
Together with, and proctored by, Dr. Eytan Raz
This scores a 10/10 on the WEBology scale. A case highlighting use of advanced imaging and treatment tools to address the most complex and demanding aneurysm situations
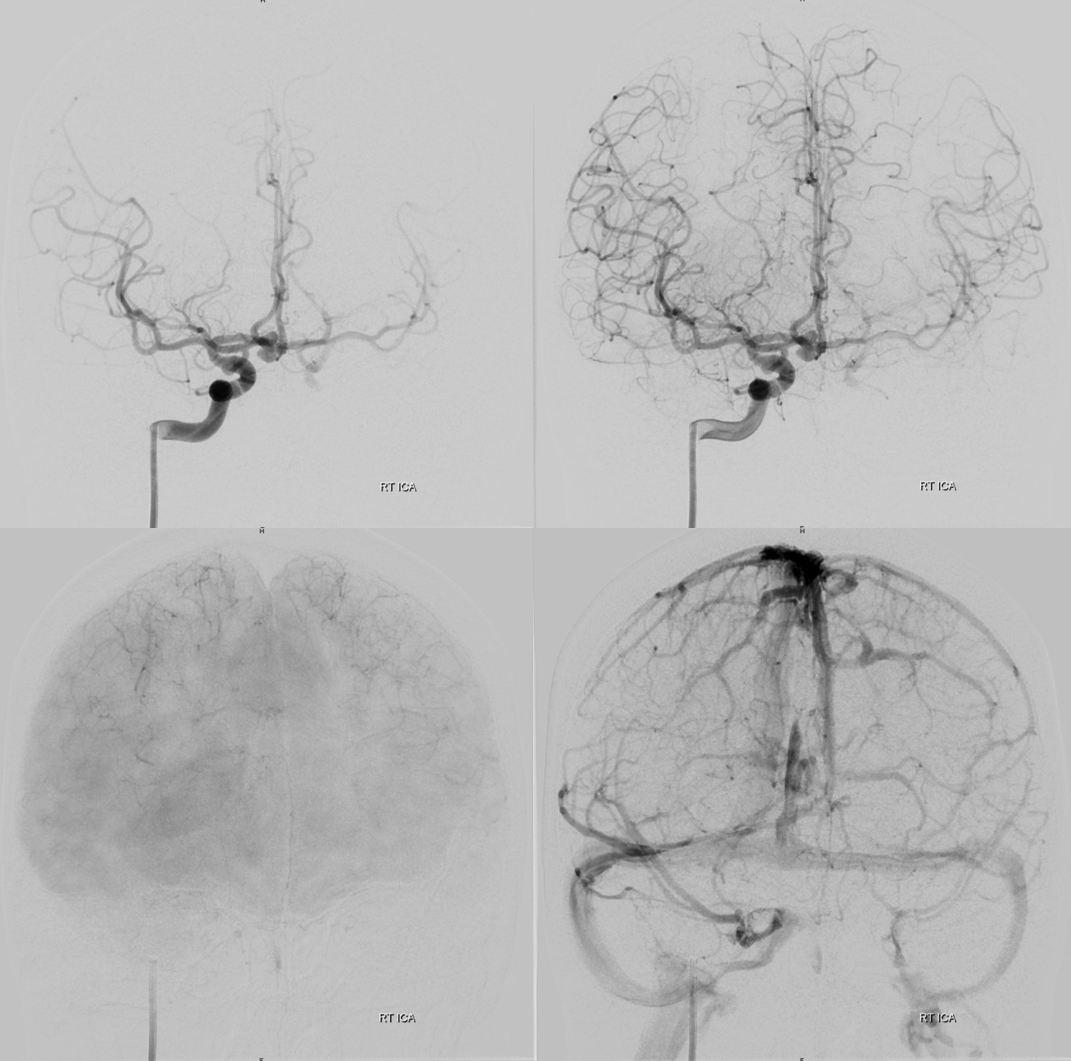
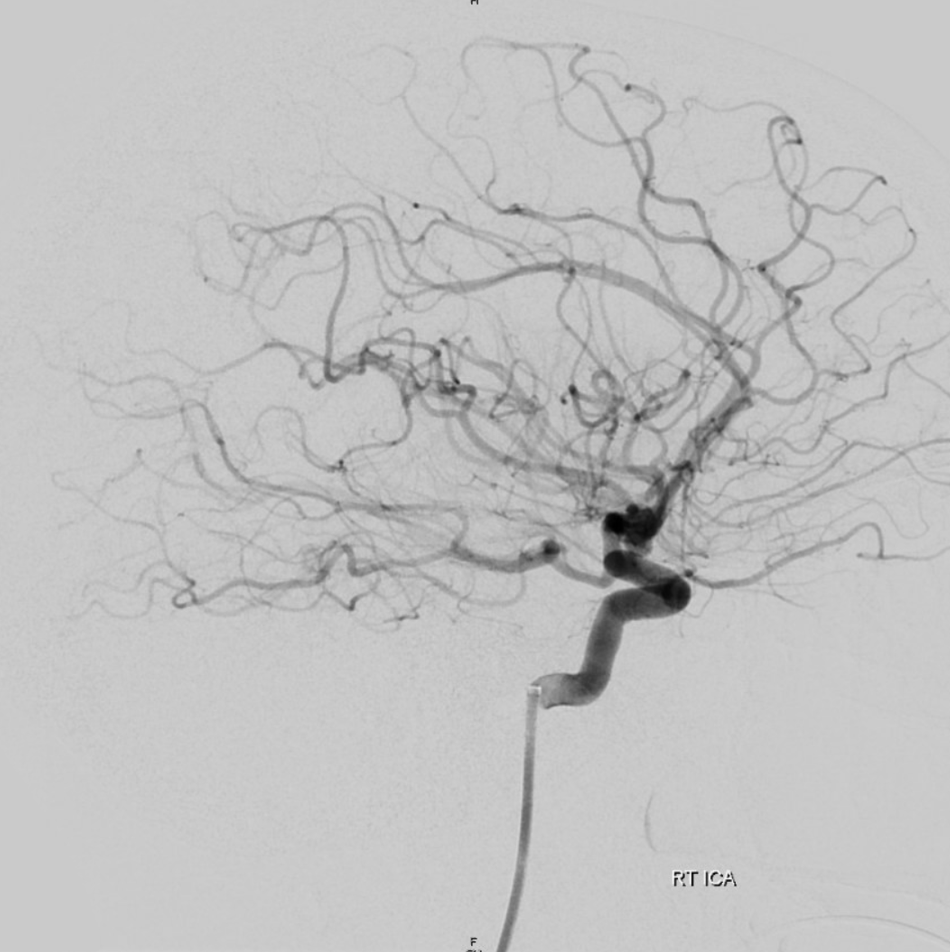
Ruptured ACOM
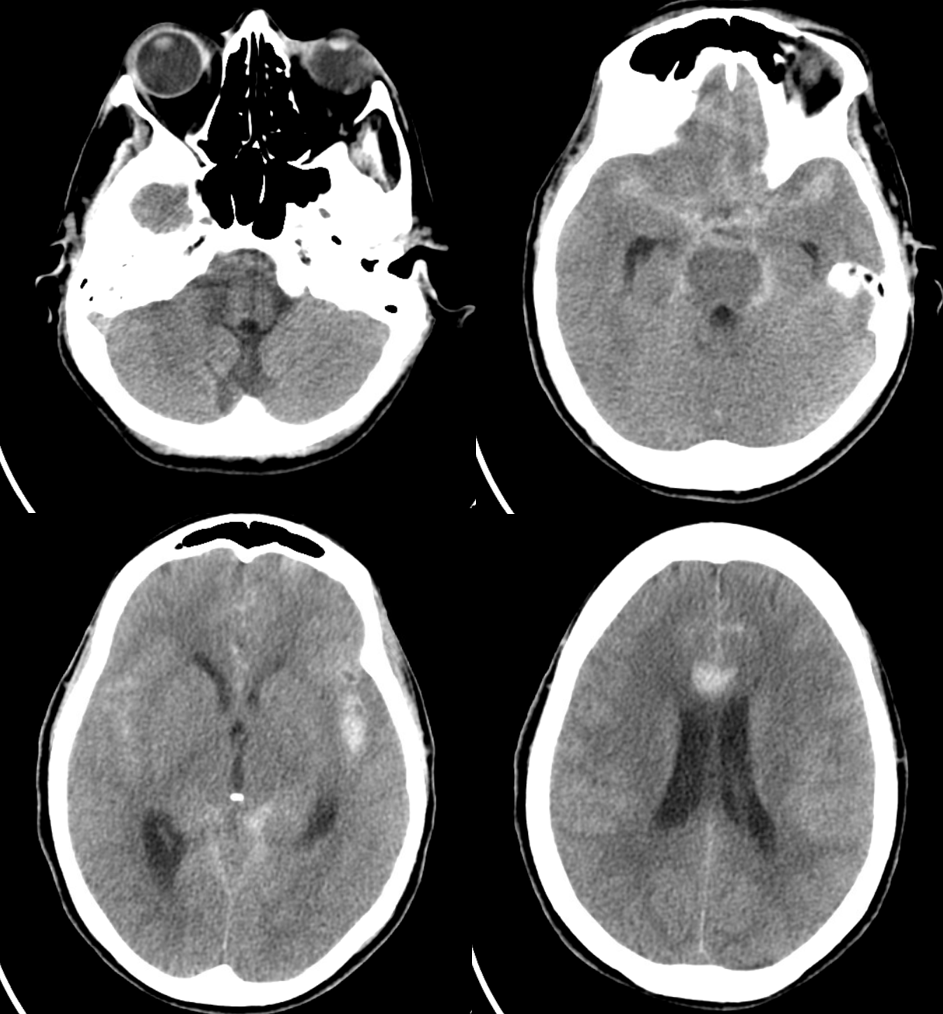
Bilobed. Left ICA is occluded. Which means the ACOM is under increased flow stress. And it must be preserved for many reasons, including smallish PCOM, future spasm.
