
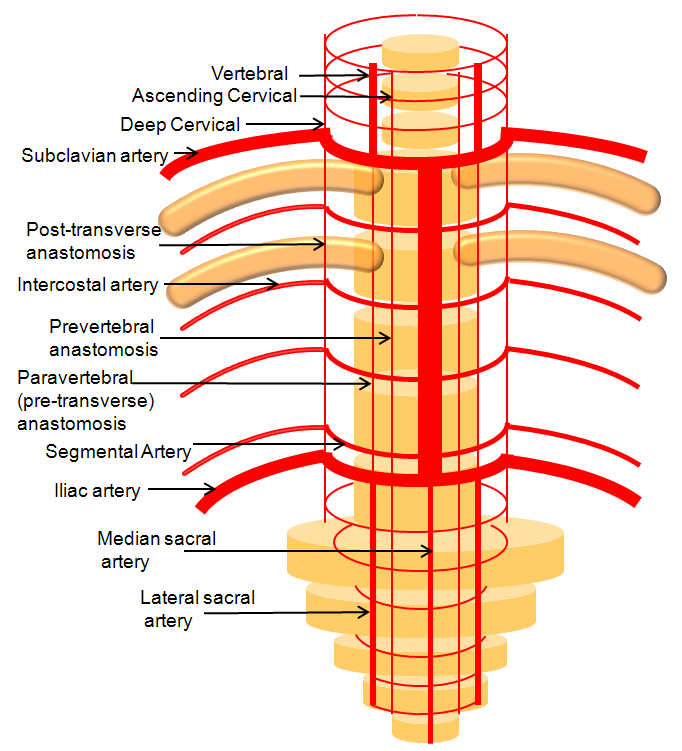
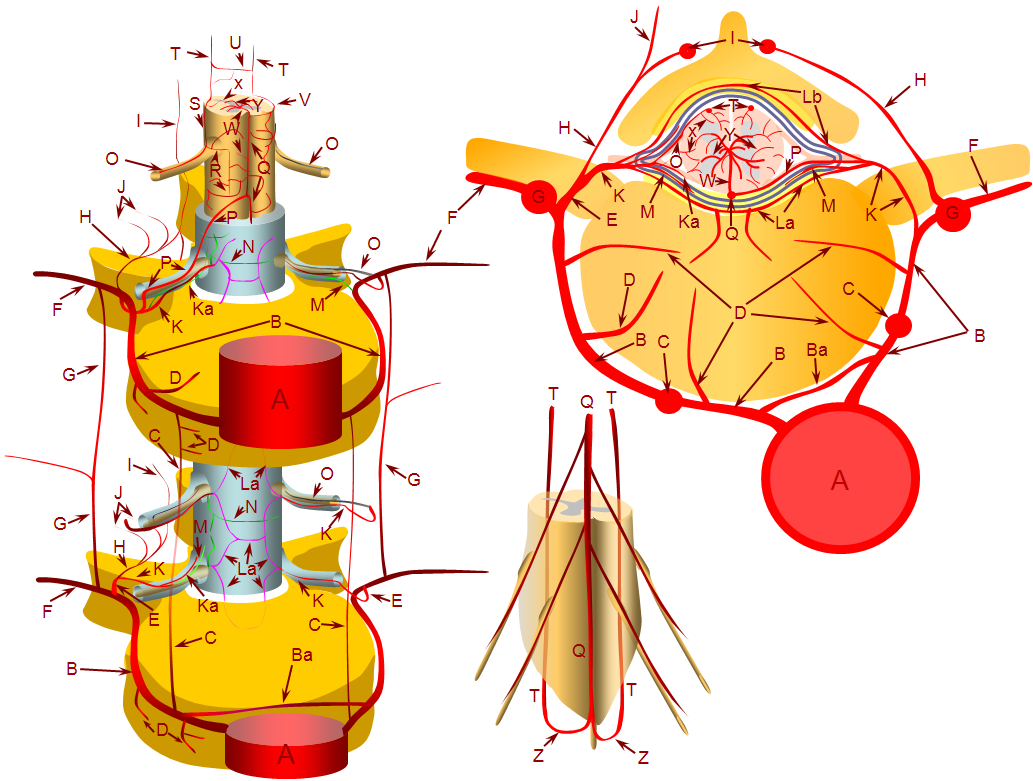
This important artery participates in supply of upper thoracic vertebral elements located above the aortic arch. Below the arch, while we have the aorta, each metamere (osseous, neural, muscular — vertebrae, nerve roots, ribs etc) is supplied usually by its dedicated segmental artery. These transverse arteries are connected by numerous longitudinal anastomoses — like pretransverse, post-transverse, etc. The basic grid-like arrangement is fundamental to understanding all vascular anatomy of brain and spine. The picture above shows the power of conceptualizing this homologous system. The vert is homologous to the prevertebral anastomosis, the median sacral to the aorta below iliac bifurcation, the lateral sacral arteries are homologs of prevertebral anastomoses below aortic bifurcation, the iliac and / subclavian vessels are just really large segmental arteries supplying legs and arms, etc. In this system, the supreme intercostal is the homolog of pretransverse anastomoses above the arch. Injecting this artery allows one to see supply to the upper thoracic vertebral bodies. Its important, as various embo targets such as fistulas and tumors can be supplied by it.
