


The cavernous sinus is, at least from the angiographic perspective, a metaphysical entity. It is a collection of extradural venous compartments, often functionally separate, which altogether constitute the venous space we have come to regard as a distinct anatomical structure. It is critical for the neurointerventionalist to understand this, because his or her treatments will be, of necessity, targeting these varied and sometimes complex subspaces. Almost everything about this structure is defined by variability — size, extent of compartmentalization, inflow and outflow sources — not to mention its embryology — thus making for a fascinating topic. The classic story is written and illustrated best by the immortal Albert Rhoton — it is a squarely neurosurgical perspective and a must read even for those who need not make a new hole to get inside the head (click here for amazing 3-D videos, the passion for which neuroangio is proud to share).
Credit for the name goes to Jacob Benignus Winslow (1669-1760), (Jacques Benigne Winslow, s’il vous plaît) who writes “The cavernous or lateral Sinuses of the Os Sphenoides are Reservatories of a very particular kind, containing not only Blood, but considerable Vessels and Nerves, as we shall see hereafter; and likewise a spungy or cavernous substance full of blood, much like that of the Spleen or Corpus Cavernosum of the Urethra.” The name stood the test of time. According to dictionary.com, cavernous means “deep-set, containing caverns, full of small spaces”.
For our purposes, the cannon holds that cavernous sinuses are paired, non-urethral dural venous structures located between the sella and Meckel caves, joined by the intercavernous venous plexus, and each individually connected to the superior opthalmic vein, the sphenoparietal sinus / superficial Sylvian veins, the superior and inferior petrosal sinuses, the pterygopalatine venous plexus, and the clival venous plexus. Each sinus contains a variable number of septations which may separate it into functionally distinct compartments. The anatomy of cranial nerves related to the sinus is well-described in a myriad places elsewhere — again Rhoton’s works being the #1 reference in my opinion — and there are many others besides, for those who shun being persons of one book.
Embryology
Now should be time to offer a suggestion, especially for the reader reactively self-assessed to the “practical” camp — to look for good clinical value in embryology. Yet the classic story of cavernous sinus development is checkered and inconsistent, in my opinion. The main sources are Dorcas Padget — a brilliant researcher and illustrator, whose work remains essentially intact today, and likely to remain so for as long as tiny human embryos are no longer dissected for gross anatomical knowledge; and George L. Streeter — Padget’s predecessor and author of seminal works using the Carnegie embryo collection.
The cavernous sinus develops very early (10 mm embryo) primarily acting as a receptacle of orbital and facial venous drainage (future superior ophthalmic vein). In this way, it comes into existence and forever remains an extradural entity — Padget holds that at birth the cavernous sinus does not participate in drainage of the cerebral hemispheres (via the Sylvian veins) — the connection between such veins and sinus maturing later. This view explains for example why the superior ophthalmic vein is always connected to the cavernous sinus, while the Sylvian veins may or may not be. Others, notably Prof. Raybaud, hold that de novo connections should not evolve for either arteries or veins at this late point in development and somehow the theory will have to be modified to explain the fact of an already-existing brain-to-sinus anastomoses. Additionally, there is disagreement about the role of the so-called sphenoparietal sinus vis a vis both cavernous sinus and the sylvian veins. The classic viewpoint holds that the sphenoparietal sinus evolves from a very early structure called the tentorial sinus which drains the developing cerebral hemispheres. Phillipe Gailloud et al, however, based on specimen and literature analysis (including original manuscripts by the likes of Brechet, Trolard, and others), believe that the sphenoparietal sinus does not in fact exist, and the Sylvian veins drain directly into the cavernous or paracavernous sinus (more on the latter later). The Gailloud viewpoint seems like the better one when angiograms are analyzed with unprejudiced eyes.
My very unproven opinion, to the propagation of which i am entitled by claim of authorship, holds that variability in form and function stem from the physiologic and anatomical location of the cavernous sinus at the crossroads of intra- and extra-cranial venous drainage. Phylogenetically, there is tremendous variability in venous drainage patterns of the intra-and extra-cranial tissues, depending on relative size of the brain to that of the head, the size and position of the eyes in the skull, preference for internal vs. external jugular systems, etc. In the human, the central anatomical location of the sinus and markedly variable development of its major tributary and drainage routes on an individual basis cannot but produce tremendous variation.
The practical lesson of embryology is to appreciate that the cavernous sinus is best understood not by regarding it as a static entity but as a receptacle of varied inflow and source for varied outputs. To understand each cavernous sinus we must understand its unique inputs and outputs. This is a distinctly hemodynamic view, which is complementary to Rhotons.
STATIC ANATOMY
Major Tributaries:
1) Superior Ophthalmic vein — typically flows into the sinus, but can easily reverse in cases of overall intracranial or specifically cavernous sinus hypertension
2) Sphenoparietal sinus — draining superficial Sylvian veins into the sinus. See discussion below on whether or not a sphenoparietal sinus really exists or whether Sylvian veins drain directly into the sinus.
3) Basal vein of Rosenthal — its first segment, when connected to the CC, typically flows into it, but easily reverses flow in cases of fistula, etc.
4) Petrosal or bridging veins of the prepontine / cerebellopontine angle cisterns
Major Egress:
1) Superior Petrosal Sinus
2) Inferior Petrosal Sinus
3) Foramen Ovale, and other skull base foramina to the pterygoid venous plexus
4) Contralateral Cavernous sinus thru intercavernous channels
5) Clival (basilar) venous plexus down to foramen magnum region, and from there into jugular veins or marginal sinus.
Angiographic Visualization
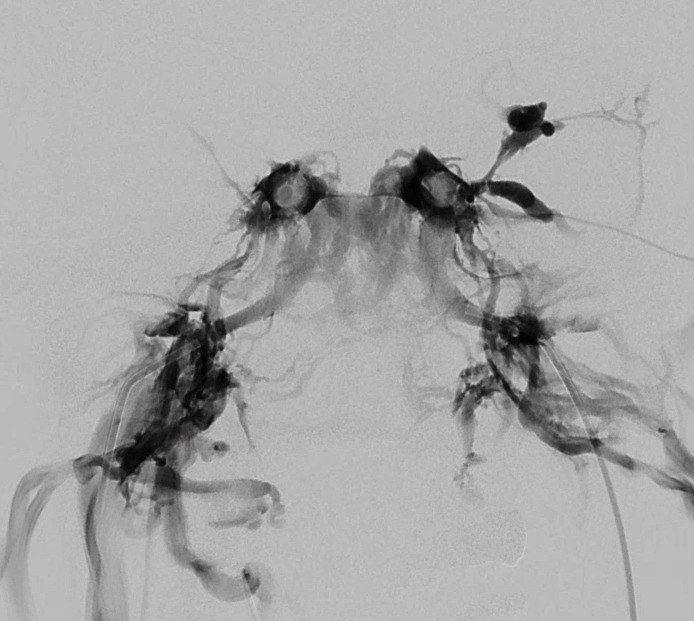
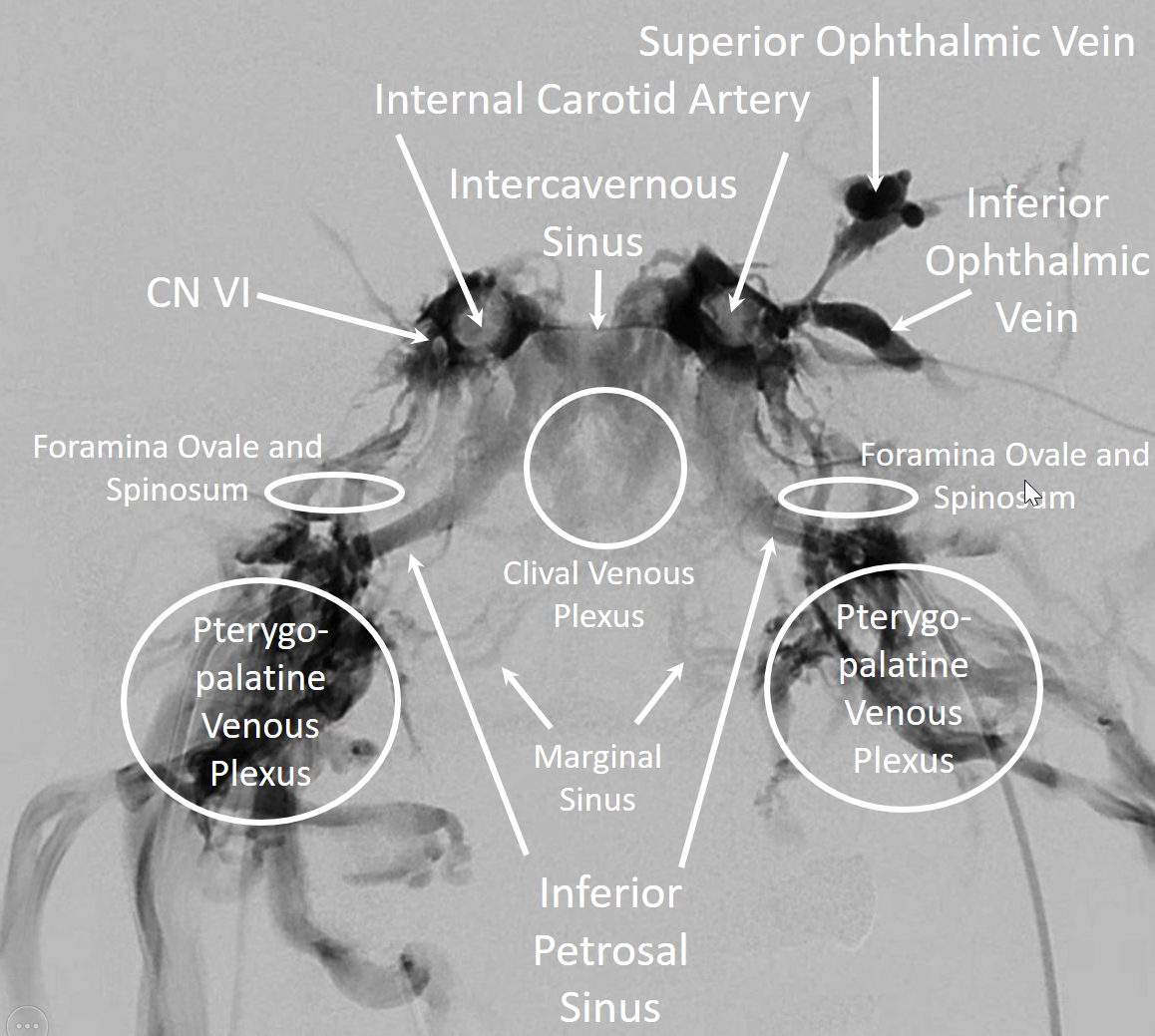
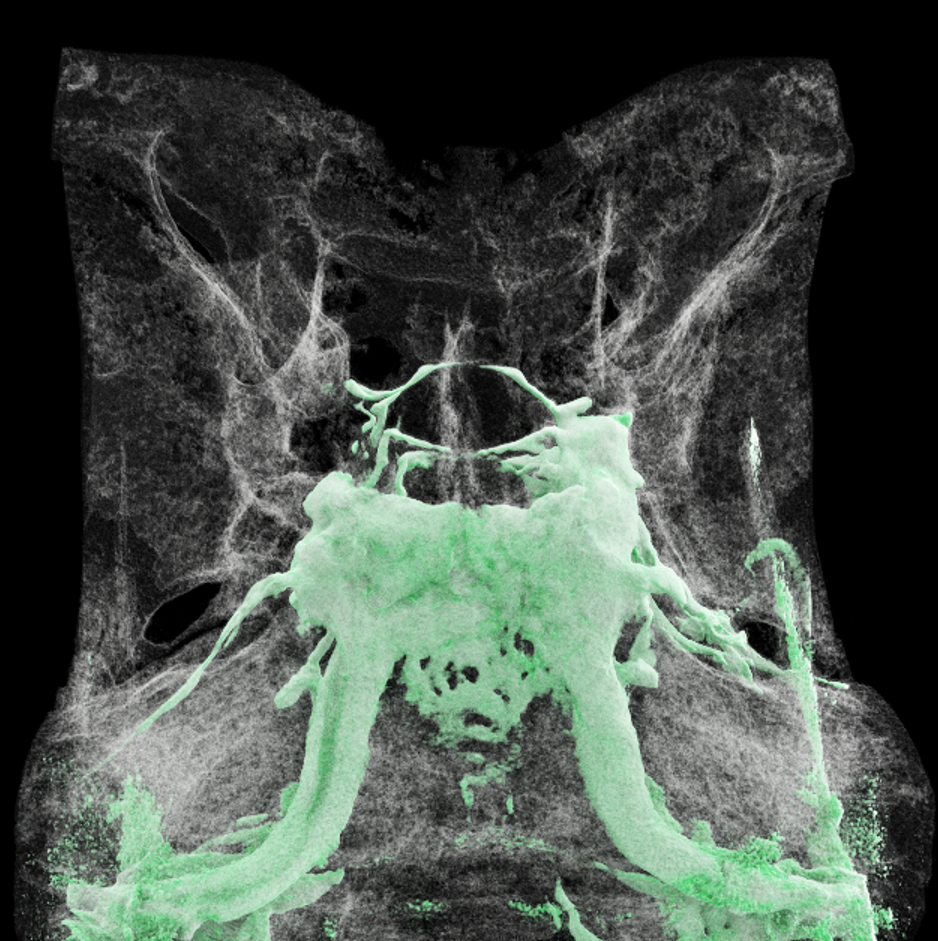
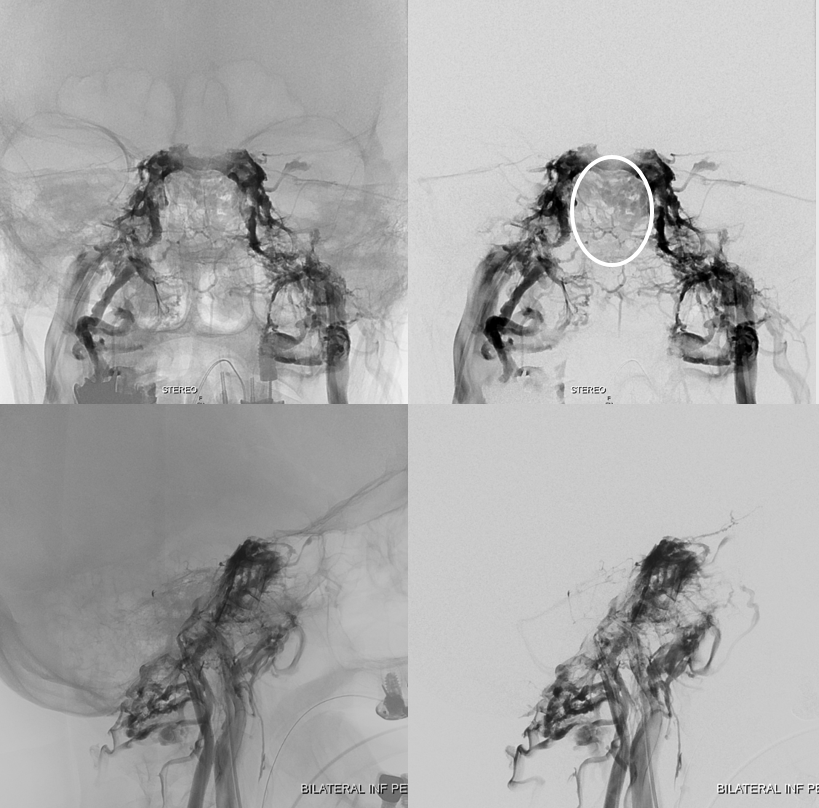
Nothing shows cavernous sinus as well as a venous injection — such as during Petrosal Venous Sinus Sampling. Look at this awesome frontal picture, courtesy of Dr. Eytan Raz
With bone

