
Case Strategy Courtesy Dr. Dan Meila, of Hannover, Germany, who has multiple successful cases. He convinced me to try it again just two days before this case.
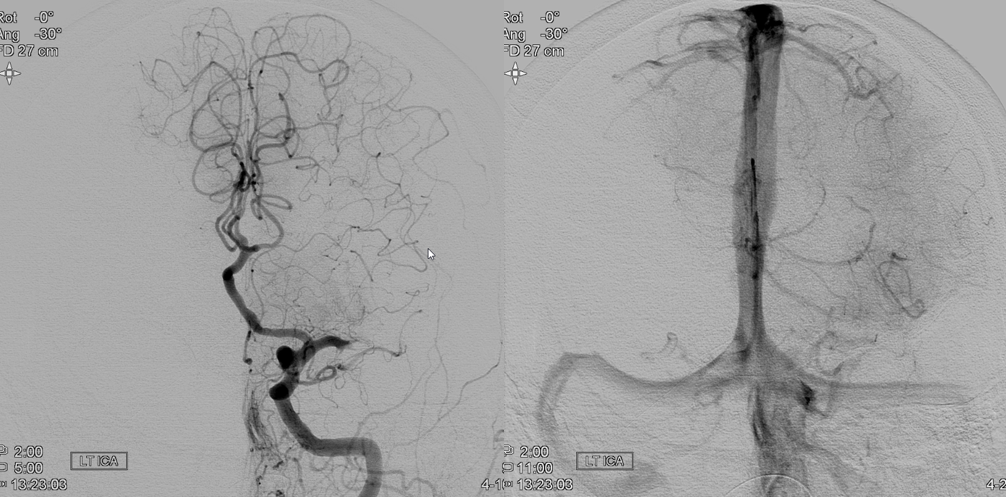
The emerging field of distal mechanical thrombectomy gives more options in acute stroke setting. Not all distal emboli dissolve, and not all are eligible for thrombolytics. This patient was last known well last night.
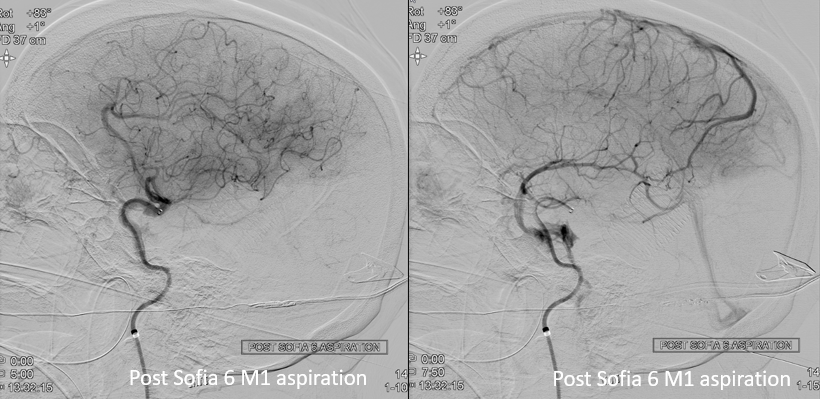
Post standard M1 aspiration with Sofia 6
Obliques show residual thrombus in the developmentally hypoplastic inferior division M3 (arrows). The Wernicke area sill looks closed
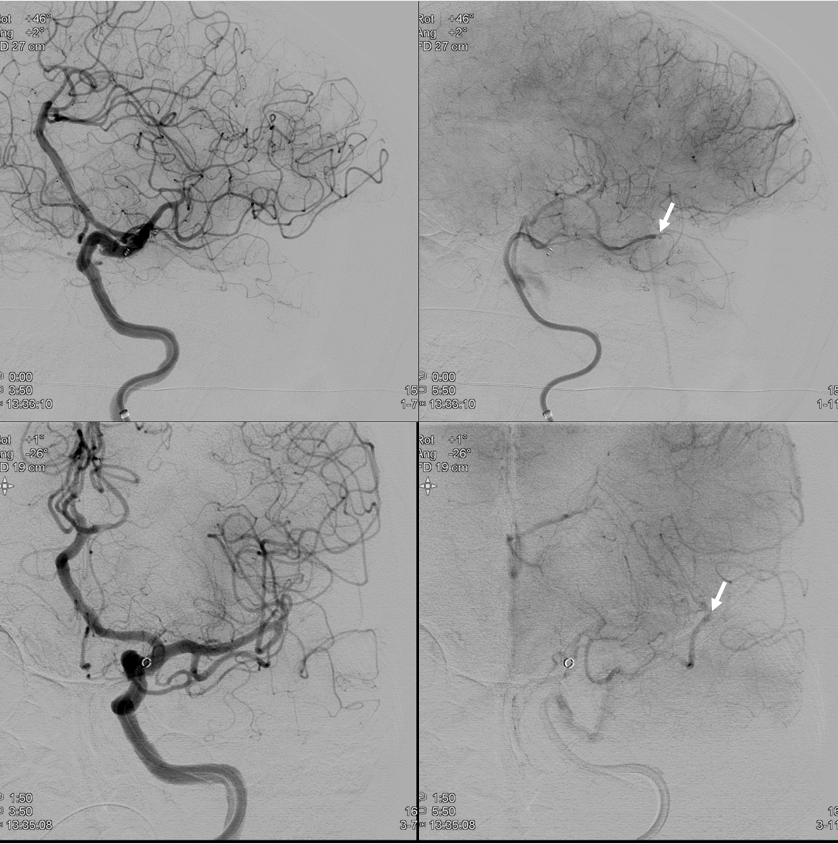