See Spinal Arterial Anatomy page for more info
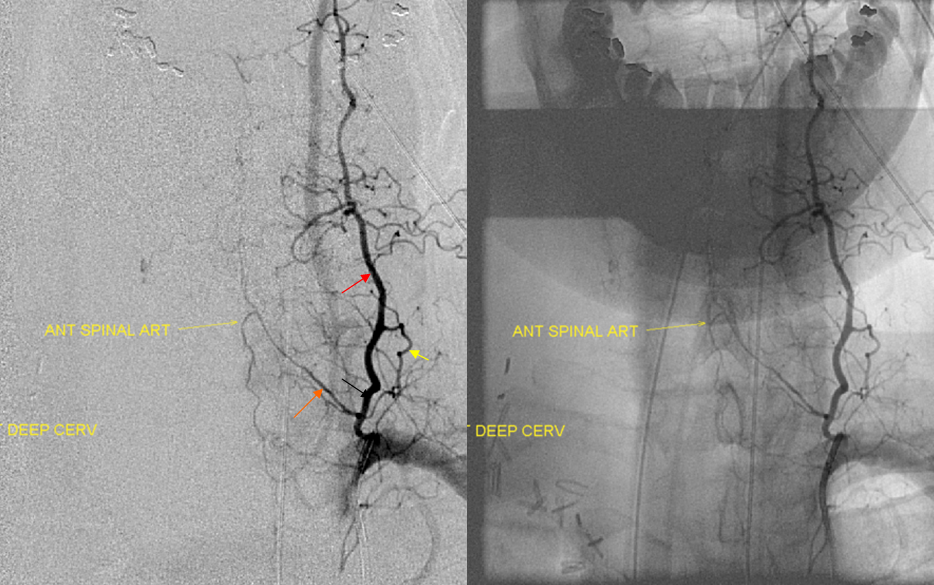
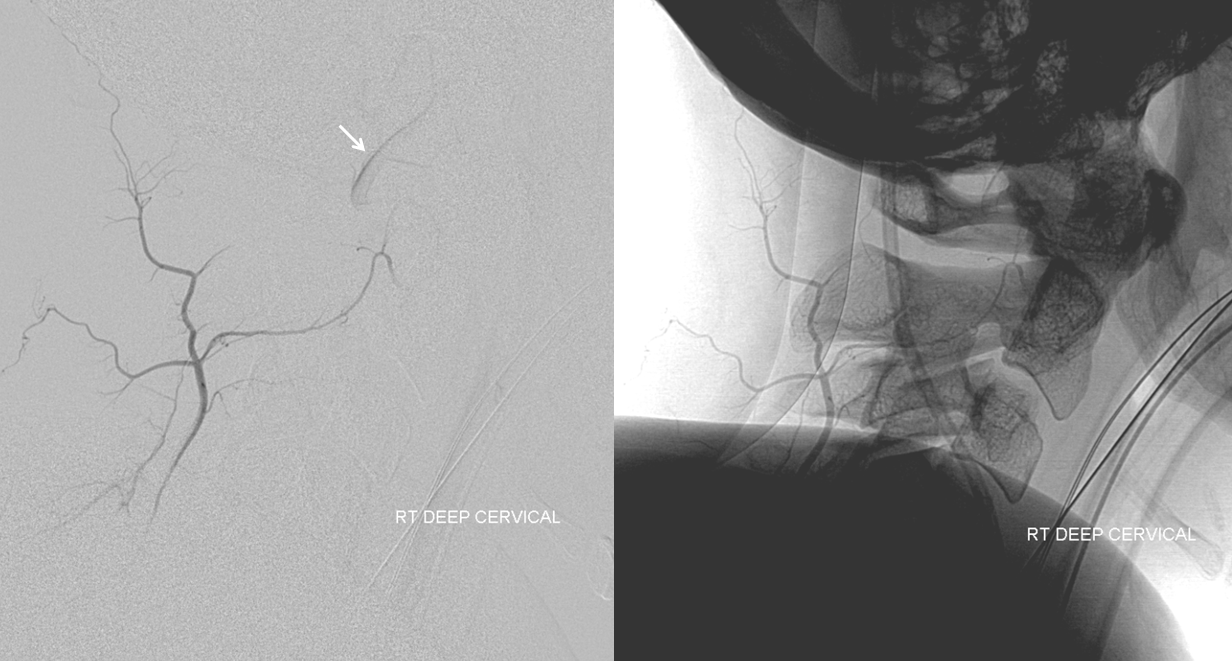
Below are images of the deep cervical artery (red), contributing to the radiculomedullary artery (orange). Notice reflux into a vessel below on the native image.
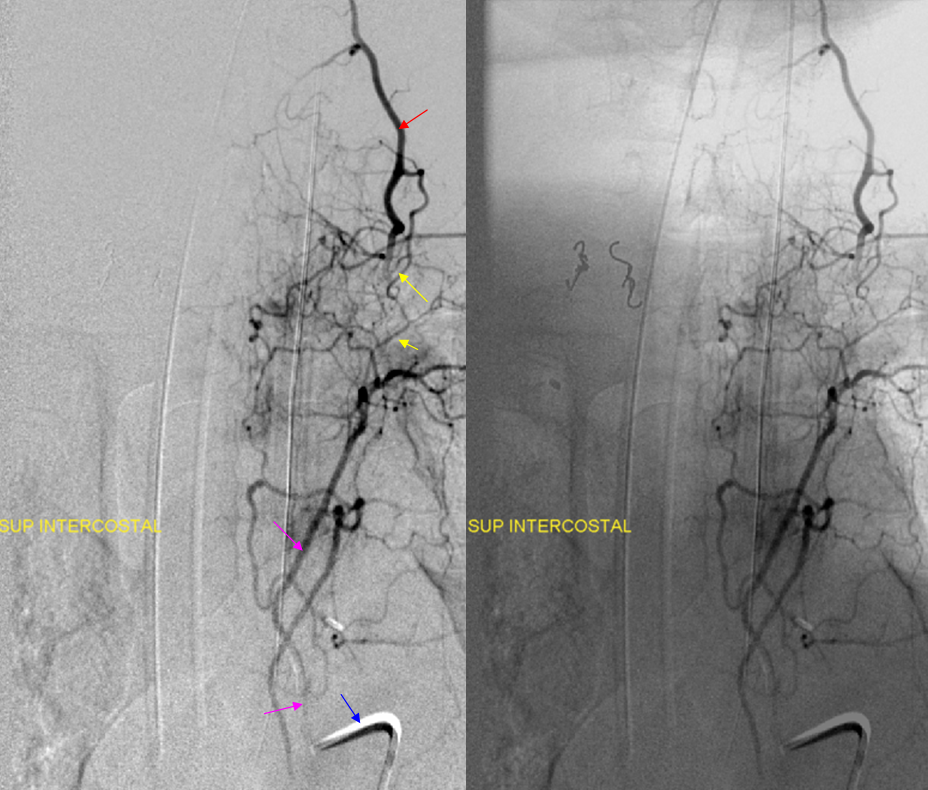
Below is an injection of he supreme intercostal artery — notice ow it opacifies the same deep cervical artery via various posterior anastomoses.



Clinical Relevance — Identification of anterior spinal artery during tumor embolization
This patient was referred for pre-operative embolization of a hypervascular metastasis in the T3 body and pedicle.

