
Overview:
The ascending pharyngeal artery, typically an early branch of the external carotid artery, participates in vascularization of the oropharynx, nasopharynx, Eustachian tube, middle ear, and skull base/dura/nerves of the jugular bulb and hypoglossal canal. Through its wealth of potential intracranial and extracranial anastomoses, the AP artery earns great importance that is far out of proportion to its ~1 mm diameter proximal size. AP injections can be invaluable in angiographic study and embolization of vascular lesions, particularly of dural location. We strongly emphasize understanding of AP anatomy as on the major goals in endovascular instruction.
Adult anatomy and anastomotic networks
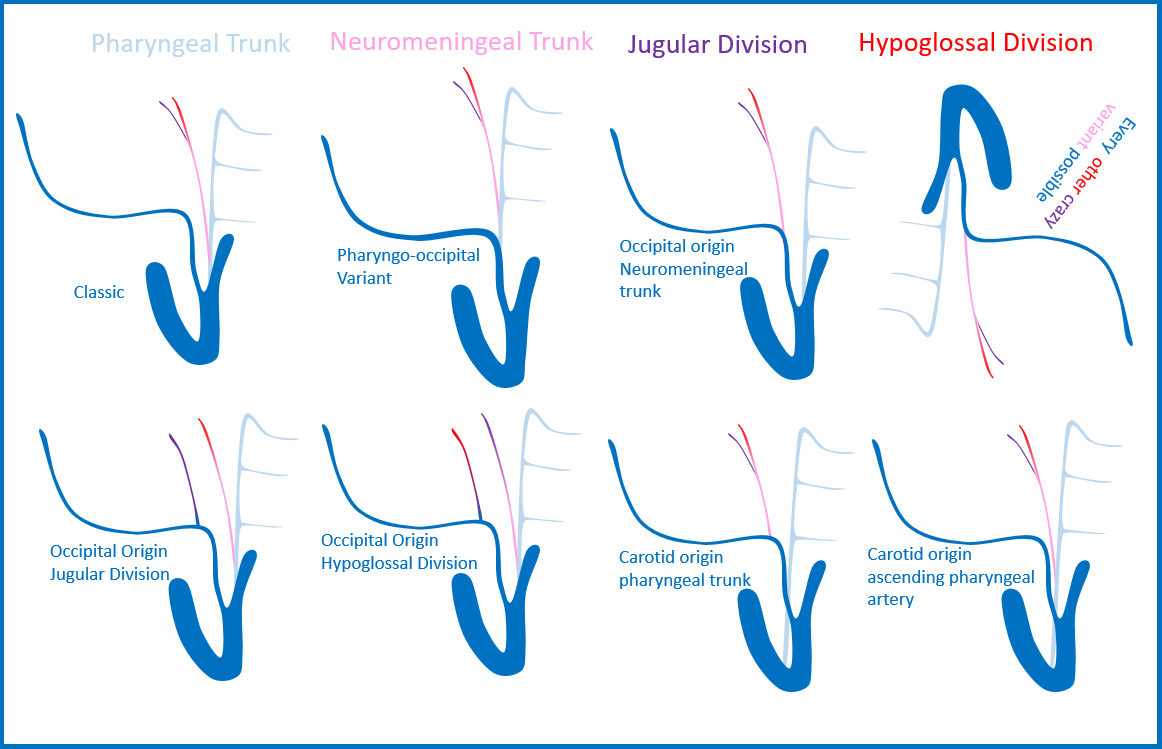
Classically, the AP artery courses straight up, anterior to the external carotid, and posteromedial to the internal carotid, outside of the carotid sheath. In its usual disposition, the AP consists of two divisions, fulfilling very different roles. The more anterior pharyngeal division participates in the supply of the posterior and lateral walls of the nasopharynx, oropharynx and hypopharynx, such as superior and middle constrictor musculature. The artery reaches skull base and can on occasion have intracranial anastomoses thru foramen lacerum and other routes. The pharyngeal branches are in hemodynamic balance mainly with divisions of the facial artery.
The more posterior neuromeningeal trunk splits up into hypoglossal and jugular divisions, participating in supply of the dura and cranial nerves. The hypoglossal division enters through the hypoglossal canal, supplies CNXII, and vascularizes the adjacent dura. It has rich anastomotic networks with branches of the meningohypohyseal trunk and middle meningeal artery. The jugular division enters thru the jugular foramen and runs poserolaterally. It vascularizes the dura and sends branches running along the course of the sigmoid sinus. Injections of the neuromeningeal trunk can be invaluable in study of fistuals and other dural vascular lesions which may otherwise be obscured on injection of larger contributing vessels. The more proximal cervial portion of the neuromeningeal branch also collateralizes with the vertebral artery and the odontoid arcade via musculospinal branches. A small but embryologically important inferior tympanic branch participates in supply of the middle ear cavity.
BALANCE OF TERRITORY
The central location of AP brings it into banace with too many other vessels and territories, some close and some not so.
Pharyngeal Trunk:
- Accessory Meningeal
- Mandibulovidian
- Ascending Palatine
- Distal IMAX
Neuromeningeal Trunk:
- Caroticotympanic (balance with inferior tympanic branch of AP)
- Vertebral (hypoglossal branch via odontoid arcade, musculospinal branch via upper cervical vert)
- MHT (descending lateral clival branches of MHT and jugular division, medial clival branches and hypoglossal division)
- Posterior Meningeal (origin often from neuromeningeal trunk, in balance with it when origin elsewhere)
IMAGES
CROSS-SECTIONAL AND NON-CATHETER ANATOMY
A review of CT and MR-based techniques before showing catheter angio pictures can be quite helpful in demonstrating nonvascular anatomical relationships. A careful review of pre-angio imaging often gives valuable insights into planning of angiographic procedures.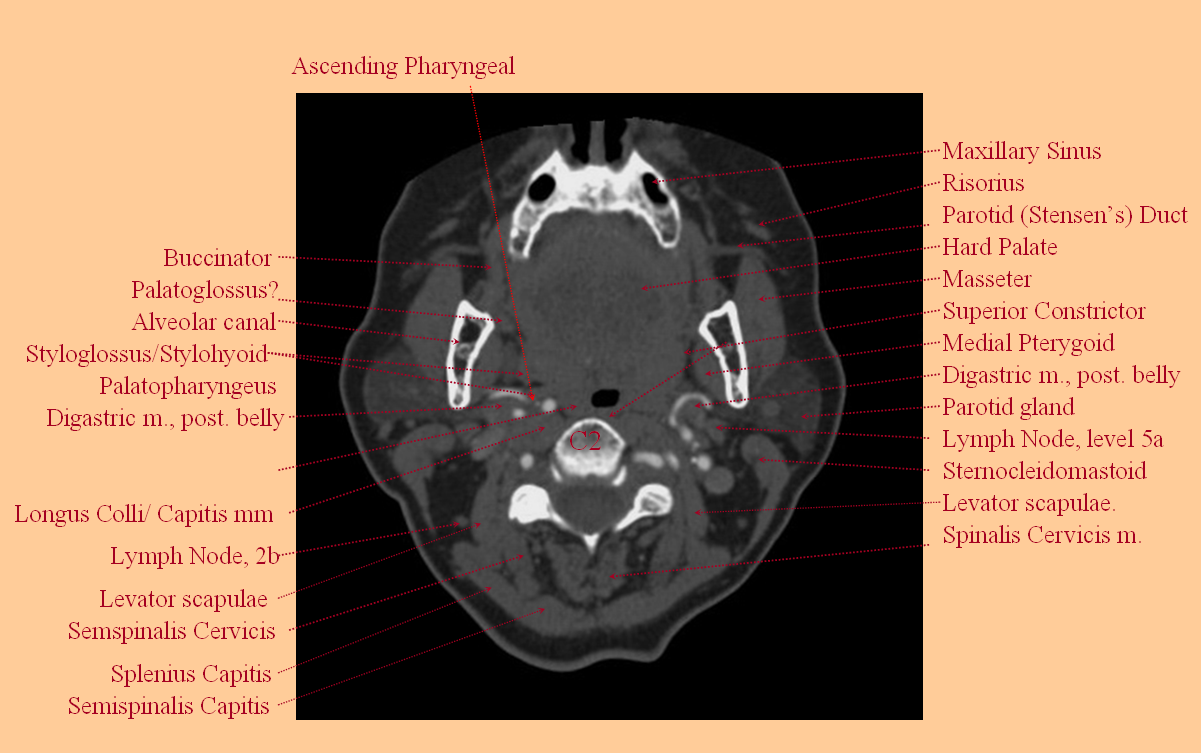
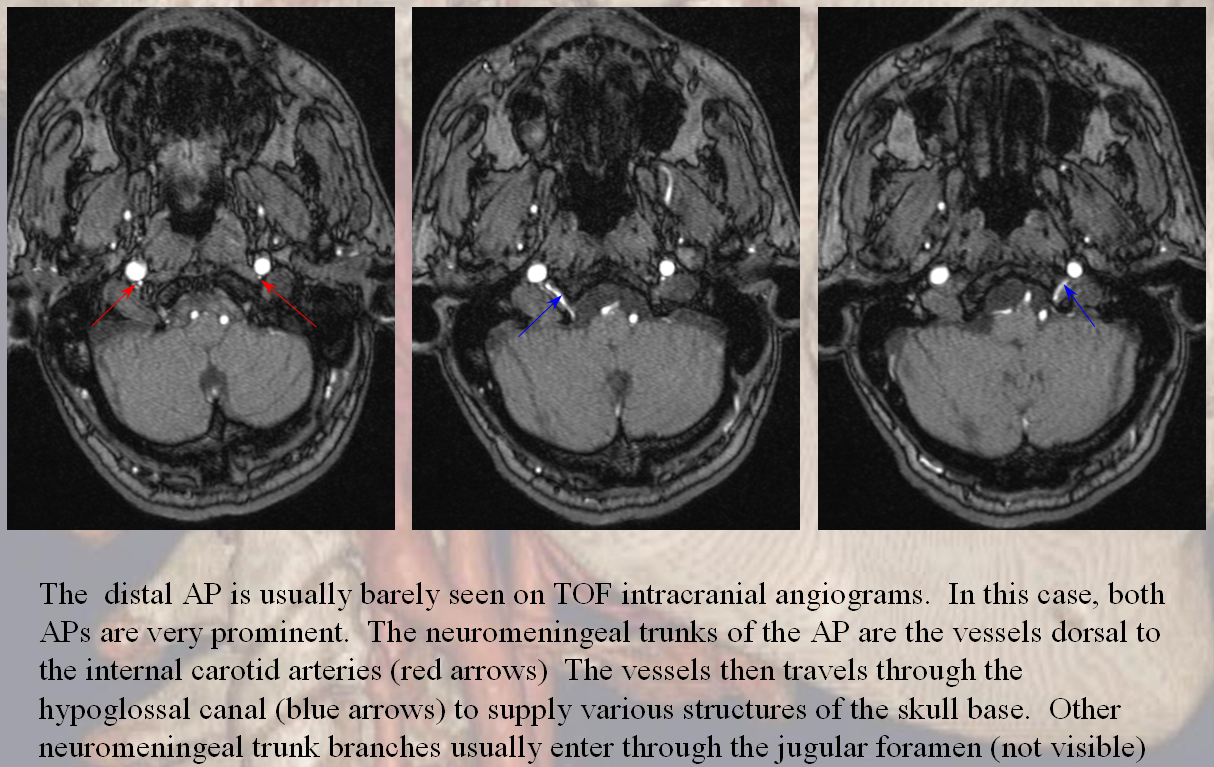
