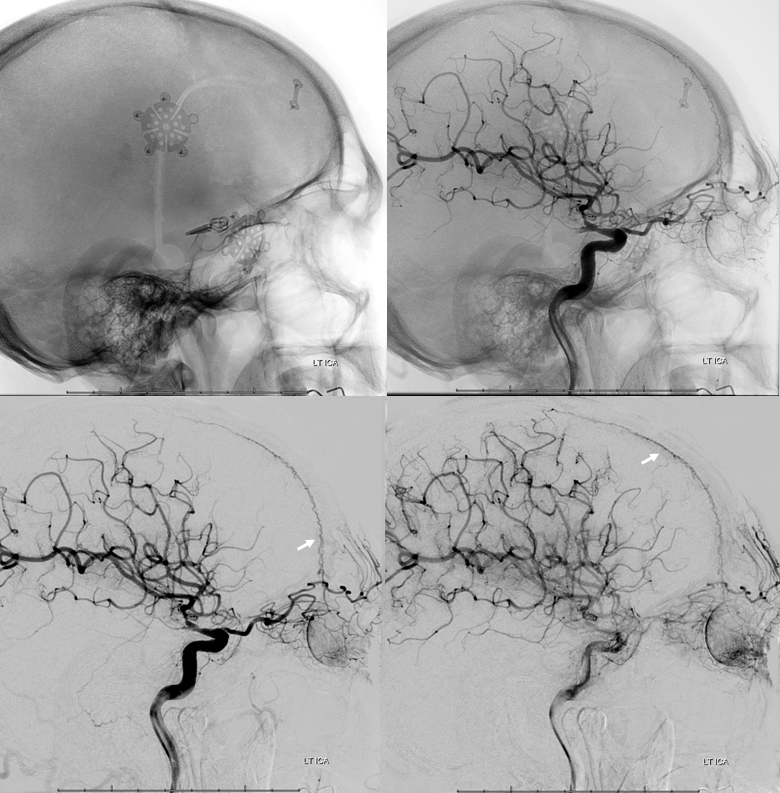
Case 1: LEFT subdural hematoma in setting of prior left pterional craniotomy. Full case HERE
Good cross-midline right to left MMA anastomoses are present
Micro injection wedge position frontal division
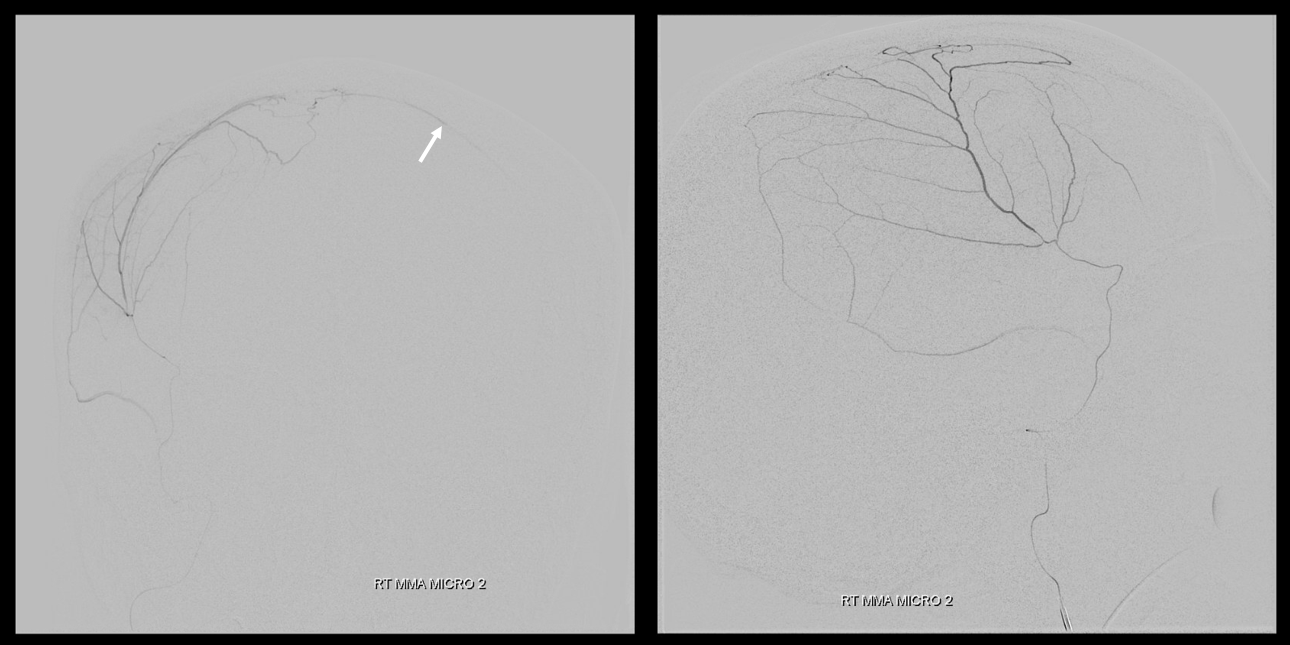
