Case by Peter Kim Nelson, MD
Importance of understanding collaterals is key in this preoperative embolization of petroclival meningioma
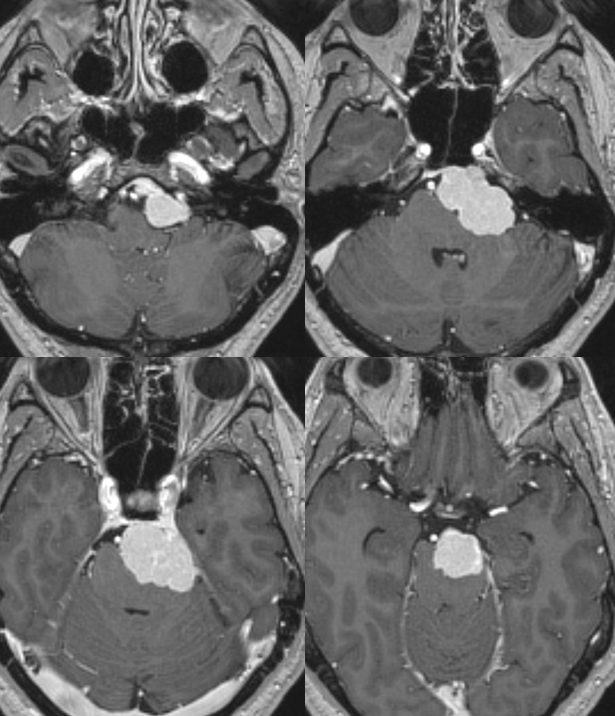
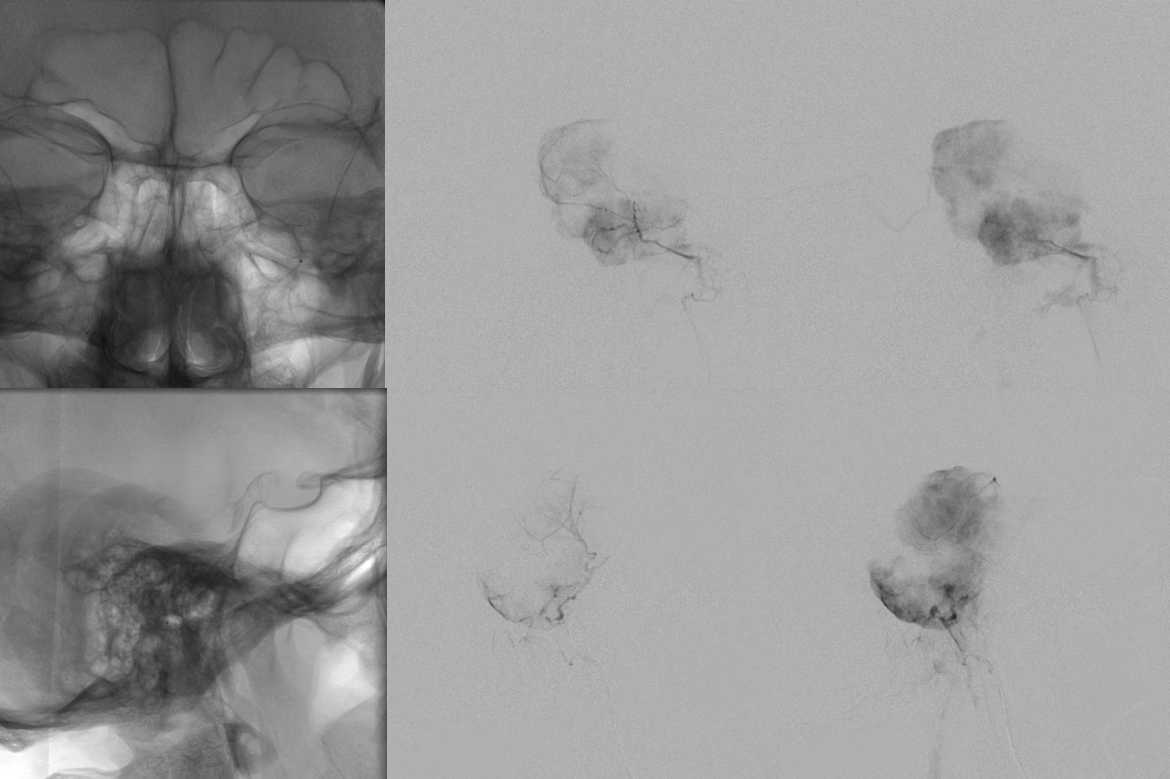
What is the usual arterial supply to this kind of tumor? MHT or ILT from above, MMA or Accessory Meningeal from the side, and Ascending Pharyngeal from below. Of course, everything is in balance. See other examples on the Case Archives page btw.
