
Page created in conjunction with Dr. Ronit Agid and Frank Silver, University of Toronto
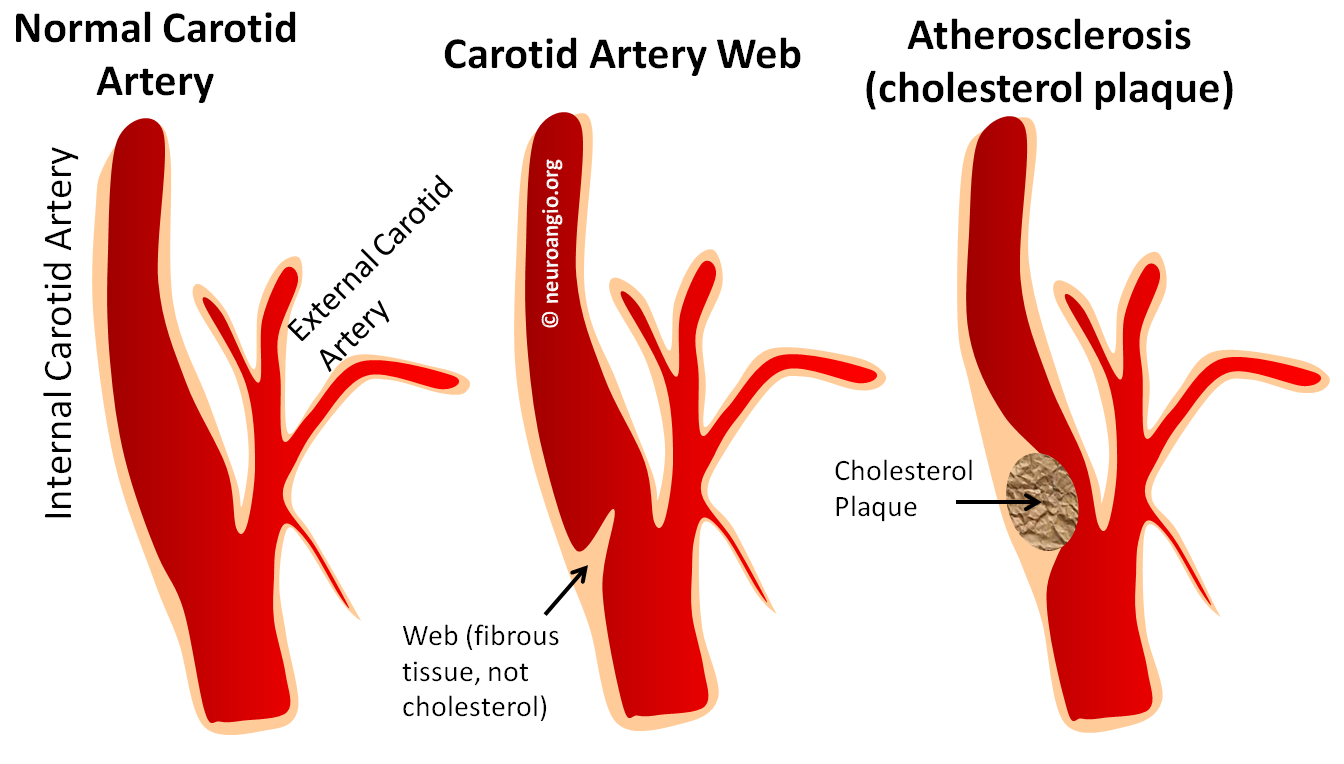
Carotid web is a thin, shelf-like protrusion of connective tissue most typically located on the dorsal wall of the carotid bulb. It is however not atheromatous in nature. Histologic evidence, which is not abundant but consistent, points towards focal connective tissue hyperproliferation. It is felt to be a variant of Fibromuscular Dysplasia. The shelf-like protrusion, especially when prominent, can produce flow alteration and particularly flow stasis between the lesion and dorsal carotid wall. As such, it is one cause of artery-to-artery embolic stroke due to slow flow behind the web and thrombus formation with subsequent embolization. We have not yet seen a proven carotid web large enough to cause significant stenosis.