Plot sickens even more…
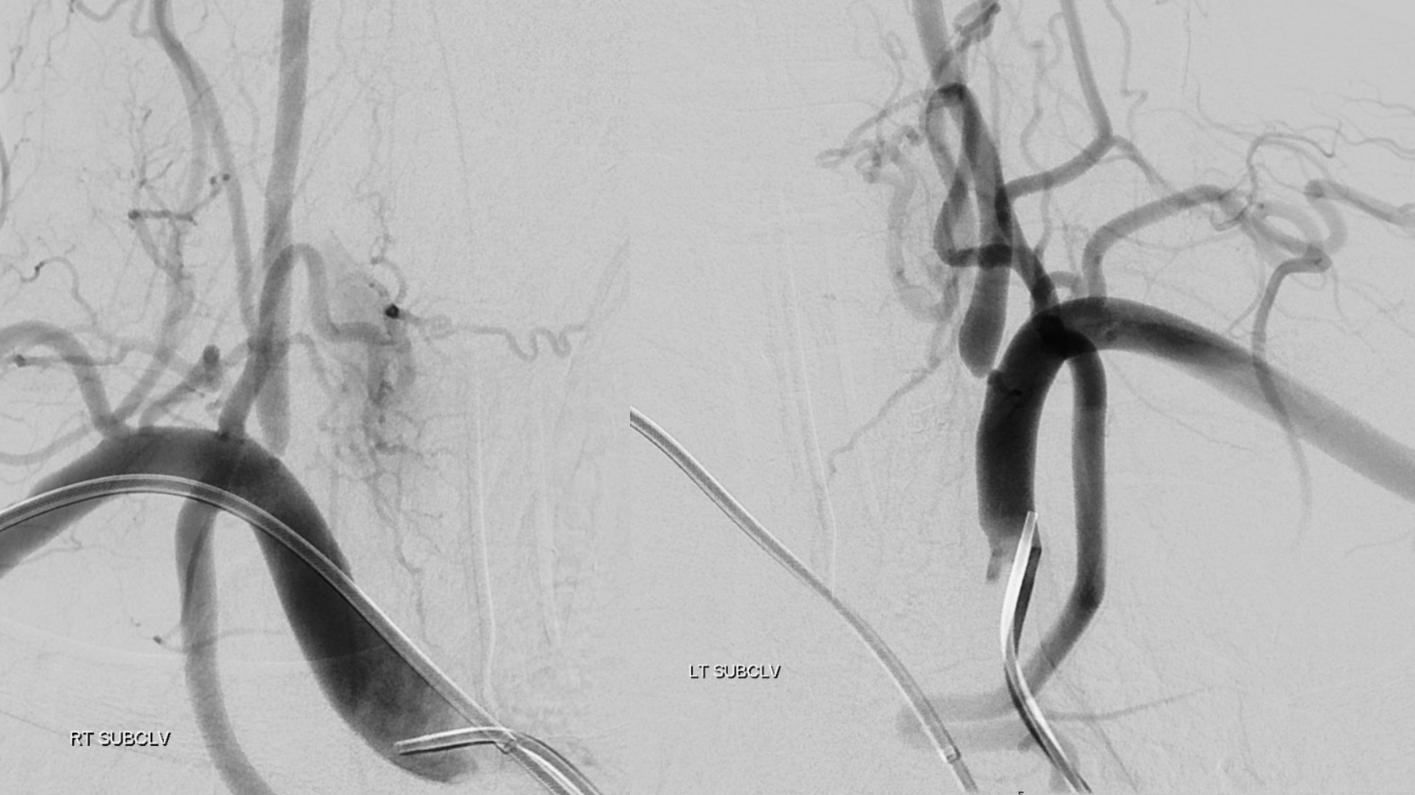
The left CCA is occluded also, with primary inferior thyroid to superior thyroid ECA reconstitution. The ICA is also occluded.
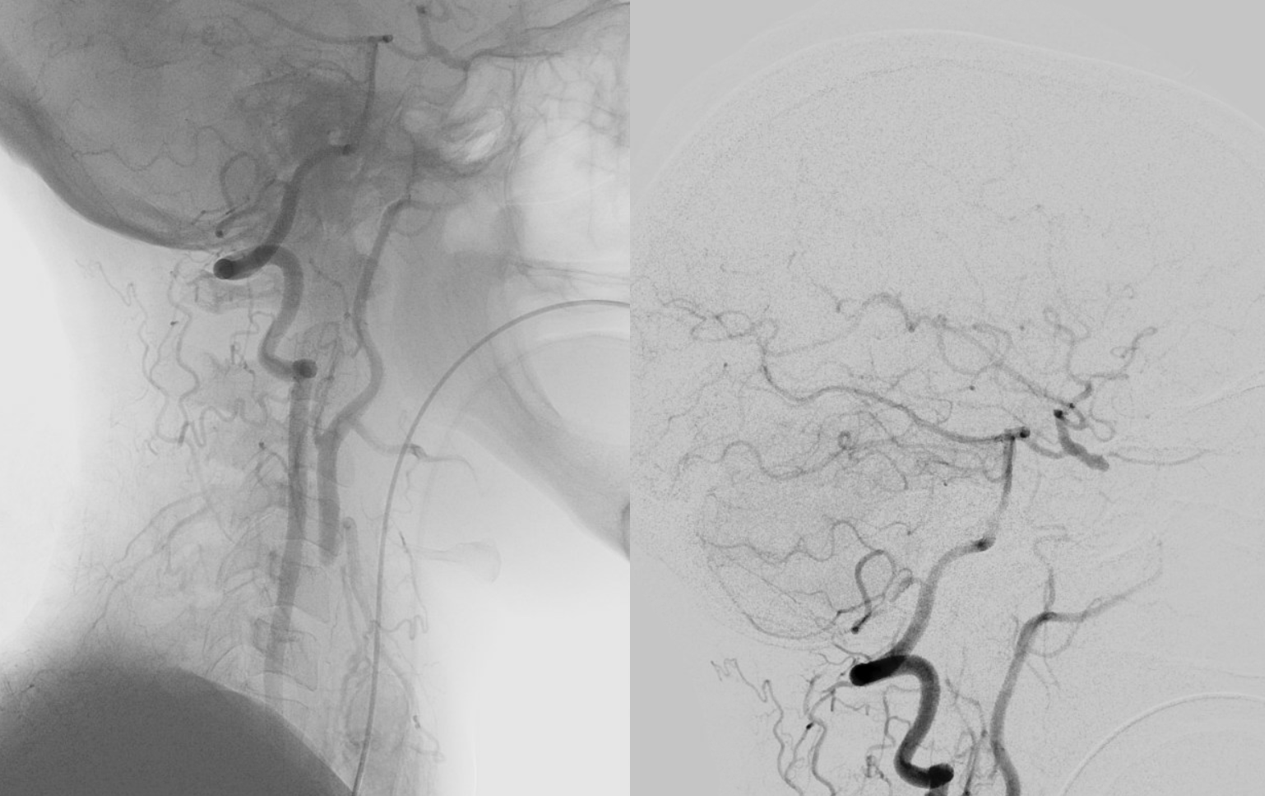
Despite very sick bilateral verts, the posterior circulation continues to support the left MCA… Also note antegrade flow in the ophthalmic — which means the left ECA must have other occlusions or