A radiculomedullary spinal artery was identified at left T7, and from the VB junction. The anterior spinal artery thus opacified was seen at the cervical and mid-thoracic levels (not shown). The upper thoracic anterior spinal was felt to be seen from the left T7 segment, however that turned out to be a visual fakeout. The tumor was supplied by the left supreme intercostal artery:
The tumor was duly embolized with particles and closing the pedicle with (thankfully) detachable soft coils (to slow down particle washout). Here is a post-embolization angiogram:

The frightfully large radiculomedullary artery (red), with its superior (pink) and inferior (purple) anterior spinal artery limbs, was completely missing on the pre-embolization injection. Why? The answer is the same as in Case 1 — the flow in the radiculomedullary, despite its size, was only a small fraction of the total flow due to the hypervascular nature of the tumor, probably somewhere on the order of 5% of total flow. Thankfully, the majority of embolization was carried out with the microcatheter distal to radiculomedullary origin, in line with our practice of as complete an embolization as possible. Proximal deposition of particles would likely have resulted in clinically significant anterior spinal artery embolization. Nevertheless, the coils are seen protruding into the priximal radiculomedullary branch (white arrow).
About 20 minutes later, the radiculomedullary artery is closed:

Angiography of left T7 segmental artery and vertebral artery show no adequate collateral reconstitution of the area. The coils must be removed, and through some persistent and skillful manipulation of snares, alligator, and buddy wire by Dr. Peter Kim Nelson, they are finally retrieved.

A Trascend-14 wire is then placed into the radiculomedullary artery to push the thrombus off to the side of the vessel. The post-salvage angiogram demonstrates re-establishment of left supreme intercostal radiculomedullary patency:

This is no guarantee that no damage is sustained, of course. The patient awoke completely intact, which is as much luck as skill, to my take.
