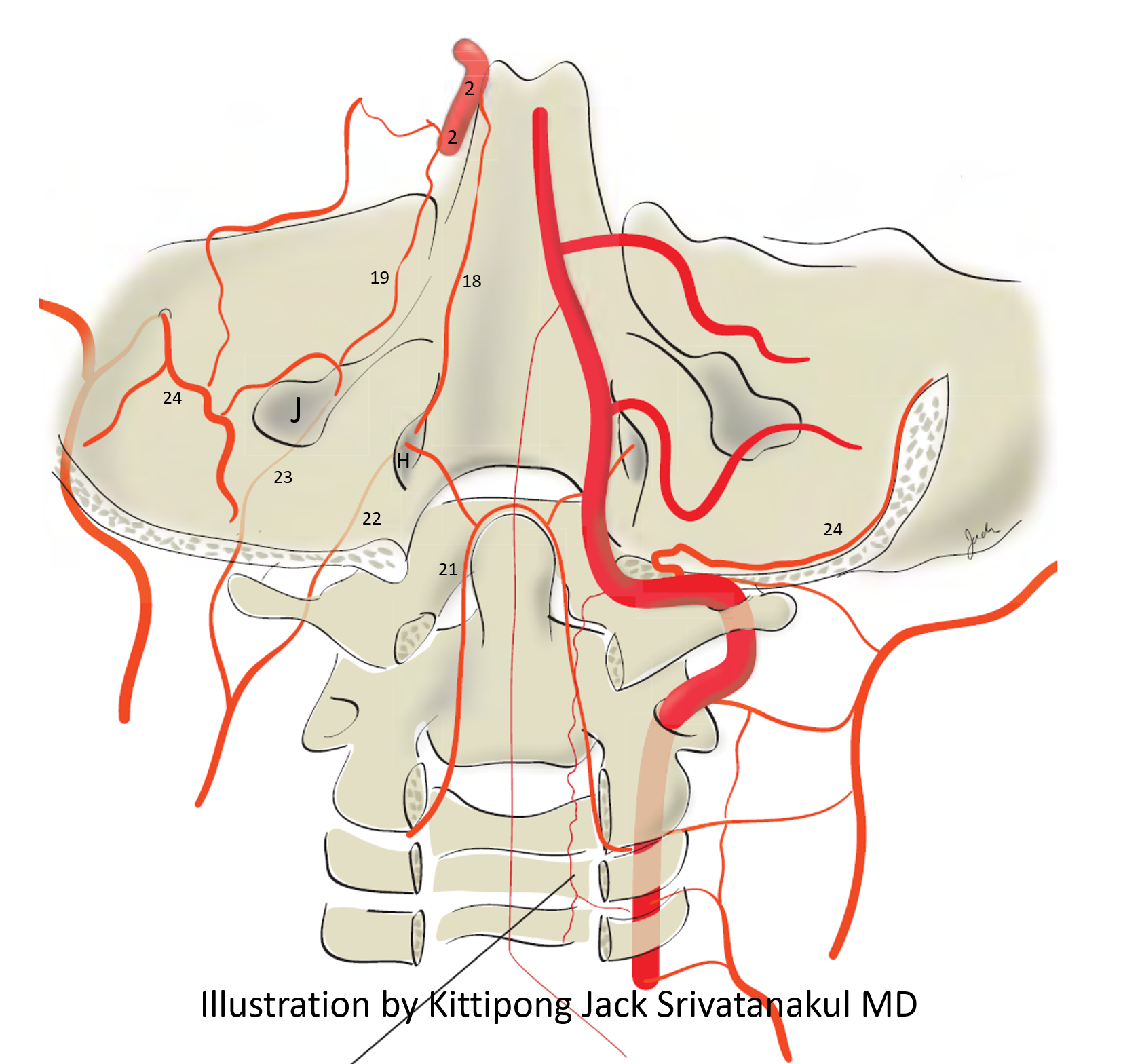
Whats the difference between medial (18) and lateral (19) arcades? Here is the classic — lateral clival arcade (19) connects the MHT (2) to the jugular division (23) of the ascending pharyngeal artery neuromeningeal trunk. Medial Clival Arcade (18) connects MHT (2) to the hypoglossal division (22) of the same. Hypolglossal canal is medial (and superior) to the jugular foramen — hense hypoglossal connection is medial and jugular is lateral. Happy now?
Below is a much better illustration of the same by Kittipong Jack Srivatanakul MD. Numbers are the same as above.
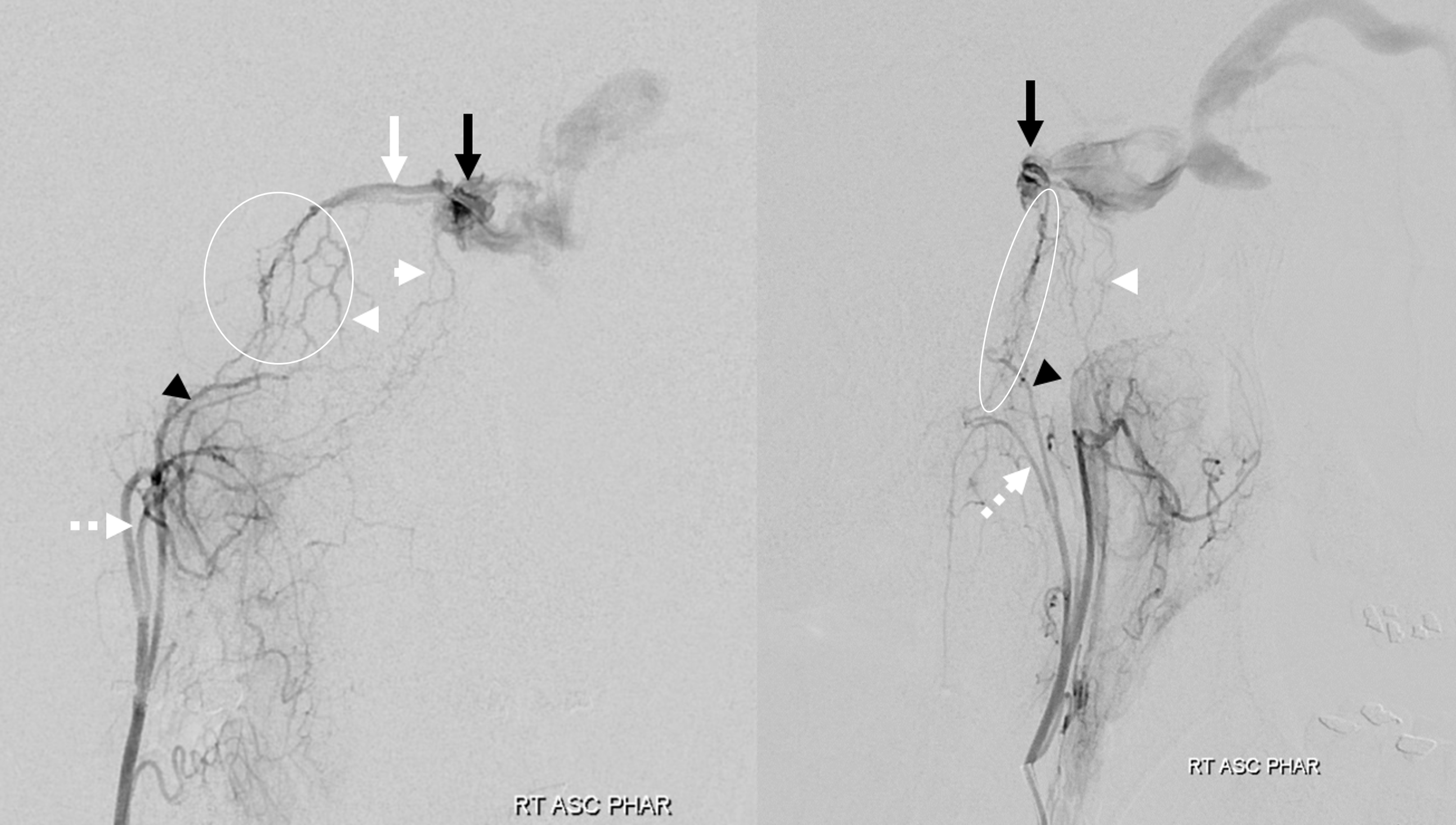
