
Nice case to show important anatomy and glue technique points
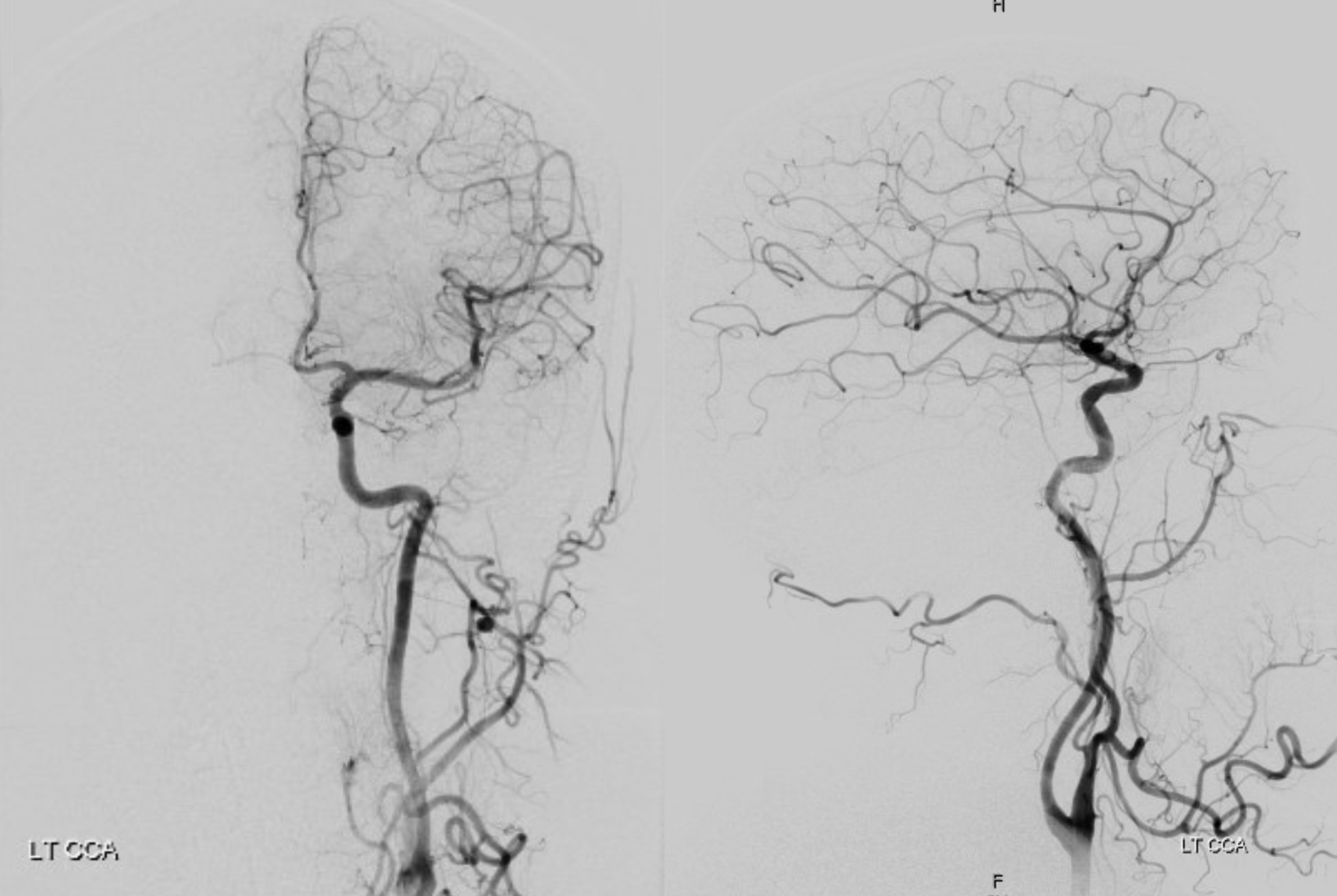
Small right sided chronic subdural in a ptnt with anticoagulation requirement
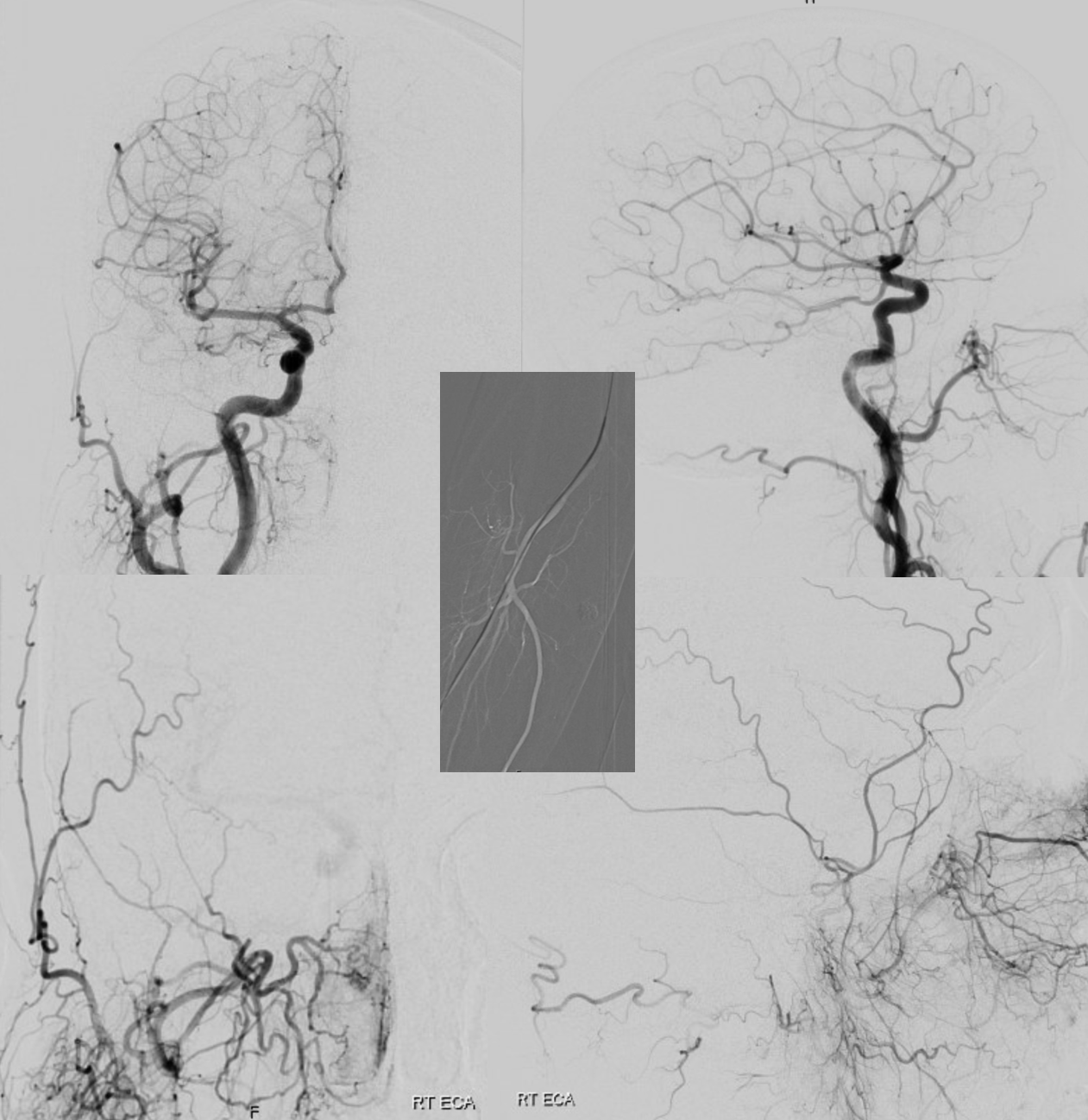
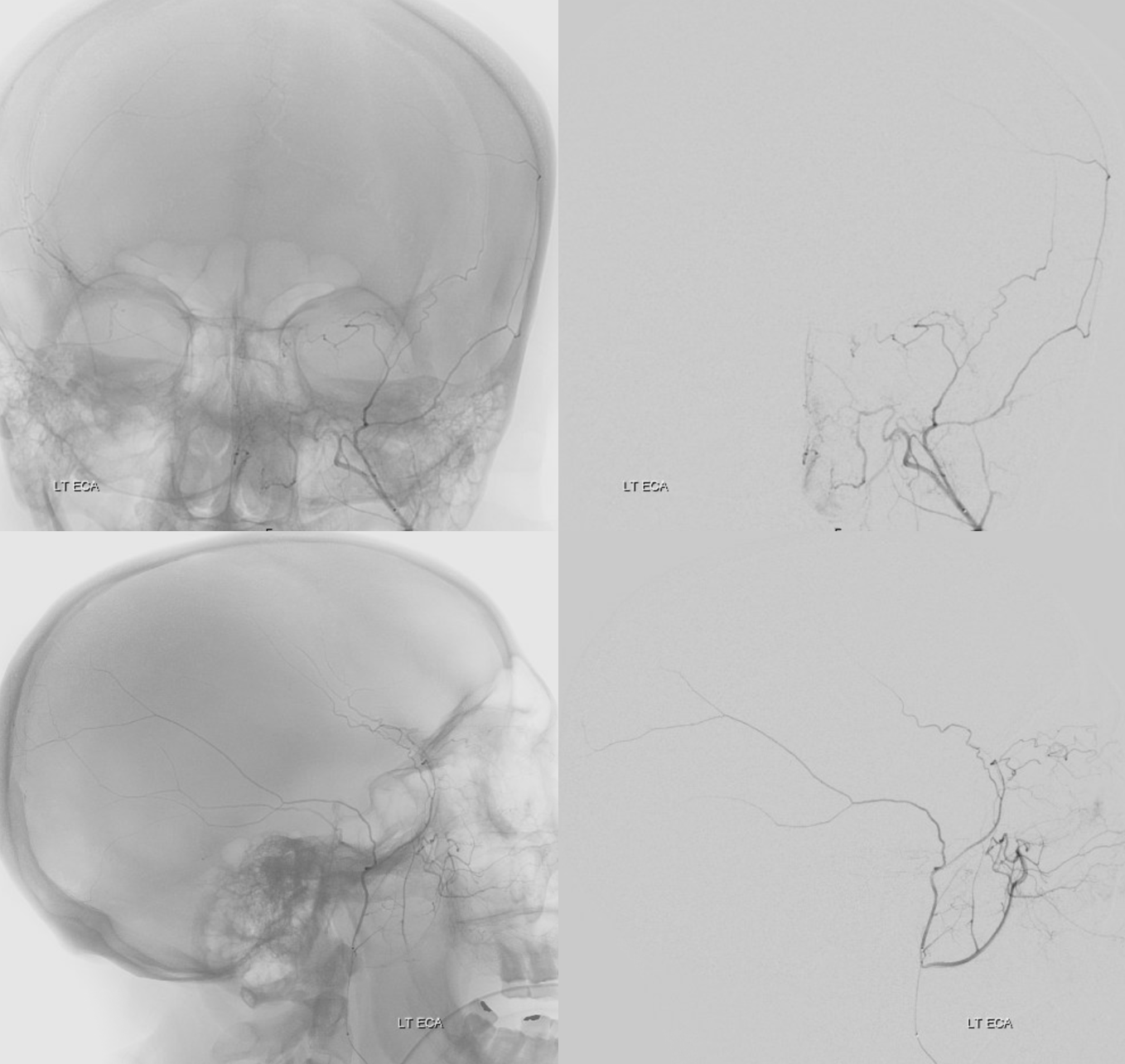
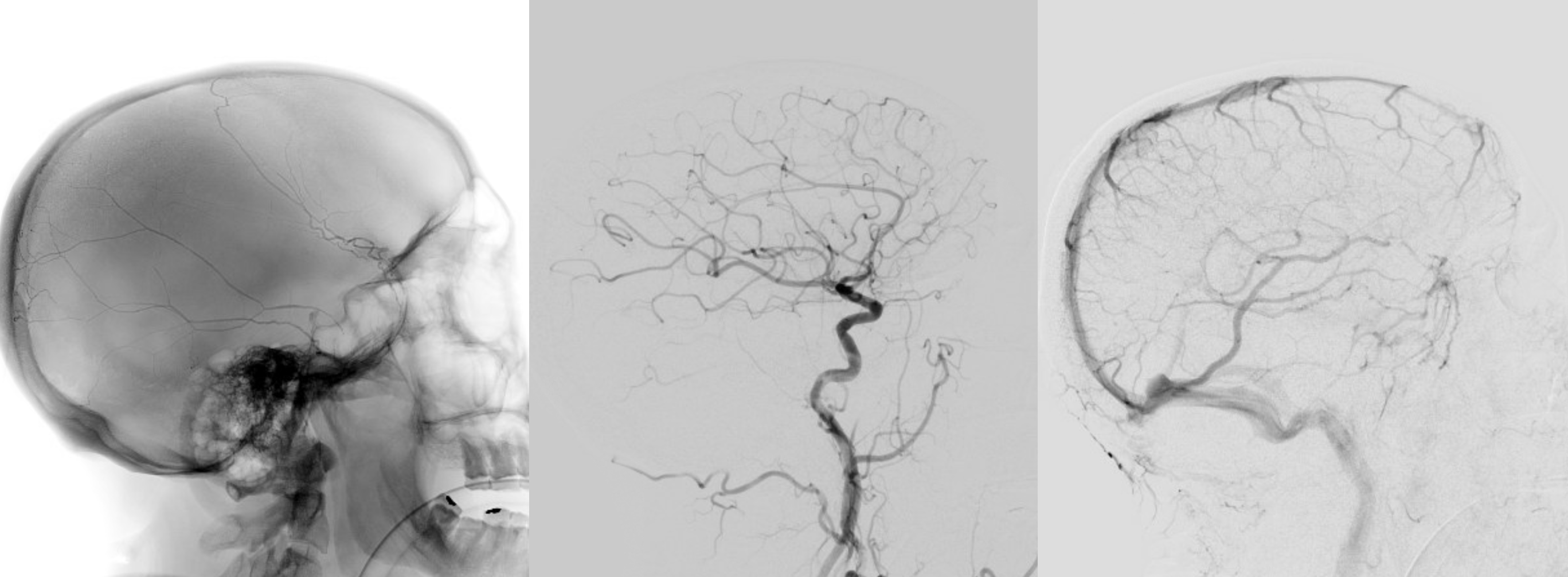