What to do? Leave it alone — too distal? Yes, if nondominant hemisphere maybe reasonable option. What here? Intra-arterial thrombolysis is not great given last known well. Distal stent-triever is very feasible. We have example here. But, why not try distal aspiration? Seems like the best choice if it works. A few days before this case, Dr. Dan Meila from Hannover showed me examples of his multiple successful cases and convinced me to try it again.
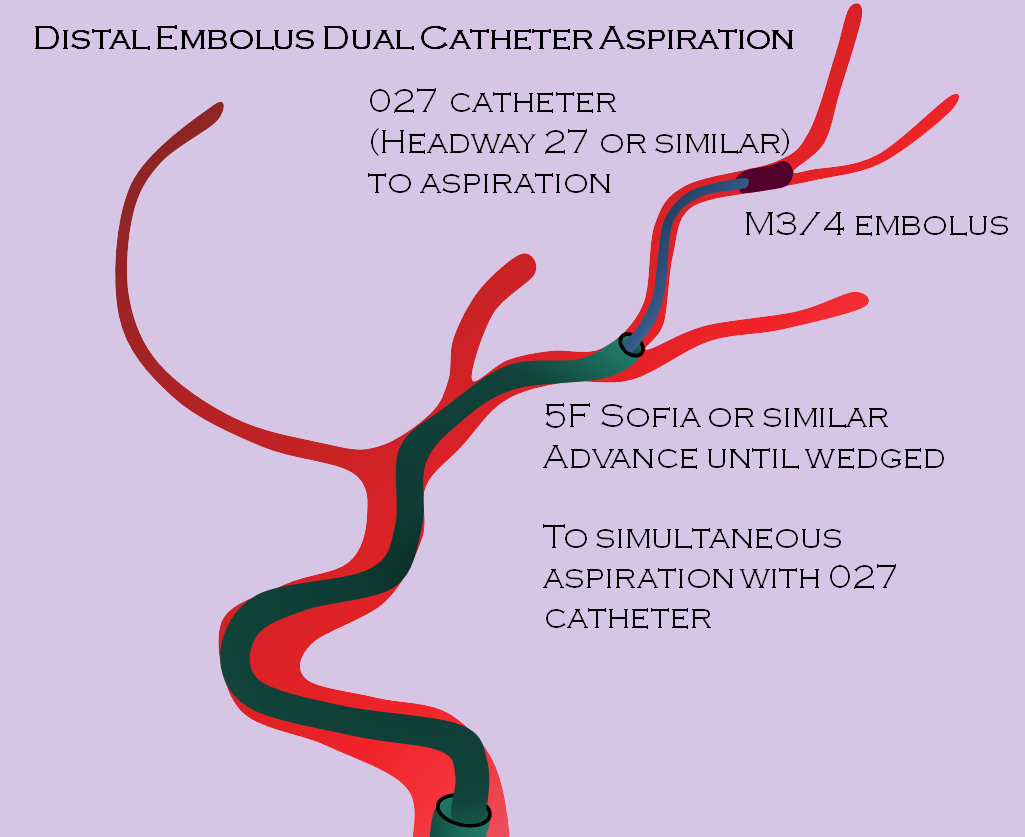
Technique is to bring up an 027 catheter (Marksman in this case) within a Sofia 5. The 027 goes to the embolus, and Sofia as distal as possible. In this case, it could not enter the inferior division.