it would have reconstituted the ophthalmic regardless of CCA occlusion
BTW, the iliacs are also occluded. This is a right radial access benchmark in the ICA
Rotational angio — stop and scroll thru individual frames
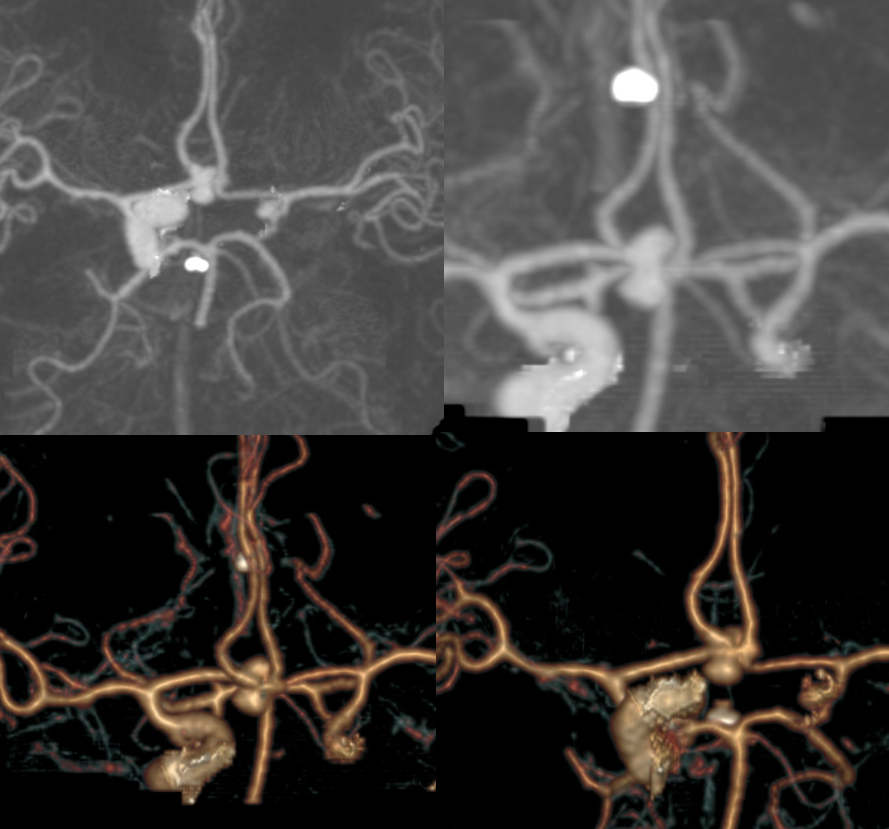
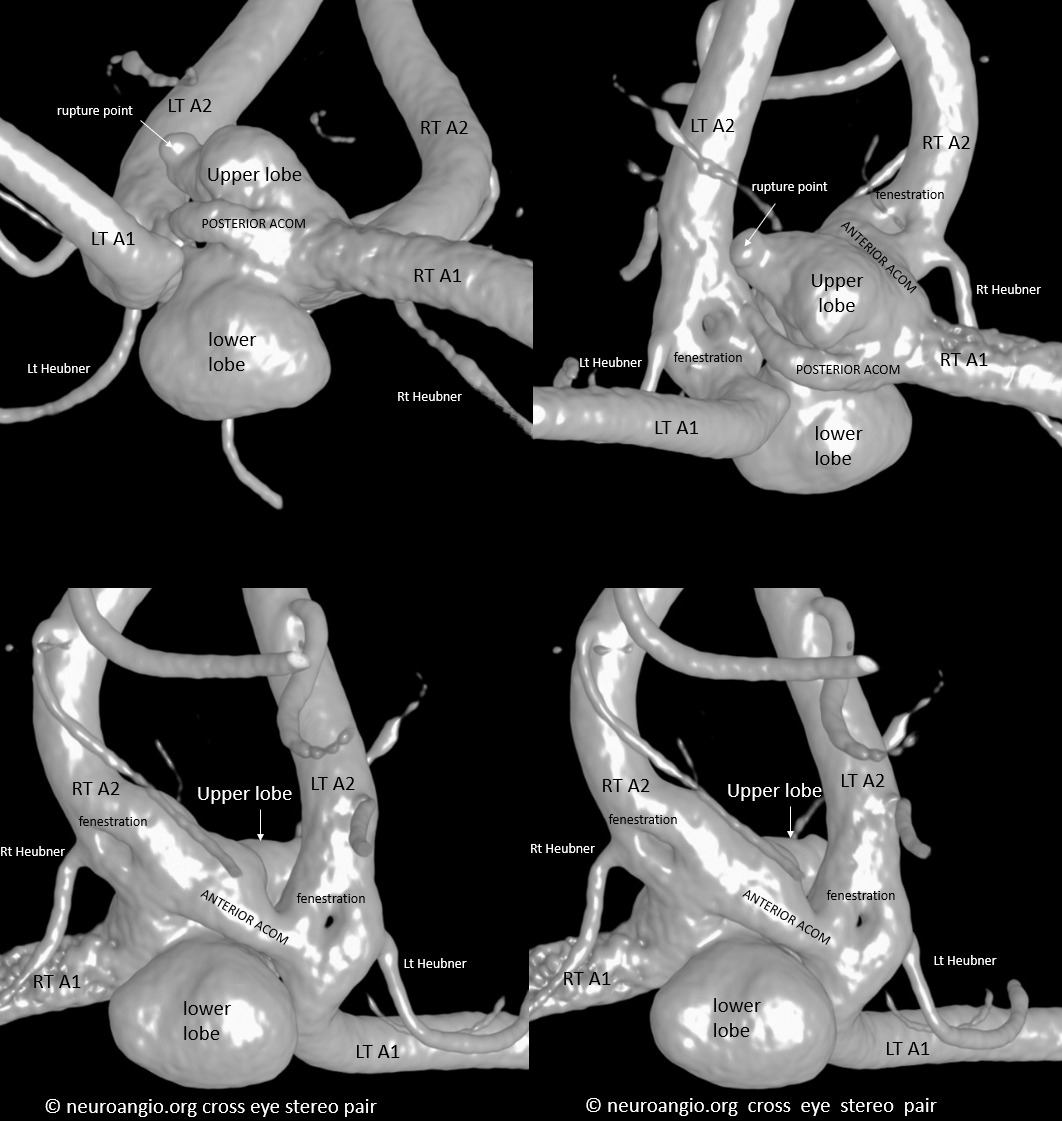
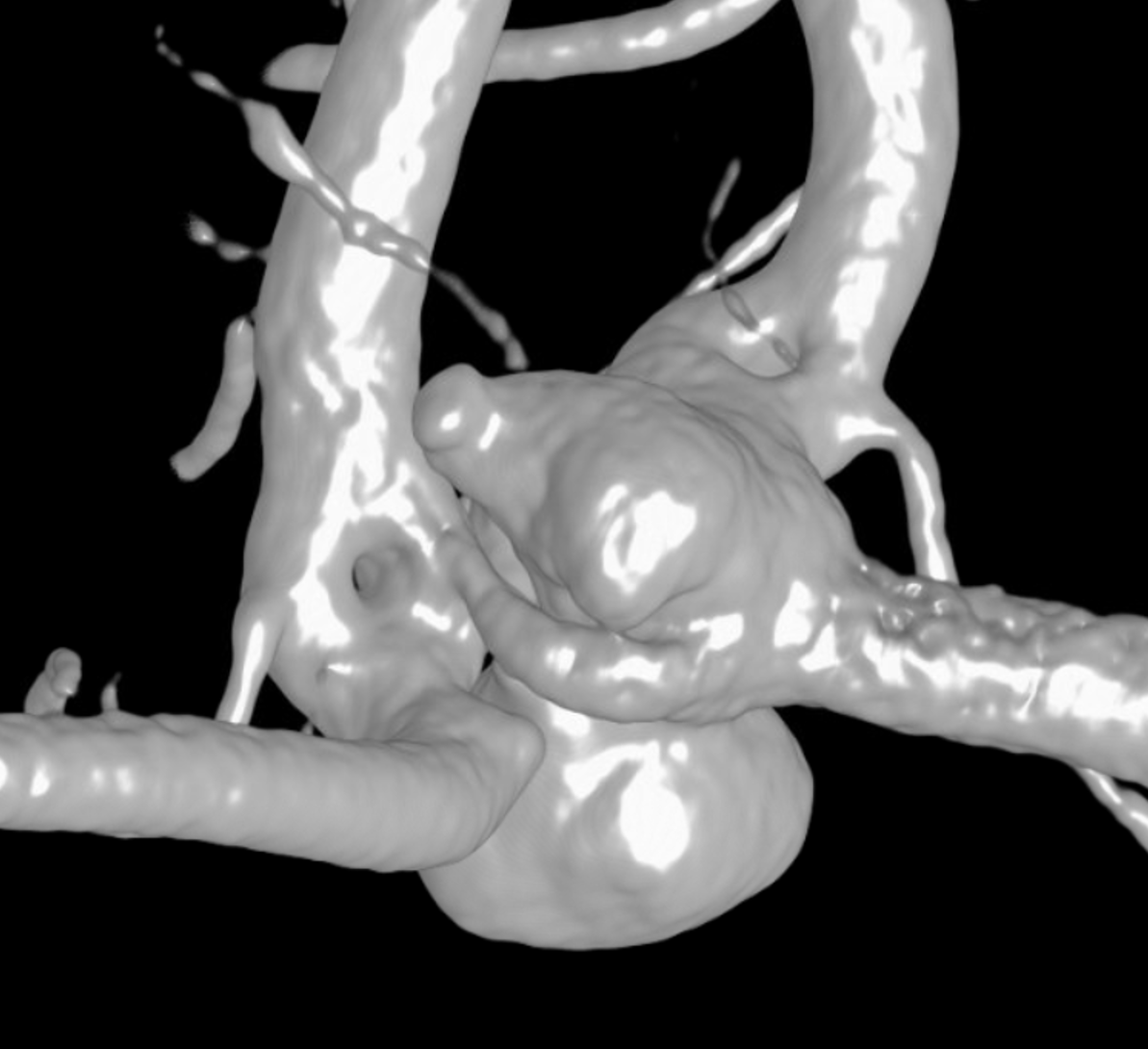
Crazy, huh. Eytan insisted on getting a DYNA CT — and it paid off hugely. Look at this