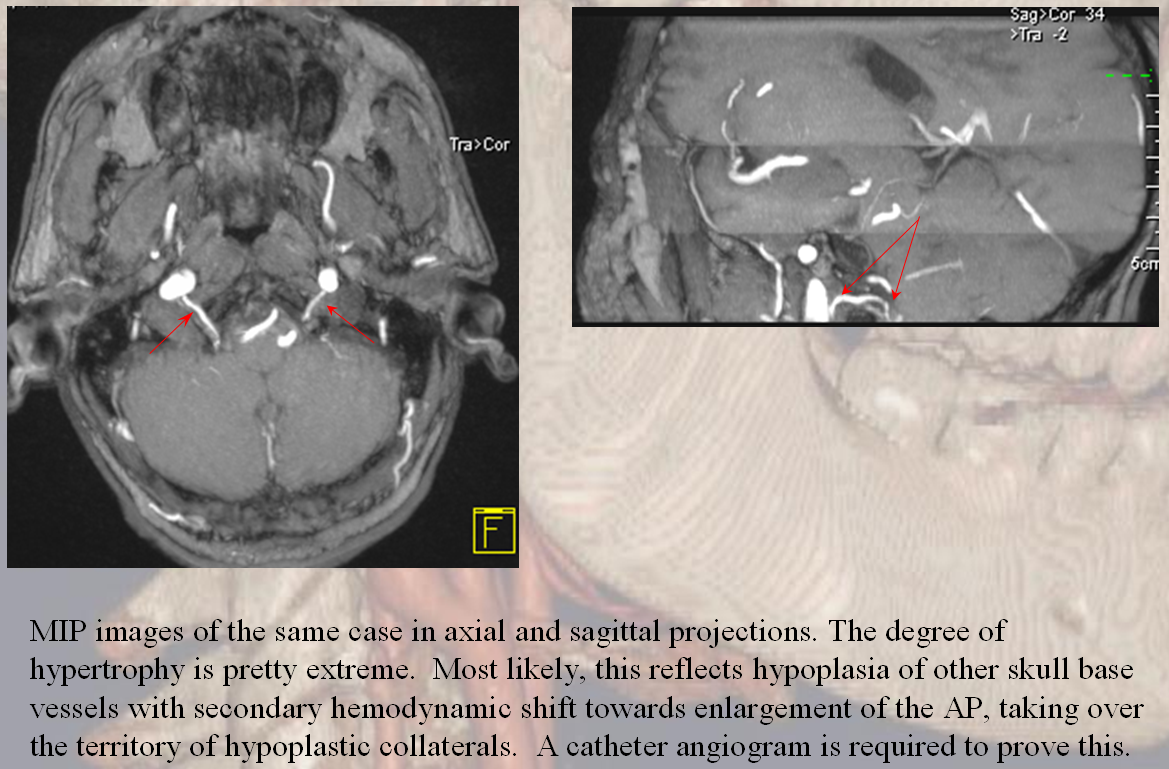
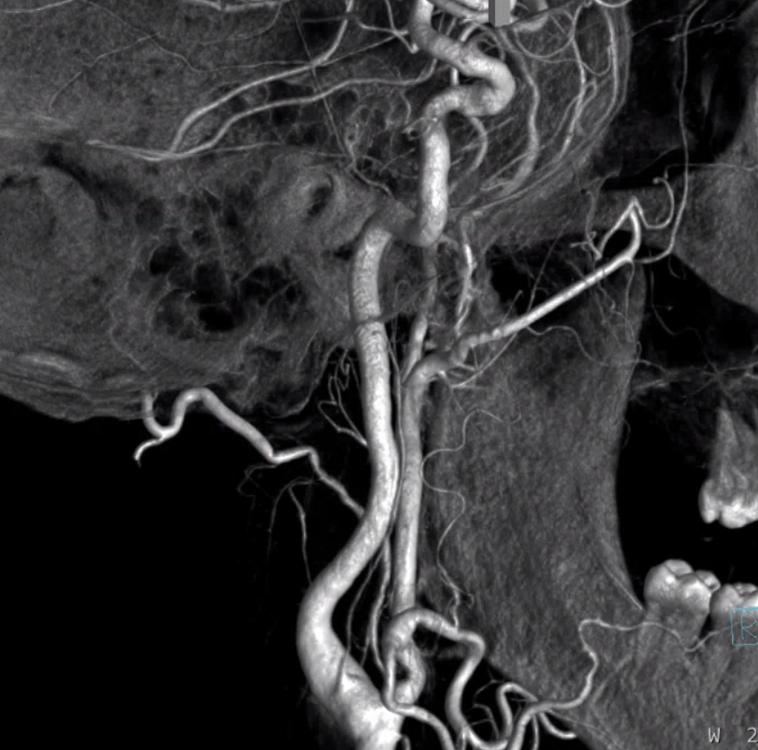
The AP artery is nearly always visible on a high-quality CT angiogram
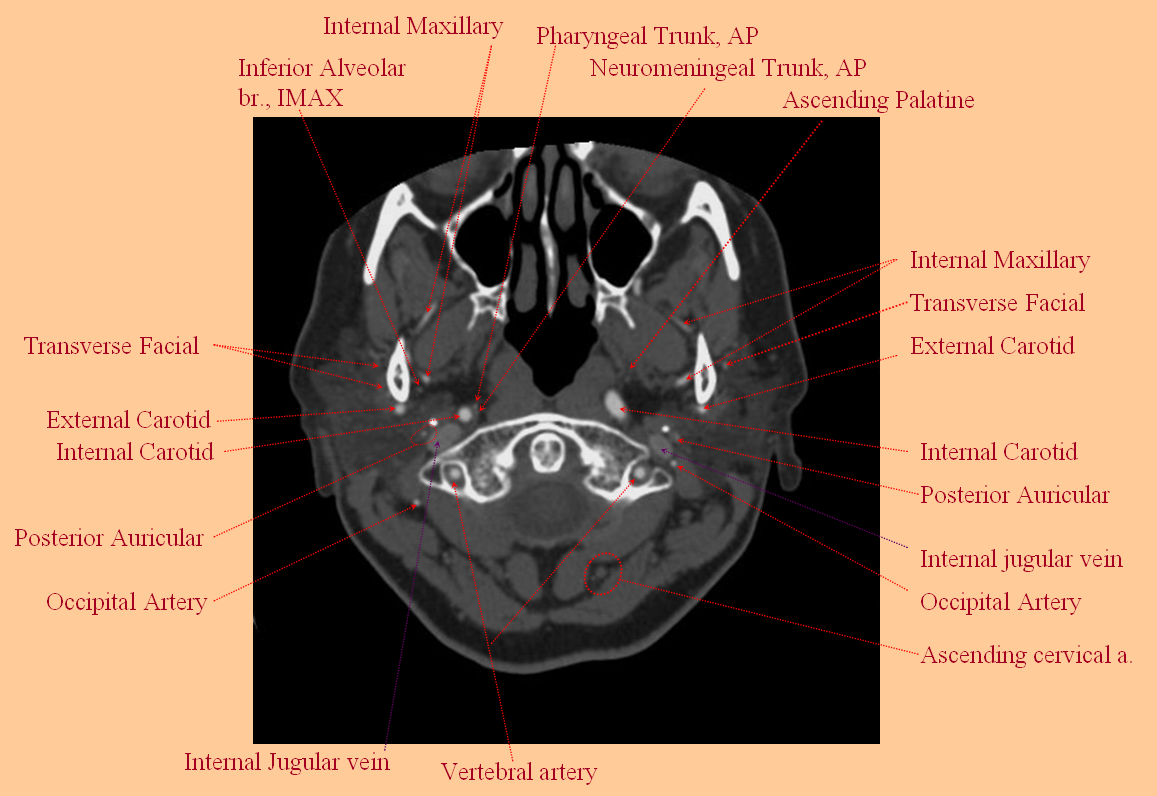
The pharyngal and neuromeninigeal trunks can sometiemes be resolved as well, depending on extent of anatomical development
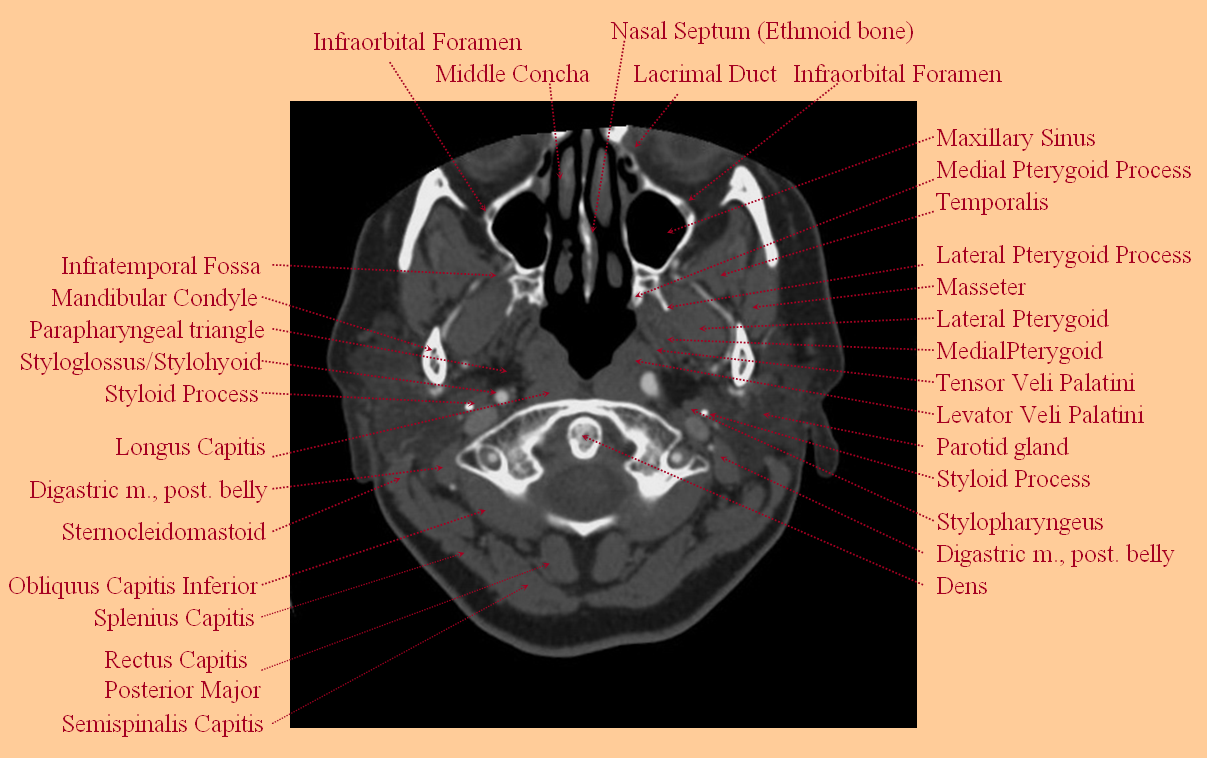
Some additional non-vascular structures of the neck at this level
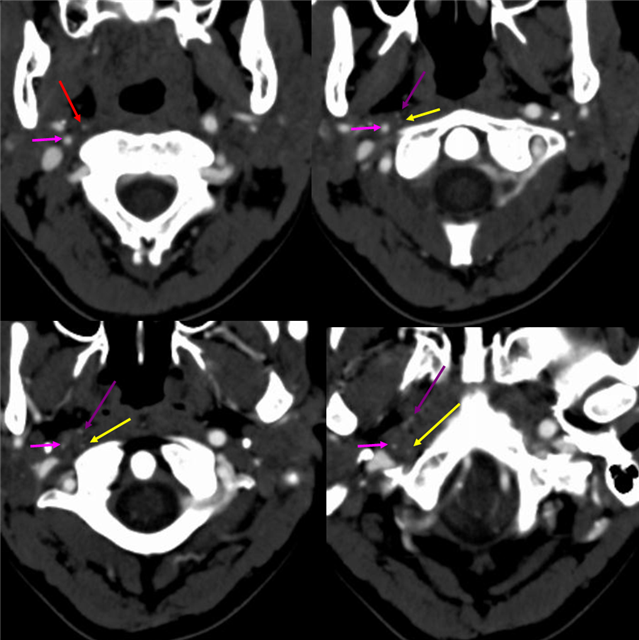
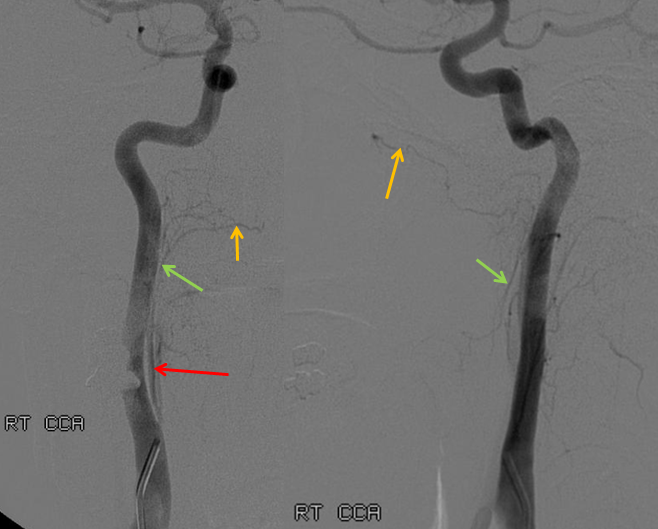
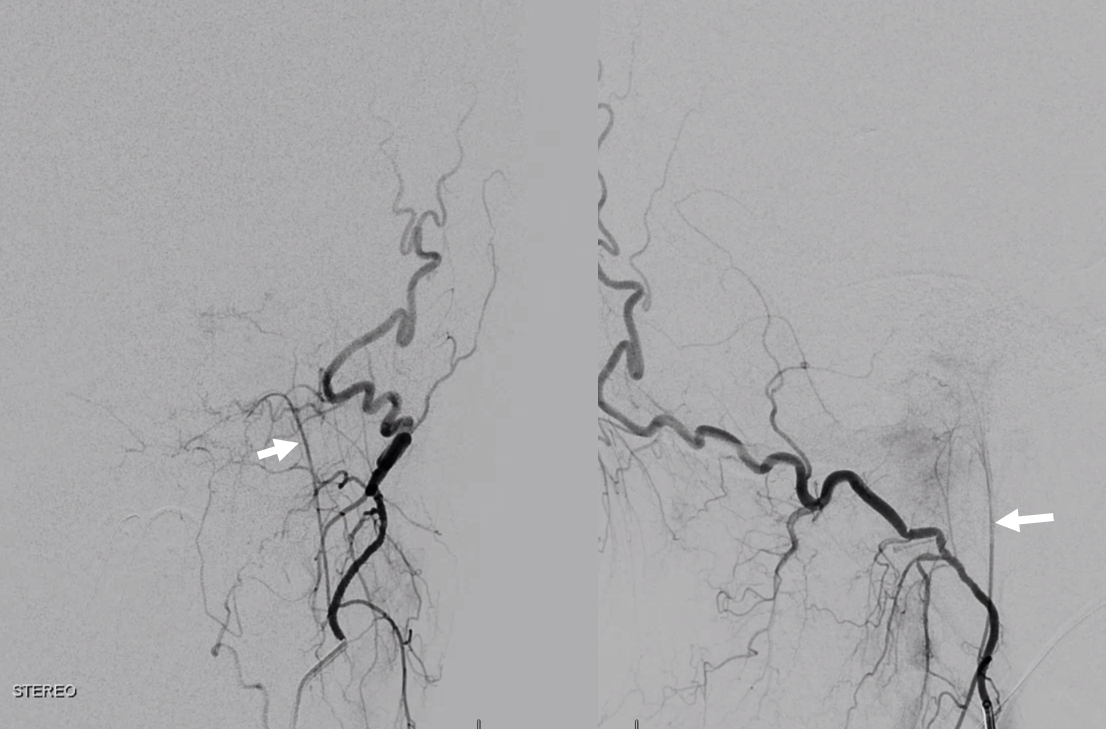
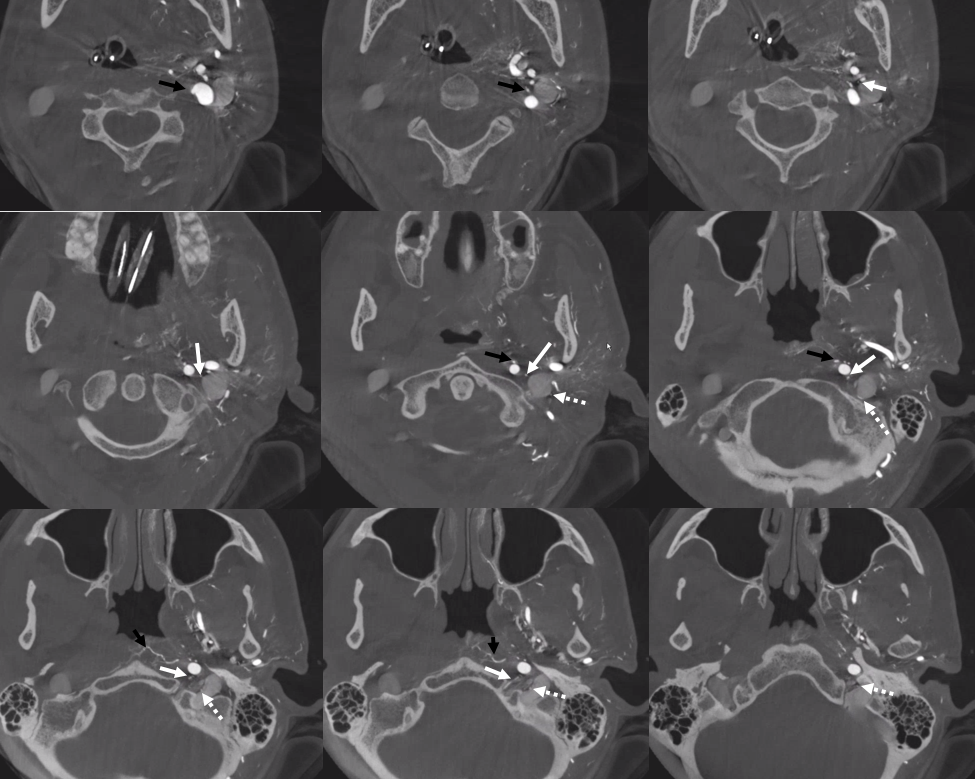
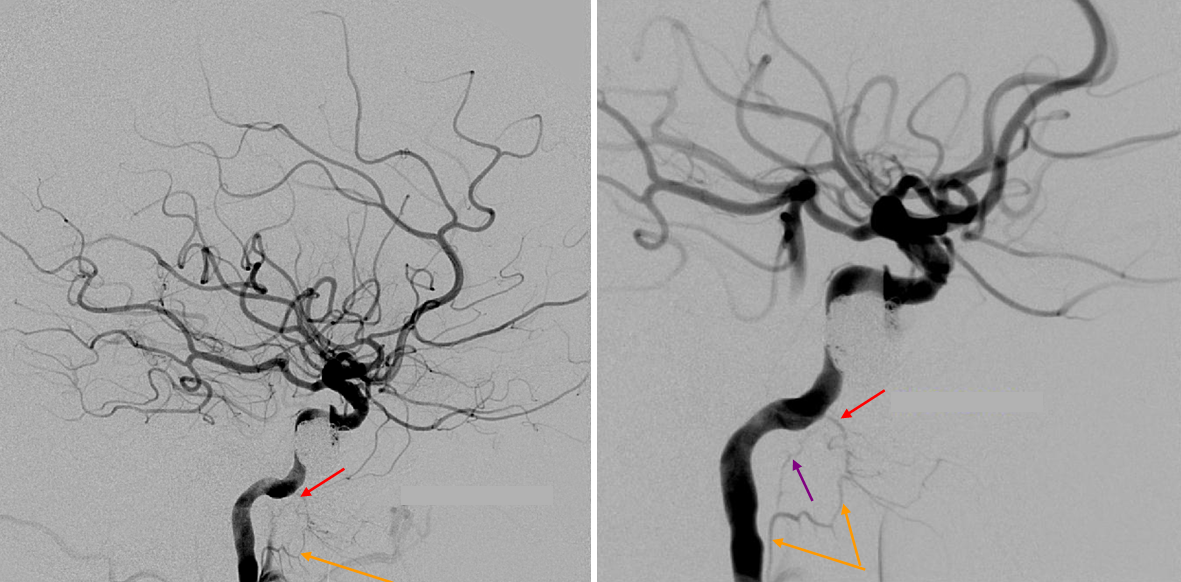
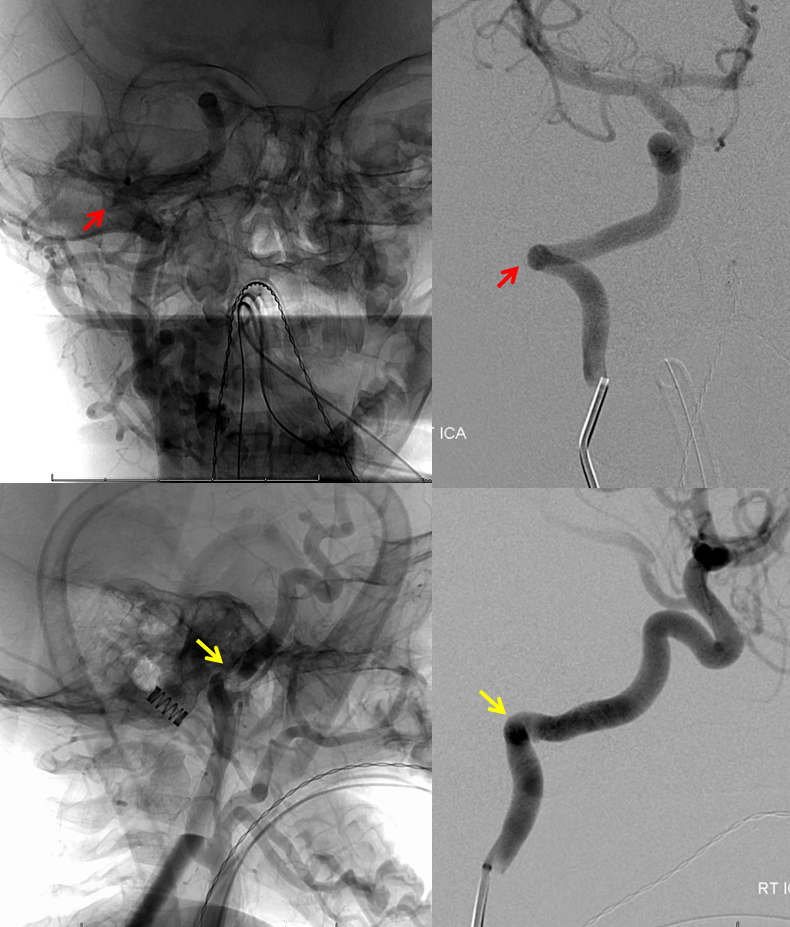
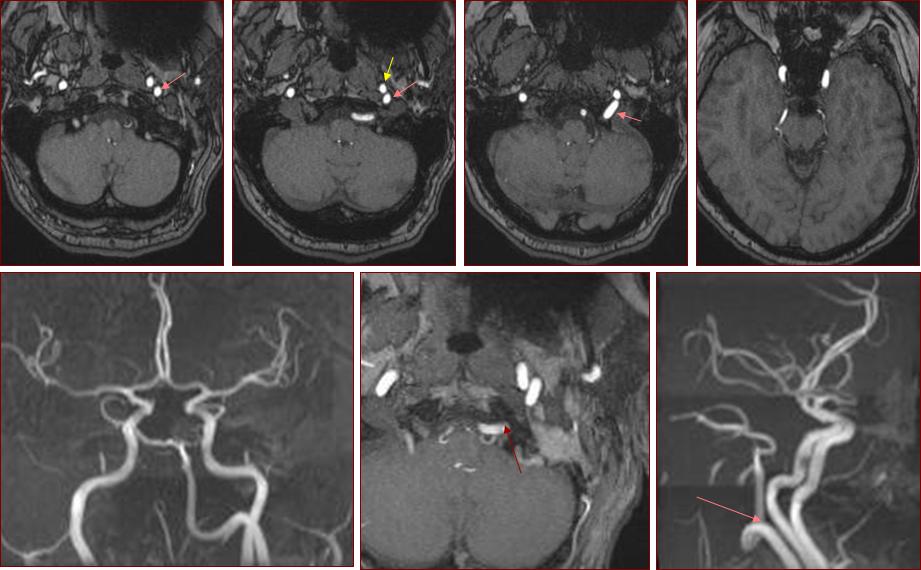
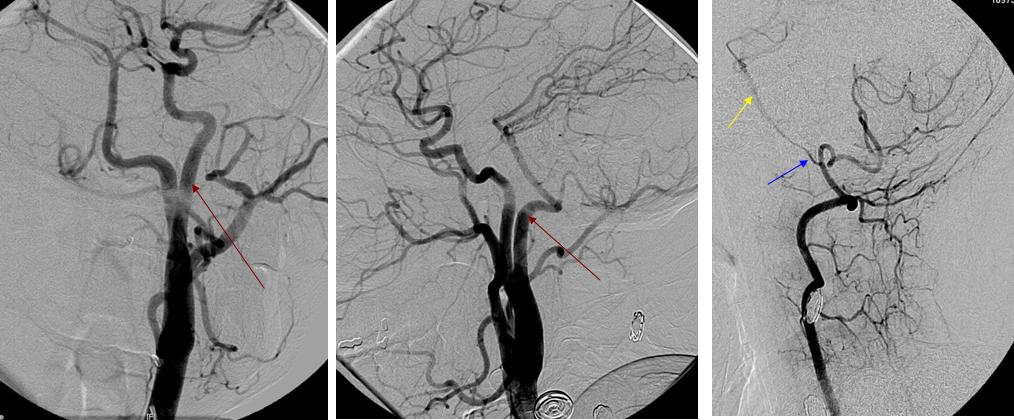
Cross-sectional imaging of disease: At times cross-sectional imaging can show suprisingly detailed information, as in this case of high-grade right distal ICA dissection (pink arrow). The AP artery (red arrow) and its pharyngeal (purple) and neuromeningeal trunks (yellow) are significantly enlarged, while the contralateral AP is normal in caliber (i.e. barely seen). The dissection is only 4 days old.
Pictorial representation overview:
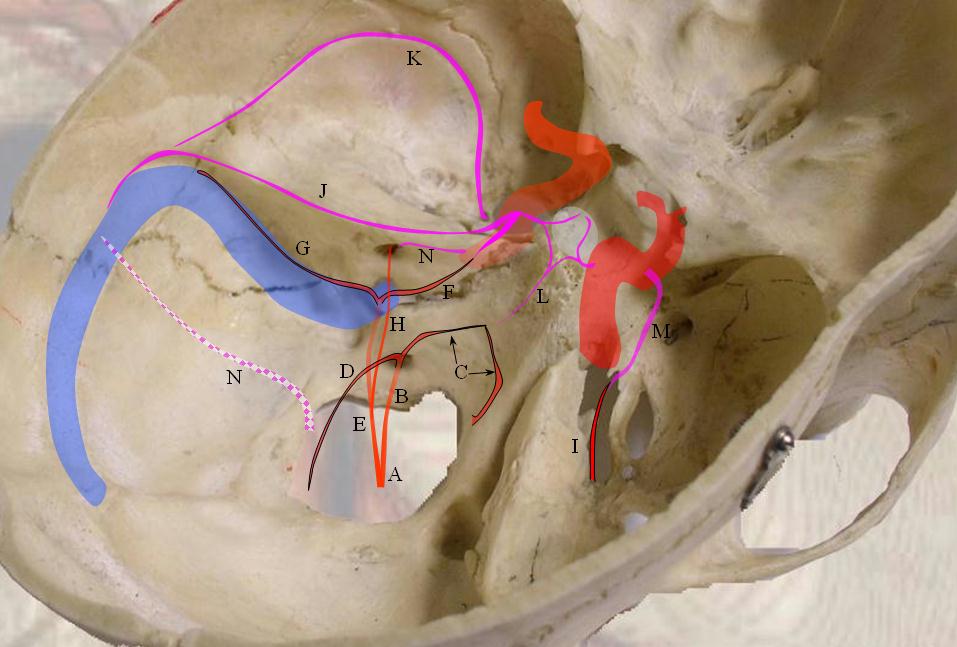
Intracranial Branches of the AP:
A: Neuromeningeal Trunk
B: Hypoglossal Division of the Neuromeningeal Trunk (medial to Jugular divion on the AP view), which typically supplies:
C: Ascending clival branches which anastomose with each other and with inferior clival branch of MHT (L)
D: Descending branch exiting thru foramen magnum and anastomosing at C3 with vertebral branches (odontoid arcade)
E: Jugular Division of the Neuromeningeal Trunk, which typically supplies:
F: Anterior branches anastomosing with lateral clival branches of the ILT near Dorello’s canal
G: Sigmoid Sinus branch along Sigmoid Sinus wall, anastomosing with petrosquamosal branches of the MMA (J),
Lateral Tentorial Artery of the MHT, and Occipital Artery transosseous branches (N)
H: Inferior tympanic branch, supplying middle ear and anastomosing with carotidotympanic branch (N) of the ICA (see aberrant carotid artery below)
I: Foramen Lacerum branch of the pharyngeal division of AP, anastomosing with recurrent lacerum branch of the ILT (M)
Glue cast imaging of the AP — How about an-BCA injection to improve visualization of the AP on a noncontrast head CT? A number of years ago this patient underwent an aggressive n-BCA embolization of an occipital region dural fistula. A generous cast of the left AP and right occipital arteries was produced.
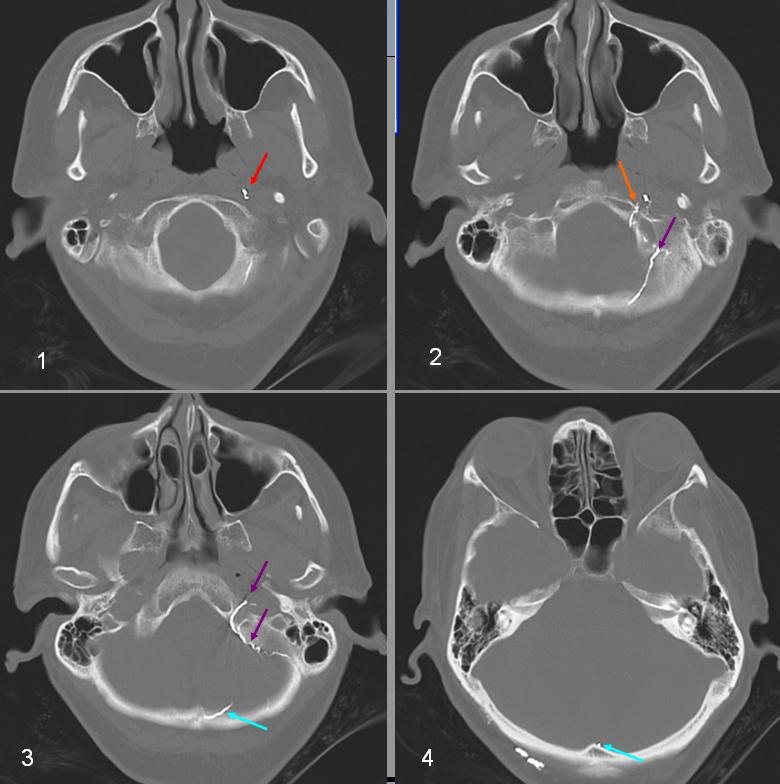
n-BCA cast. Inferior to Superior is 1 through 4. Injection of NBCA with glue cast outlining the neuromeningeal trunk (red), the hypoglossal (orange) and jugular (purple) divisions of the AP artery with glue cast ascending along the sigmoid sinus into the torcular region (blue), typically territory of the posterior meningeal artery. Some glue cast is also present in the right occipital artery on (4)
CATHETER ANGIOGRAPHY 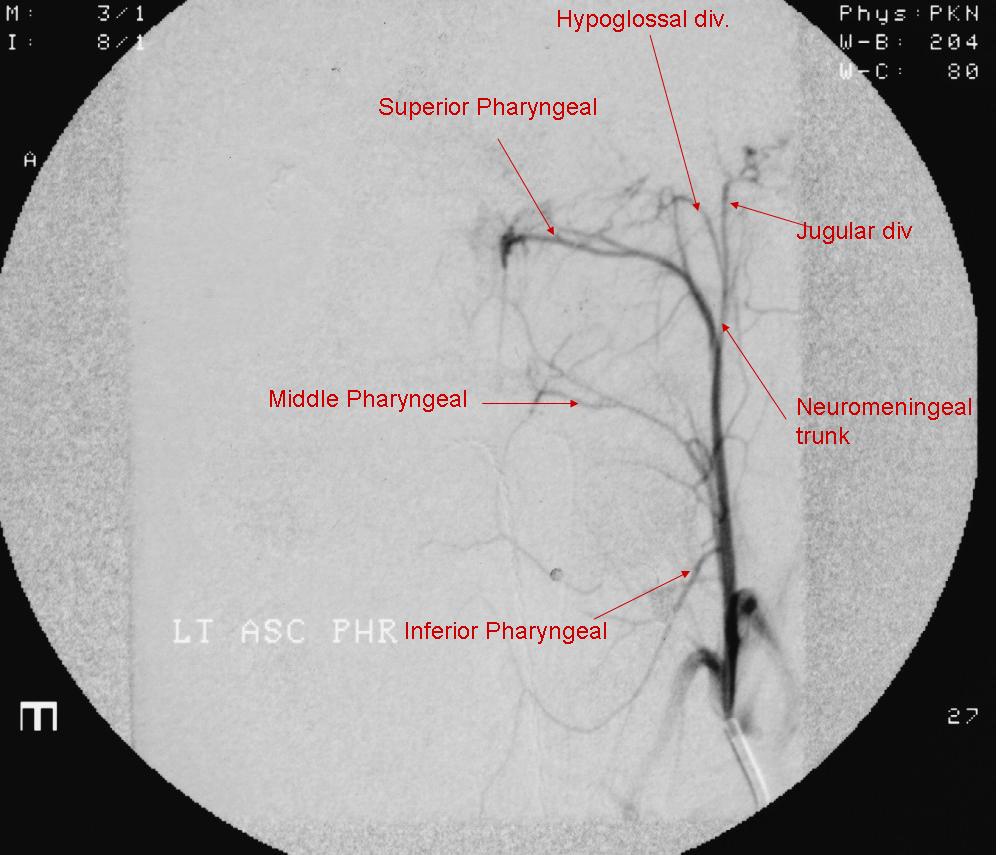
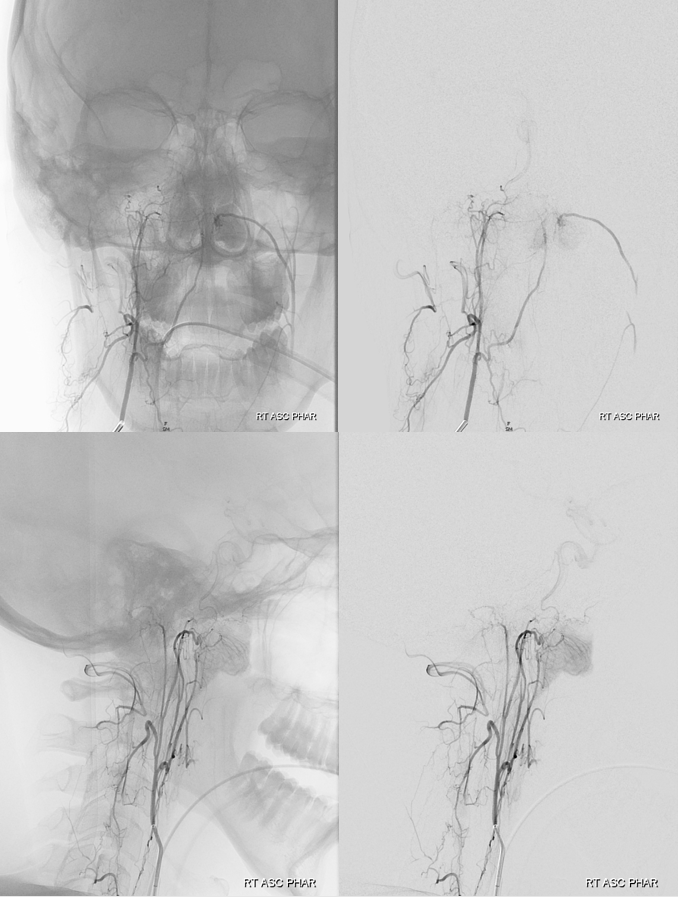
Fronal View, AP artery. The Jugular division branches are lateral to the hypoglossal branches. The latter run towards the midline, ascending along the dorsum of the clivus. All three pharyngeal branches are clearly visible, a classic arrangement which is not seen very often as there is great variability in extent to which the various pharyngeal arteries are developed.

