By Eytan Raz MD PhD
Preview….
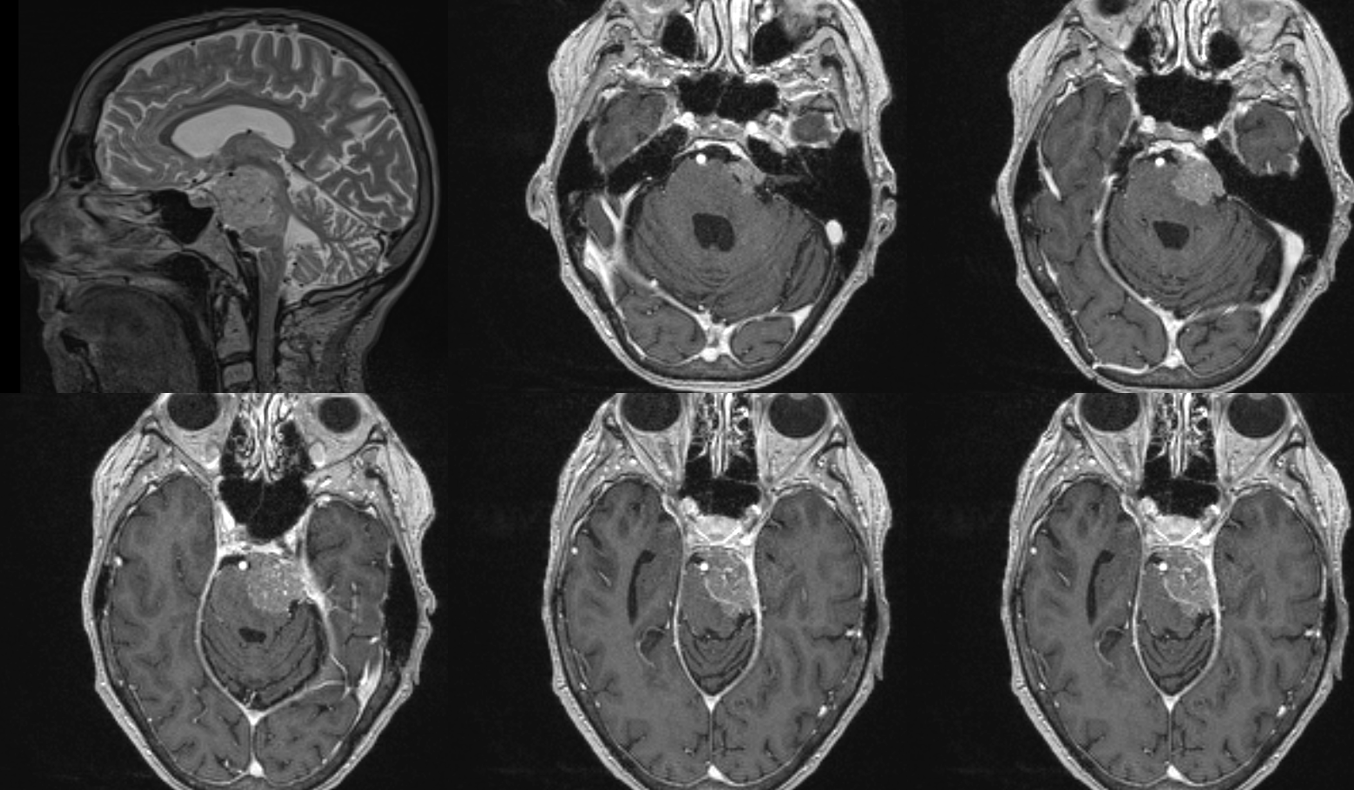
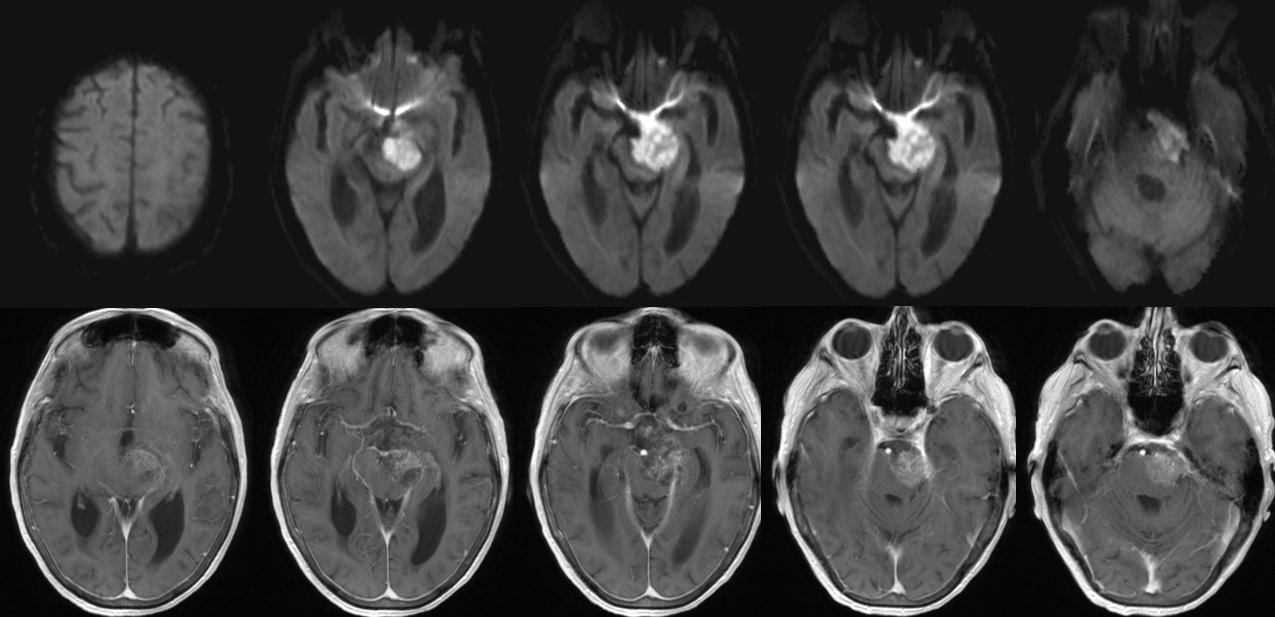
Typical mass effect. No obvious pial supply. Good for embo. How much more can one see? not much.