And now, with labels
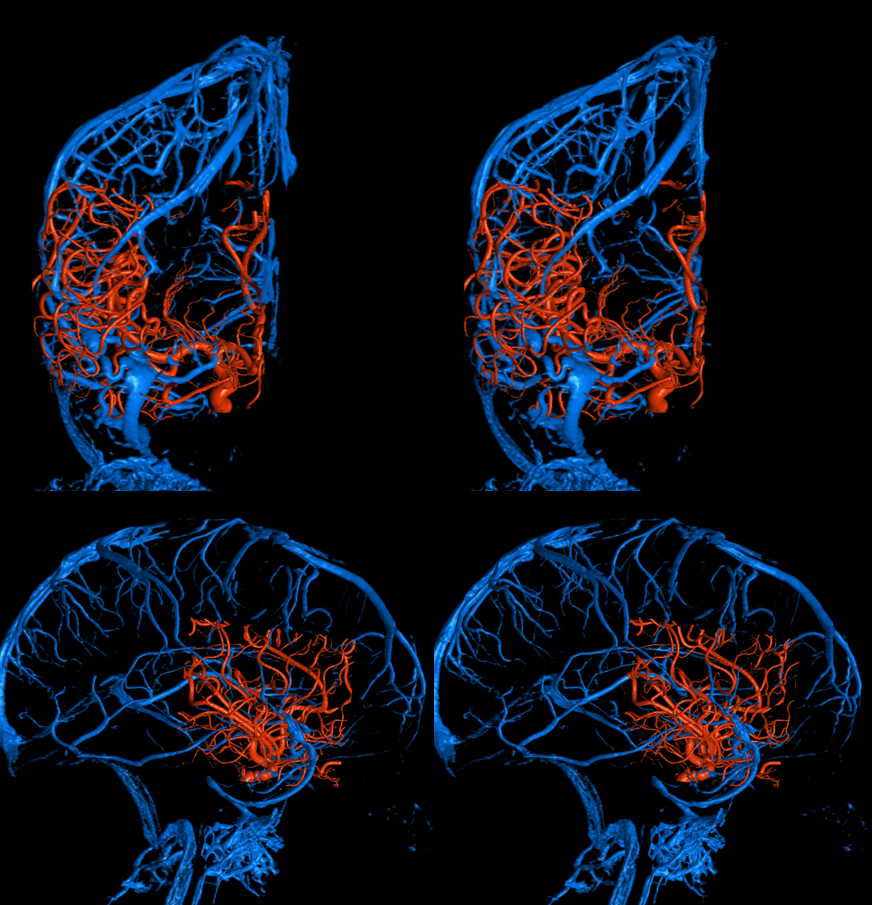
A gorgeous Cinematic Rendering by Dr. Matthew Young, of Cavernous sinus injection in context of petrosal sinus sampling.
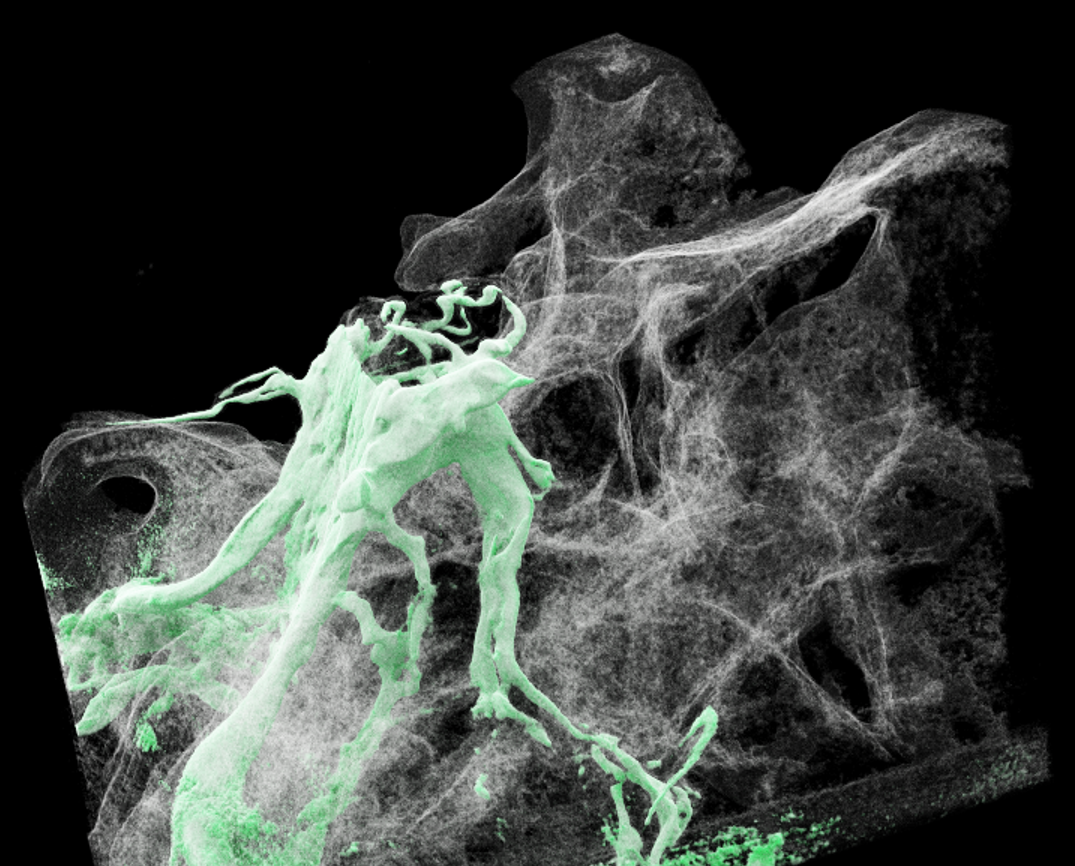