Movie of particularly large posterior meningeal branch — coursing through walls of sigmoid and transverse sinuses and straight sinus! Connections are everywhere…
Separate Origins of Neuromeningeal and Pharyngeal Trunks — another example
In this patient however the pharyngeal trunk (yellow) and the neuromeningeal trunk (red) arise separately from the occipital artery — probably reflecting different embyologic origins of the two trunks.

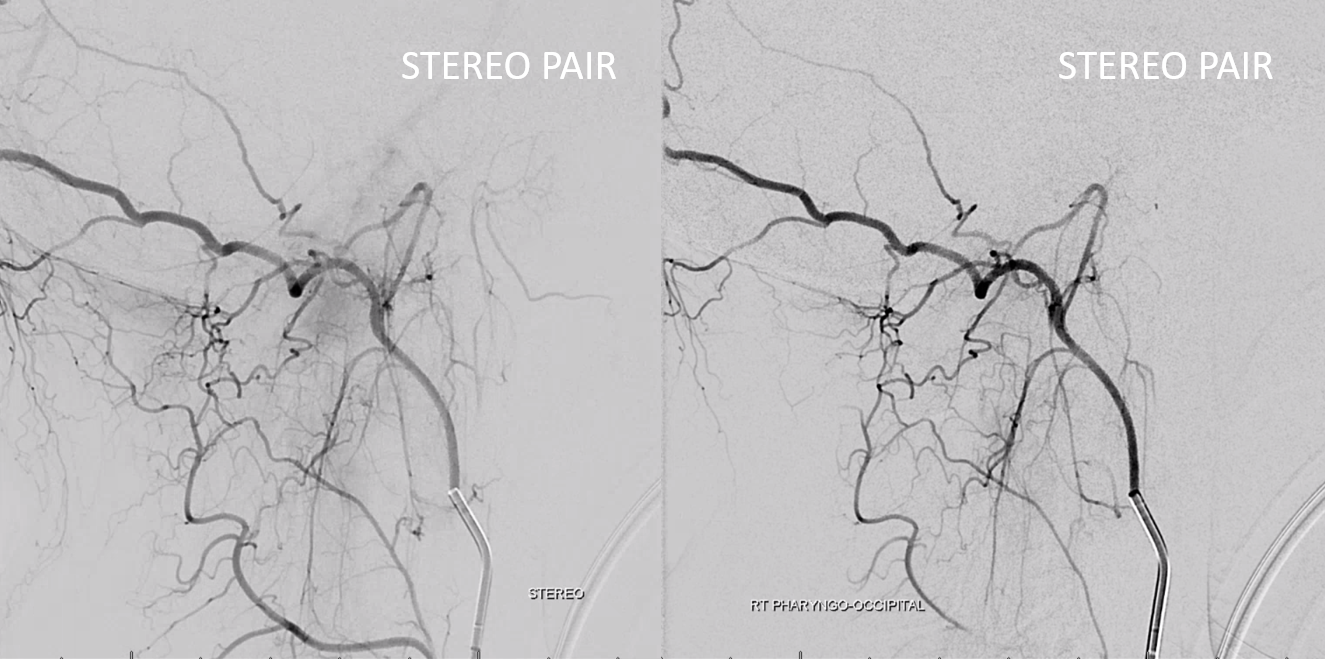
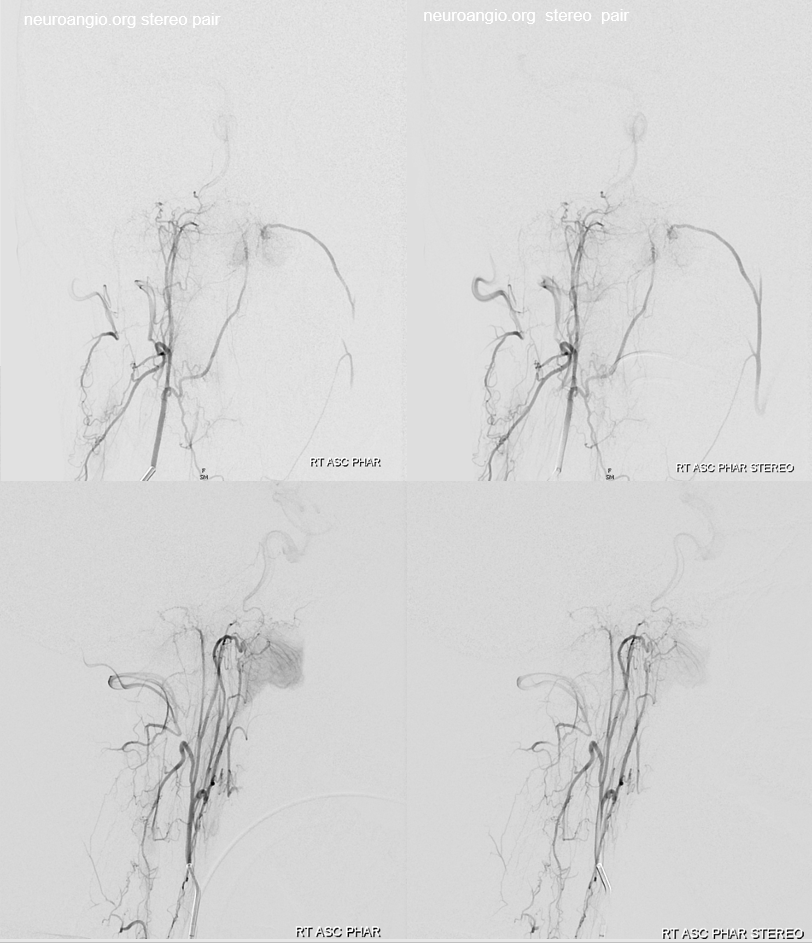
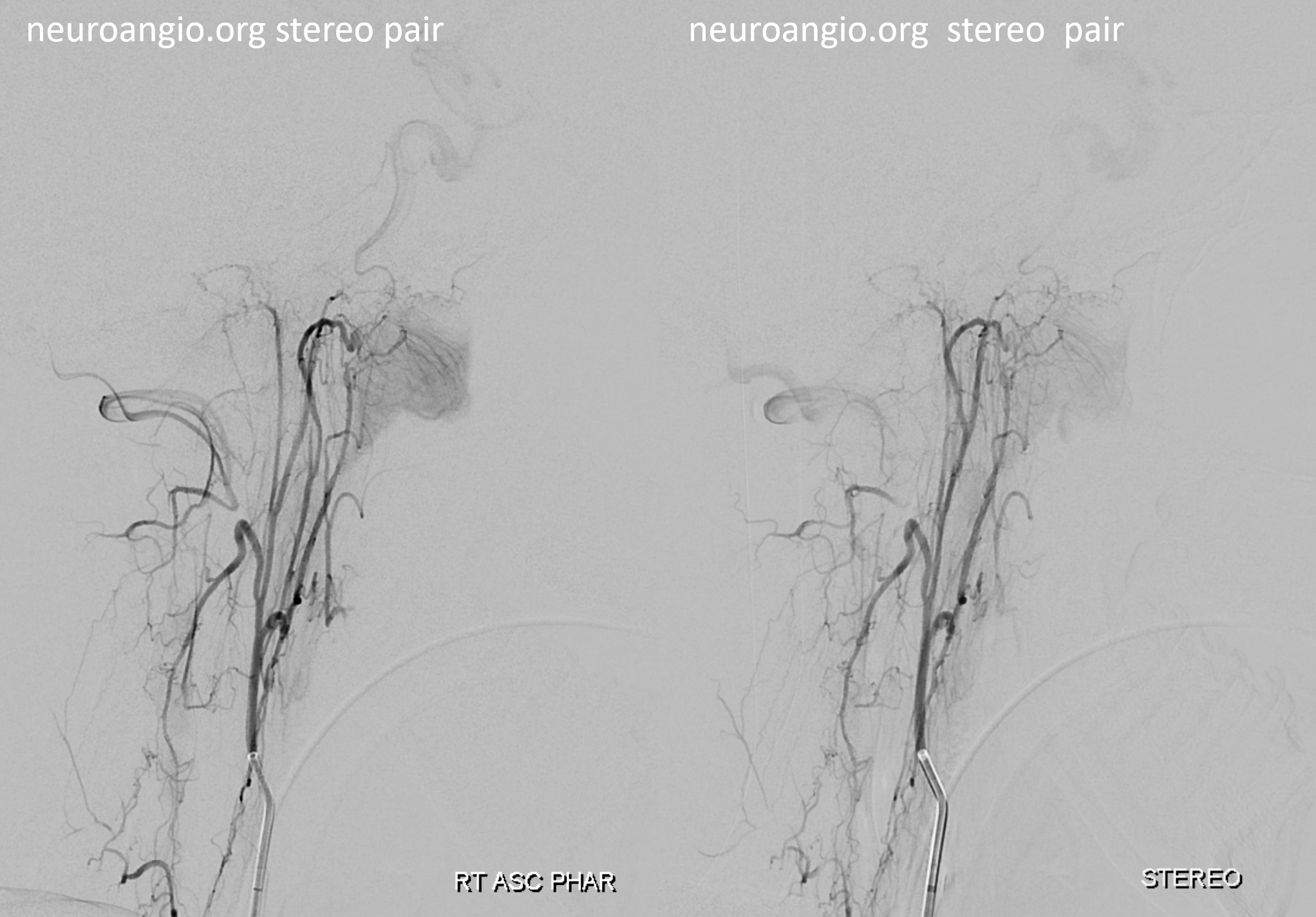
Stereo views

Movie of DYNA CT — both jugular and hypoglossal divisions are off occipital — supplying posterior fossa meningeal tissues. Nice odontoid arch connection with hypoglossal. You can scroll through individual movie frames.
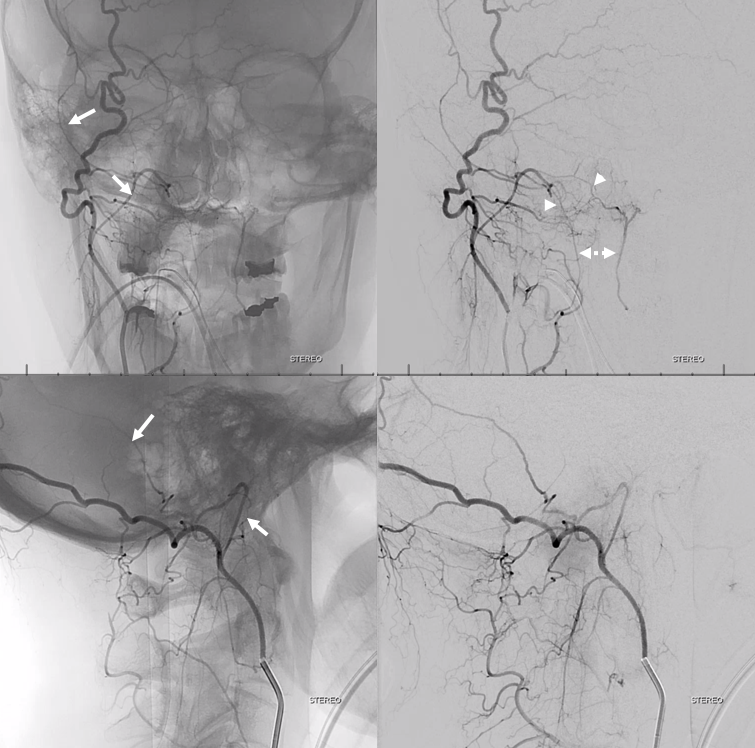
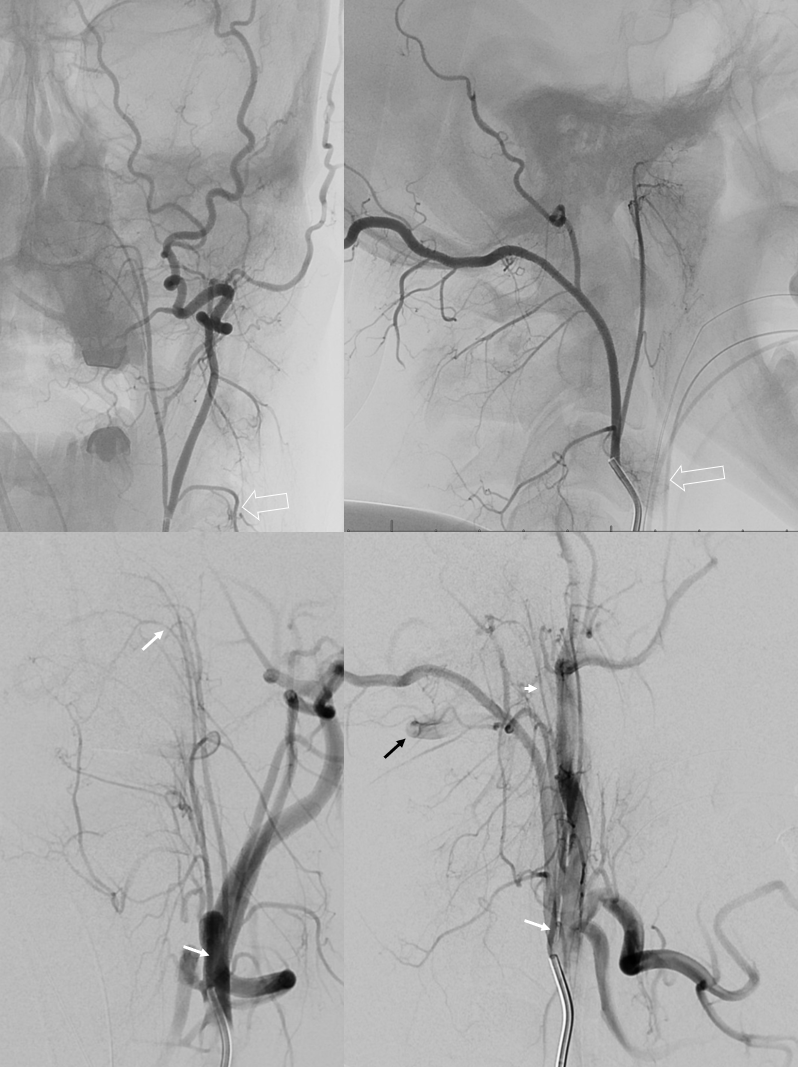
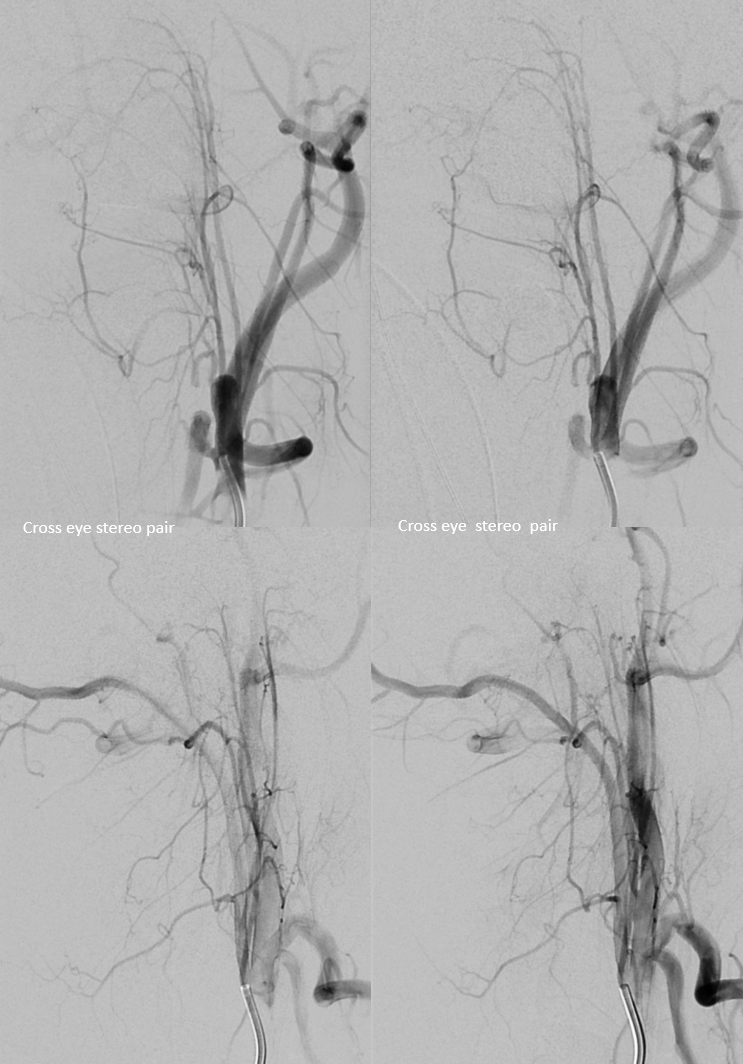
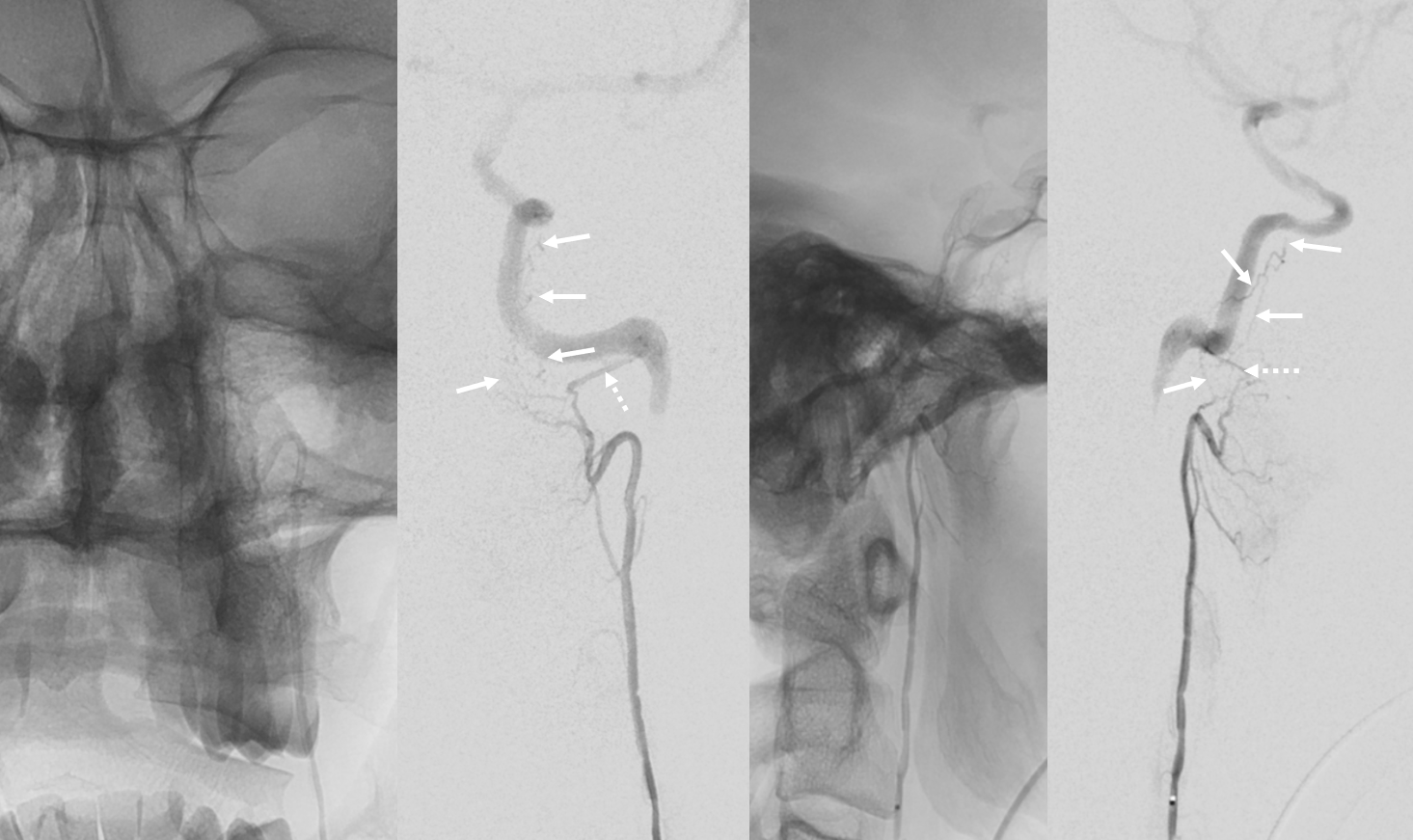
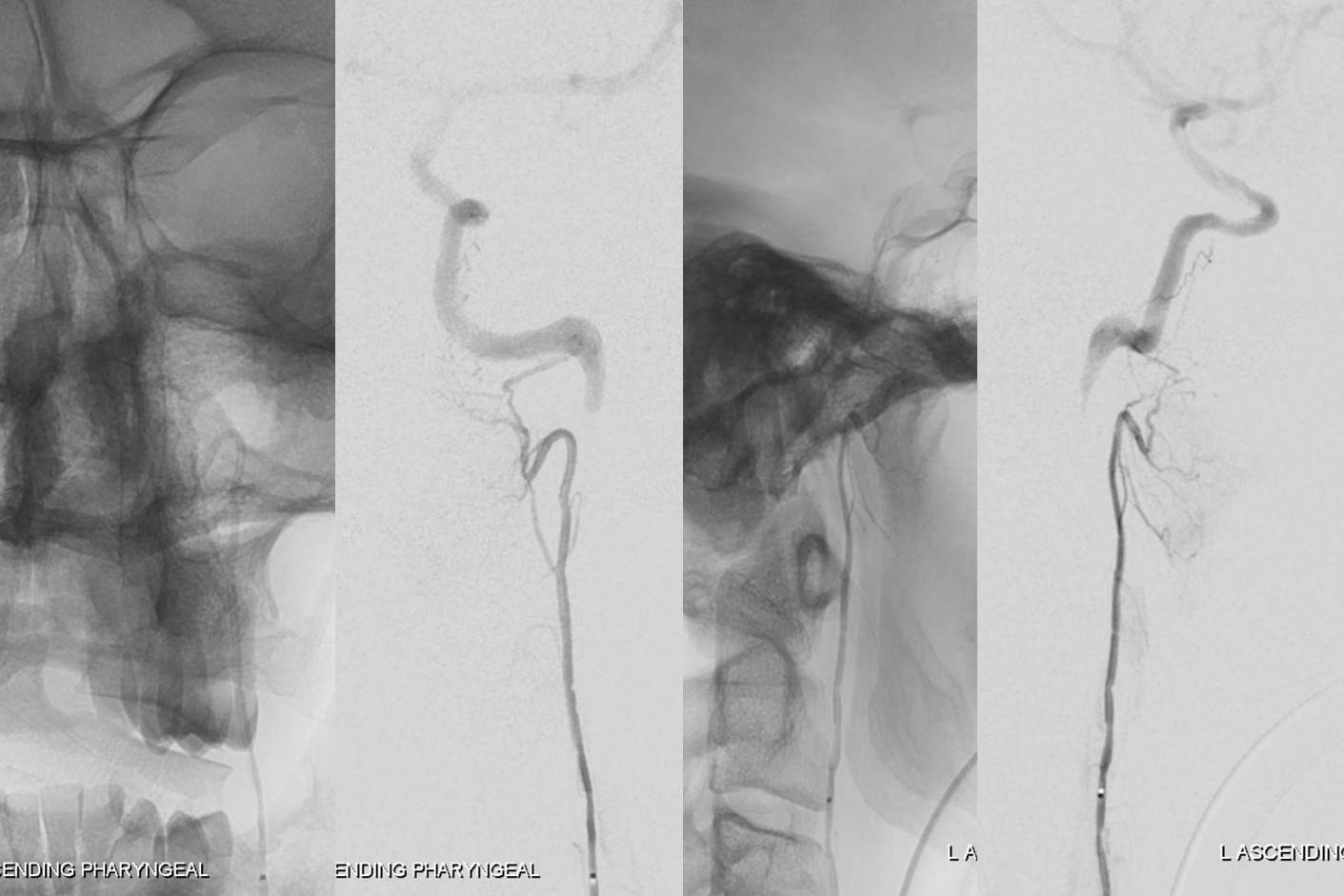
Pharyngo-occipital split variant
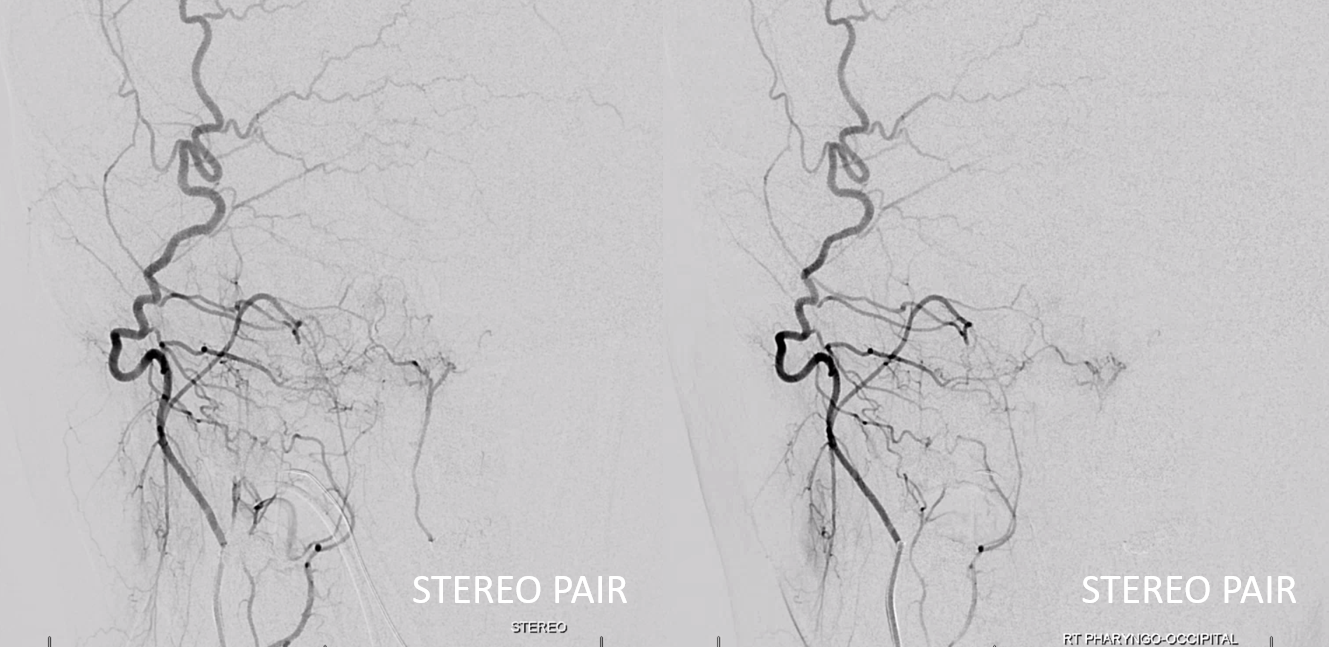
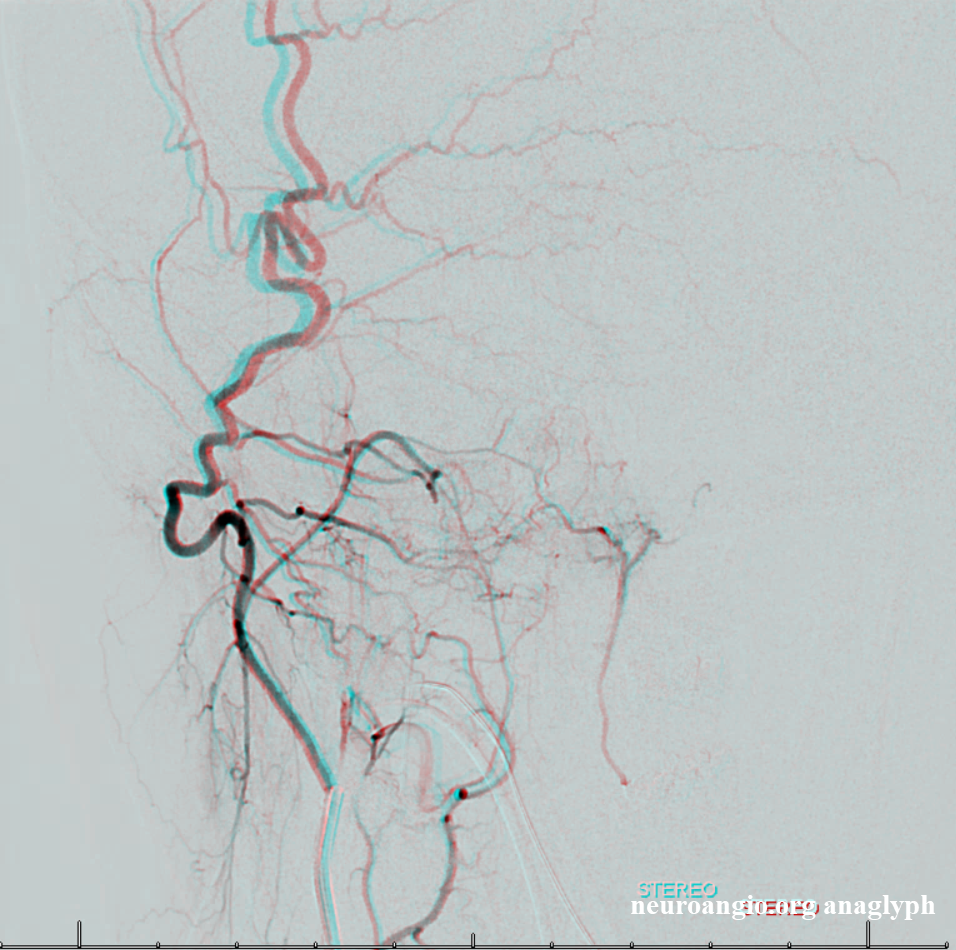
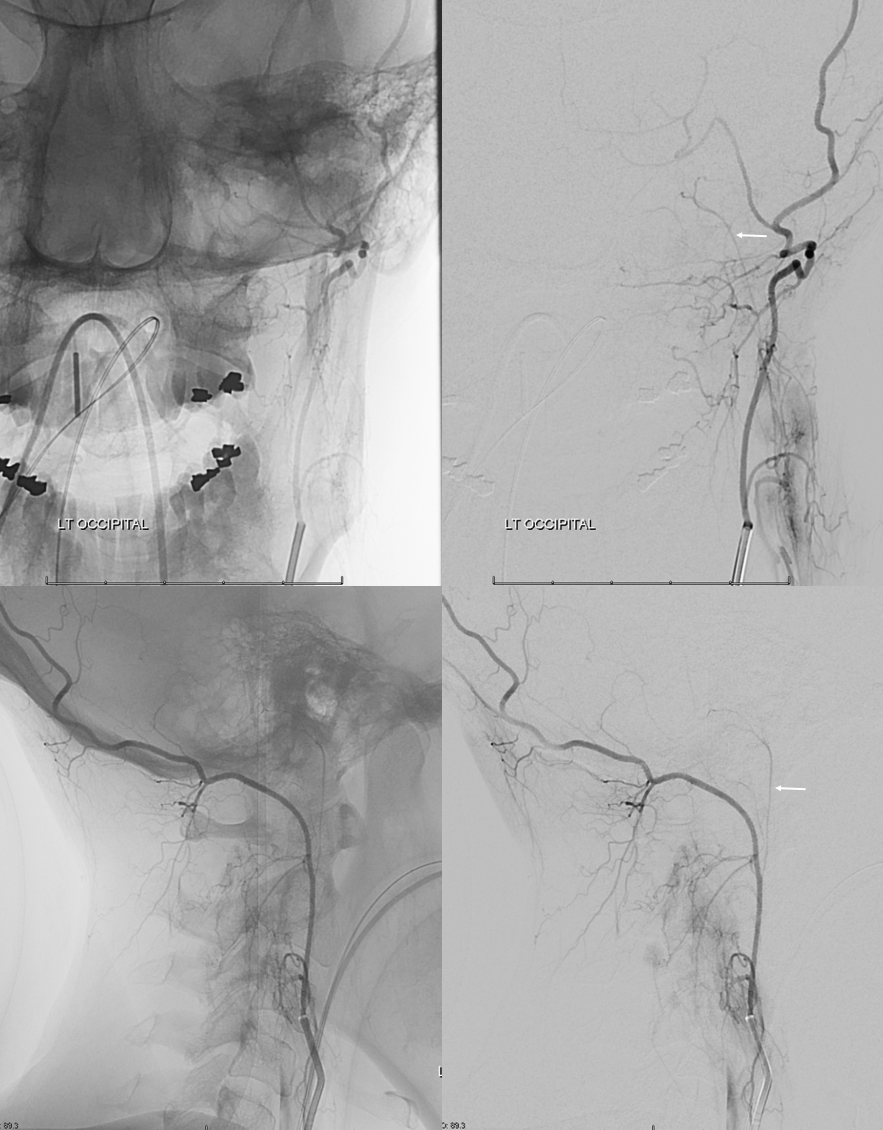
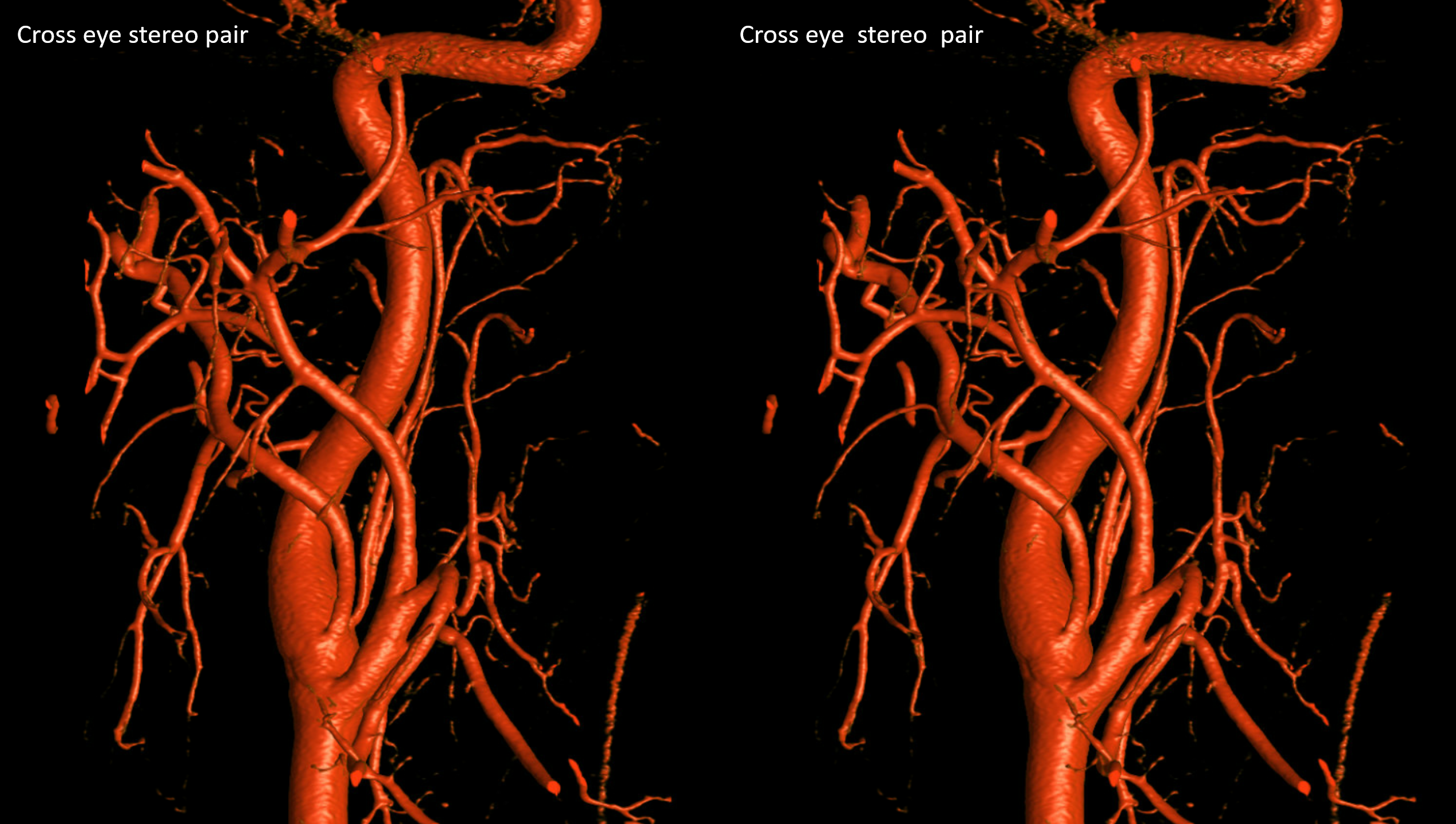
Just a name i gave it. There is no name for all these variants. Just shows that life does not read our books… Here, the “pharyngo-occipital” only supplies the pharyngeal trunk (top images). The neuromeningeal trunk (white arrows) comes off more proximally, at takeoff of the occipital (bottom images). Notice that it is the neuromeningeal trunk and not occipital that opacifies the vertebral artery (black arrow). Also present is fairly rare supply by the proximal pharyngeal trunk of the submandibular gland (open white arrow)
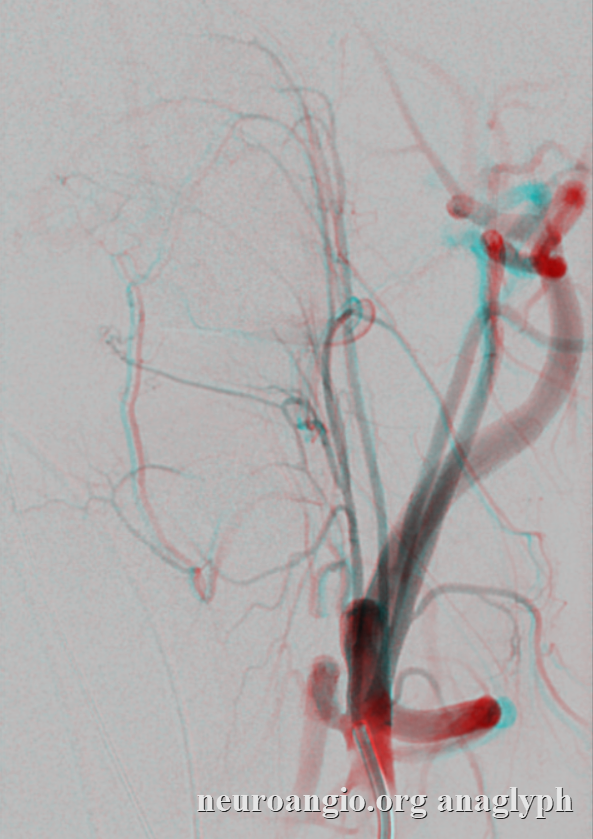
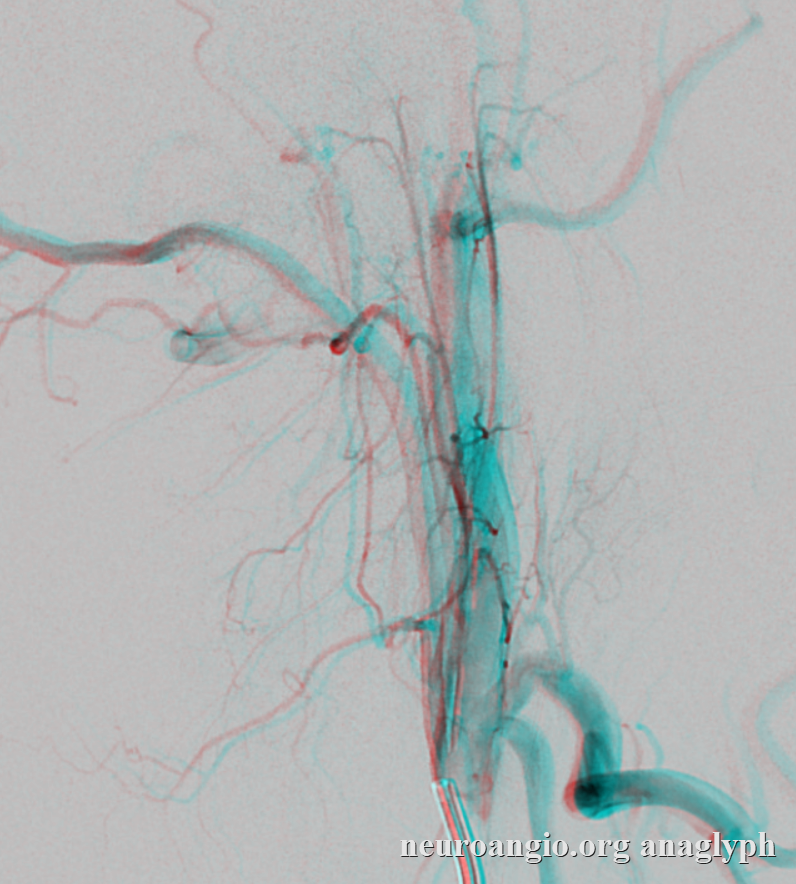
Stereos
Anaglyphs
AP pharyngeal origin off ICA