what is the supply?
Stereos

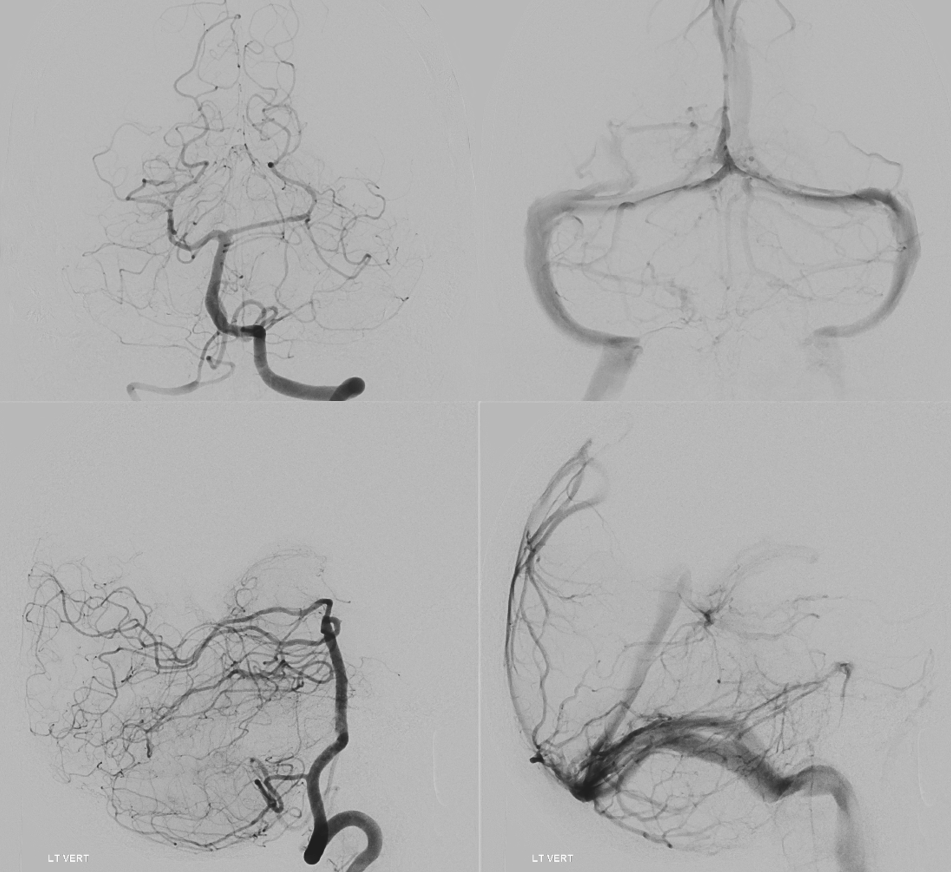
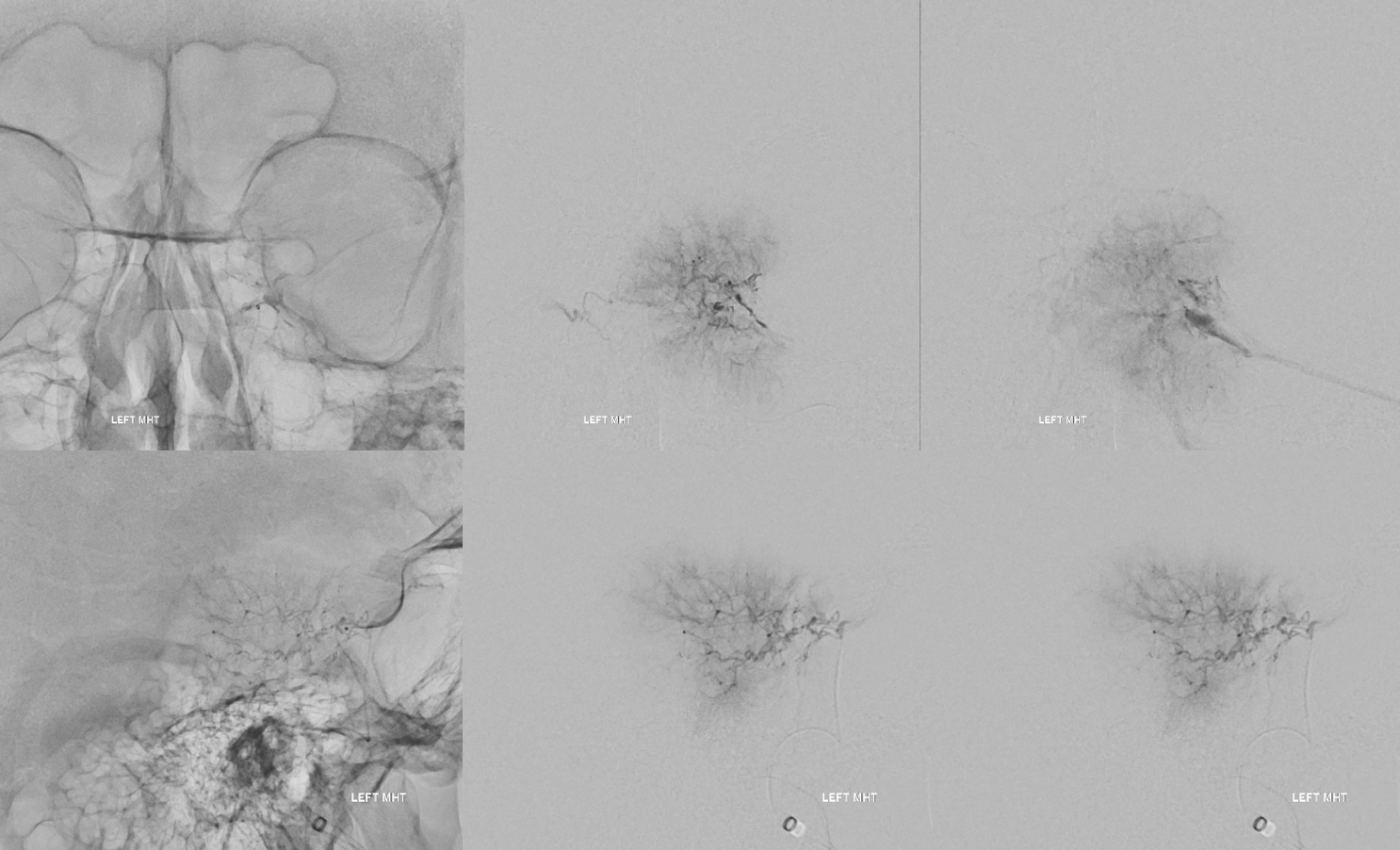
Views for catheterizing the ILT. Ultimately, the Aristotle 14 wire went in, but duo was too large. MHT is a sure thing though.