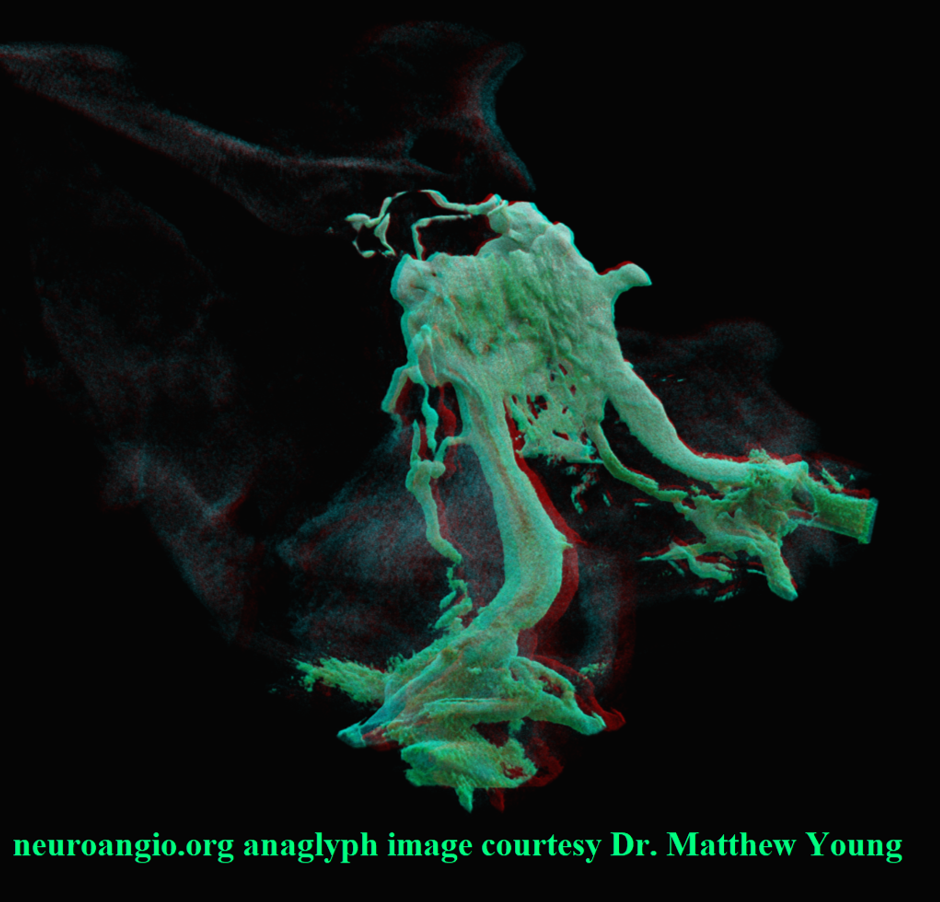
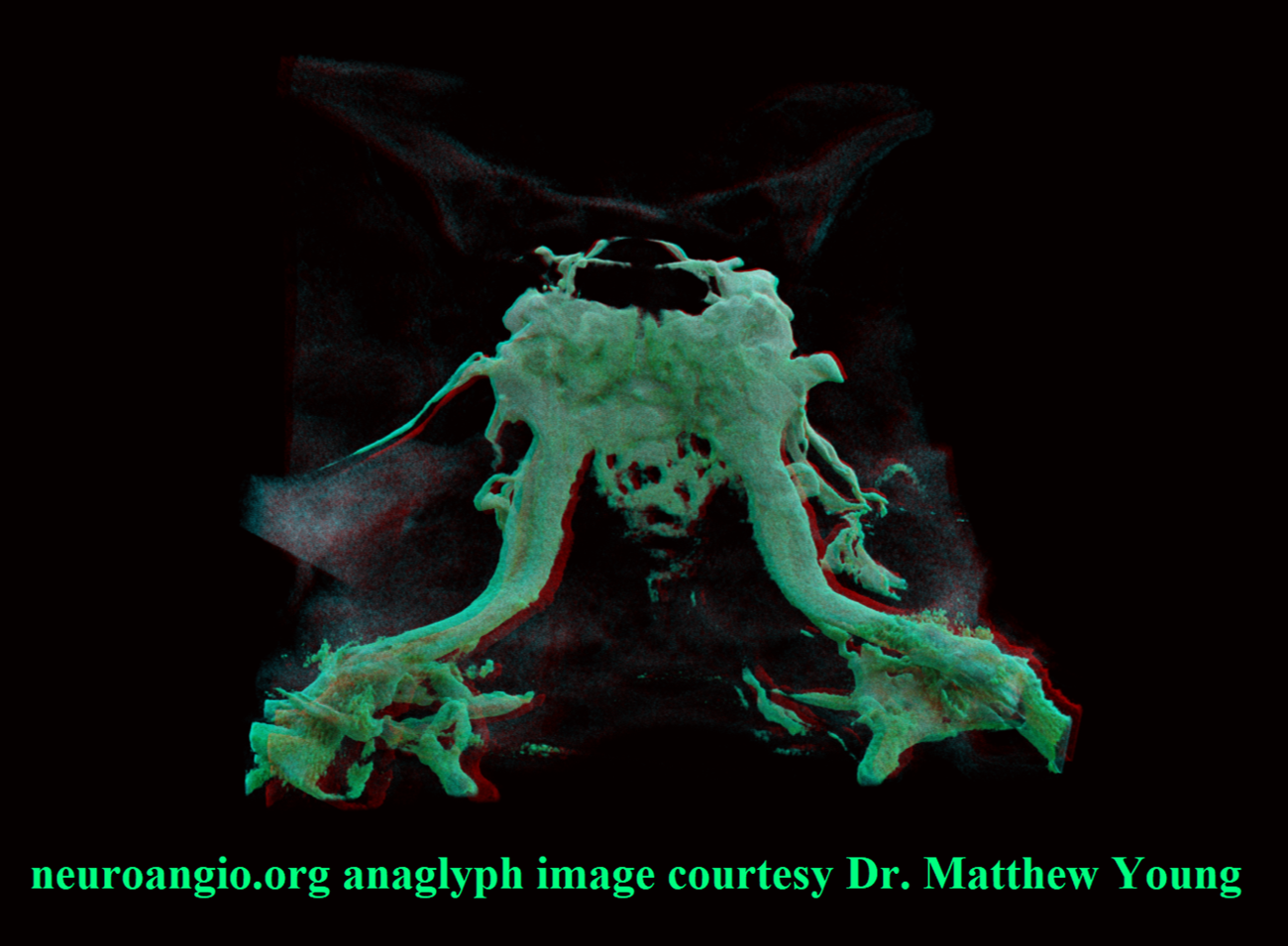
Anaglyph stereos courtesy Dr. Matthew Young
Movie of source DYNA CT for above images — tremendous amount of anatomical information there… You can stop the movie and scroll through it
Another one — bilateral inferior petrosal sinus injections
CC fistula — very large direct fistula opacifies practically all skull base venous apparatus — down to anterior spinal vein. Usually CC fistulas better show cavernous connections than IPS sampling injections because of increased pressure in the fistula more effectively overcoming competing inflows from other sources.
Movie of source data — incredible. Stop, scroll, and learn
Clival Plexus
Another Cavernous Sinus Sampling. Probably can see 100 times more veins that way than with arterial injection. In this patient, the ophthalmic venous connection is hypoplastic. Like everywhere else, variation is the rule. Here, drainage is mostly via inferior/posterior routes. No large brain connections either. The Clival plexus can be a problem surgically when approaching tumors such as high foramen magnum meningiomas in trans-clival fashion.
Movie — there is a “suboccipital cavernous sinus” nicely seen around the C1 right vert. With septations to boot…
Here it is — around the horizontal C1 vert
Another movie because its beautiful — and shows the marginal sinus and hypoglossal venous plexus a bit — the “anterior condylar confluence”
Inferior Petrosal Sinus Drainage Variability
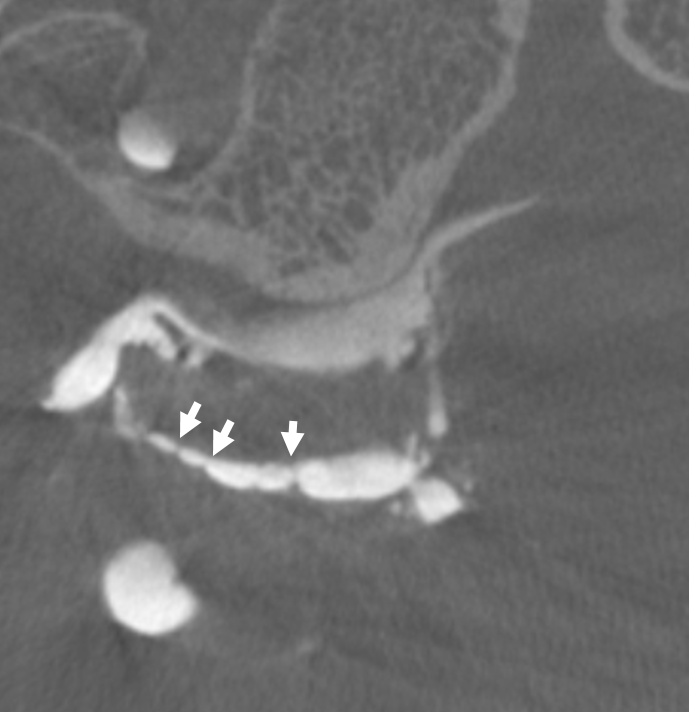
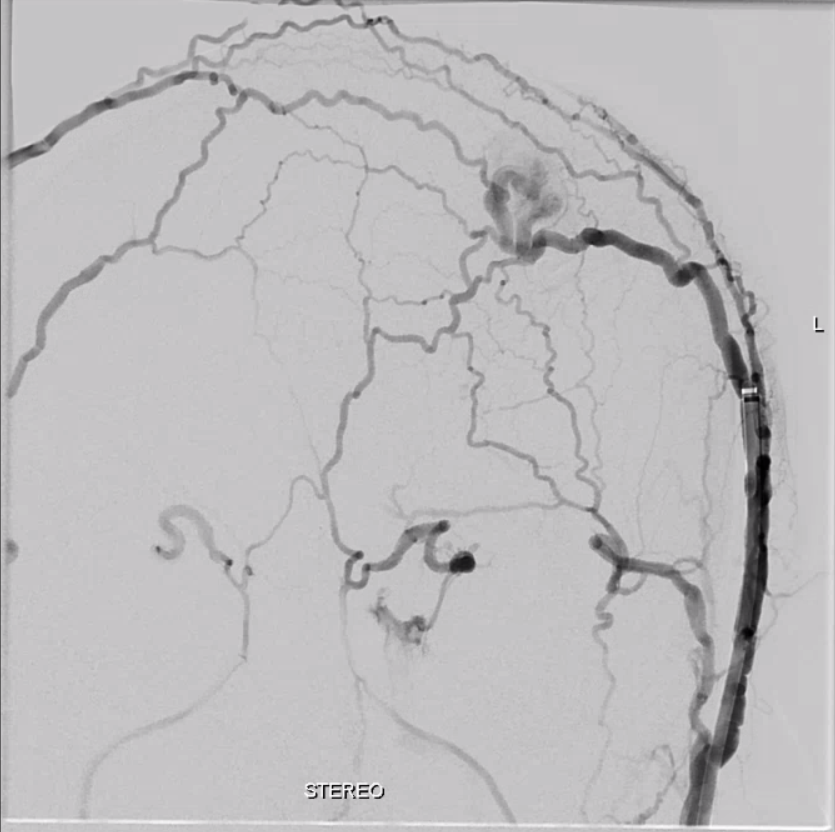
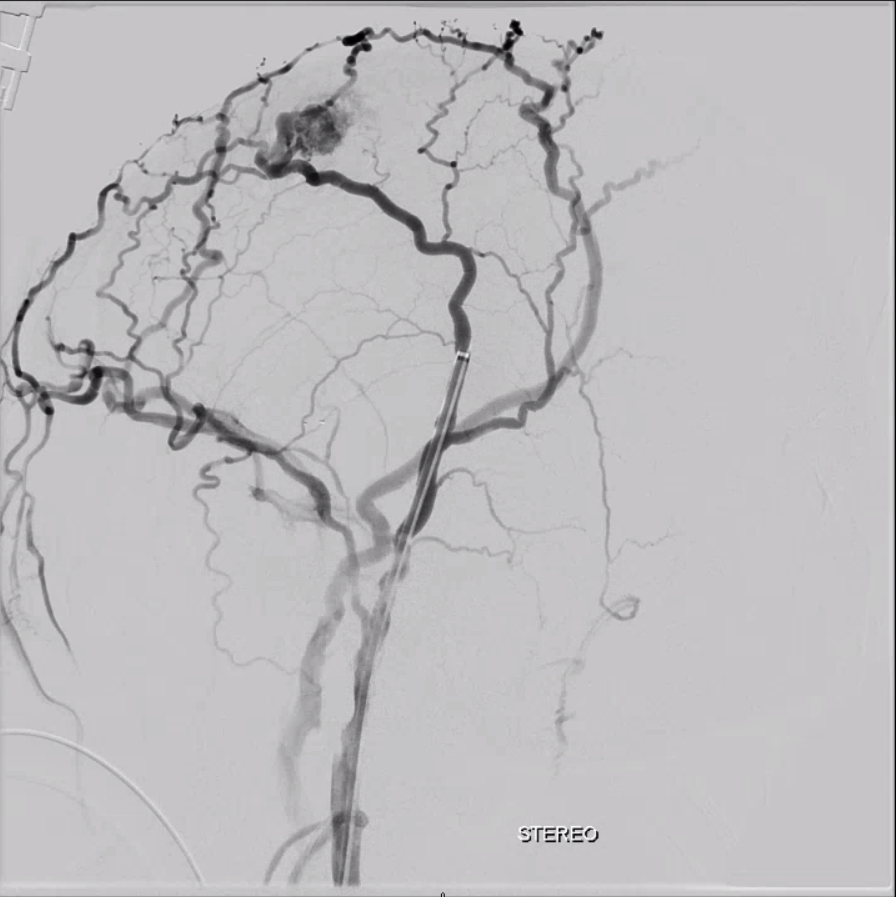
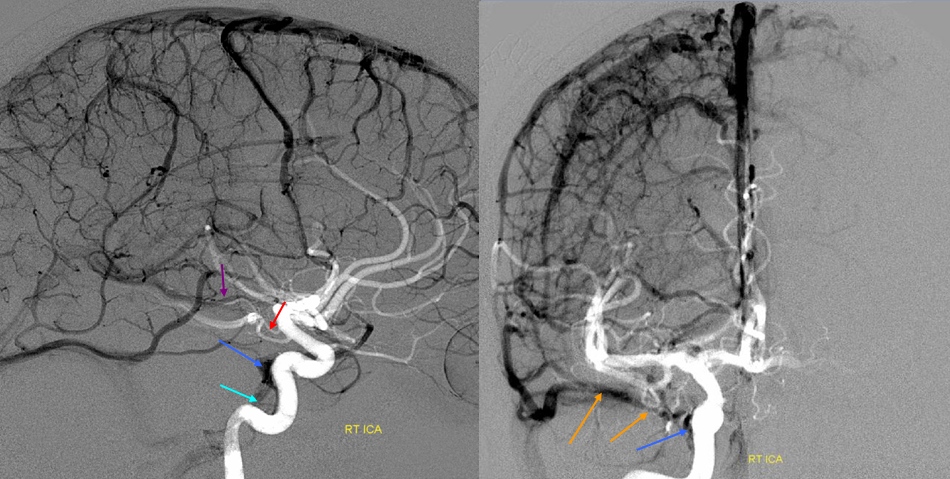
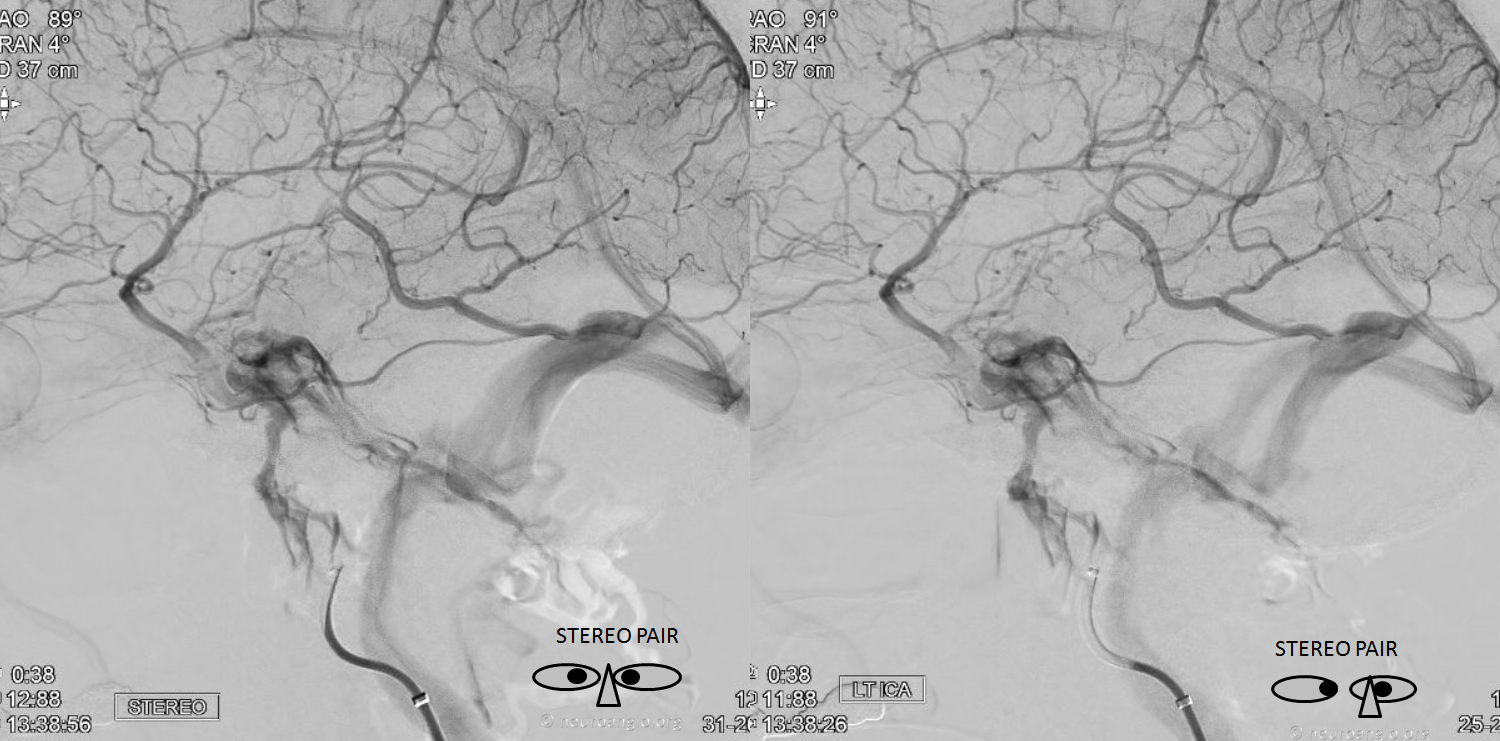
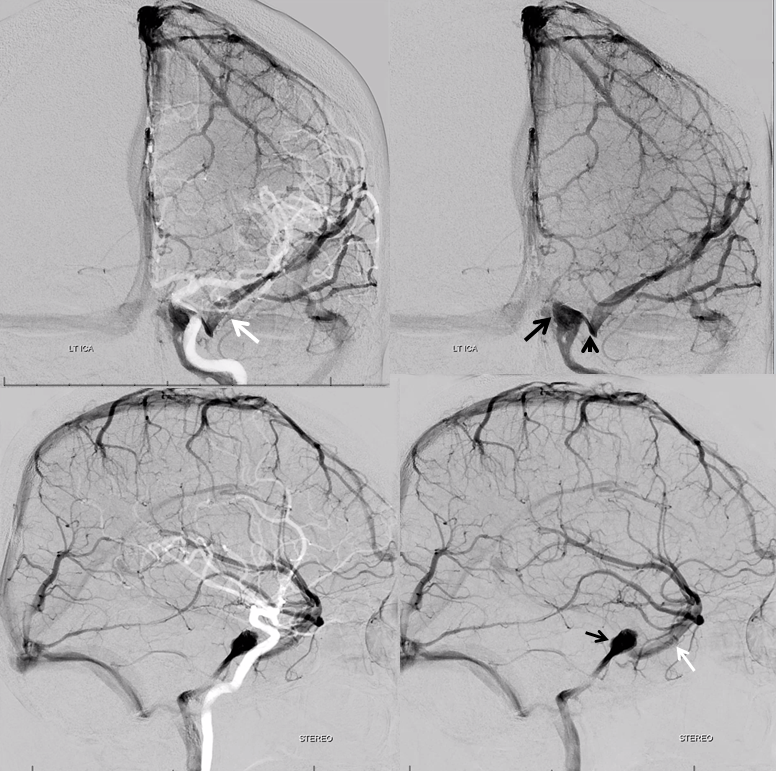
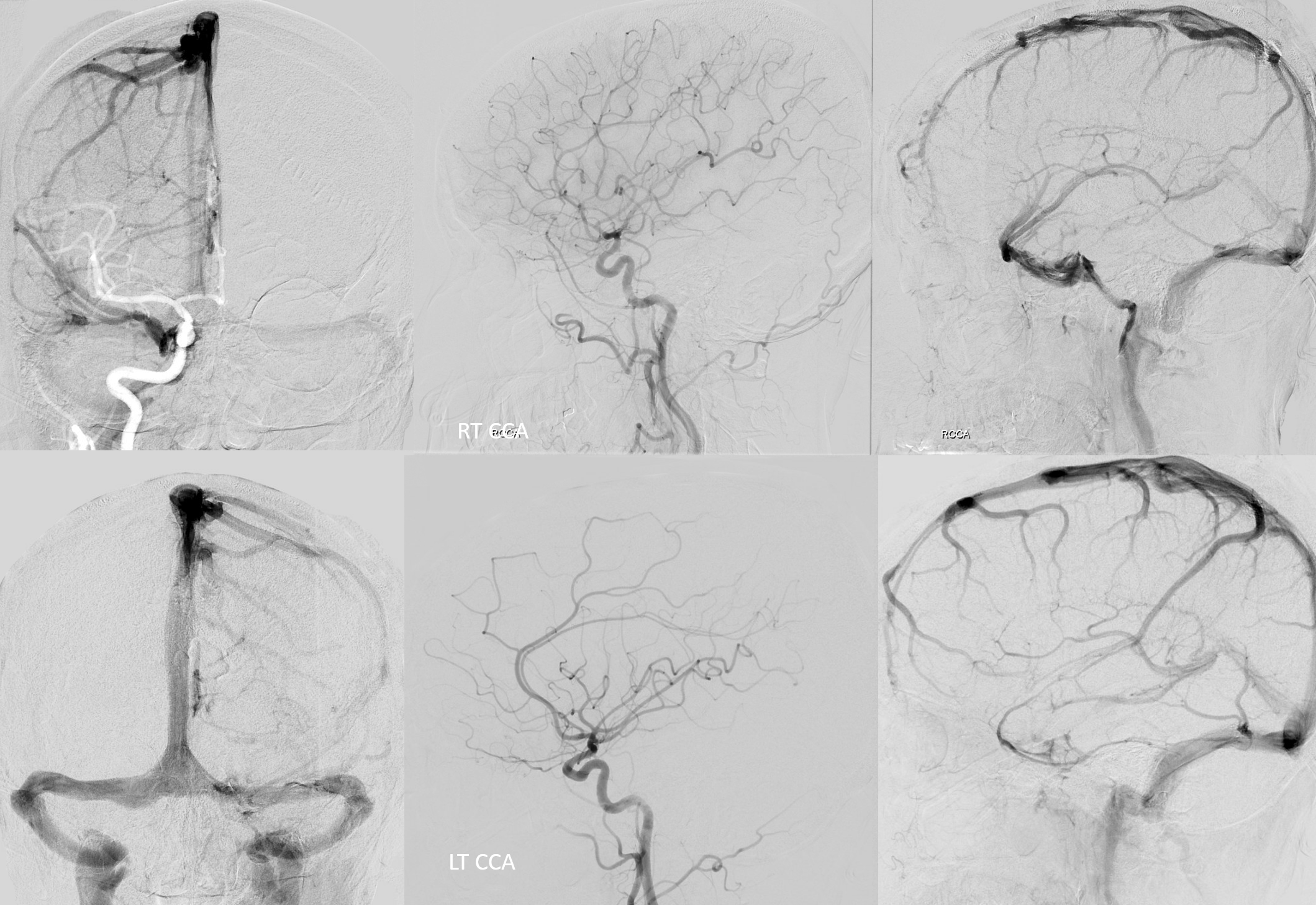
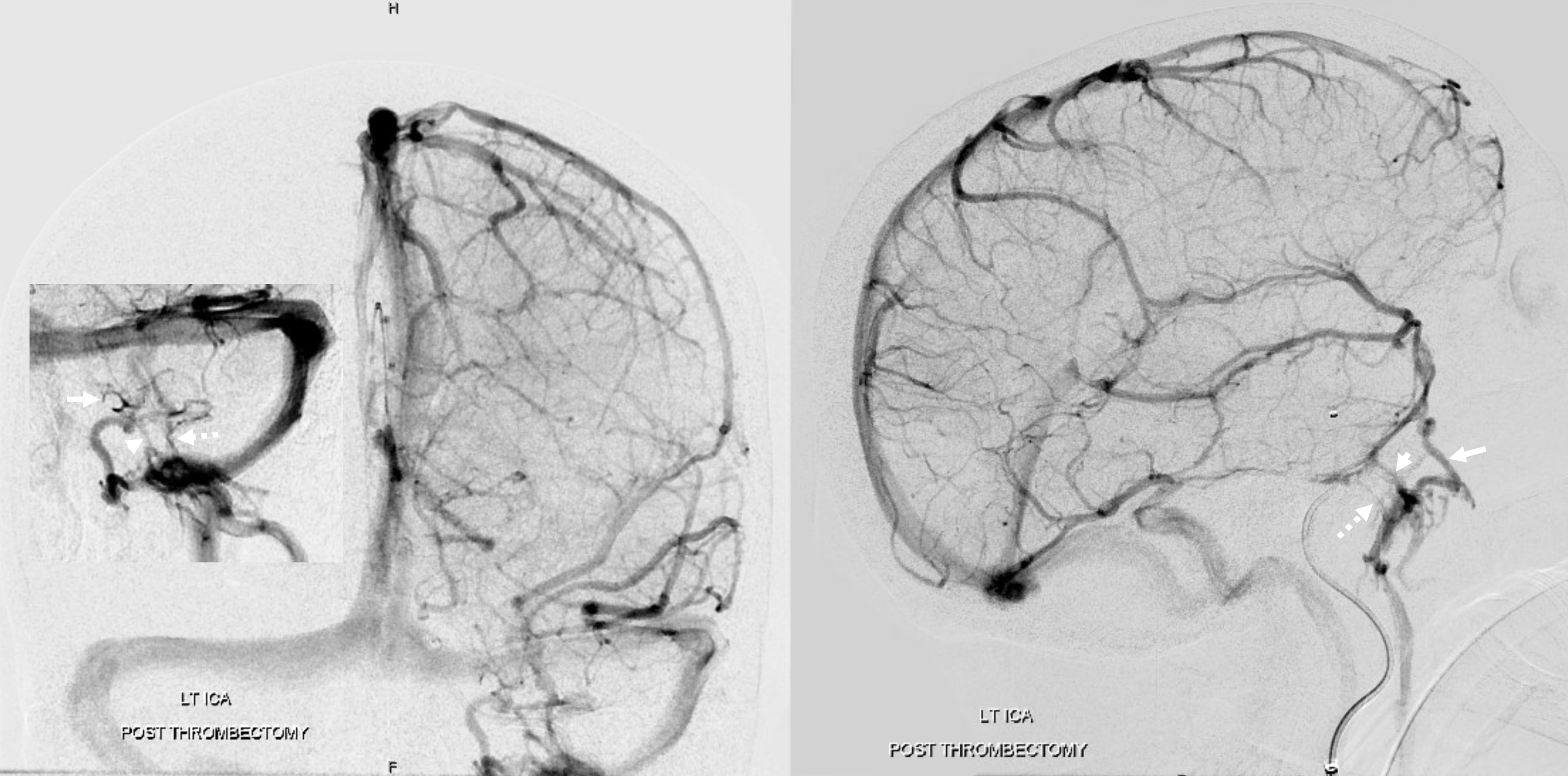
While on subject of IPS, which is the place for IPS sampling, and the standard route into the cavernous sinus for closing fistulas, etc — the classic connection is between IPS and the upper cervical internal jugular. That’s often not the case and knowing where to find it is important. Below in one individual are the two most common variants — low confluence with the jugular (left side, arrows), and alternative drainage into the vertebral venous plexus (right side, dashed arrows). Stereo pairs.

