


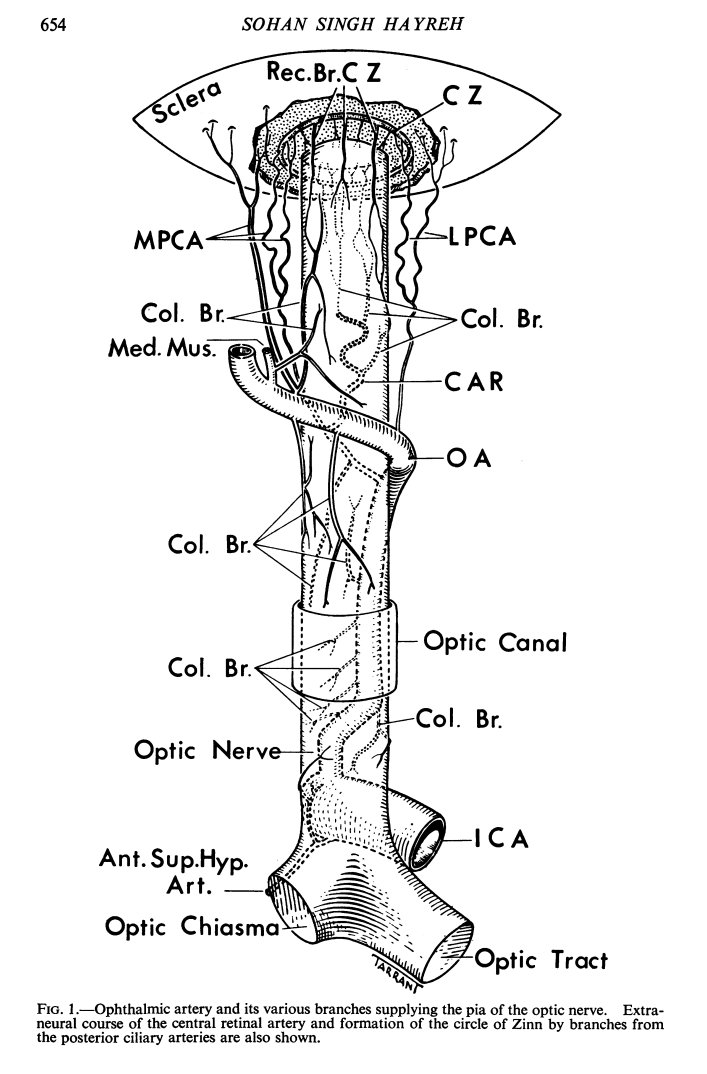
Dorsal Ophthalmic Artery Diagram. Same numbers as Diagrams and Drawings page, with some additions. 12a — “Collateral Branches” supplying optic nerve sheath complex, according to Hayreh. 12b — “recurrent ophthalmic artery” — a name given by neuroangio.org to a consistent vessel along the optic nerve sheath in subjects with dorsal ophthalmic artery disposition. 12 — central retinal artery. 14 a — superior hypophyseal artery, which consistently supplies the intracranial optic nerve, as well as variably the canalicular segment, in balance with the “collateral branches” 12a
When ophthalmic artery originates from the cavernous segment of the ICA, it has generally been called “dorsal ophthalmic” — a vessel present in early embryonic stages (#38 above). For the aficionados of embryology, this is a controversial subject, since the nomenclatures of “dorsal” and “ventral” ophthalmic artery differ in the descriptions of the two most powerful figures in this debate — Dorcas Padget and Pierre Lasjaunias. The “dorsal ophthalmic” term above follows Lasjaunias’ convention, only because it is now the generally accepted terminology. It may be wrong. The problem is that Padget actually had the little data that there was. The whole thing is a mess, in my opinion, the main problem being paucity of data. We have tried to either correct the mess, or add to it, depending on what you feel, by arguing that the missing piece in the debate is the superior hypophyseal artery, which was completely ignored by Lasjaunias, and almost completely by Padget.
Aside from whatever embryology is, there are clear facts in the adult. In about 1% of subjects, the main contribution to ophthalmic artery is from an extradural vessel that enters the orbit via the superior orbital fissure, NOT the optic canal. Lasjaunias believed that dorsal ophthalmic is an enlarged anteromedial branch of the inferolateral trunk. This i believe is true (the controversy is the embryology, not the adult appearance). We will call it “dorsal” for the sake of convention, and I will hear about it from Padget at some point, hopefully later rather than sooner.