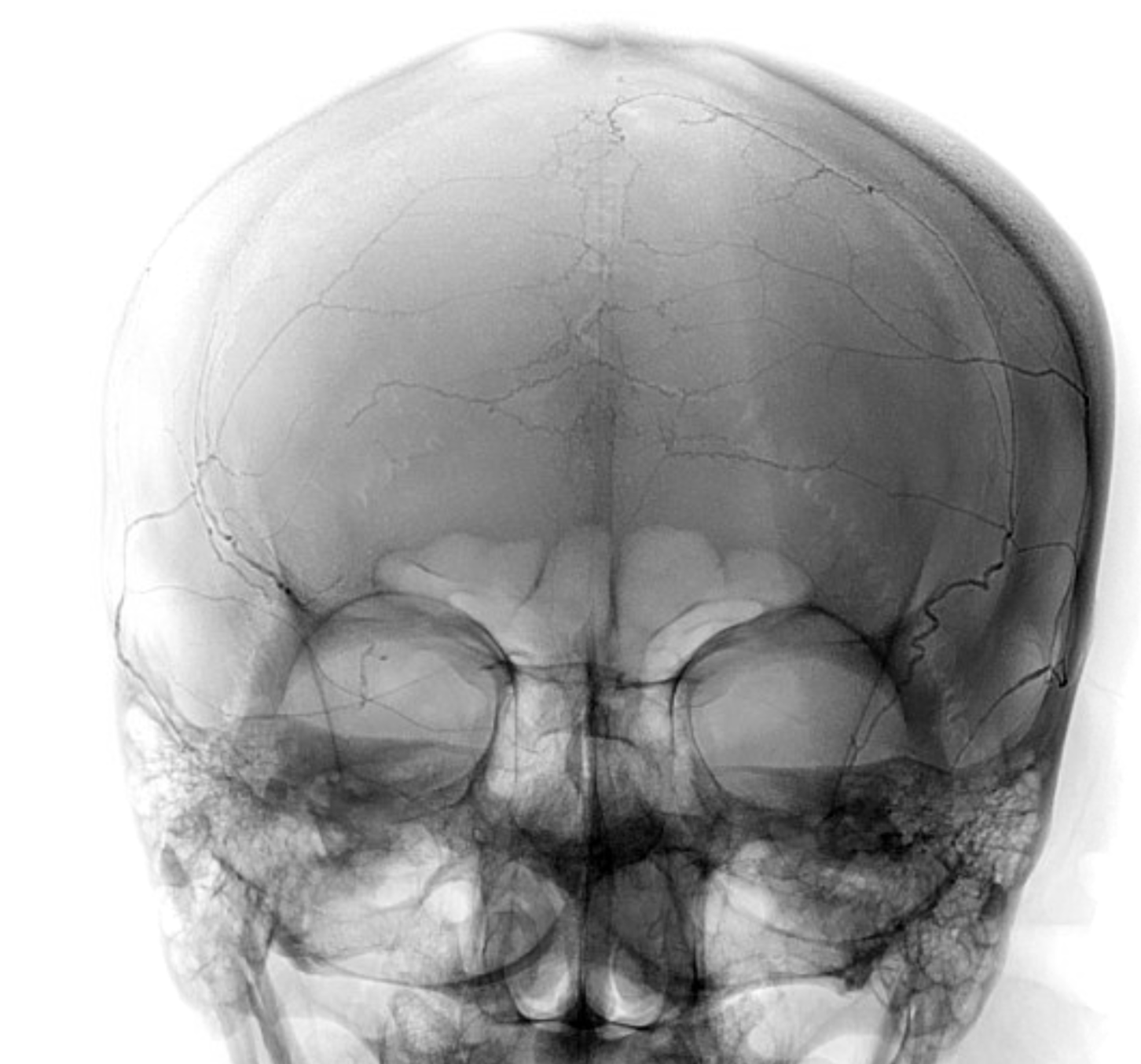
ECA — vessels projecting over orbit in frontal views are either occipital artery or in the orbit — and most often in the orbit. For MMA injections, its in the orbit. There seem to be two branches from the frontal division contributing to orbital supply
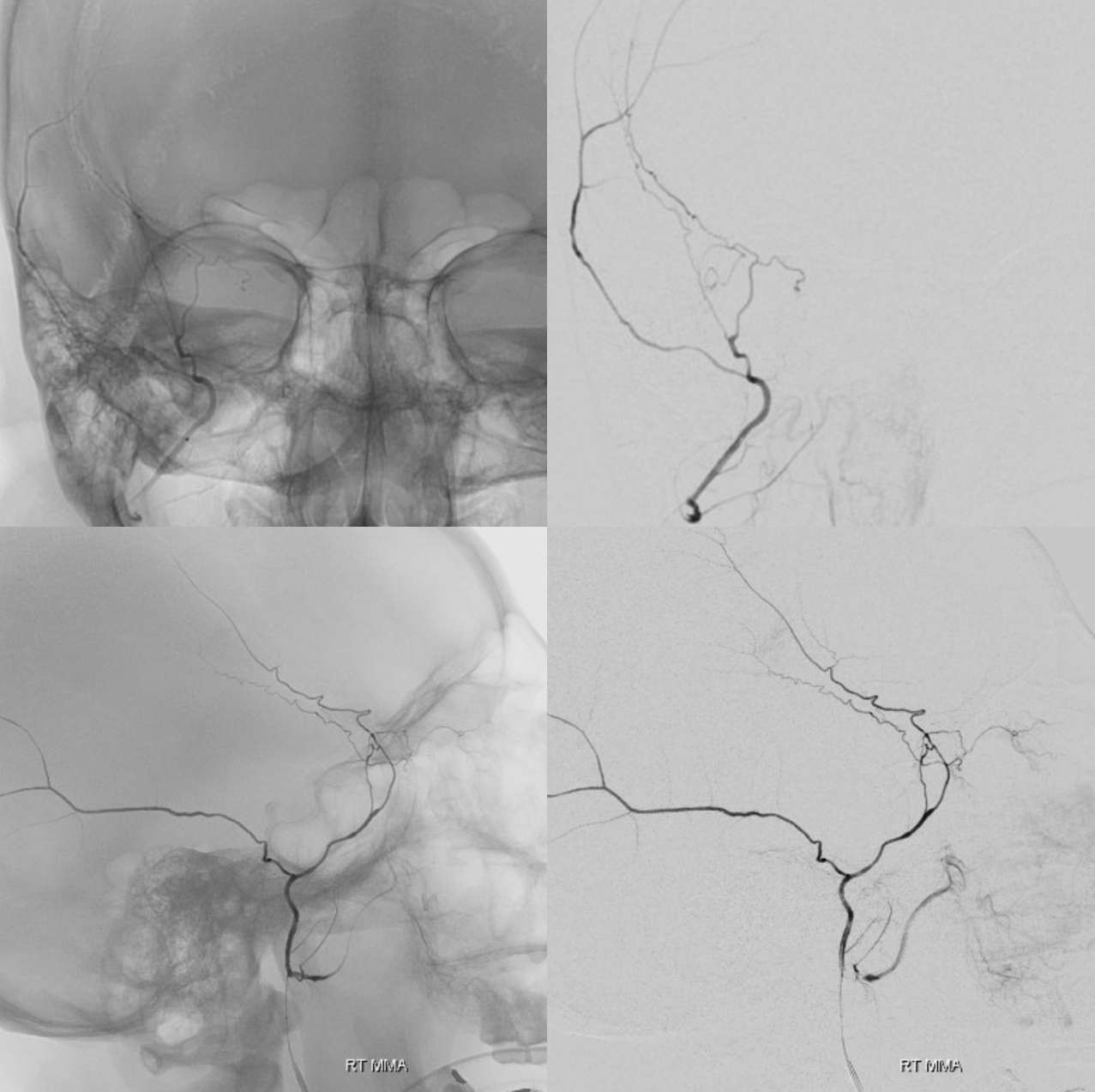
