
Number 31
A really (so far) invisible branch of the petrous ICA, coursing posteriorly towards the middle ear. Cant see it on Cone Beam CT either. Pesumably, it is invisible because of the extreme density of the temporal bone within which it reportedly lives. The fact is that we see so much on Cone Beam CT — including within the temporal bone — for example see the Subarcuate Artery, and of course the Facial Arcade. Not number 31 though…
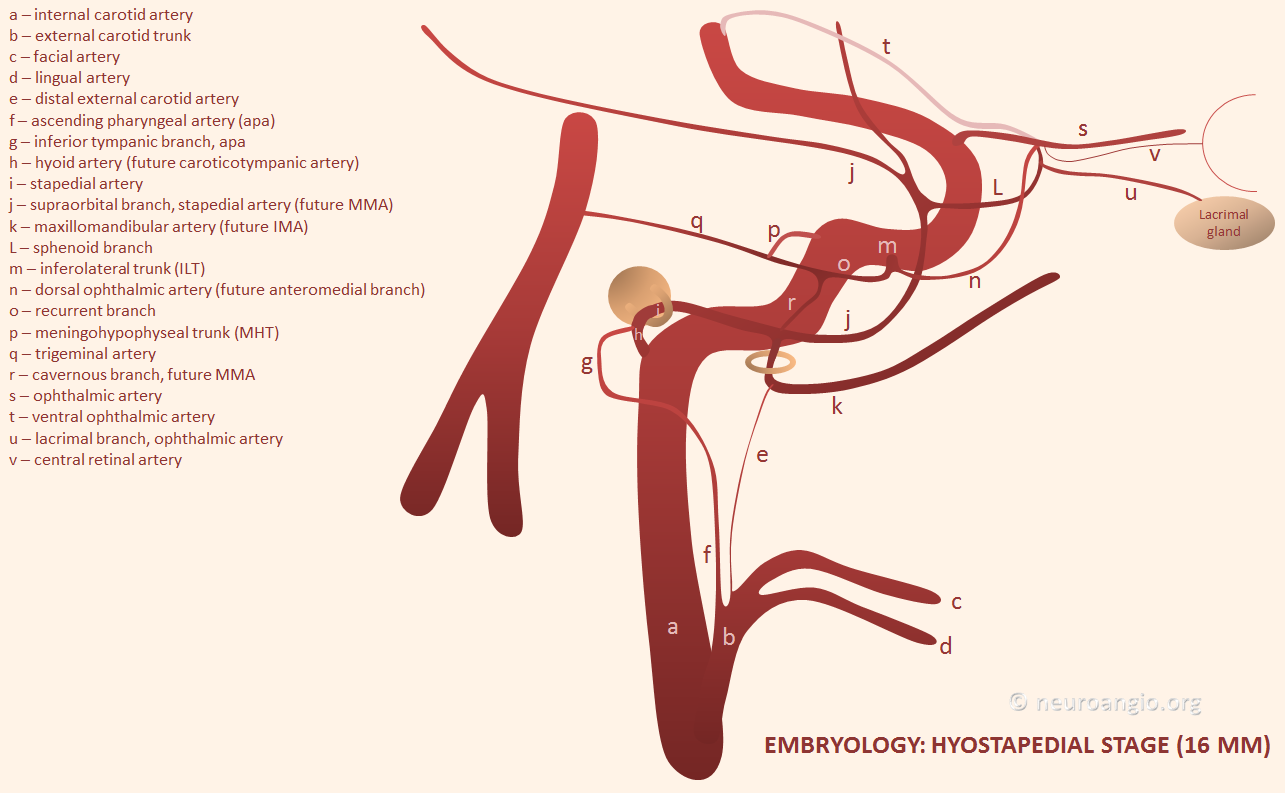
The embryology seems convincing enough that it does exist — as the “hyoid” artery. In hyostapedial stage of embryology, it seems to do quite a lot — supplying the MMA and IMAX territories, before their annexation by the ECA. See image below – “h”
Its main claim to fame is that it constitutes part of the “aberrant carotid” artery variant. This is what happens when the carotid artery traverses the middle ear — just behind the eardrum. This is the classic bluish – reddish mass behind the tympanic membrane that one is NOT supposed to biopsy.
The aberrant carotid is not a carotid — it is an adaptation to cervical carotid agenesis. The petrous carotid is reconstituted by the ascending pharyngeal artery via the inferior tympanic-caroticotympanic anastomosis to the petrous ICA – f-g-h – in the image above.