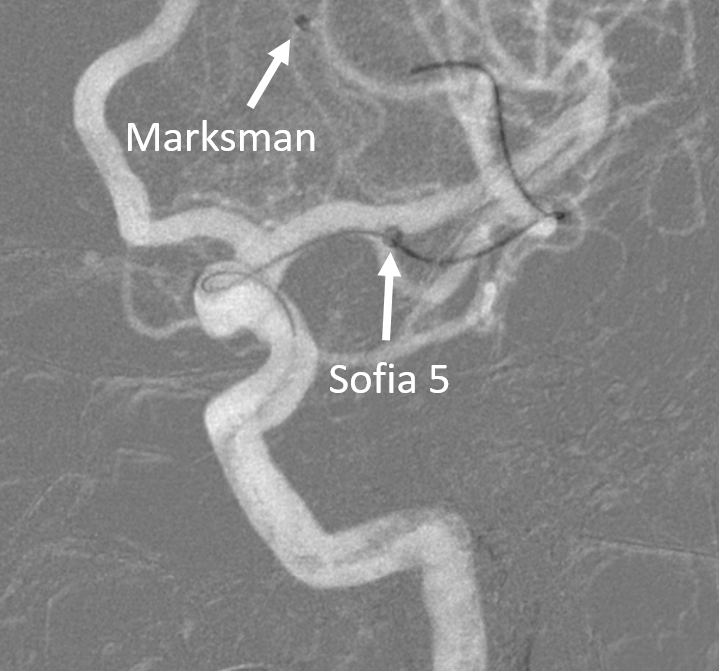
Aspiration positions. Aspirate with 60 cc syringes on both catheters. Some use 10 cc for the 027

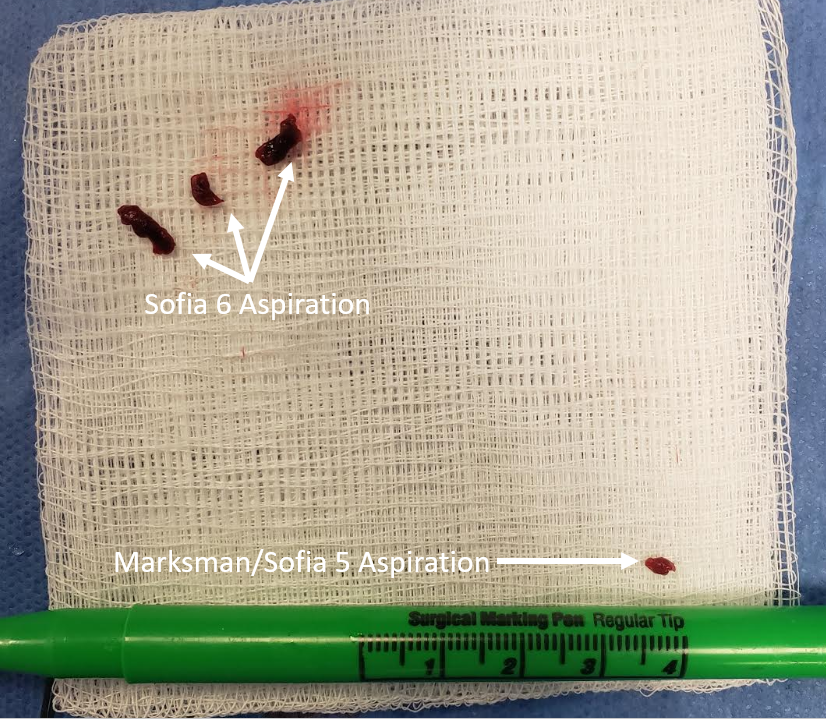
Simultaneous aspiration of Sofia and 027 is next. The 027 was withdrawn into the Sofia. No flow was seen in the 027 until it entered the Sofia, and there was no flow in the subsequently pulled Sofia until its withdrawal into the supraclinoid ICA. Image