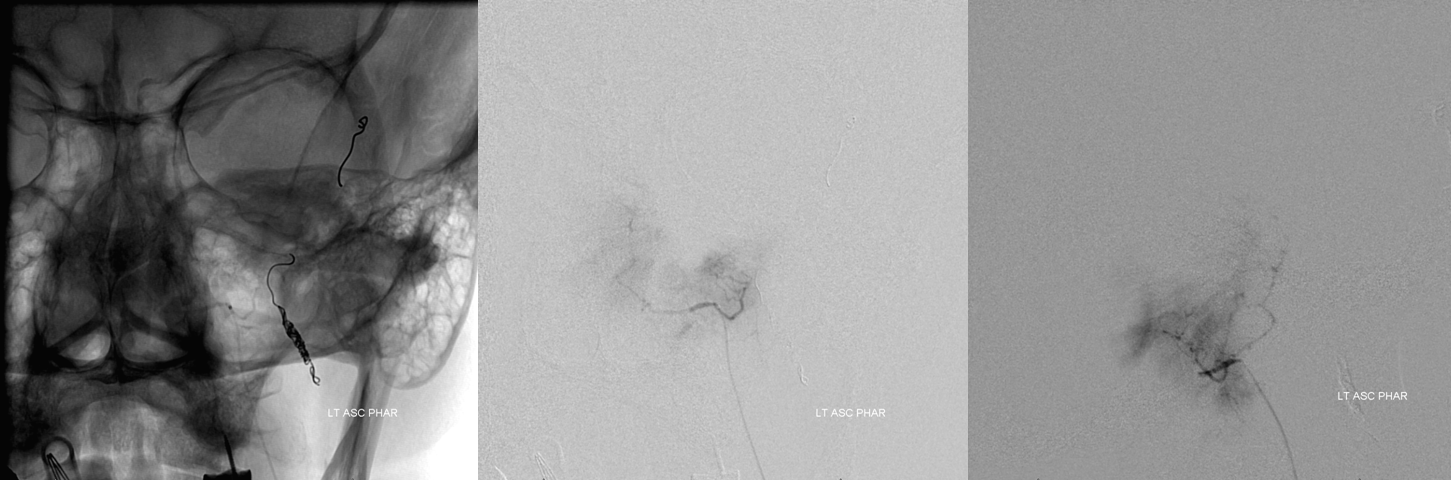
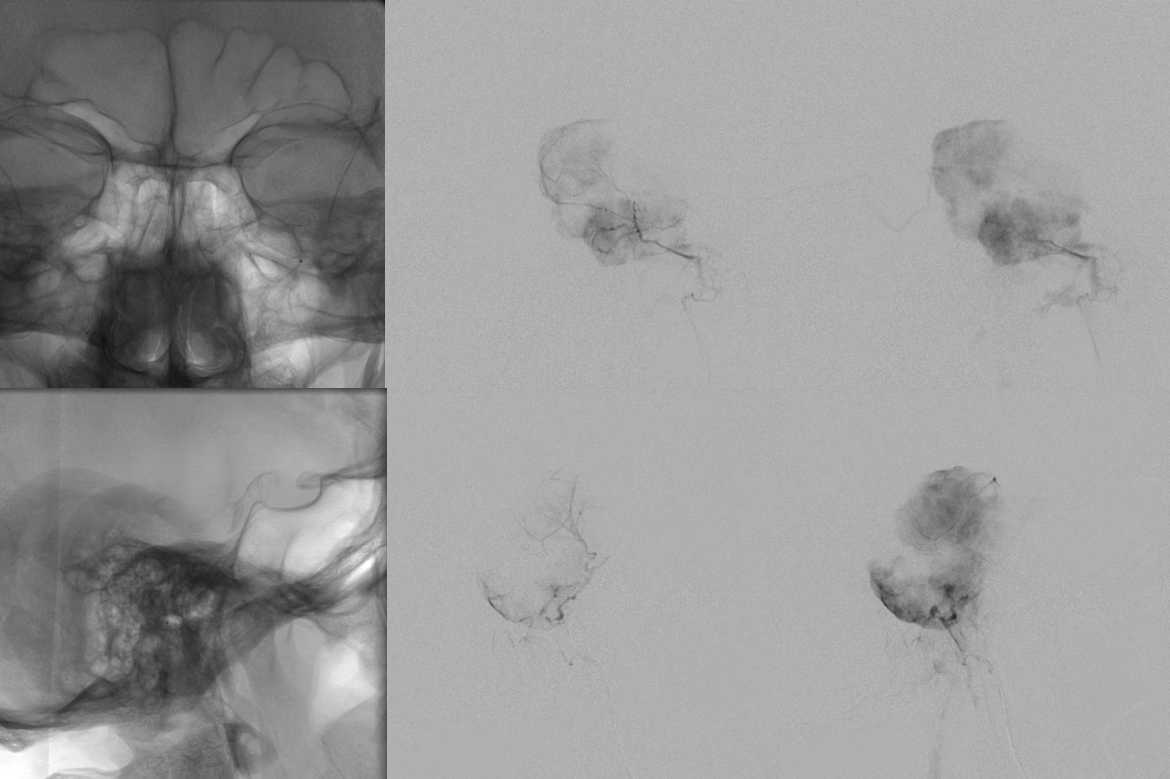
Really, though, half of the lateral arcade is BS. The other half of BS is the medial one… They are all part of the same “spectrum” — a sheet of arteries running along the posterior clivus. The nice picture above are not exactly reality. Reality is below — both arcades supplying a posterior cavernous sinus dural fistula(black arrows). Hypoglossal division = dashed white (lower and more medial) than the jugular (black arrowhead) one. White arrowheads are on transosseous branches of the pharyngeal division. Full case is here.