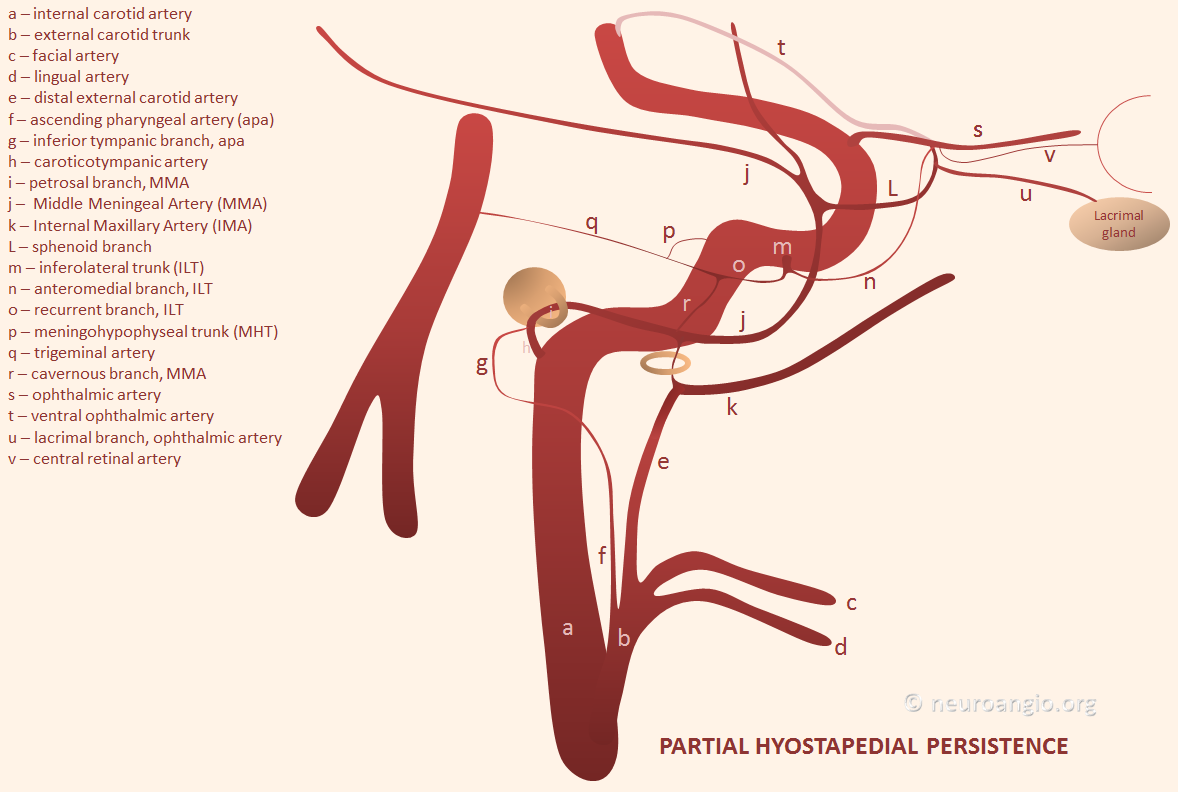
Rarely, it keeps its middle meningeal territory, appearing as carotid origin of the MMA — known as “partial hyostapedial persistence” — see image below
Real life examples below
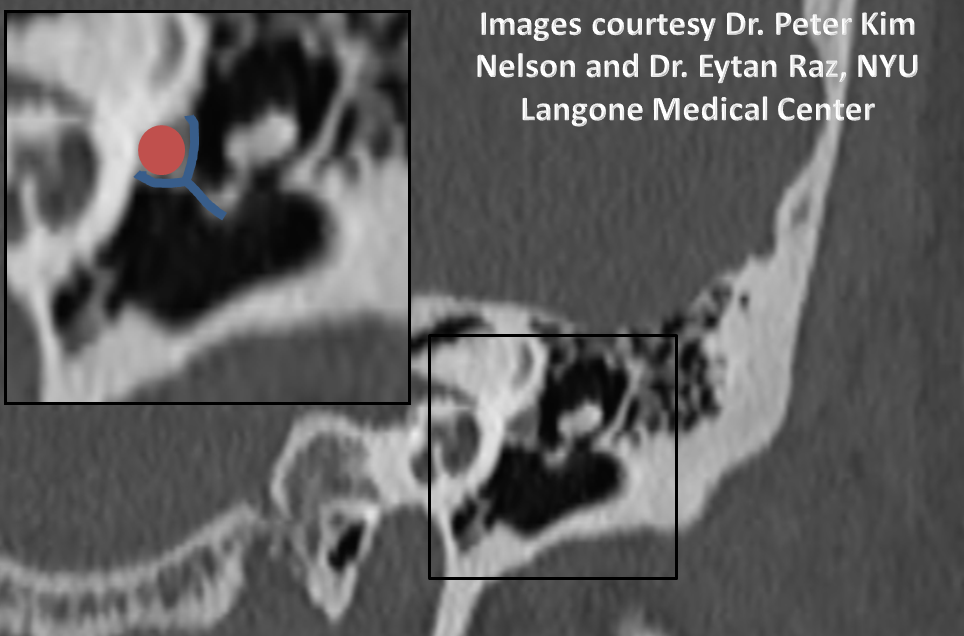
The stapedial adult part of the hyostapedial artery courses exactly inside the crura of the stapes bone. Most people with this do not have pulsatile tinnitus. Because they were born like that.