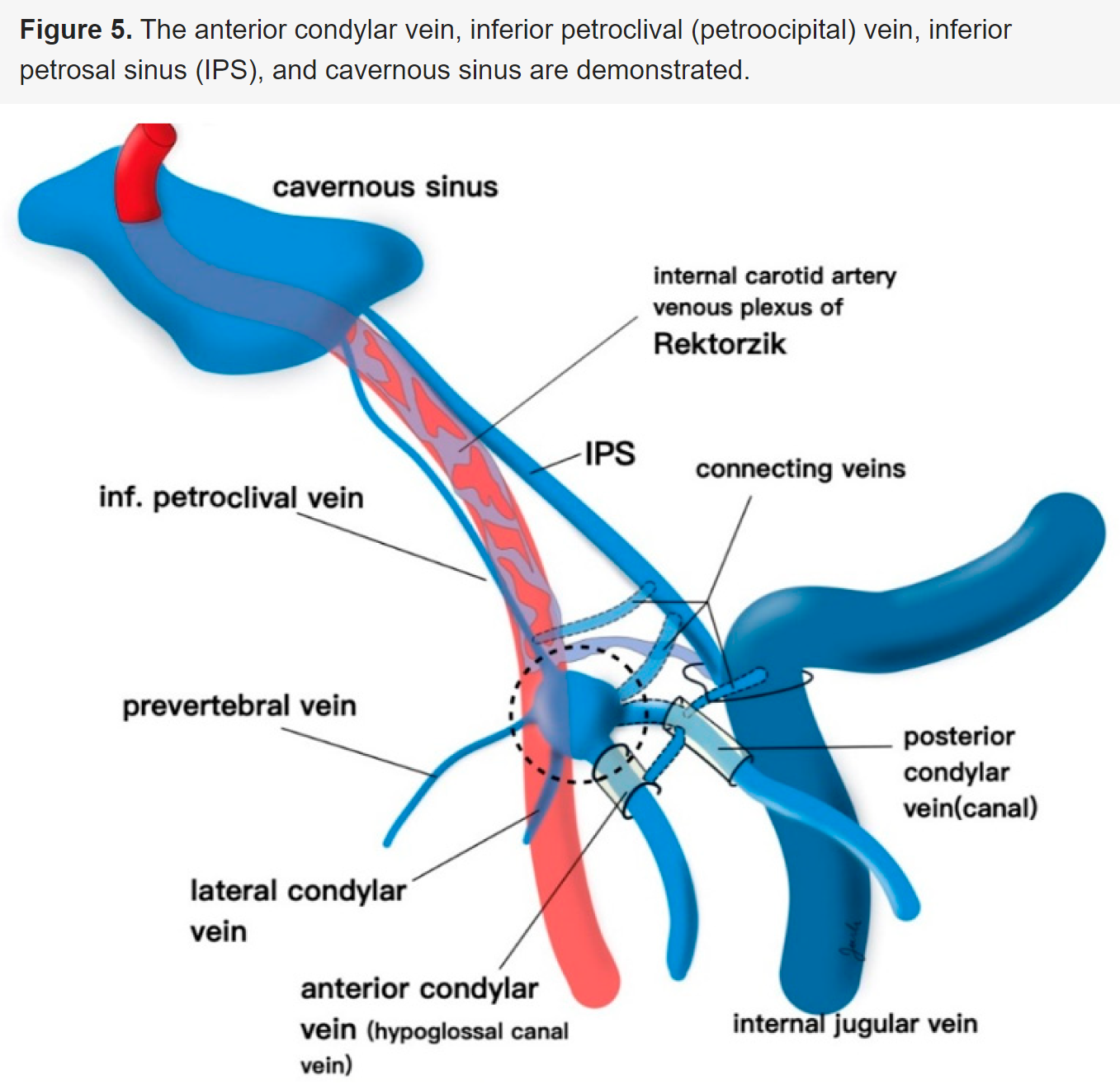
Petroclival (petrooccipital / petro-occipital) Venous Plexus
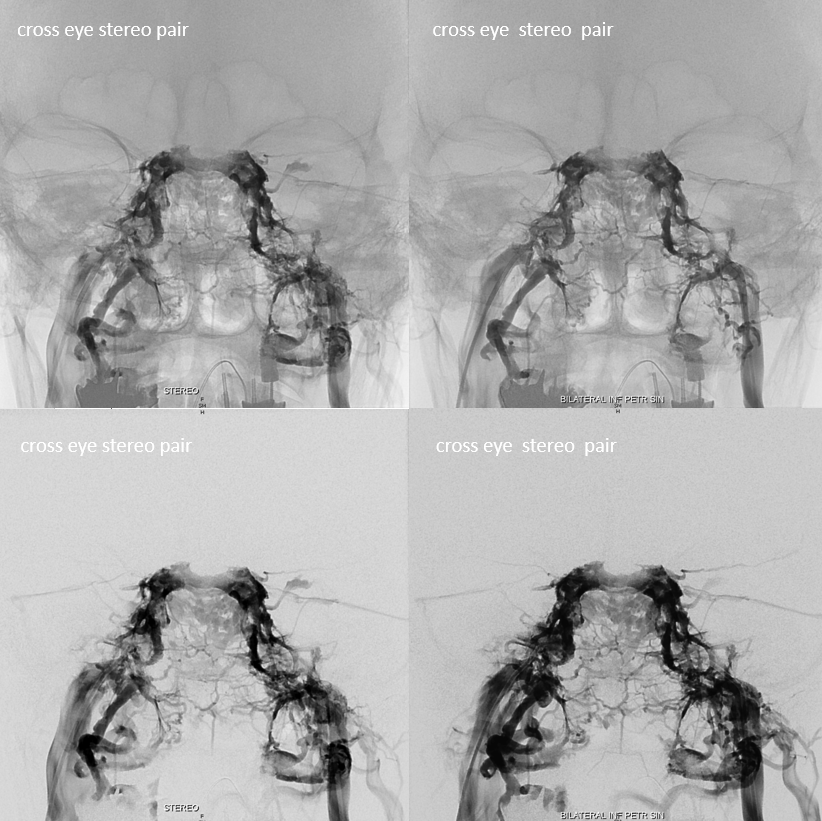
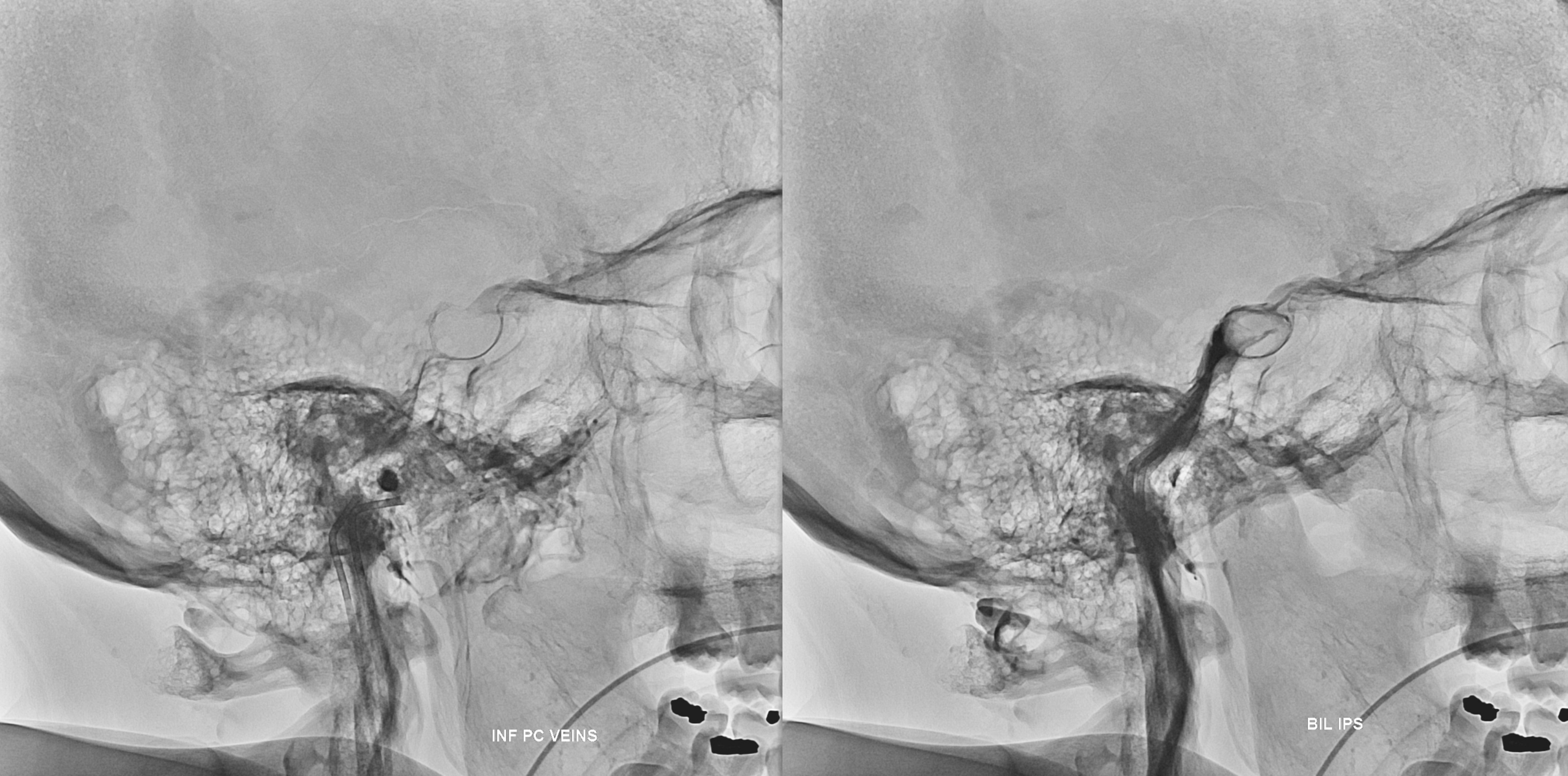
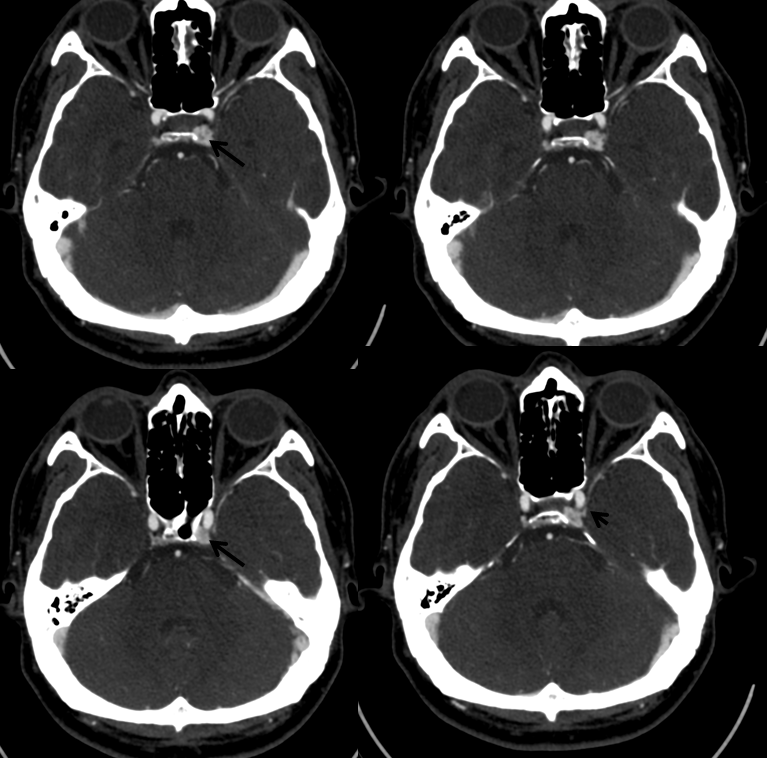
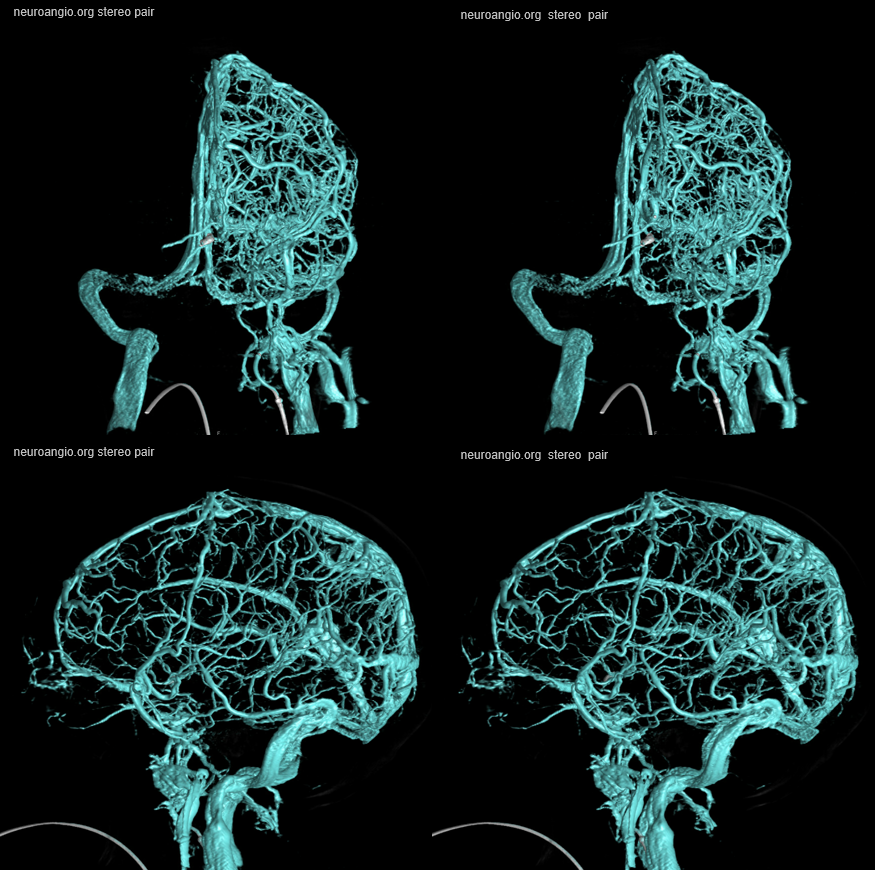
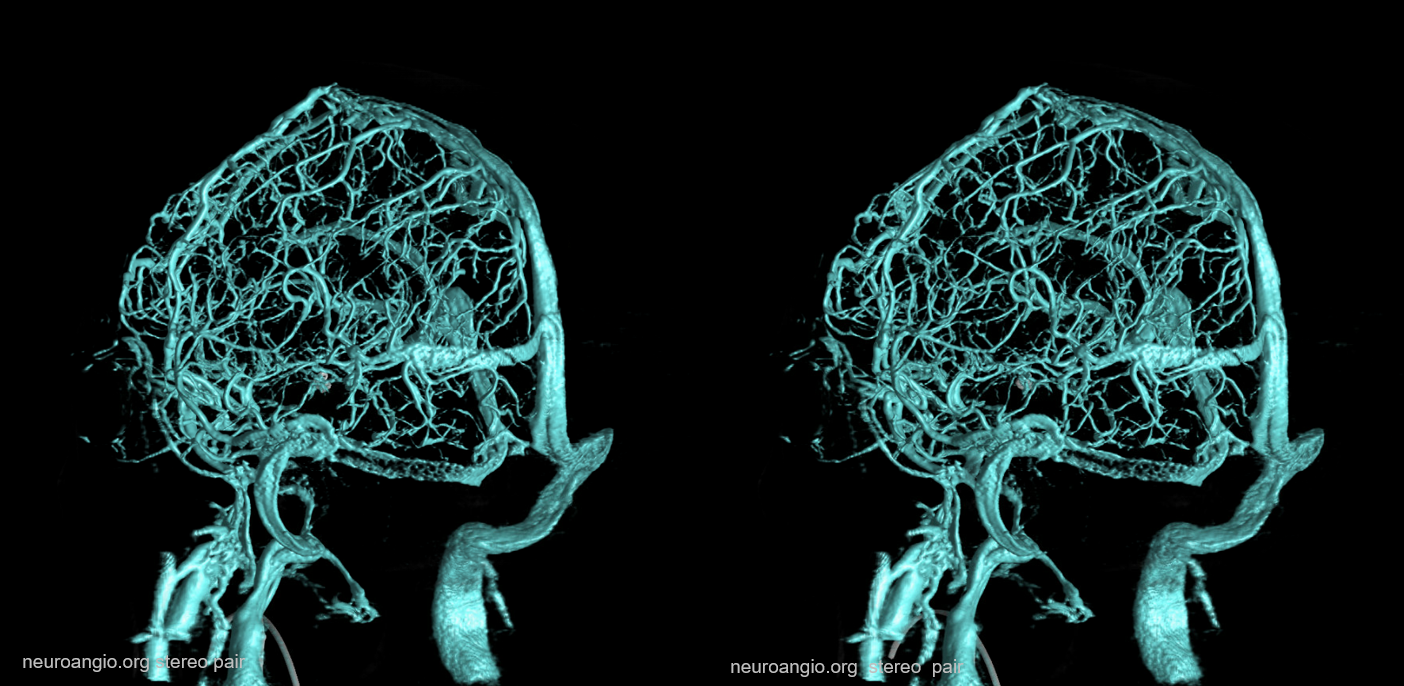
Little known but important plexus just underneath the skull base from the inferior petrosal sinus — basically the IPS and the petroclival plexus run more or less in parallel, separated by the bone. For that reason, its important not to confuse one for the other. The petroclival plexus does not, as a rule, have direct access to the cavernous sinus. See difference in example below, by Dr. Eytan Raz
Top row — bilateral petroclival vein injections — lots of opacification of the adjacent pterygopalatine plexus, and the “suboccipital cavernous sinus” — but not of the Cavernous Sinuses.
Bottom row — bilateral IPS injections. Much cleaner views of the Cavernous Sinuses. The petroclival venous plexus and the IPS are seen on both sets of images, with bone in-between.