Again, this relatively rare variant attests to separate embryologic origins of the pharyngeal and neuromeningeal trunks (as may be predicted given very different territory). The pharyngeal trunk (red) originates from the proximal ICA, giving off a small inferior (orange) and larger superior (yellow) pharyngeal branches. The neuromeningeal trunk (purple) is opacified from the ipsilateral ECA injection via a pharyngooccipital trunk. See “aberrant carotid artery” section below.
Another case of the same, also opacifying the nasal septal branch (yellow) via the sphenopalatine anastomosis from the superior pharyngeal division (green)
One more example of how nature does not read books — in this case, all three major parts — pharyngeal, jugular, and hypoglossal originate separately.
The pharyngeal division comes off the proximal ICA (unlabeled)
The hypoglossal division (white arrow) comes off separately from the occipital artery. The jugular division is not really seen here
It takes a DYNA to see the jugular division (dashed white arrows) originating from the distal occipital artery — well beyond the area we might be looking for a dangerous anastomosis. The pharyngeal is black arrow, and dominant hypoglossal division is white arrows
Yet one more example — just to underscore how variable the supply to jugular and hypoglossal areas is, variable origins of ascending pharyngeal components, etc.

Occipital injection with “neuromeningeal trunk” (arrow) supply to jugular and hypoglossal regions
Occipital and AP origins from ICA
Variability is truly endless — and one can only take embryologic theories so far. Here, both occipital and ascending pharyngeal arteries originate from the ICA, separately. Go figure. Stereo pair below
Anaglyph stereo

Superior Pharyngeal Division Mandibulovidian Collaterals
Two lateral views of internal carotid injection demonstrating a mandibulovidian artery (red) collateralizing with superior division of the ascending pharyngeal (orange). The foramen lacerum branch (purple) is also visible.
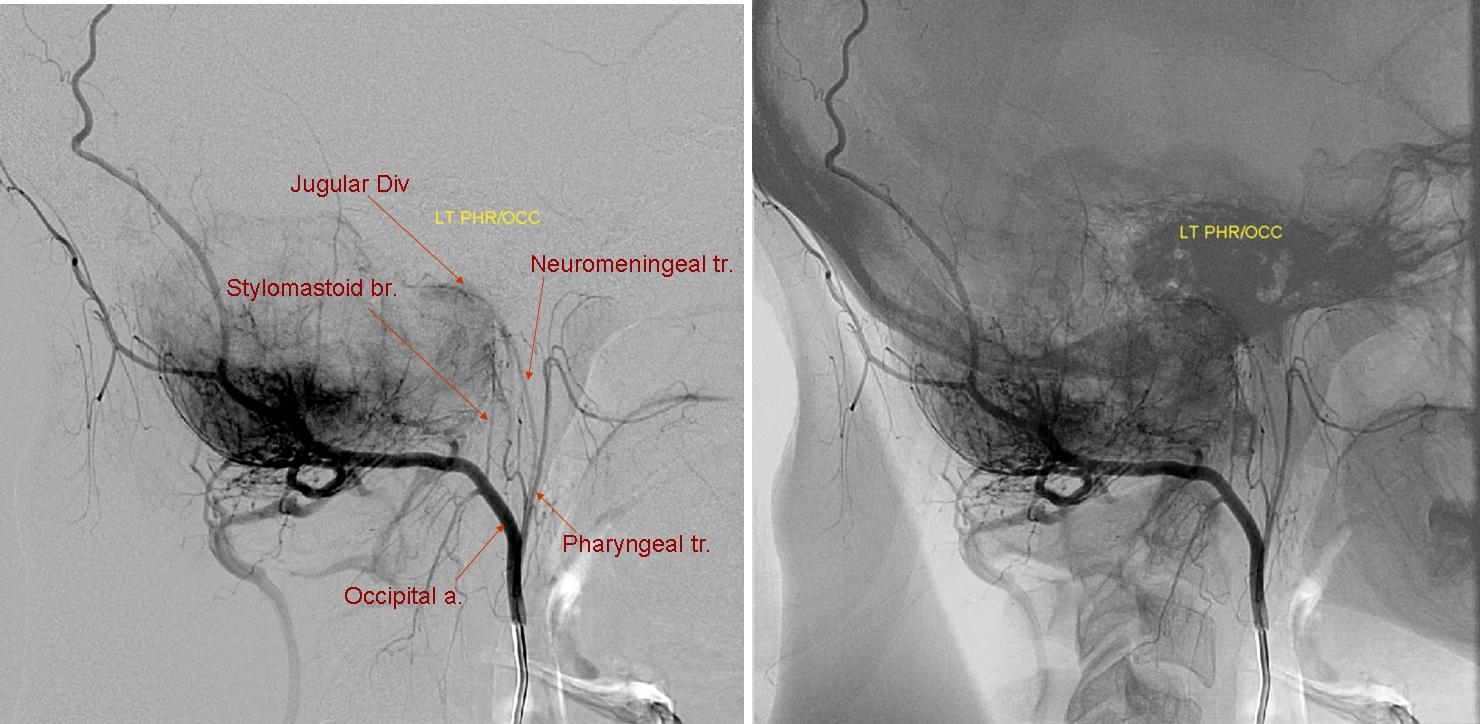
Lateral angiogram in case of a skull base tumor, showing a common pharyngooccipital trunk. The Stylomastoid branch of the occipital artery, which often supplies portions of the facial nerve, is well seen. Particle embolization of the tumor should be carried out from a position distal to this vessel.
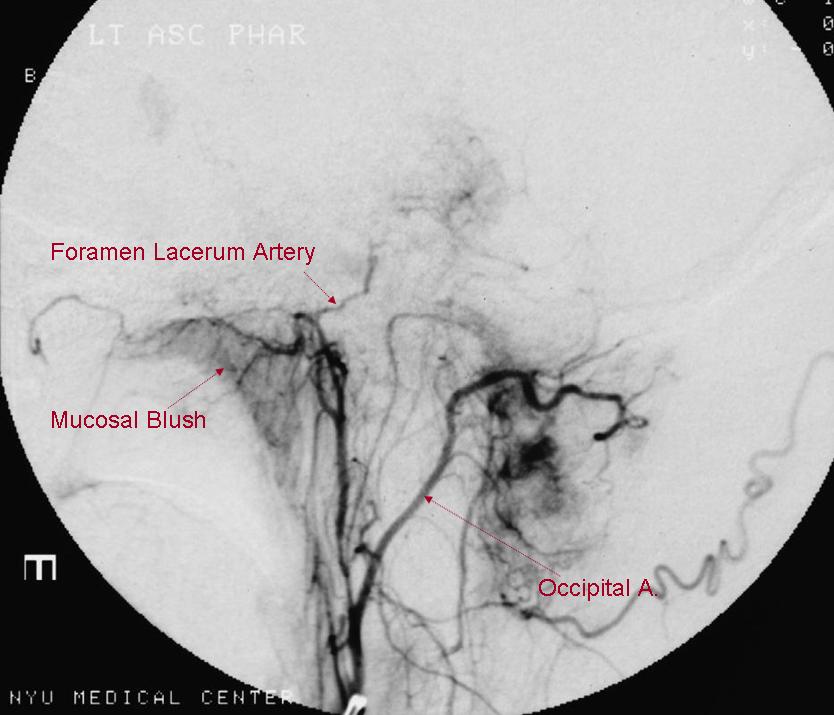
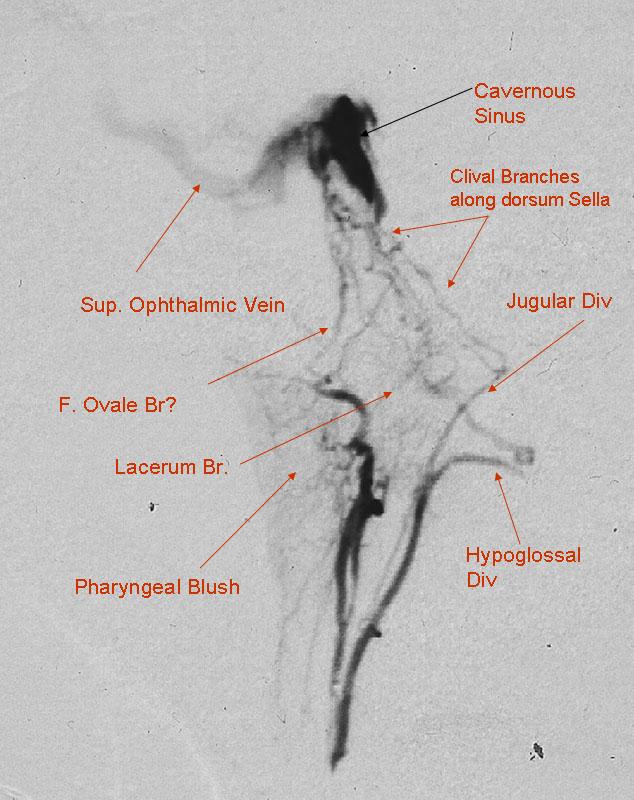
Lateral view, pharyngo-occipital trunk. The AP and occipital artery have a common origin. A prominent pharyngeal mucosal blush is often present on injection of the pharyngeal branch. A hypertrophied foramen lacerum artery vascularizes a meningioma. This vessel can be a convenient route for embolization as there is no cranial nerve associated with foramen lacerum. Foramen Lacerum branch arises from the superior pharyngeal branch and enters the skull alongside the carotid artery. Can collateralize with the vidian branch of the carotid.
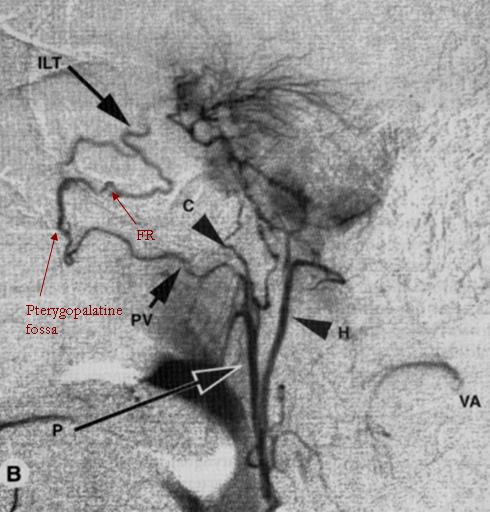
This remarkable lateral angiogram demonstrates multiple extracranial-to-intracranial anastomoses of the pharyngeal division. A pterygovaginal (Vidian) anastomosis of the AP artery leading to the pterygopalatine fossa, from where the artery of foramen rotundum (FR) re-enters the cranium to supply a meningioma and collateralizes with the Inferolateral trunk of the cavernous ICA. The carotid branch (C) a.k.a. artery of foramen lacerum is also nicely visible. The hypoglossal division (H) contributes extensively to supply of the meningioma. Muscular collaterals to the vertebral artery are also present (VA) Image taken from Lasjaunias and Berenstein, first edition.
Carotid Branch
Rarely seen. Connects the superior division of the pharyngeal trunk to the ICA, running in the FORAMEN LACERUM / CAROTID CANAL to join the ILT (arrows). The lacerum / carotid canal course is key. Much more frequently, the superior division of pharyngeal trunk connects with the ICA via the vidian branch (dashed arrows). This is NOT the carotid branch, although it is frequently mistaken for it. On 2D-DSA, the characteristic thing about the carotid branch is that it really runs parallel to the ICA, just below it. Best seen though on Cone Beam CT — definitively in the carotid canal etc. Most commonly seen as a collateral in cervical ICA occlusion, as in case below. Even for a rarely seen branch such as this, there is really a network rather than single vessel — best seen in frontal view. Underscores how much more there is than seen by the eye
without arrows
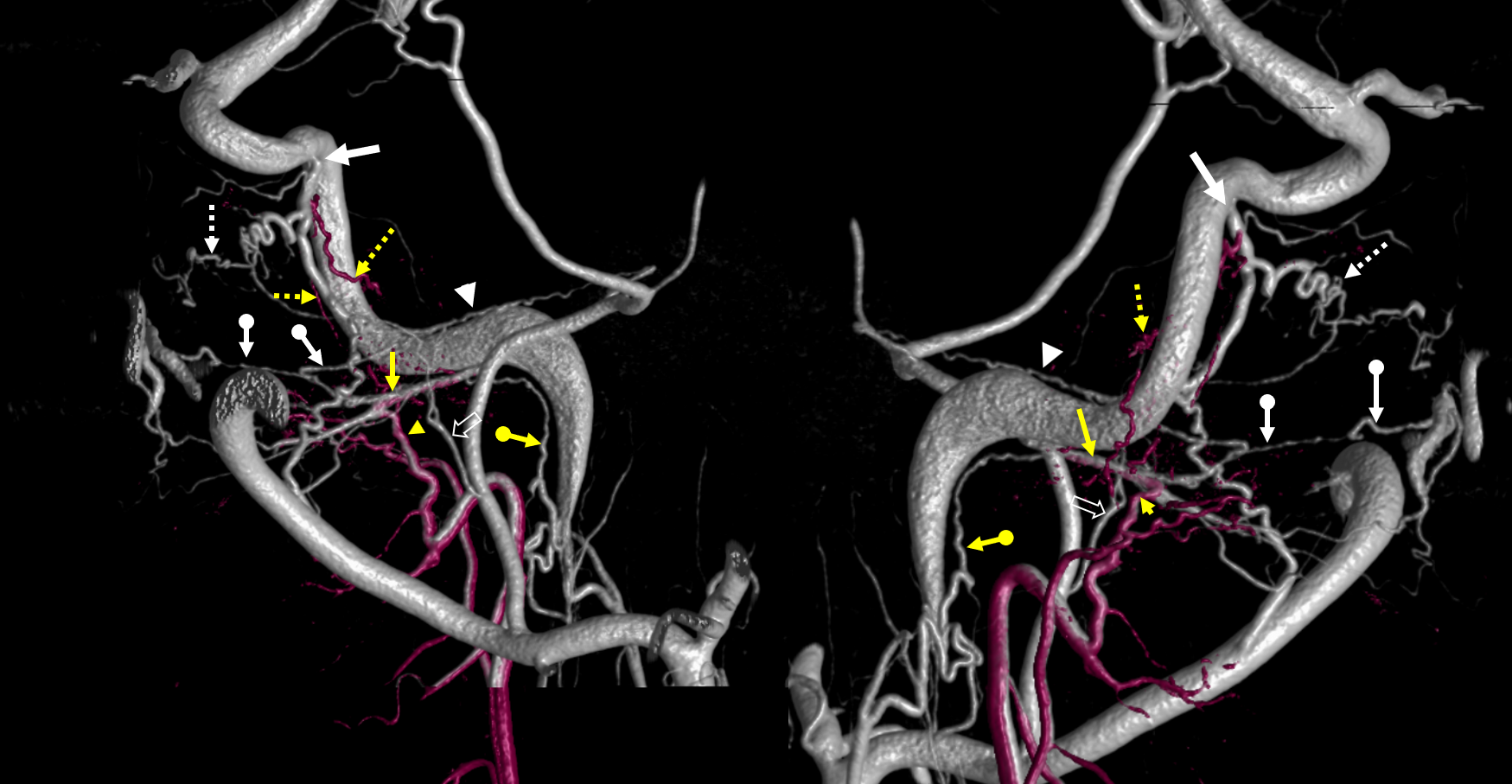
Cone beam fusion of pharyngeal division hand injection (purple) and ECA global injection. Superior division AP = yellow arrowheads; vidian = yellow arrows; Carotid AP branches = dashed yellow arrows; ILT = white arrow; Foramen rotundum branches = dashed white arrows; palatovaginal / pterygovaginal = ball white arrows; neuromeningeal trunk lacerum anastomosis with the vidian = ball yellow arrows; cavernous branch of the MMA = white arrowheads; Accessory Meningeal = white open arrows
Stereos