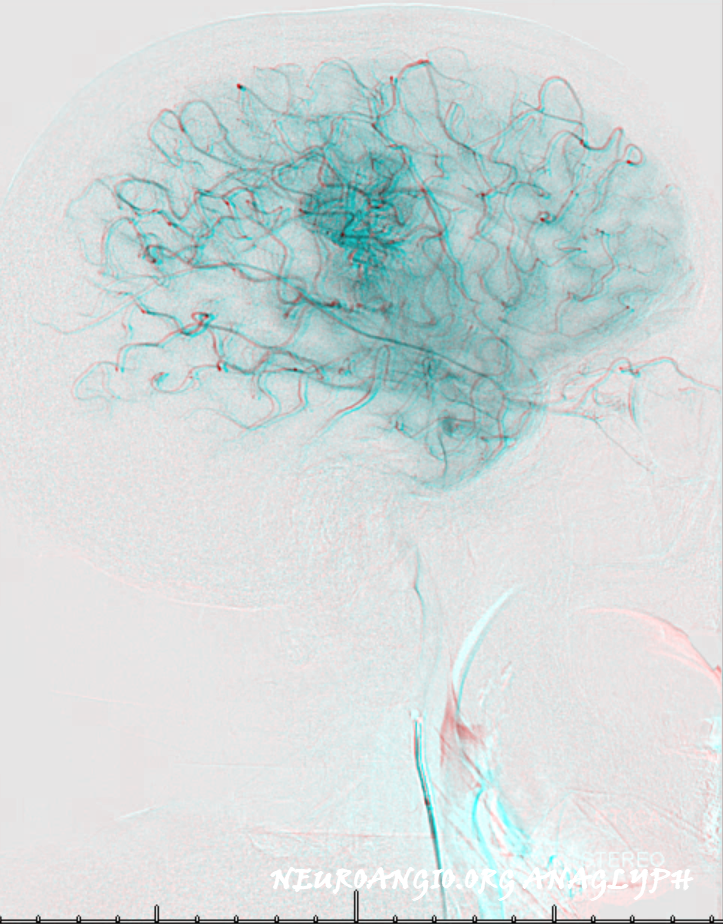
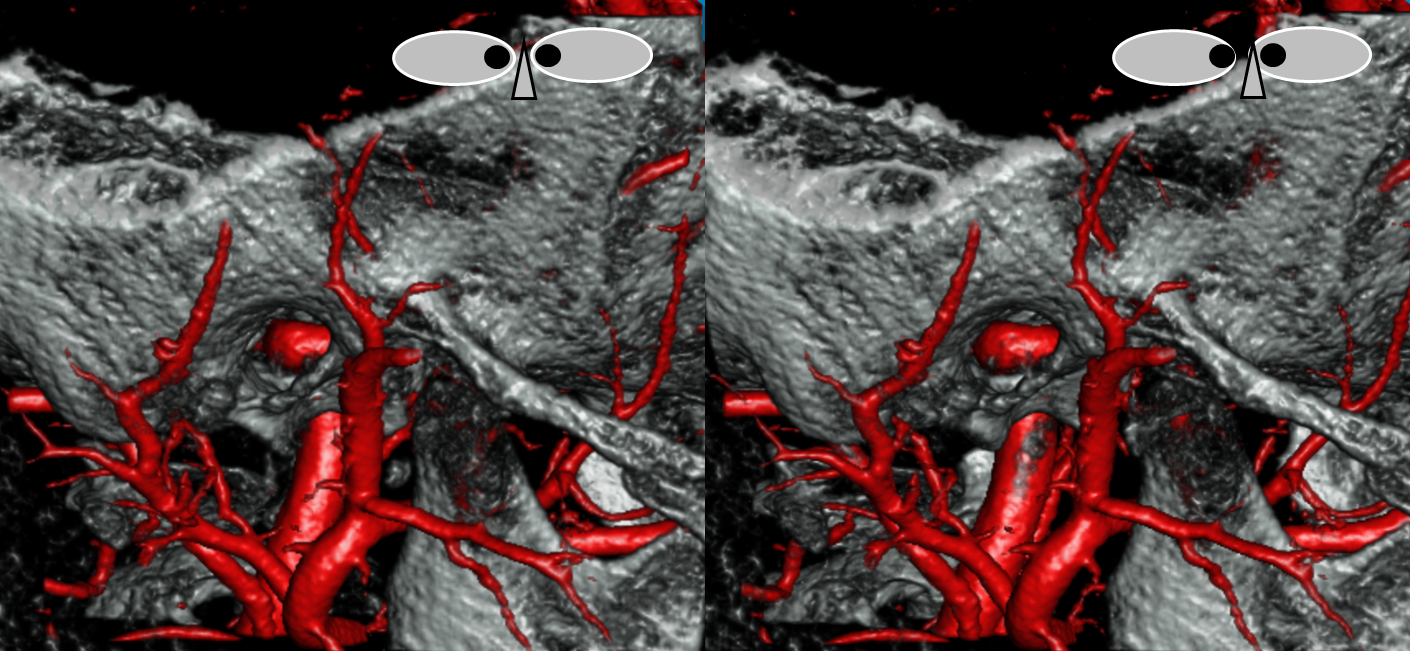
Anaglyph stereo

Corresponding lack of MMA from the ECA
Complete Hyostapedial Persistence — supply of both IMAX and MMA by the hyostapedial artery (schematic below) is extremely rare.
