Excellent case of advanced stroke management. Presentation is left MCA syndrome. There is an old, likely balloon-mounted stent in the left ICA — thrombosed. Morphology of ICA bifurcation suggests thrombosis is chronic
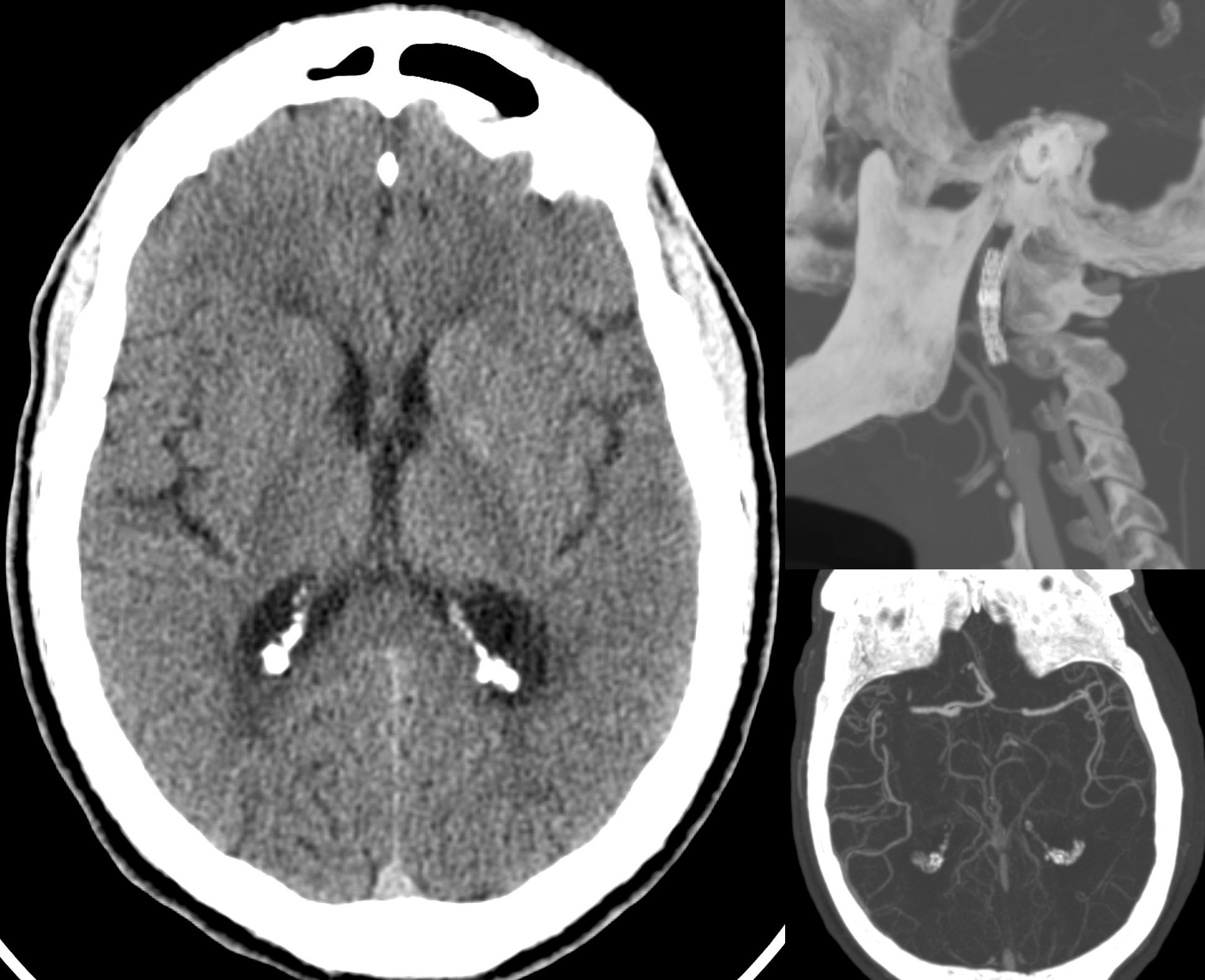
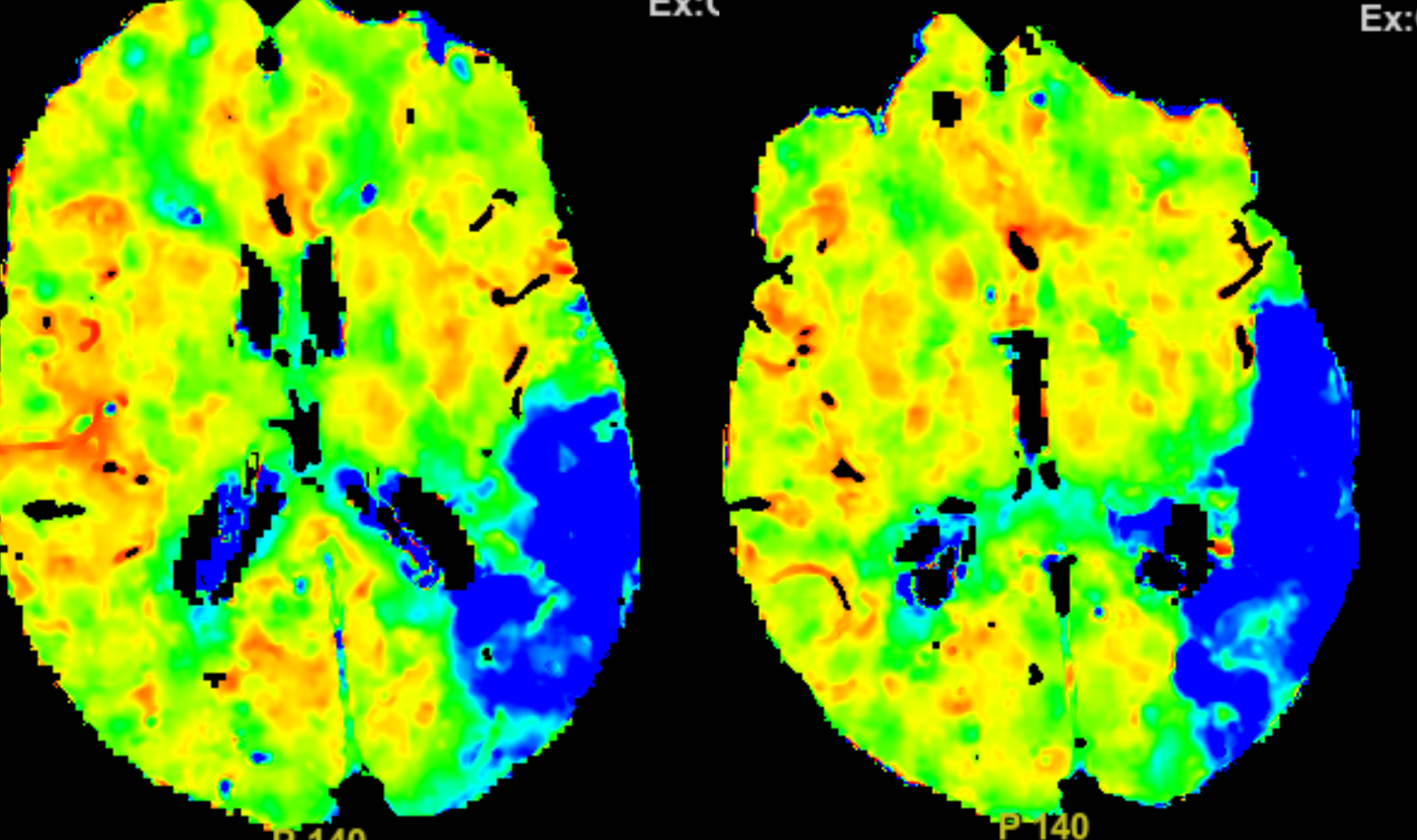
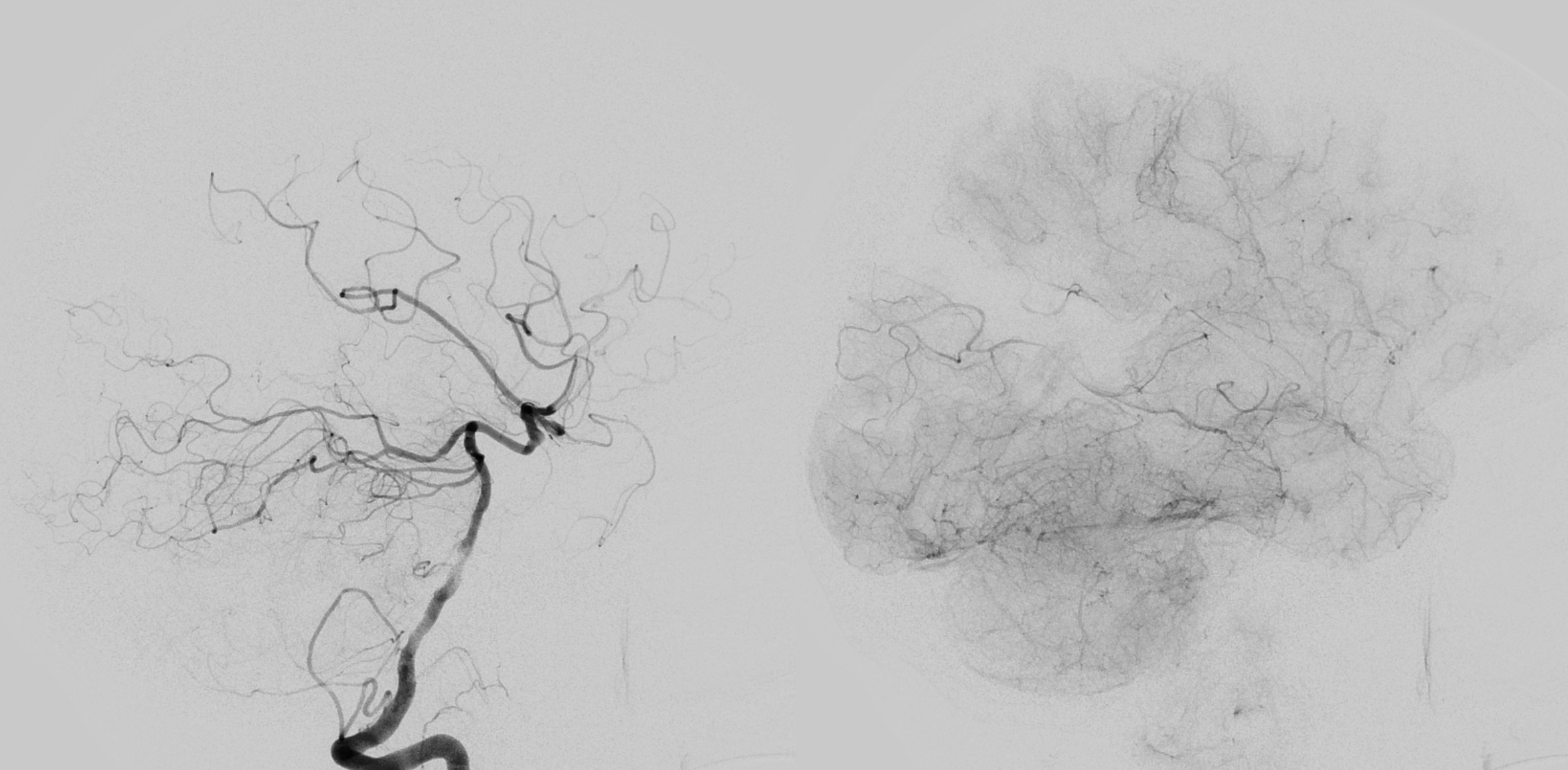
Perfusion as diagnostic tool — it doesn’t matter what maps therese are really (its Tmax). The point is that there is an arterial occlusion with preserved brain on CT. The role of perfusion is to show where occlusion is, especially in complex cases and distal location. The rest of left MCA perfusion is “normal”, an indicator of chronicity of left ICA occlusion.