Dilute nBCA:lipidol (1:4) injection — notice, in addition to desired filling of the SSS collateral network and penetration to the left, a frequenly seen major glue filling of the anterior meningeal artery (arrow). This of course is connected, via ethmoidal arteries, to the ophthalmic artery system, and should be watched carefully. However, it is also important to fill this branch so as to shut down this major collateral reconstitution route to the target left dural convexity
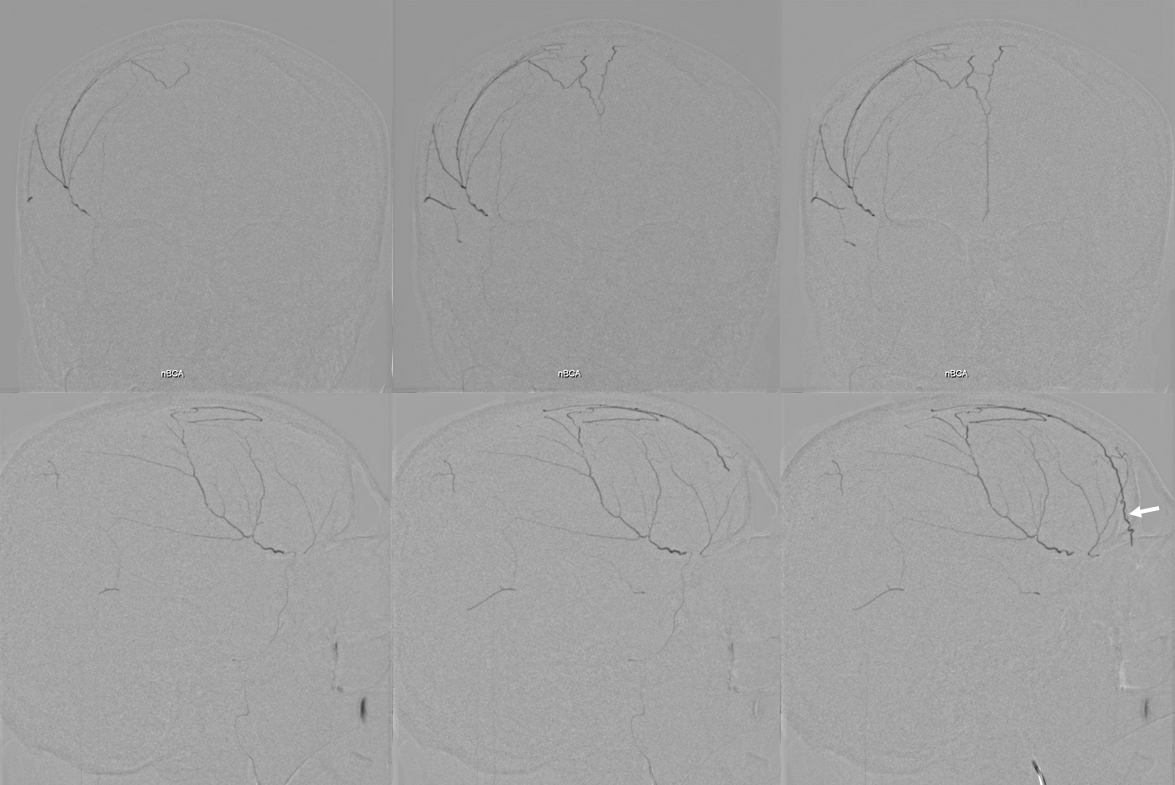
Case 2: Penetration of dulute nBCA into the anterior meningeal artery / artery in wall of the SSS. Full case HERE
Wedge position micro DSA on top and nBCA cast on bottom. Notice that we