What has been largely overlooked is the supply to the optic nerve, aside from the central retinal artery. what about the rest of the nerve — from the intracranial to canalicular to the orbital apex segments? In all cases… And what can we learn from the analysis of “dorsal ophthalmic” dispositions. Read below to find out.
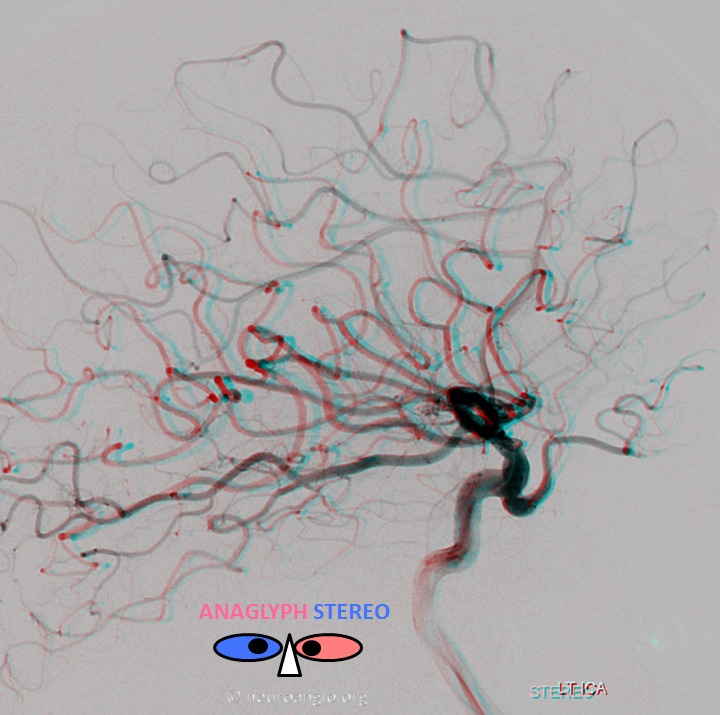
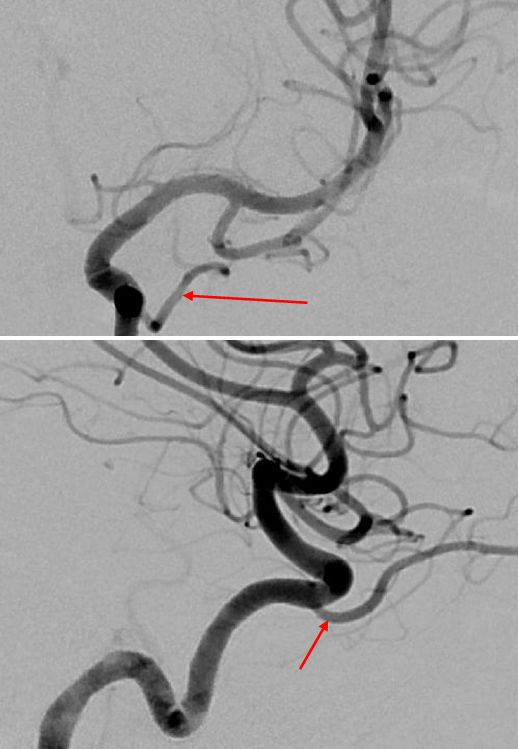
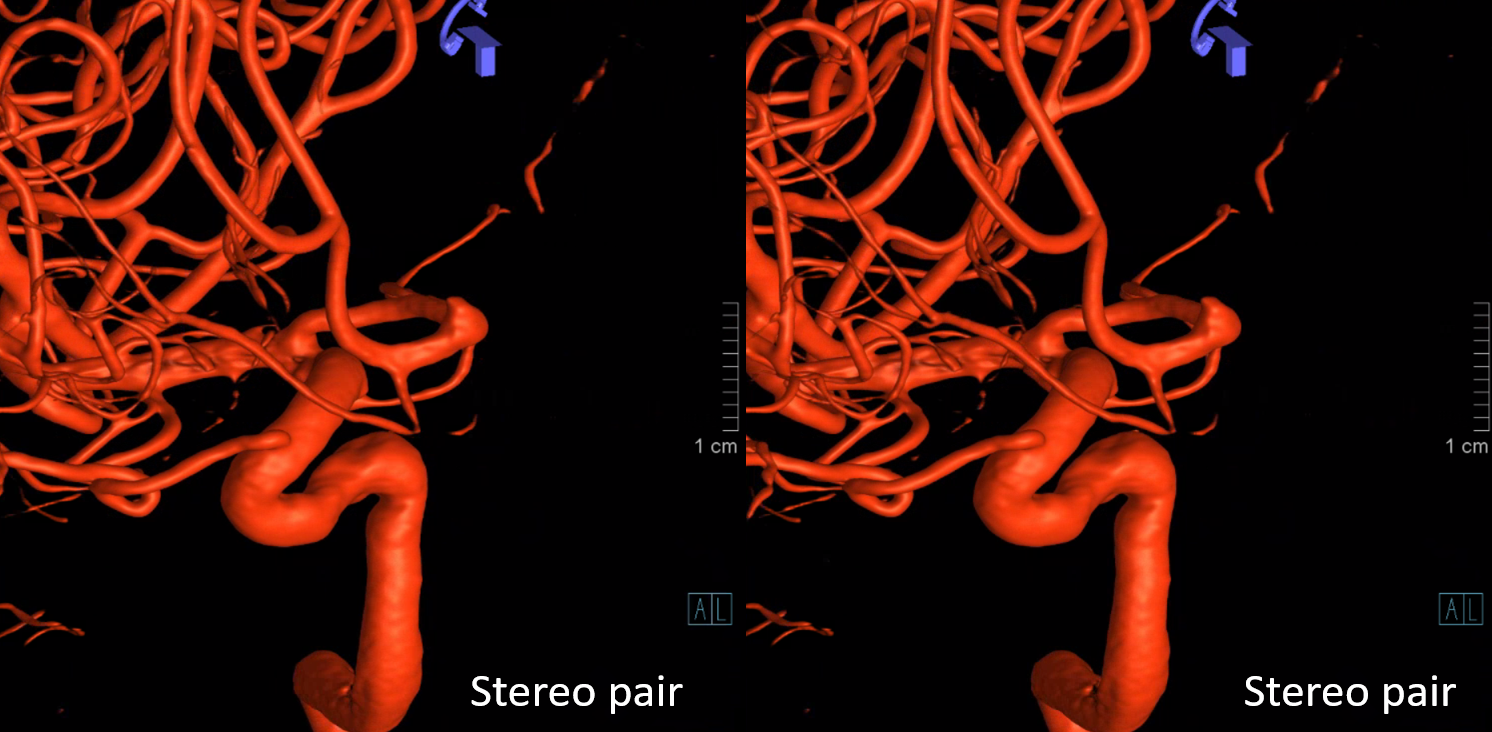
This is the typical 2D-DSA appearance of the dorsal ophthalmic (in Anaglyph stereo)
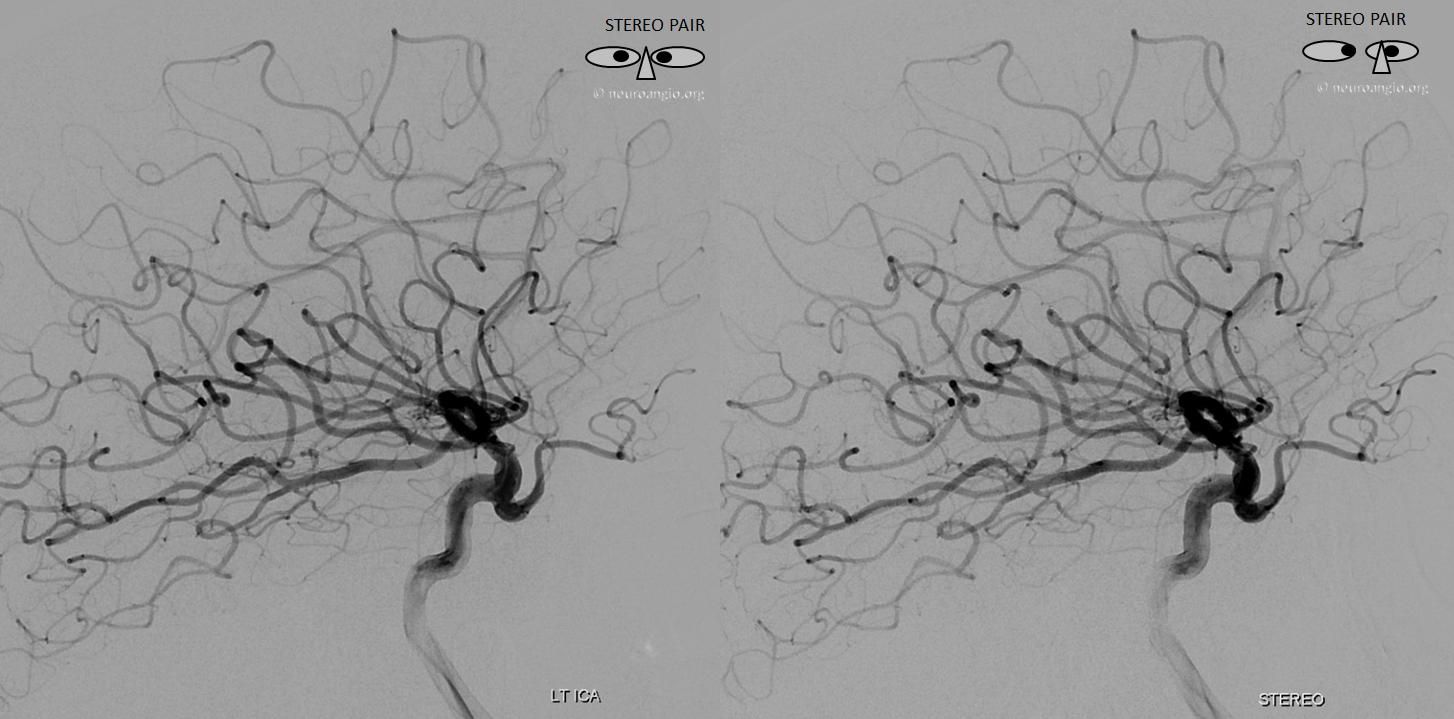
The same in cross-eye stereo
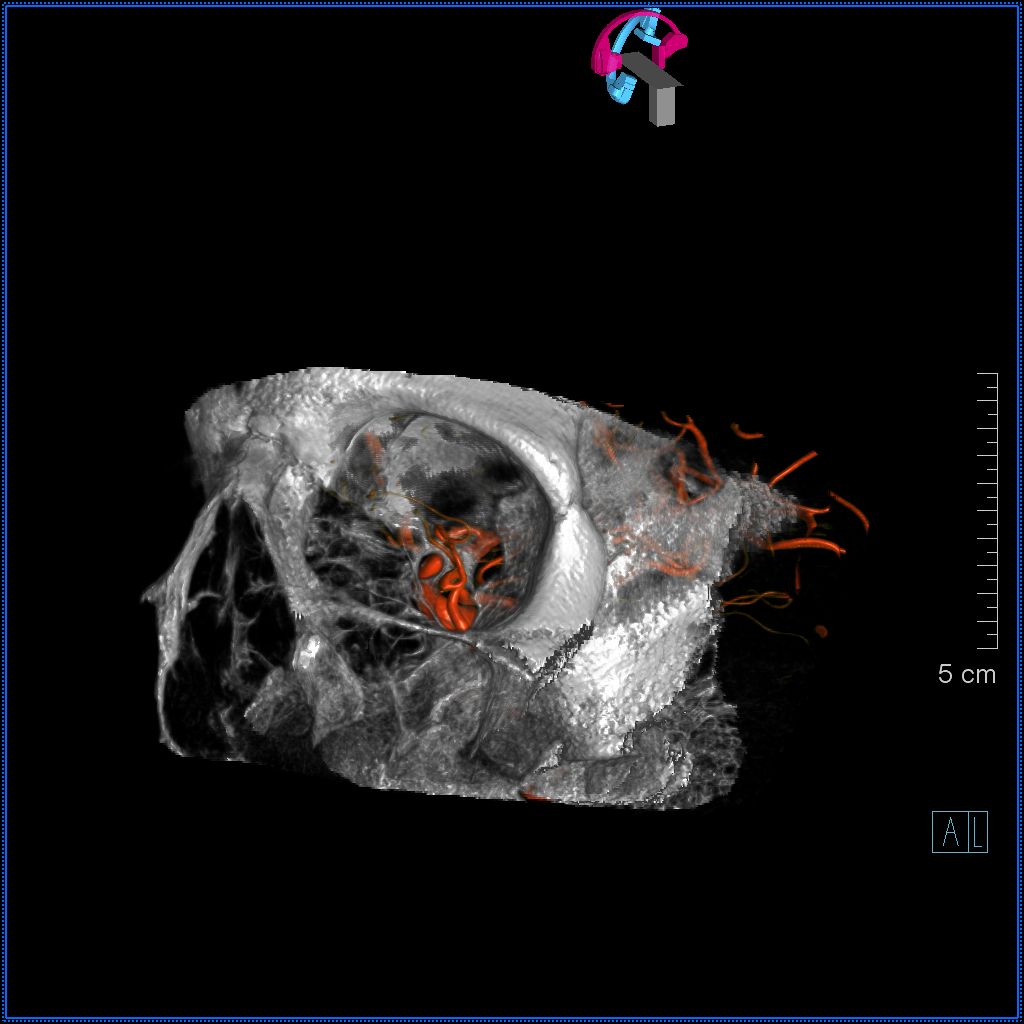
Dual volume image showing dorsal ophthalmic course through the superior orbital fissure.
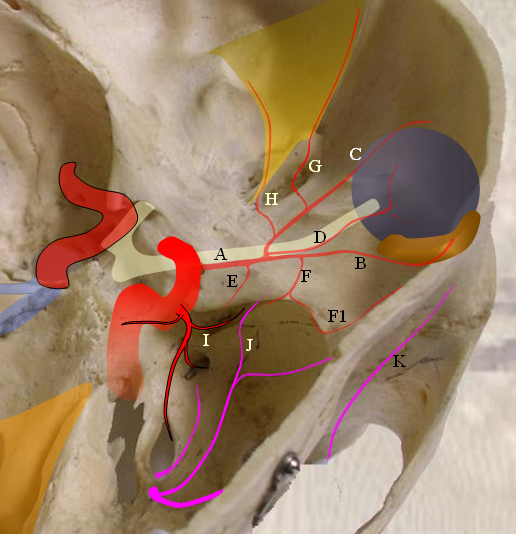
In the image below, “I” is the anteromedial branch of the ILT, which is the equivalent of the dorsal ophthalmic in the adult. The “normal” anteromedial branch is rarely visible on 2-D angio, while frequently seen on Cone Beam CT. More information is found on the “Ophthalmic Artery” page, the companion “Ventral Ophthalmic Artery” page, the ILT page, and the superior hypophyseal page.
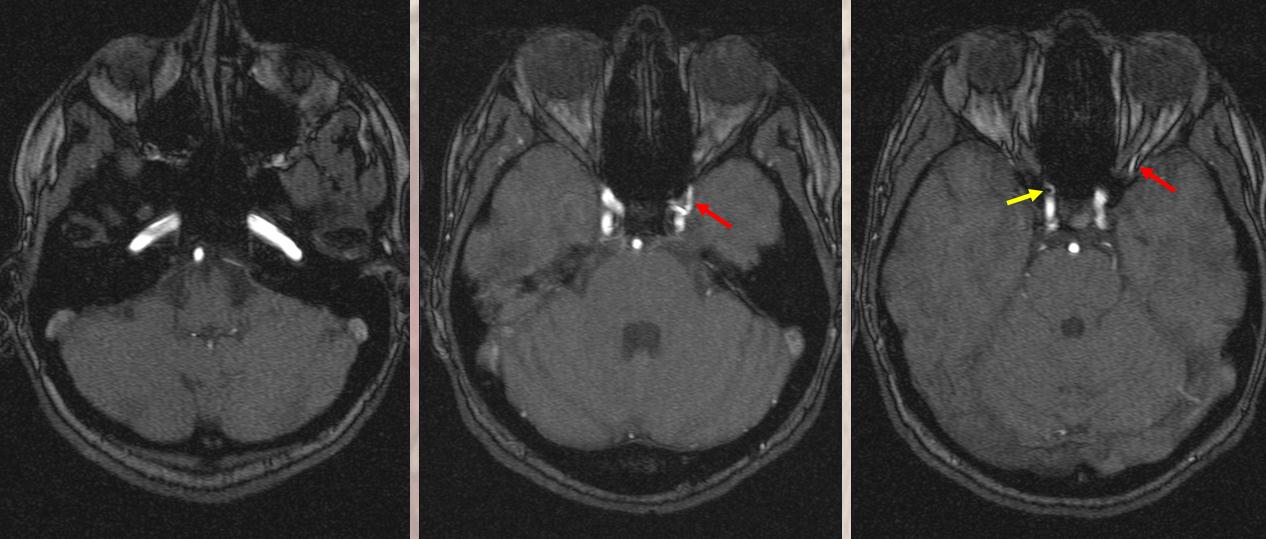
MRI appearance is reasonable. On the right (yellow) the ophthalmic origin is “normal”. On the left (red) it is dorsal.
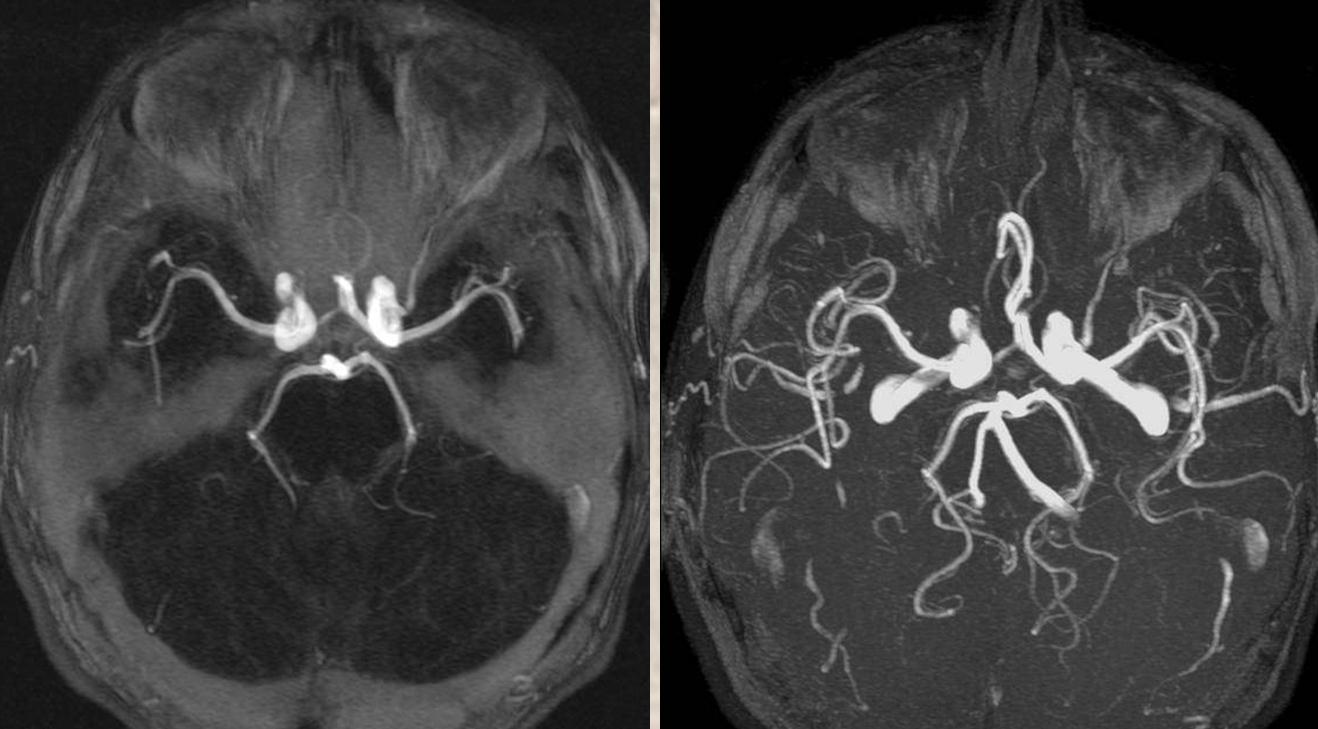
MIP images
A different patient with dorsal ophthalmic ILT origin
Another, old 2D-DSA
Even with 2D-DSA, its obvious that nature reads books except when it does not. All is a spectrum. The notion of discrete dorsal, ventral classical, menino-ophthalmics, menino-lacrimals in nonsense. All can exist together. The orbit can be supplied by some or all — the MMA, regular, dorsal ophthalmic simultaneously, and contributions of each can change with disease, spasm from catheterization, etc.