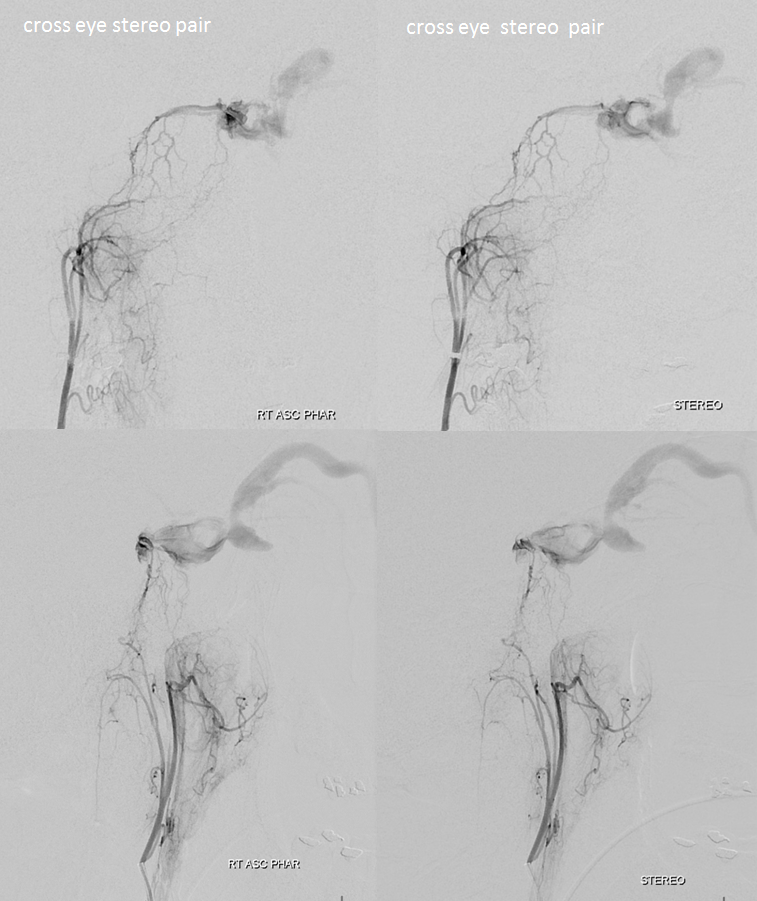
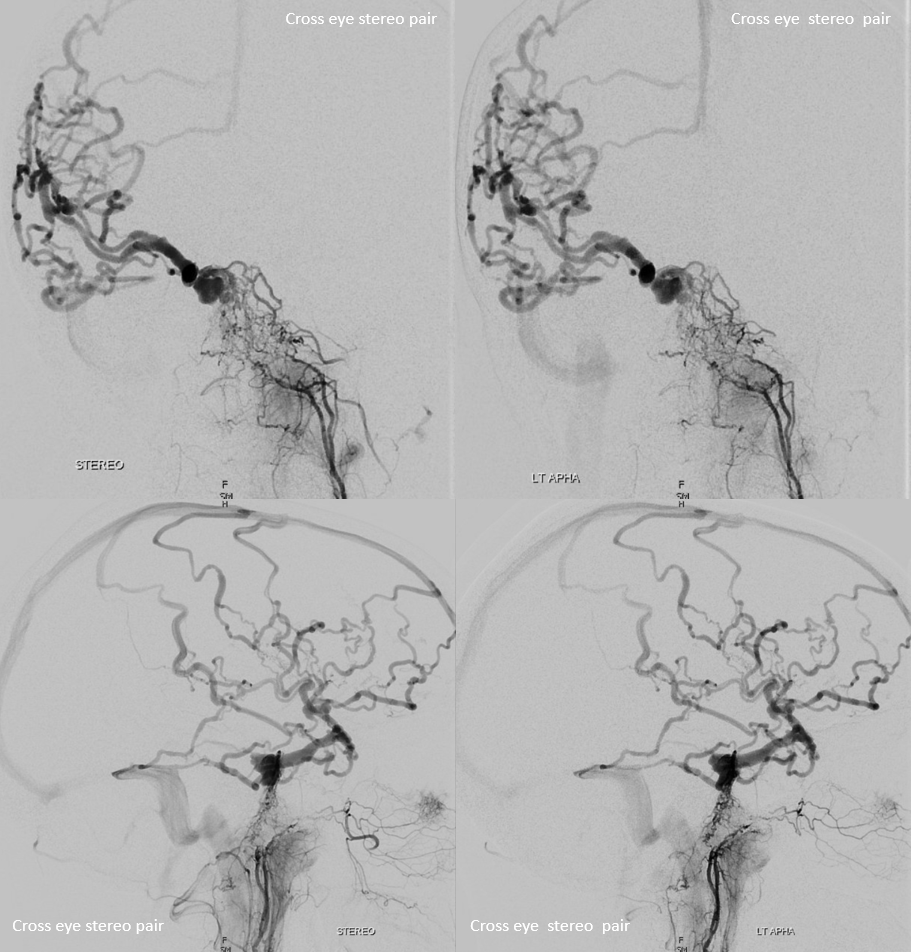
Stereos
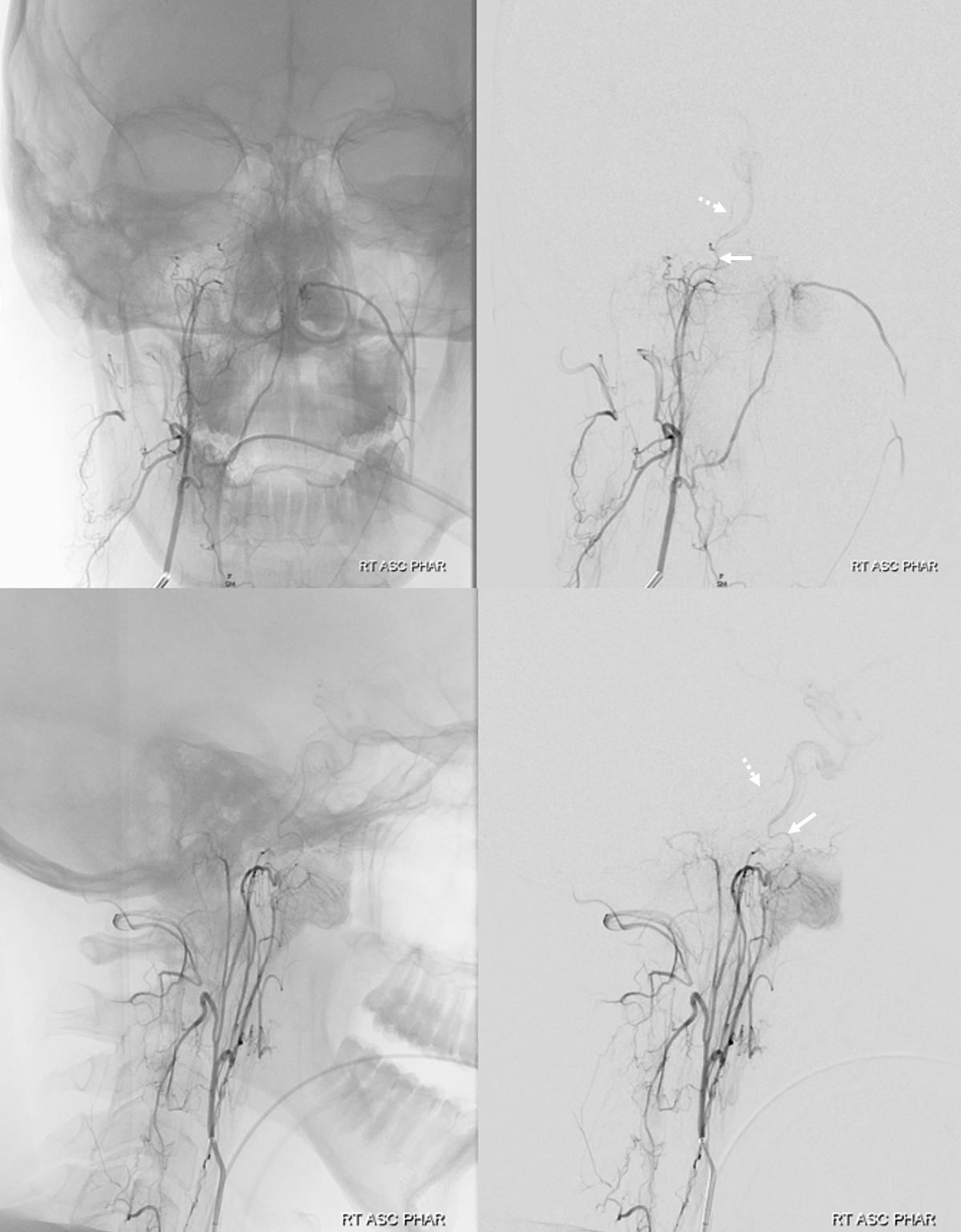
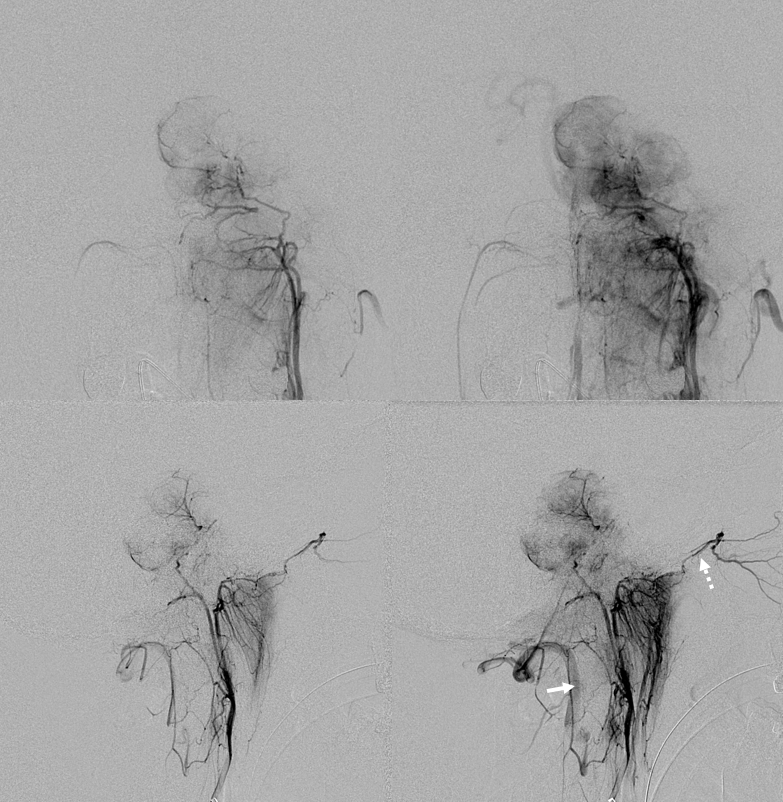
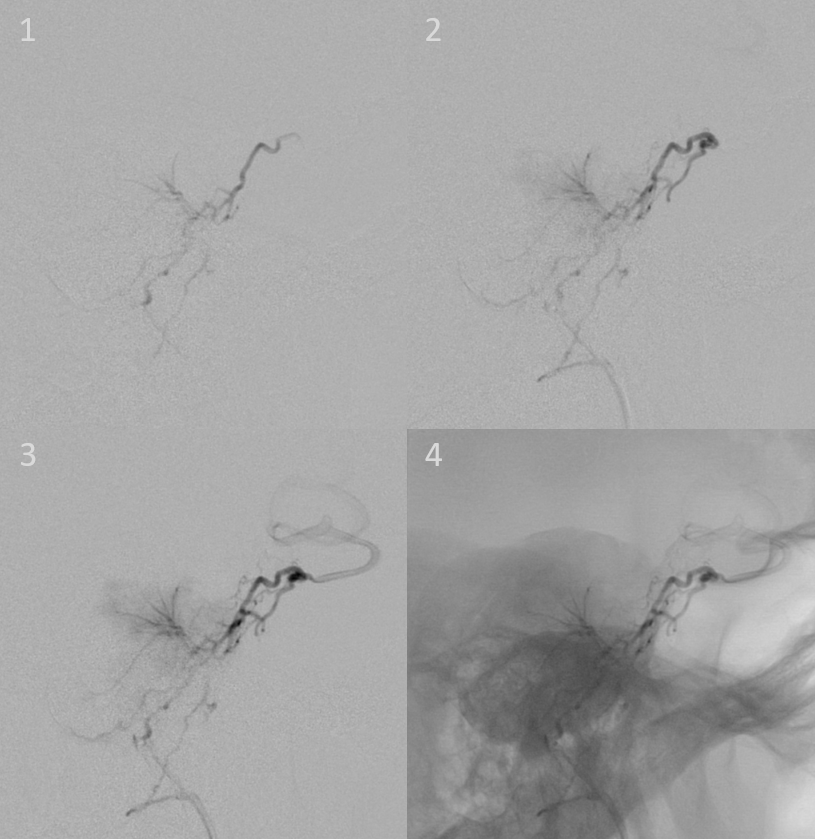
Below is another injection of the ascending pharyngeal where the main connection to the ICA is NOT via the neuromeningeal trunk (and hense NOT via lateral or medial clival arcade). It is via the superior pharyngeal branch connection with the vidian