Literature consists mostly of individual cases and small series Treatments vary. Asymptomatic, incidentally discovered webs are often managed with low dose aspirin or another antiplatelet. Those presenting with emboli have been treated by medical management, using antiplatelets or anticoagulation, endarterectomy, and stenting. The number of cases is small and there is no standard of care. The mechanism of thrombus formation favors antcoagulation rather than antiplatelt treatment. However this is not how most atheromatous carotid lesions are managed and the web remains under-recognized. Furthermore, many patients are relatively young and life-long anticoagulation is not a popular choice in many cases. Most groups familiar with the disease prefer carotid stenting to endarterectomy though, again, there is a paucity of data as to whether this or endarterectomy is best. Personally i think they both work just fine when appropriate technical expertise exists.
Below are some examples of webs
Case 1: This person had the web, initially misdiagnosed as a disssection, followed by every imaging modality available. It is a nice illustration of what a web looks like on Ultrasound, CTA, MRA (contrast and noncontrast) and finally catheter angiography.
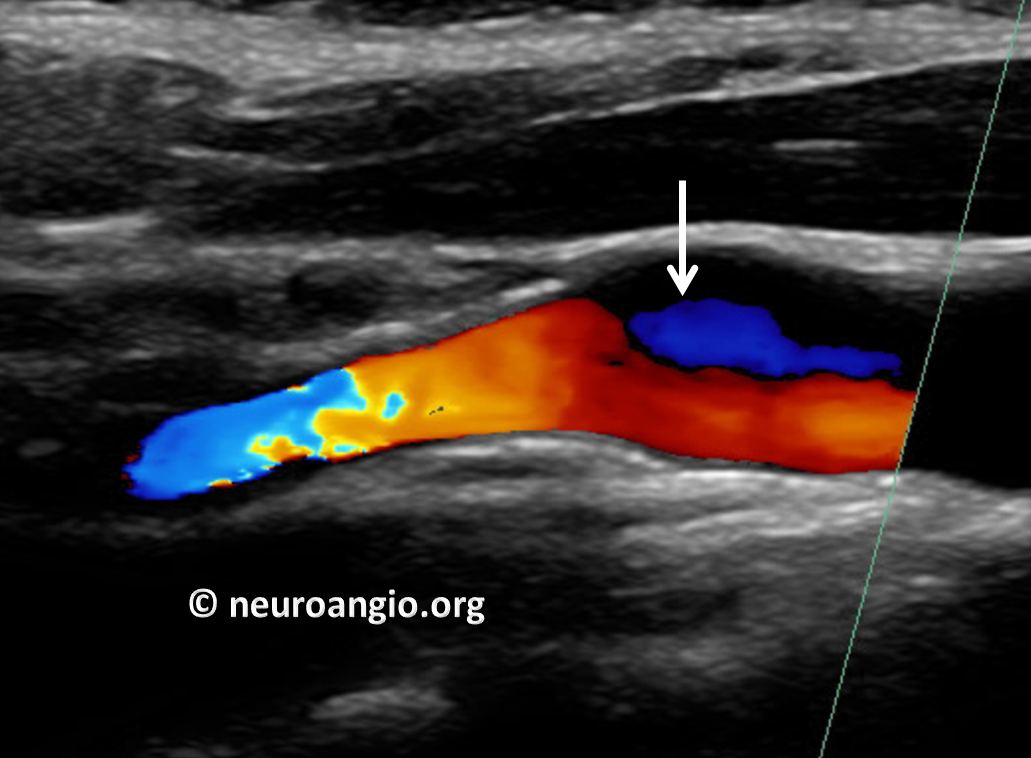
First evaluated by Carotid Duplex. Because it relies heavily on flow, the web can be difficult to differentiate from cholesterol plaque on duplex. A flow change is seen (white arrow)
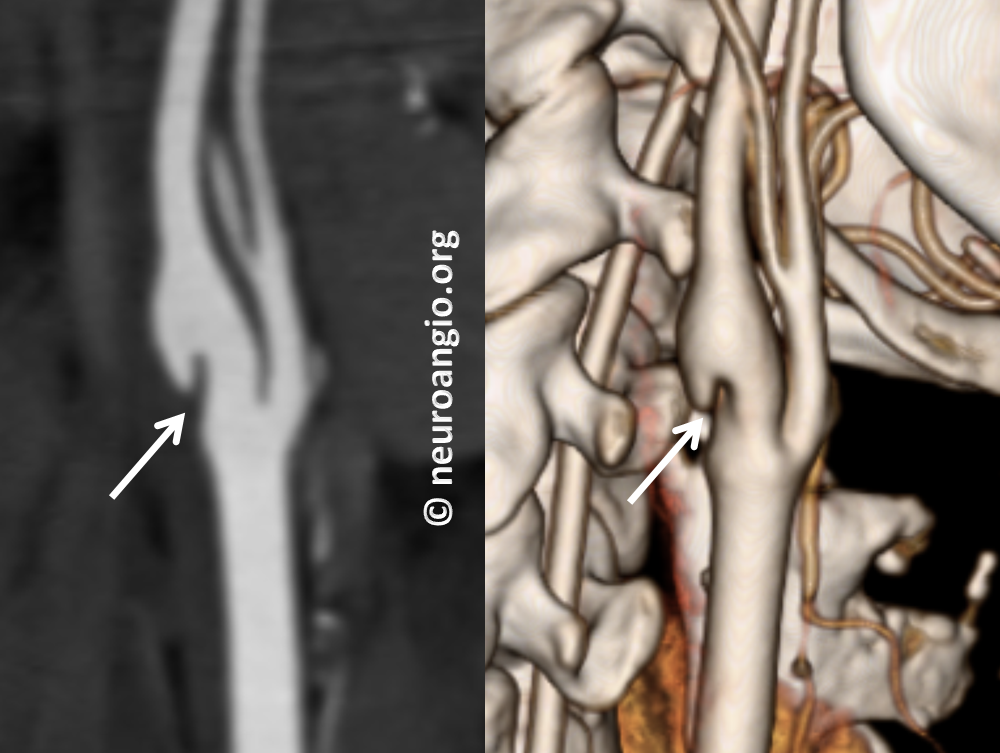
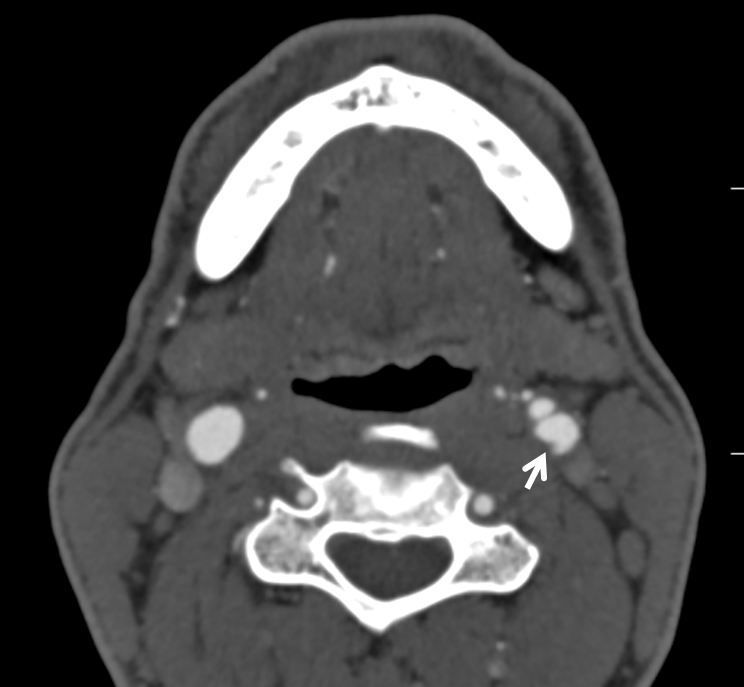
Then came CT Angiography (CTA), where the web is beautifully seen. It is an excellent way to look at the Web, but requires administration of contrast and has some radiation cost