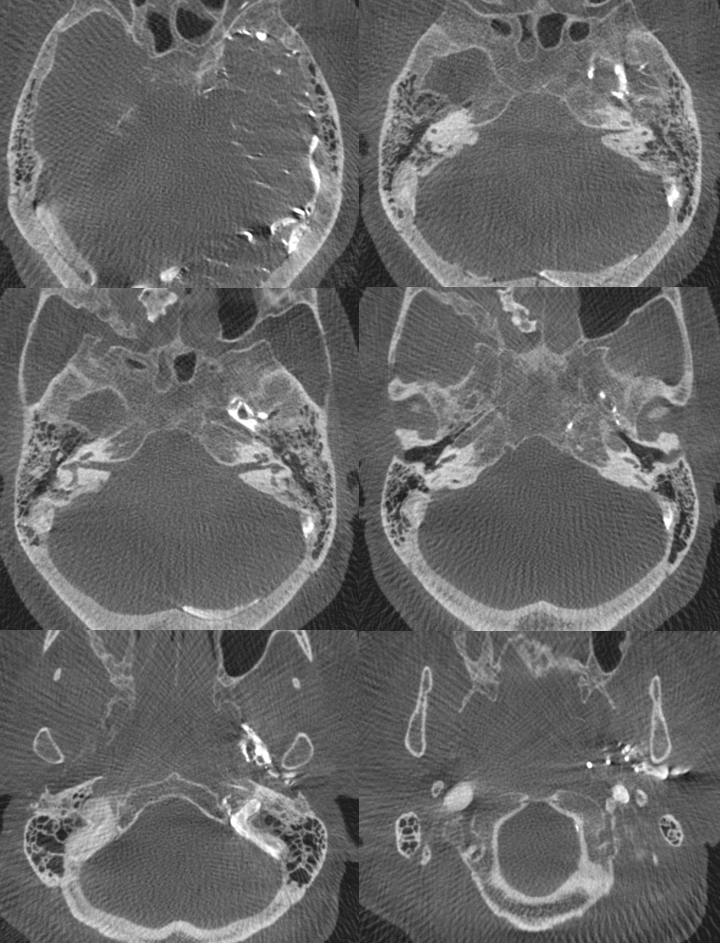
Unsubtracted views of catheter positions in the petroclival veins (left) and IPS (right)
Below is an infrequent drawing of the petroclival veins, from this very nice review articles on venous approaches to the IPS
Angiographic Visualization — look at all vessels!
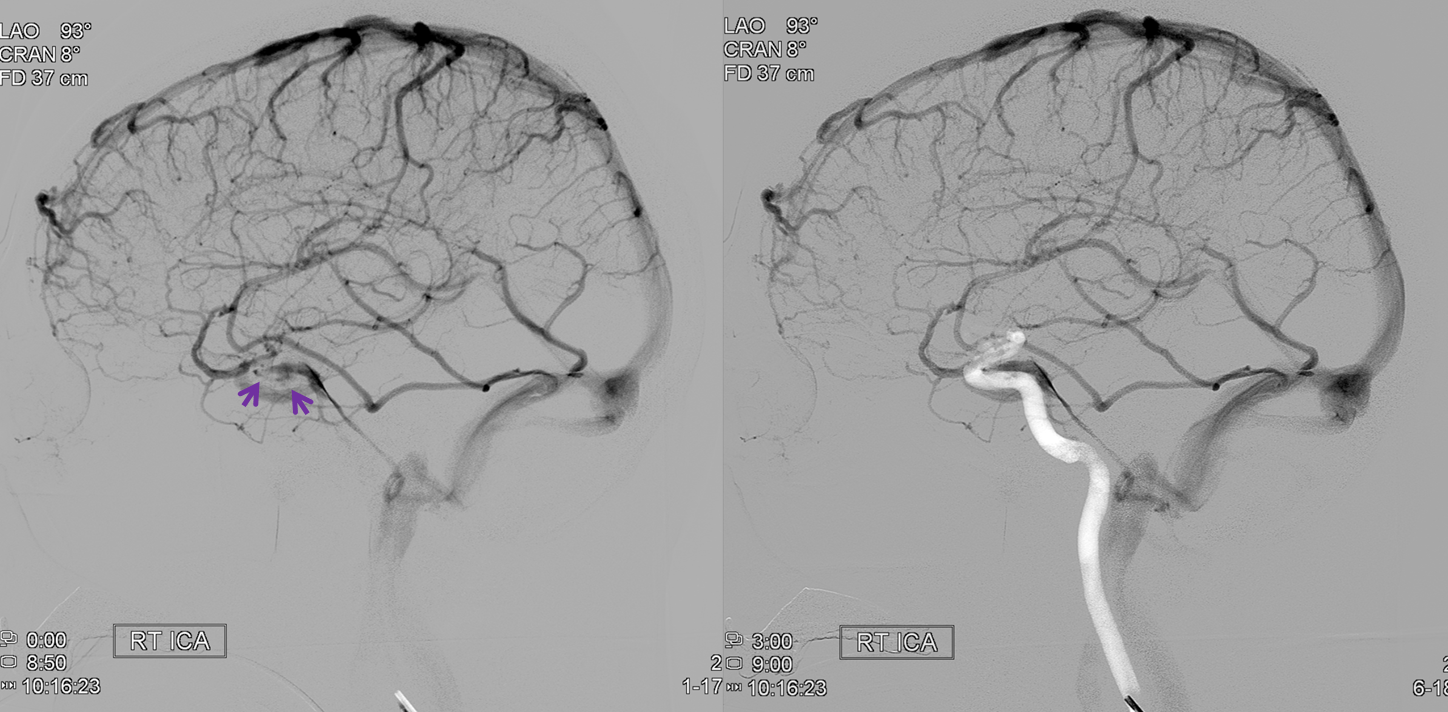
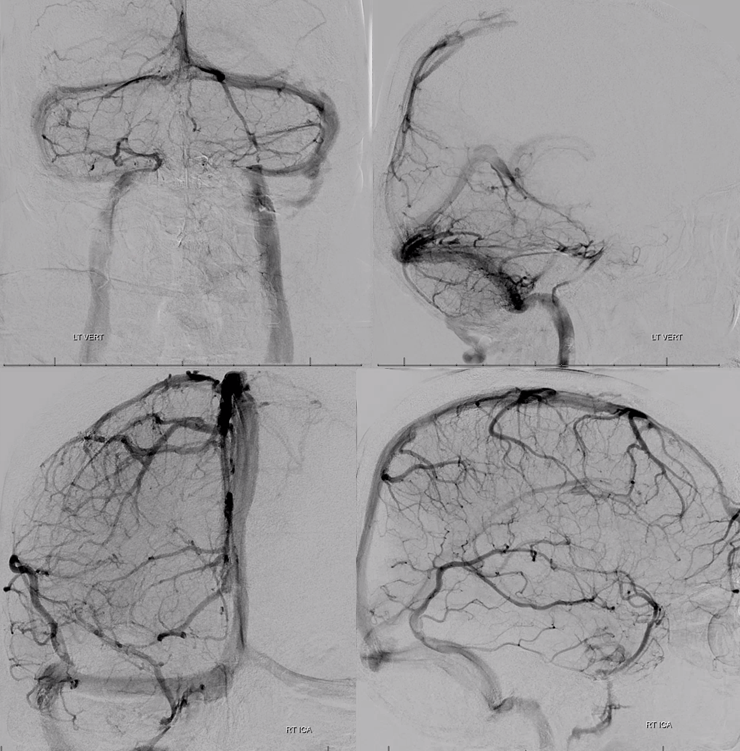
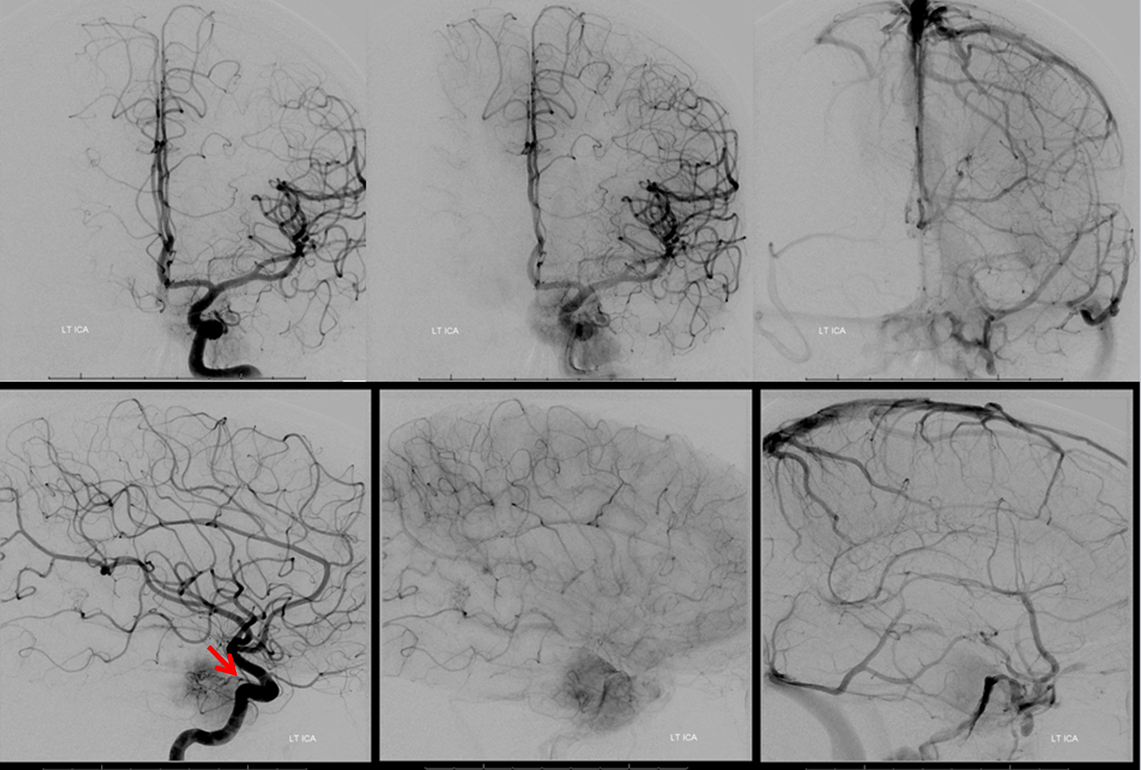
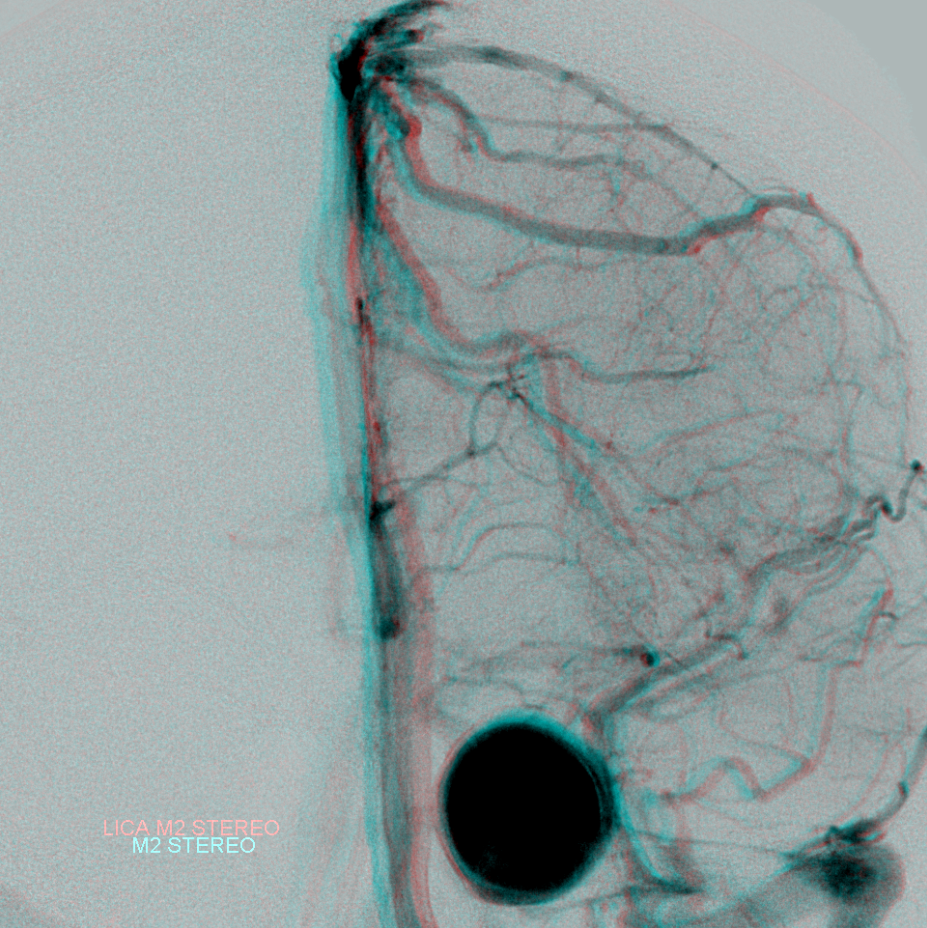
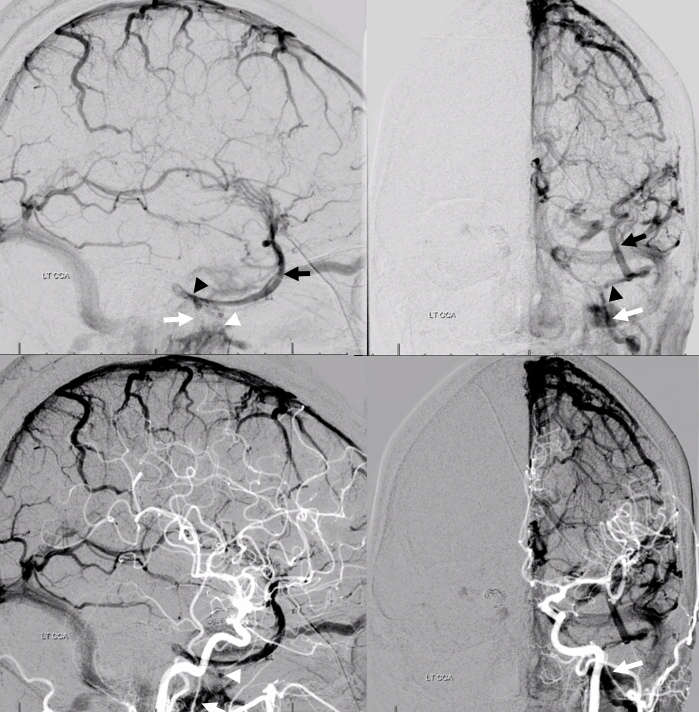
Remember this — angiography does not study the whole head at once — all vessels should be injected before making conclusions about a particular structure. For the cavernous sinus, even though the major tributaries are related to the anterior circulation, sometimes these do not drain into cavernous sinus. However, large portions of the posterior circulation, via petrosal or bridging veins, often do. In the following example, right ICA injection shows no cavernous sinus. The deep sylvian tributaries (light blue) of the basal vein (purple) drain towards the Galen, and another set of deep Sylvian veins (white) drains via a short probably sphenoparietal sinus (black) into the orbit (orange, strange also)

Same thing on the left, there is no cavernous sinus opacification

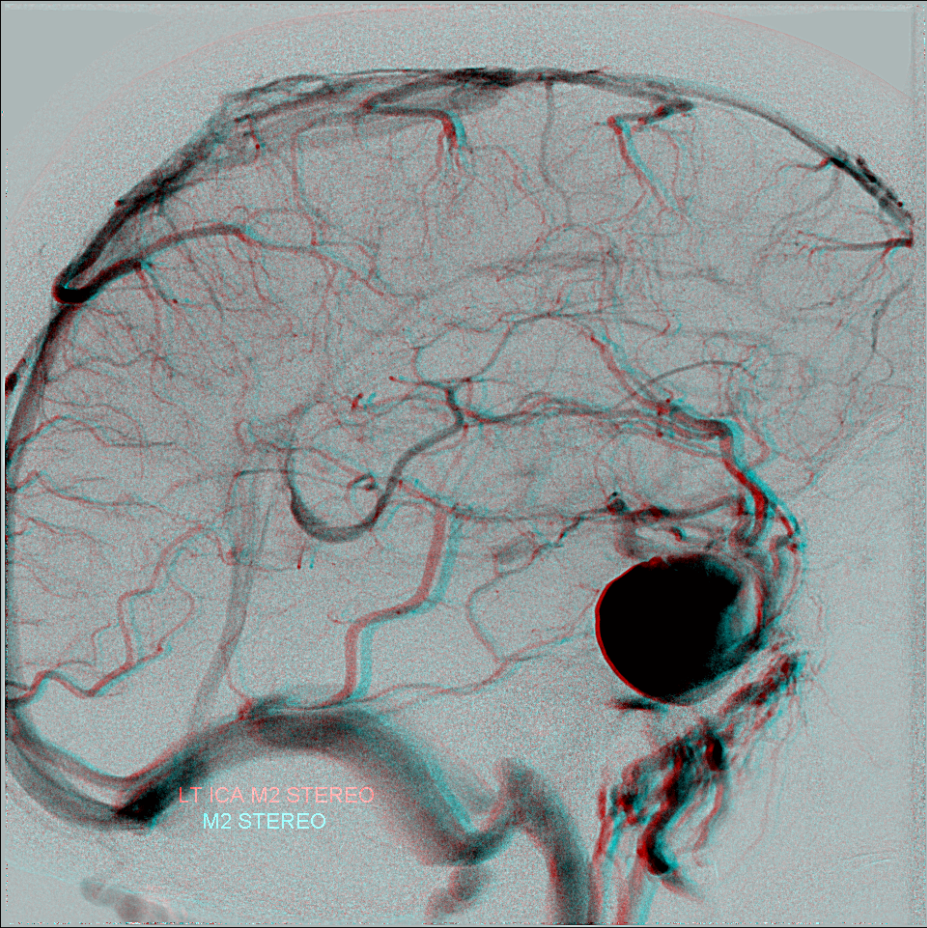
It is however unwise to conclude that this homo sapiens lacks both cavernous sinuses, which are very much alive and well, as you can see below from the following very neat stereoscopic projections

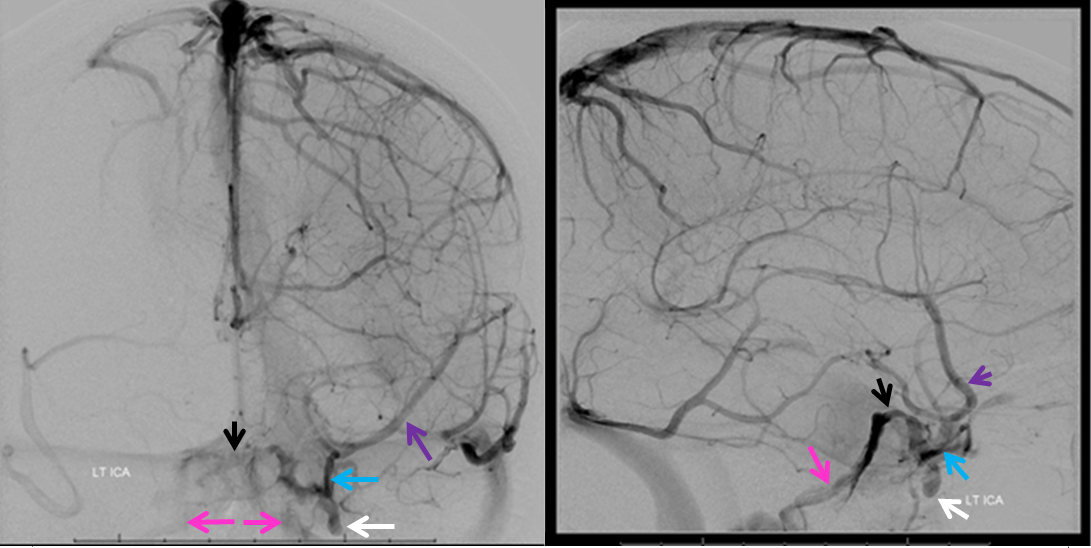
The legend below explains how in this case the superior petrosal sinuses (purple) are somewhat hypoplastic and not connected to the transverse sinuses. Instead, the anterior group of cerebellar veins and bilateral lateral recess veins drain into the petrosal veins (blue), which then empty into a very much alive and well cavernous sinuses (white) and from there into the inferior petrosal sinuses (black). Notice silhouette of the ICA (red).