amazing DYNA. Its impossible to decide how to treat an aneurysm like this without really understanding the anatomy.
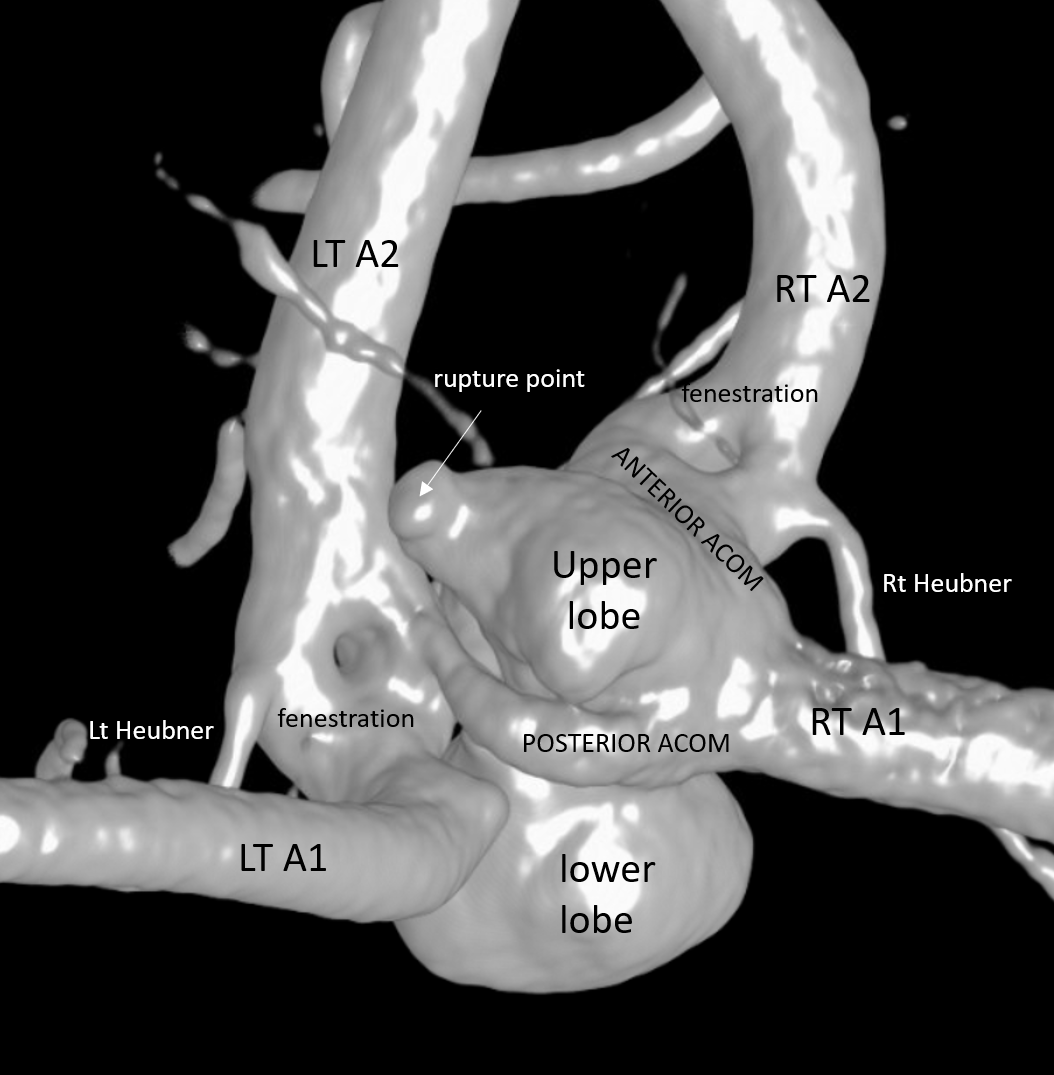
The aneurysm is figure 8 configuration. The lobes are connected along the waist of the 8. The rupture point is at the upper lobe, along principal A1 flow vector. There are TWO ACOMS — larger right and smaller left one. There are also TWO fenestrations of the proximal A2s.