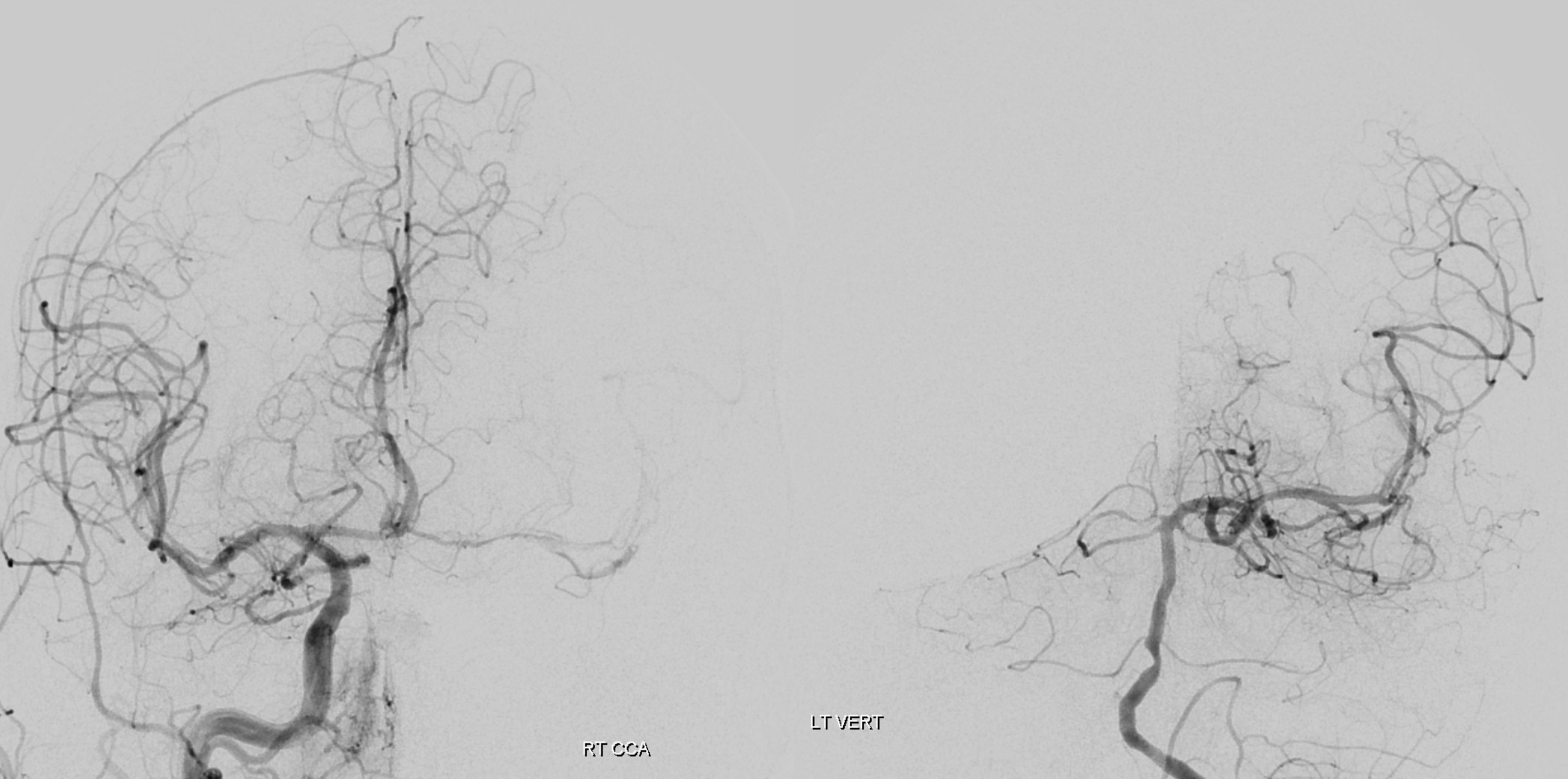
Left ICA — chronic occlusion. Accessory Meningeal and Foramen Rotundum reconstitution of the carotid via the ILT — look ’em up!