got the anterior meningeal — good stuff, another reconstitution route closed. Usually one side is better connected with the anterior meningeal than another
Case 3: In setting of meningolacrimal supply to orbit and other points. Full case HERE
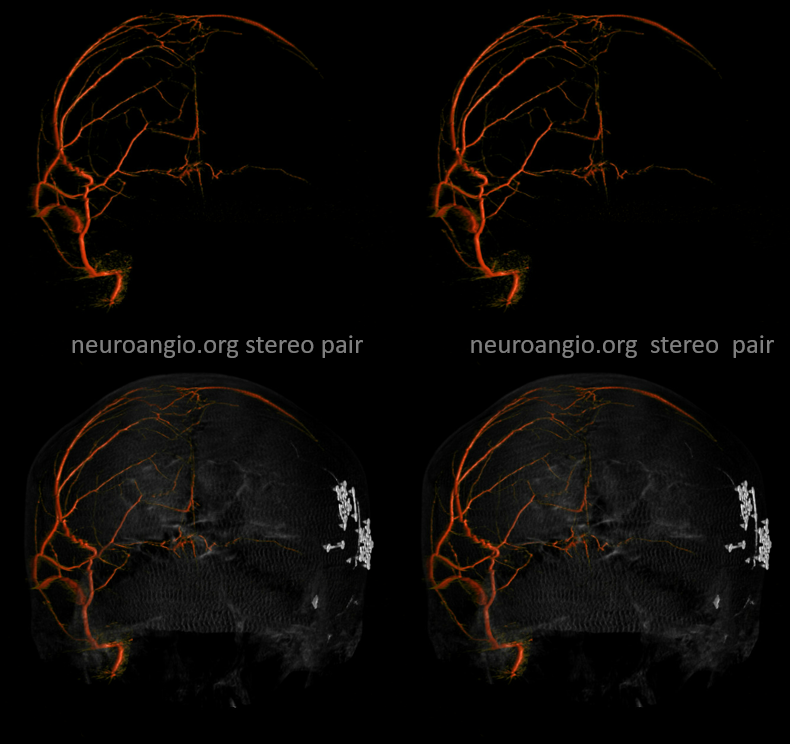
Stereos
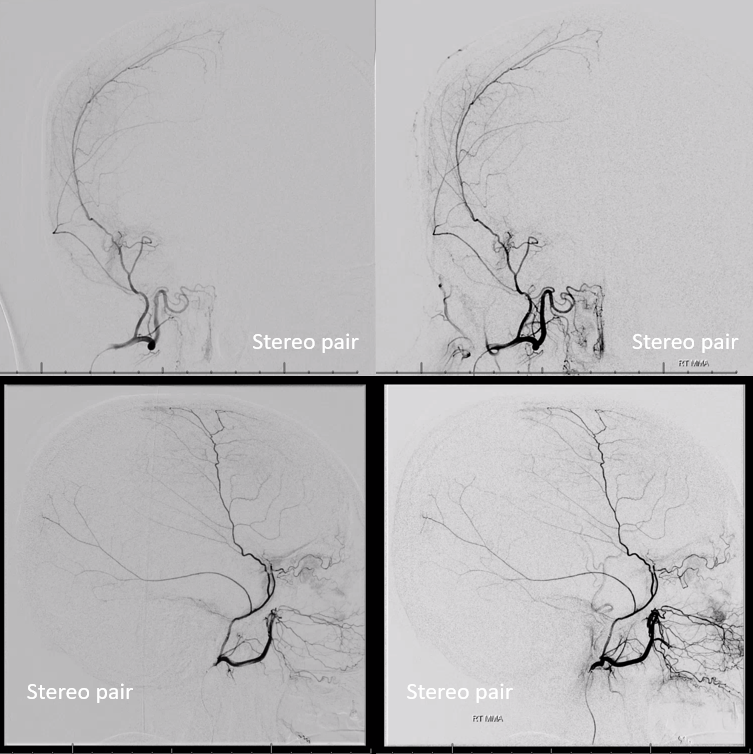