Superior Ophthalmic Vein — External Carotid Injection
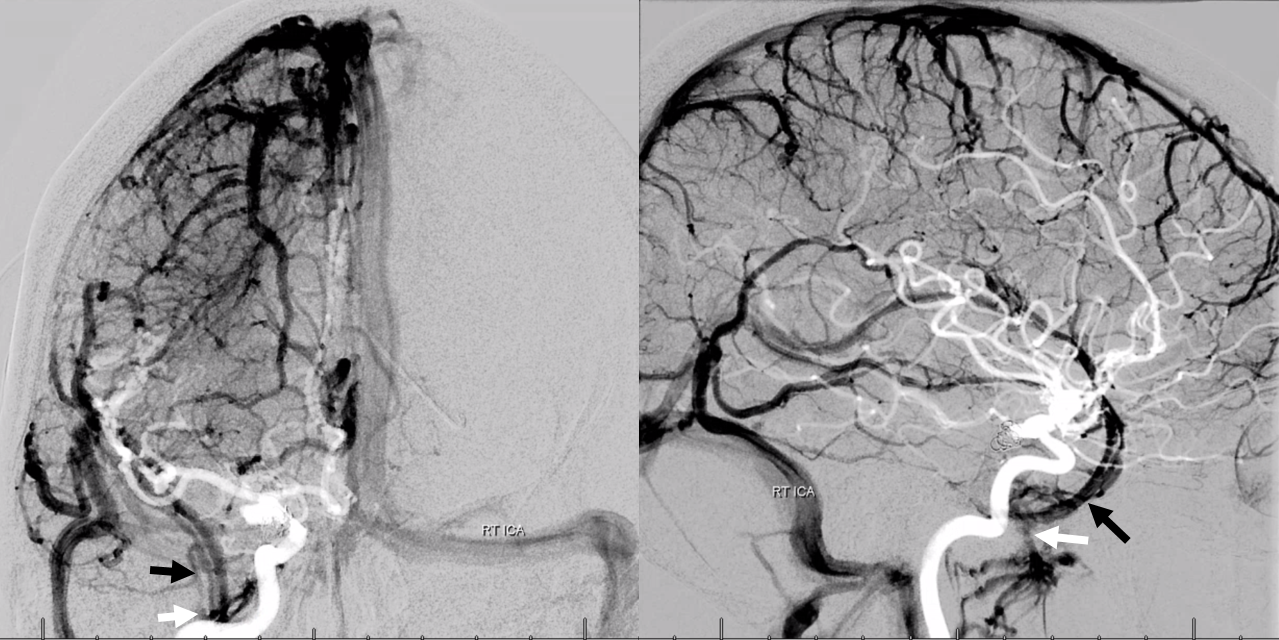
Even more importantly to the point of injecting every possible tributary is the study of the external carotid artery. As all good medical students know, there is a facial triangle where veins drain via the SOV into the cavernous sinus. Not that any of us in the USA will ever see a cavernous thrombophlebitis from a facial zit (we do have a case of course! — see here). But the nasal soft tissues are the most vascular ones that will drain into the cavernous sinus. So, don’t forget to get a common or external carotid view.
Here is an internal view with only the back of the cavernous sinus (orange) opacified, and of course the SOV is not seen because there is no intracranial hypertension and the flow in it is from outside into the cavernous sinus.

External carotid injection, however, shows prominently vascular nasal soft tissues (red), and in venous phase beautifully shows both SOVs (white) draining into both anterior cavernous sinuses (purple). Notice right angular vein (yellow).

Another example — the ophthalmic vein is not seen on ICA injection, but is quite prominent with ECA. Bilateral filling of SOV is common, reflecting mostly the midline location of the nasal venous apparatus which drains into the SOV. Antegrade flow from the face and orbit into the cavernous sinus is indirect evidence of relatively normal intracranial pressures. One of the angiographic findings of intracranial hypertension, of any cause, is retrograde ophthalmic vein flow. On the other hand, incidental finding of such retrograde flow is not necessarily pathologic, in my experience.

Ipsilateral ECA injection

Scalp Drainage into the Cavernous Sinus
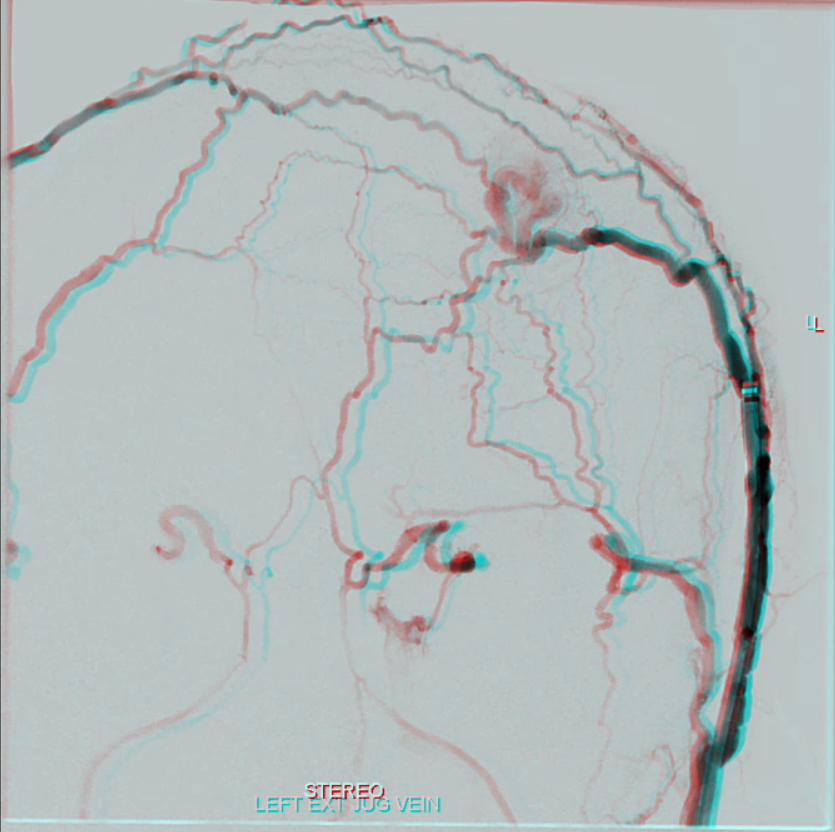
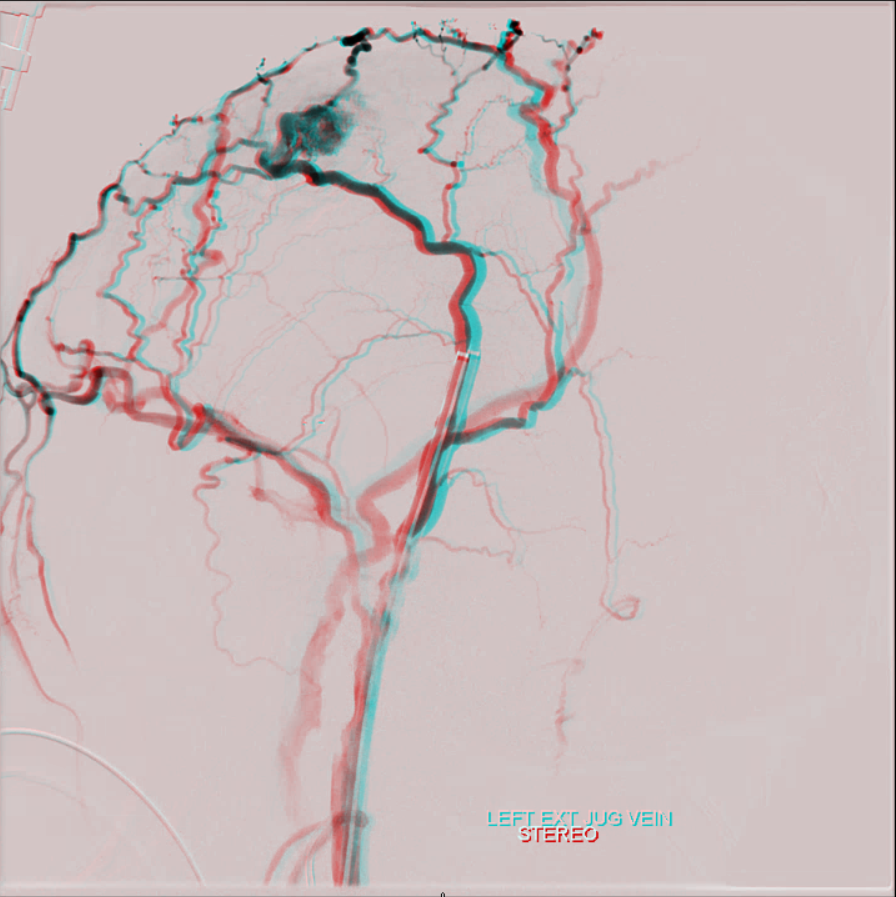
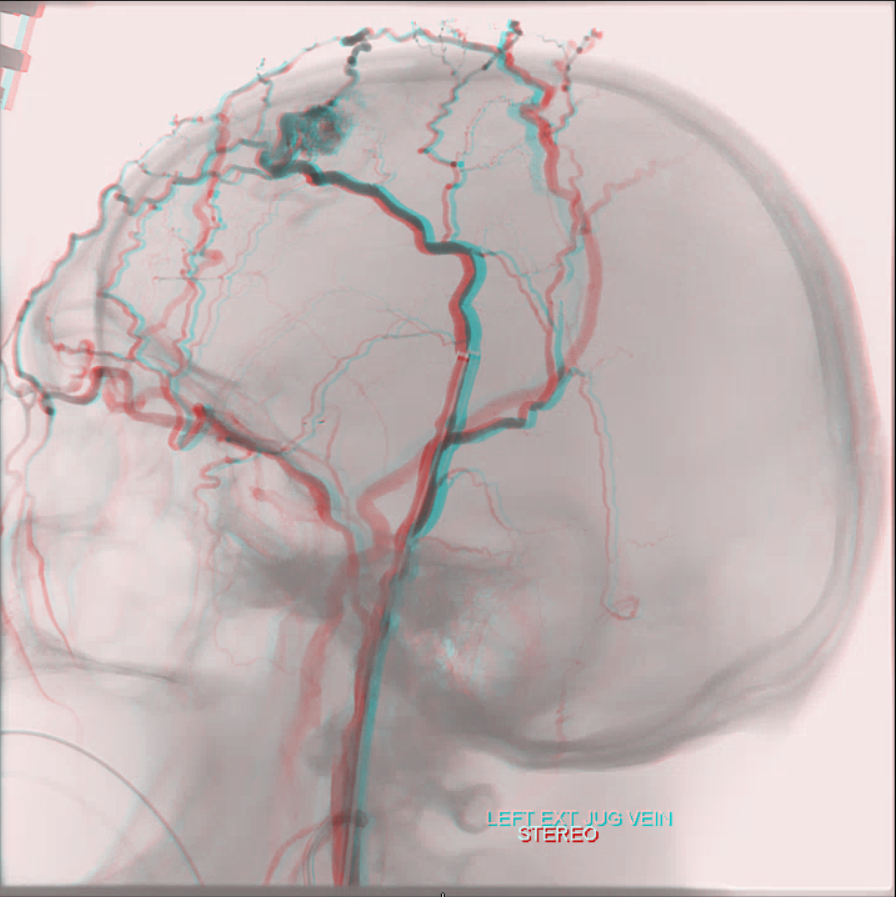
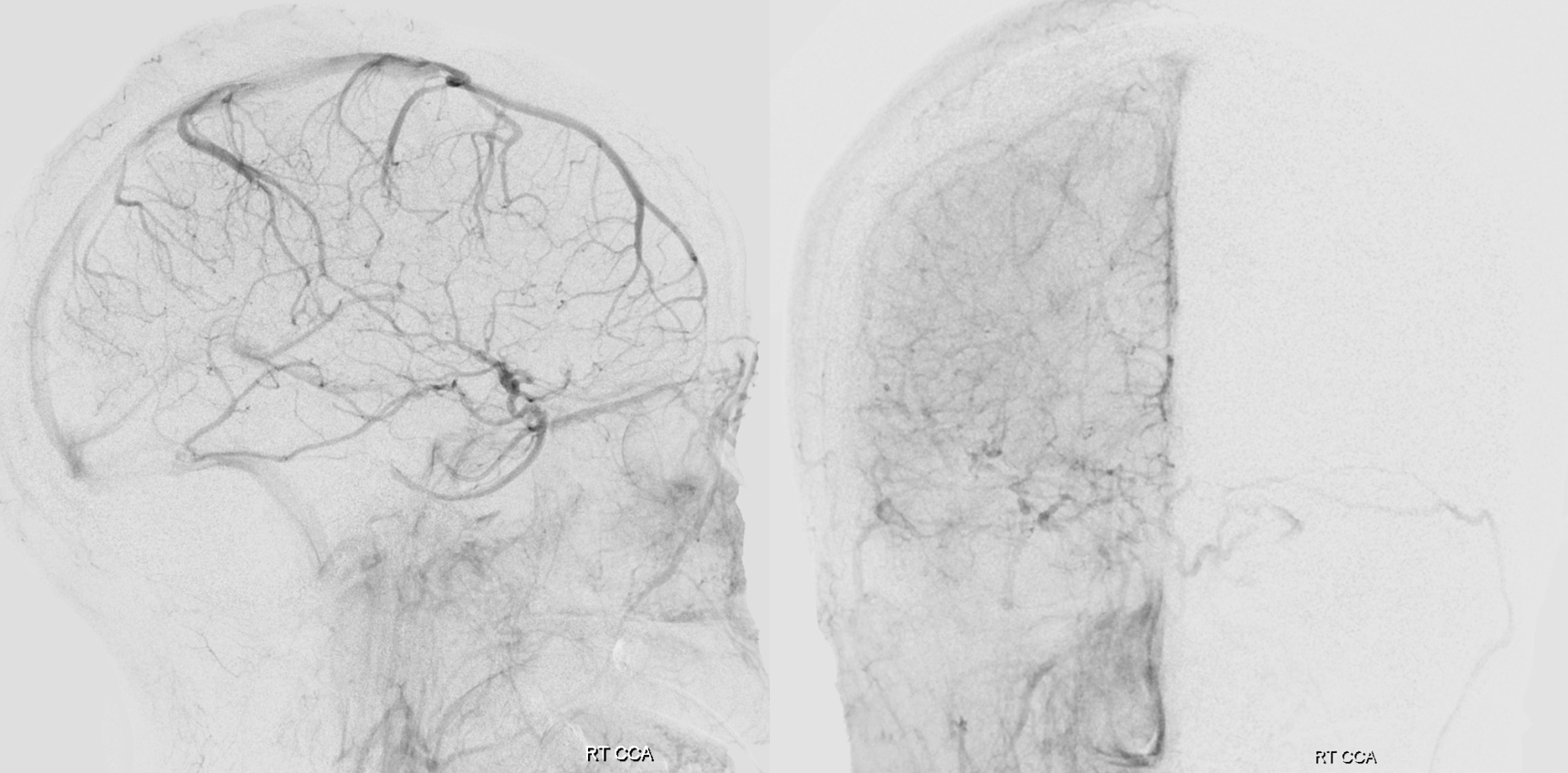
yes, all veins are connected. And no, you cant see all the veins that well by injecting arteries. Try injecting veins to see veins. The scalp also drains into the cavernous sinus — we just dont have too many scalp infections yielding cavernous thrombophlebitis to have this fact taught in med school. Here is an example of a scalp AVM draining via both superior ophthalmic veins into the cavernous sinus — case courtesy Eytan Raz MD PhD. The catheter is in the superficial temporal vein. No labels.
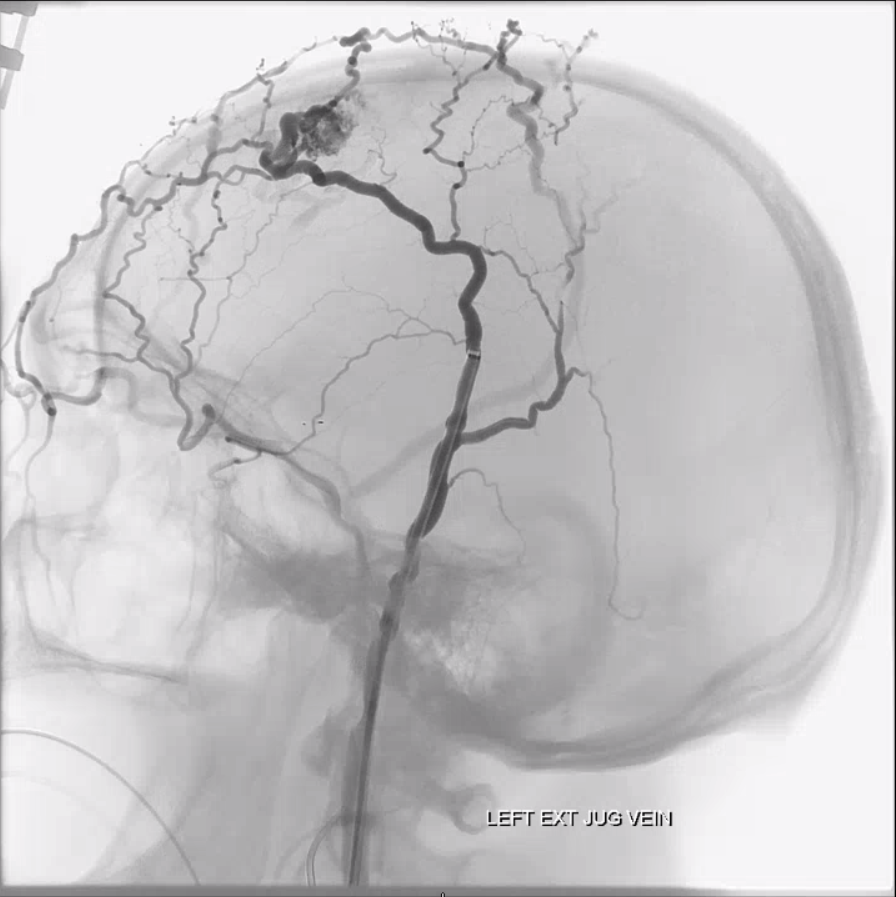
Beautiful Anaglyphs
Angiographic visualization — mask image
A neat way of projecting arterial phase as a mask for venous phase to demonstrate carotid artery relationship to the cavernous sinus. Notice the intracavernous lucency (purple) corresponding to the carotid artery. The dominant inflow arrives from the superficial sylvian veins, and outflow is into the inferior petrosal sinus.
Below is another example of a cavernous sinus opacified mainly by the superficial sylvian veins:
Cavernous Sinus (dark blue). The sylvian network and “sphenoparietal sinus” (orange) are drain into the cavernous sinus with a well-developed inferior petrosal sinus (light blue). Notice superimposition of the basal vein (purple) and the anterior choroidal artery (red)
How low does the cavernous sinus go?
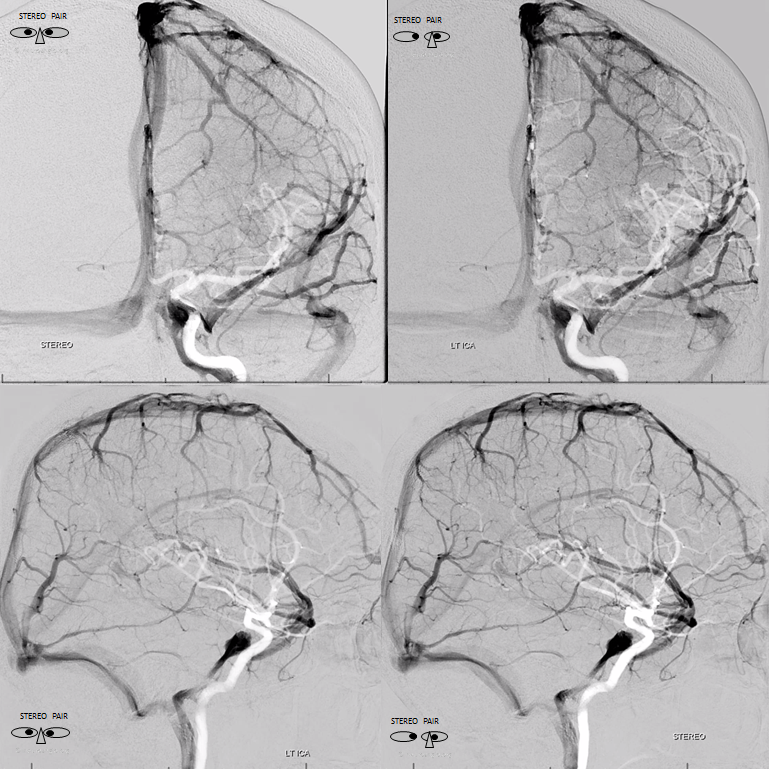
A relatively well-known classification of the internal carotid artery segments by Bouthillier lists the “lacerum” segment. The alternative and unfortunately less well known classification by Zial dispenses with the lacerum segment on the grounds that the cavernous sinus extends all the way down to the petrous bone where the carotid enters the sinus distal to the petrolingual ligament. Well, Zial is right. The cavernous sinus indeed extends very low, in most people. This can be beautifully shown angiographically. Here are ANAGLYPH stereoscopic images of the cavernous sinus in double mask images with carotid artery as mask image, showing its very low extent.
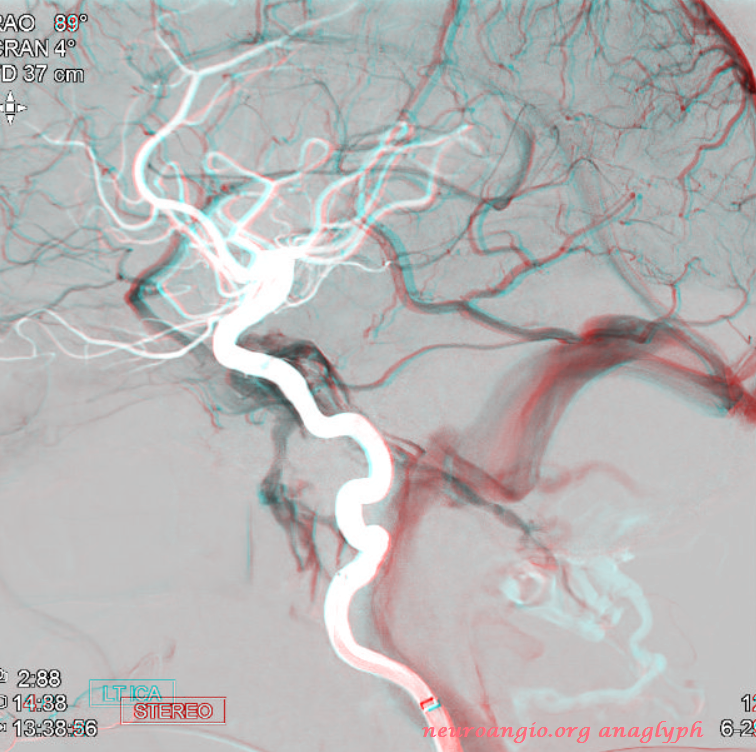
Even better are “triple mask” with bone added to boot
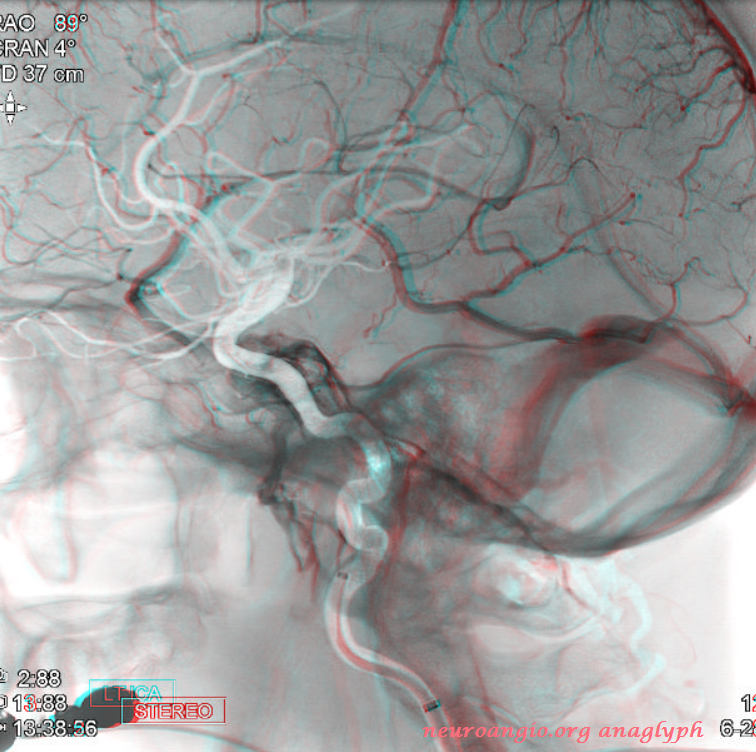
Here are the usual crosseye stereos