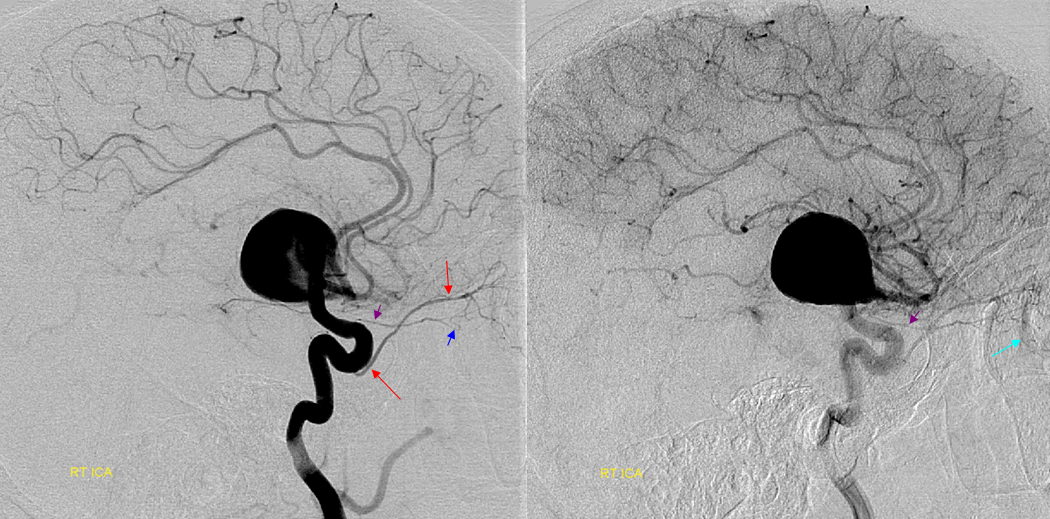
Here is a 2D example of dual supply to orbital contents by the “classic” (purple) and “dorsal” (red) ophthalmic. The embryology gugus will tell you this is due to failure of formation of an intraorbital arterial ring connecting these two embryonic vessels in the orbital apex at early stages. Since there is no ring, both vessels have to persist. Its a nice theory, but i would probably not take it too far… What is true is that in such cases the “classic” ophthalmic typically supplies the central retinal, although there is much more to the story. See a really nice case of this much below.
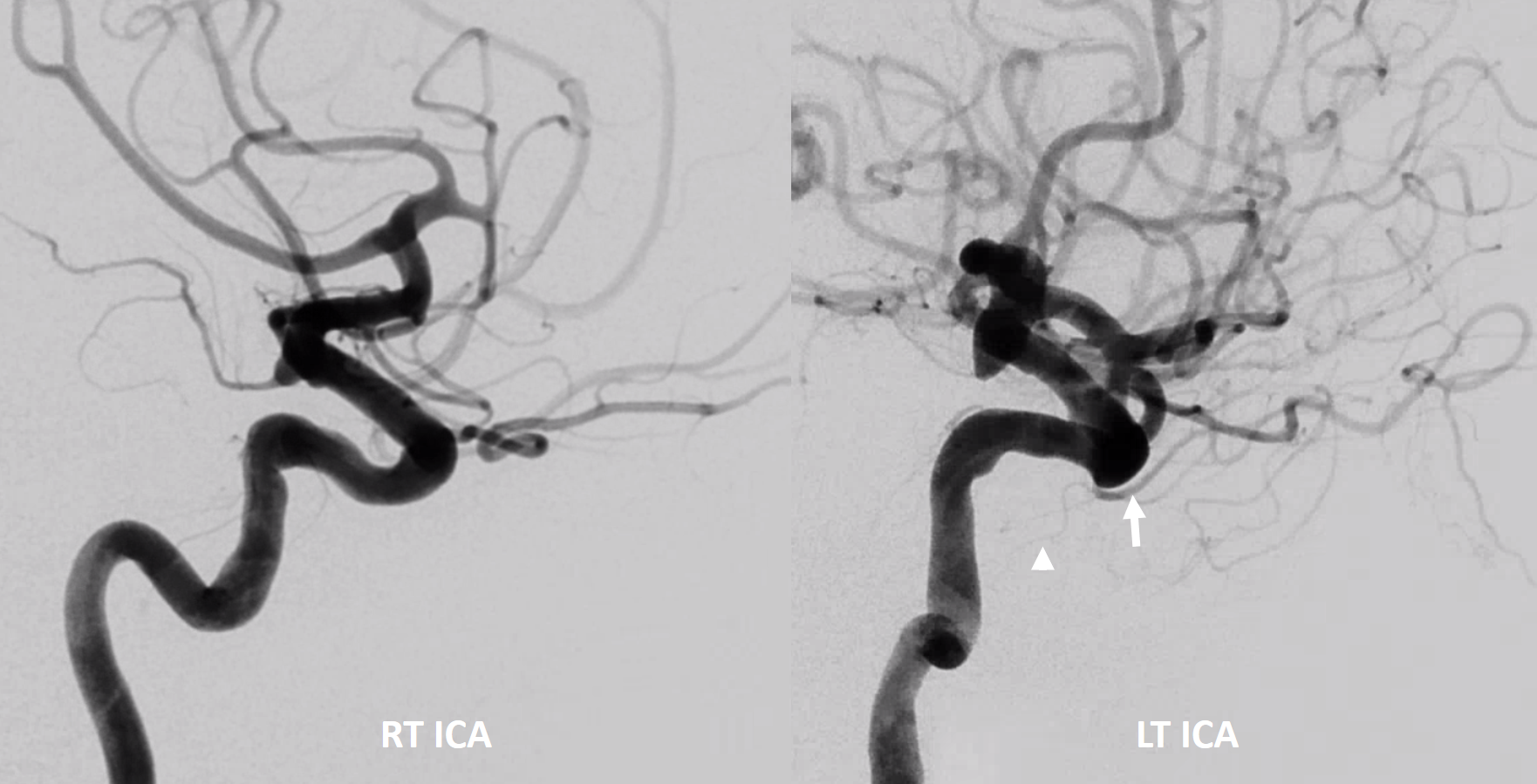
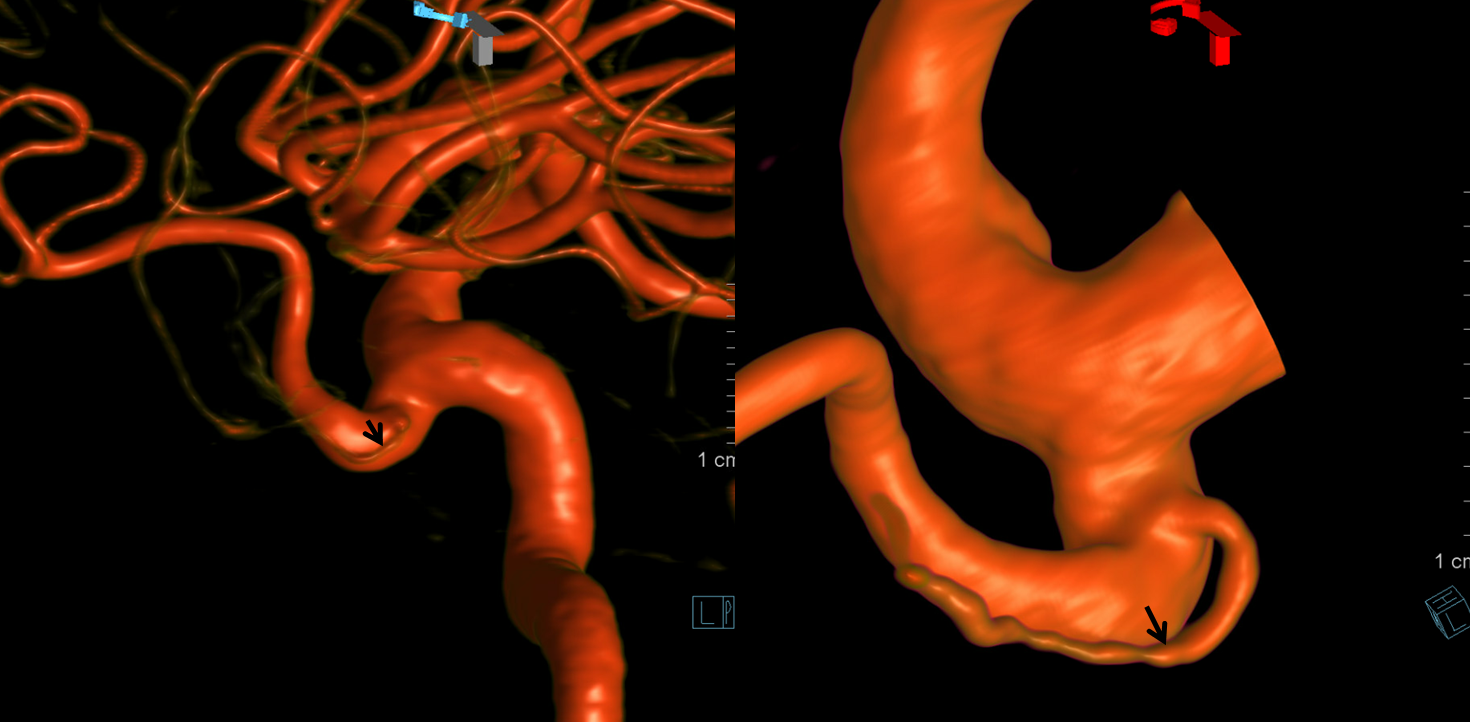
Another example of co-existence on the left (dorsal = arrow), while on the right a curious loop of the proximal ophthalmic is present. Some would postulate both sides to be representative of incomplete ophthalmic ring in early development.