Here we have pretty robust MHT supply. Note two separate MHT pedicles. More on MHT page on that.
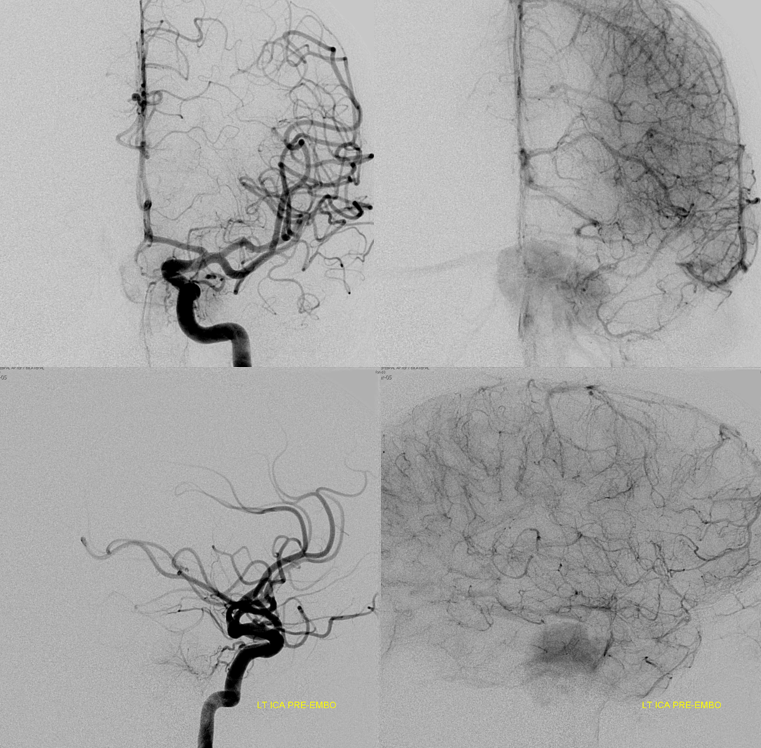
Global ECA injection is not very impressive
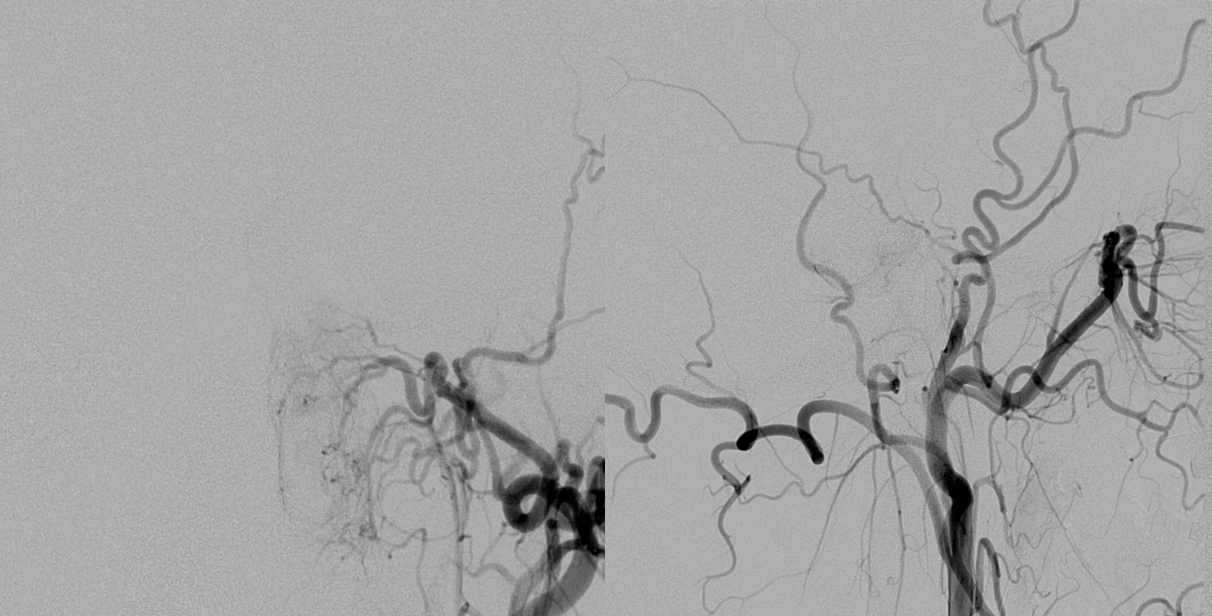
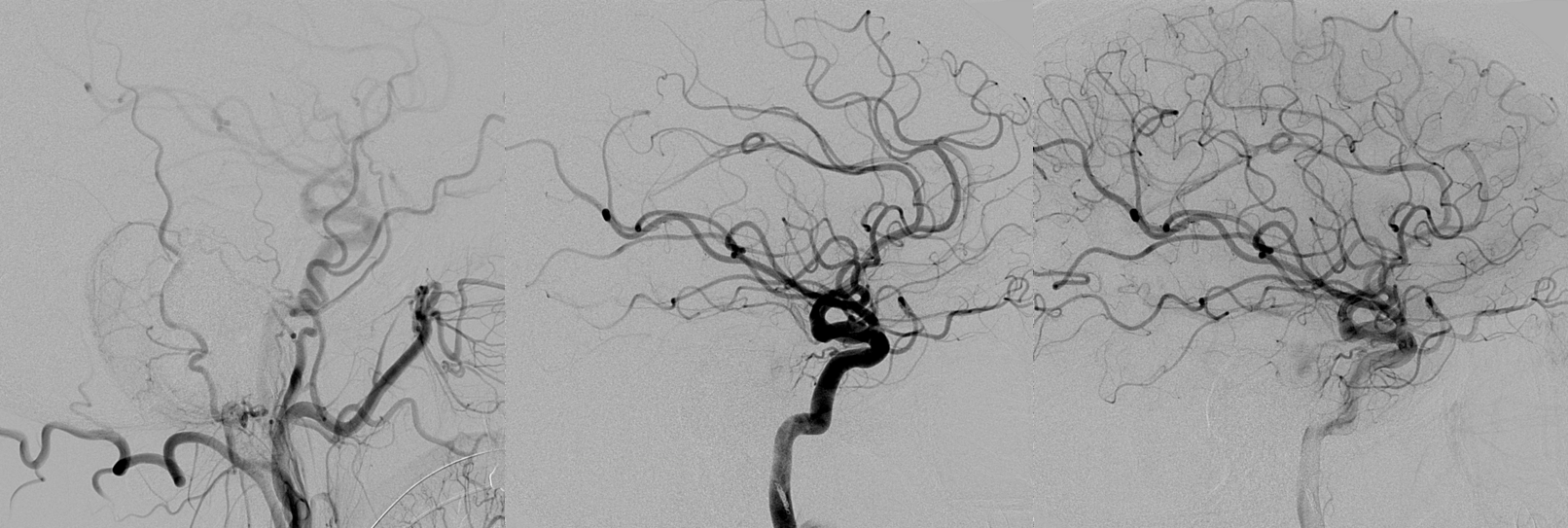