MHT. What is the important thing seen in the middle images? Is there a connection with the territory of the ILT?
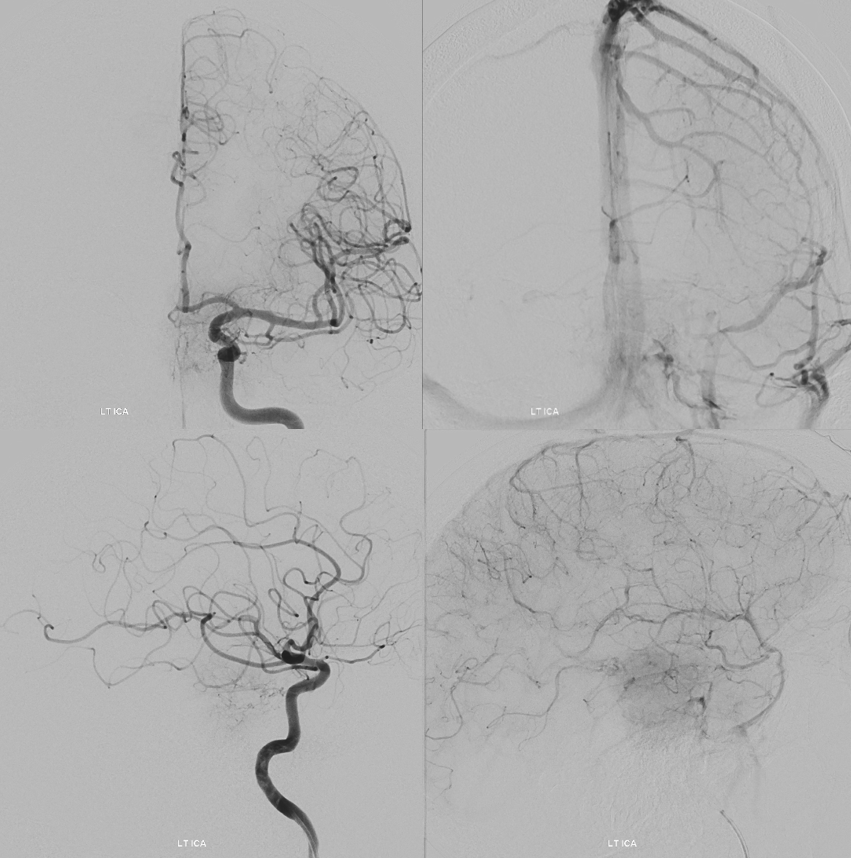
Post embo next stop is ECA. Do u see the supply?