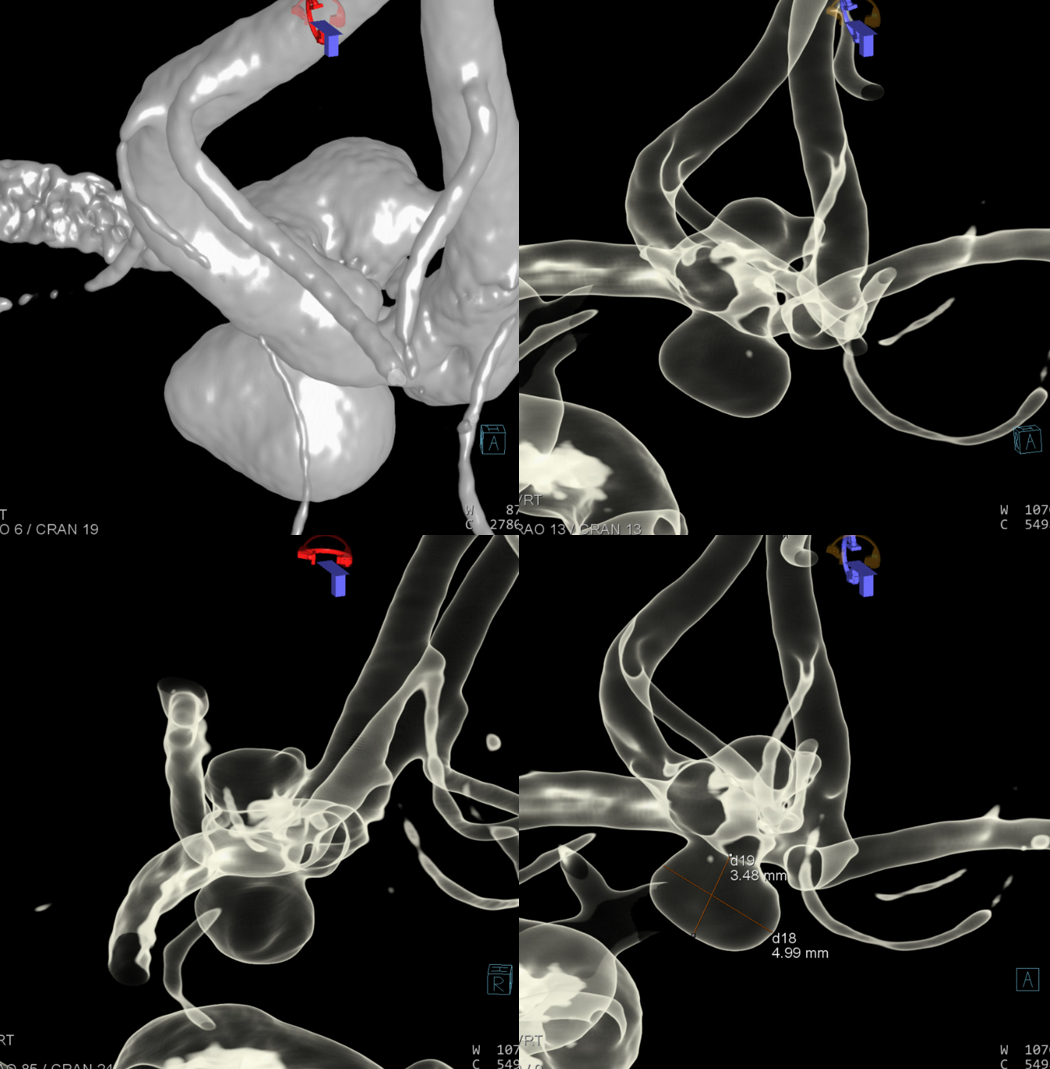
The LOWER set of images are stereo pairs
Single best image to see everything
Without text — view from posterior
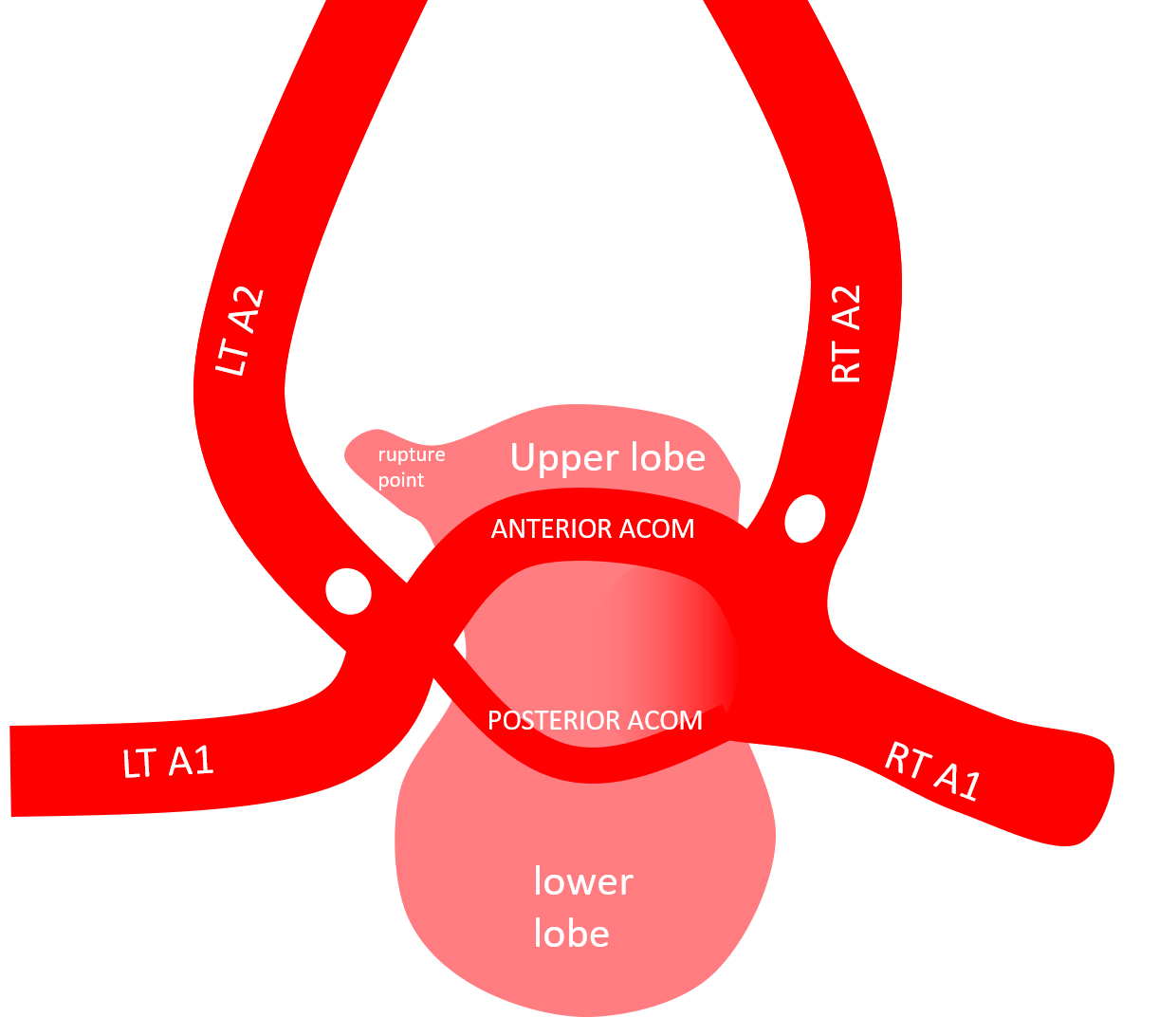
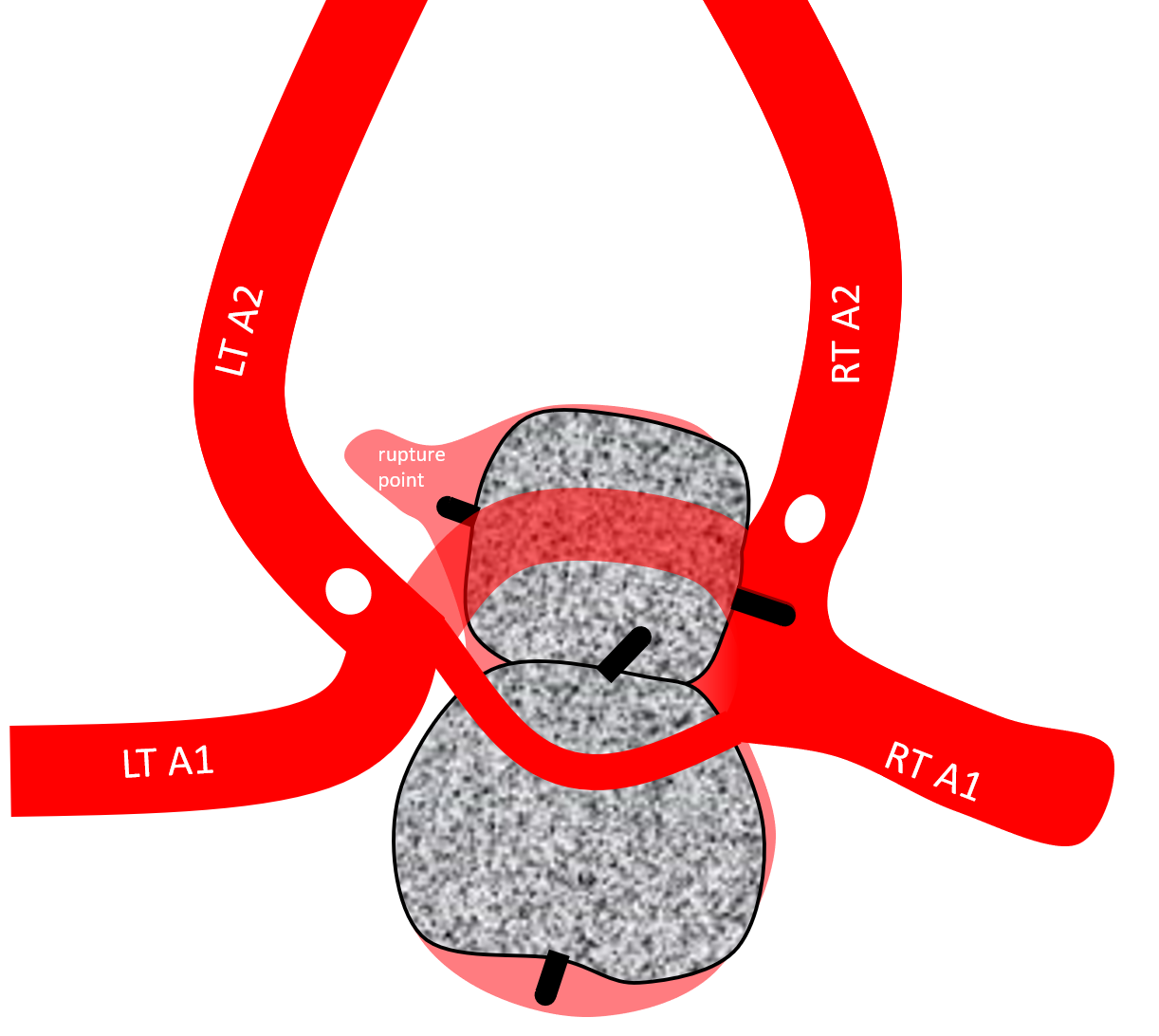
Finally, a simplified schematic — view from posterior
Treatment video — stop and scroll thru individual frames — by far the best way to see this