Conclusion: ALWAYS make sure to demonstrate anterior spinal artery at the level of embolization when hypervascular lesions are the target. If that cannot be done, one must assume that the radiculomedullary contribution is coming from the pedicle to be embolized, and cannot be visualized because of flow competition. In other words, it is not enough to show that the pedicle to be embolized apparently does “not” supply the radiculomedullary artery — it very well may, you simply can’ see it — not yet.
Case 2: Supreme intercostal origin of right vertebral artery

A rare but sometimes critical anatomical variant to know (See Aortic Arch — A Guide to the Perplexed for more).
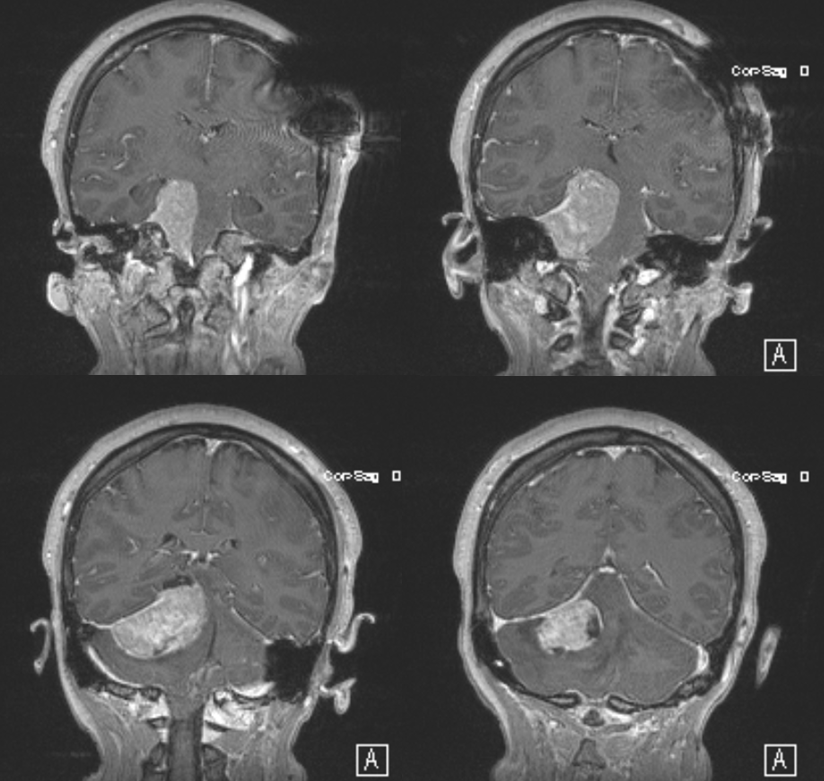
Sometimes you need to find that right or left vert and its not enough just to inject everything else. This patient presents for preoperative angiographic evaluation
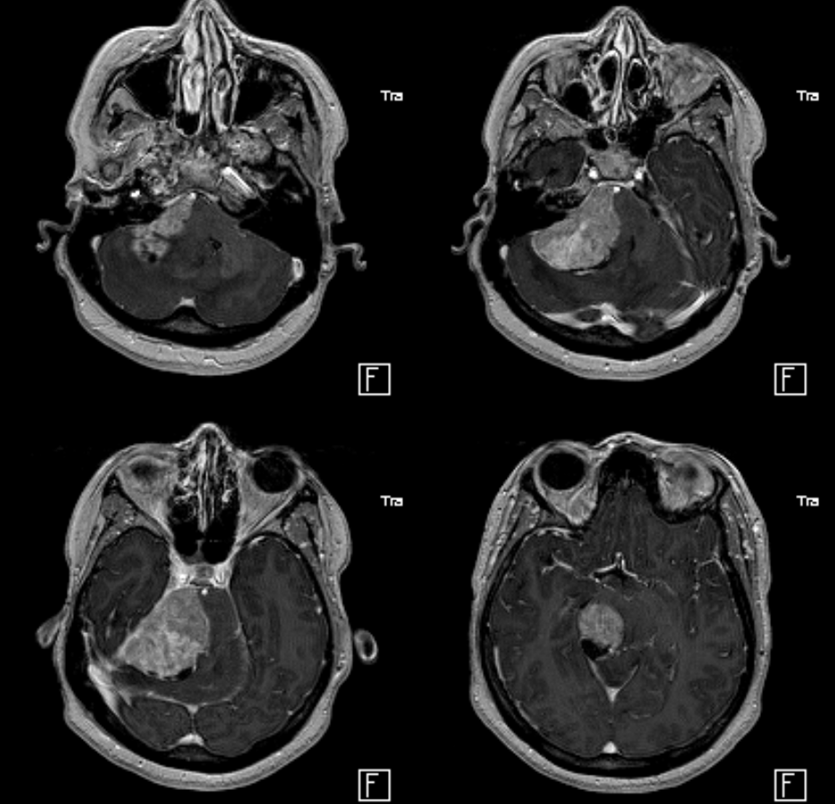
It is essential to find the right vertebral artery, for many reasons.
Here is the left, notice reflux into hypoplastic distal right vert (arrow)
The vert is not found in its usual location