below shows two sets of thrombi — three larger ones from initial M1 pull, and small one from 027 pull. Likely the 027 held the embolus until its entry into the Sofia, when it came off but was then ingested by the Sofia
Final
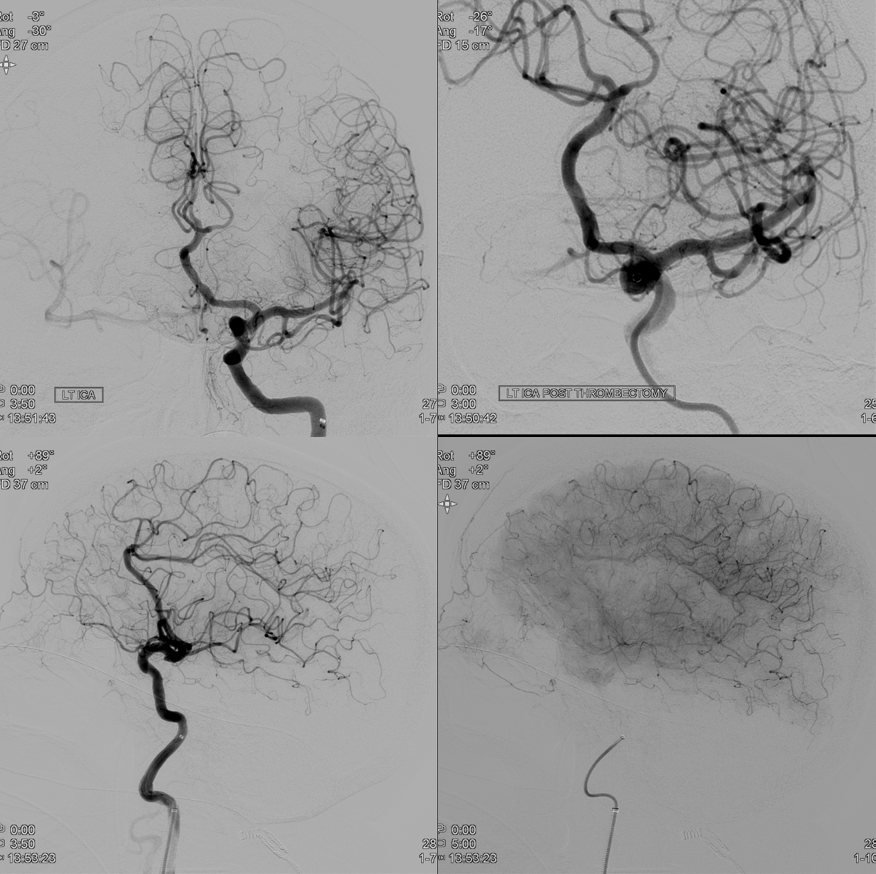
Final
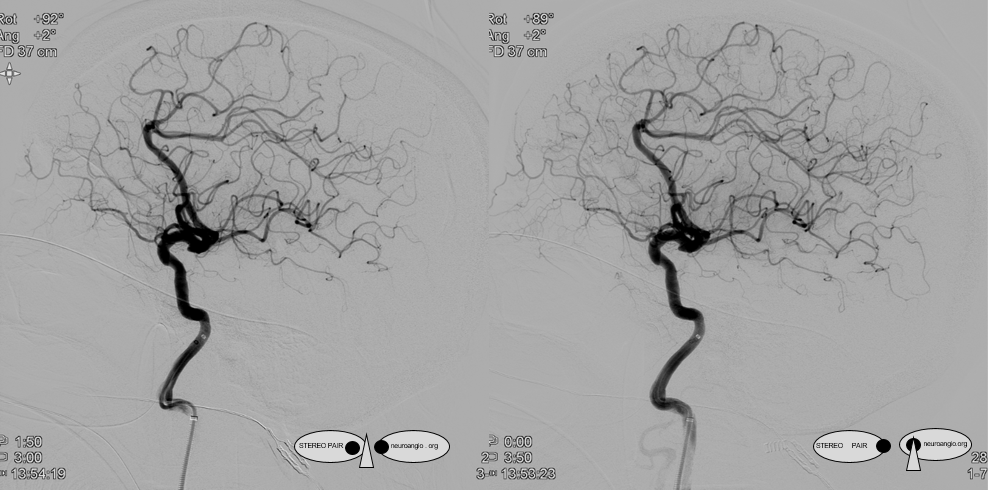
Conclusion
Distal aspiration is feasible, without need for distal stent-triever deployment and keeping costs down