For planning — especially to understand projections and safety zones, translucent recons are key — they are hard to understand in isolation, but extremely helpful in real time
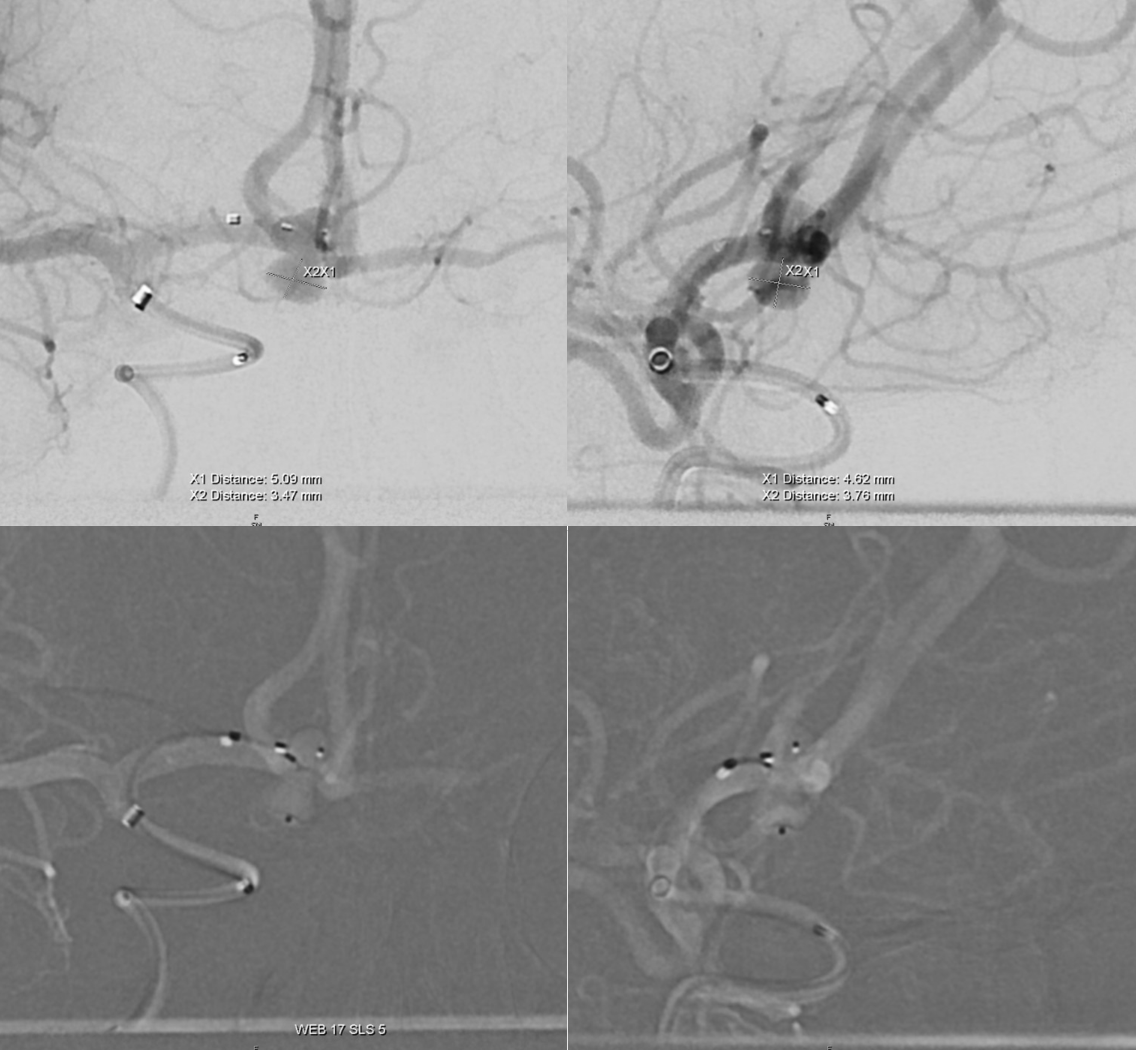
We attacked the more challenging, shallower upper lobe first, thinking that if it didn’t work, we would go for clipping. What helped a lot is the bottom of WEB sitting in the waist between the two lobes.