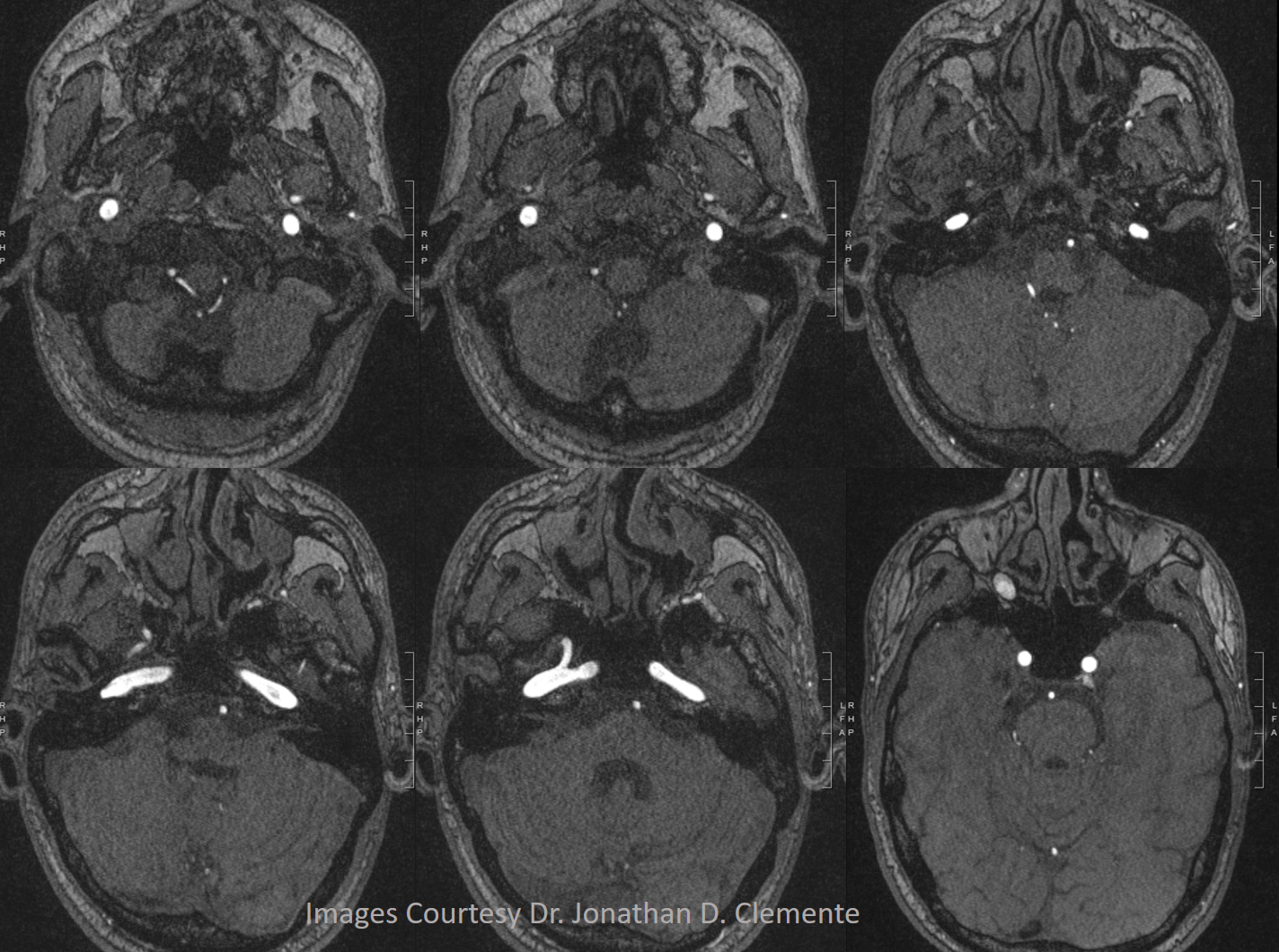
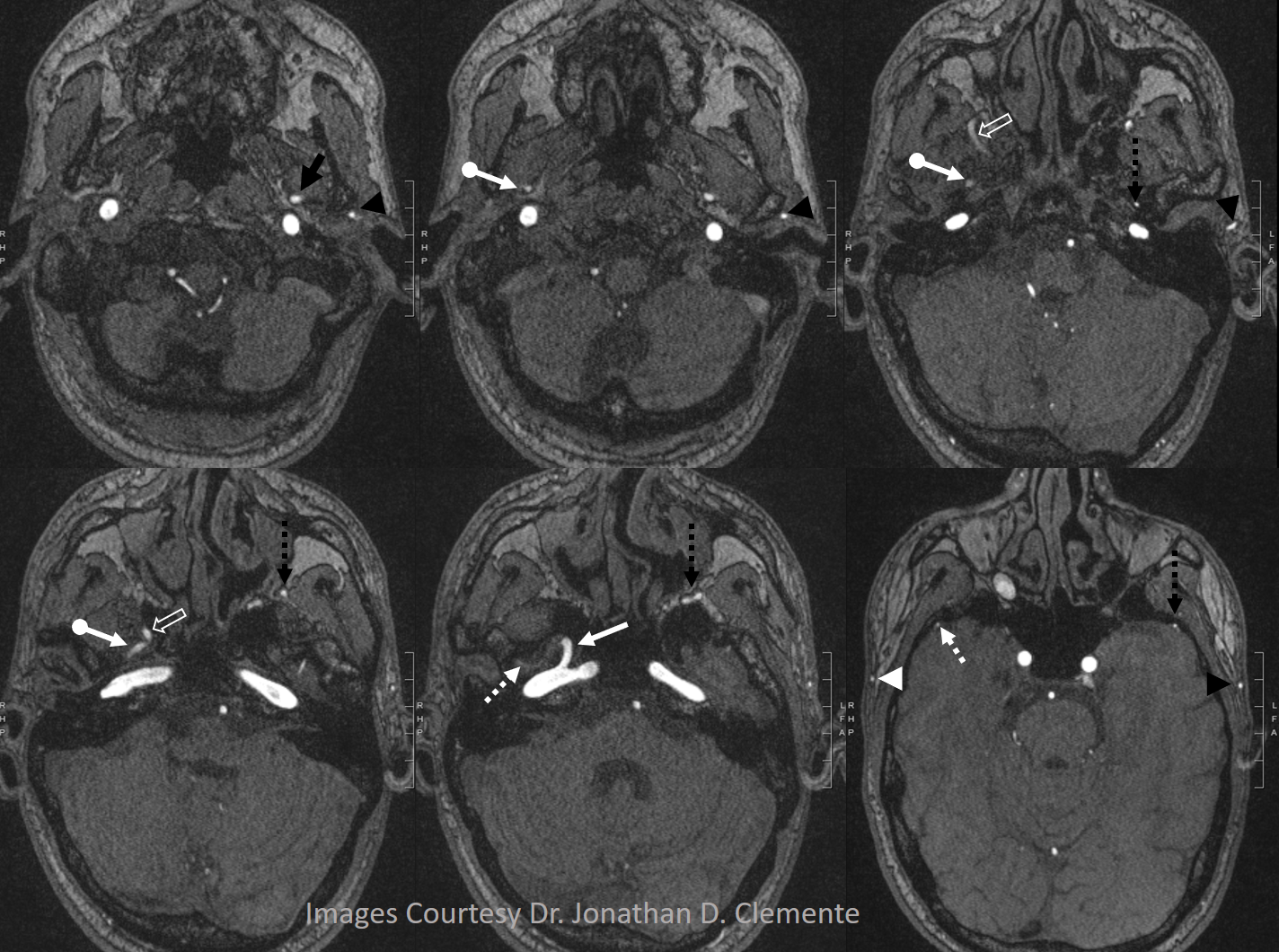
Example by Dr. Jonathan D. Clemente.