Typical appearance of cavernous sinus (black) on an ICA injection — major inflow is via the superficial sylvian veins (pink) and the deep sylvian vein – basal vein conduit (yellow, notice full extent of basal vein between CC and the Galen), and outflow into inferior petrosal sinus (white) and pterygoid venous plexus (purple)

The same in stereo:

Another example of normal cavernous sinus anatomy, silhouetting the vertical and horizontal segments of the cavernous internal carotid artery segment (light blue). Again, remember the typical deep inferior extent of the cavernous sinus, projecting just above the petrous bone.

Stereo image. Notice dominant superficial Sylvian inflow and egress into the inferior petrosal sinus. Notice how, oftentimes, dominant superficial Sylvian veins are multiple in number — there are two coursing in parallel to join the cavernous sinus — to me this argues against presence of a unique sphenoparietal sinus.

Stereo with carotid artery as mask image

Why is the superior ophthalmic vein not seen on the above injections? The answer is again the same — one cannot see the vein if the drainage territory of this vein is not injected. Because the superior ophthalmic vein drains extracranial territory towards the cavernous sinus, the SOV is only rarely seen via ICA injections (it can be seen because ophthalmic artery can extensive supply nasal tissues, as in cases of failed IMAX epistaxis embolization). Usually, though, it is the external injection that shows the SOV.
This case illustrates an internal carotid injection which does not visualize the SOV (catheter marked by white arrows)

A common carotid injection (white arrows external branches) of the same patient shows the SOV (blue arrows)

Another example of SOV visualization via ECA injection, draining in antegrade intracranial fashion

ICA injection of the same patient, in stereo, barely visualizing the SOV draining the intraorbital tissues (notice blush of choroid and extra-ocular muscles, not labeled). There is, however, a normally elusive inferior ophthalmic vein (purple) here

Ophthalmic Vein Cavernous Sinus anatomy via a carotid cavernous fistulogram
Left ICA injection demonstrating enlarged superior (purple) and inferior (light blue) ophthalmic veins draining a carotid-cavernous sinus (dark blue) fistula. The fistula was approached via surgical exposure, gaining access into the superior ophthalmic vein (lateral center and AP right images) and closed by coiling. The microcatheter is labeled in red.
Cavernous Sinus Asymmetry
Dominance of one transverse sinus over another is routine. Cavernous sinuses are usually symmetric in their development — spectrum from very large to essentially absent. Except when they are asymmetric. Rare but still normal. Important to exclude pathology such as thrombosis, tumor, etc. However, when one sinus is bigger than another, the usual reason is simple variation. Here is an example of a patient who got an angio for suspected left cavernous sinus dural fistula.
CTA (poor technique, venous phase contamination) shows asymmetric prominence of left cavernous sinus (arrow) A tail (arrowhead) is seen also (see below).
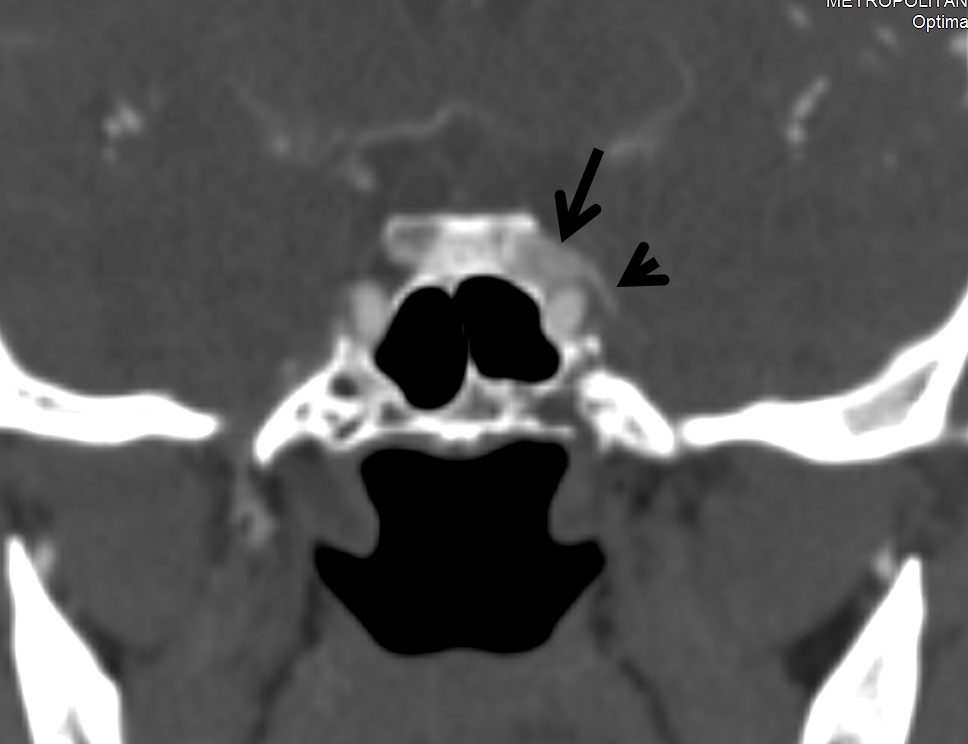
Notice absence of other dural fistula signs such as congestion of SOV or other nearby veins
Angio of vert and right ICA. The right cavernous sinus is hypoplastic
The left one is definitely not. Sylvian veins drain into the paracavernous sinus which connects (arrowhead) to the main cavernous sinus (arrow). The connection corresponds to the “tail” on CTA. More on paracavernous sinus below.
Stereo views
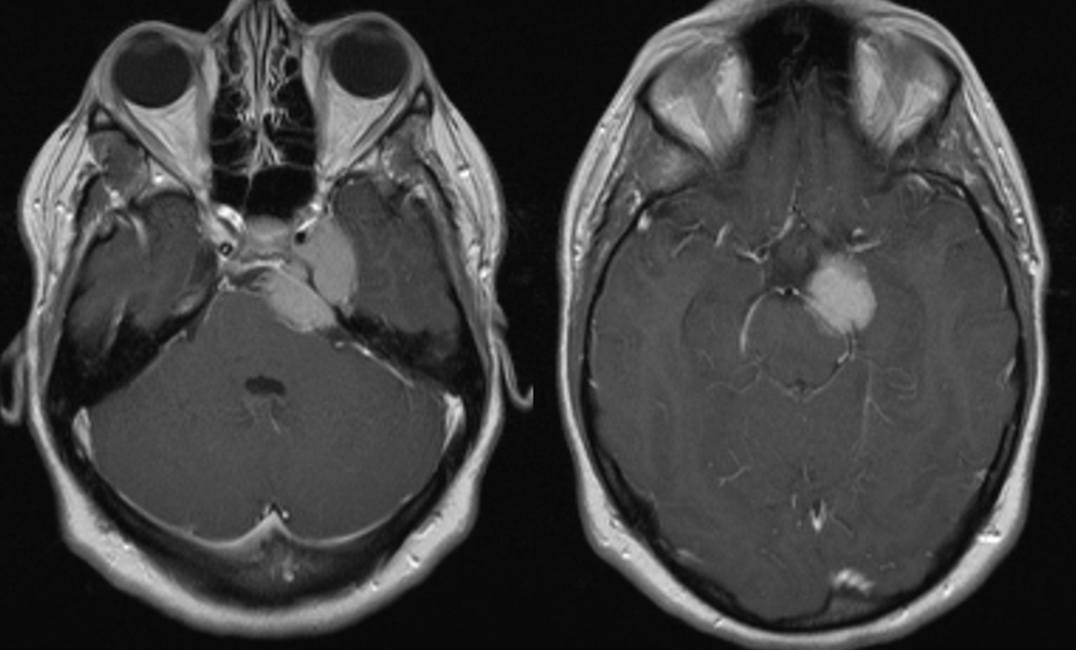
Another example — the best. Most asymmetric sinus so far. Repeatedly misdiagnosed as a dural fistula — first on CTA, then MRI and MRA — still called that. See below and do a mental exercise “for” and “against”. The actual diagnosis is on the MRI images.
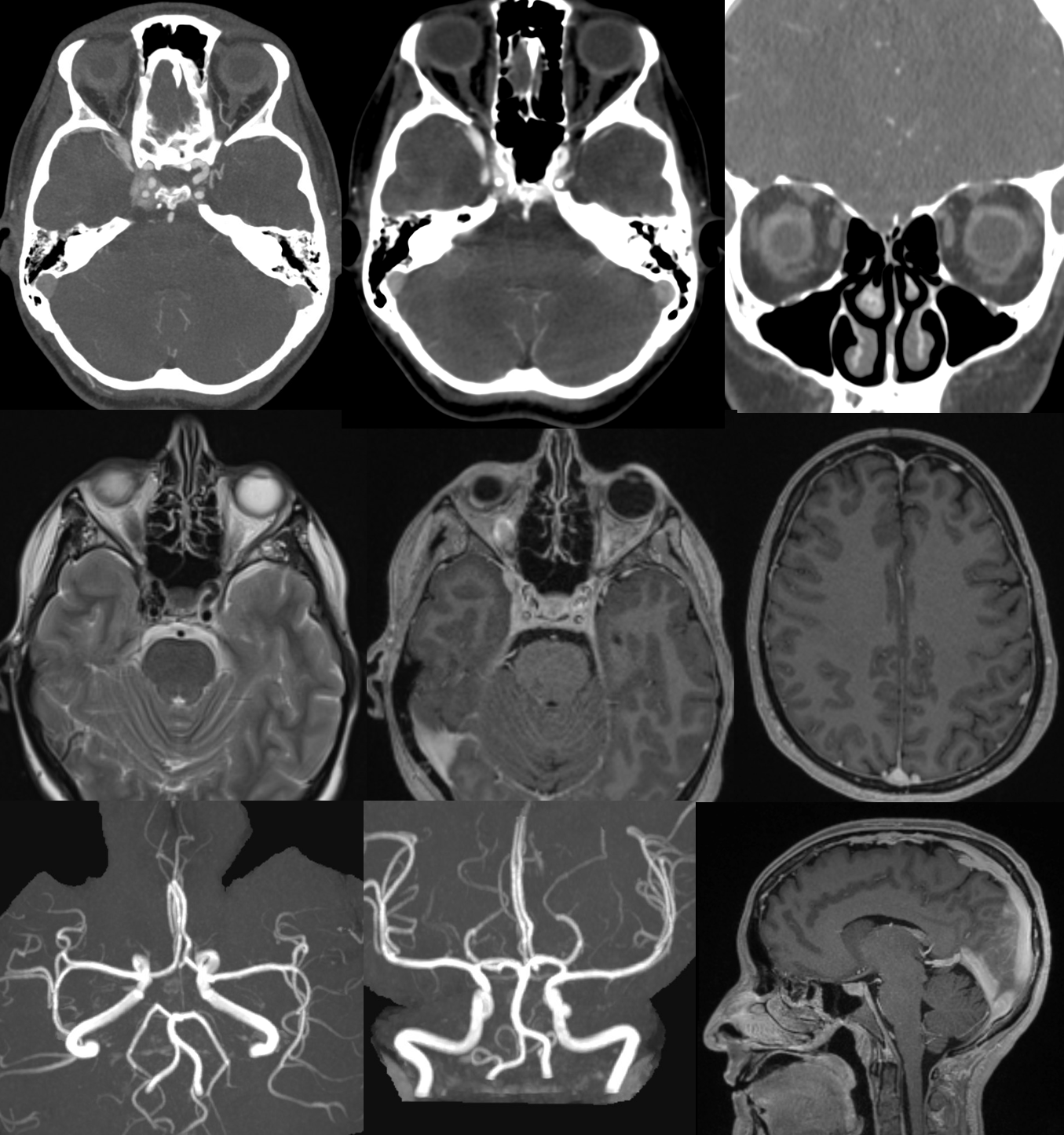
Angio
Diagnosis?