Post embo
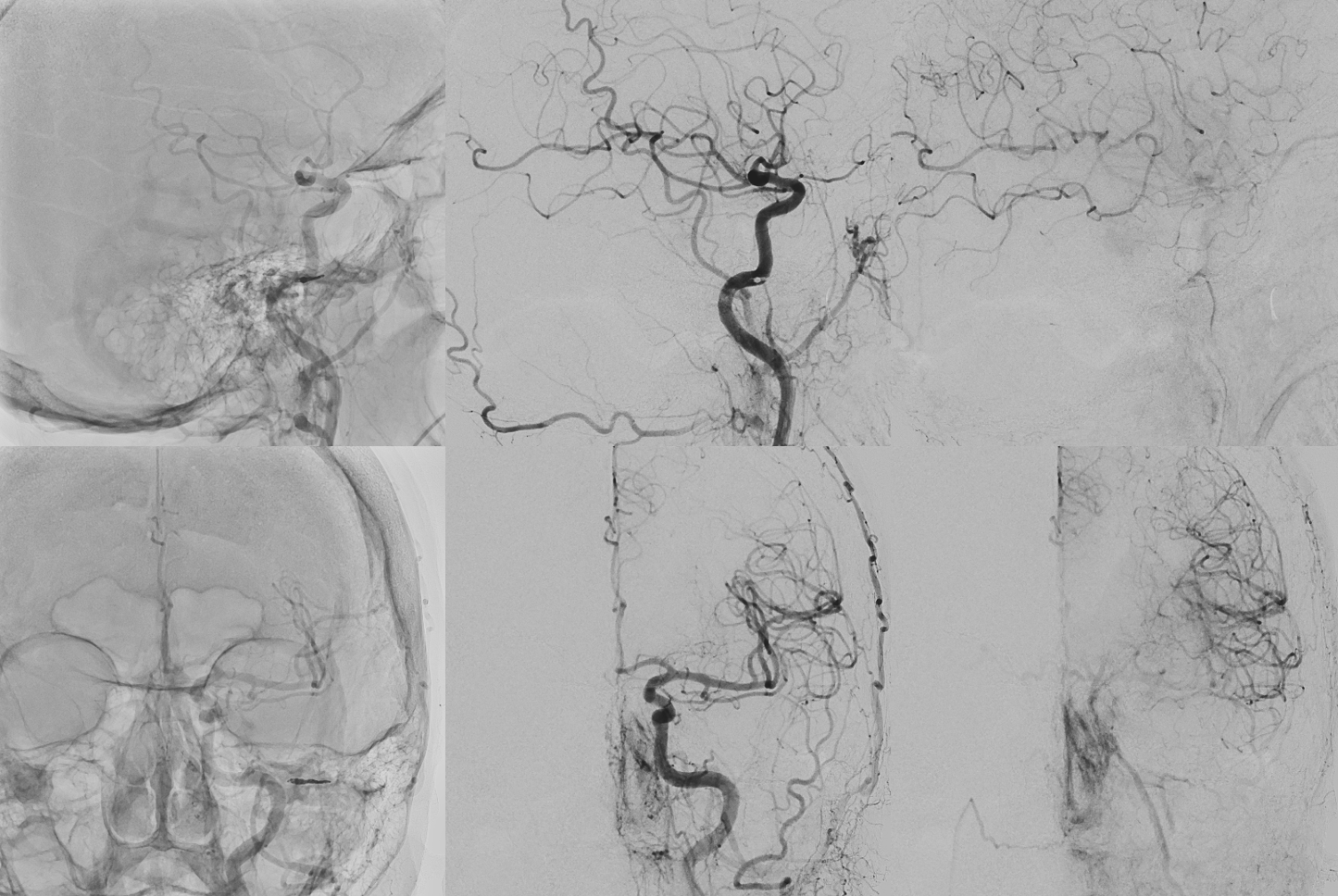
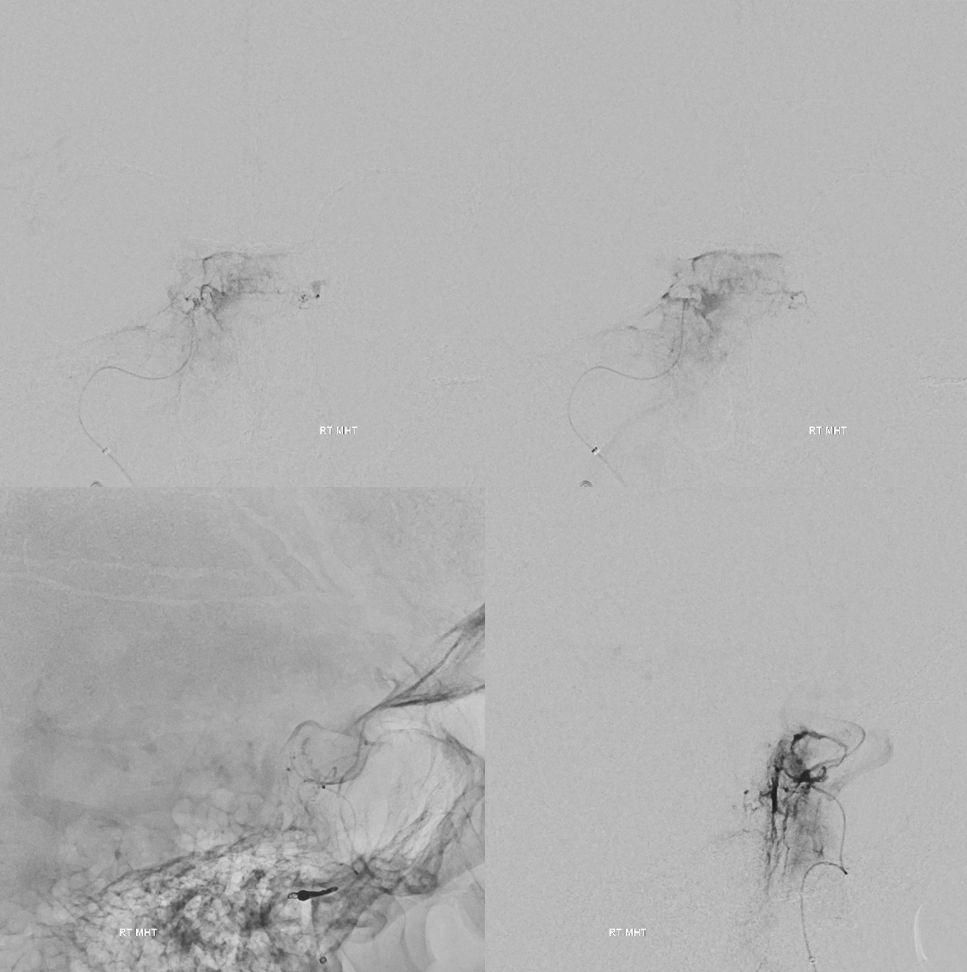
Right MHT. No embo was done.