DYNA helps. Spectrum of variation — see ophthalmic and MMA pages. There are two orbital anastomoses — via the lacrimal branch (foramen of Hyrtl) and via sphenoid ridge branch to the SOF — this one mainly supplying extra-occular muscles. They don’t read books, except ours 🙂 See the JNIS MMA anatomy and embo paper too…
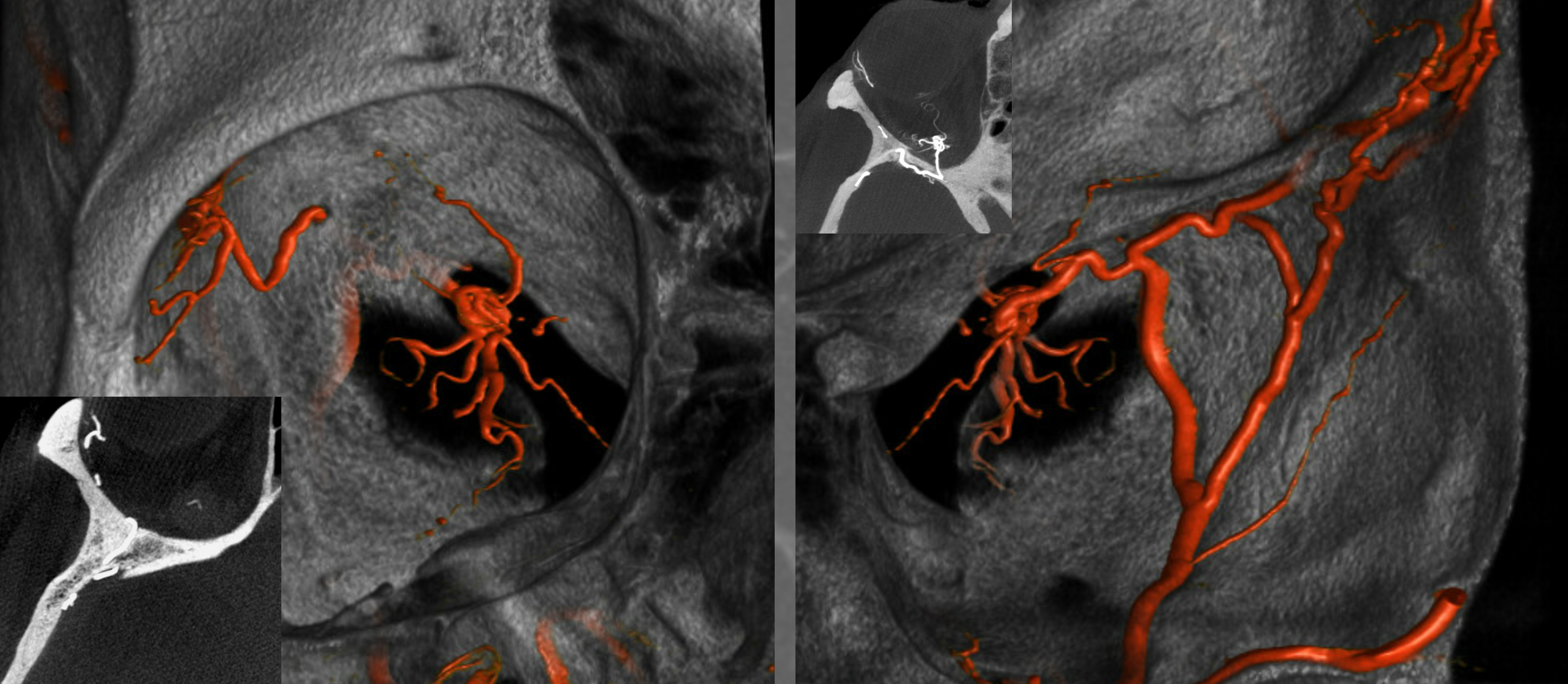
What to do? Get beyond the origin of orbital contributors (headway duo)
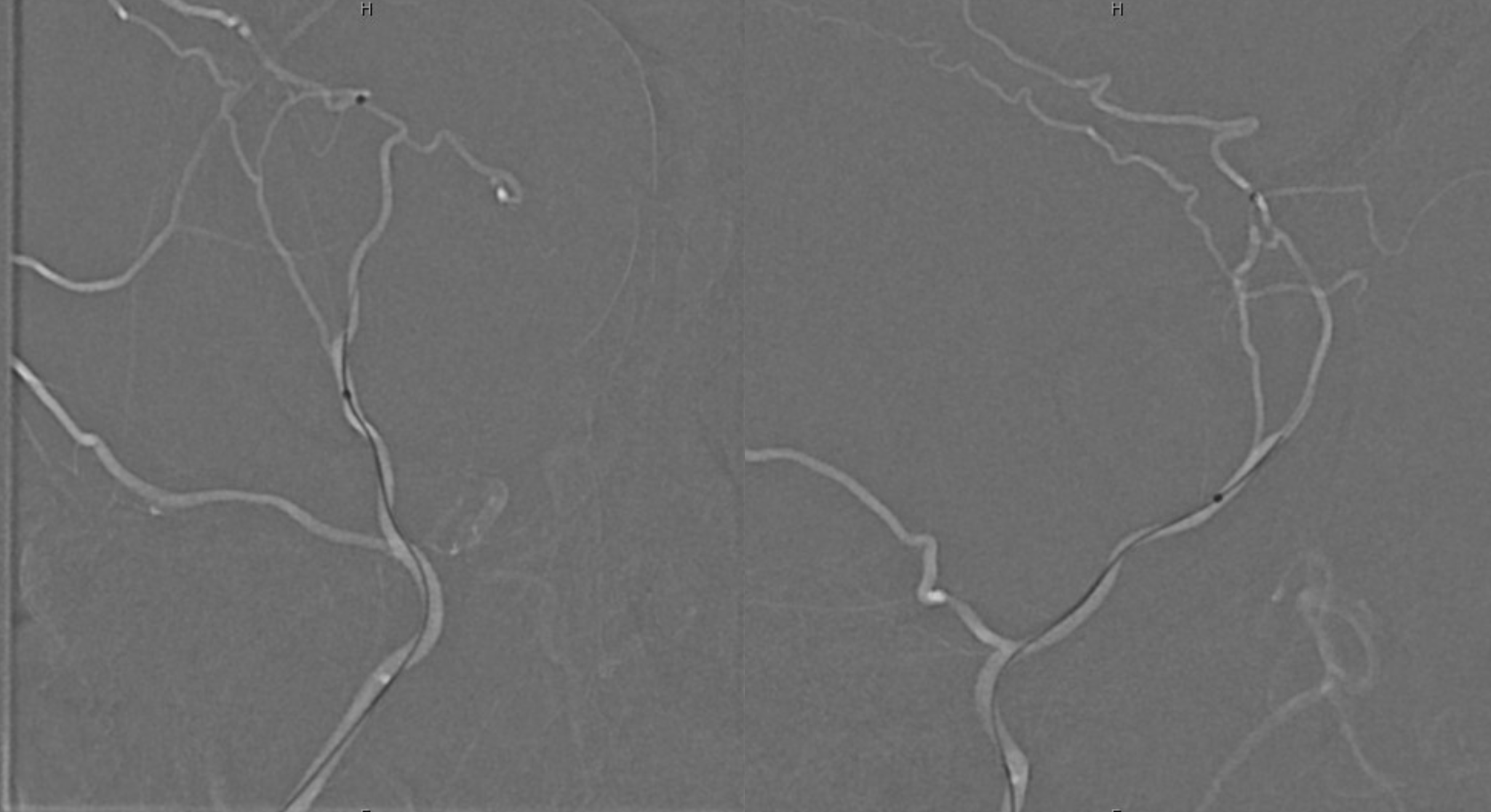
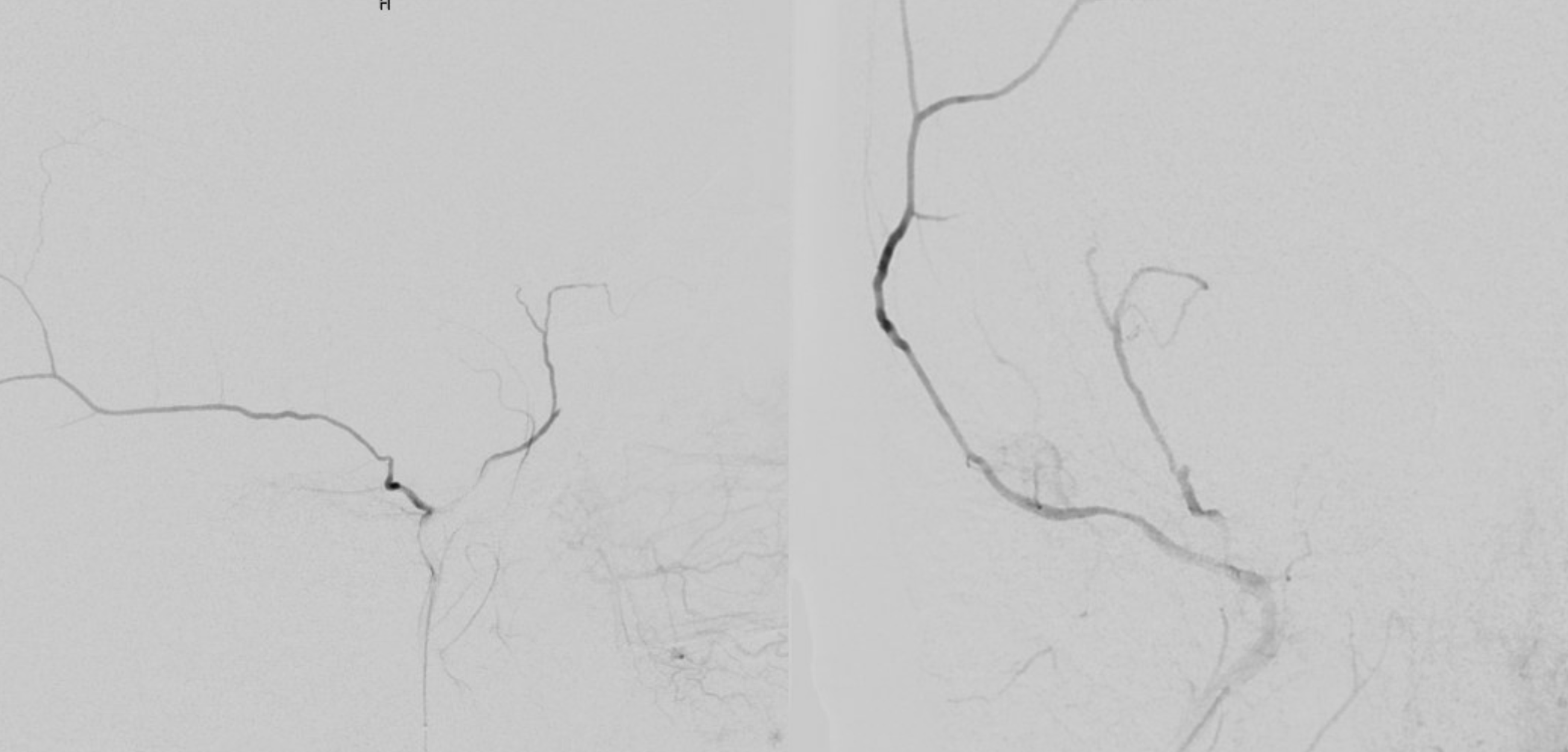
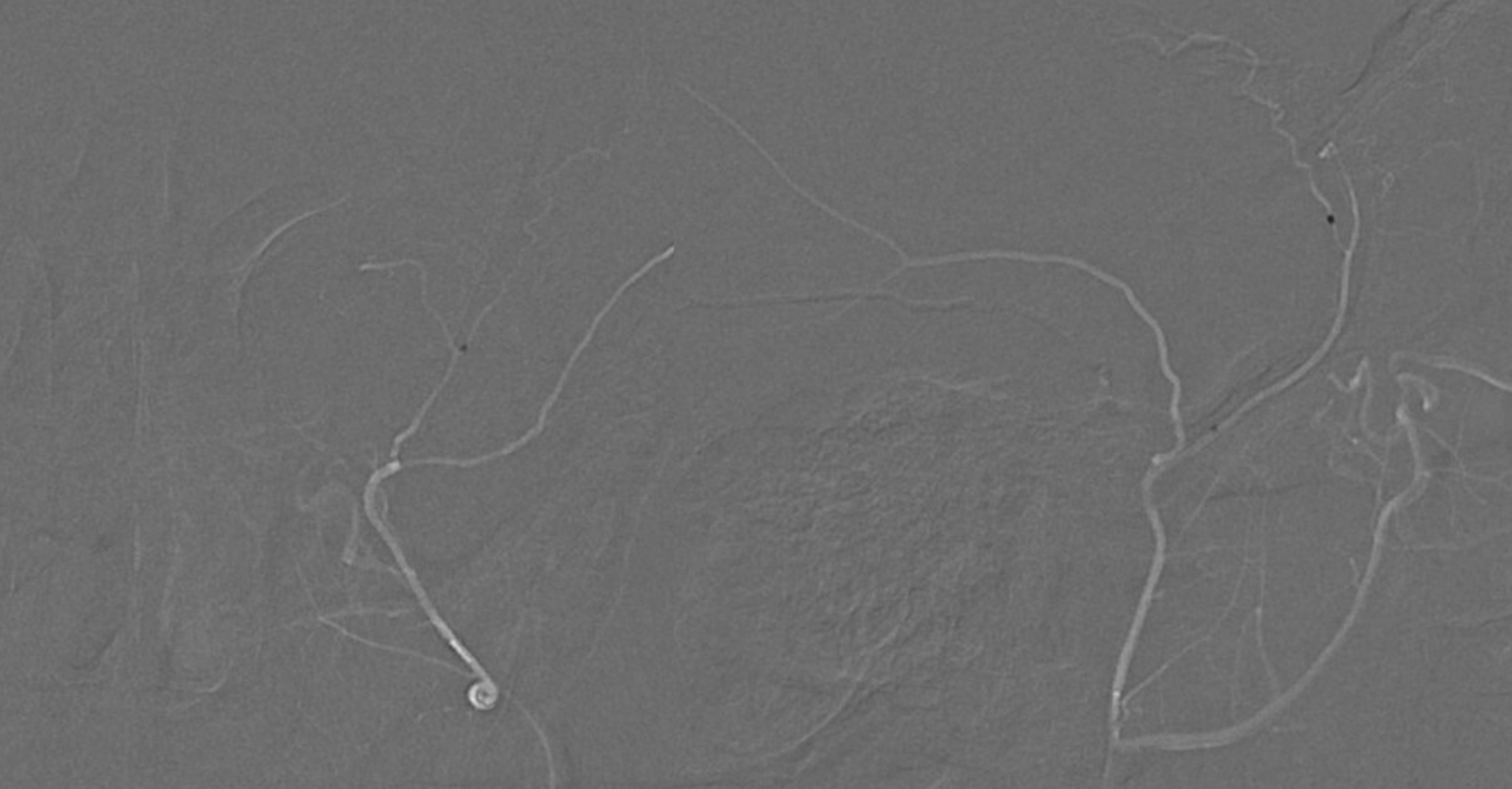
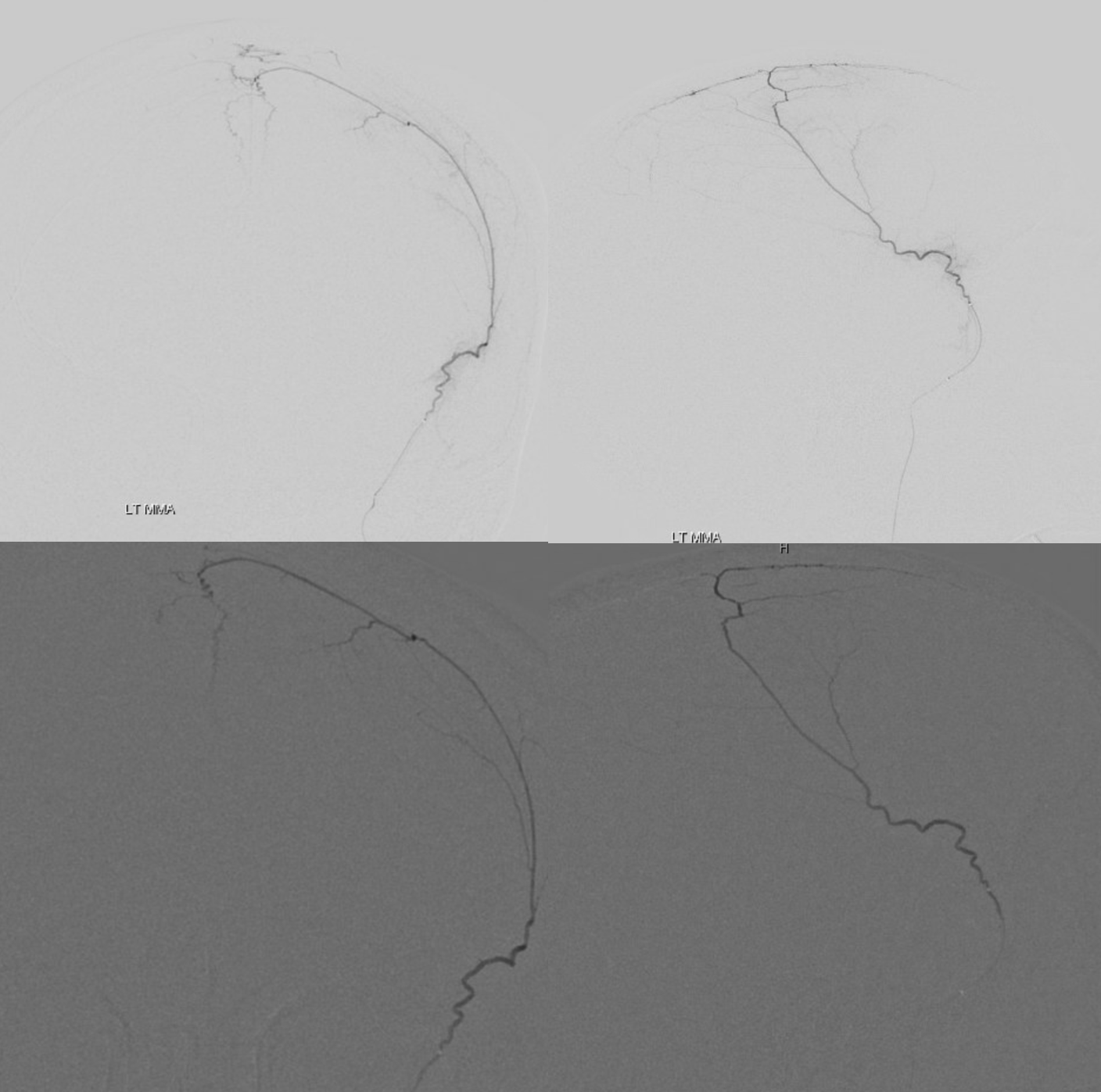
Injection here is interesting — there is significant