Left ACA mostly supplied through ACOM. The MCA via left PCOM. The large size of the PCOM, congruent with M1 segment, is also indicative of long-standing left ICA occlusion. The mid-basilar stenosis probably does not help, but is asymptomatic a the moment.
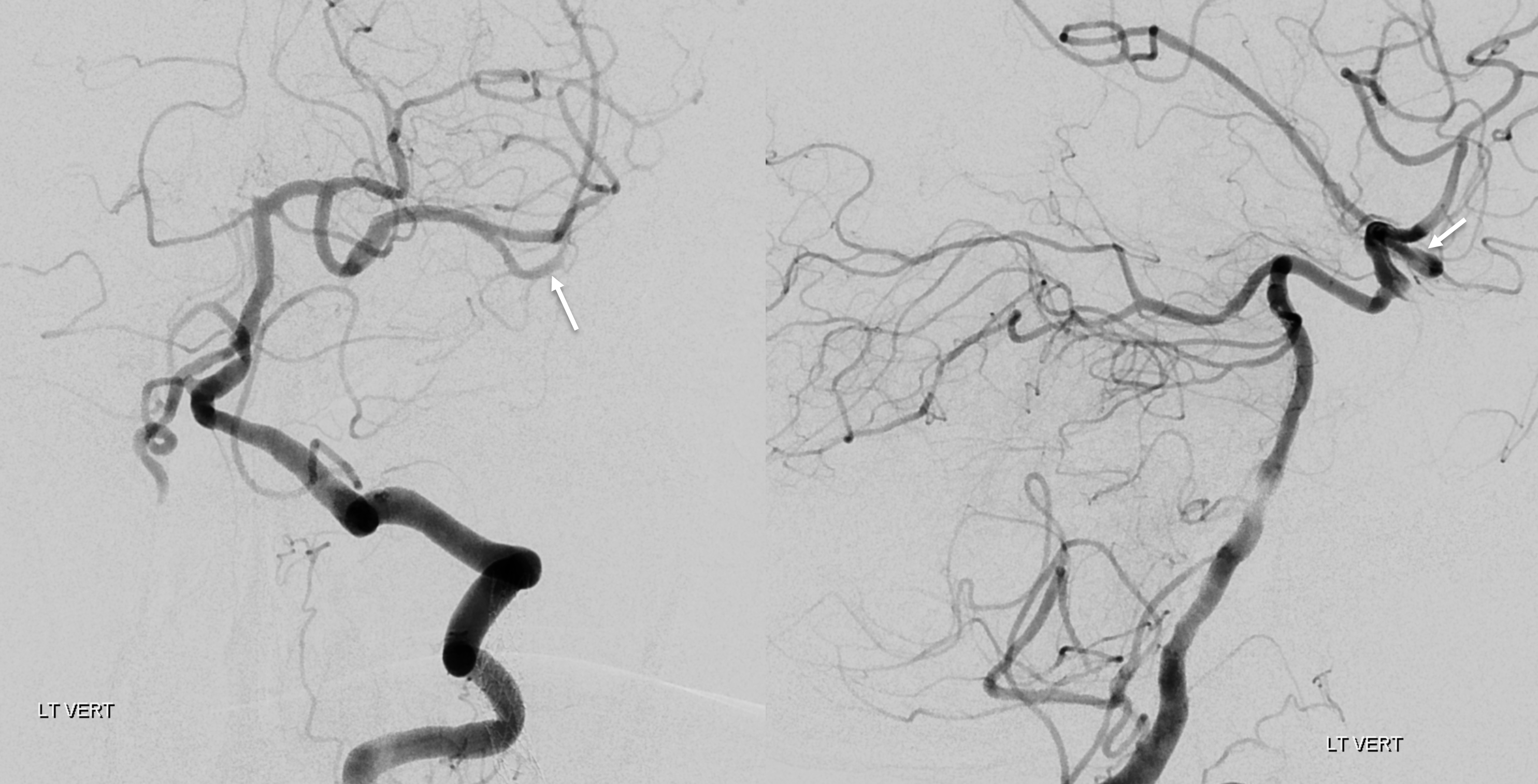
