
Case Courtesy Dan Meila, M.D., Ph. D. Head of Pediatric Neurointerventional Radiology and Vascular Anomalies Center, of Hannover and Neuss, Germany This case is young at heart
History is left MCA syndrome, TICI 2b M1 thrombectomy, with a residual M4 occlusion. Possible Wernicke compromise? Most of us would leave this one alone. But should we? What is the morbidity of aspiration attempt by an experienced practitioner in a patient under general anesthesia? May well be worth the try.
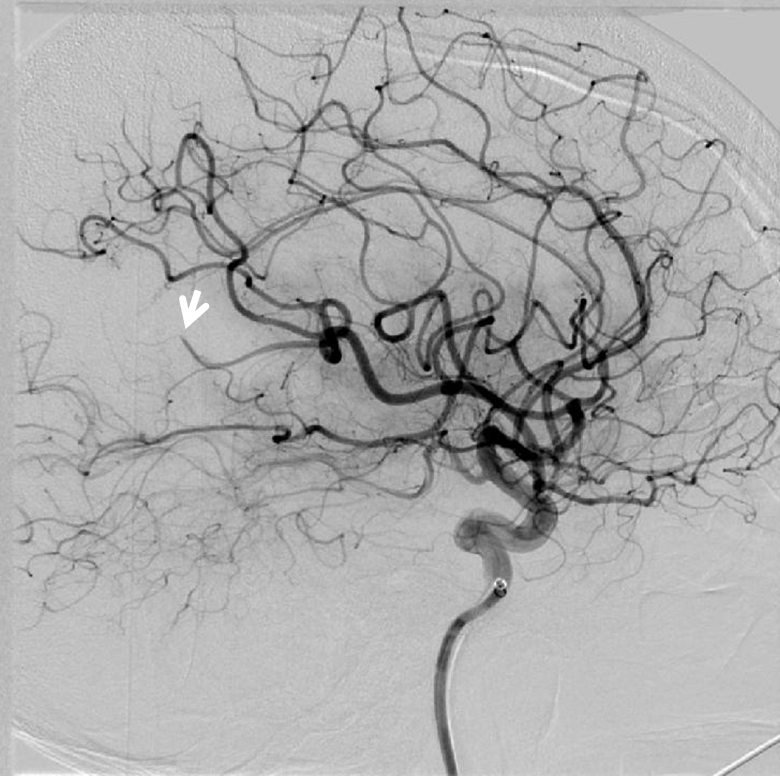
Its an M4 all right…

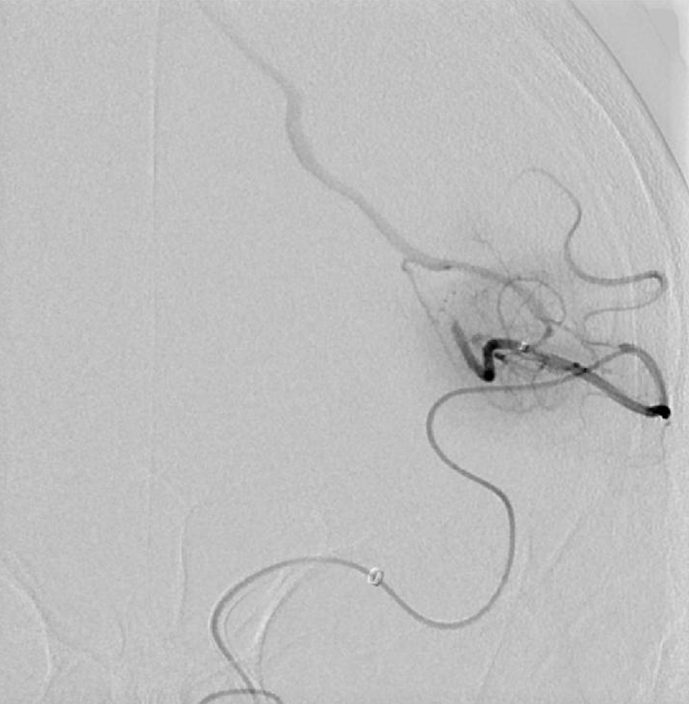
The longest headway is still too short, so Sofia 6 (125 cm) was removed, and is not there to help with aspiration. The 027 needs to go it alone (with guide aspiration of course).