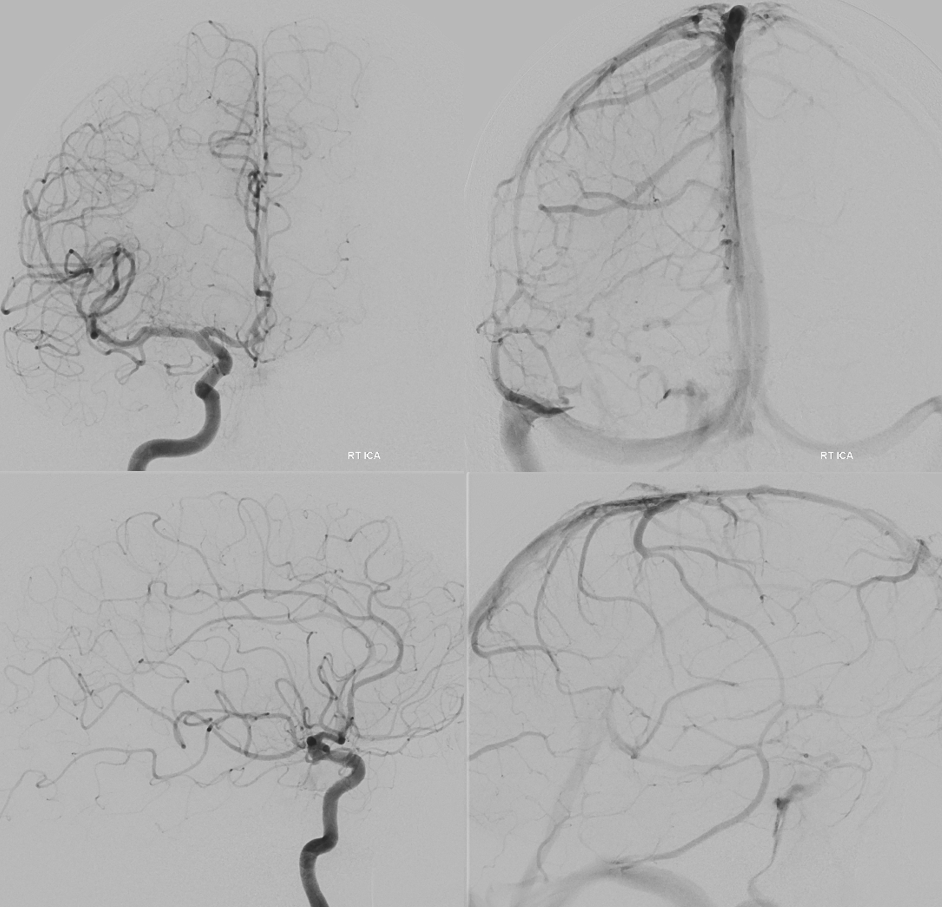
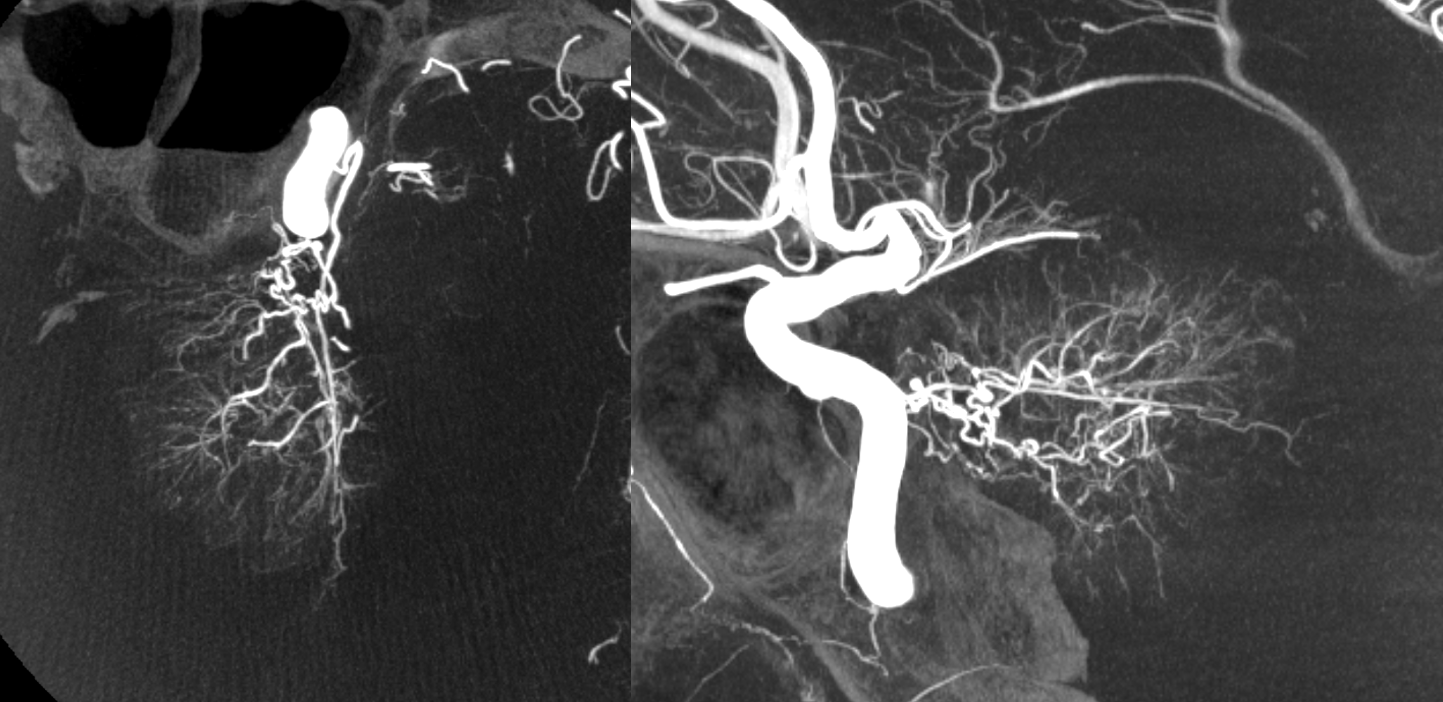
Now that you have seen the classic 2D-DSA, see how much more there is…
MIP images. Study the territories of MHT and ILT. See how they do not really connect in this case at any point. This means that MHT embolization is not going to help with devascularization of the ILT supply. Nor will