Working projection views — inferior division M2 occlusion (arrows)
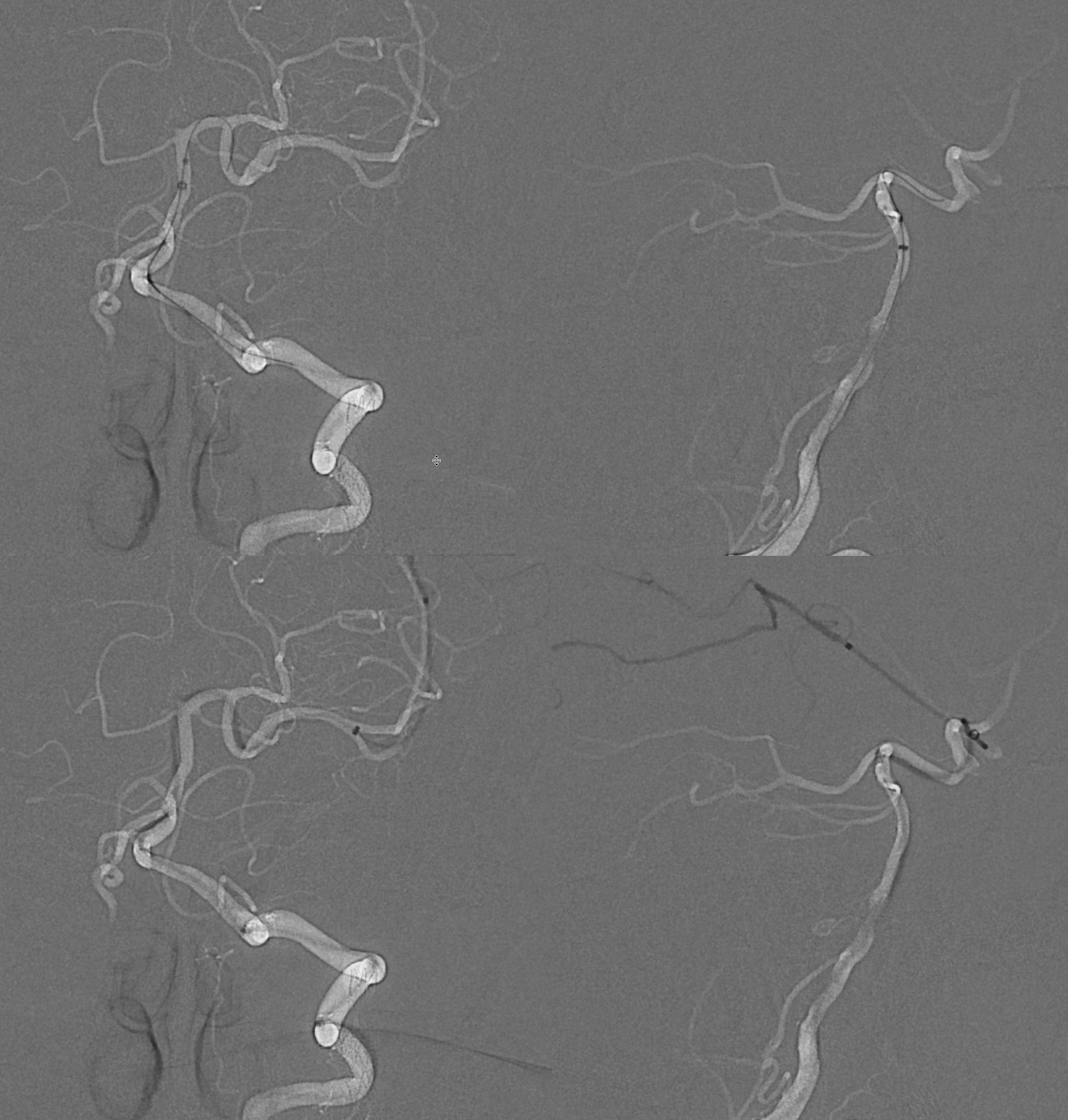
Setup is BMX 80, Sofia 5 125 cm, Marksman 160 cm, Aristotle 014 soft
The Sofia is extended as much as possible distally to aid in aspiration. Both Sofia and