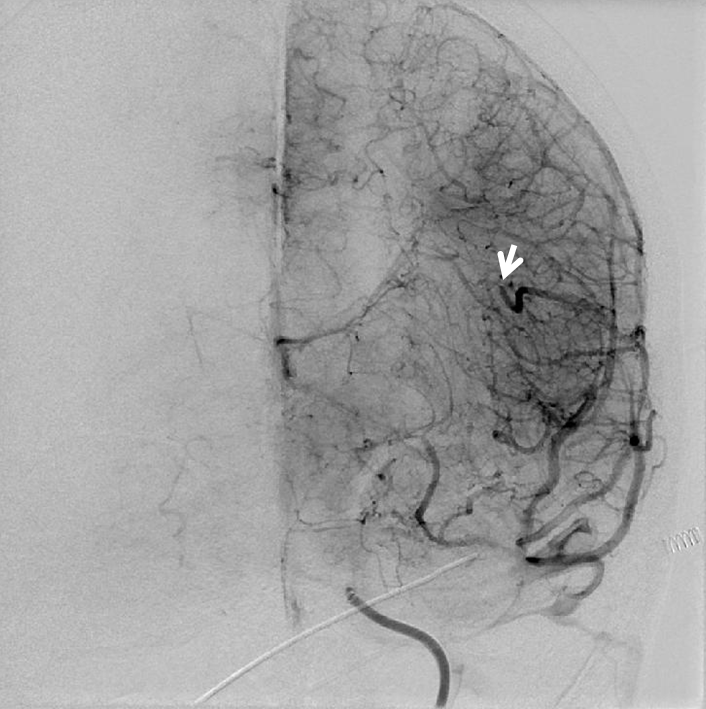
Post aspiration
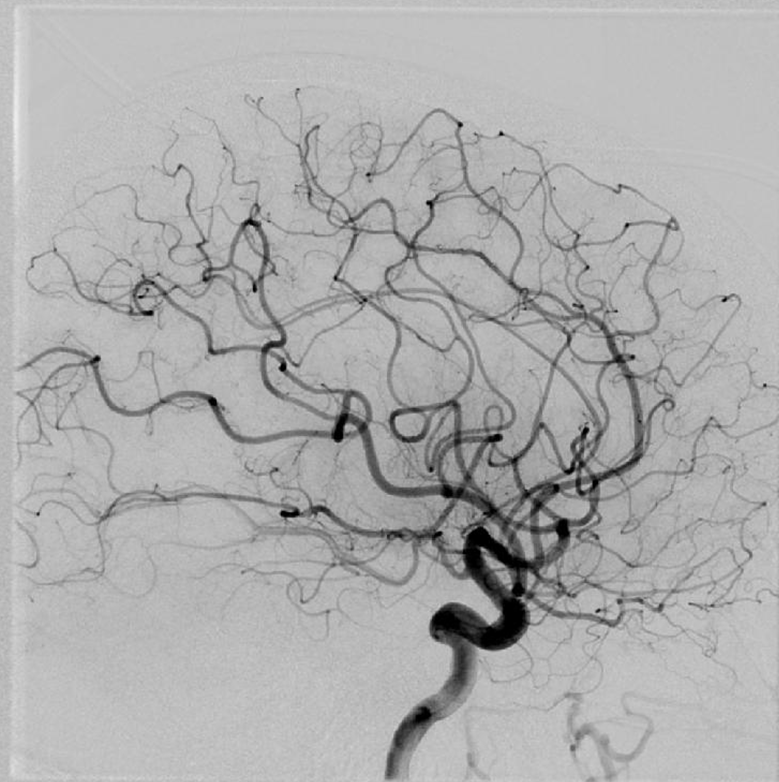

Notice how even in this M4 the clot is larger than the 027
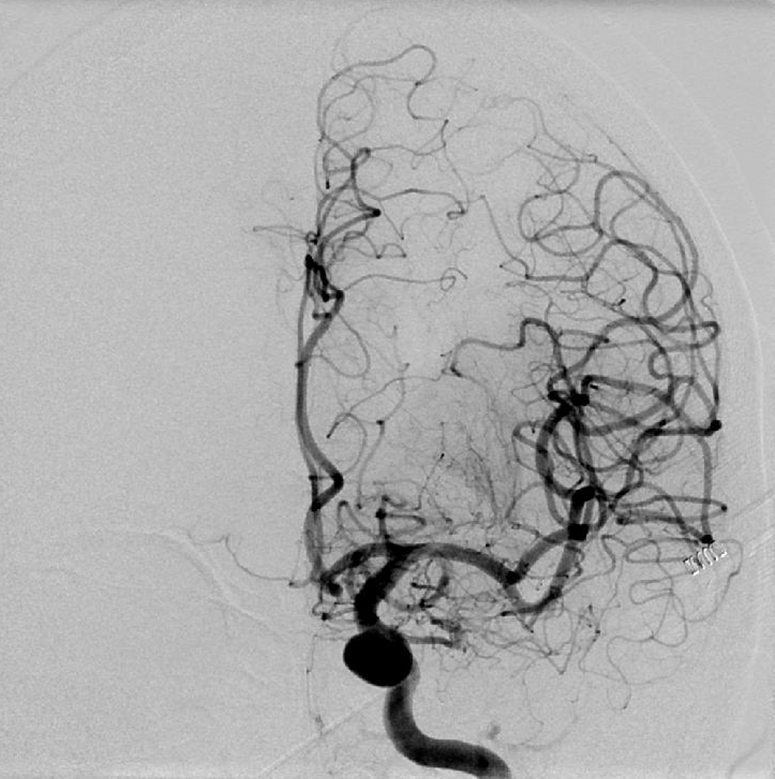
Pretty neat. Now, if this didn’t work, Dan has a TIGERTRIEVER 13 up his sleeve also. We in 2019 New York don’t. Currently available are 3 mm Trevo and 4 mm Solitaire, 3D revascularization device — hmm… Probably not the right tools for this location
Bottom line is when u need that M3 or M4 re-opened, try aspiration. Companion case here