Notice on left the ovale / MMA branch of ILT (white arrowhead) as well, together with the classic anteromedial / dorsal ophthalmic ILT branch (white arrow)
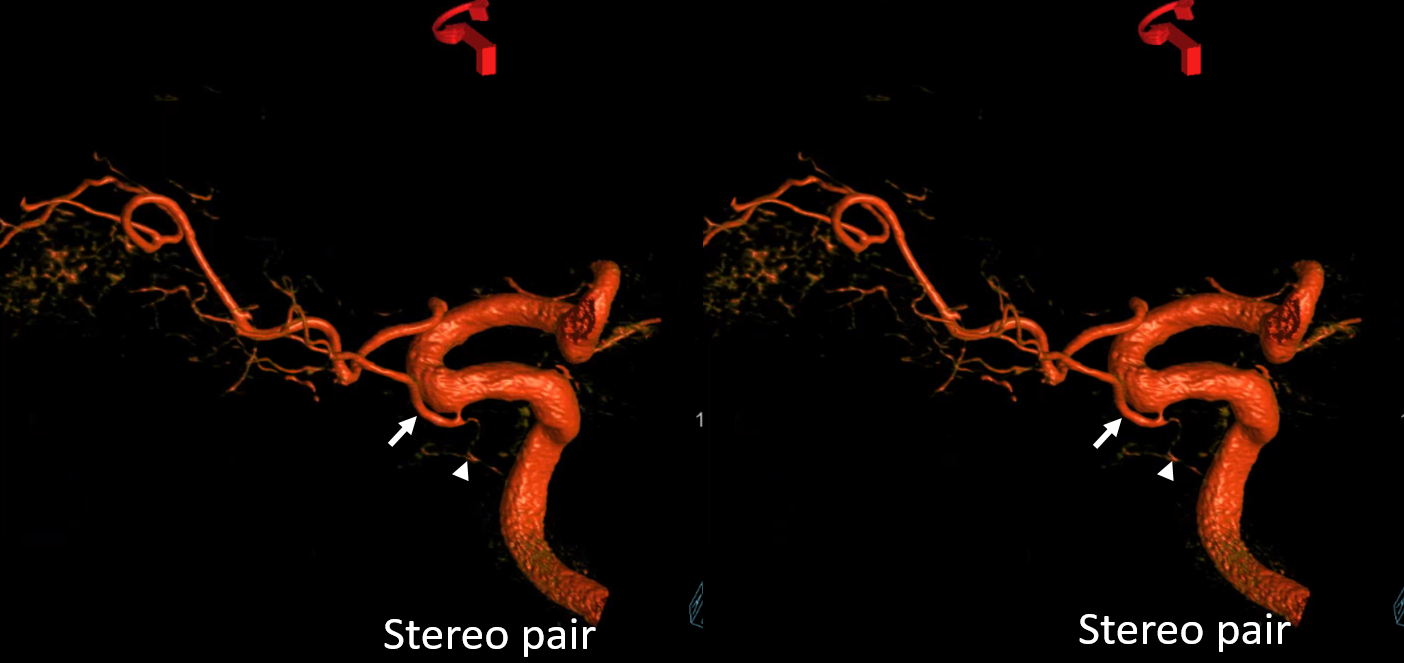
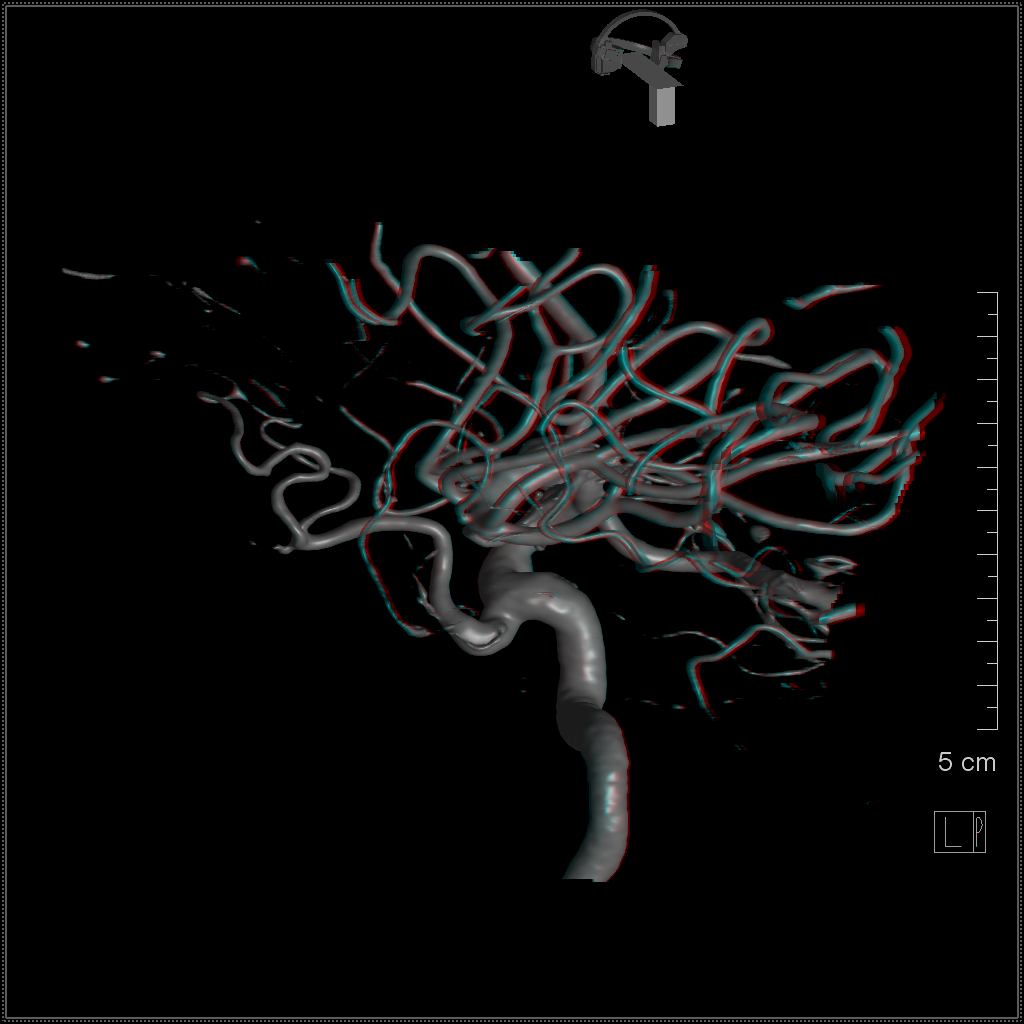
VR stereos. The theory is that the ring is meant to be where the two vessels cross each other in the orbital apex
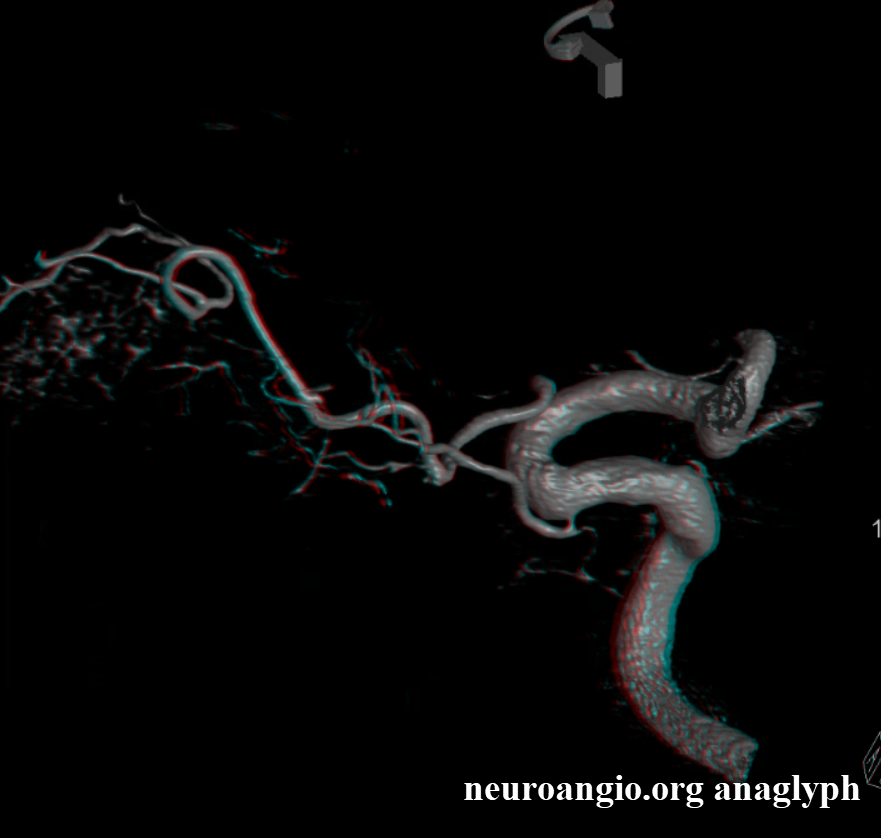
Anaglyph stereo.
Cross-eye stereo of the ring anomaly
Anaglyph

ILT relationship
Another case, showing another branch of the ILT/dorsal ophthalmic (black arrows), possibly heading towards the lacrimal region. The point is that Cone Beam CT allows us to establish the vascular disposition on case-specific basis, instead of hoping our imperfect theories are right somehow. Knowing the theories is important, especially when you don’t have adequate imaging. But when you do, get the pictures…
ADVANCED ANATOMY
Optic Nerve Supply in Dorsal Ophthalmic Disposition
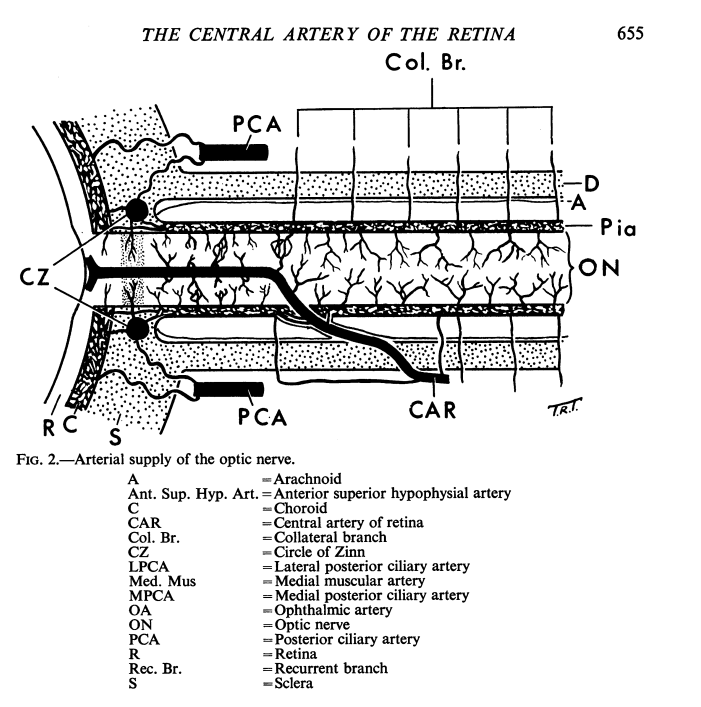
One of the key questions is supply to the canalicular and apex / retrobulbar portions of the optic nerve. The best data to date comes from work of Sohan Singh Hayreh. In classic ophthalmic disposition, central retinal artery supplies the nerve distal to its point of entry through the nerve sheath (locations are intraorbital, intravaginal – inside sheath, and intraneural). Proximal to the central retinal artery, the supply is less clear. Pial branches from the central retinal seem to be present, along with “collateral” branches from the ophthalmic artery. Both types supply the dura and the nerve “from the outside” — there is little support for consistent presence of a “central artery of the optic nerve”. The superior hypophyseals dominate the chiasm and the intracranial portion as well as the canaliculus, and are in balance with the “collateral branches”. The following diagram from Hayreh’s “THE CENTRAL ARTERY OF THE RETINA: ITS ROLE IN THE BLOOD SUPPLY OF THE OPTIC NERVE” is probably the best pictorial representation — all applying to the classic ophthalmic artery disposition.
What about dorsal ophthalmic, which does not traverse the optic canal? This seems to be an entirely unexplored subject, as far as we know, and again cone beam CT suggests the answer.
In the dispositions we have studied with cone beam CT, the supply comes not from recurrent branch of the central retinal, but separately from the more proximal intraorbital “dorsal” ophthalmic. At limit of CBCT resolution, there appear to be both dural and intradural branches, in balance with the superior hypophyseals. Both seem to be located at the periphery of the expected optic nerve location. More proximally, the superior hypophyseals — which are an extremely constant set of vessels — supply the chiasm and nerve.
These observations make sense to the extent that they seem consistent with the “pial” or peripheral supply of the optic nerve / sheath complex proximal to the central retinal artery. The only difference is that in dorsal ophthalmic disposition there is some kind of “recurrent ophthalmic” branch, if you will, which supplies the dura, optic nerve, and probably other structures of the orbital apex.