MHT embo result in inadvertent embolization to the the ICA via ILT anastomosis.
Fusion of vert and left CCA injections. Understand the relationship between the tumor, AICA, basilar perforators, SCAs, and PCA — the SCAs and basilar perforators are encased.

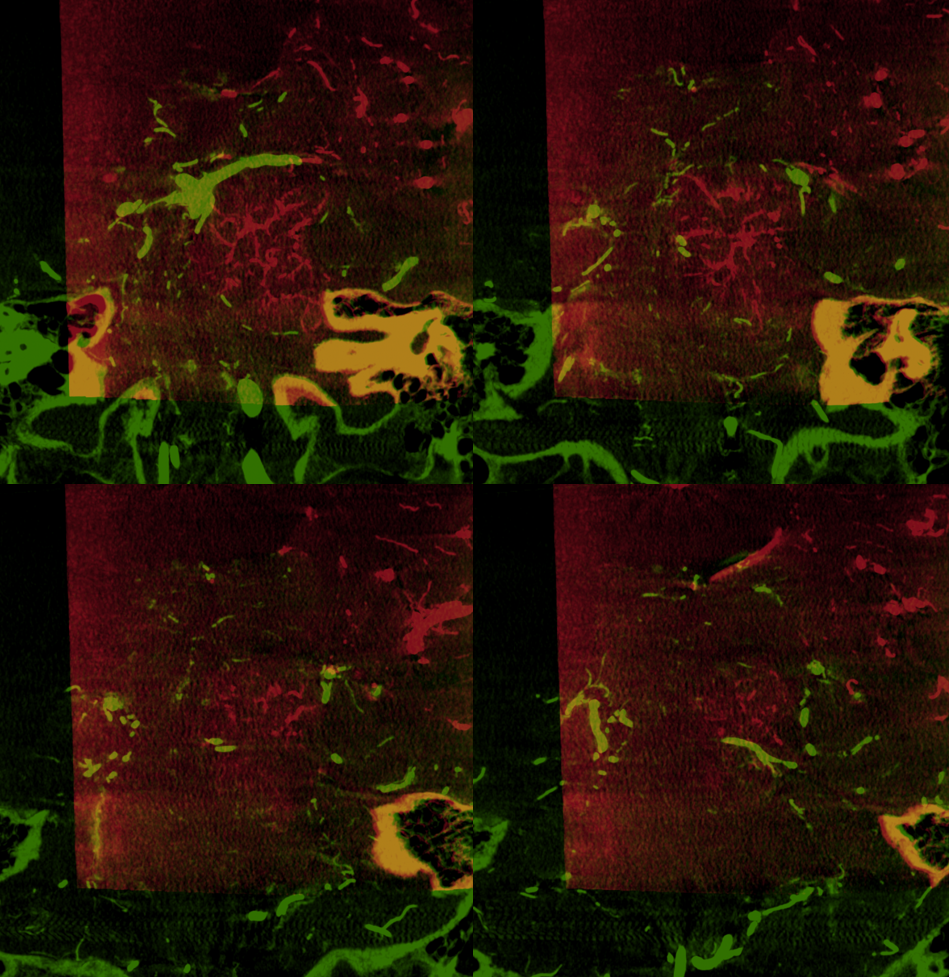
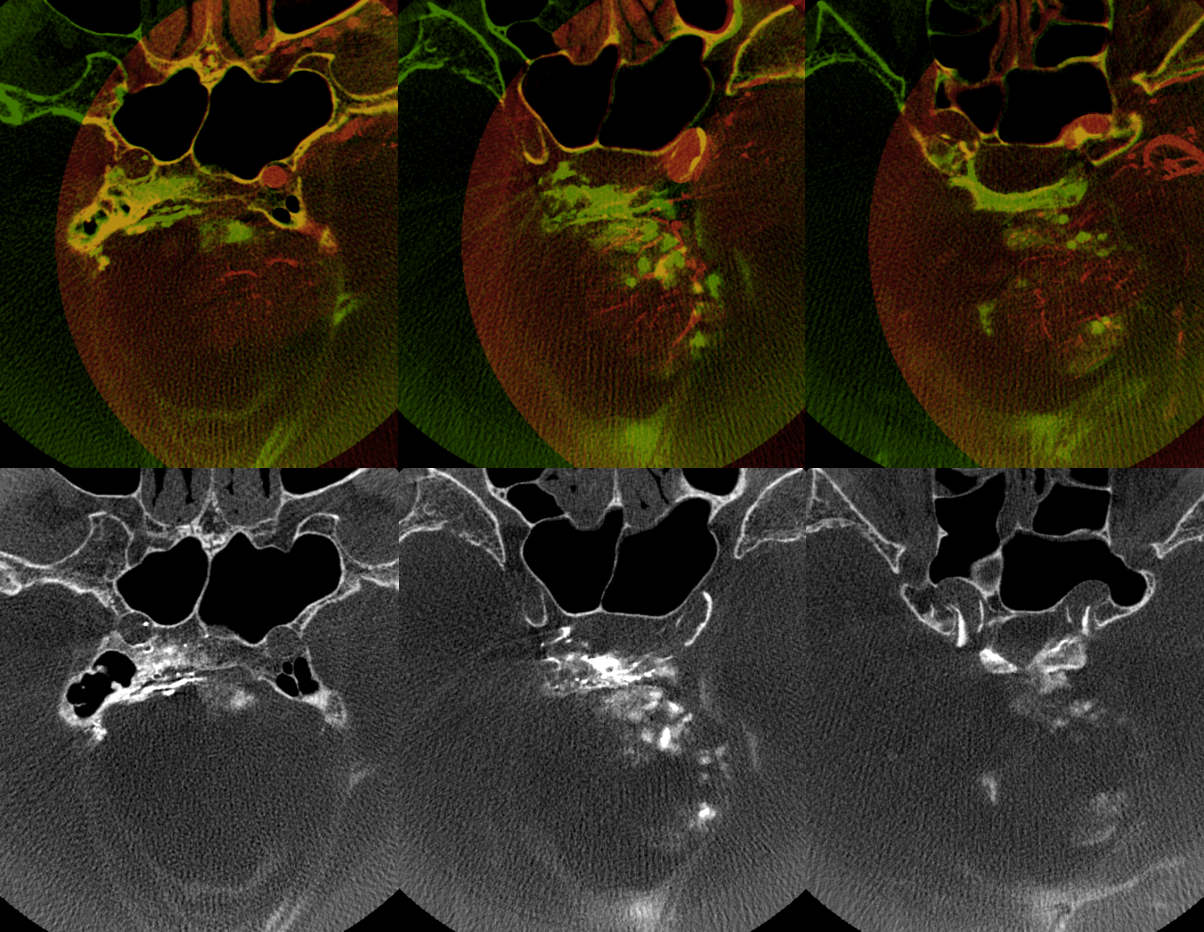