reflux. Why? Either vessel is larger than catheter, or something else. Notice how the catheter is pointing into a turn (arrow). That’s not good. it is basically pointing into the vessel wall.
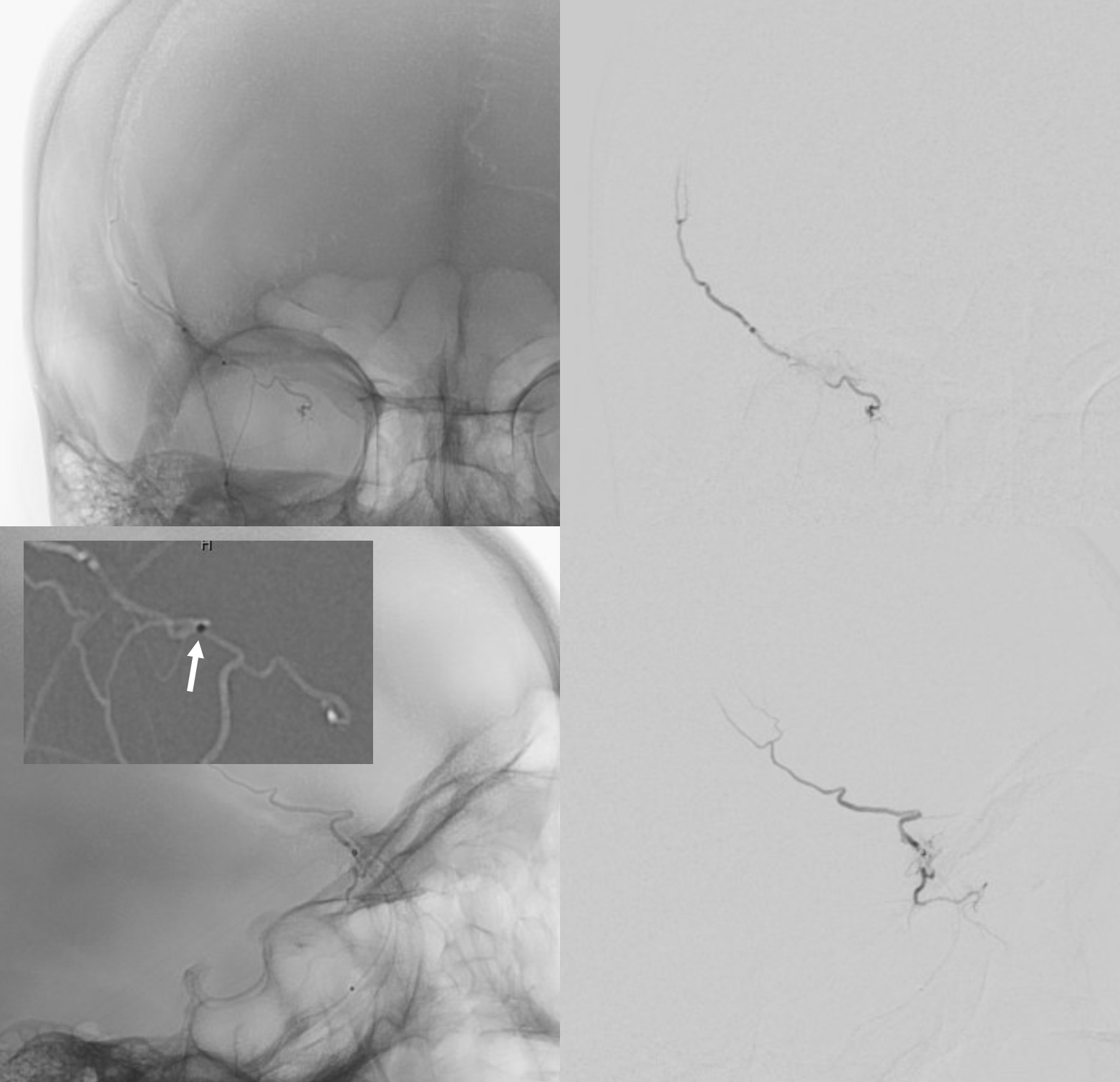
Pulling it back a bit helps — even though it seems counter-intuitive for achieving wedge position.