However, experience tells us to look better. Subselective Ascending Pharyngeal injection with “wedge position” of the vert catheter. Big difference huh… Note anatomoses with the vert (arrow) via the musculospinal branch and pterygovaginal artery (dashed arrow) via the pharyngeal division
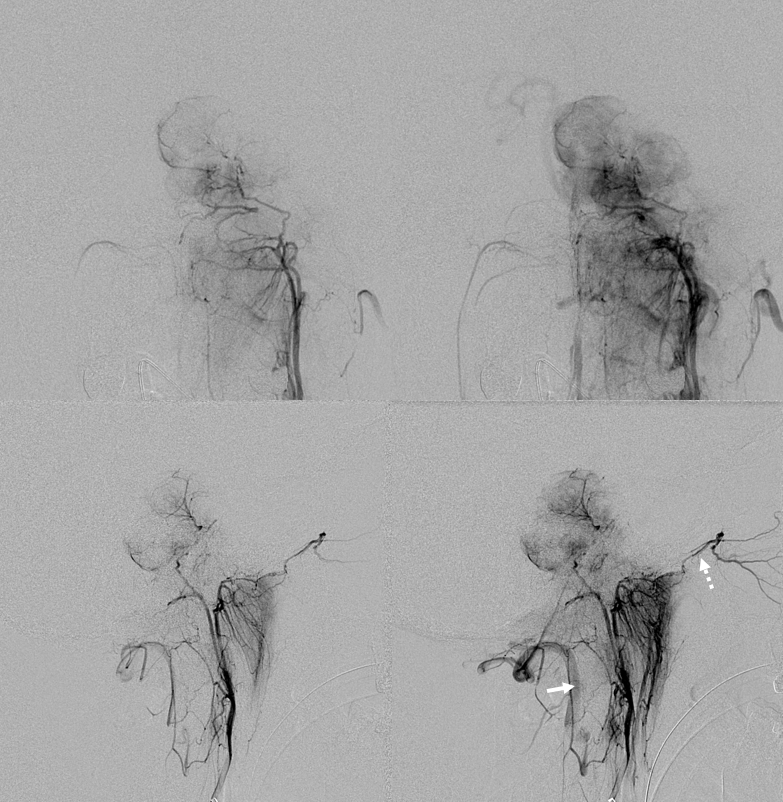
Microcatheter position in the jugular division shows extent of contribution to tumor supply
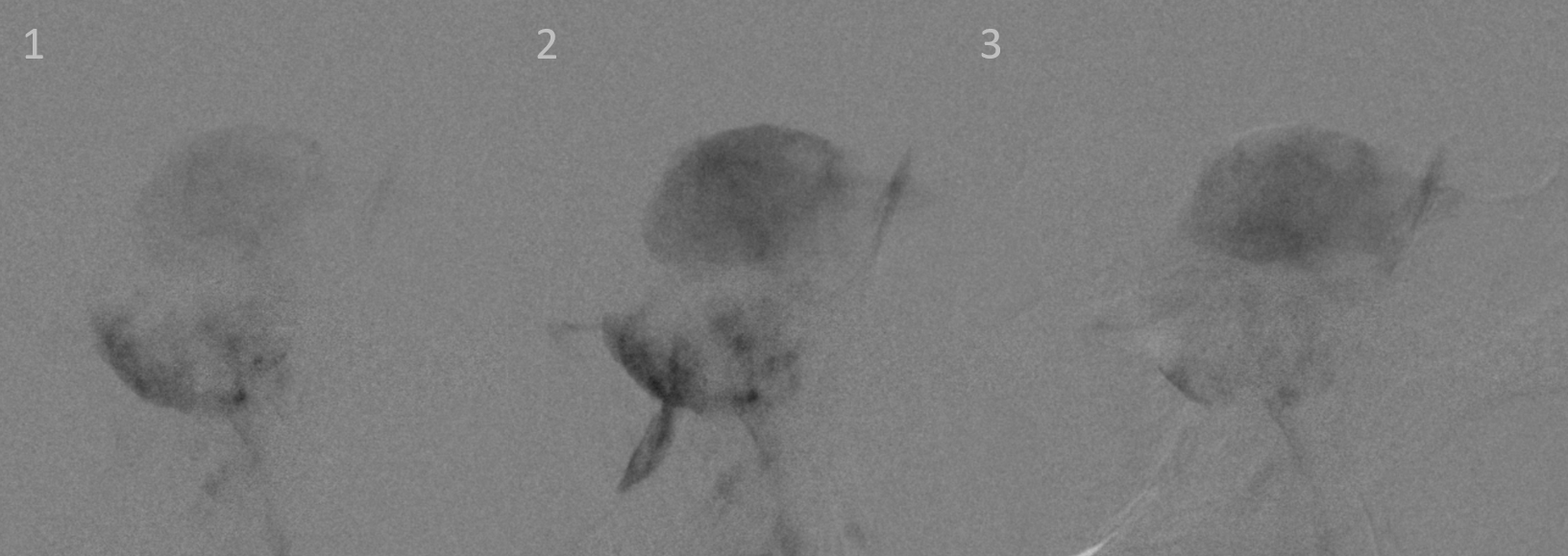
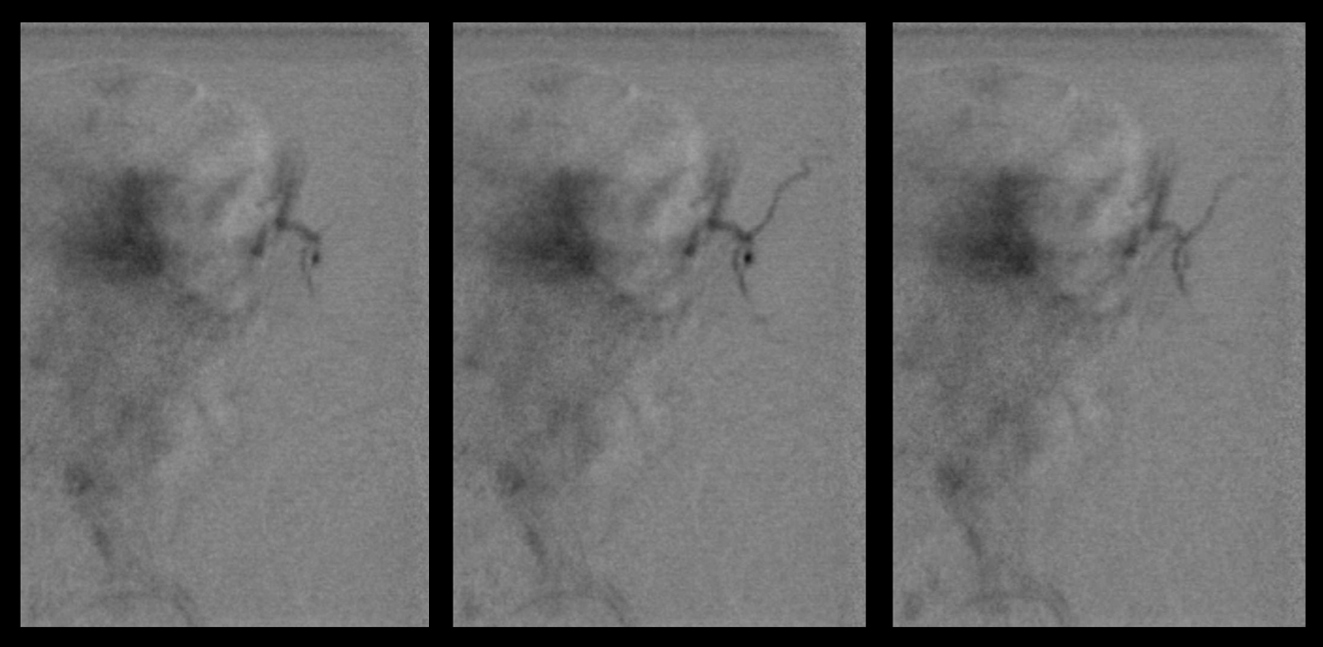
Sequential images of Contour 45-150 micrometer particle embo. Its generally ok to do these particular particles in the jugular or hypoglossal division in our experience. Also note progressive shift of particle deposition from lower part of the tumor in frame 1 to upper part in frame 3. Why?