Below are some examples
Raw Data Movies
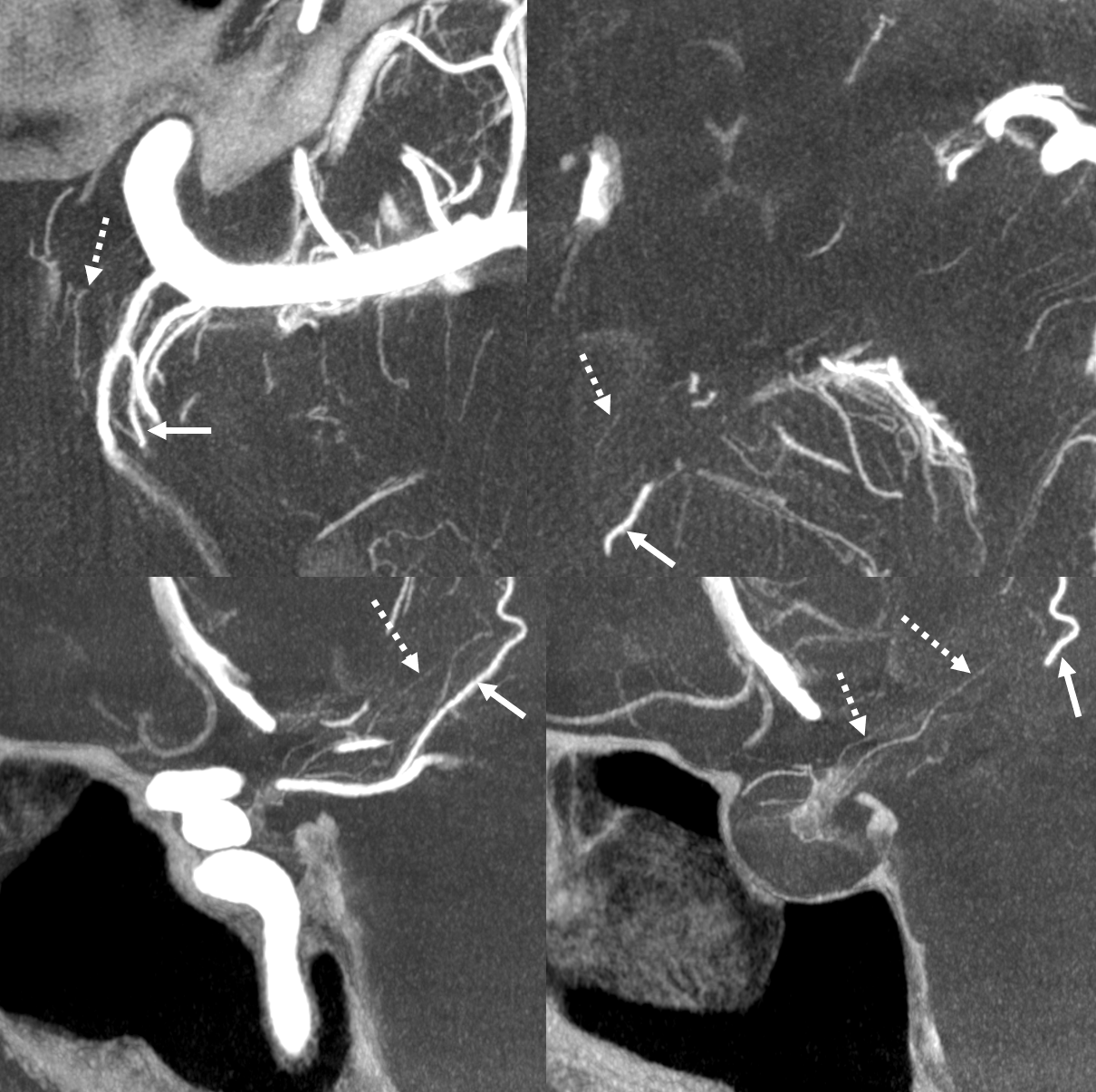
Various reconstructions of the above raw data. Dorsal ophthalmic (anteromedial trunk of ILT), with recurrent tentorial branch (ball arrow) extending posteriorly as the artery of the free margin of tentorium (Bernasconi-Cassinari). A separate origin of the spinosum/ovale ILT branches (posterolateral) is shown by square end arrow. MIP images show the “recurrent ophthalmic” branch (arrows) coursing posteriorly from the orbit towards the apex and optic canal. Some of its branches appear to supply the optic nerve sheath (dashed arrows) as well as proximal optic nerve (arrows). The intracranial portion of the nerve is supplied by the superior hypophyseals (arrowheads)
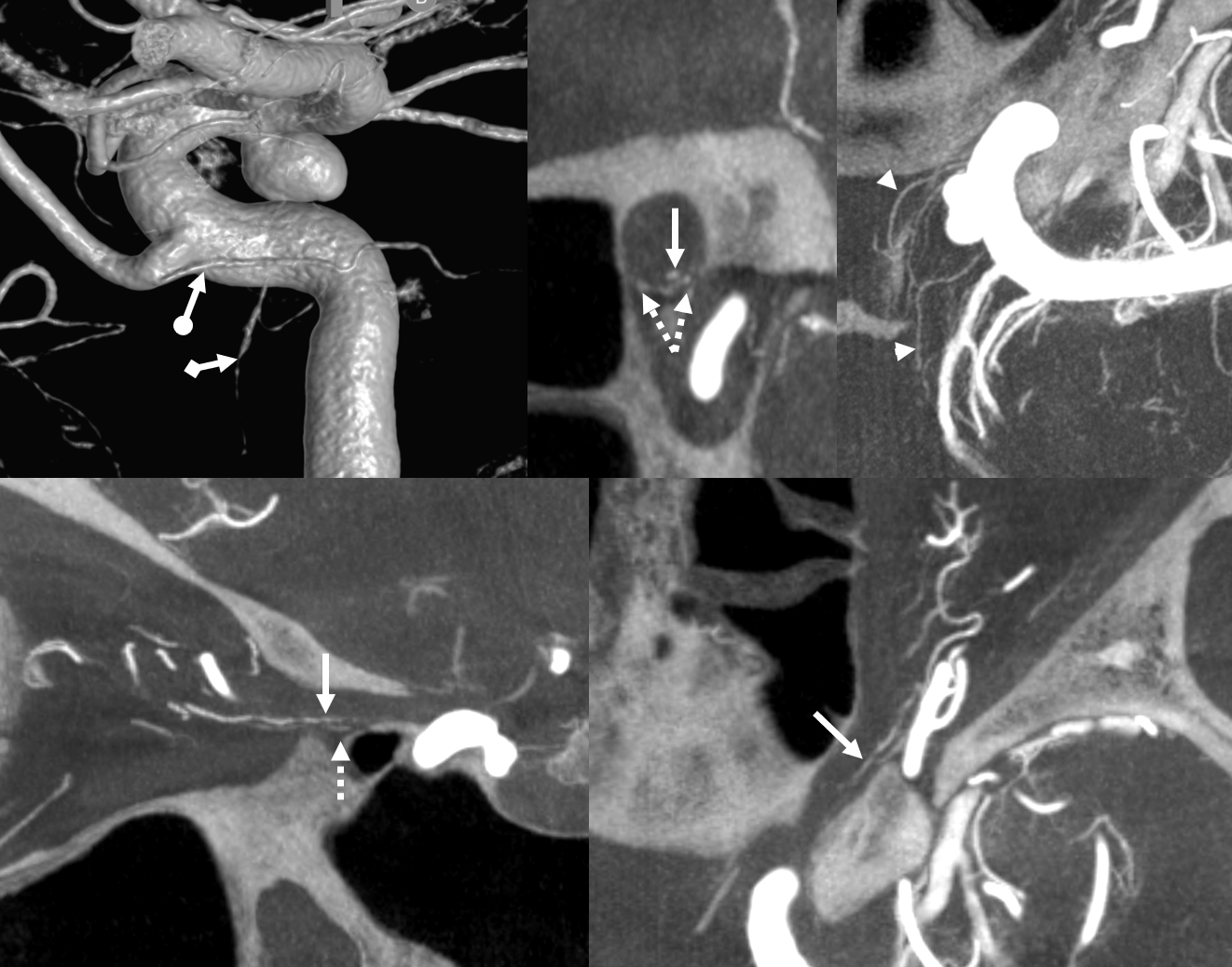
Interestingly, in the same patient, the superior hypophyseals (dashed arrows in image below) also appear to supply at least some portions of the hypothalamus. The dominant PCOM anterior thalamoperforator (also known as the tuberothalamic artery) is shown by solid arrows
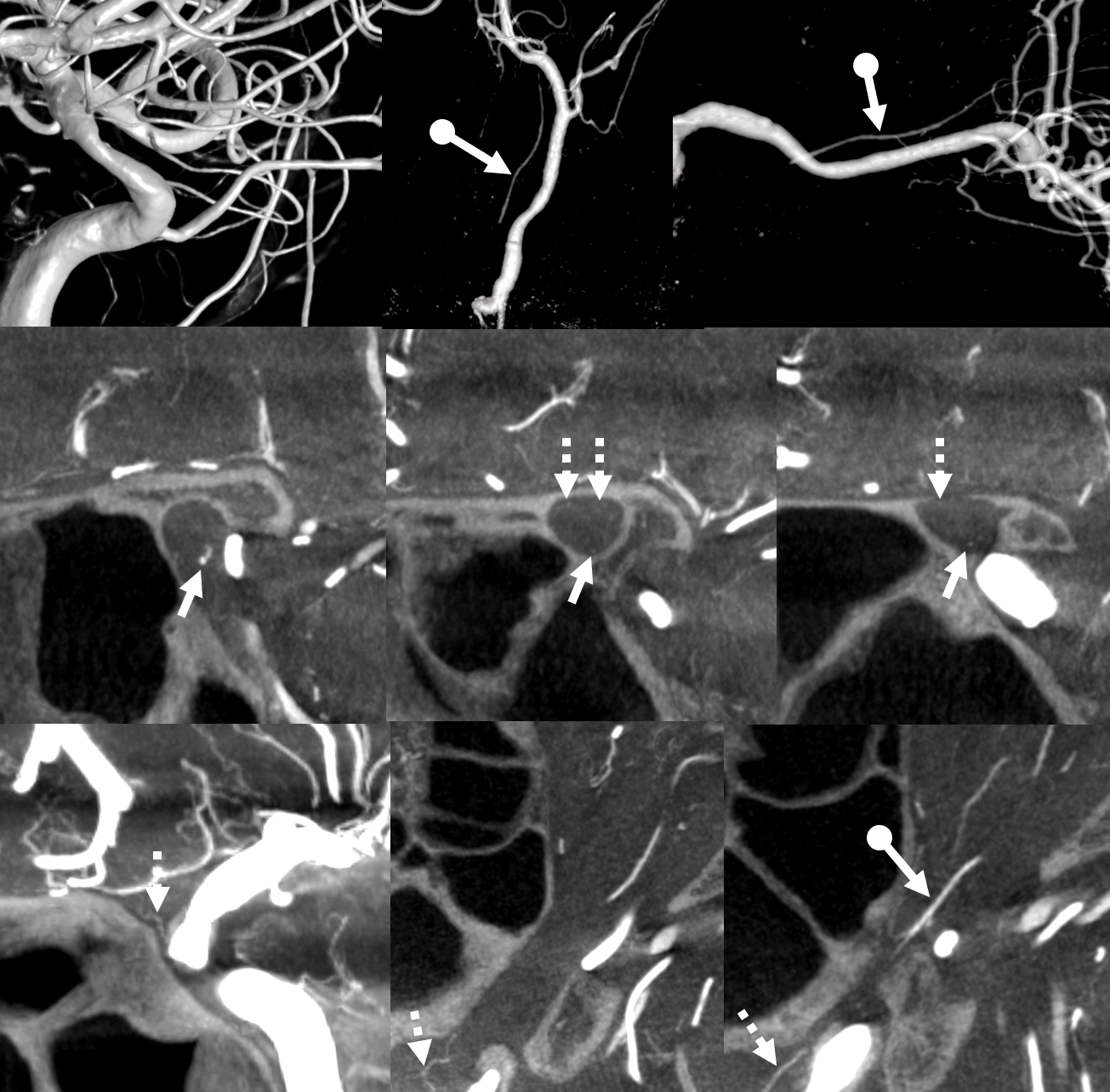
Another case, raw data below
The “recurrent ophthalmic” artery is shown by ball arrows, supplying the dura and probably the canalicular / apex portions of the optic nerve (arrows). These are in balance with the prominent superior hypophyseal arteries (dashed arrows)
SUPPLY TO GLOBE
The point here is that there is much more to optic nerve and globe supply that the central retinal artery. There are short and long ciliary arteries, which contribute to not only choroid but variably to retina in at least one third of people (circle of Zinn, various connections inside the globe). Then again there is the uncertain, variable, but extremely important supply to the optic nerve proximal to the central retinal, as you saw above.