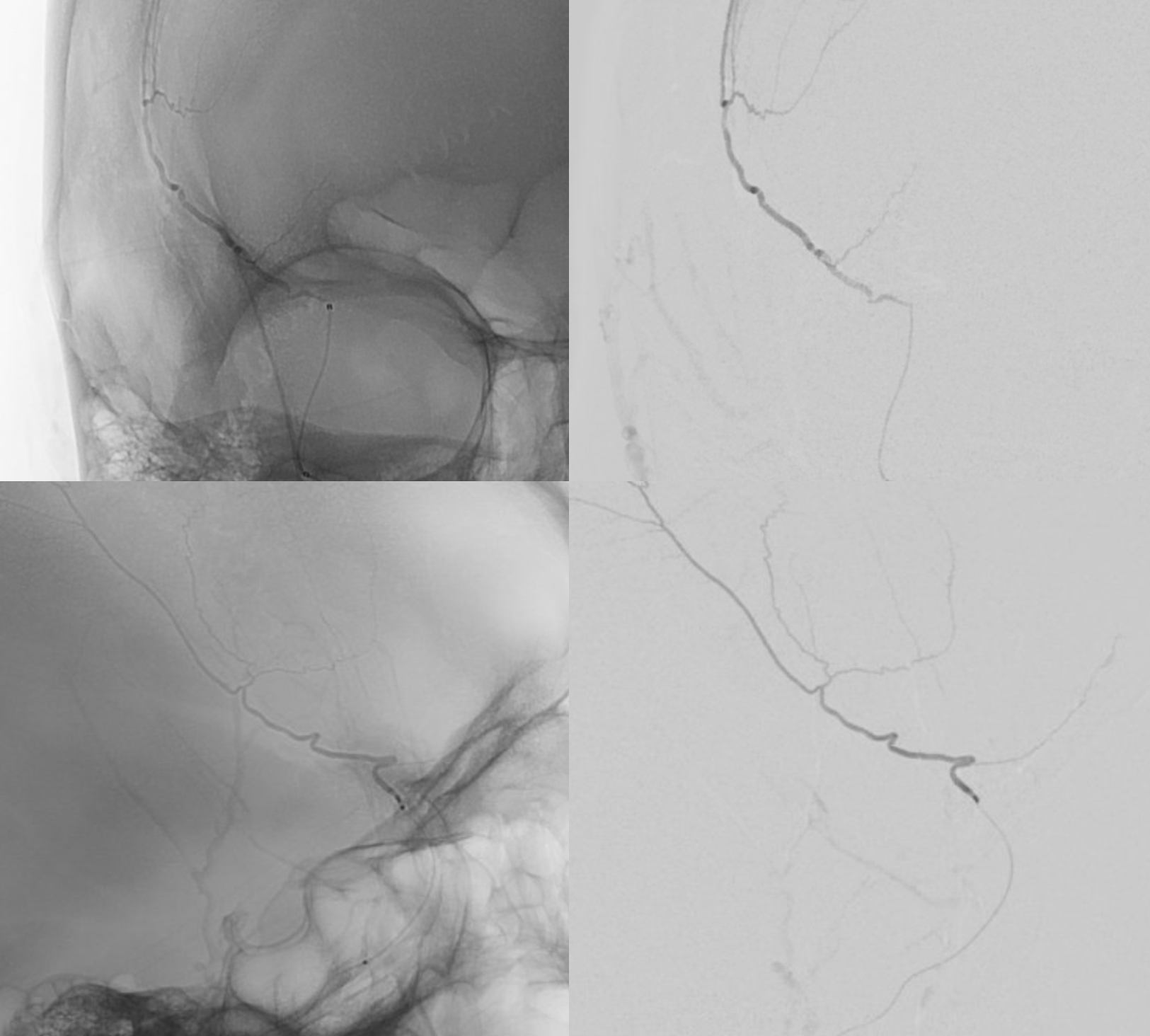
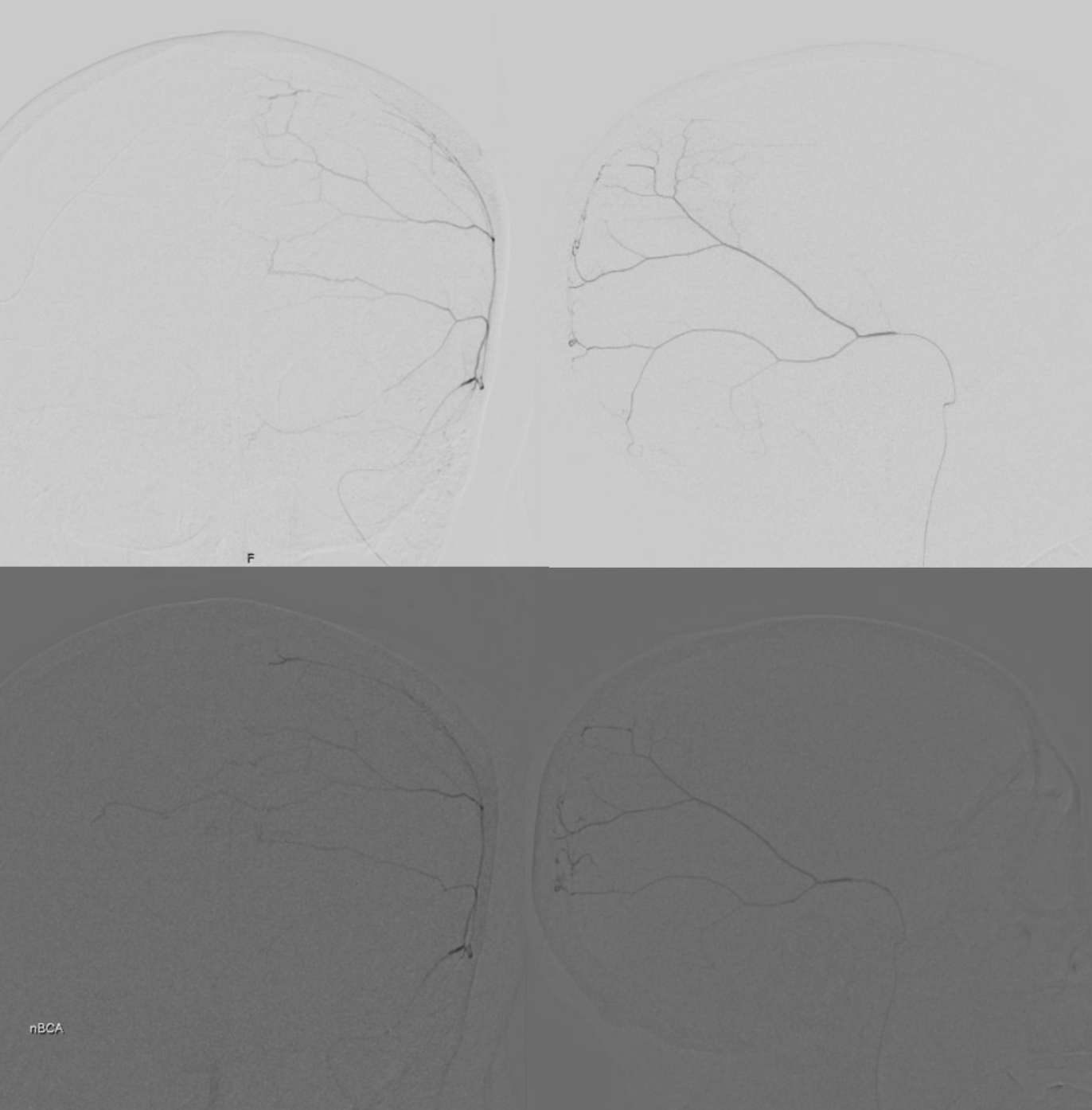
Now we ready to glue. Typically we like glue to be very dilute for MMAs (25-33% nBCA, rest Lipidol). The key is to stop as soon as there is reflux. The frontal views are thus magnified as it is the better projection to see the reflux. Lateral view is large since glue can go very far and needs to stay in the field of view. As soon as some reflux is seen (right-sided images, we pull)
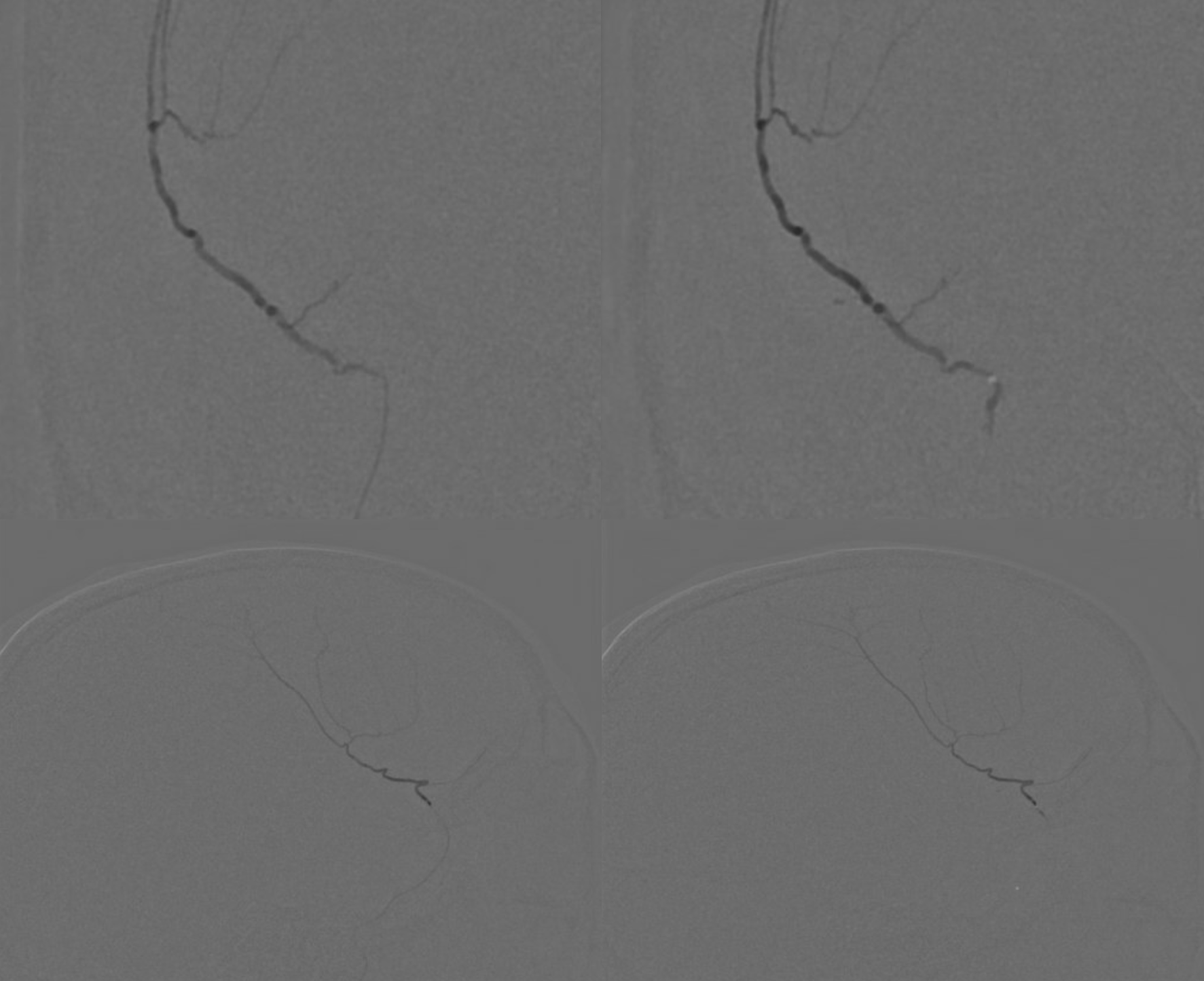