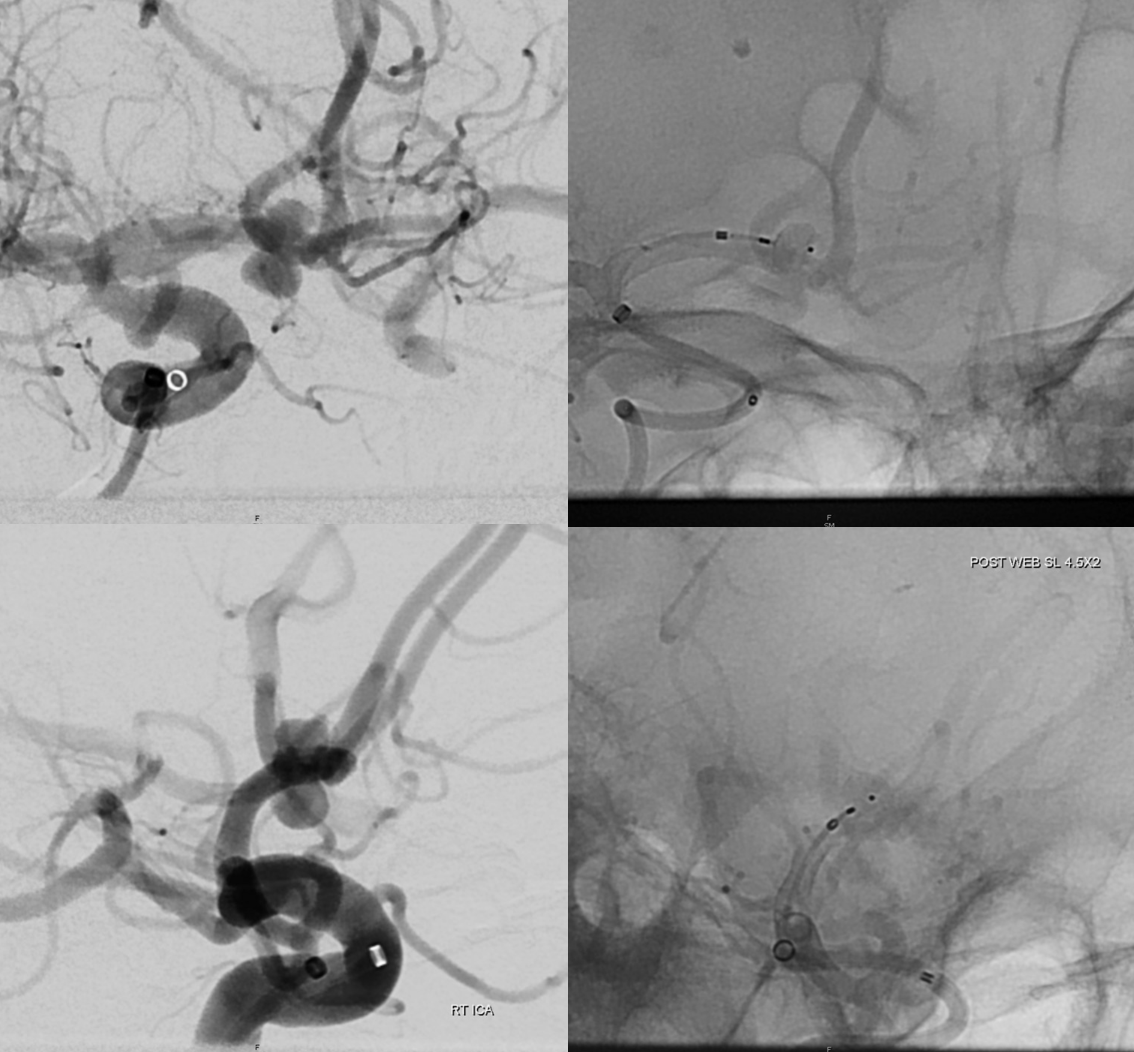
For the lower lobe, an SLS seemed like a better choice. It was slightly oversized, but rotated nicely to sit up against the bottom of the upper WEB
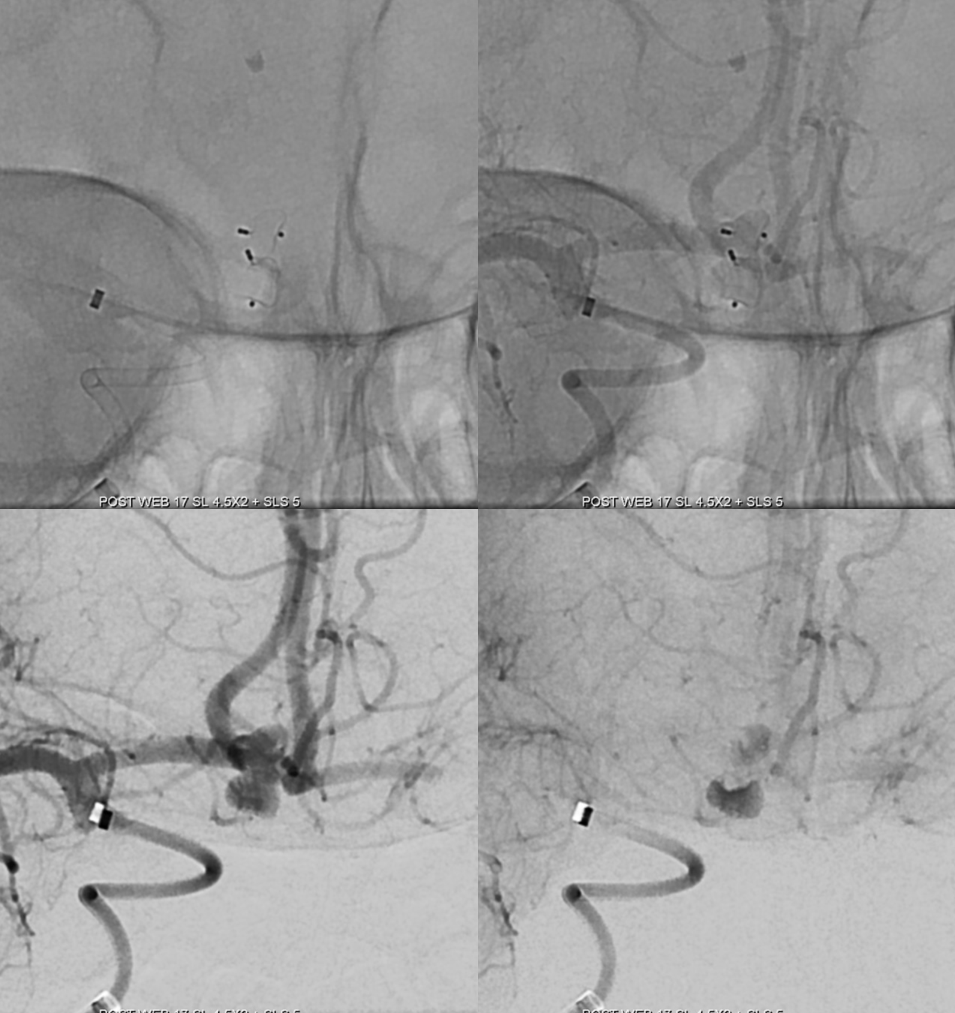
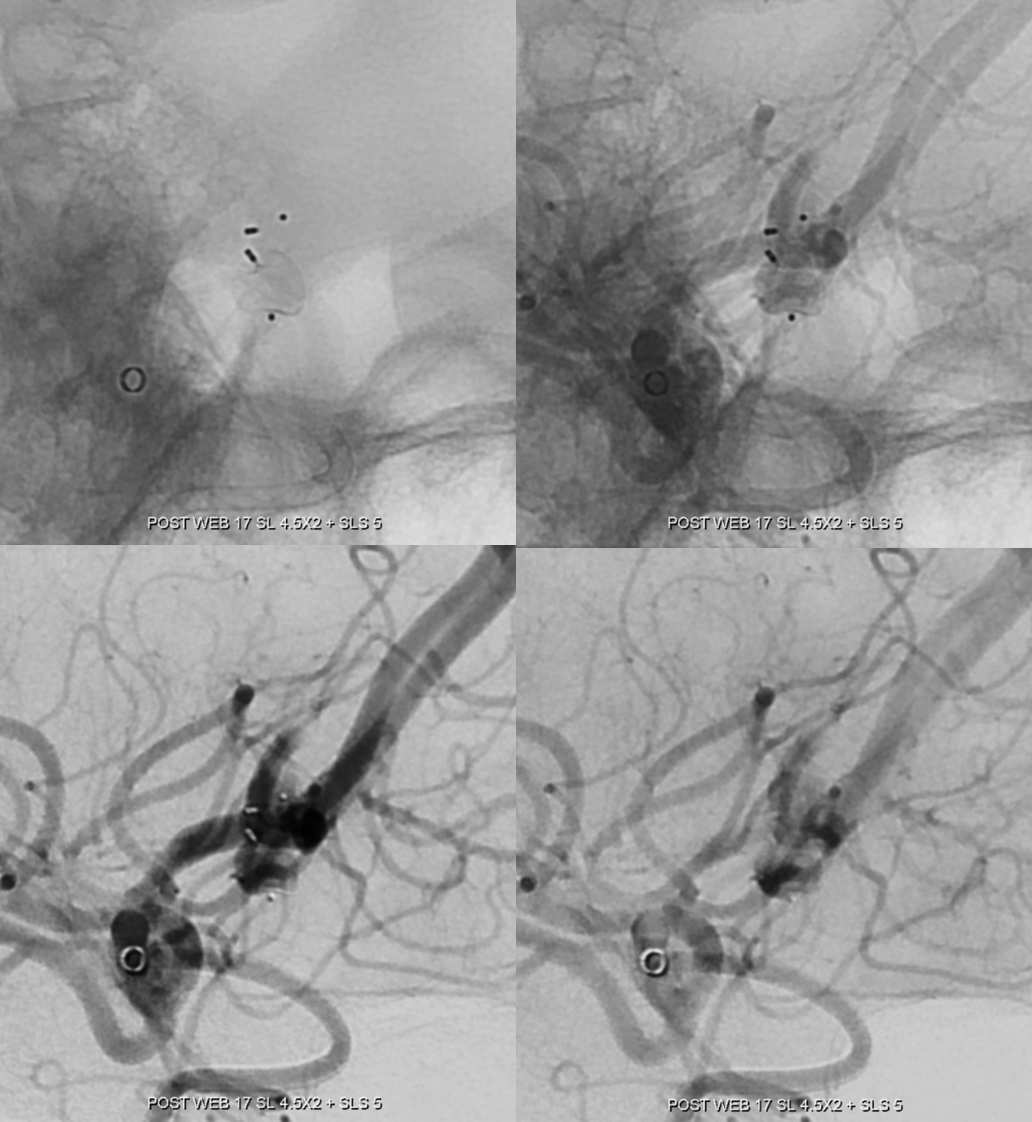
Post
Post schematic
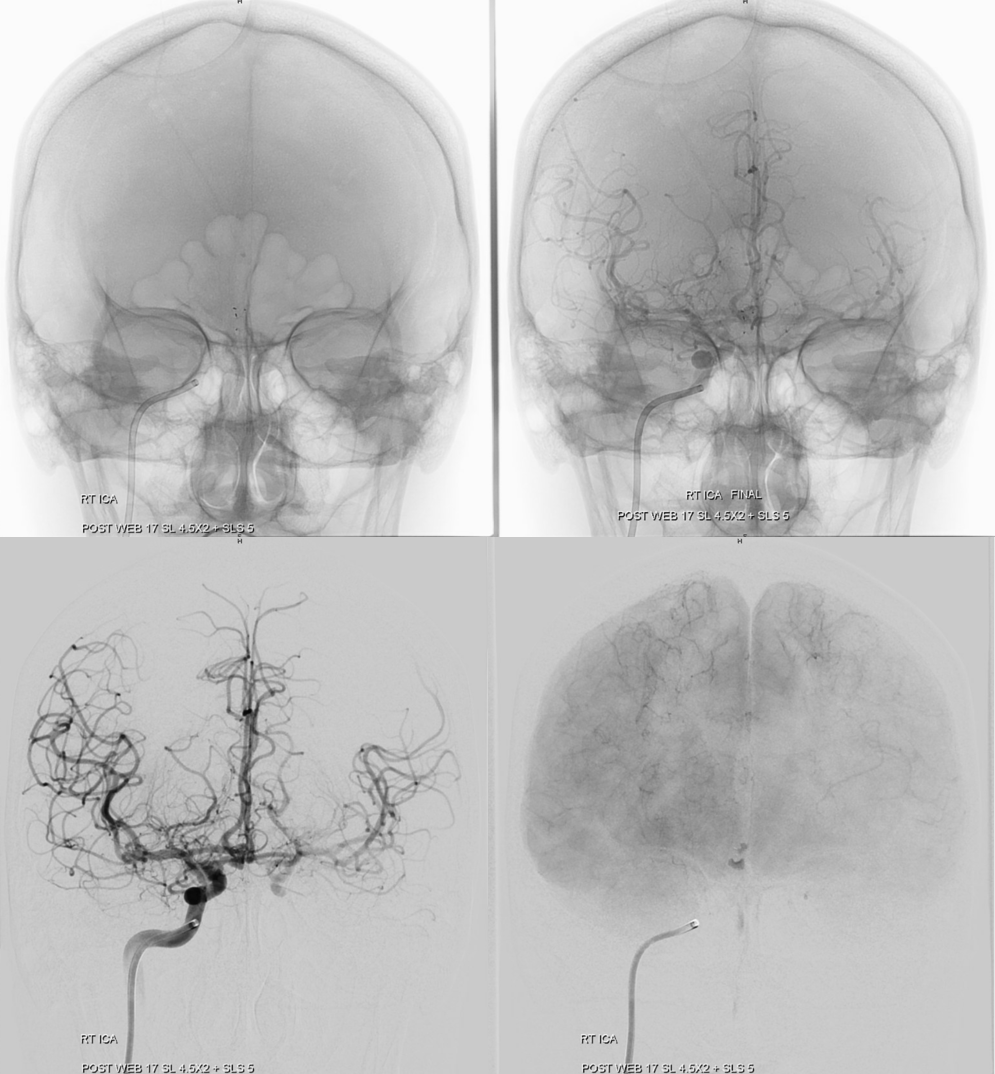