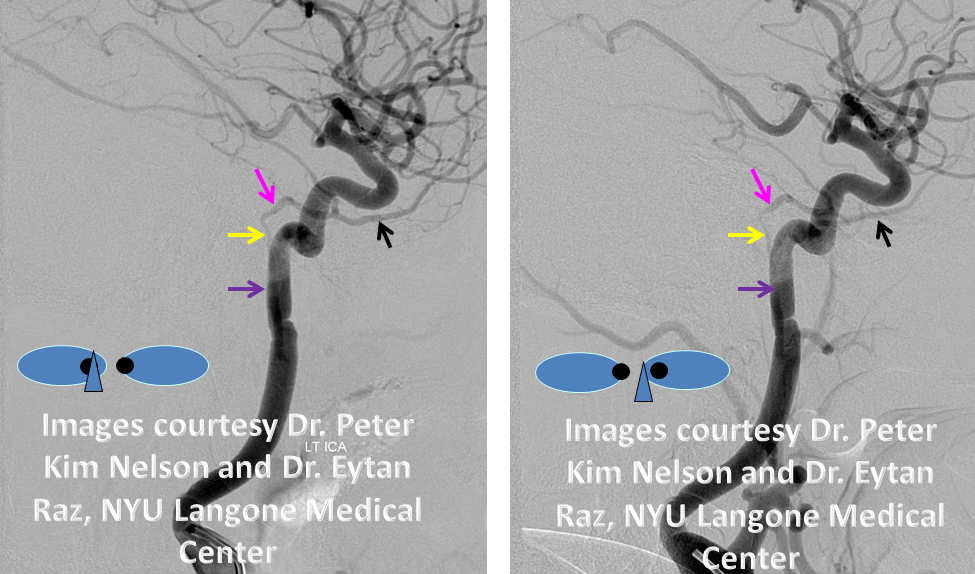
Below is one with arrows. On the normal left side, the IMAX (black arrow), STA (black arrowhead), and MMA (dashed black arrow) are all in usual places. On the right, the vidian artery (white arrow) supplies both proximal (white ball arrow) and distal (open white arrow) IMAX. The IMAX “gives rise” to both MMA (dashed white arrow) and STA (white arrowhead). Not bad, huh!

Aberrant Carotid Artery
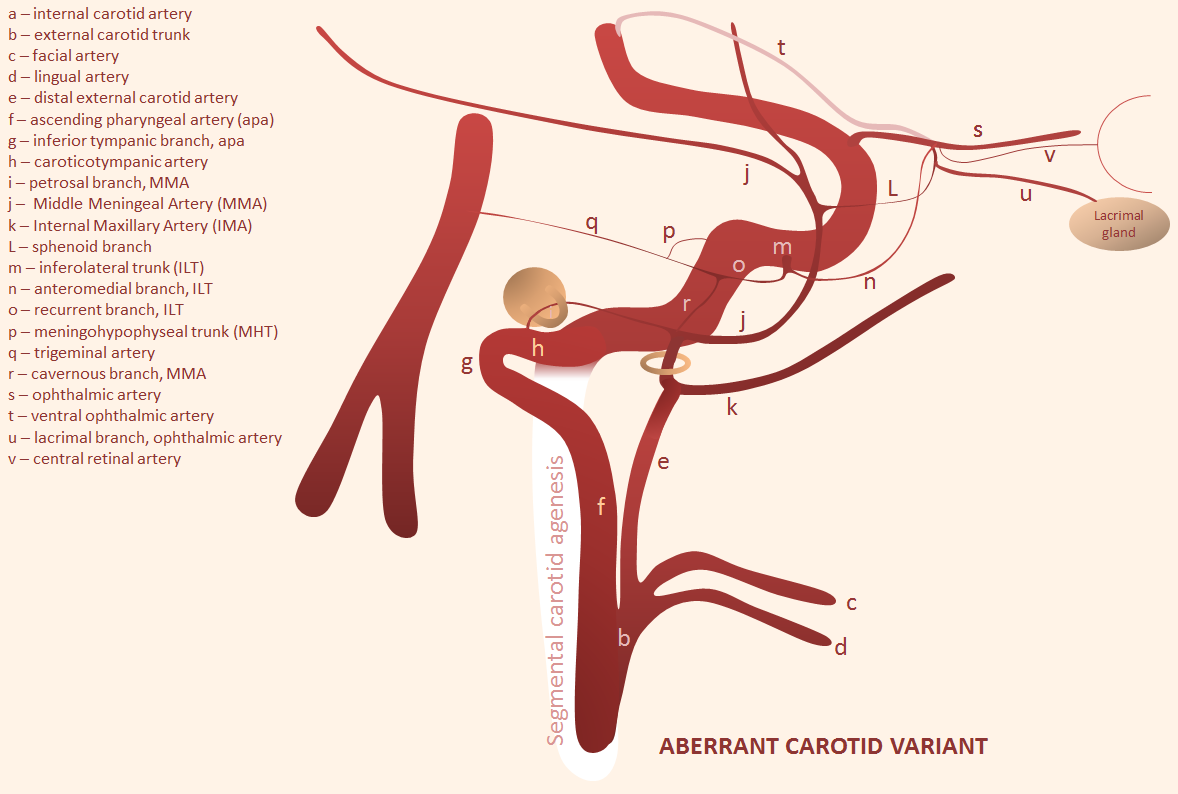
This is classic embryology — understanding that there are no “new” vessels — just existing ones repurposed for some need. The idea here is that for some reason there is agenesis / failure of development of the cervical segment of the ICA. The compensation is a kind of “bypass” — an anastomosis between the ascending pharyngeal artery inferior tympanic branch to the caroticotympanic branch to the presumably normally forming petrous ICA — see image above. This “aberrant” ICA courses through the middle ear. The classic ENT disaster is a biopsy of a presumed “retrotympanic” mass, leading to massive hemorrhage.