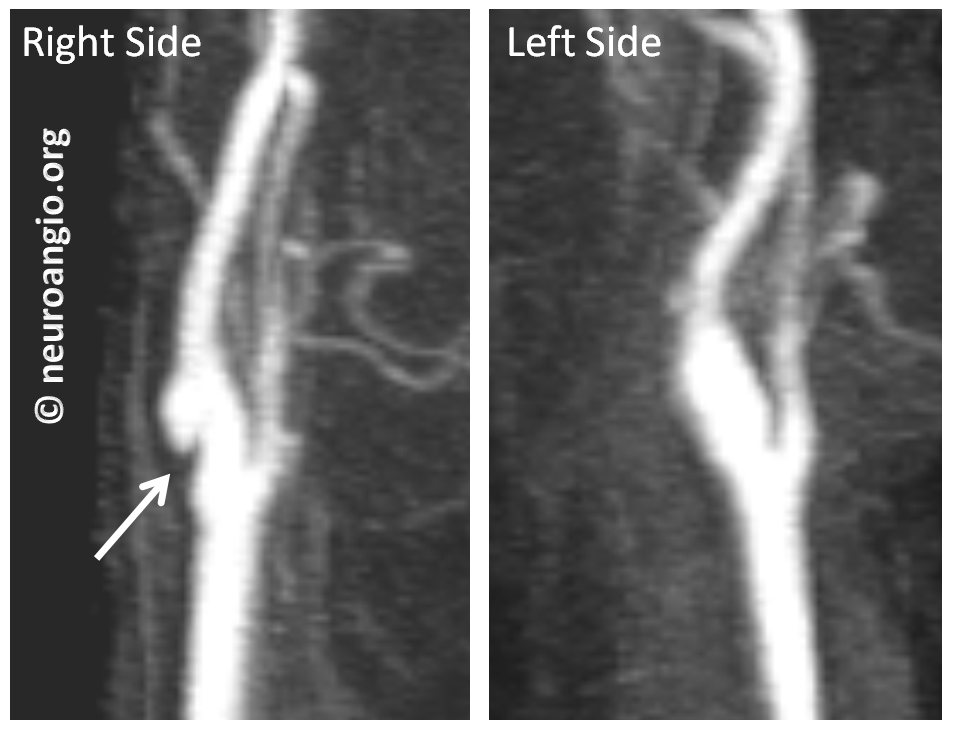
Noncontrast Time of Flight (TOF) MRA was done next; Time of Flight technique relies on flow-related enhancement. Because flow in the back of the web is slow, it is not well seen on MRA. So, it is not very helpful differentiating web from atheromatous disease here
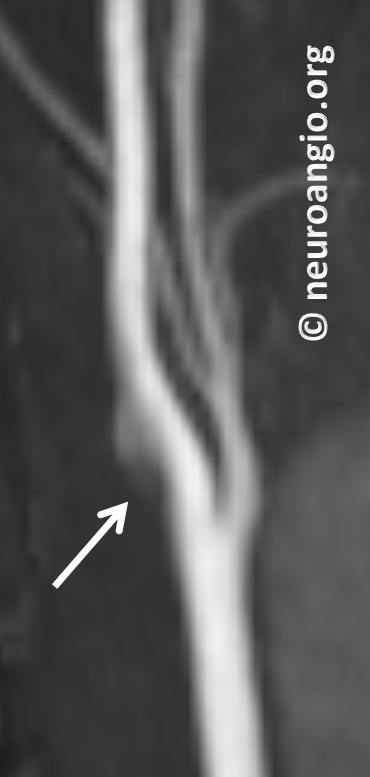
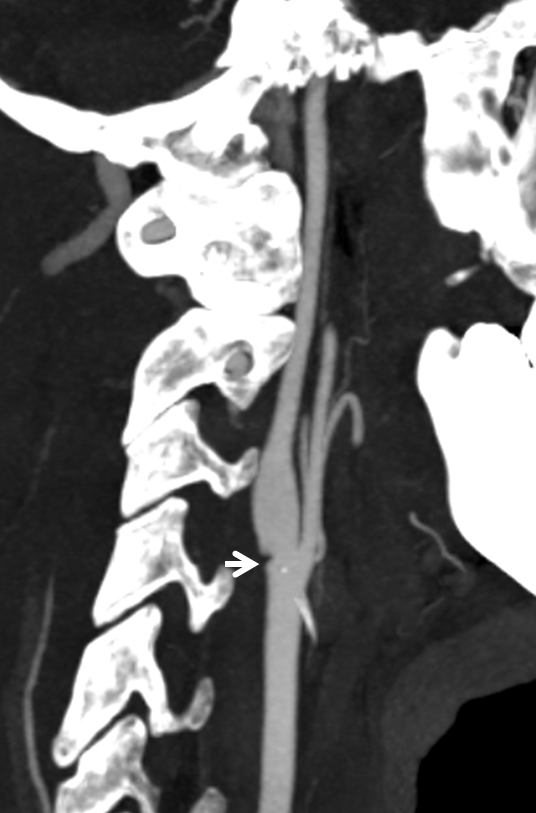
Contrast-enhanced neck MRA, still all in the same patient. Not as good as CTA, but definitely good enough. It is our preferred method for following webs, as no radiation is involved. The left side is normal
Finally, because of another question (possible aneurysm) the patient underwent a catheter angiogram. It shows the web best, of course. However, it is invasive and we do not usually perform angiograms for the diagnosis of webs — a CTA or contrast MRA is sufficient.