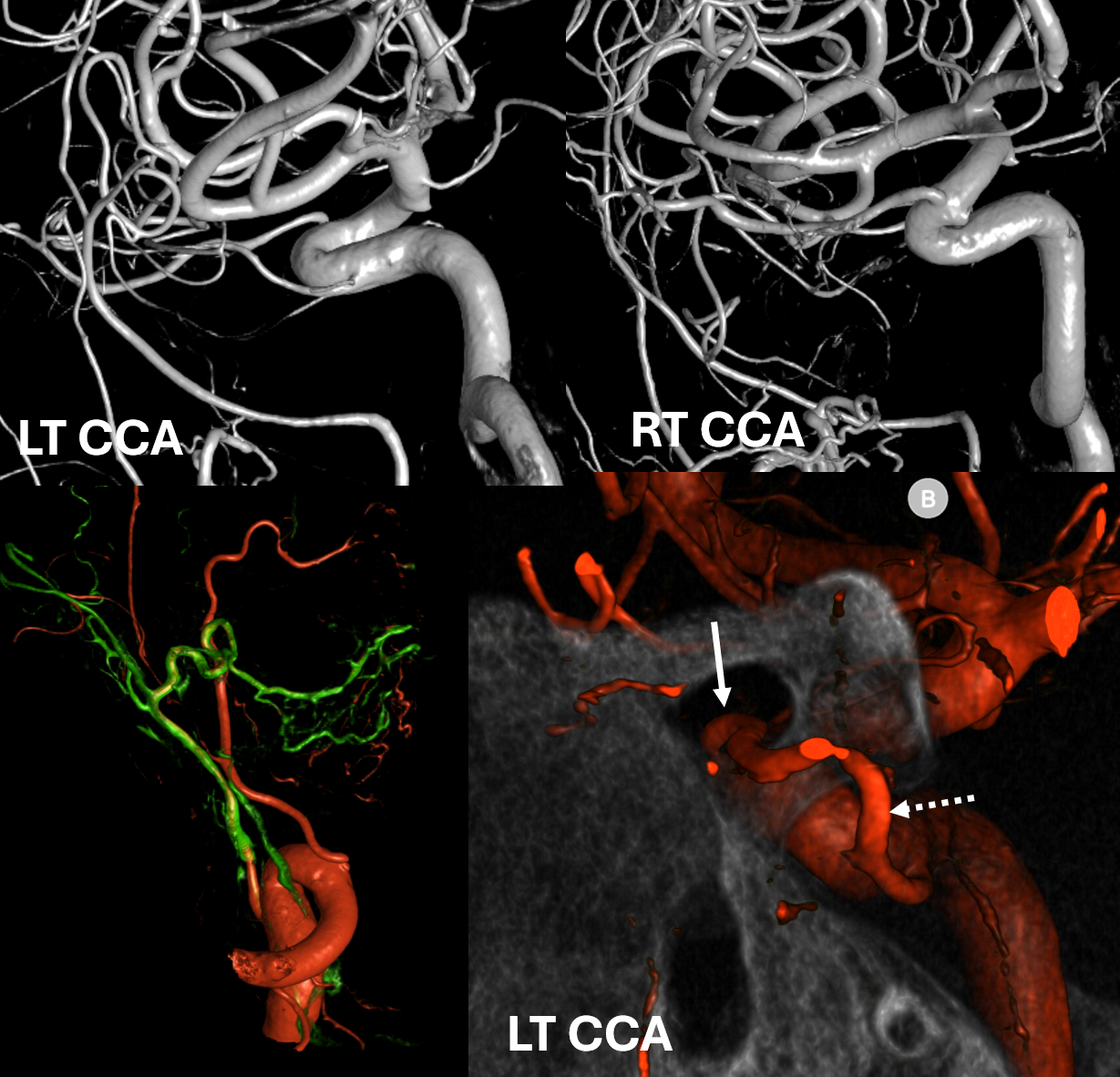
Here is a unique case of a frontal base meningioma, with bilateral ophthalmic supply — except one is mix of classic and dorsal. Lets see what happens
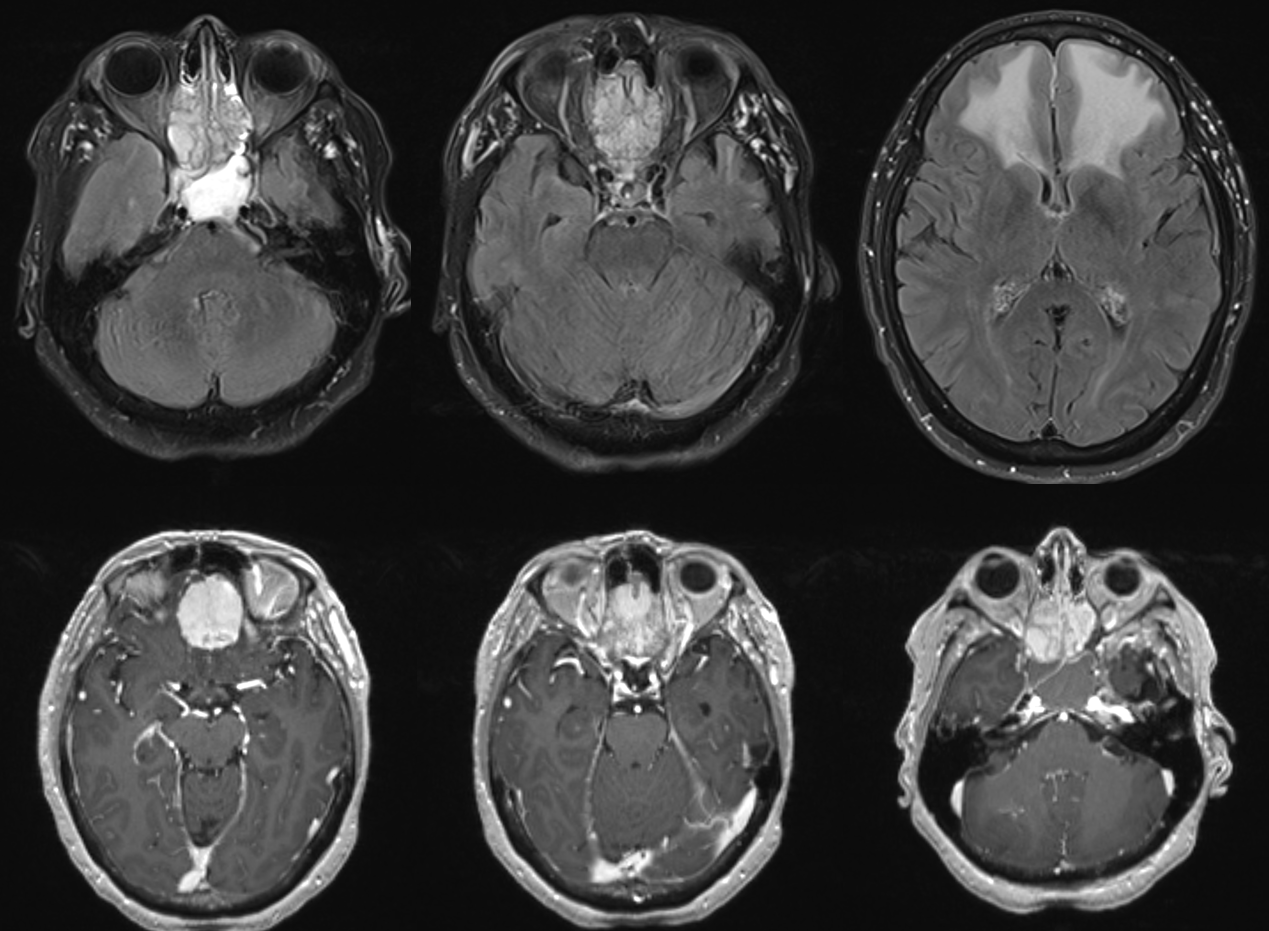
On the right, classic ophthalmic. On the left, a mix of classic and dorsal. Note classic in the optic canal (arrow) and dorsal in the SOF (dashed arrow)
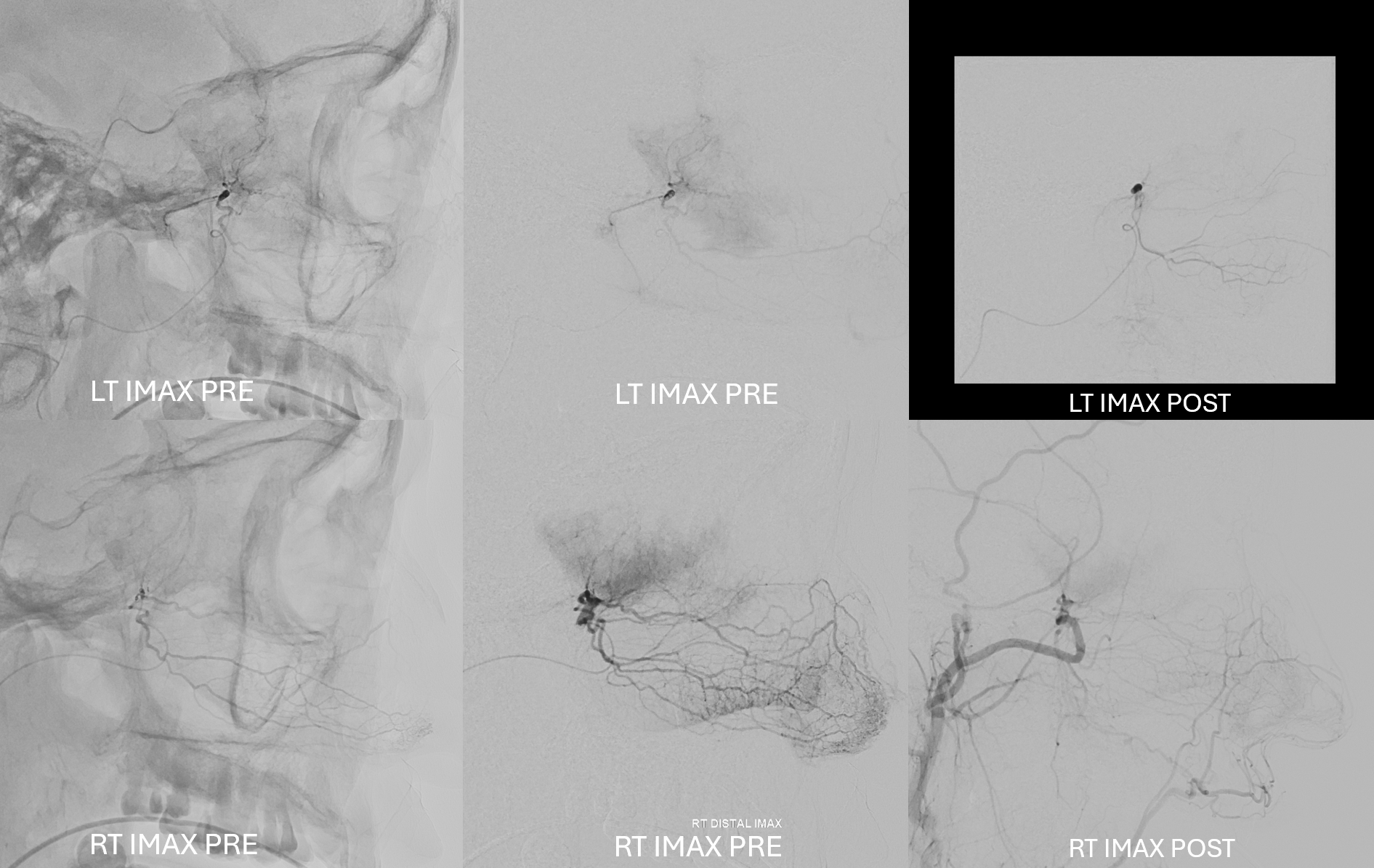
Some good embo can actually be done from the distal IMAX. Note preferential supply to the septum from the right
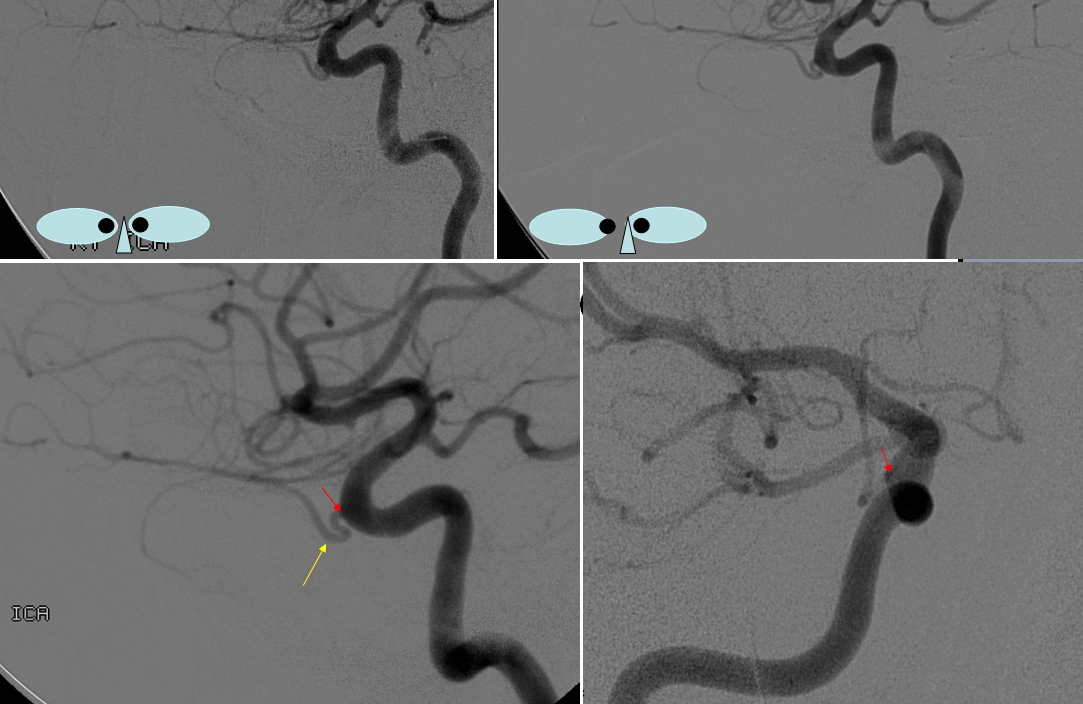
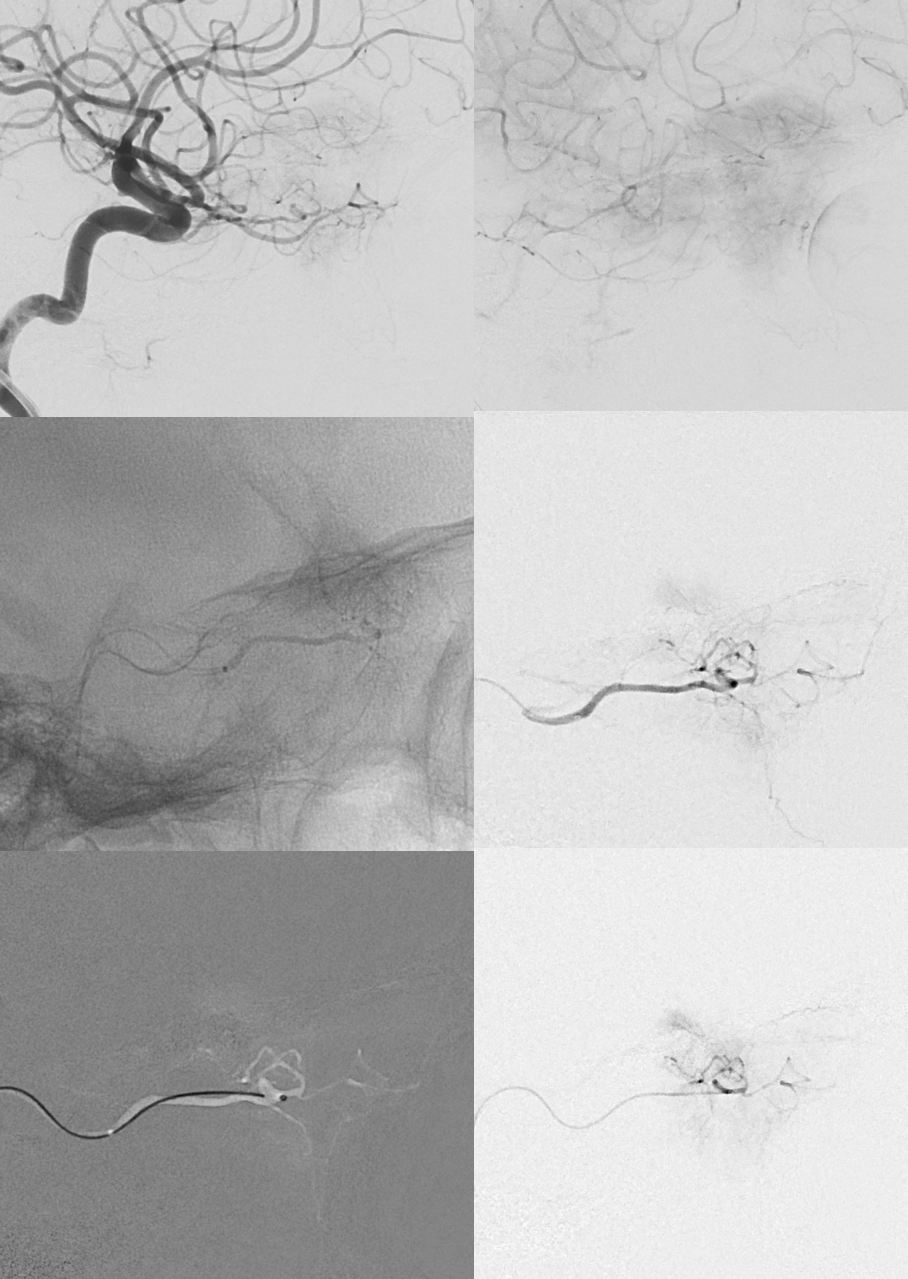
Here’s what happens. Top views are left ICA. Middle views are a relatively proximal position in the dorsal ophthalmic, while bottom views are from more distal position. Neither position, in 2D-DSA, shows globe blush. Note, however, something that looks to be projecting along the expected location of the optic nerve/canal in middle images. This is no longer present in distal (bottom) row.