Marksman are aspirated. Even with atheromatous disease, as suspected here, aspiration doesn’t hurt if something is stuck on the Marksman. Here the sofia is at M1 bifurcation
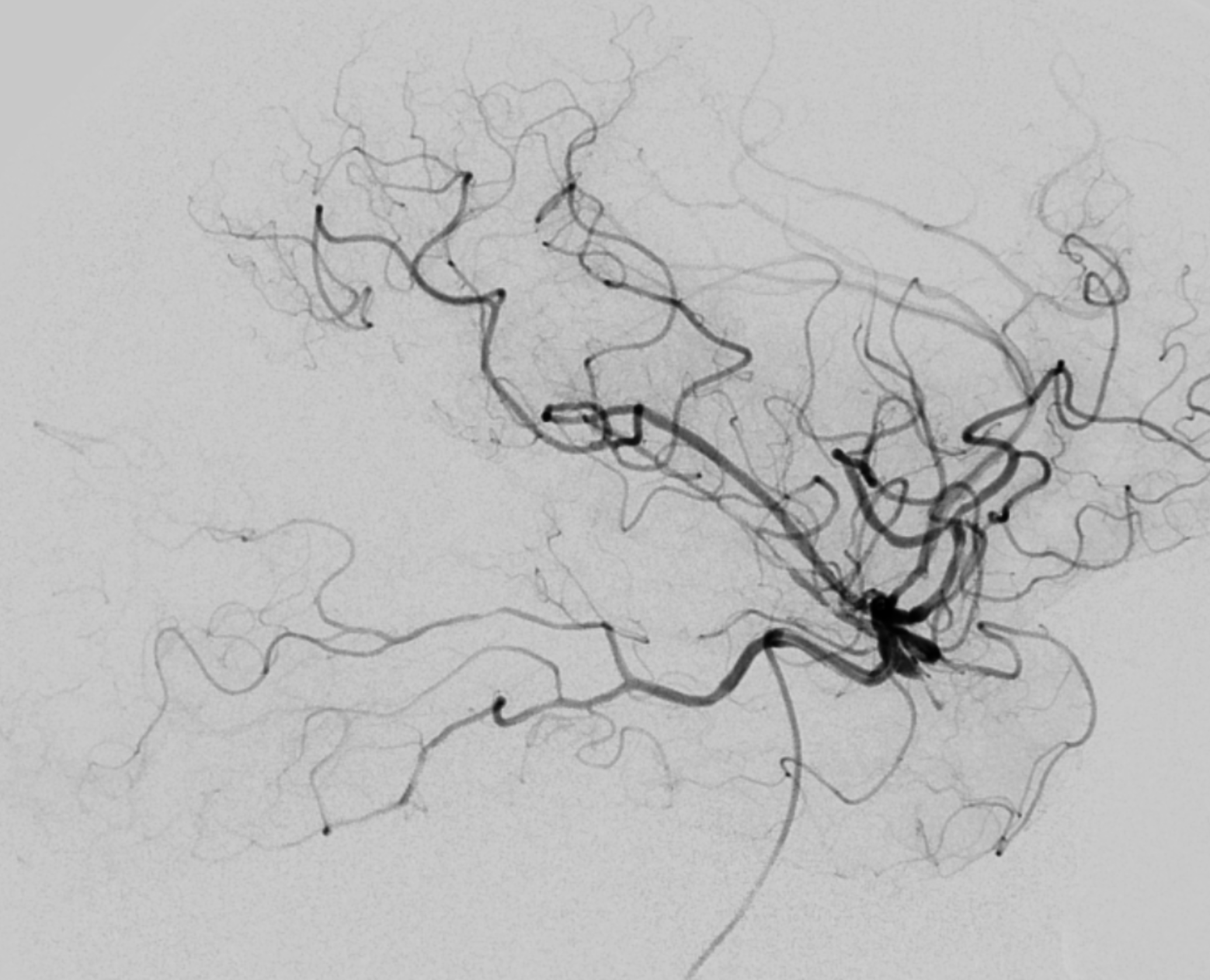
Post. Arrows show irregularity in the M2. Embolus or intrinsic disease?