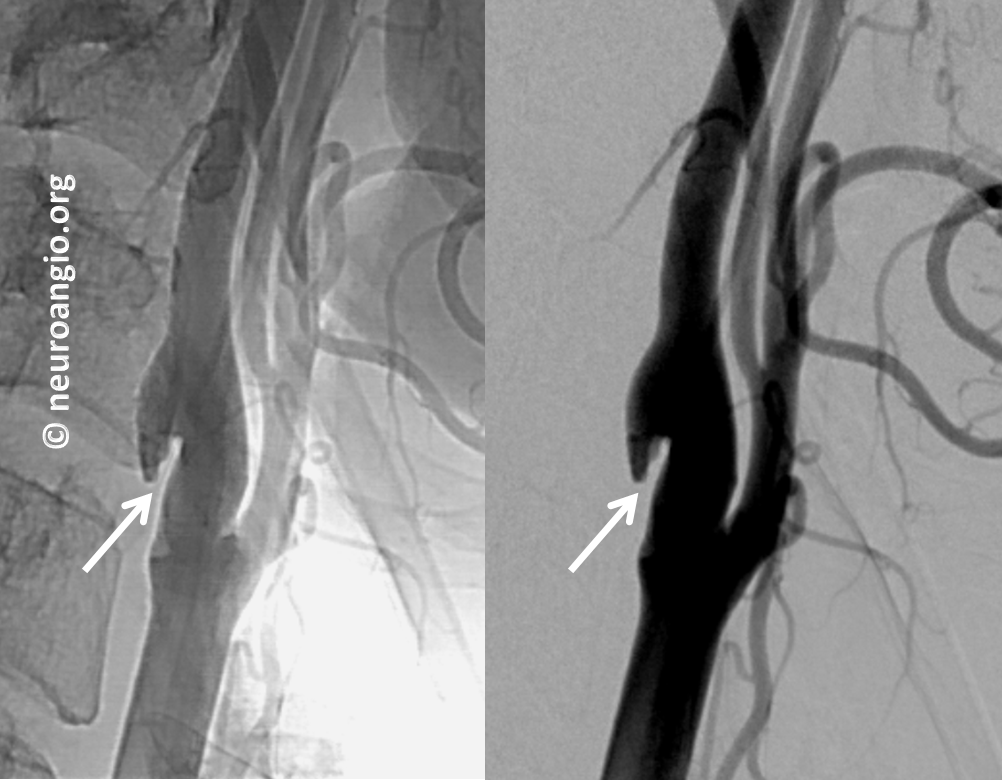
Late phase image (right) shows marked stagnation behind the web (black arrow)

This is not a dissection and not a plaque. Management is with a baby aspirin since there is no history of stroke.