This is how it looks like on an older cone-beam CT
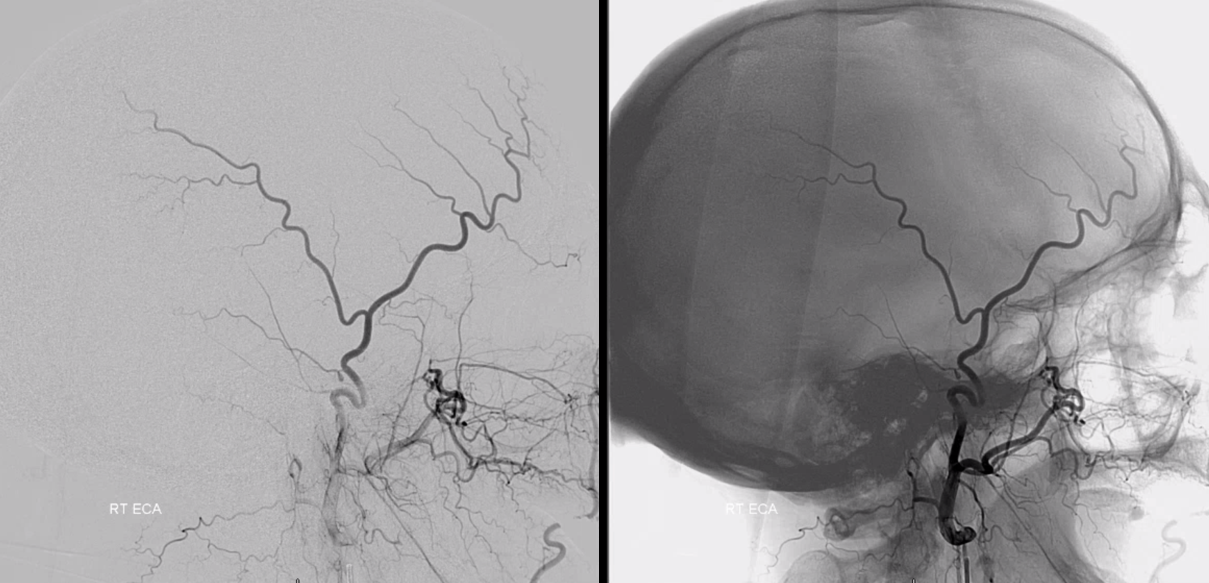
2D-DSA — lateral and posterior course of the artery
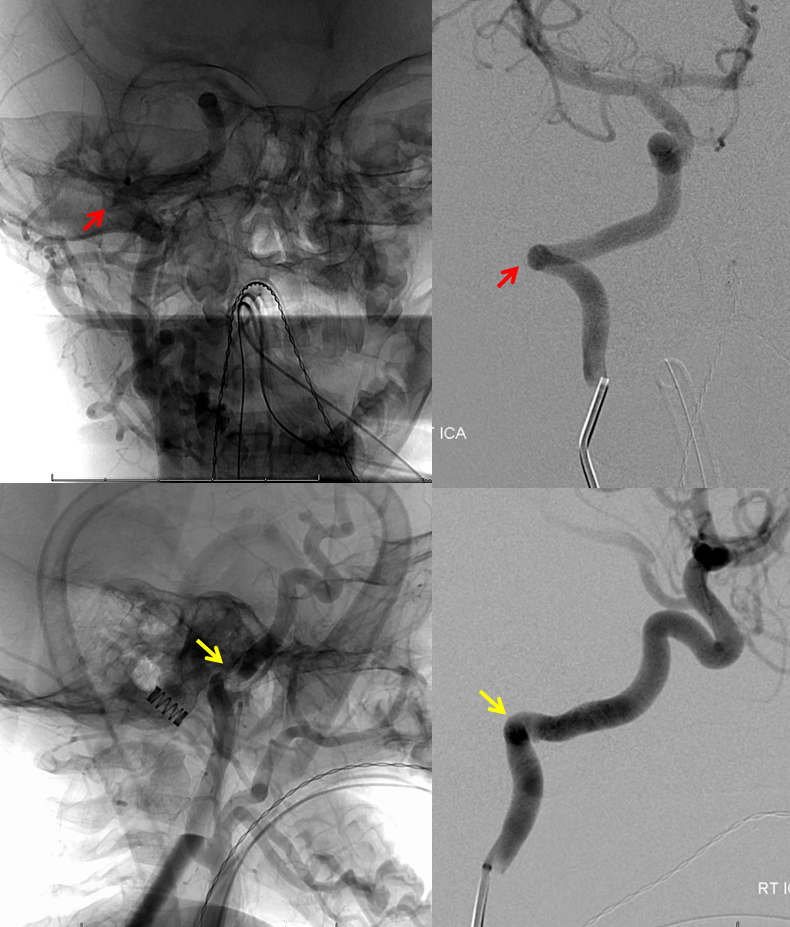
The same case — MRA — much harder to differentiate from normal ICA
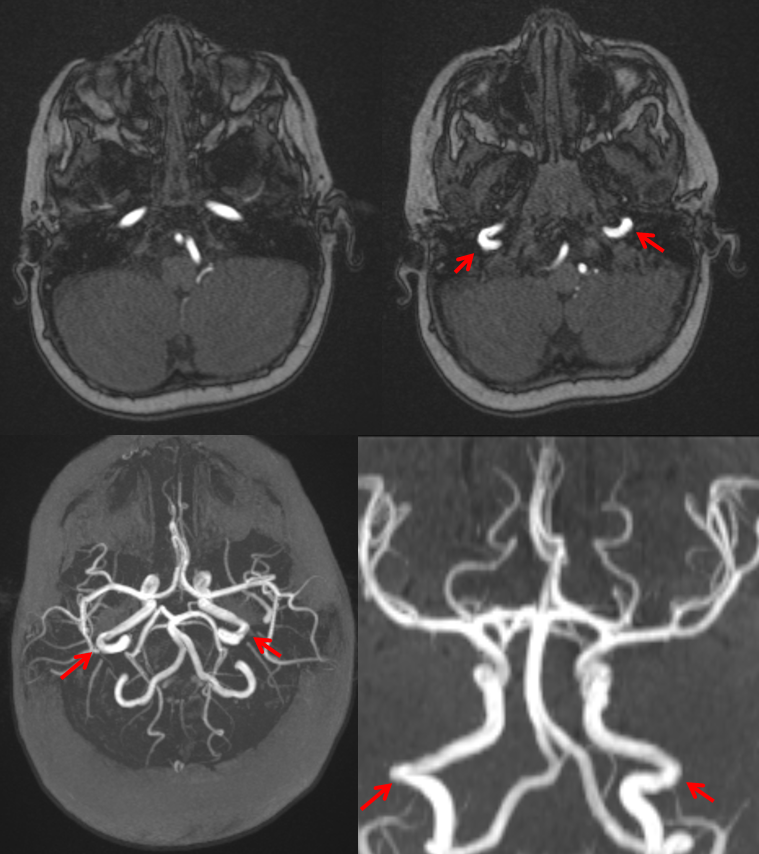