Embo is with Contour 45-150 particles only. Deep tumor penetration is essential. Post embo DYNA — there is contrast stagnation (bottom row standalone, fusion green top row) in the embolized tumor, fused with left CCA pre-embo DYNA (top row) Note lack of contrast in the inferior part of the tumor — why?
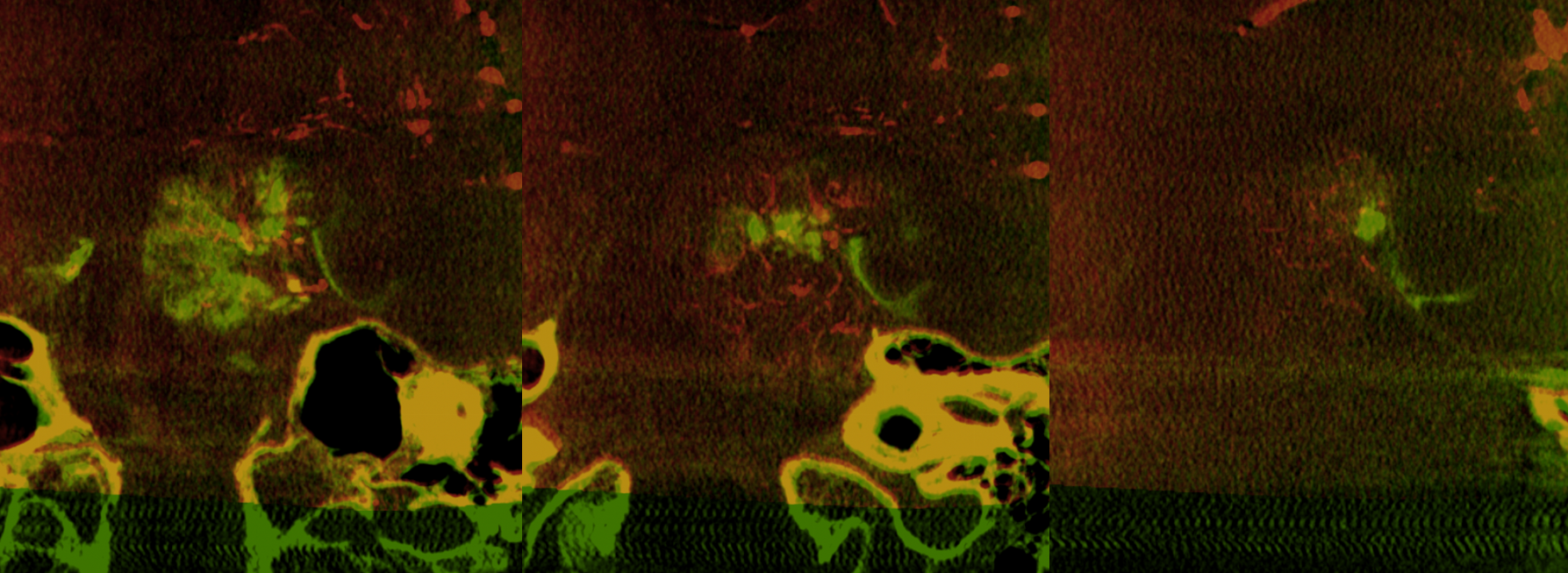
See the difference between MHT and ILT portions?