Cone Beam CT axial MIP — Pharyngeal division micro – Siemens ICONO 10 second dual volume non-binned FOV 22, hand injection 100% contrast, with “secondary reconstruction”
Same dataset with fusion of ECA and above AP injections
ECA injection — multiple anastomoses with the ophthalmic artery also
Carotid Branch Supply of Posterior Pituitary
Anything is possible. Here is a carotid occlusion case. The AP carotid branch (arrows) traverses the lacerum, ultimately supplying the posterior hypophysis (the carotid is occluded from cervical bifurcation, and MHT is apparently out our hypoplastic also). Note optic nerve network (black oval) that is often prominent when ICA is closed
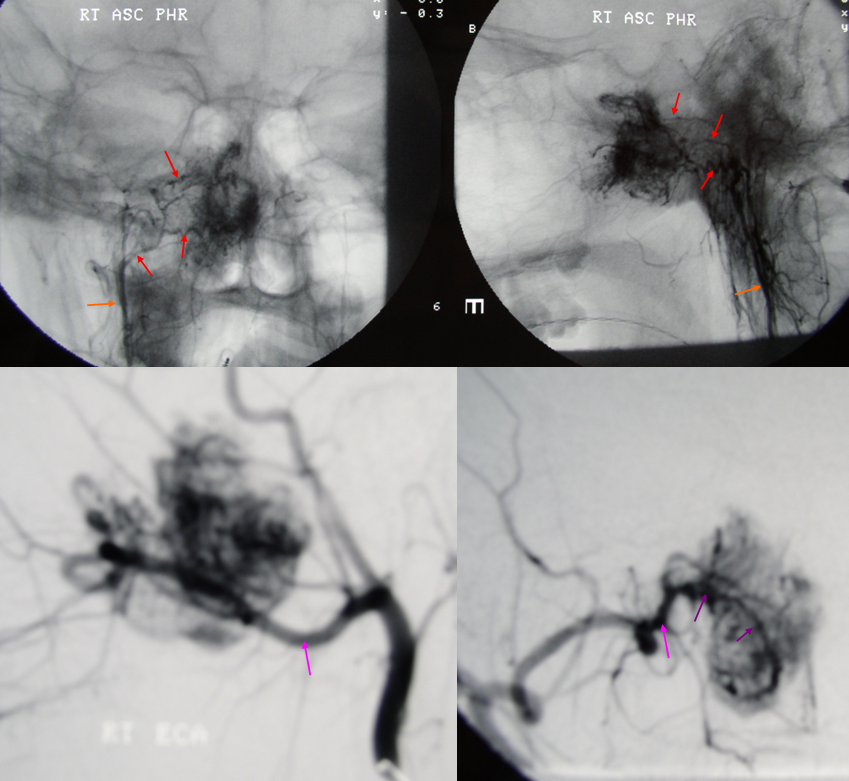
Ascending pharyngeal and vidian artery supply of Juvenile Angiofibroma
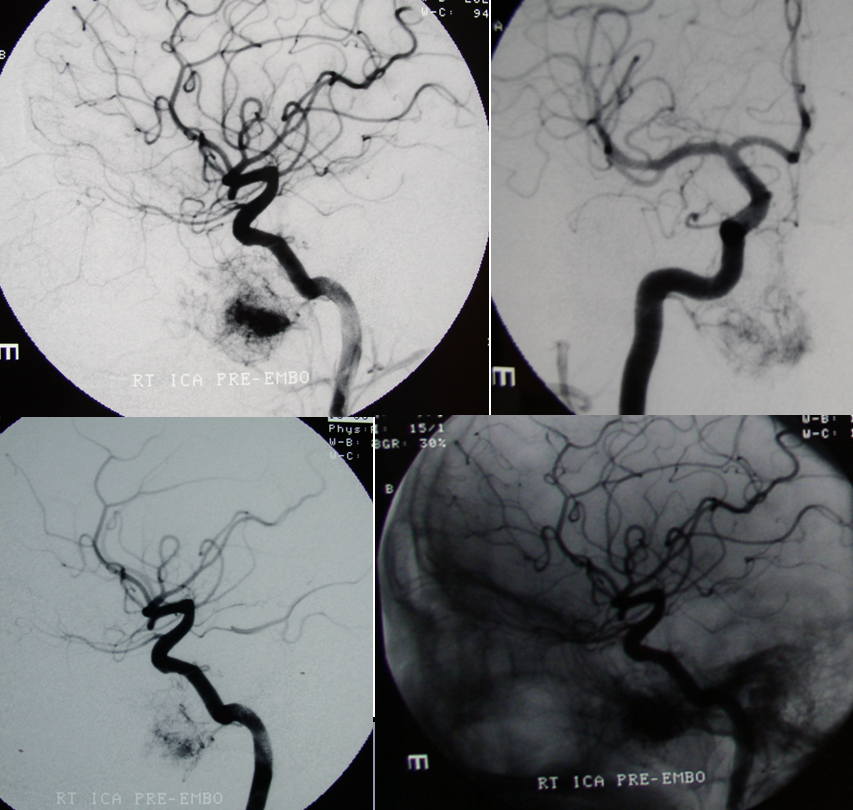
Emergency angiography performed after biopsy of nasopharyngeal mass, a JNA, shows extensive supply from the MV artery. Notice also extensive supply of same tumor via ascending palatine branches (red) from the ascending pharyngeal artery (orange) and sphenopalatine branches (purple) of the IMAX (pink)
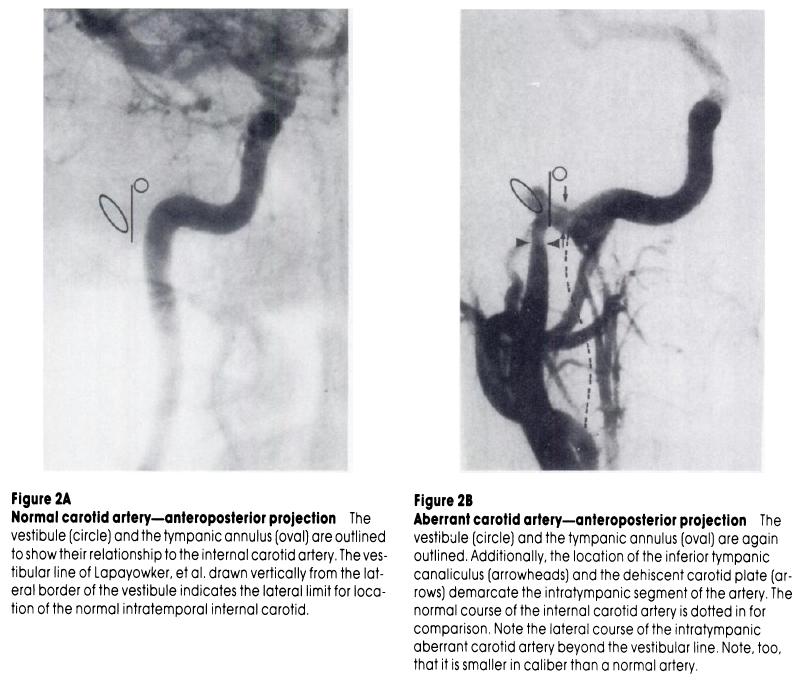
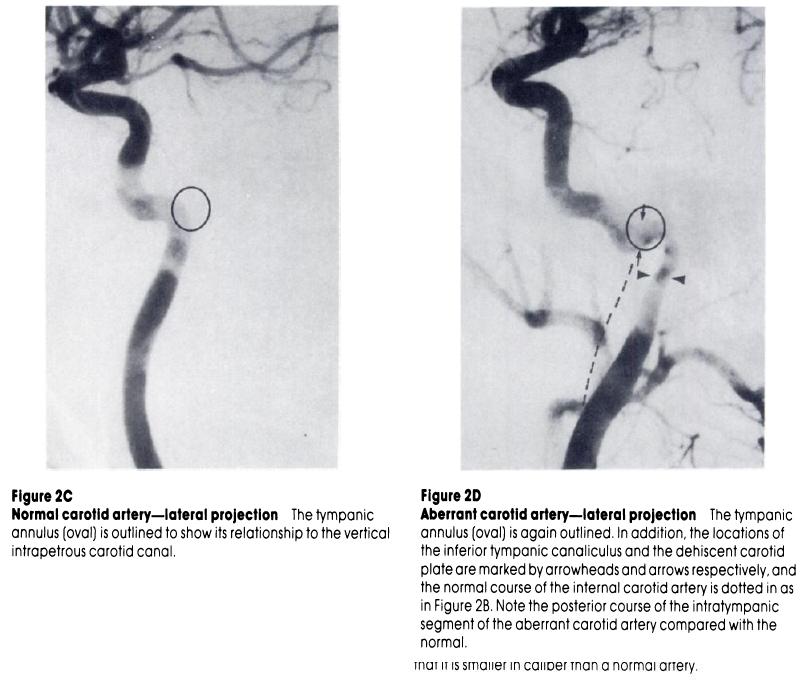
The inferior tympanic branch and aberrant carotid artery
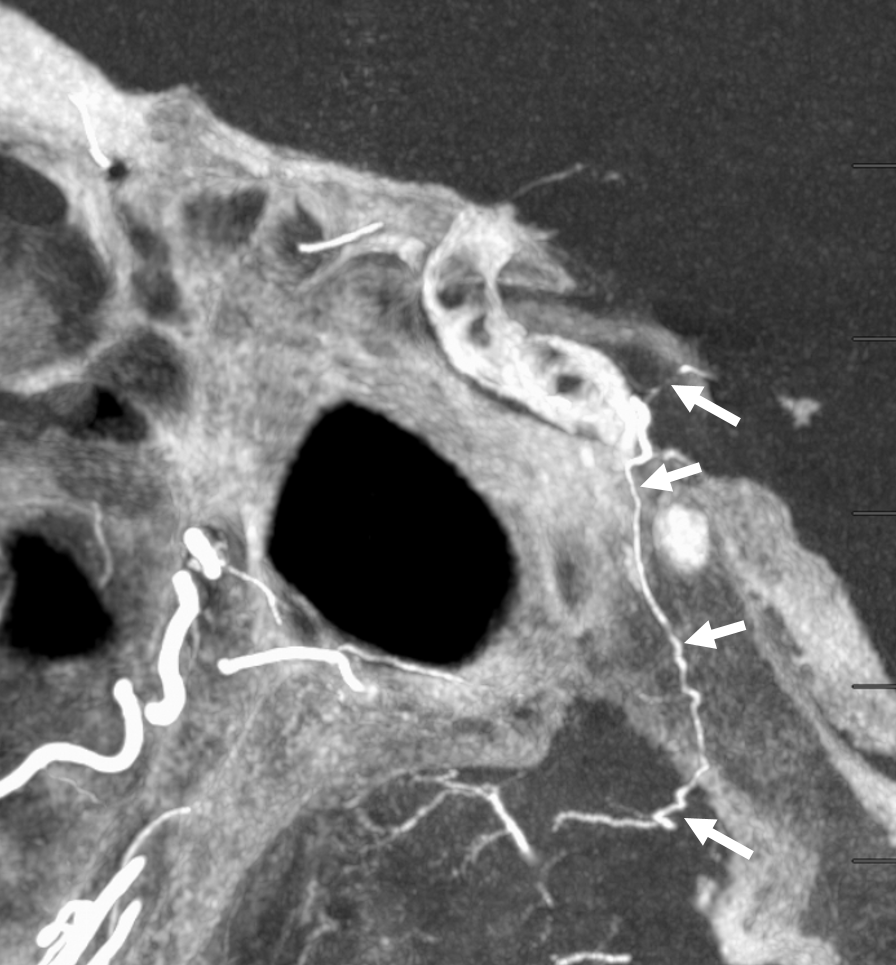
A small but quite important branch can be seen on the lateral projecting between the pharyngeal and neuromeningeal trunks, and supplies the middle ear cavity. In the middle ear, it is in hemodynamic balance with the caroticotympanic branch of the carotid artery (petrous segment), the IAC branch of the AICA, and the posterior tympanic branch of the Posterior Auricular artery. The inferior tympanic branch is important from an embryologic standpoint as it in fact represents the “Aberrant Carotid Artery.” When the cervical portion of the carotid artery fails to develop, the petrous portion is reconstituted via the inferior tympanic-caroticotympanic anastomosis which takes place in the middle ear, which is why the laterally projecting aberrant carotid presents as a vascular middle ear mass. (As an aside, other segments of the internal carotid artery agenesis are similarly reconstituted at a higher level — for example primitive maxillary artery, or reconstitution across the ACOM) The inferior tympanic artery is also important as a source of glomus tympanicum supply.
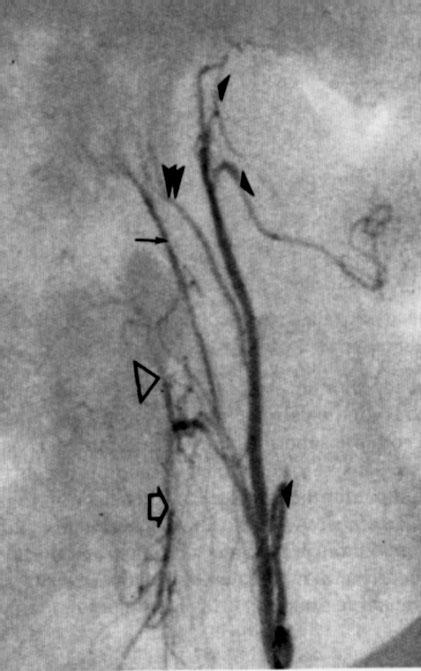
Inferior tympanic branch is labeled with double arrowheads.
Inferior Tympanic branch in setting of multiple meningiomas
The ascending pharyngeal arises from proximal ICA. The inferior tympanic branch (dashed arrows) continues into the carotid canal as the caroticotympanic branch (white arrows). In the venous phase, the tissues drain into the venous plexus surrounding the petrous carotid artery, known as the plexus of Rektorzik (black arrows)

The same branch in the carotid canal is opacified via injection of the external carotid artery (DYNA CT images, white arrows). Notice also a faintly seen artery of the facial nerve (black arrows)