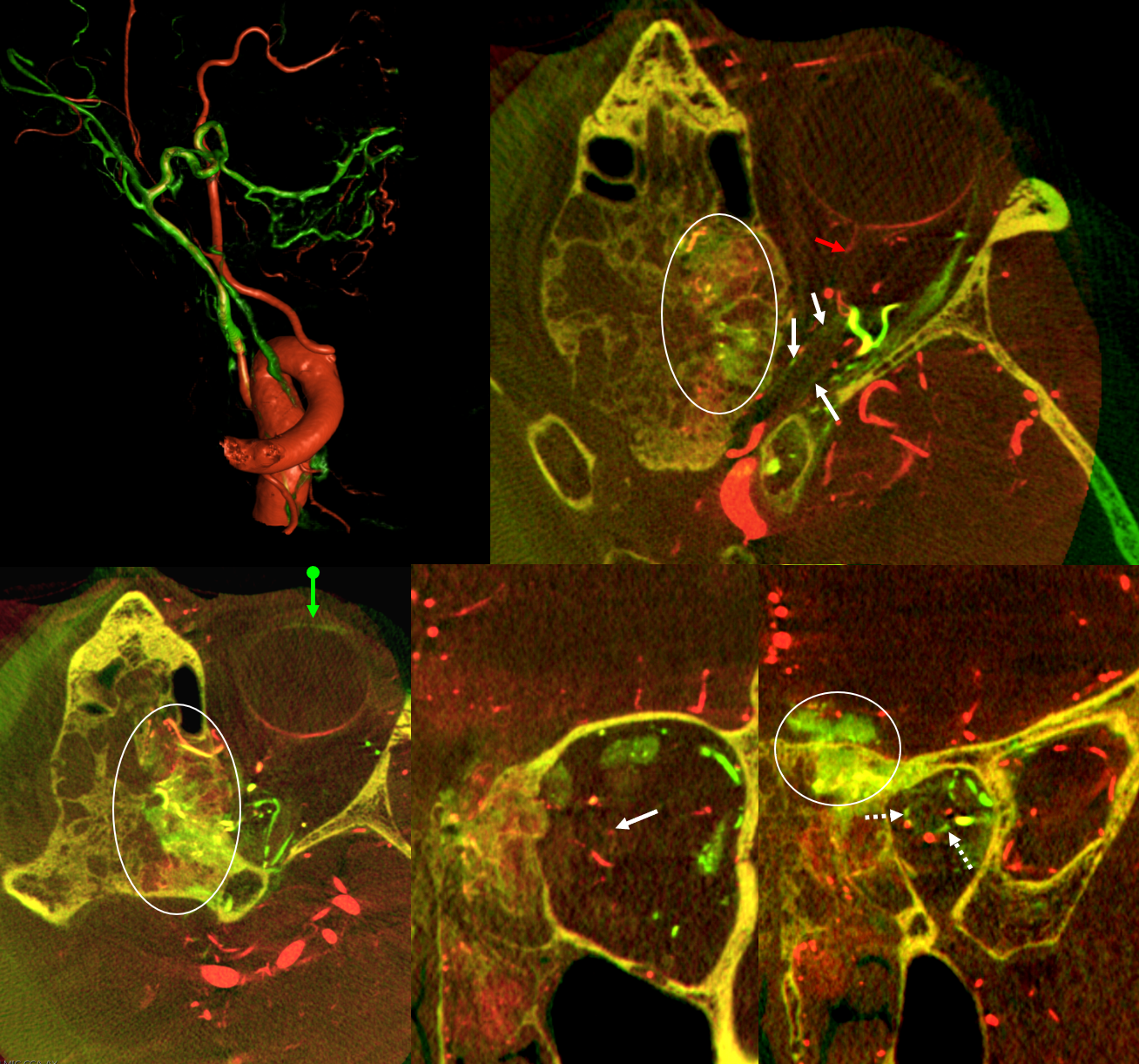
Below is a 6D fusion of left ICA (red) DYNA and subselective dorsal ophthalmic proximal position micro DYNA (green). Where these fuse you see yellow. Look at the wealth of actionable information here. The hyperostotic tumor is supplied by both (ovals). The central retinal (red arrow) comes off the classic ophthalmic. But there is so much more. Note supply to the proximal optic nerve sheath (white arrows axial, dashed arrows coronal oblique) from dorsal ophthalmic in green. The anterior chamber / lens region also green (ball arrow)
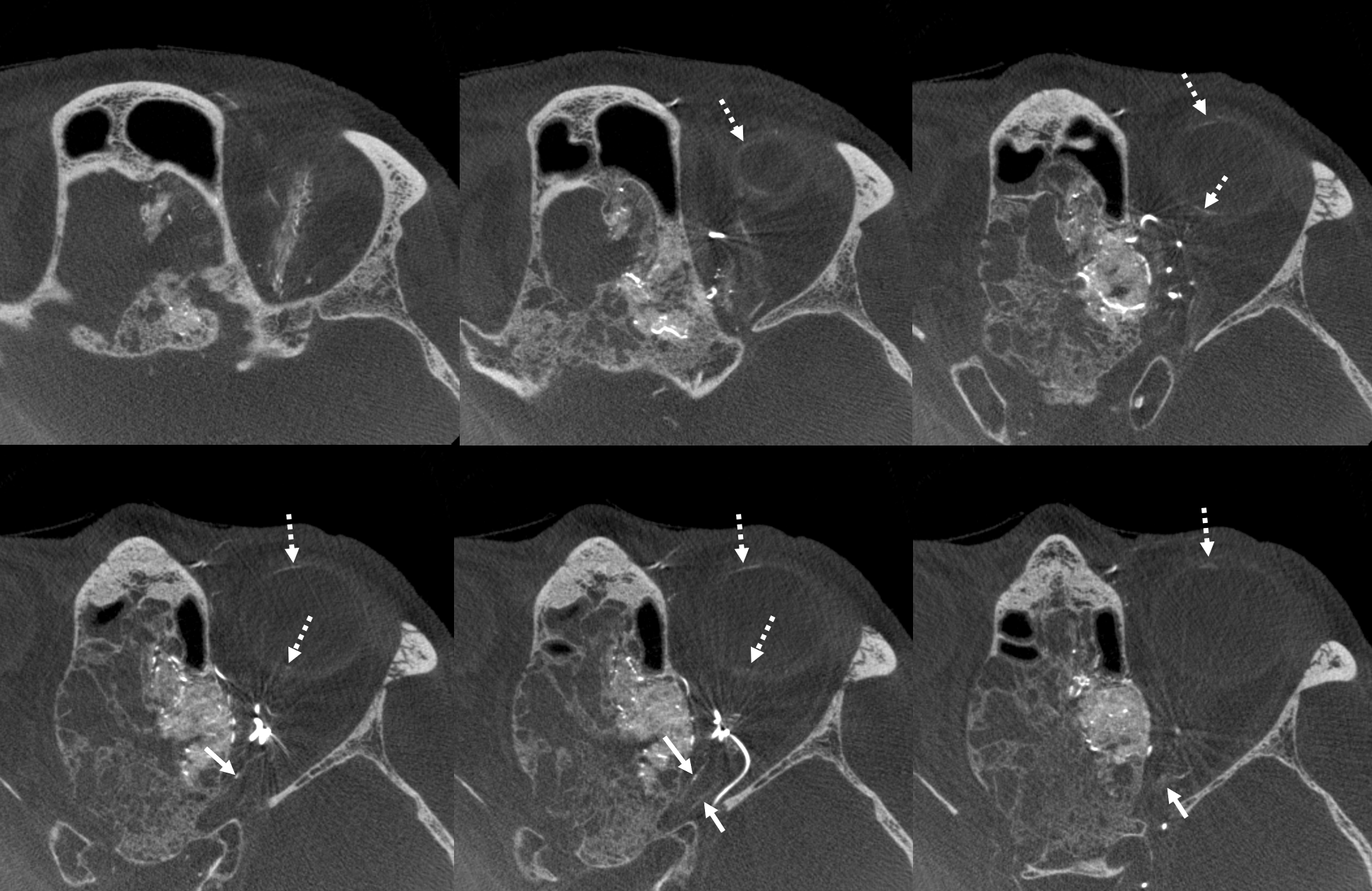
Single phase HR-CBCT of the dorsal ophthalmic (3D, not 6D). It is easier to see the extensive contributions to the globe (dashed arrows), including posterior globe (probably choroid, but could be retina also), as well as long segment of the proximal intraorbital and intracanalicular optic nerve (arrows).
6D Datasets