artery (white arrows). A very small (but equally treacherous) lateral clival arcade branch (dashed arrows) is seen as well
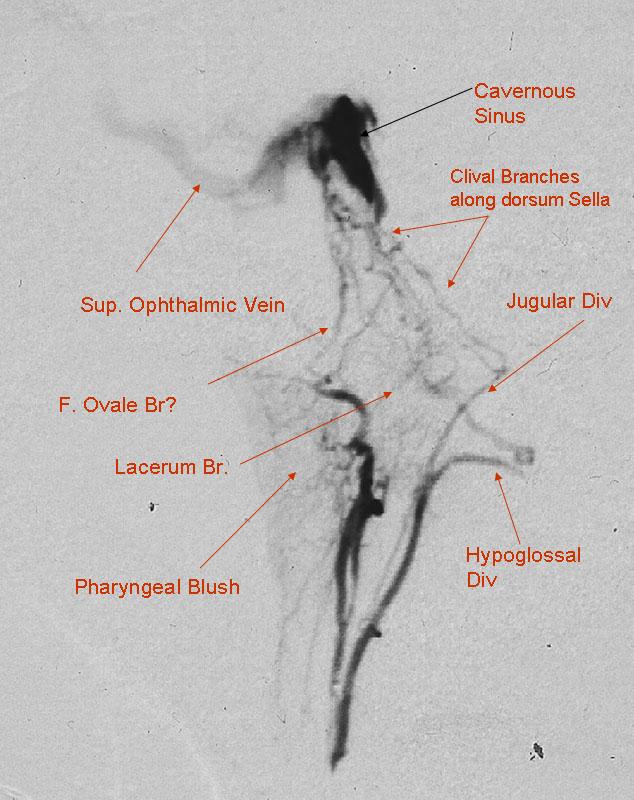
Another old example — note circular analog detector and “backwards” orientation of the image. The anatomy is the same though… and maybe even better seen in this very high photon density image…
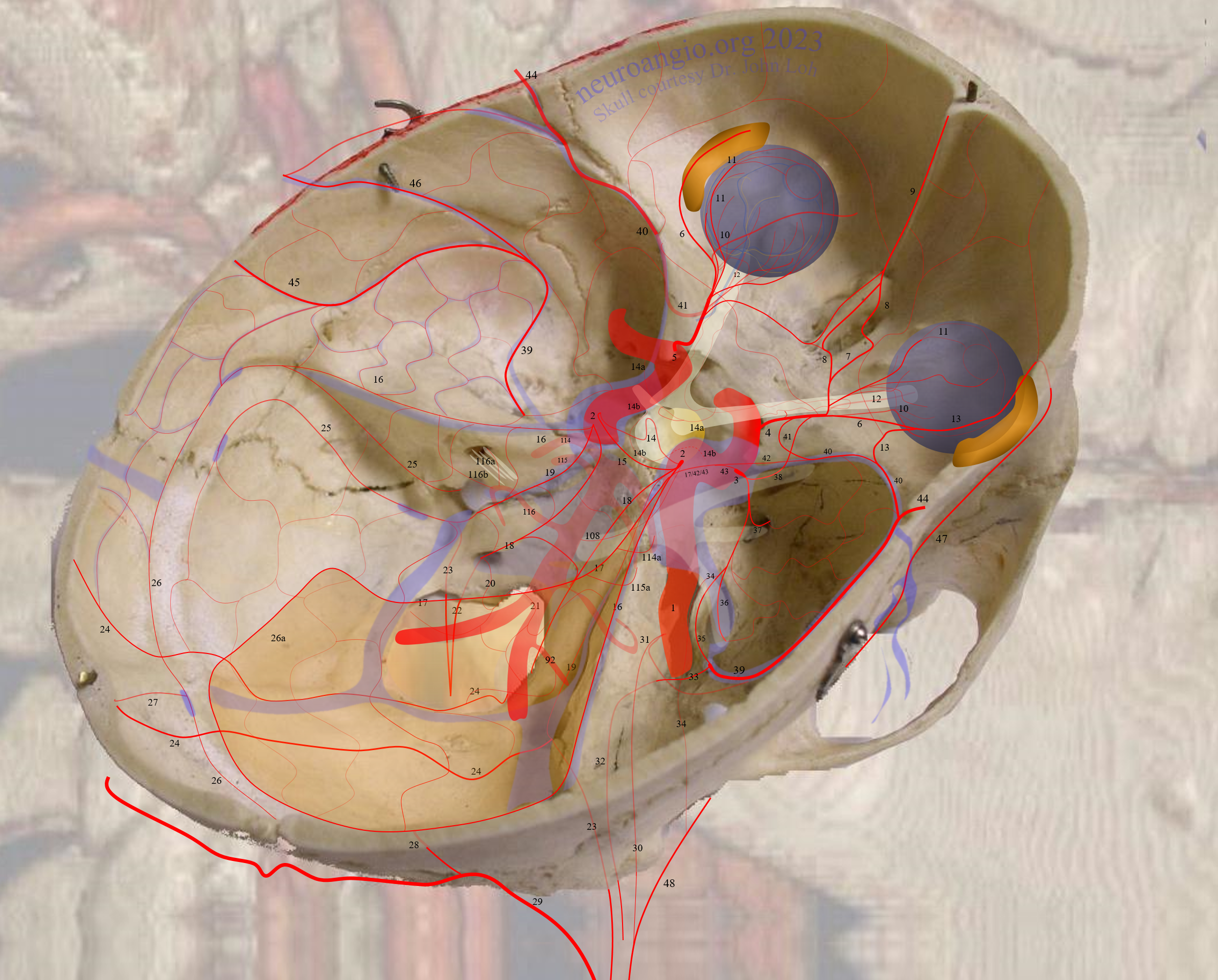
Another older image (see Ascending Pharyngeal Artery Page) showing the lateral clival arcade (orange) among many other things