Inferior tympanic branch in a patient with parietooccipital meningioma. Posterior meningeal artery origin from jugular division of the ascending pharyngeal artery. The inferior tympanic branch projects over the auditory canal, and follows the expected course of the aberrant carotid artery.
Neuromeningeal trunk=red; Jugular division=orange; posterior meningeal artery=purple; inferior tympanic artery=blue; meningioma blush = yellow
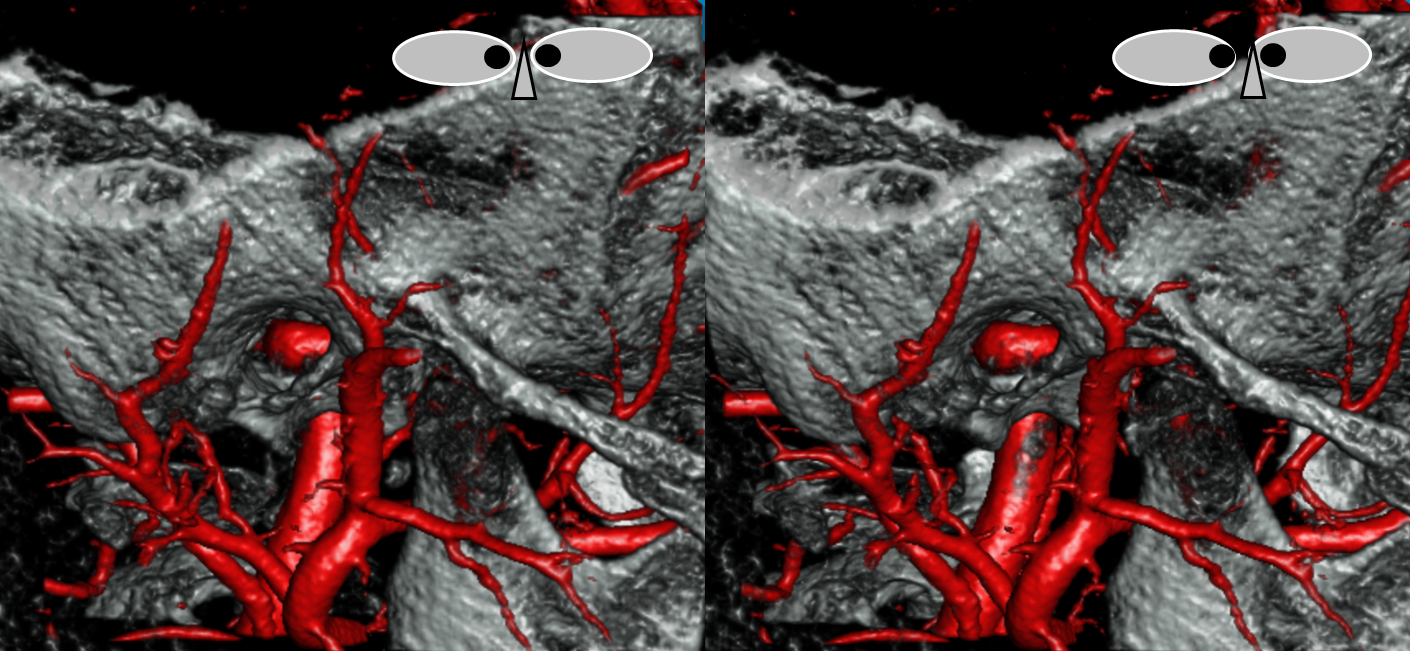
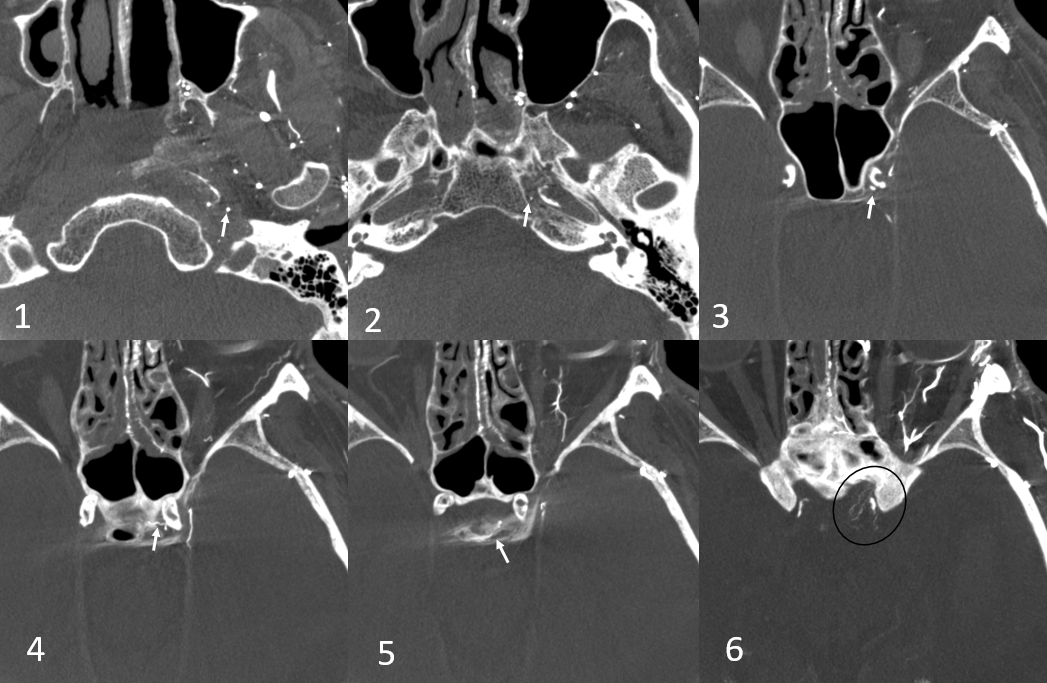
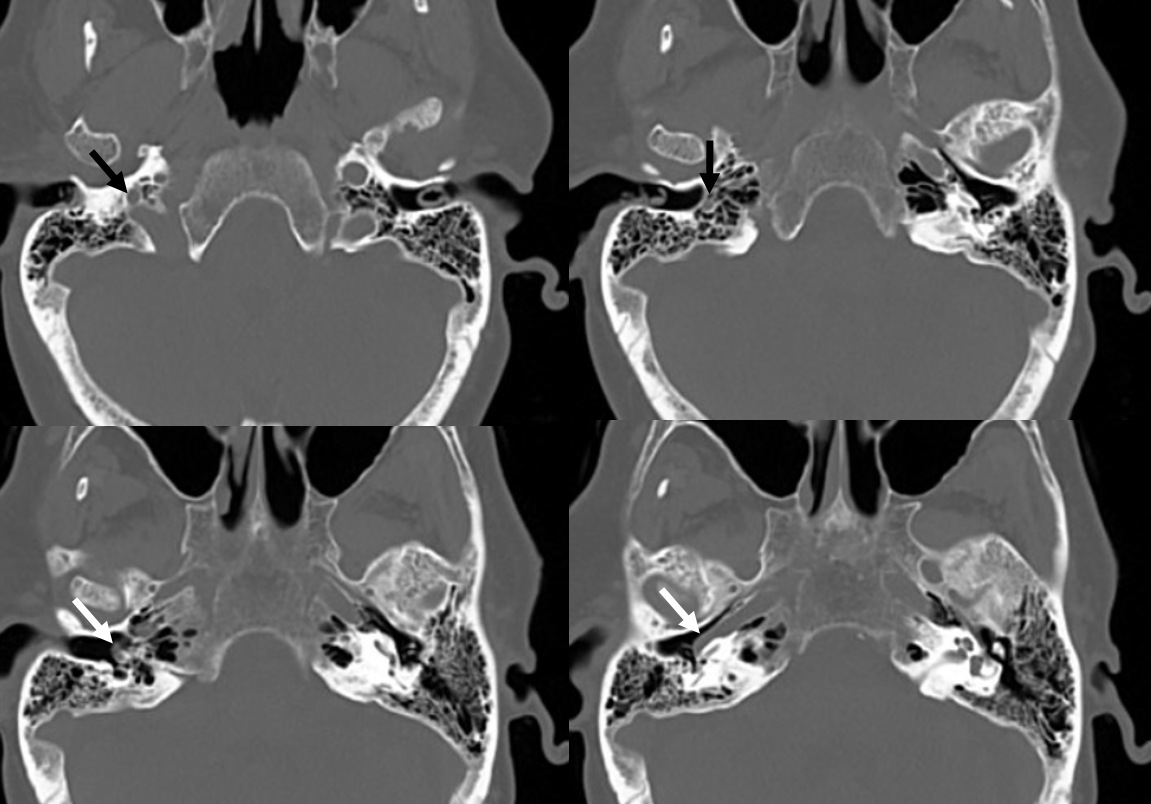
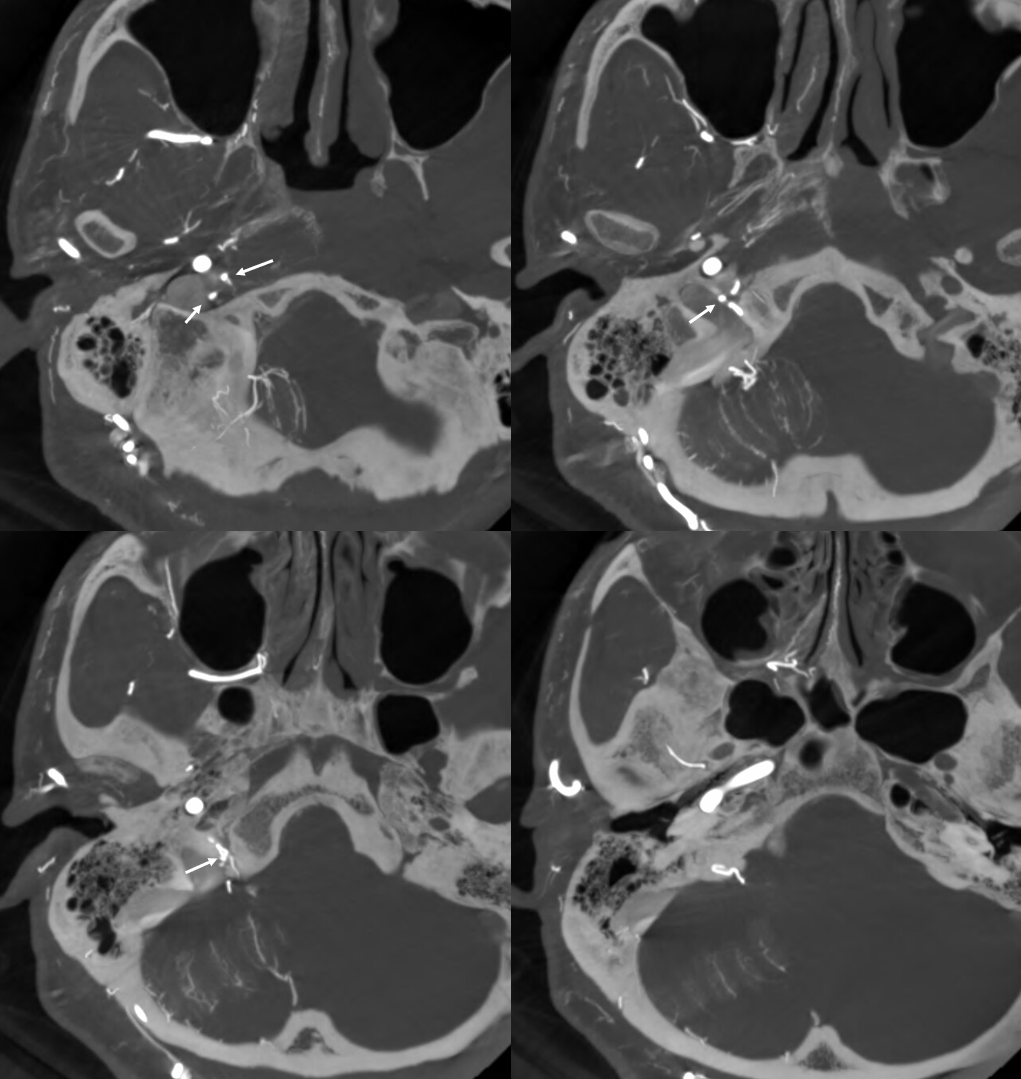
Aberrant Carotid Artery CT
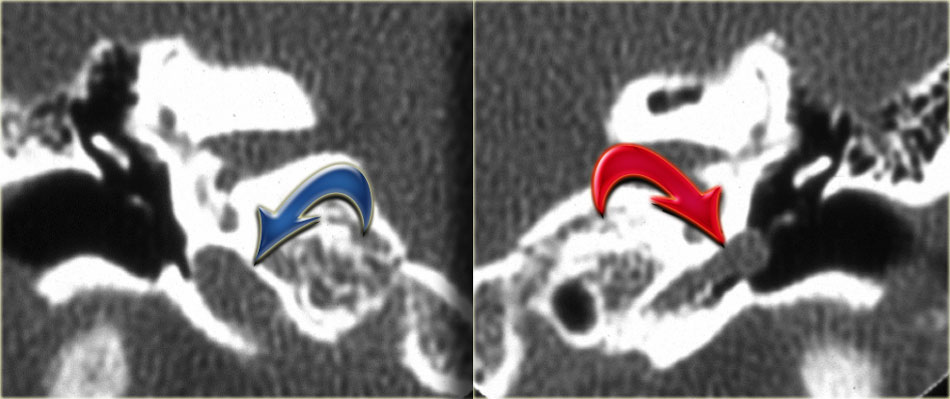
Blue arrow points to normal course of the ICA. The red arrow shows a laterally deviated “aberrant carotid” artery projecting into the middle ear cavity. This corresponds to the course of the of the normally invisible inferior tympanic artery. Image courtesy of http://www.radiologyassistant.nl/images/4a3ea4f5be088Afbeelding-3.jpg
{kind=link}
Aberrant Carotid Artery Schema, from Lo, W; Solti-Bohman, L; McElveen, J. Aberrant Carotid Artery: Radiologic Diagnosis with Emphasis on High-Resolution Computed Tomography. Radiographics 1985; 5(6), p 985-993 http://radiographics.rsna.org/content/5/6/985.abstract
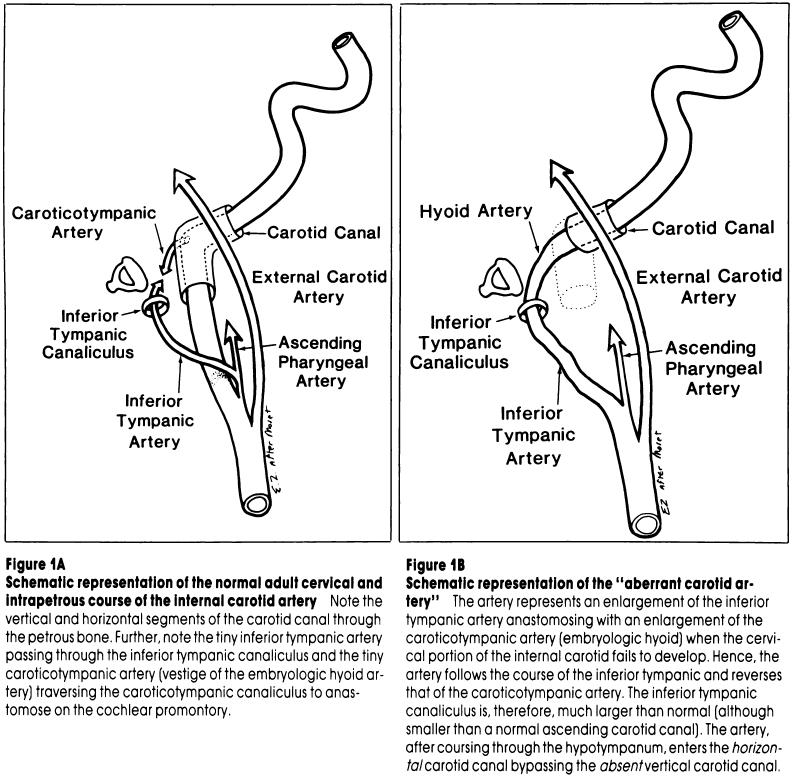
Aberrant Carotid Artery Schema, from Lo, W; Solti-Bohman, L; McElveen, J. Aberrant Carotid Artery: Radiologic Diagnosis with Emphasis on High-Resolution Computed Tomography. Radiographics 1985; 5(6), p 985-993 http://radiographics.rsna.org/content/5/6/985.abstract
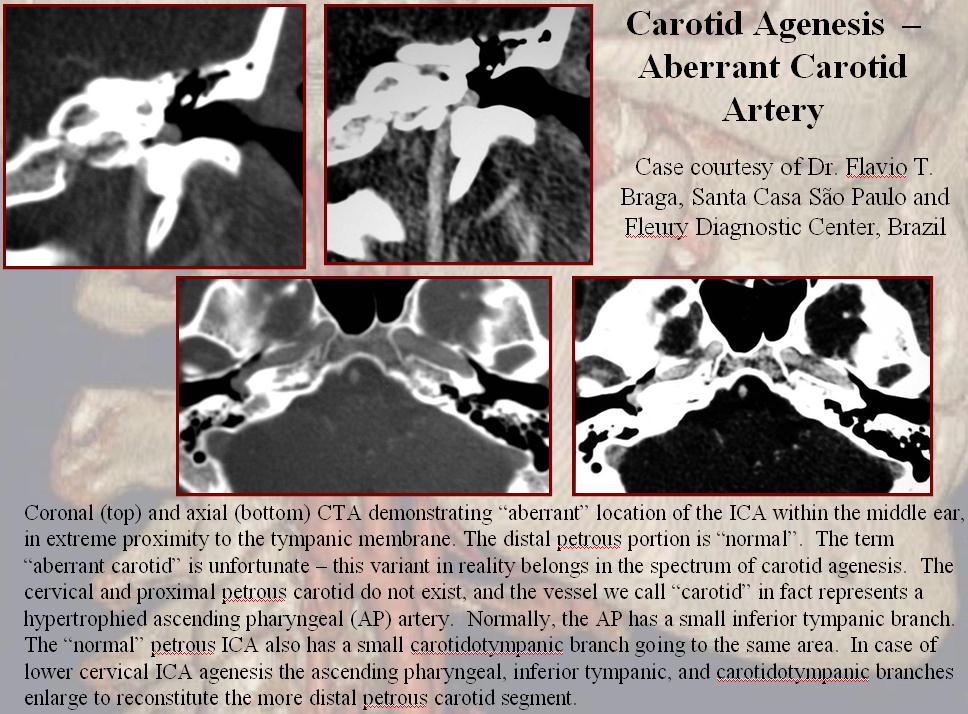
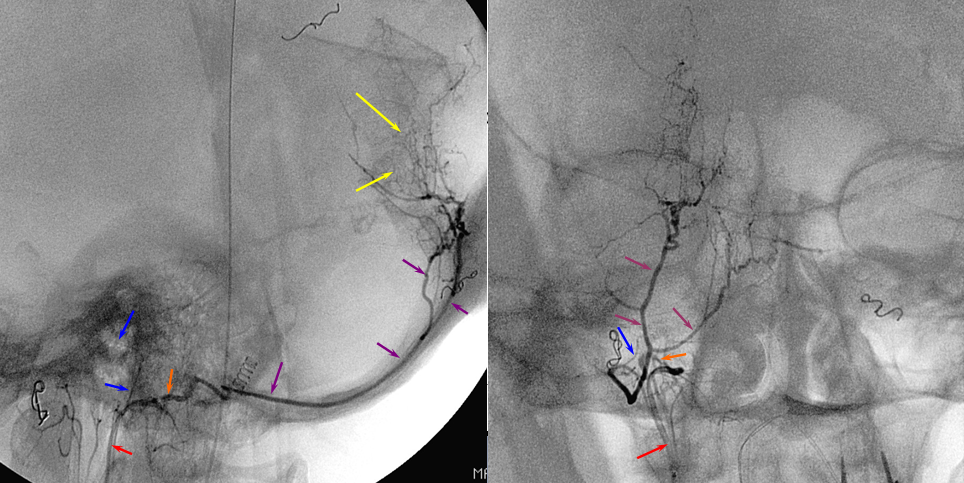
More Aberrant Carotid Artery — The vessel has a characteristic lateral swing within the petrous bone (red arrows), bringing it into the middle ear cavity, which can be appreciated on MR, CT, and angio, as above. Case courtesy of Dr. Howard Antony Riina, NYULMC
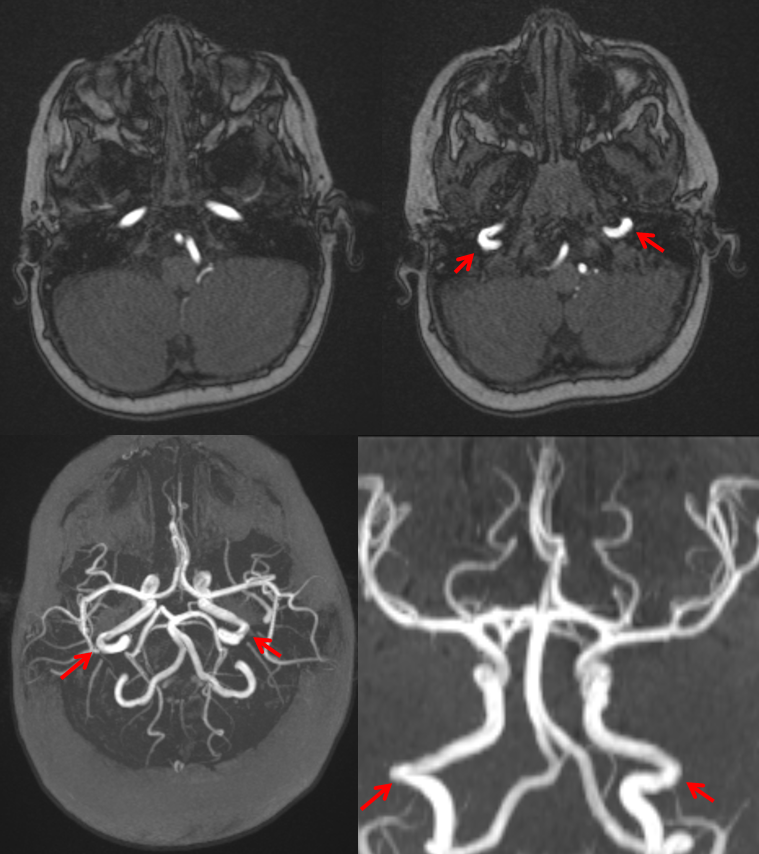
The same appearance angiographically, with a somewhat posterior course in the lateral projection (yellow arrow)
Finally, a VERY cool stereo 3D-DSA, visualizing the aberrant ICA within the ear canal.
Adult example aberrant carotid — Courtesy Dr. Todd Miller, Stamford Health
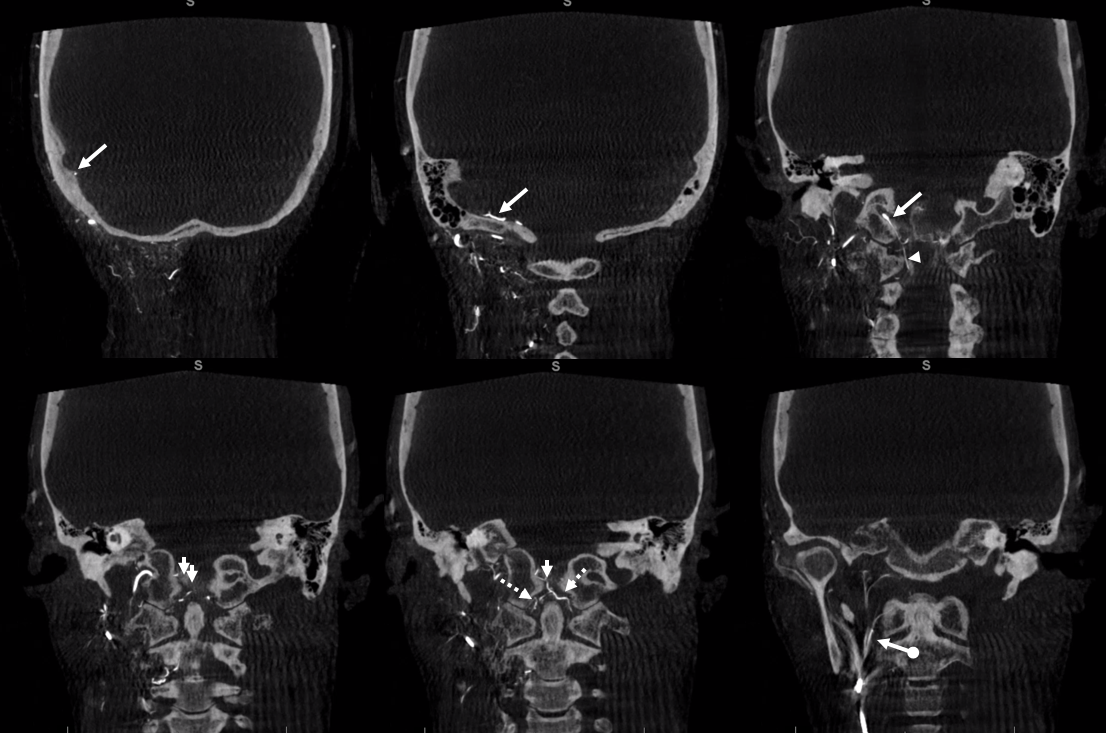
You don’t even need contrast to see an aberrant carotid on high-res CT such as t-bone or thin section helical CT like this one. The path through temporal bone, and over the cochlear promontory (arrows) is really obvious. Below is a pre-contrast mask of a CTA
post contrast images are below — really the precontrast ones are just as good for diagnosis
Caroticotympanic Branch
Pretty much Impossible to see on DSA due to dense petrous bone overlap. Can be fairly often seen on high quality cone beam CT. Below is an example (arrows)
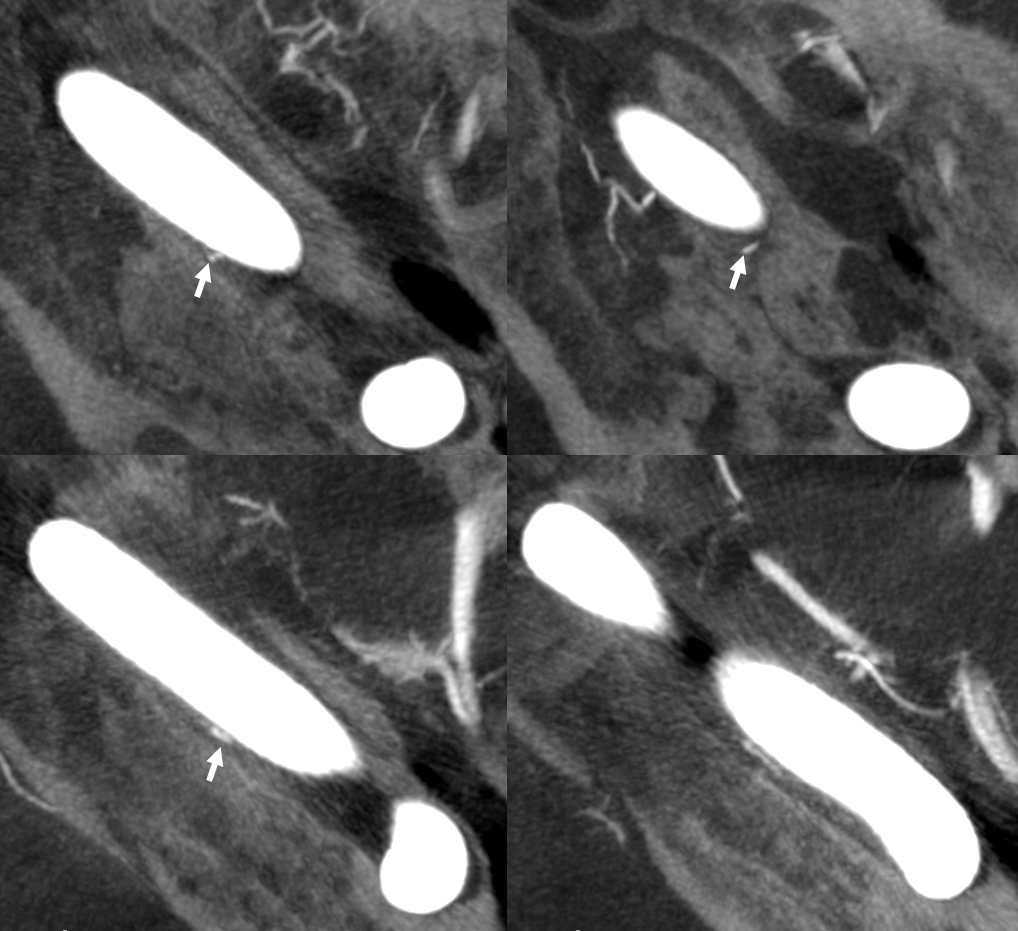
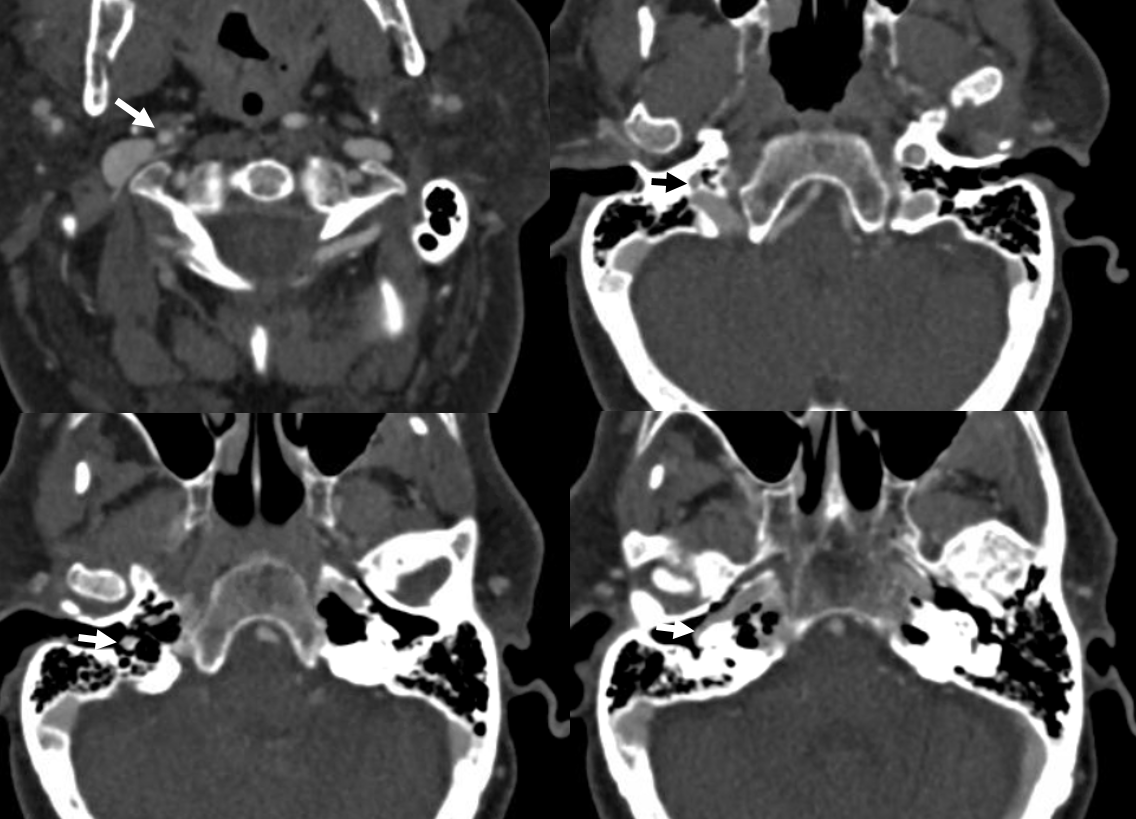
Ascending pharyngeal supply of internal carotid artery — non-aberrant variant
Here is a disposition that, to my knowledge, defies existing theories of embryology. Unfortunately, there is no catheter angiogram. The CTA shows a small, but otherwise “normal” carotid canal on the left (green arrows). There is nothing to suggest extension of the vessel into the middle ear cavity. Normal caliber canal (blue) is on the right

Curved MIP images of the CTA show a vessel originating at the level of the thyrocervical trunk (red), and ascending to fill the carotid canal (green). A twig of superior pharyngeal artery (yellow) is seen. There was no identifiable neuromeningeal trunk arising from this artery. So, is this the ascending pharyngeal? Not in its true sense, as that should follow the “aberrant carotid” disposition and this one does not. Is the ascending cervical artery a closer relative of the ICA than the AP? Don’t know. Suggestions welcome.