CT — different case
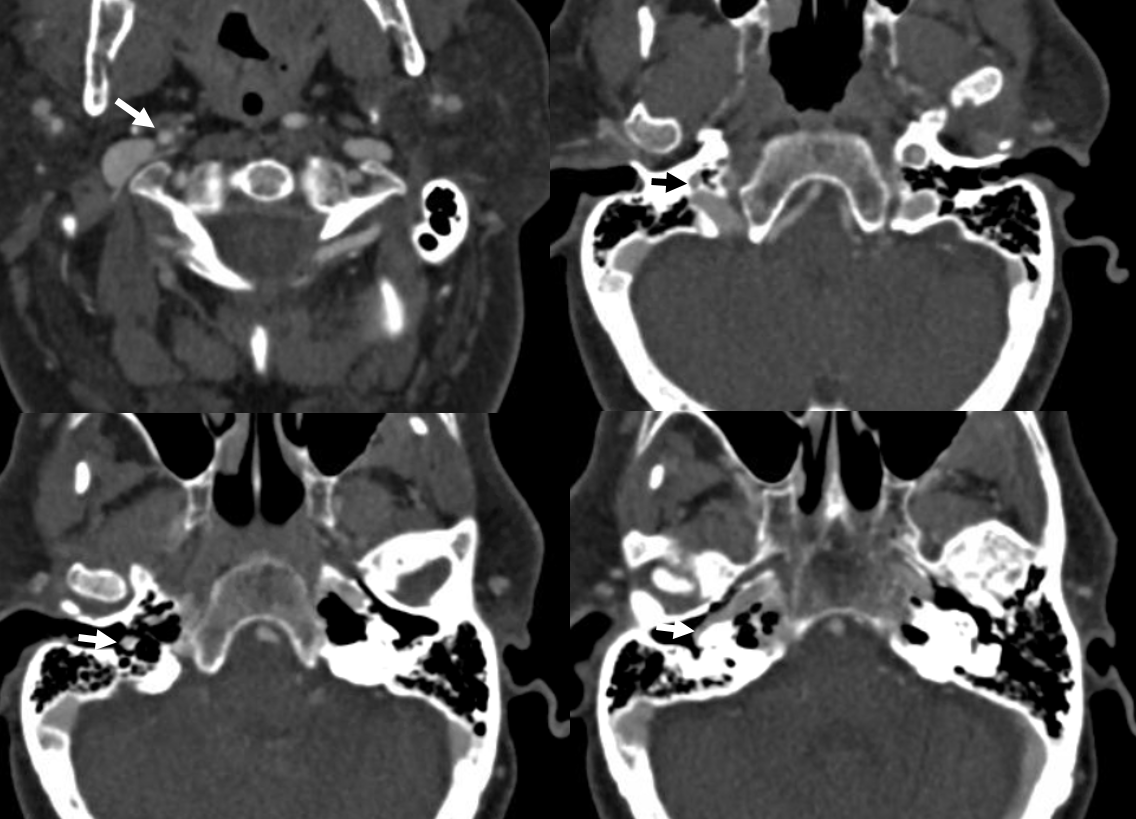
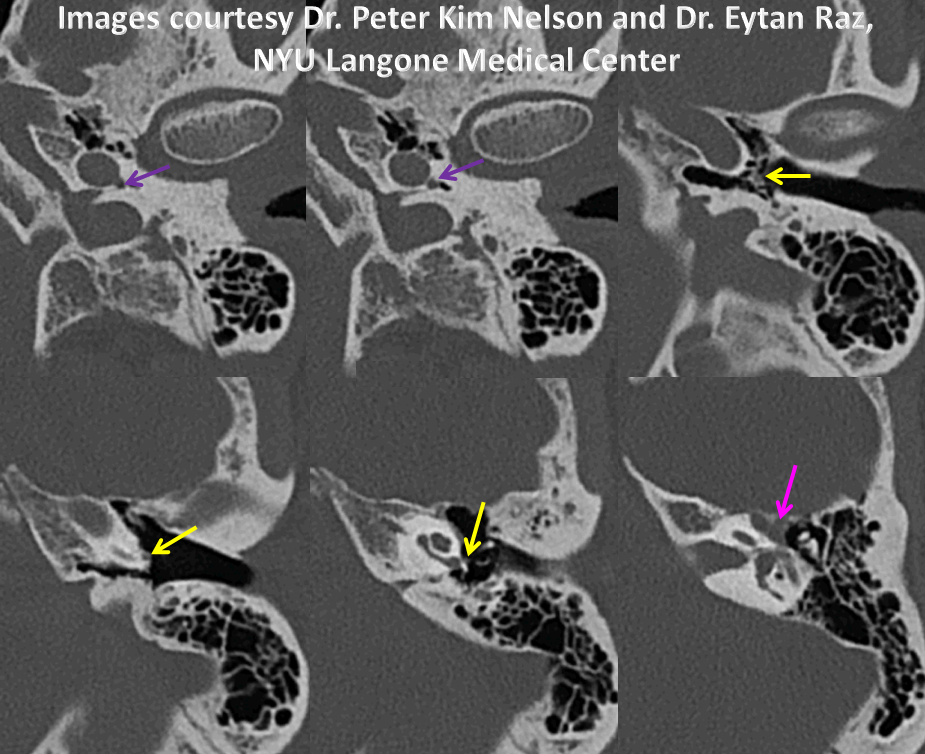
Probably best seen on thin section CT — where relationship with bony structures and middle ear is clear — Courtesy Dr. Todd Miller, Stamford Health