Even though dorsal ophthalmic does not directly supply the central retinal, there are plenty of other structures to be concerned about with embo — and it would not at all be apparent without HR-CBCT. No embo was done
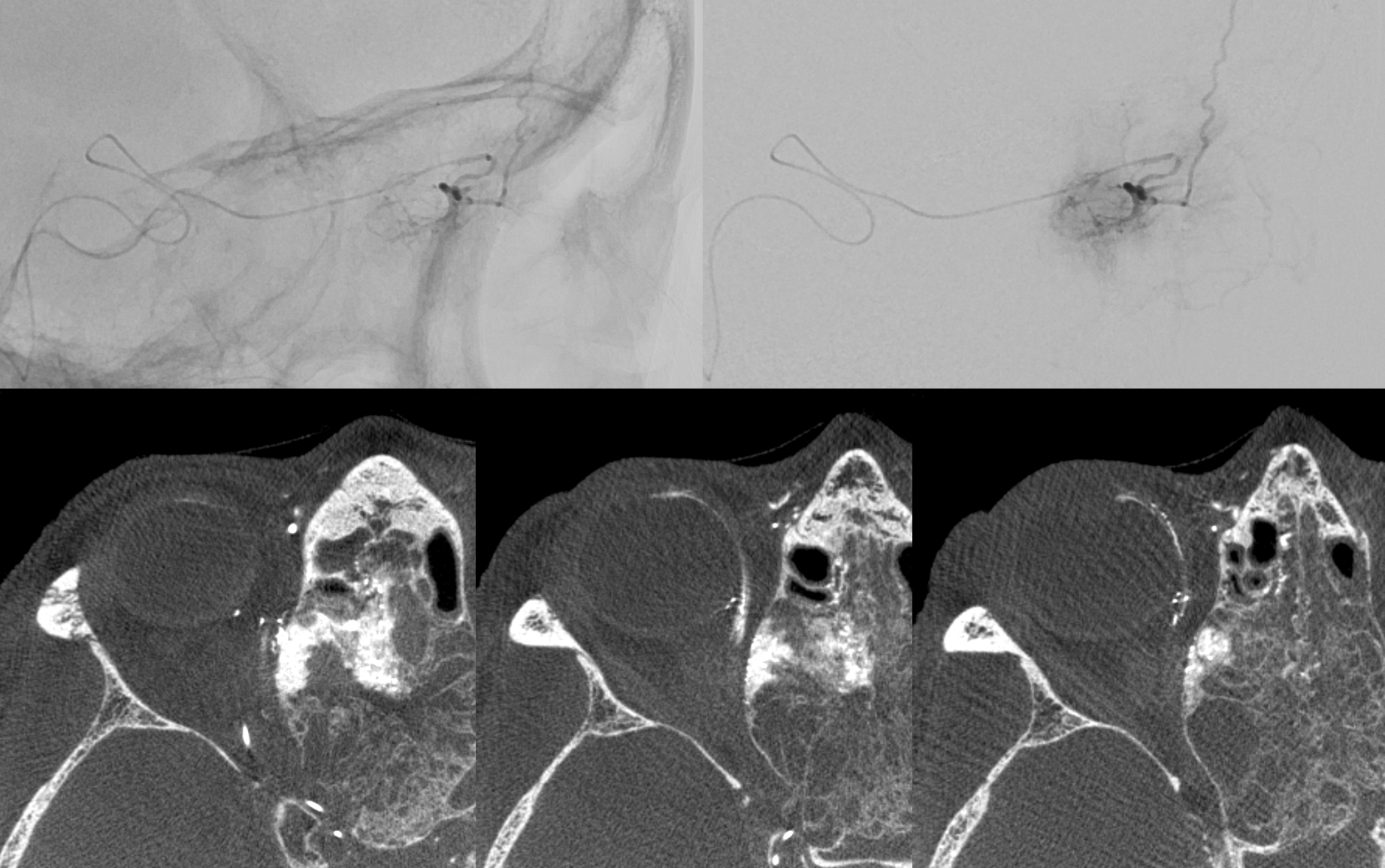
What about the “classic” ophthalmic on the right?
Distal microcatheter position there — note contributions to the globe via the ciliary arteries. No indication of anything else important. This may be a reasonable embolization position, but given small amount of not very vascular tumor, its not worth it
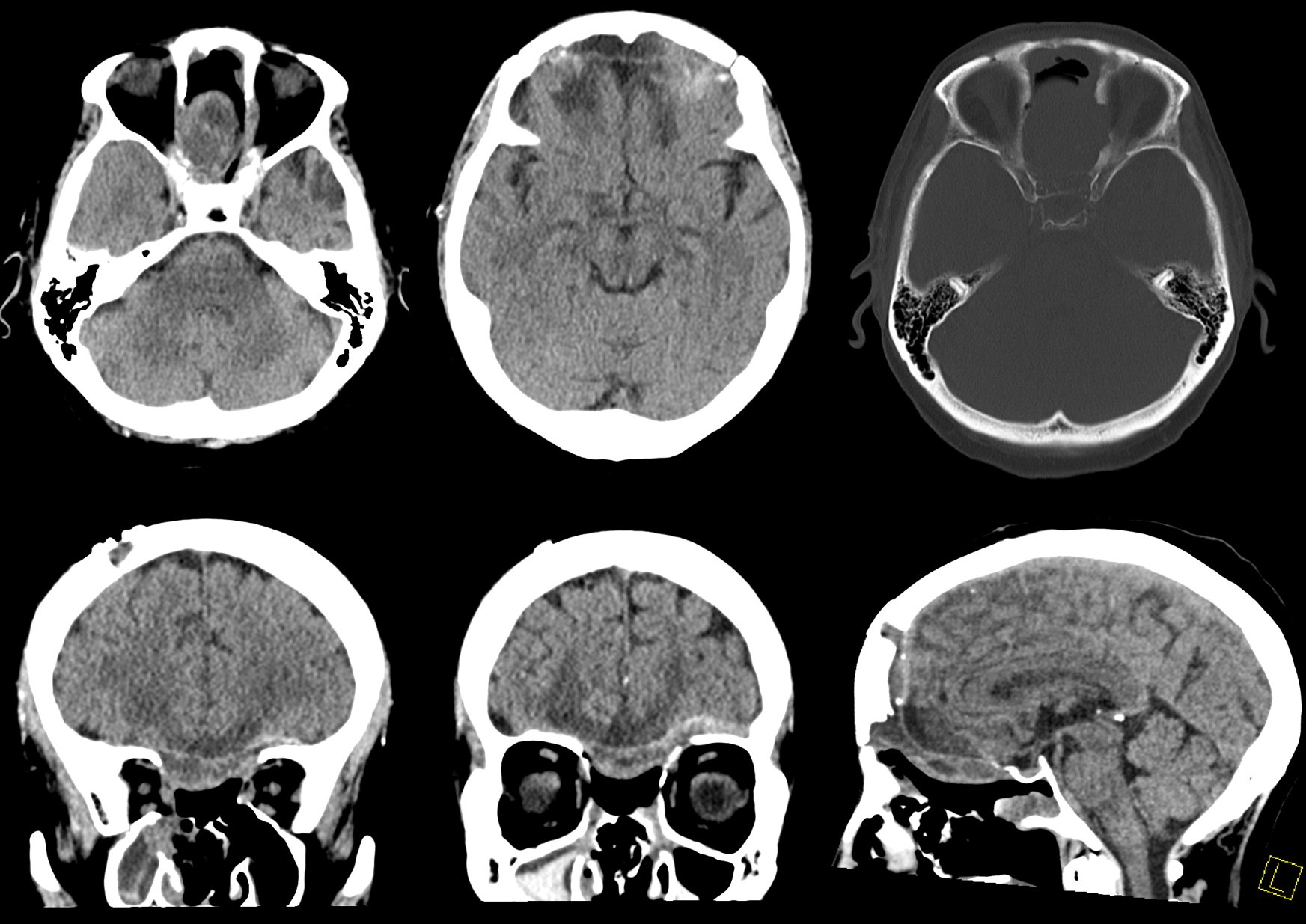
Post resection
Conclusions
There is much more to the eye / globe than central retinal artery. HR-CBCT is essential for safety. Some distal positions are known to be better than others — namely the ones that lead outside the orbit — the ethmoidal position for its corresponding fistula, or recurrent meningeal position above the orbital roof for its potential contribution to meningiomas. Inside the orbit, buyer beware.
Back to Ophthalmic Artery