Post nBCA. Notice how there is some glue in that sphenoid ridge branch. No worry — there will be plenty of collaterals from the ophthalmic and its fine. Reflux with particles here would be bad, as they would likely travel downstream and lodge wherever. Glue stays local here. it was however also important not to reflux so much as to occlude the other frontal branch, which comes next.
Post embo — second frontal branch still alive.
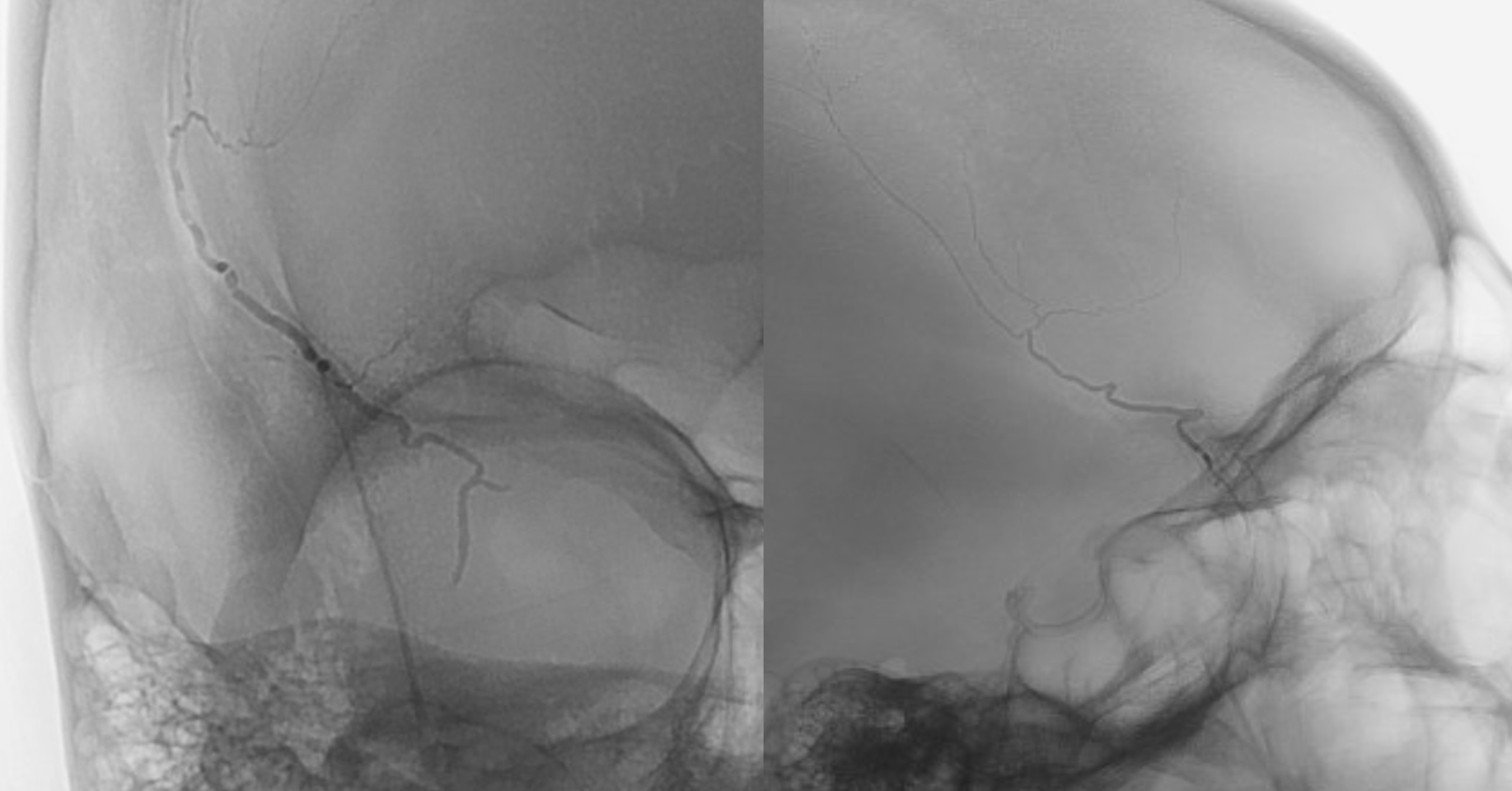
Wedge position in second frontal branch, beyond lacrimal. Note an unusual anastomotic channel heading down towards the skull base? That’s the danger.