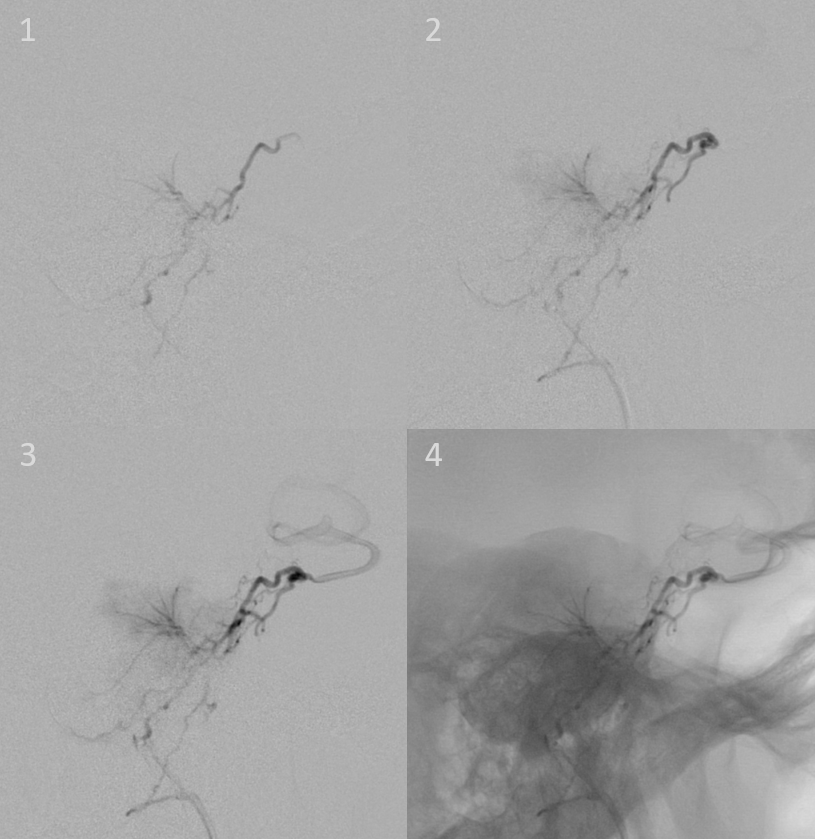
Here is why. Contrast injection from same position as above, after some particle embo. Robust anastomoses are present with the MHT via the lateral clival arcade. This allows contrast filling of the upper part of the tumor supplied by the MHT, eventually opacifying the ICA (frames 3 and 4)
Not bad huh. There are two ways to respond to this information. One is to say “oh no time to stop”. The other is to say “excellent, lets use this anastomosis to embolize the rest of tumor without having to catheterize the MHT“. The latter is the better approach. Particle will not go where contrast does not. Thats just how it is. Careful injection to the level of the MHT, without too much pressure, will deliver the embolic material where you want it, and not where you dont. See images below.
Final post. Minimal amount of residual via the MHT
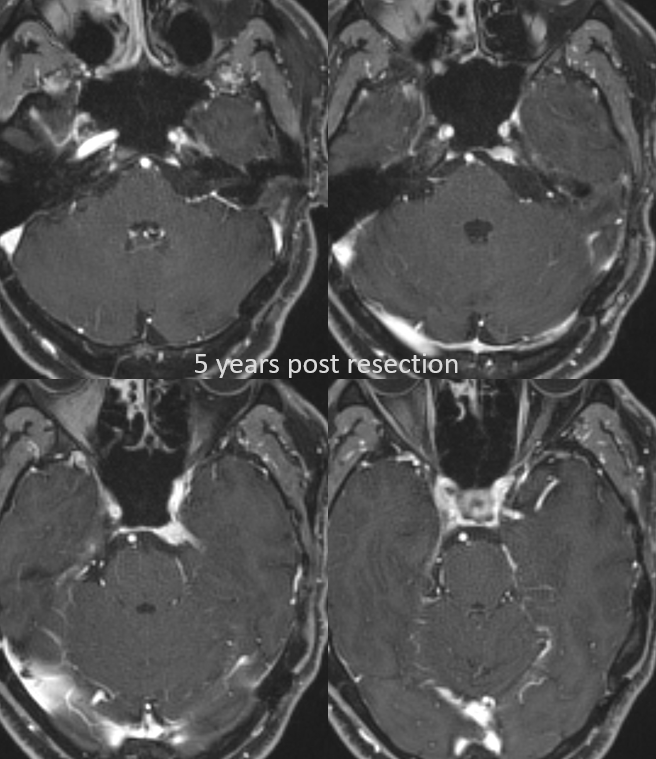
5 year post resection follow up. Excellent result. The residual in back of cavernous sinus is quite minimal and is being watched.