You don’t even need contrast to see an aberrant carotid on high-res CT such as t-bone or thin section helical CT like this one. The path through temporal bone, and over the cochlear promontory (arrows) is really obvious. Below is a pre-contrast mask of a CTA
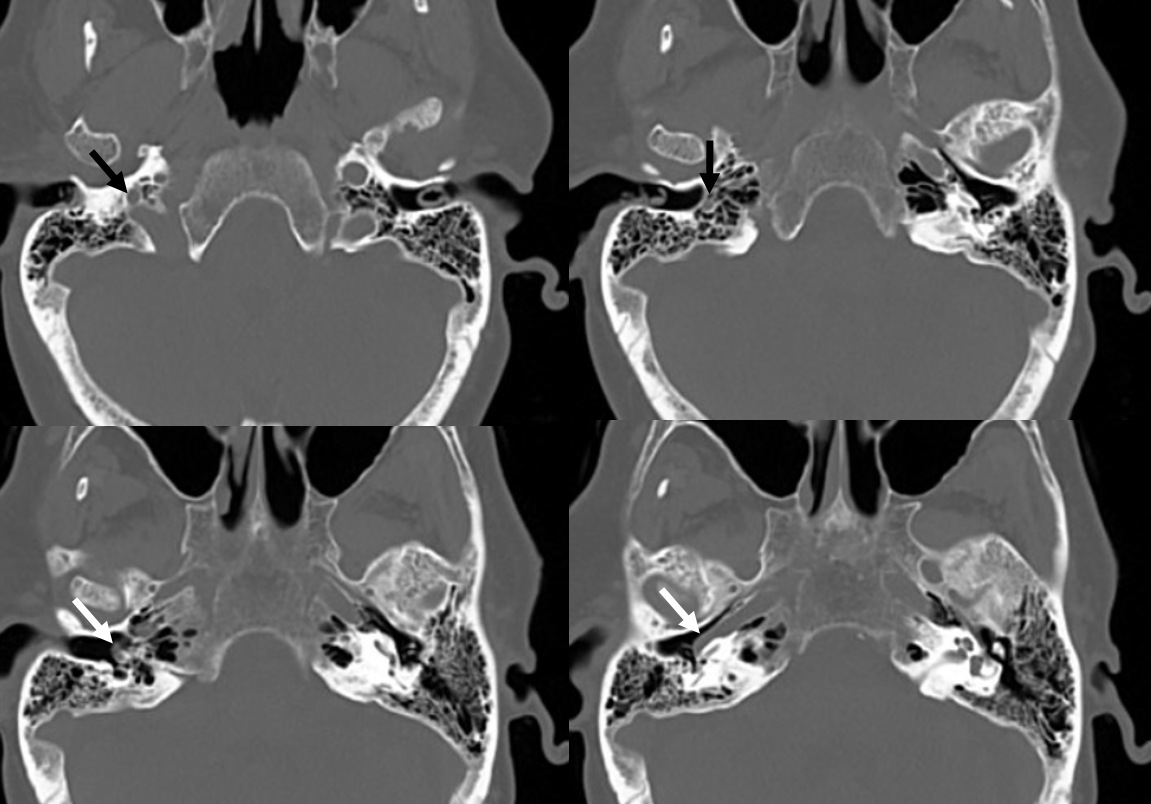
Post-contrast