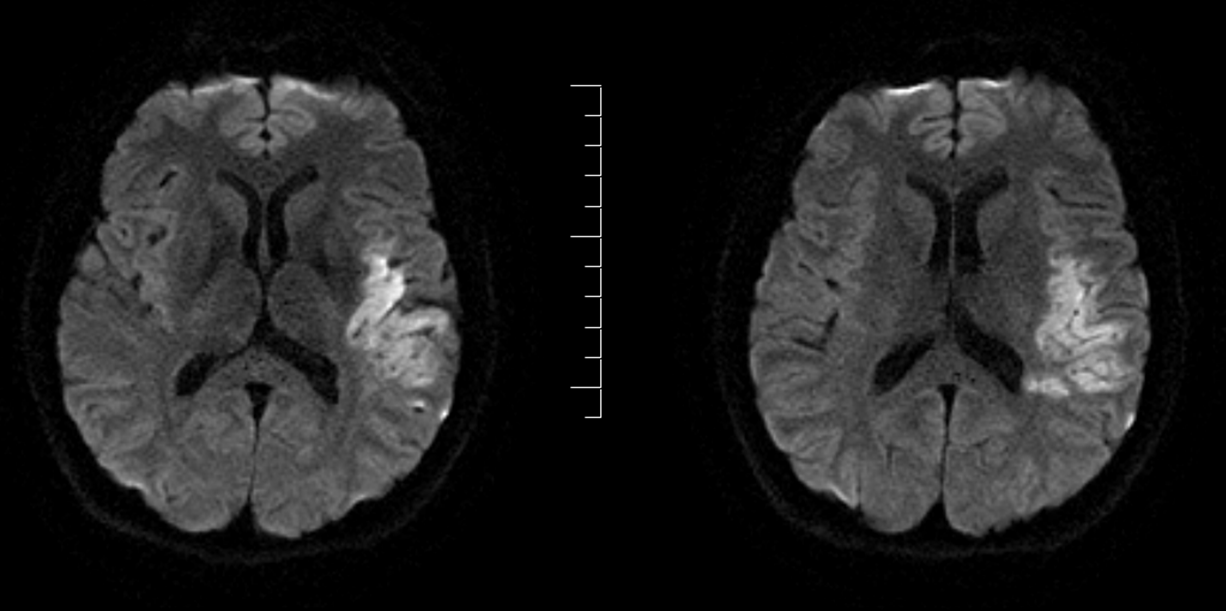
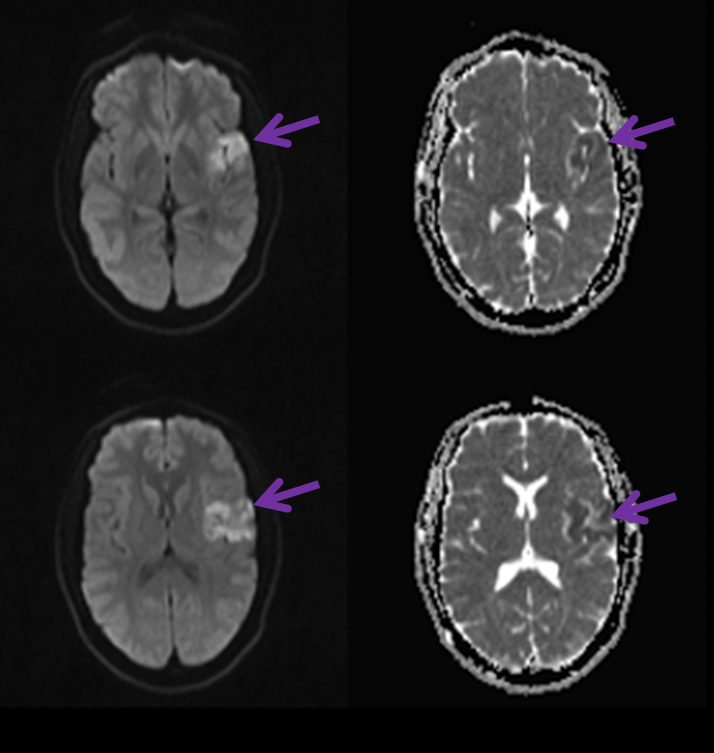
Case 2 – Web-related embolic stroke
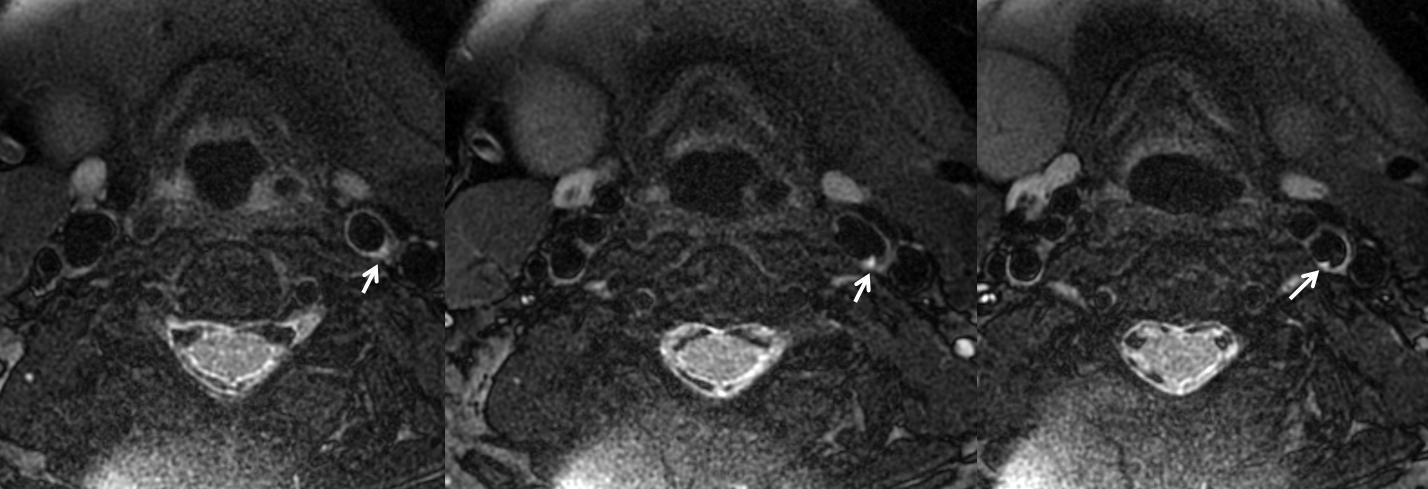
MRI, vessel wall imaging. The web is a thin, shelf-like structure marked by white arrows.