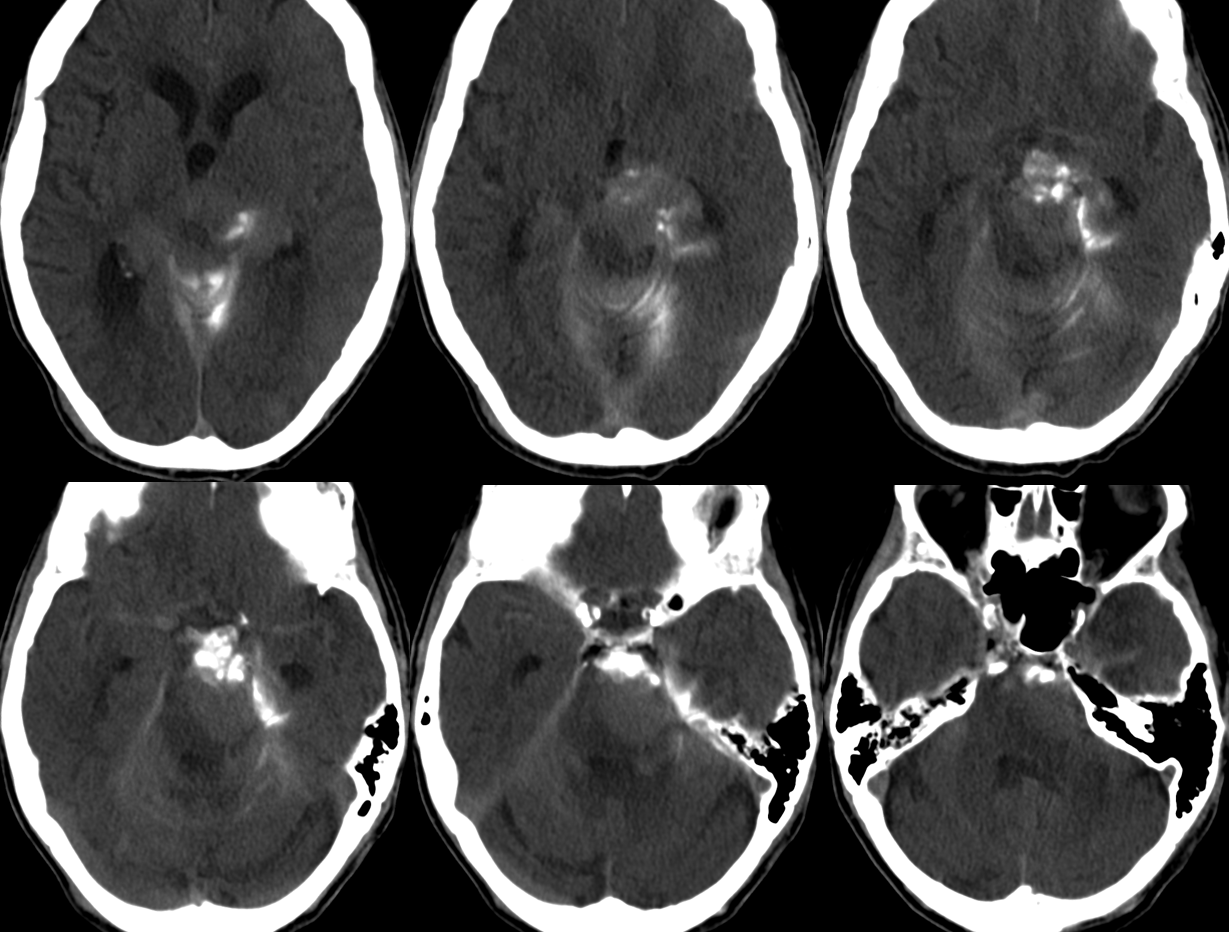
CT Post
MRI 1 day after. There are no unintended diffusion hits. The MHT portion shows avid diffusion restriction and lack of enhancement. The inferior part, supplied chiefly by the ILT, is alive. It is very rational.