An injection of the right deep cervical artery shows transient opacification of the vert (arrow) via the C2 muscular anastomosis; we know the vert is there
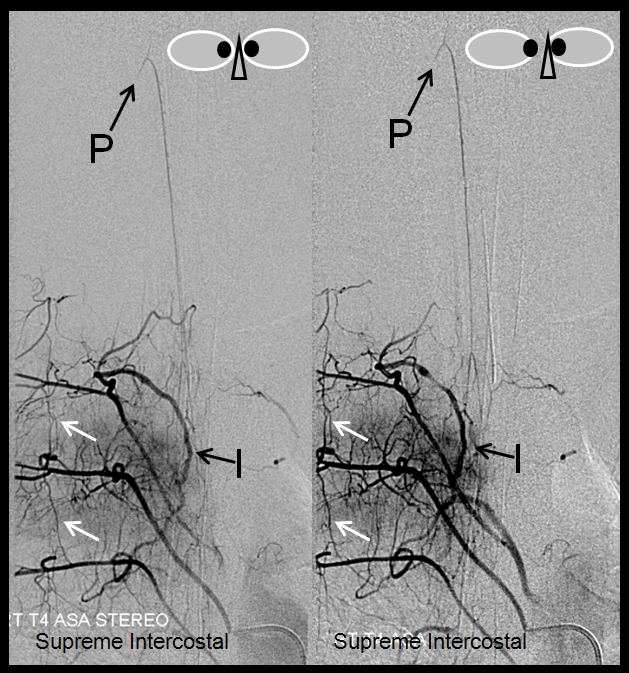
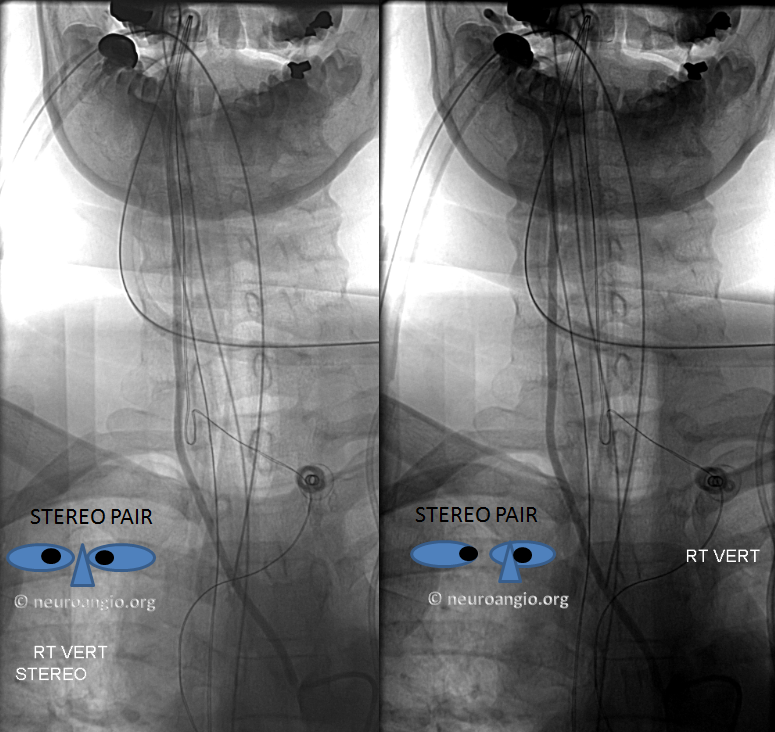
Where is it? The answer is aortic arch. When the right vert is apparently missing in action, the origin is usually in the upper thoracic descending aorta — at the supreme intercostal artery
Stereo views are below
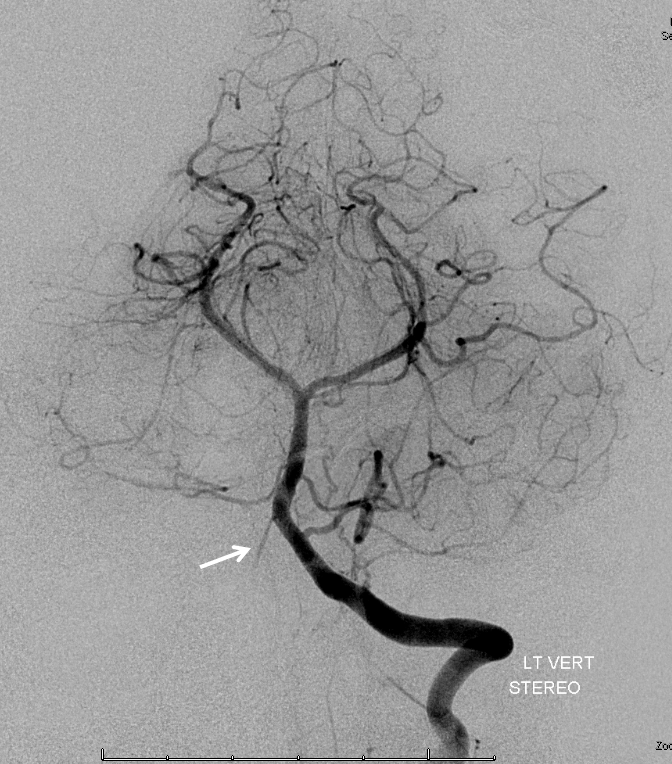
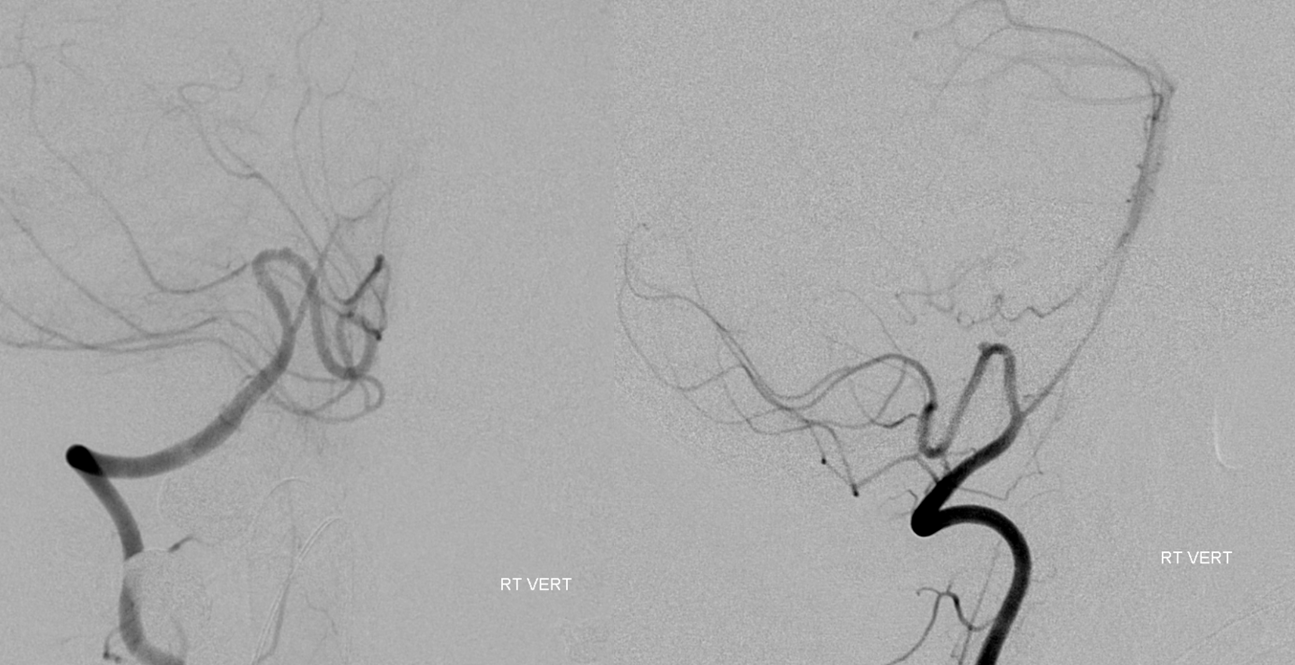
Distal vert images prove the usefulness of finding this vessel. Notice anterior spinal artery origin from the distal intradural vert (above the PICA), and a small aneurysm at the apex of the medullary PICA loop.
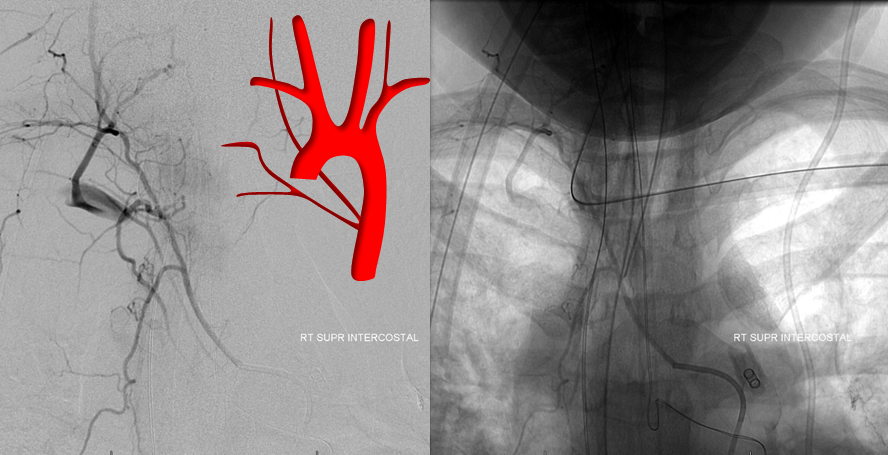
The vert appears to come off by itself. However it is not the case — the rest of the supreme intercostal trunk is just a small turn of catheter away. Notice how the supreme intercostal supplies the T1 intercostal artery and anasomoses with the proximal deep cervical artery, transiently opacifying the subclavian.
See Aortic Arch — A Guide To The Perplexed for other arch variants also