Source image of CTA, same morphology, but MRI axials are more informative
Reconstructions show typical morphology
Finally, catheter angiogram volume-rendered image with a nice shelf

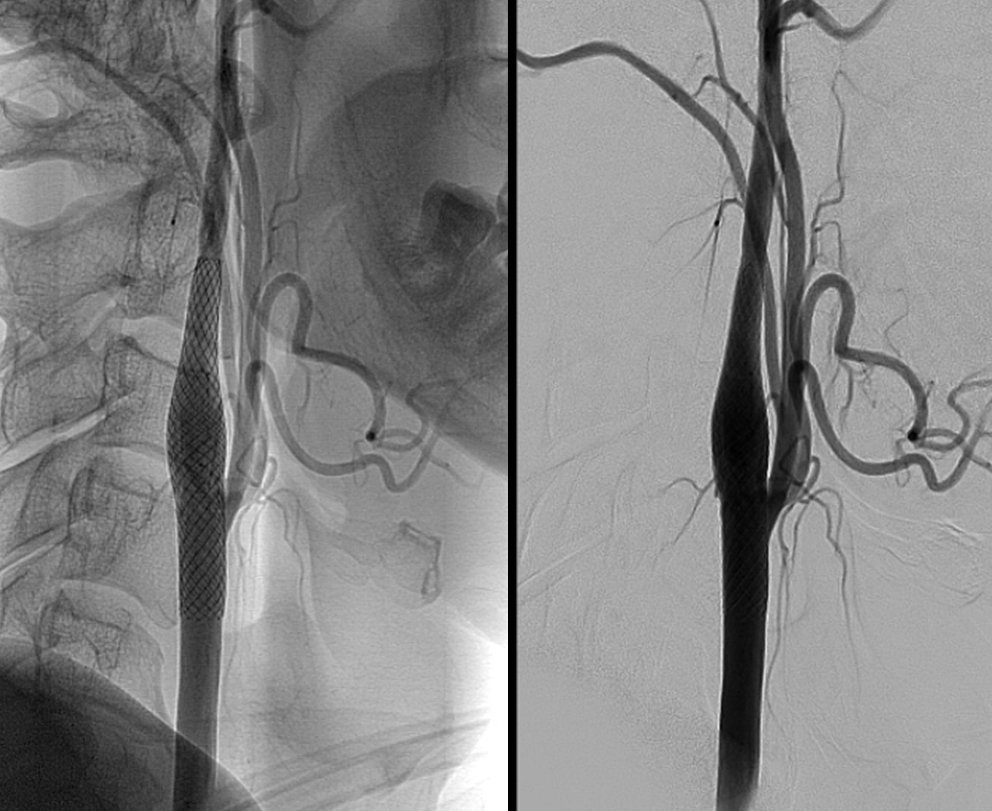
In this case, treatment was stenting (the more common modality among those familiar with the lesion). You can see how the web is flattened by the stent, and therefore no longer a source for turbulence and thrombus formation.