Cavernous sinus connections demonstrated by cavernous sinus dural fistula.
Nothing demonstrates the limits of anatomical plasticity quite like pathology. What better way to show all available cavernous sinus connections than a high-pressure cavernous sinus state, exemplified by the various complex and challenging fistulas which afflict it. This one, though “dural” or “indirect” in origin (first term being appropriate, and second frankly short-signed), is high-flow enough to expect that every exit will do its duty.
Red= Distal ECA (catheter seen on lateral view below the lower red arrow); Orange=foramen rotundum branch; Yellow=MMA; green=cavernous sinus; dark blue = superior ophthalmic vein; light blue=facial angular vein; purple=basal vein; bright green=straight sinus; black=sigmoid sinus; brown=jugular bulb; pink = petrosal vein congesting inferior cerebellar veins; white=inferior petrosal sinus; double yellow=sphenoparietal sinus; double light blue=reflux into brain veins via basal vein.
As one can see, not every egress is available. For example, the superior and inferior petrosal sinuses are either hypoplastic or thrombosed as a result of the fistula. The superior ophthalmic and contralateral cavernous egress is insufficient, with congestion of the supra- and infra-tentorial brain parenchymal veins.
Intercavernous Sinus
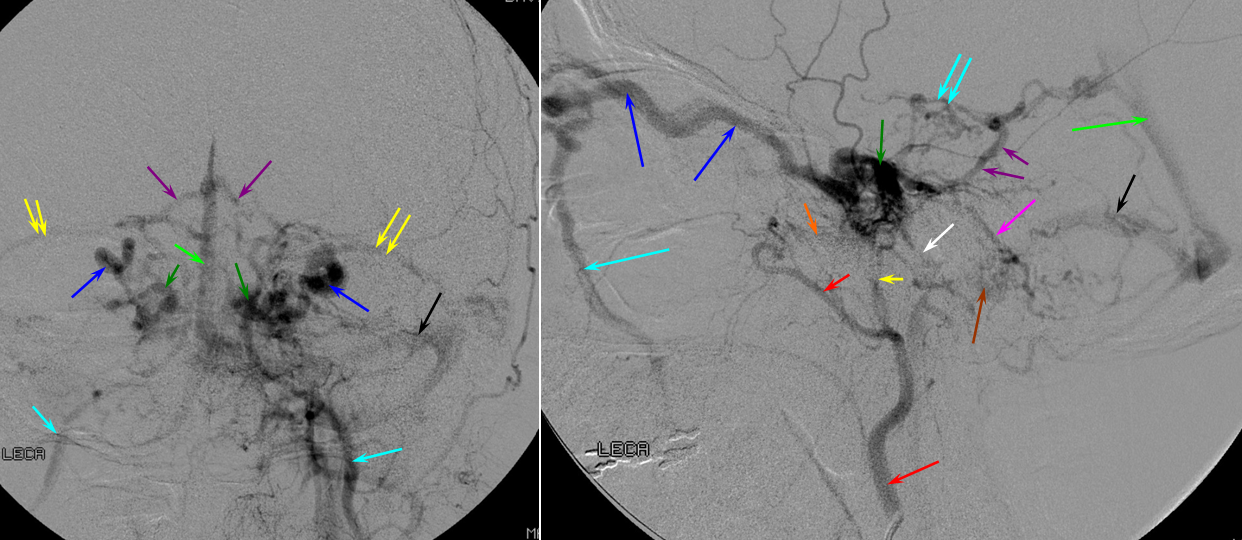
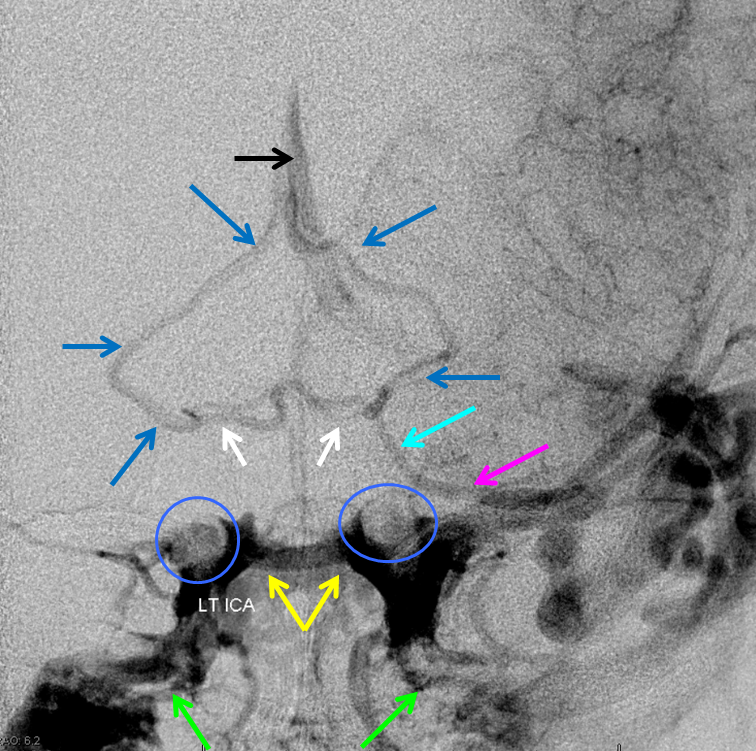
Although it is a safe bet that this sinus usually exists, its visualization in the nonpathologic state is hampered by lack of pressure gradient for contrast to flow from one side to another. The sinus is best seen in pathologic sates of cavernous sinus hypertension (fistulas again) which frequently either congest both sinuses or lead to a pressure gradient between them. Here is an angiographic example of an intercavernous sinus (yellow) in a patient with a large left temporal lobe AVM. The carotid artery flow voids are inside blue circle/oval. Lots of other good information is here. The interpeduncular vein is shown in white. Basal vein middle and posterior portions (dark blue arrows) outline the midbrain. Anterior portion of the basal vein (light blue arrow) is contiguous with the deep sylvian (a.k.a. middle cerebral ) vein (pink). The pterygopalatine plexi are marked by green arrows.
Another example of a cavernous sinus venogram, with the posterior intercavernous sinus (some would call it the upper segment of the basilar venous plexus) shown in white. Superior petrosal sinuses are pink, and carotid artery silhouettes are red.

Superficial Sylvian veins, “laterocavernous sinus” and “paracavernous sinus”
The debate as to whether the sylvian veins drain directly into the cavernous sinus or by way of the “sphenoparietal sinus” or Brechet is, in my opinion, won by those who believe in direct venous drainage. A sinus does appear to exist along the sphenoid ridge, and is developmentally related to the middle meningeal veins which are called “anterior parietal”, for good embyologic reasons though they in fact are in the frontal bone. That sinus is likely not connected to the Sylvian veins. In many instances, also, several superficial sylvian veins seem to course in parallel to join the cavernous sinus individually. Either these represent multiple sphenoparietal sinuses, or perhaps all but one of them are true veins, or perhaps all are in fact veins and there is no sphenoparietal sinus related to these. The latter seems to be the preferred option. In the following example, three separate superficial Sylvian veins (purple) run adjacent to the sphenoid ridge to join a common channel (white) which may be a common vein or perhaps a short sphenoparietal sinus.

Stereo of the same

Lateral stereo

So, lets drop the “sphenoparietal sinus” name for now.
The Sylvian veins may be more or less developed in any given individual (see Superficial Venous System page). When prominent, they collect opercular territory and course along the sphenoid ridge. Then, several possibilities exist:
1) Direct drainage into the cavernous sinus, with subsequent outflow via the usual suspects (petrosal sinuses)
2) Drainage into a space which appears to be lateral to the cavernous sinus, from where flow is directed via foramen ovale into the pterygopalatine venous plexus. Some have termed this space “paracavernous or lateral cavernous sinus”, though I am not familiar with such a concept existing in the neurosurgical literature, nor in the opinion of my neurosurgical colleagues (Jafar Jafar, M.D., personal communication). It is likely an example of a hemodynamically isolated compartment (metaphysics).
3) Drainage via an inferior temporal vein into the transverse/sigmoid sinus junction
Below is an example of dominant Sylvian (purple, pink arrows) egress into the pterygopalatine venous plexus (dark blue), via a compartment quite lateral to the internal carotid artery which angiographically marks the location of the cavernous sinus (light blue double arrow) — this (purple arrows) would be considered a “laterocavernous sinus”

Beautiful Examples of Cavernous Sinus Compartments
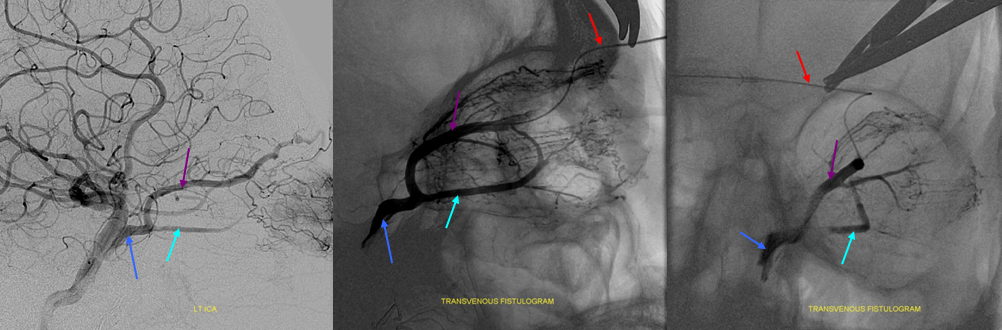
Below, the compartmentalization of the cavernous sinus is elegantly shown by pathology, again in form of a cavernous sinus dural arteriovenous fistula. Injections of the right and left carotid arteries demonstrate a fistula at the posterior aspect of the left cavernous sinus medial compartment (pink), supplied by various branches of the left and right MHT. The venous drainage of this compartment is directed into the engorged superior ophthalmic vein (red). Despite left cavernous sinus congestion, as evidenced by the precarious state of the superior ophthalmic vein, the patient’s normal hemispheric venous drainage proceeds, completely unimpeded, via dominant superficial sylvian veins (light blue) into the “laterocavernous sinus / lateral cavernous sinus compartment (purple) and through foramen ovale (yellow) into the pterygopalatine venous plexus (black). How’s them apples?

The same arrangement is shown in the lateral projections of early (left) arteriovenous shunting and brain venous phase (right) lateral compartment (purple) drainage. Neither compartment communicates with the other, as evidenced by their mutually separate drainage routes. Understanding this anatomy allows the operator to consider transvenous coiling of the fistulous medial compartment without compromise of the sylvian venous outflow.

Another Example of Cavernous Sinus Comparmentalization — Meningioma
Here is a complex petroclival meningioma going for pre-resection angio and embolization (see full case here, part of neuroangio.org extensive collection of pre-operative tumor embolization).
Usually, in cases like these, the ipsilateral cavernous sinus is occluded. However, one value for preoperative angiography is to look for all kinds of potential problems. Here, we see tumor supply arising from the ILT (red arrow) . Venous phase shows that, contrary to expectations, the cavernous sinus is still open, and necessary, receiving superficial sylvian venous drainage — another example of laterocavernous sinus.
Venous phase images show superficial sylvian veins (purple) draining into the lateral cavervnous sinus (blue). The foramen ovale egress into the pterygopalatine fossa is closed (white arrow points to stump). Instead, venous drainage proceeds toward the posterior left cavernous sinus, and into both inferior petrosal sinuses (pink), via the intercavernous sinus (black). All important information for the surgeon.
Yet another example of lateral sinus compartment — giant cavernous aneurysm
In this giant aneurysm the dominant sylvian veins continue to drain via the lateral compartment of the cavernous sinus. The images below are ANAGLYPH STEREOS


Venous phase shows drainage of dominant sylvian veins into lateral compartment around the aneurysm
Same in lateral
Paracavernous Sinus
Really, it is a different sinus. Instead of running along the lateral wall of the cavernous sinus, it projects along the floor of the middle cranial fossa completely independently and usually drains via ovale or spinosum into pterygopalatine venous plexus. Some believe this to be remnant of the embryonic “primitive parietal sinus” — see venous embryology page for that. Here is an example. Runs along the anterior aspect of middle cranial fossa (black arrows), then along the floor (black arrowheads) and out via ovale (white arrowhead) and spinosum (white arrow). Arterial phase mask images below show relationship to the MMA
Another example — actually same patient on right. More medial course but still not in cavernous sinus (black arrows). Exit via ovale (white arrows)
Another example — note lateral location with respect to carotid of the paracavernous sinus draining the sylvian veins, and the true cavernous sinus opacified in the venous phase of common carotid injection
Stereo ICAs

Common venous
Stereo fused VRs. The paracavernous sinus receives deep sylvian (middle cerebral) vein parallel and below the M1 segment, draining via the ovale into the pterygopalatine venous plexus. This is an extremely common drainage pathway for all 3 — cavernous, paracavernous, and laterocavernous.
Finally, to emphasize the point that all foramina are potential venous egress routes, below is example of paracavernous sinus draining into all 3 major middle cranial fossa holes: rotundum (arrow), ovale (arrowhead), and spinosum (dashed arrow).
Superficial sylvian drainage into ovale via paracavernous sinus on DYNA CT venous phase
Deep Sylvian veins and Basal vein to Cavernous Sinus Anastomoses
The basal vein, in its full expression, is an unbroken conduit between the cavernous sinus and the vein of Galen (see Deep Venous System page for dedicated info). Below is an example of a fully contiguous basal vein (purple), with its deep sylvian component (pink) draining into the cavernous sinus (white) near the confluence of the superficial sylvian vein(blue). The main outflow of the cavernous sinus is the inferior petrosal sinus (black).

Another example of the same, also shown previously. Basal vein (yellow) usually connects with superficial sylvian veins (pink) just before the common trunk empties into the cavernous sinus (black)
In the example below, the basal vein (purple) is not connected to the cavernous sinus, which is hypoplastic — the deep sylvian vein (pink), with well-displayed uncal and lenticulostriate tributaries (yellow) drains via the basal vein towards the Galen.

Related pages:
“Case Archives Cavernous Sinus Thrombophlebitis” page for example of this classical entity diagnosed, of course, by catheter angiography(!)
Direct Ophthalmic Vein access to cavernous sinus dural fistula
MHT nBCA embolization of Cavernous Sinus dural fistula