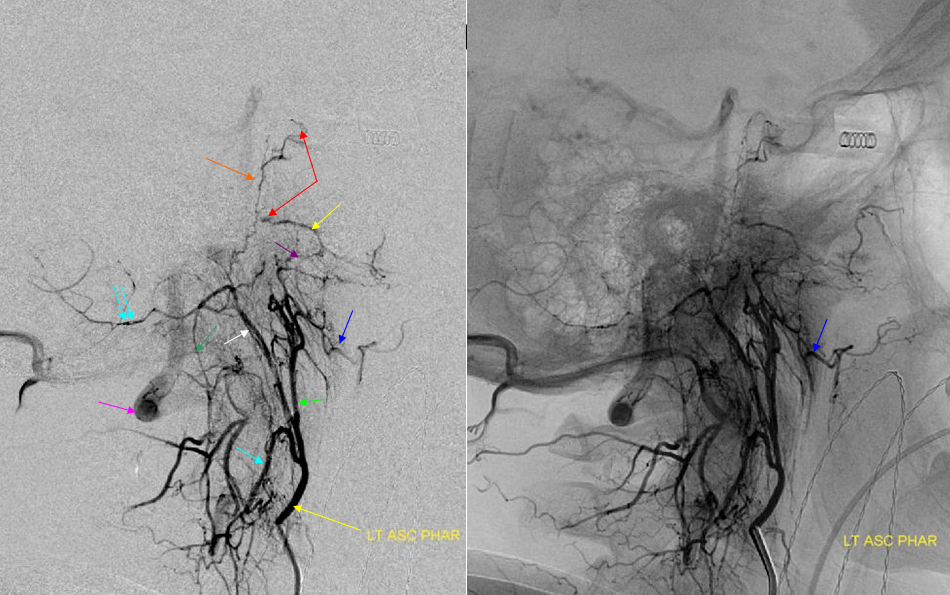
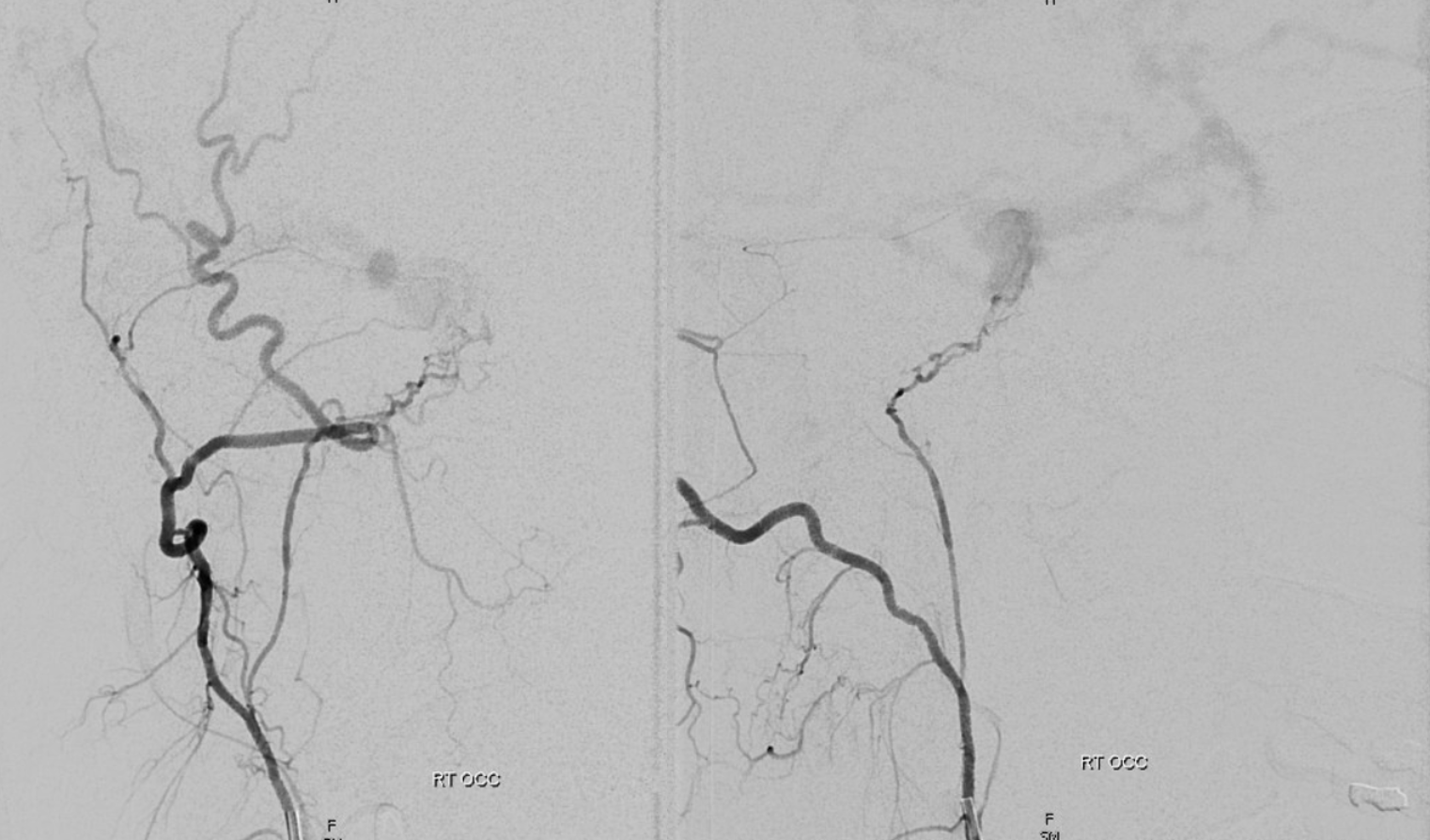
A fantastic case of dural fistula (To See The World In A Grain of Sand Case) — image below is of isolated jugular division origin from occipital artery supplying a cavernous fistula
In the same case, a sheet of transosseos branches of the LEFT pharyngeal division is also seen — again, no single branch here — its a spectrum.