Case 3 — another web-related stroke
Typical images of the culprit carotid web on an MR angiogram

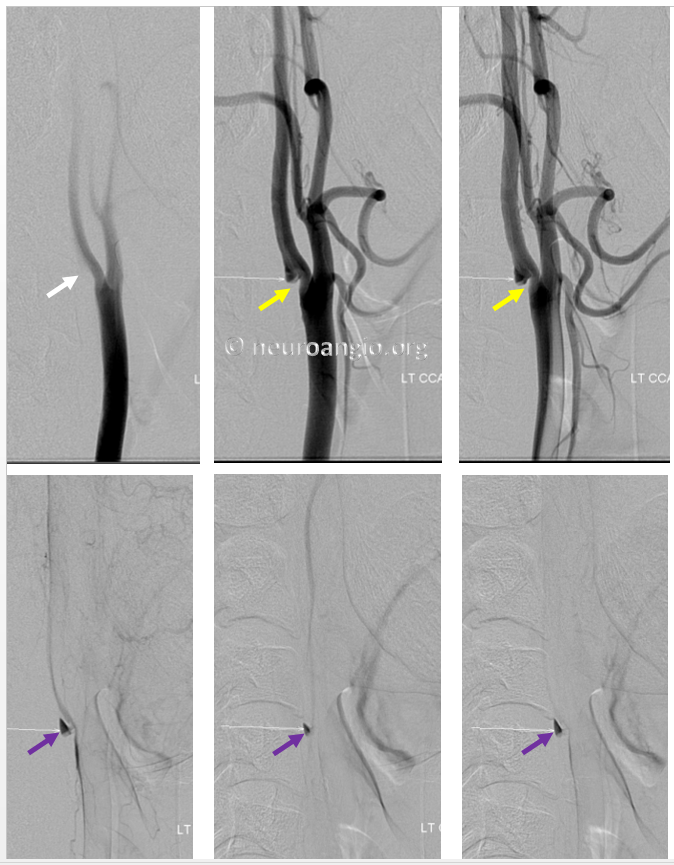
Here is a web on a catheter angiogram. The yellow arrow points to the web. The purple arrow points to slow blood flow behind the web. Clots can form in the area of slow flow (purple arrows) and cause artery to artery emboli just like the one above
Another case from an older page where it used to be case 2. As you can see, they all look pretty much the same

Conclusion: Don’t forget about the web especially not in young patients with recurrent stroke events in same territory and with “no underlying cause found”. Not all carotid bifurcation disease is atheromatous. A young person with the above picture spectrum is not a cholesterol plaque case. Its a web.
Don’t believe it? Check out some traditional literature. Here is one of the first reported cases in AJNR
http://stroke.ahajournals.org/content/strokeaha/22/1/94.full.pdf
Angiogram from this manuscript, same as any other web

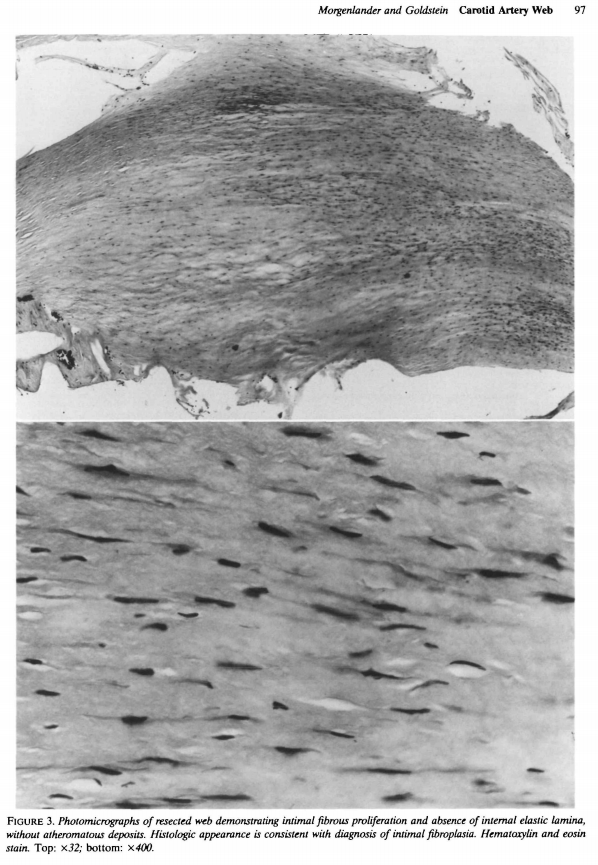
Histology from same article, nonatheromatous connective tissue
Still don’t believe in web? MR CLEAN authors do, as well as whoever on “Radiology” reviewer roster reviewed their manuscript. Now, “Radiology” is a very serious journal, and we do owe the MR CLEAN group BIG TIME, even if they haven’t figured out how to do stroke under general anesthesia 🙂 Check out their publication here
Here is an early web report, in a surgical publication from 1968, Fibromuscular hyperplasia of the carotid artery causing positional cerebral ischemia. A very rare web large enough to manifest as a hemodynamic issue