The right ICA is normal in caliber, but not altogether so. This curved MIP is missing the ECA

Volume rendered images show separate origins of the right ECA and ICA from the brachiocephalic artery (blue arrow) … Some dispositions defy explanation.

Persistent Stapedial Artery — this is another rare variant. In the same way the inferior tympanic-caroticotympanic connection results in ascending pharyngeal reconstitution of the petrous carotid artery, a persistent inferior tympanic can maintain an embryonic connection to the middle meningeal artery via the petrous branch of the MMA that makes us the facial nerve arcade. Embryologically, the middle meningeal artery does not belong to the IMAX — it instead arises from the petrous ICA via the primitive hyoid artery. The hyoid connects to the inferior tympanic, which goes thru the stapes crura (called stapedial artery at this point) and then via the facial arcade supplies what is ultimately the MMA. This connection is rudimentary in adulthood for most of us. However, in some cases the ascending pharyngeal-inferior tympanic-petrous-MMA connection persists. Simply put, the MMA is a branch of the ascending pharyngeal. Here is an example of this, on MRA; images courtesy of Dr. Eytan Raz. Blue – inferior tympanic branch; red = stapedial; yellow – petrous/horizontal facial nerve canal branch; white = MMA

Axial views, with right AP in clandestine black; the IAC is orange

NEUROMENINGEAL TRUNK:
Jugular Division:
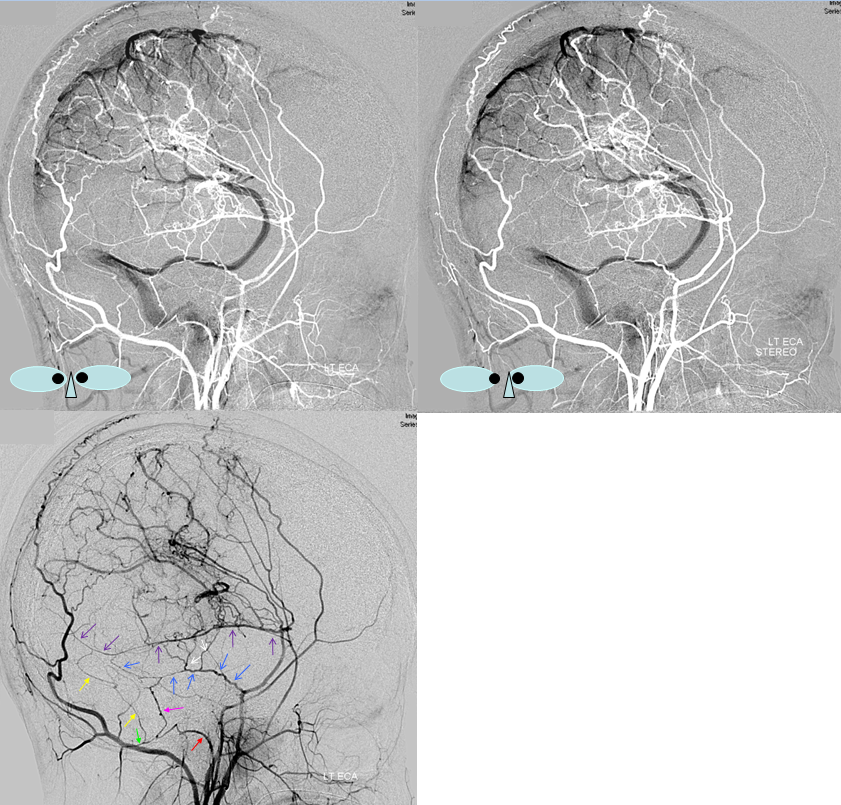
The jugular division enters the jugular foramen, where it supplies the relevant cranial nerves, and adjacent dura. It collateralizes with branches of the hypoglossal division, the posterior meninigeal artery, and arteries of the tentorium. Jugular division branches tends to run laterally along the sigmoid sinus, whereas the hypoglossal branches project anteromedially towards dorsum sella. Although diagnostic injections of this division can be very useful in study of posterior fossa and other lesions, embolization is treacherous since there is a risk of CN IX, X, and XI palsy.
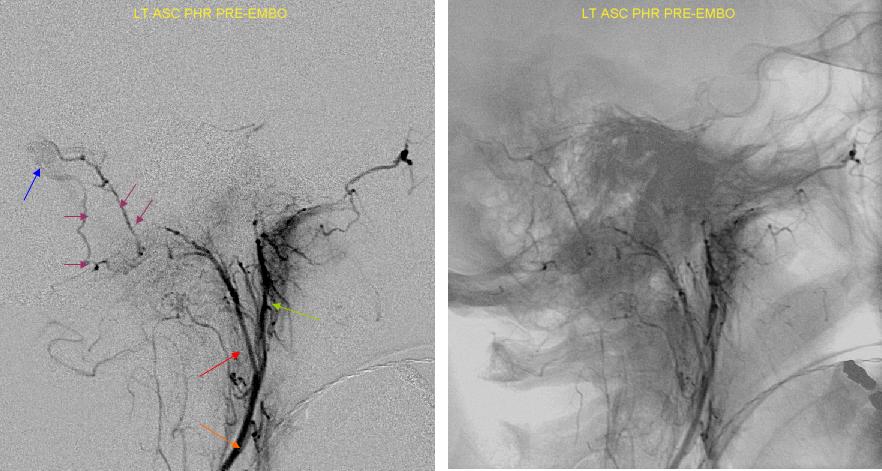
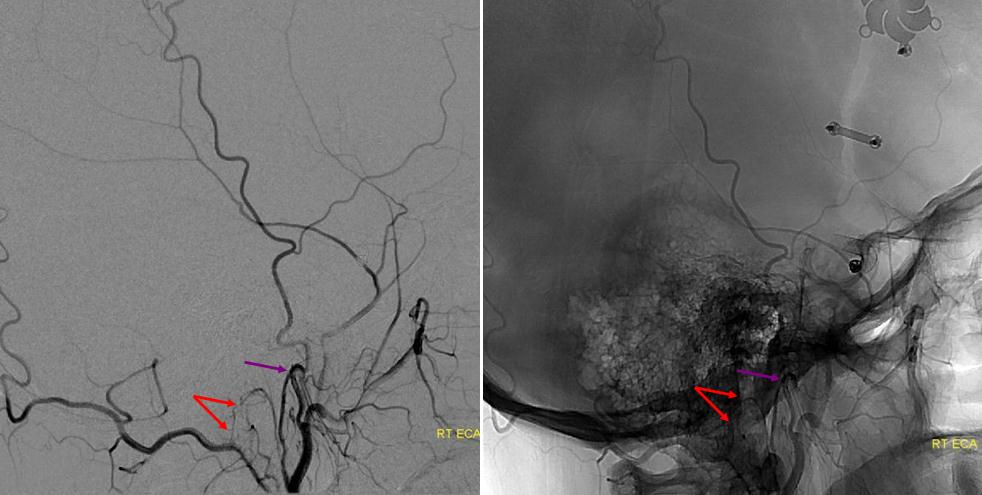
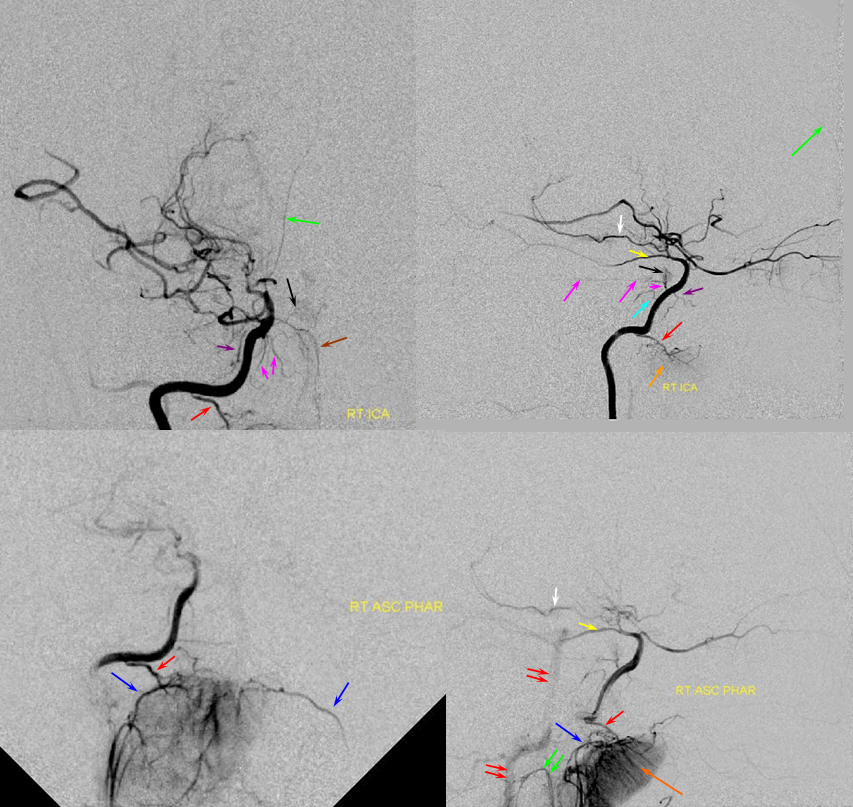
Blue arrow points to a dural fistula adjacent to the sigmoid sinus. The sigmoid branch (purple) of the jugular division (red) is well demonstrated on this injection, running along both superior and inferior dural reflections of the sigmoid sinus (faint blush, blue arrow). The pharyngeal branch is labeled with green arrow.
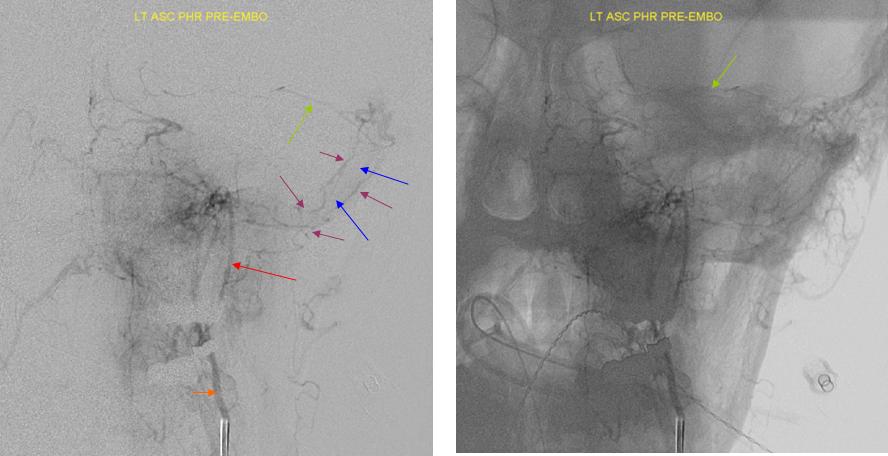
AP views of the same patient again demonstrate jugular division sigmoid branches (purple) running alongside the sigmoid sinus (blue). Green arrow points to the basal tentorial arcade which is projecting towards the cavernous sinus region.
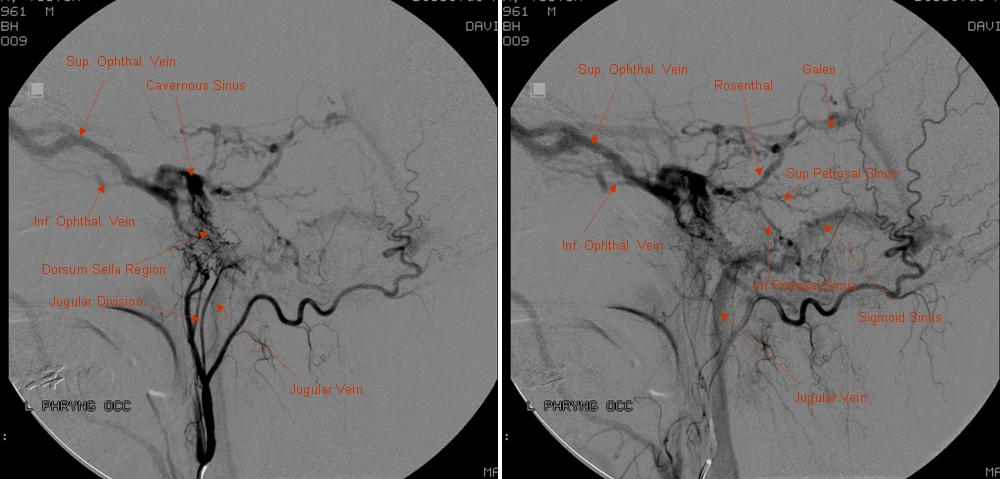
Lateral projections in case of a complex cavernous sinus dural fistula. The fistula is extensively supplied by clival branches of the hypoglossal division, which ascend along the Dorsum Sella. The entire dura of the region is involved, with myriad arteries and arterioles carpeting the Dorsum Sella’ no dominant feeder is apparent. This is seen quite often. During surgical exposure of such cases, the dura is seen as a virtual sheet of small vessels.
Jugular division origin of the posterior meningeal artery in a patient with “en plaque” meningioma of the parieto-occipital skull
Neuromeningeal trunk=red; Jugular division=orange; posterior meningeal artery=purple; inferior tympanic artery=blue; meningioma blush = yellow
Sigmoid sinus fistula, neuromeningeal trunk:
Another demonstration of sigmoid branch supply to a sigmoid sinus fistula, also being fed by occipital and lateral tentorial (MHT) branches. Notice also musculoskeletal branch contribution to the fistula which on the lateral may be mistaken for an odontoid arch branch.
Red=neuromeningeal trunk and jugular division thereof; white=sigmoid branch; yellow=hypoglossal division; pink=musculoskeletal branch; green=superior pharyngeal branch; purple=inferior tympanic?
Micro-injection of neuromeningeal trunk in a patient with a skull base meningioma. On the frontal view, jugular division projects laterally and hypoglossal division medially