Axial MIP movie — see contributions from both arcades
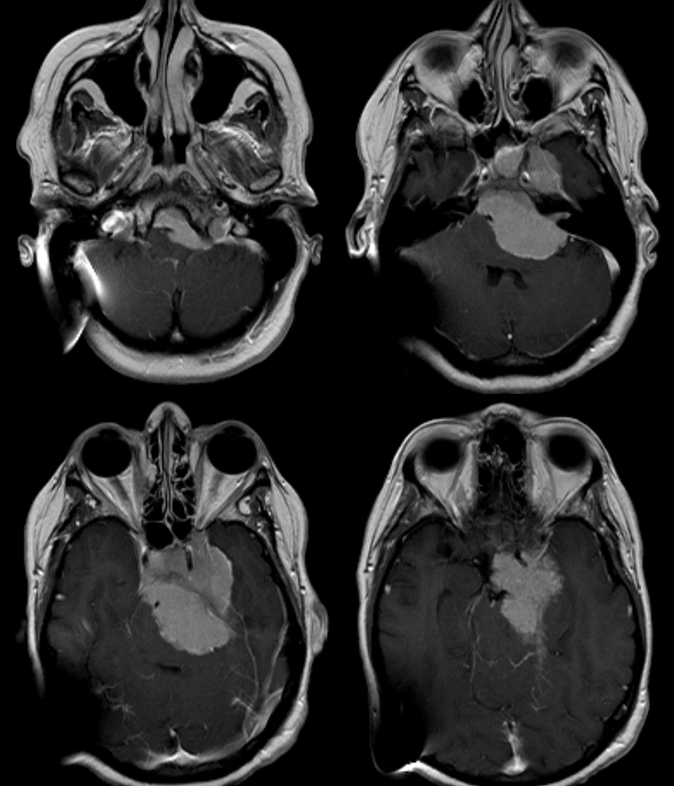
Petroclival Meningioma Embolization
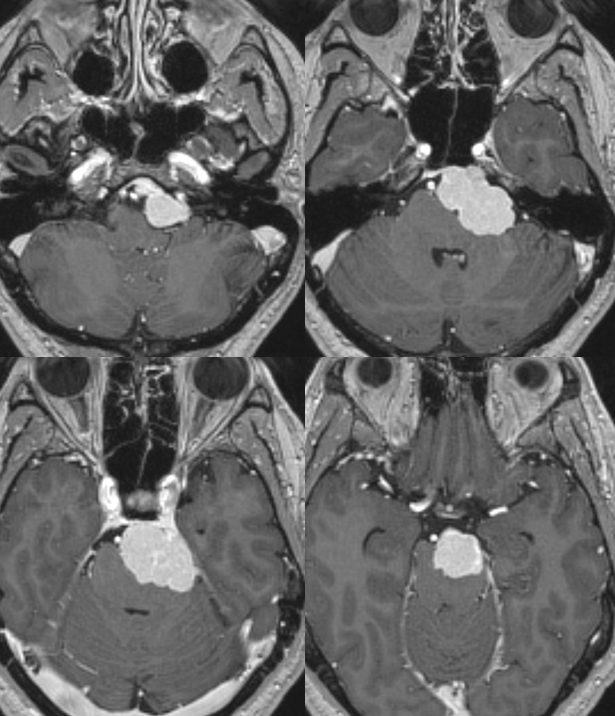
One setting where clivus supply comes up consistently. Meningiomas along the clivus will derive supply from multipel sources. Embo can be quite complex. See case 1, 2, 3, 4 for example. In terms of the arcades, by definition, an arcade connects things. Jugular and hypoglossal divisions with MHT in this case. So, tumors of clivus area will derive supply from either division, MHT, or both — the extent being determined by developmental and tumor growth factors. Those cases 1, 2, 3, 4 are really quite useful. For example, this tumor:
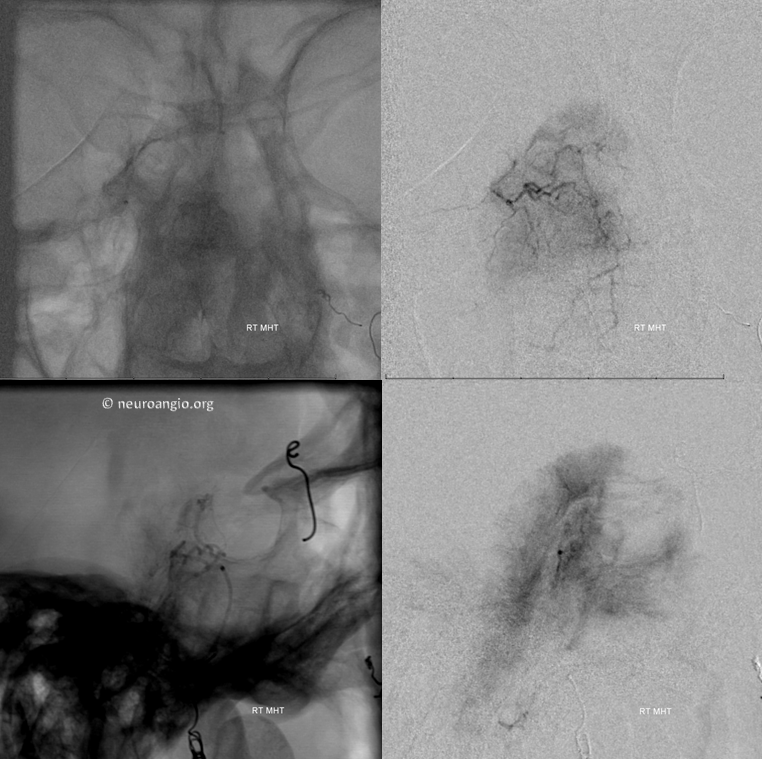
Has this supply from the MHT (subselective catheterization)

This supply from right AP

This from left AP
Intratumoral Anastomoses — key determinant of embolization strategy and efficacy
The above case shows poor intratumoral anastomoses — each compartment is supplied by its own network. Thus, it is difficult or impossible to embolize more tumor from any compartment than its intrinsic supply.