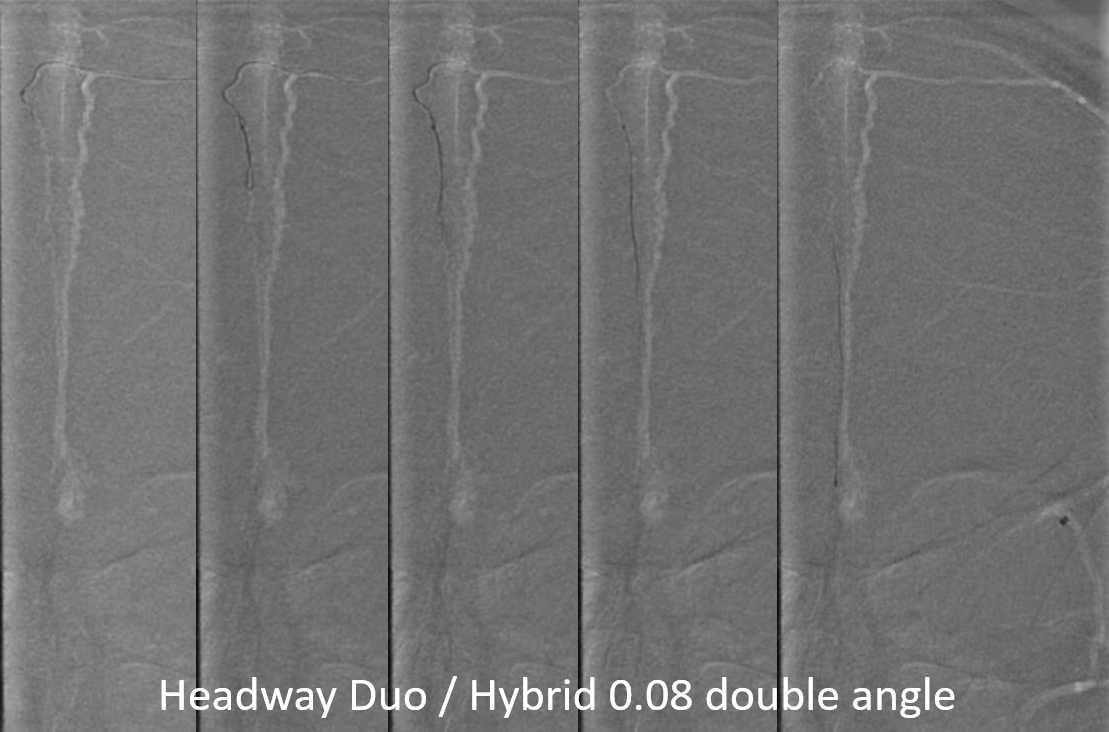
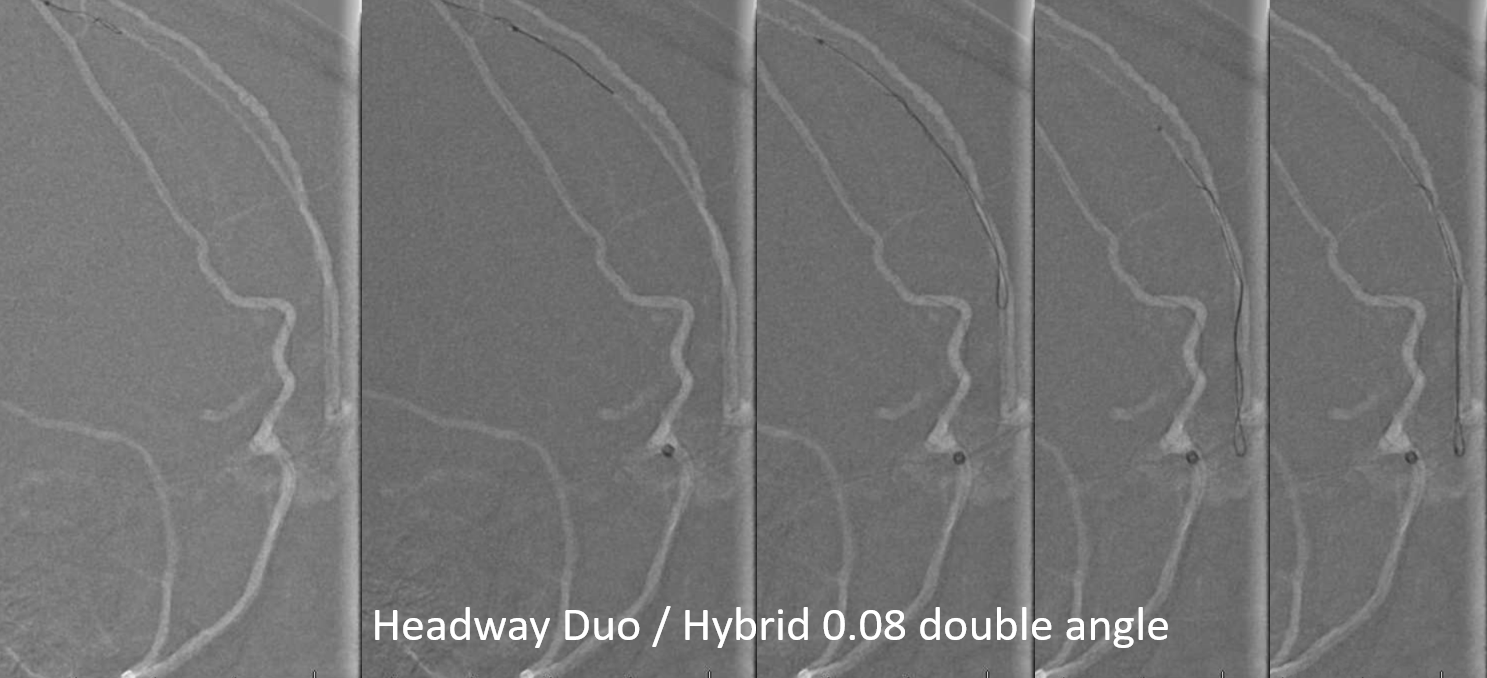
What to do — go distal to the meningolacrimal branch with a scepter C
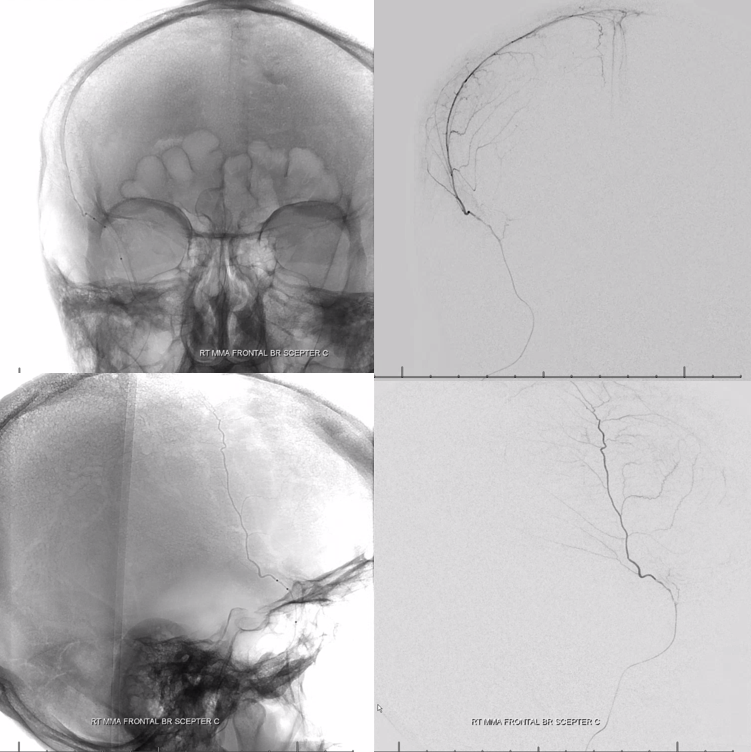
Late phase
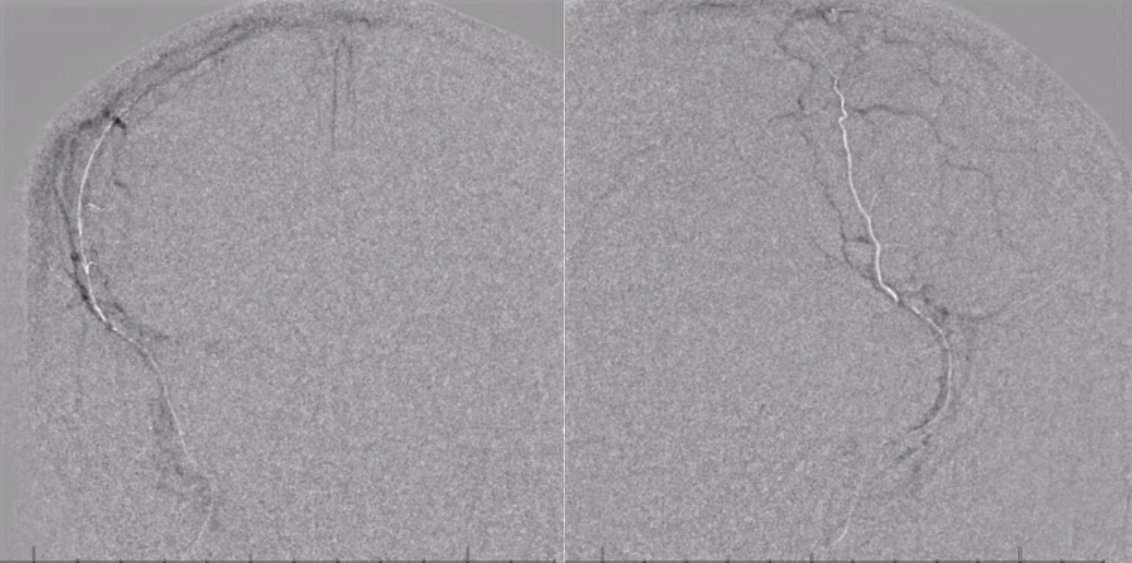
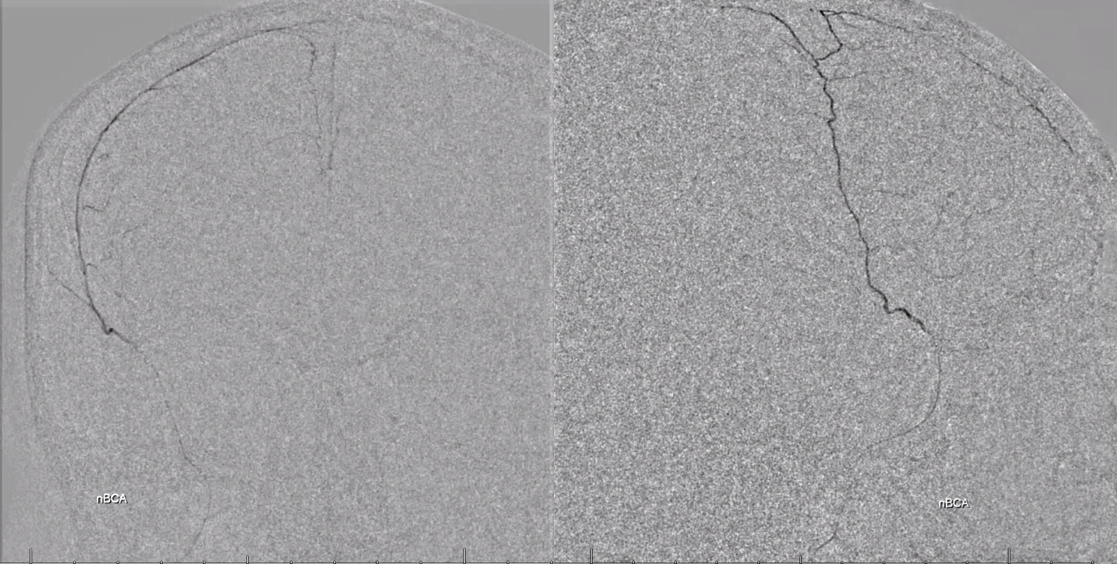
Now inflate the scepter gently but effectively to stop reflux, and inject 2:1 Lipidol:nBCA — excellent penetration into secondary MMA branches and the anterior falcine / anterior meningeal branch in wall of the superior sagittal sinus. Scepter ensures no reflux into the orbit
Conclusion: Think balance and spectrum. Balance with MMAs principally. Use it to your advantage