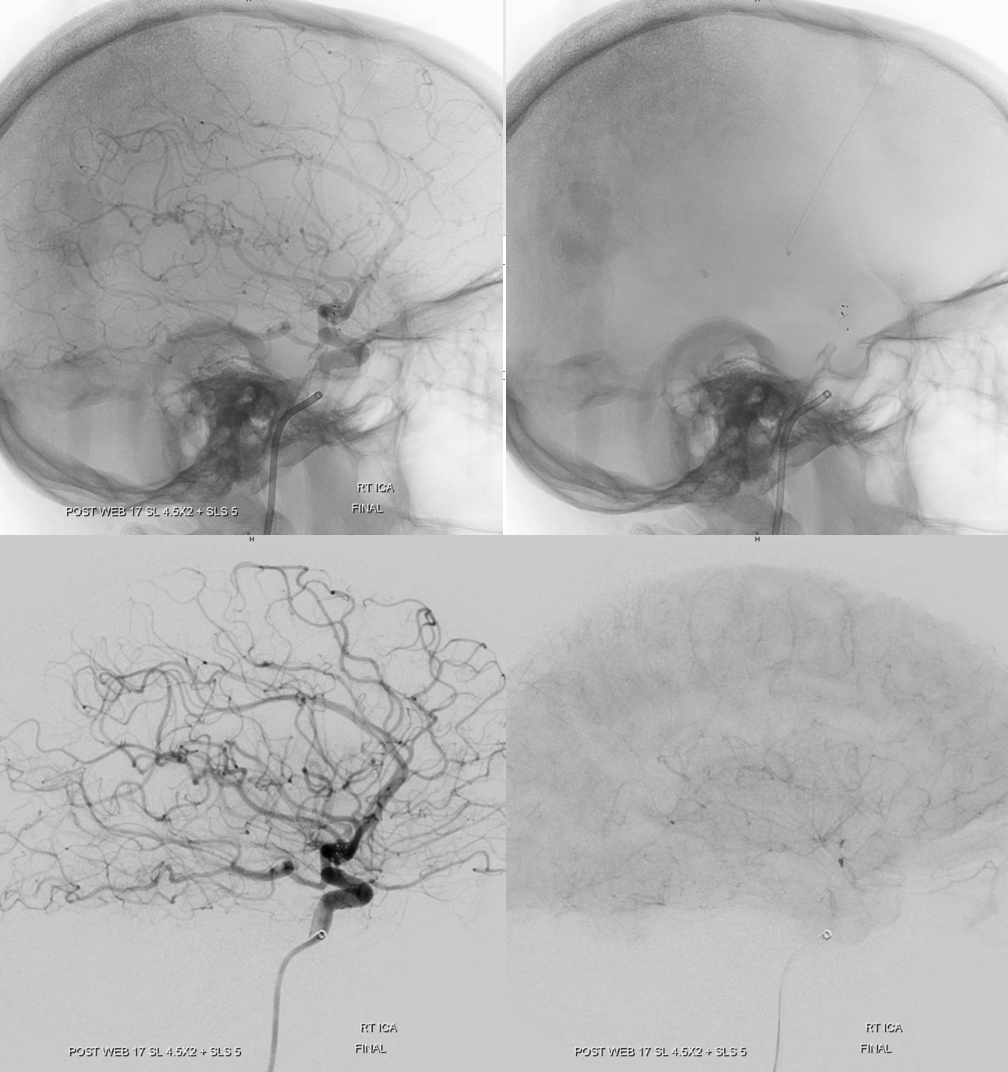
Treatment of this kind of aneurysm is not be possible without detailed understanding of the anatomy provided by the DYNA, whether is WEB or surgery. Knowing how to maximize use of angiographic equipment is not only art — its best practice, and everyone needs to know how to do it.