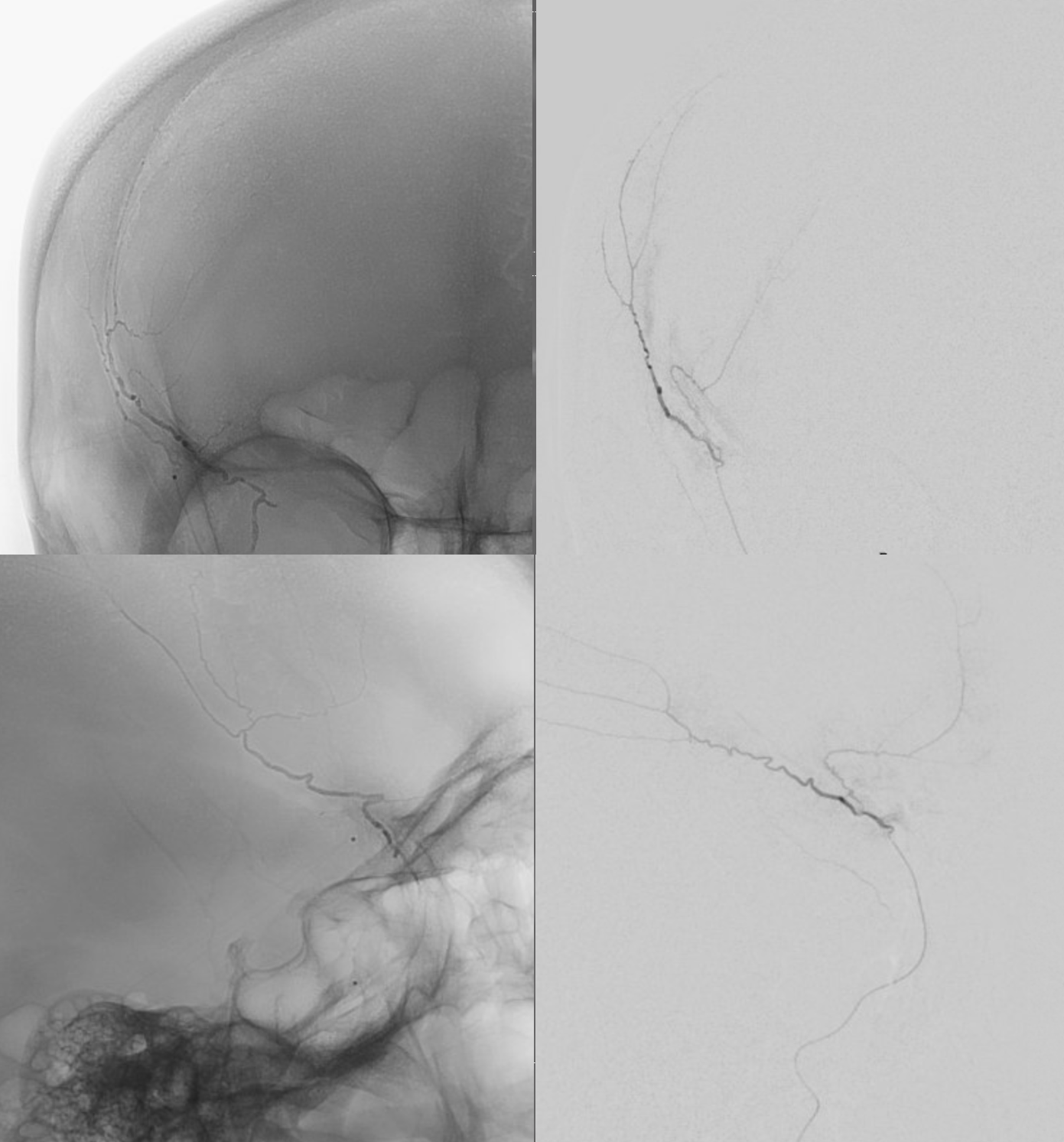
post nBCA — stopped when glue reached low enough in that inferiorly-heading branch.

Now to the posterior division — wedge position on top, glue cast on bottom. See how much cross-opacification you can get? It’s good to put glue into the arterial network around SSS to prevent reconstitution. Also see that petrous branch? The catheter position is too proximal. It was advanced before taking glue shot (left lower image)
Post right side
Done? Maybe yes, maybe no. We prefer embolizing bilaterally in many cases to help minimize recurrence — time will tell if this is the right approach.
A neat trick for catheterizing something with a sim select that does not want to go into the ostium. In this case, an 014 Synchro soft helps point the Sim into the left CCA

Another orbital connection
Posterior division wedge position and glue cast — often reaches further to the contralateral side since there is no antegrade flow there. Stopped when reached sigmoid sinus network — further down will be jugular and hypoglossal territory of the ascending pharyngeal. Also good to watch for midline branches in the falx cerebri and possible dural-pial connections with vertebrobasilar axis
Last one — frontal branch — beyond orbital connection — not a lot of “safety” but its ok. Again, some reflux into the sphenoid ridge branch is ok.
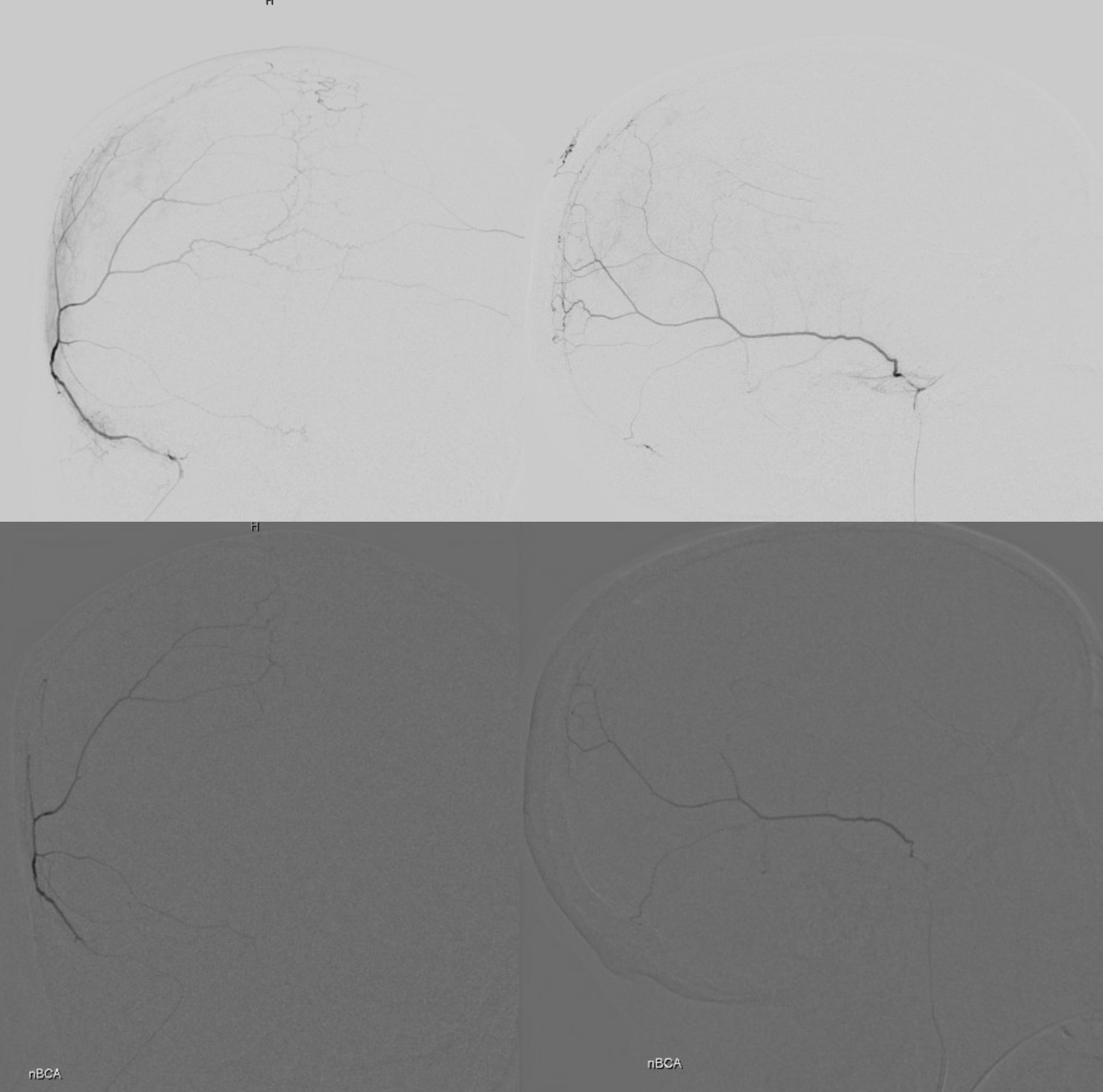
Wedge position micro DSA on top and nBCA cast on bottom. Notice that we got the anterior meningeal — good stuff, another reconstitution route closed. Usually one side is better connected with the anterior meningeal than another
Post
Post frontal view — that’s what a good nBCA embo should look like
Movie?
K. So long.