Other times, like in the case below (full case is here), there are good macroscopic intratumoral anastomoses. This allows one to embolize substantially more more tumor from a given catheter position by pushing the embolic material (particles, liquids) into other comparments via these anastomoses. In the case below, excellent MHT/lateral arcade anastomoses allowed for embolization of the whole tumor from neuromeningeal trunk position, using Contour PVA particles. These aspherical particles are particularly good for preop embolizations. They are less likely to cause necrosis (of tumor and vasa nervosum…) than spherical types. Thus, our experience with these from neuromeningeal trunk and other eloquent positions has been excellent. Spherical particles and liquid embolics are a completely different matter.
MHT supply
Ascending Pharyngeal
Jugular division micro
Progressive embo — see deposition of particles in the upper aspect of tumore supplied by MHT?
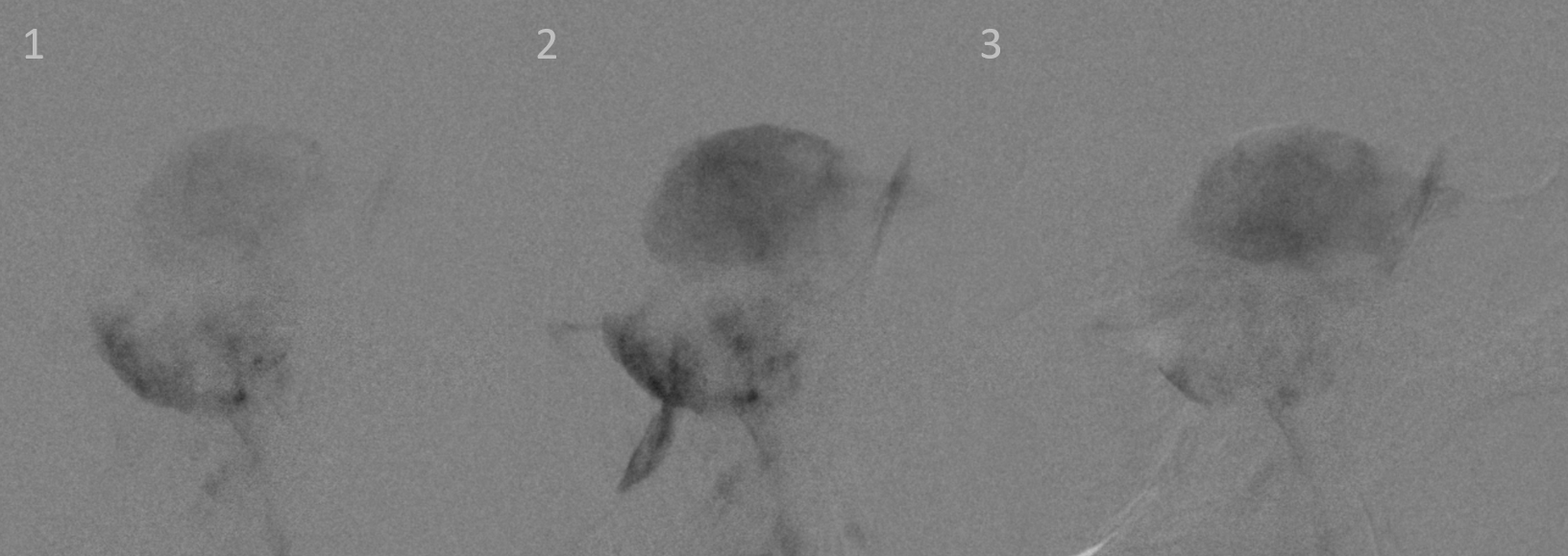
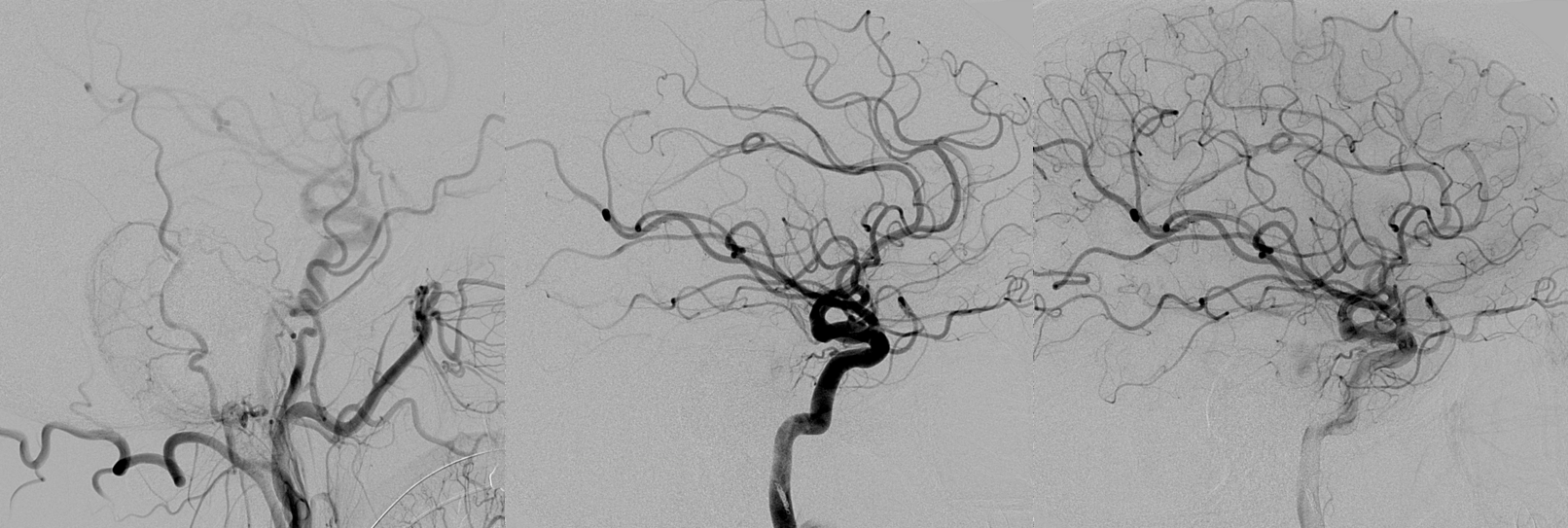
Contrast (not particles) injection after some particle embo shows the robust clival arcade connecting to the ICA
Now more particle embo can be done carefully, pushing the particles to the MHT but not beyond — in effect the clival arcade becomes an extension of the microcatheter, allowing for embolic material to be deposited into the MHT territory
Post embo — all from jugular division position
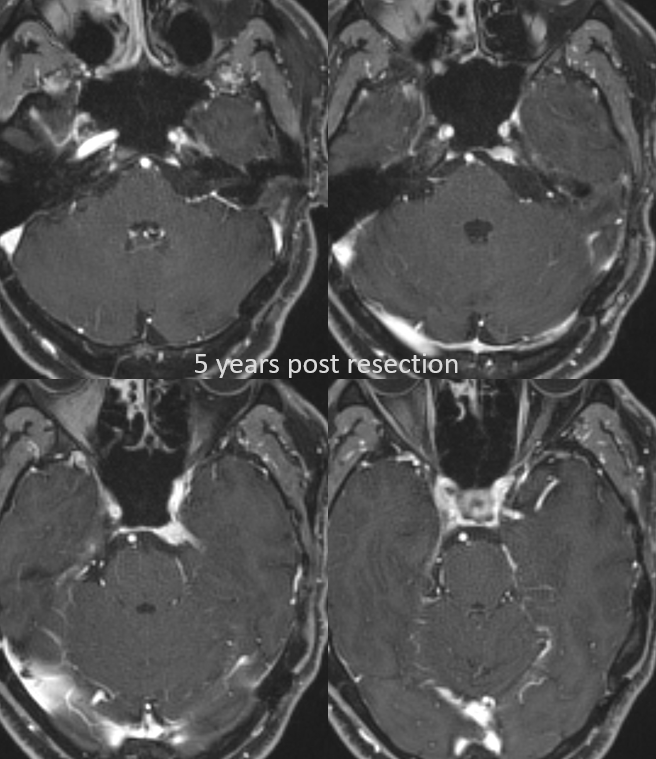
5 years post resection
Views from MHT
As you can see from the case above — again, its an arcade… The typical discussion of clival arcade (including all of the above) is when it is seen from injections of the neuromeningeal trunk. This is just half the story. The same network can be seen by looking at the MHT. But, it goes by a different name — the “descending” or “clival” or “medial clival” and “lateral clival” branches of the MHT are the same arcade. Because vascular anatomy was originally studied using ex-vivo methods, with not much appreciation for anastomoses, flow, and spectrum, the various names reflect study of varnous anatomical regions by different people. For example, the “cavernous branch” of the MMA and the spinosum branch of the ILT are the same thing.