Jugular branch and extensive anastomoses in setting of Moya-Moya and synangioses.
Patient with bilateral Moya-Moya, post bilateral dural synangiosis and burr hole (see Intracranial Collateral Pathways for the remainder of this case). Stereo image pair on top, with dural/ arterial vasculature in white, and venous outflow in black, outlining an arterial arcade which runs within the dural sheath of the transverse/sigmoid sinuses, partly made up by the jugular branch of the neuromeningeal trunk. Anastomoses with middle meningeal and occiptal branches are clearly demonstarated. These arteries frequently participate in supply of sigmoid sinus dural fistulas.
•Red – ascending pharyngeal artery, neuromeningeal trunk
•Pink – ascending pharyngeal artery, jugular branch
•Blue – middle meningeal artery, basal tentorial branch
•Purple – middle meningeal artery, petrosquamosal branch
•White – anastomotic connections between basal tentorial and petrosquamosal branches
•Green –mastoid branch, occipital artery
Hypoglossal Division:
The hypoglossal division enters through the hypoglossal foramen where it supplies CN XII, and branches into several vessels supplying the adjacent dura. On the frontal projections, it courses medially, while the jugular division goes laterally. On the lateral projection, it enters the skull posterior and lower than the jugular division. Its vessels tend to project medially and anterior once inside the cranium towards dorsum sella (where it often supplies fistulas and meningiomas) Jugular division branches tends to run laterally along the sigmoid sinus.
Lateral AP Injection of a sigmoid sinus dural fistula patient. Both neuromeningeal trunk divisions (Hypoglossal lower and posterior to the jugular division) supply the fistula with multiple branches running along the back of the clivus. Additional supply routes from pharyngeal division through various skull base foramina are also present.
Odontoid Arcade
The odontoid arcade represents a pathway whereby both AP and vertebral arteries can all connect to each other at the C1-C3 level. The arcade is formed by branches of the AP and vertebral arteries. It outlines the odontoid process and upper cervical region, coursing behind the odontoid process and C2 body. The arcade is formed as follows: 1) The hypoglossal division enters the hypoglossal canal. 2) A descending branch from this division exits from the foramen mangum and heads inferiorely along the back of the dens and C2 body, eventually anastomosing with the vertebral artery at the C3 level. 3) Transverse branches at C1 and C2 levels project from this descending branch to its contralateral homolog, eventually connecting to the contralateral vertebral and ascending pharyngeal arteries. Thus, a system exists whereby both AP and vertebral arteries are connected to each other.
Fundamentally, the odontoid arcade is part of the ventral epidural arterial arcade of the spinal canal — see spinal arterial anatomy for more information. Because the odontoid process is a kind of “funny bone” the arcade looks slightly different at this level compared with the diamond-shaped structure elsewhere in the cervical, thoracic, and lumbar spine. However, it is the same thing.
Descending branch (red) of the hypoglossal division is relatively prominent in this patient. The jugular division and other branches of hypoglossal division are not visible. The superior branch of the pharyngeal trunk (purple) is dominant.
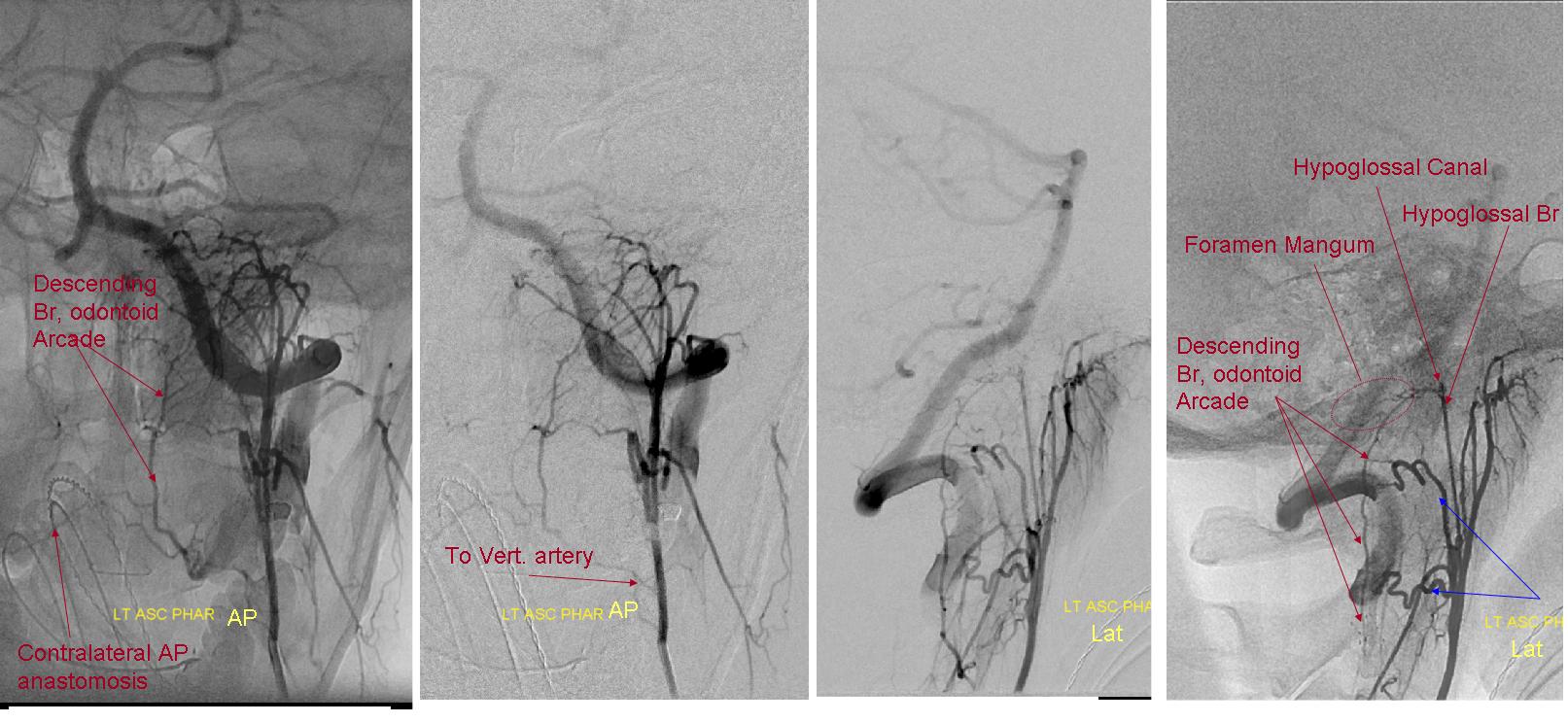
AP and lateral bone and native mask injections of the AP artery in a patient with high-grade vertebral artery stenosis at C3 level. The descending branch of the hypoglossal divison exiting FM and running along the posterior aspect of C1 and C2 is well seen on the lateral projections. In the AP, it is off-midline, sending branches to its contralateral homolog (not visible)
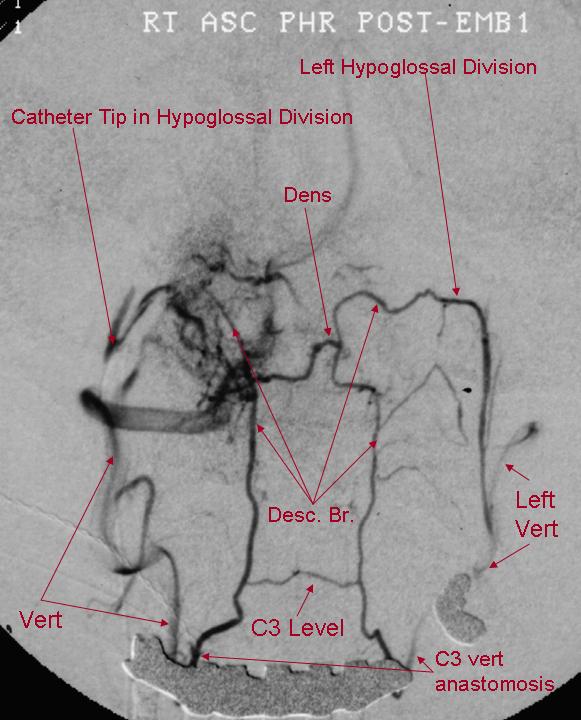
AP view of right Hypoglossal division microcatheter injection, with exquisite demonstration of the odontoid arcade. A descending branch of the right hypoglossal division opacifies the arcade with visualization of the contralateral AP anastomosis and vertebral arteries. The arcade is seen to advantage because the remainder of right hypoglossal division has been embolized, thereby diverting flow into the arcade.
Odontoid arcade, Vidian artery, and other AP anastomoses
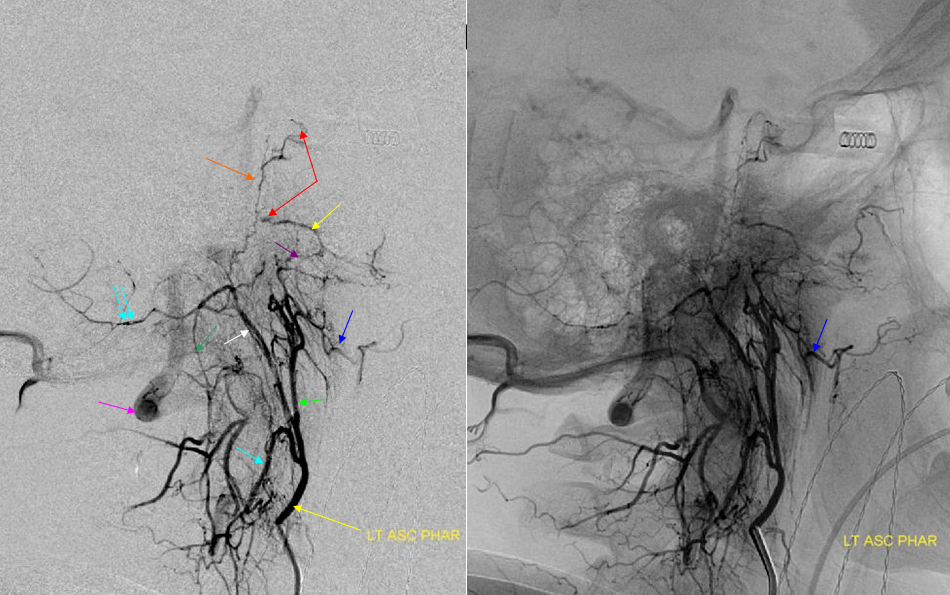
AP (above) and latearal (below) views of an ascending pharyngeal injection demonstrate a number of very instructive findings. The pharyngeal trunk (green) superior branch anastomoses wtih the ascending palatine artery (blue) and the vidian artery (yellow) which opaficies petrous ICA with a small blush (red). The neuromeningeal trunk (white) hypoglossal branch shows prominent ascending clival branches wich reconstitute the proximal cavernous carotid artery a the level of the MHT with another small carotid blush (red). The descending branch (green) of the hypoglossal division opacifies various components of the odontoid arch (black arrows). A prominent musculospinal branch (blue) reconstitutes the vertebral artery (pink).
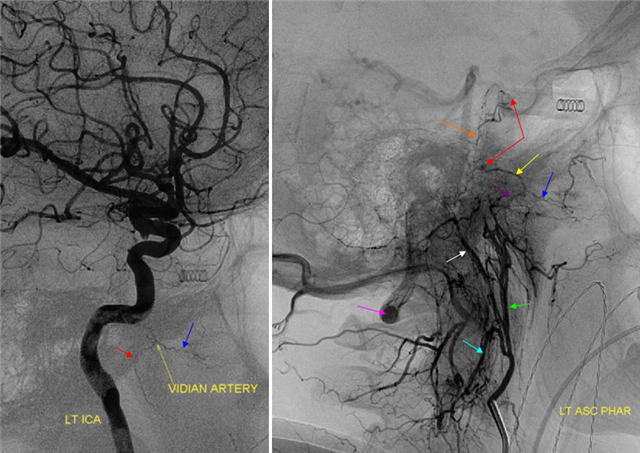
Same case, with ICA injection with a prominent vidian artery( yellow), which is retrogradely opacified on the AP injection.
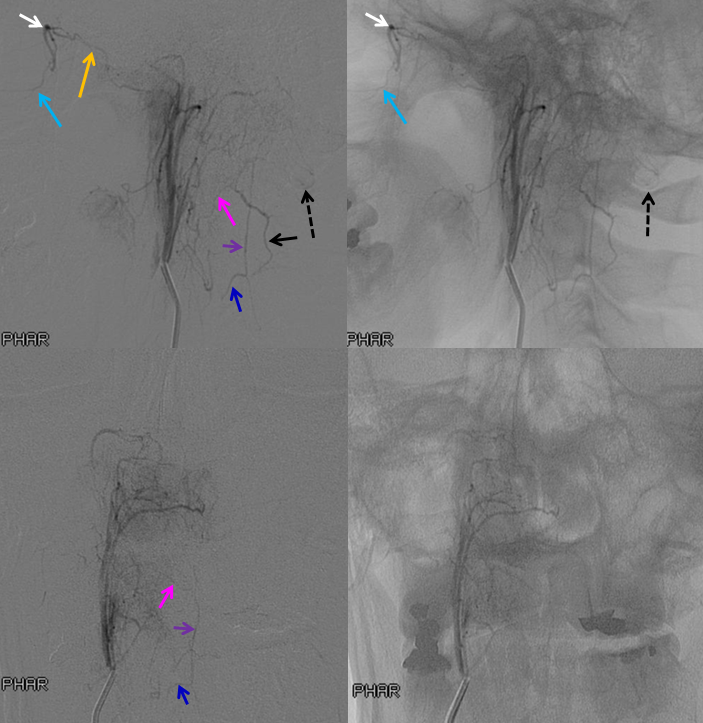
Ascending pharygeal to anterior spinal (purple) anastomosis via the odontoid arcade — for those who wish to embolize to vertebral and anterior spinal artery from the AP simultaneously, the way is through the odontoid arcade. This AP (originating directly from the internal carotid artery) opacifies the anterior spinal artery (purple) via the odontoid arcade (pink) which also demonstrates the vertebral artery (discontigous black). The C3 contribution to the anterior spinal artery is retrogradely opacified (blue). The nasal septal branches (light blue) are opacified via the superior pharyngeal artery connection to the sphenopalatine artery (yellow).
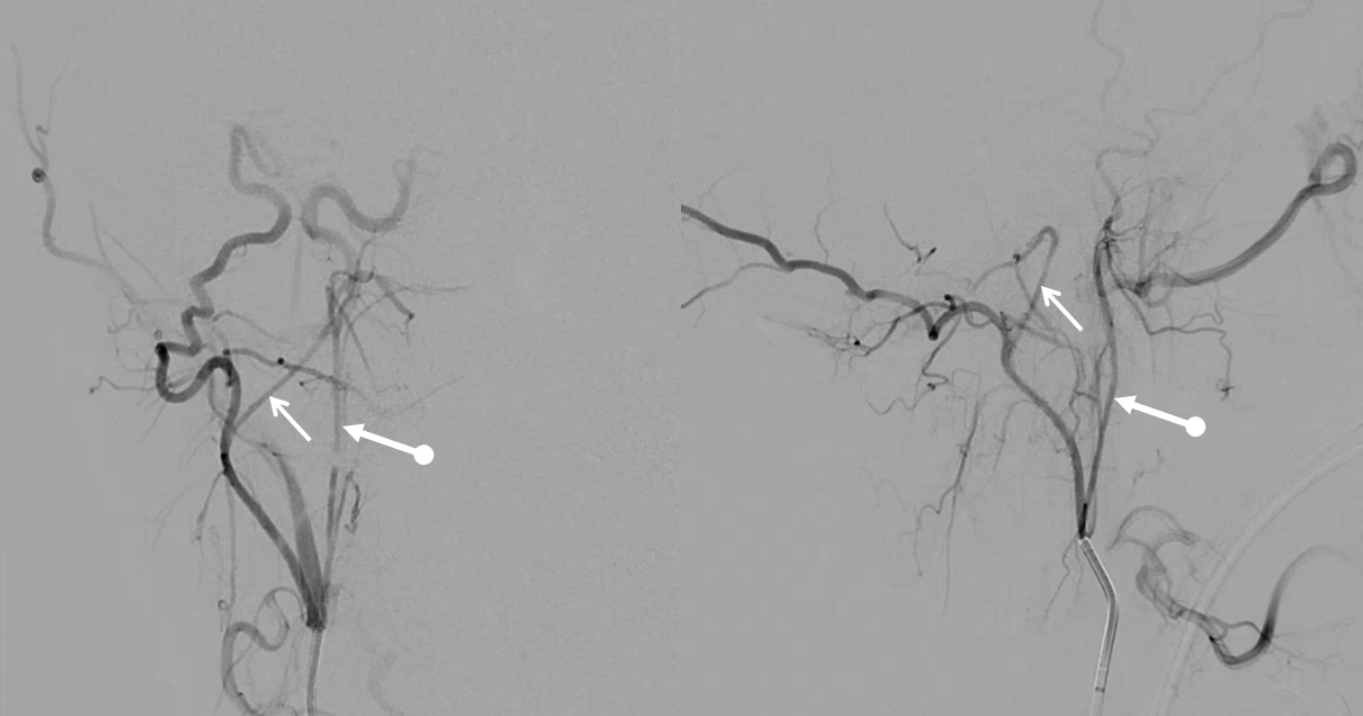
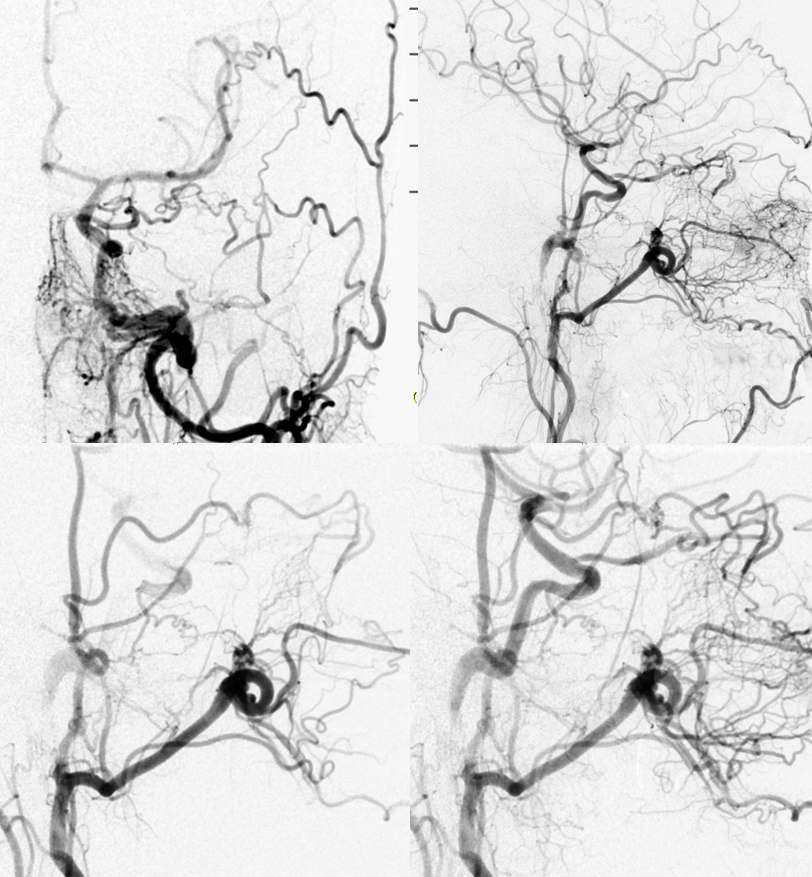
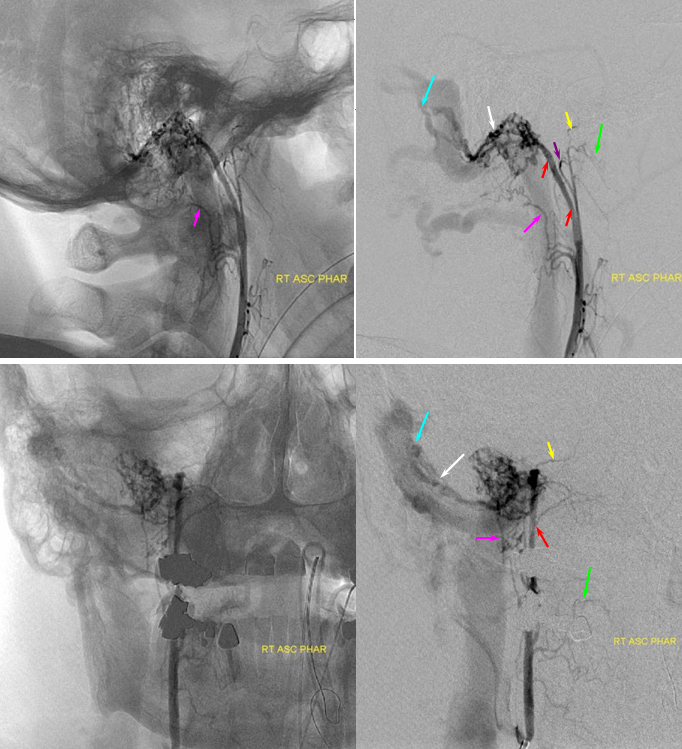
Ascending pharyngeal Artery reconstituion of both vertebral artery and internal carotid artery in a patient with M1 dissection. A child with spontaneous right M1 dissection. Right ICA runoff is diminished and all dural branches are well-seen. The mandibulovidian artery (red) is prominent and is briskly opacified via the AP injection through the superior pharyngeal division (bottom set of pictures). There is also collateral connection with the vertebral artery present via the odontoid arch.
Red=mandibulovidian branch; Orange=mucosal blush of the posterior nasopharynx; dark blue=Ascending Pharyngeal, superior division (contralateral side also visible on the AP ascending pharygeal projection on bottom left); Purple=ILT; Pink=MHT; Black=pituitary blush; Yellow=PCOM; White=anterior choroidal; Green=anterior meningeal (off ophthalmic, origin outside field of view on the lateral ICA projection); Double Green=odontoid arch of the neuromeningeal division of the ascending pharyngeal artery; Double Red=vertebral artery.
More EC-IC anastomoses — “wedge” position injection of diagnostic 4F vert catheter in the ascending pharyngeal allows for identification of “dangerous anastomoses” — vert via the musculospinal branch and ICA via the carotid branch of AP connecting with mandibular branch of the ICA
Deeper Stereo lateral
Persistent Hypoglossal Artery (PHA)
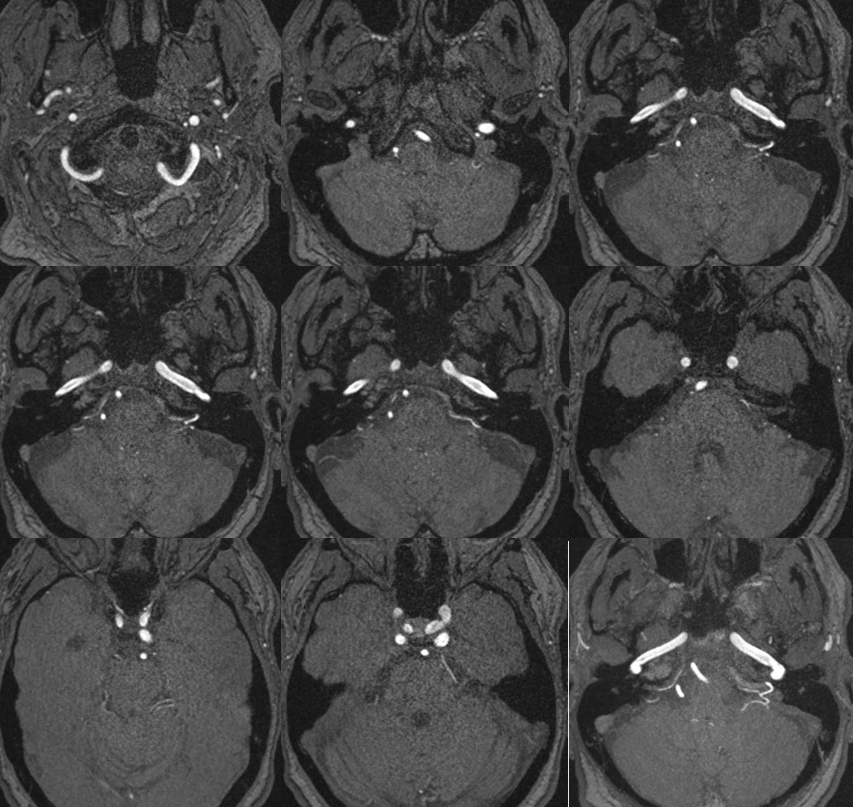
This is essentially hypoglossal division taken to the extreme. See Vascular Neuroembryology Section for relevant origin of this vessel. Briefly, the hypoglossal artery (a.k.a. hypoglossal division of the AP) is a metameric vessel which in early fetal life serves as an anastomosis between the external carotid and vertebral systems. Usually, as the vert develops these segmental anastomoses (which also include trigeminal and proatlantal vessels) nearly completely regress but never disappear. Should the vertebral artery fail to develop, the hypoglssal represents one way of supplying the territory in question. It is essentially a hypertrophied hypoglossal division of the AP which anastomoses with the vertebral artery intracranially. On MRI (see below) the vessel is unmistakably identified as it enters the hypoglossal canal. When seeing the PHA on angio, look for other branches of the AP either coming off the PHA or from elsewhere.
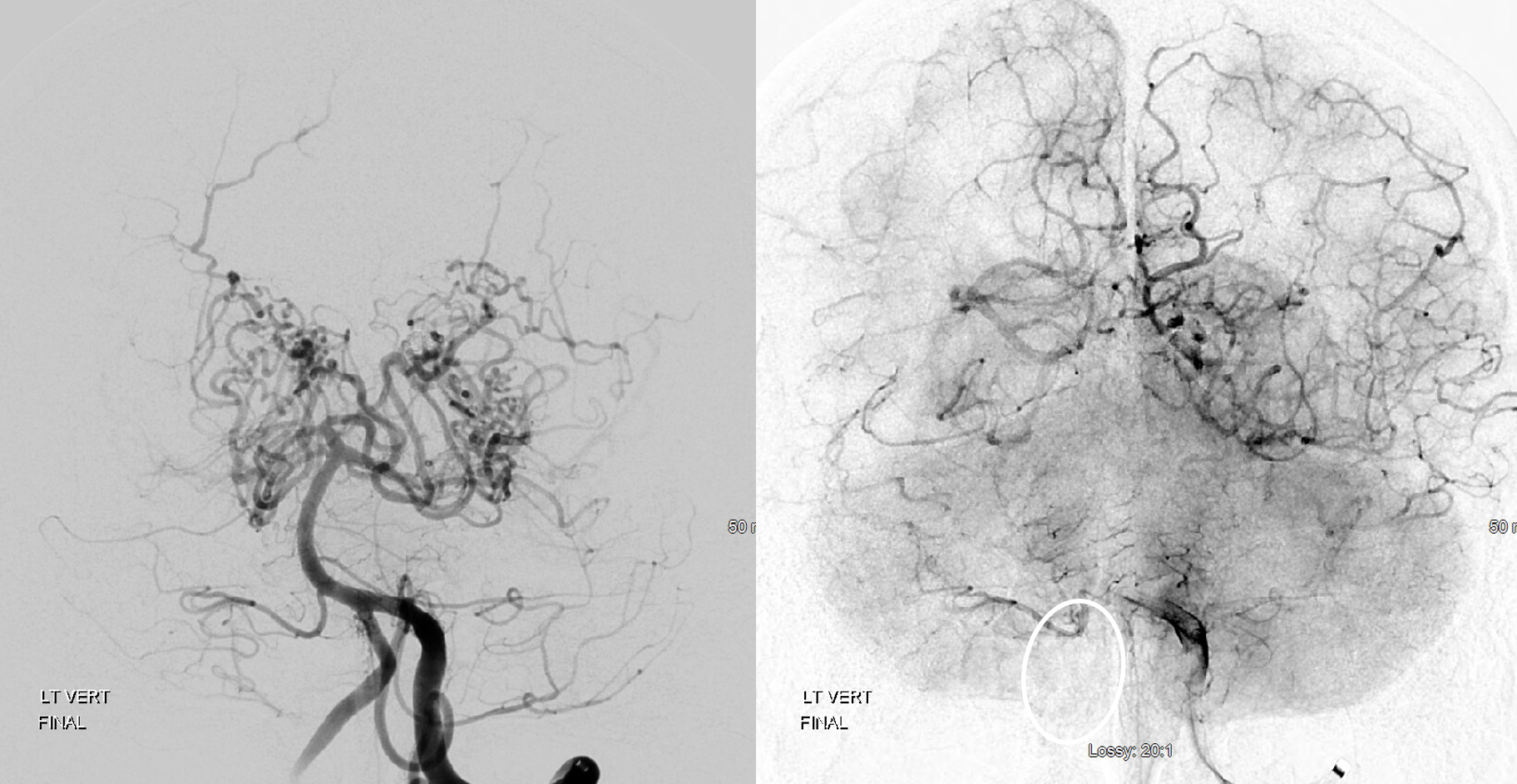
3-D TOF MRA demonstrating persistent left hypoglossal artery.
Catheter angiogram of another patient demonstrating large persistent hypoglossal artery (brown). Injection of the contralateral vertebral artery shows a rudimentary vertebral segment (blue) distal to the PICA. At the basilar level, PHA washes in vertebral contrast (yellow).
Ascending Pharyngeal Supply of PICA. On the same spectrum as persistent hypoglossal, with embryonic connection of hypoglossal division (arrow) to PICA. Typical cerebellar venous pattern (oval) Courtesy Dr. Eytan Raz. Best seen on DYNA CT.

Notice that there is a PICA present on the right — the hypoglossal supply here is limited to vermian area. The extensive Moya-Moya is likely a coincidence — at least the AP-PICA supply is not a hemodynamic consequence of Moya-Moya.
Ascending Pharyngeal Supply of the AICA
Very very rare. Here is an MRA example — via pars nervosa of jugular foramen. Outlined by solid white circle. SCA is dashed white circle. By Eytan Raz MD PhD
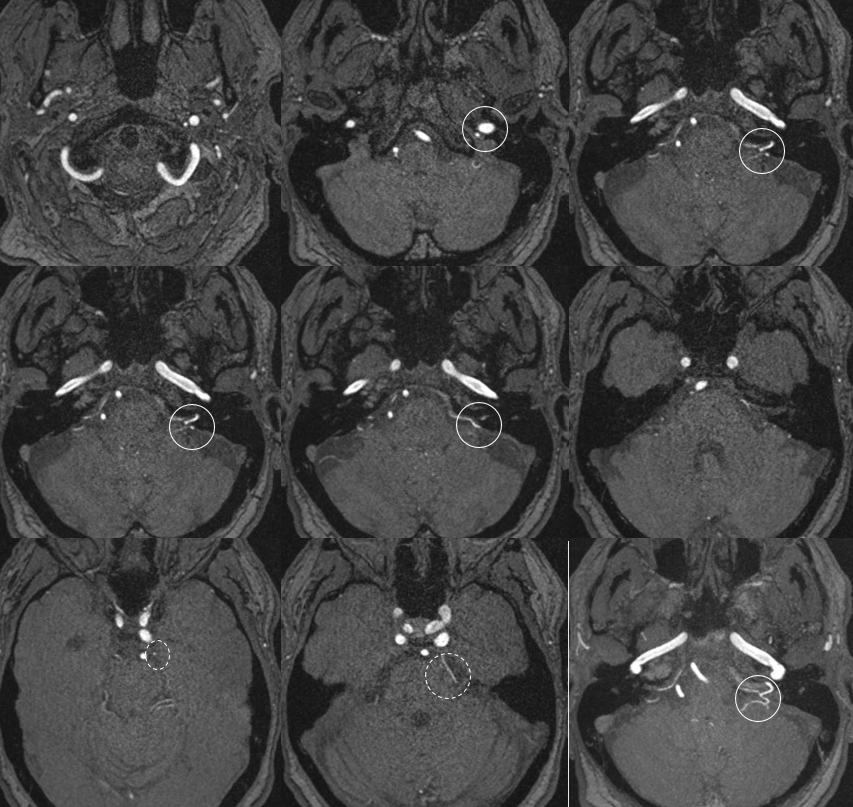
Without circles
Musculospinal Branches:
This branch (or branches) typically originate from the neuromeningeal trunk at C3 level (variable) and supplies adjacent cervical musculature, the cervical sympathetic ganglion, and branches of CN XI. These branches typically have extensive anastomoses with vertebral, ascending, and deep cervial arteries and is a potential avenue for inadvertent intracranial embolization from the ascending pharyngeal artery.
AP and lateral bone and native mask injections of the AP artery in a patient with high-grade vertebral artery stenosis at C3 level. The musculoskeletal branches of the neuromeningeal trunk (blue arrows) are reconstituting vertebral artery flow distal to the area of stenosis at C1 and C2 levels. Notice also a well-developed odontoid arcade participating in reconstitution as well.