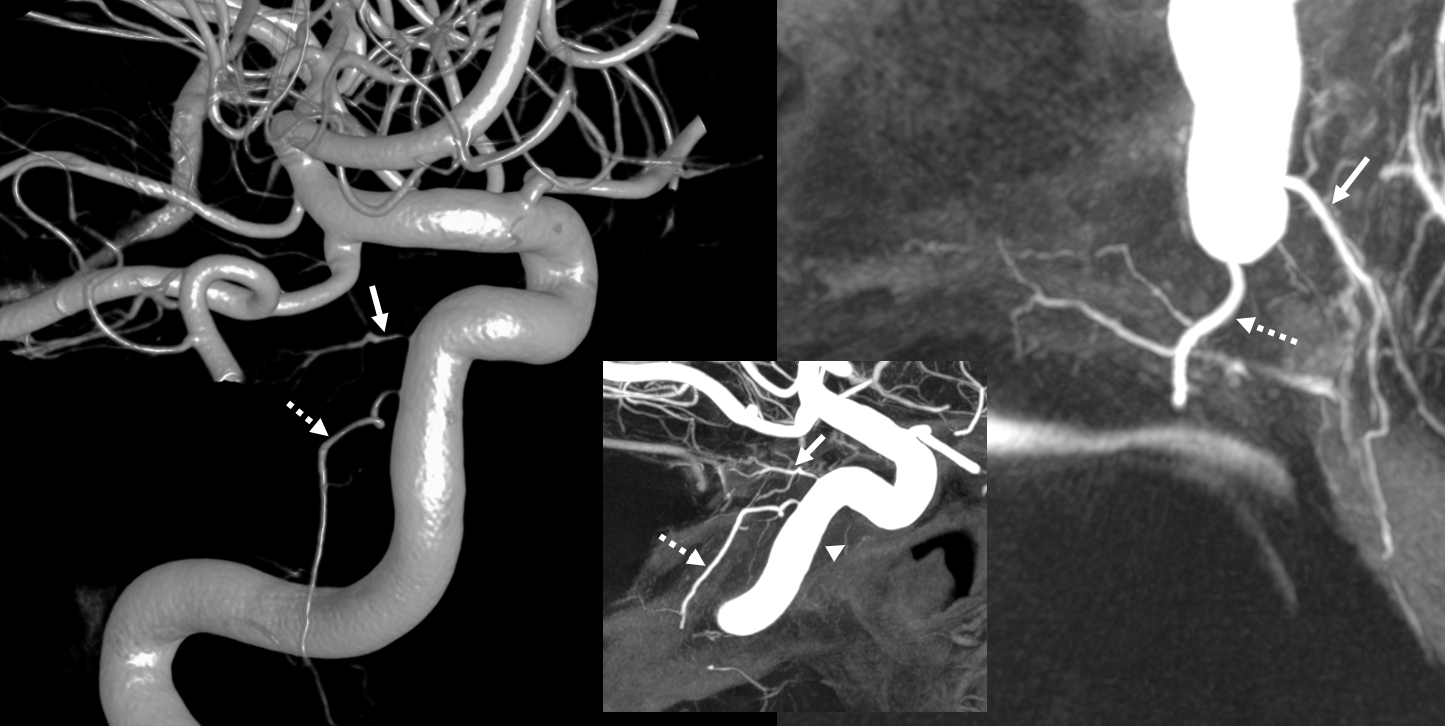
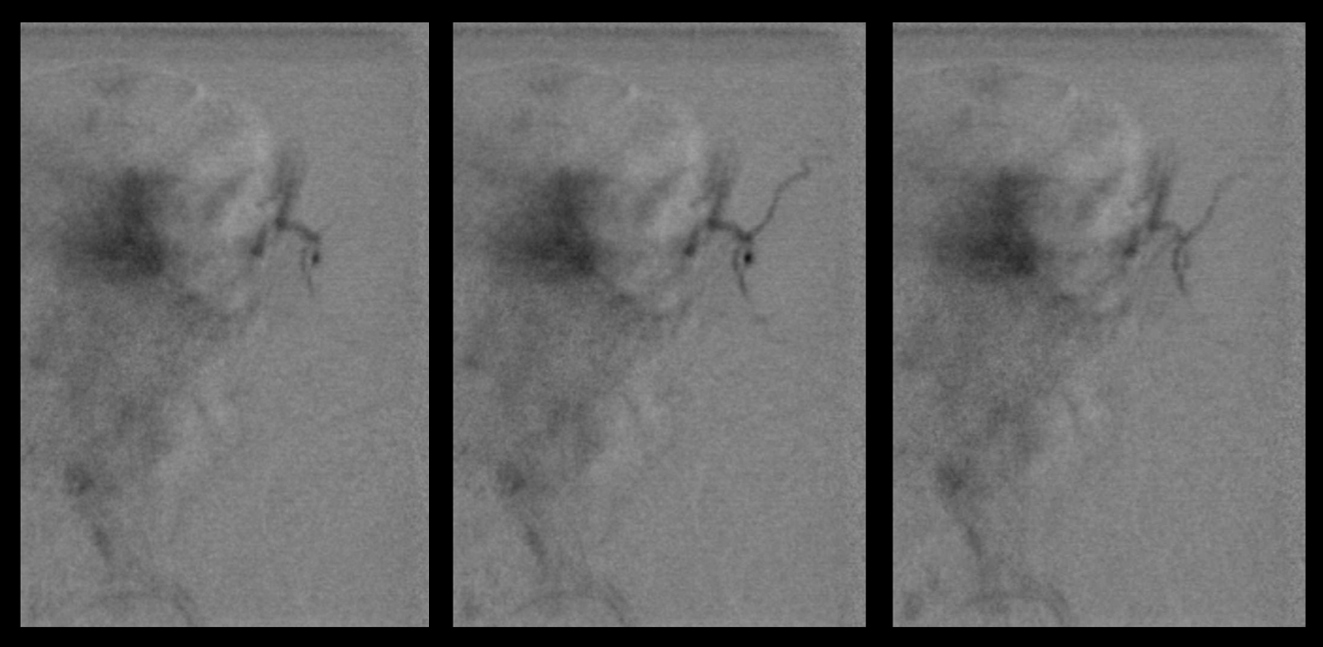
DYNA VR images showing well-developed clival branch (dashed arrows) of the MHT. Note commonly seen separate origins of the clival branch and the inferior hypophyseal (solid arrow)