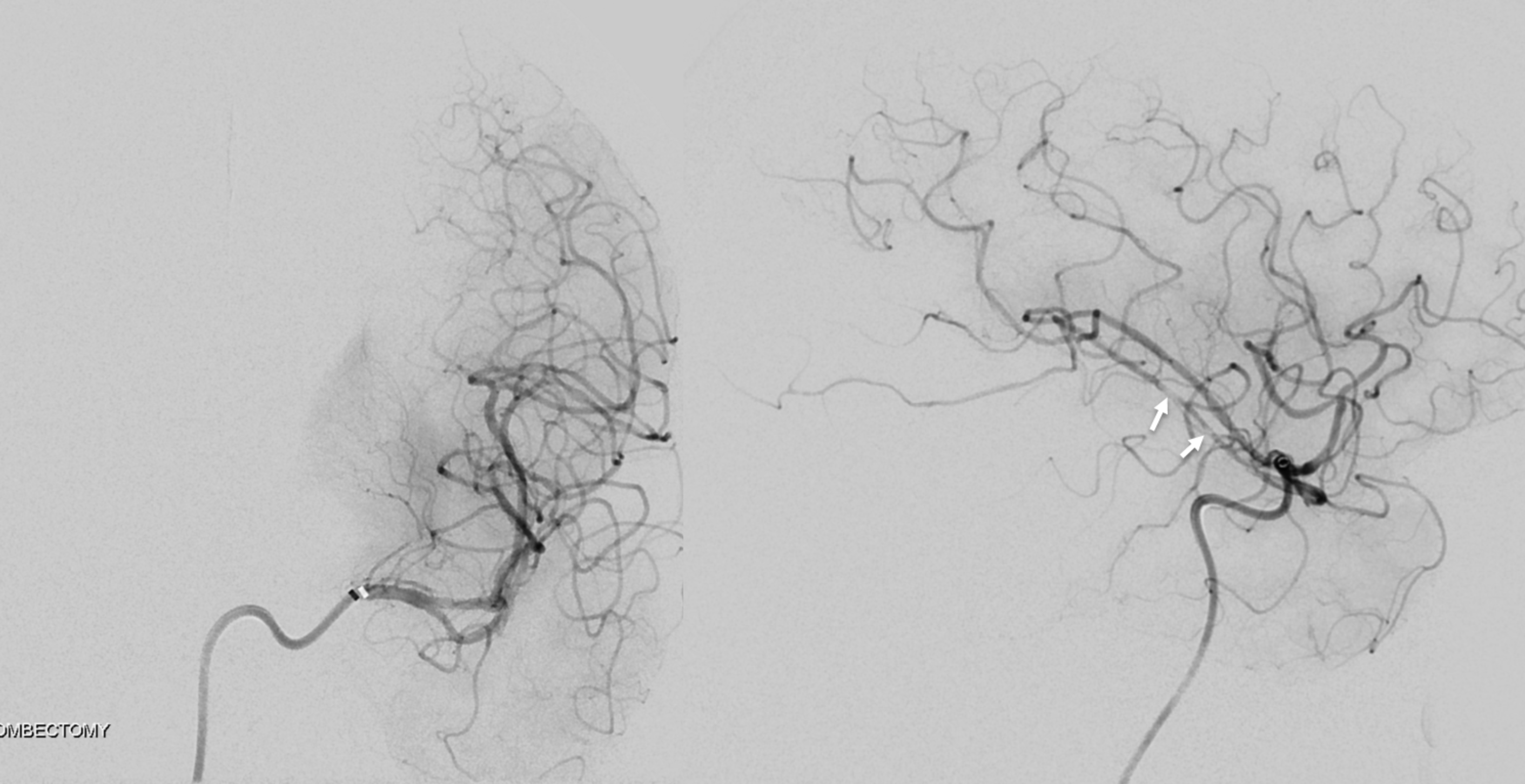
Several minutes later there is near-reocclusion. Could still be embolic, but overall unlikely.
IV integrilin is the way to go now. Takes a full loading dose but works wonders.
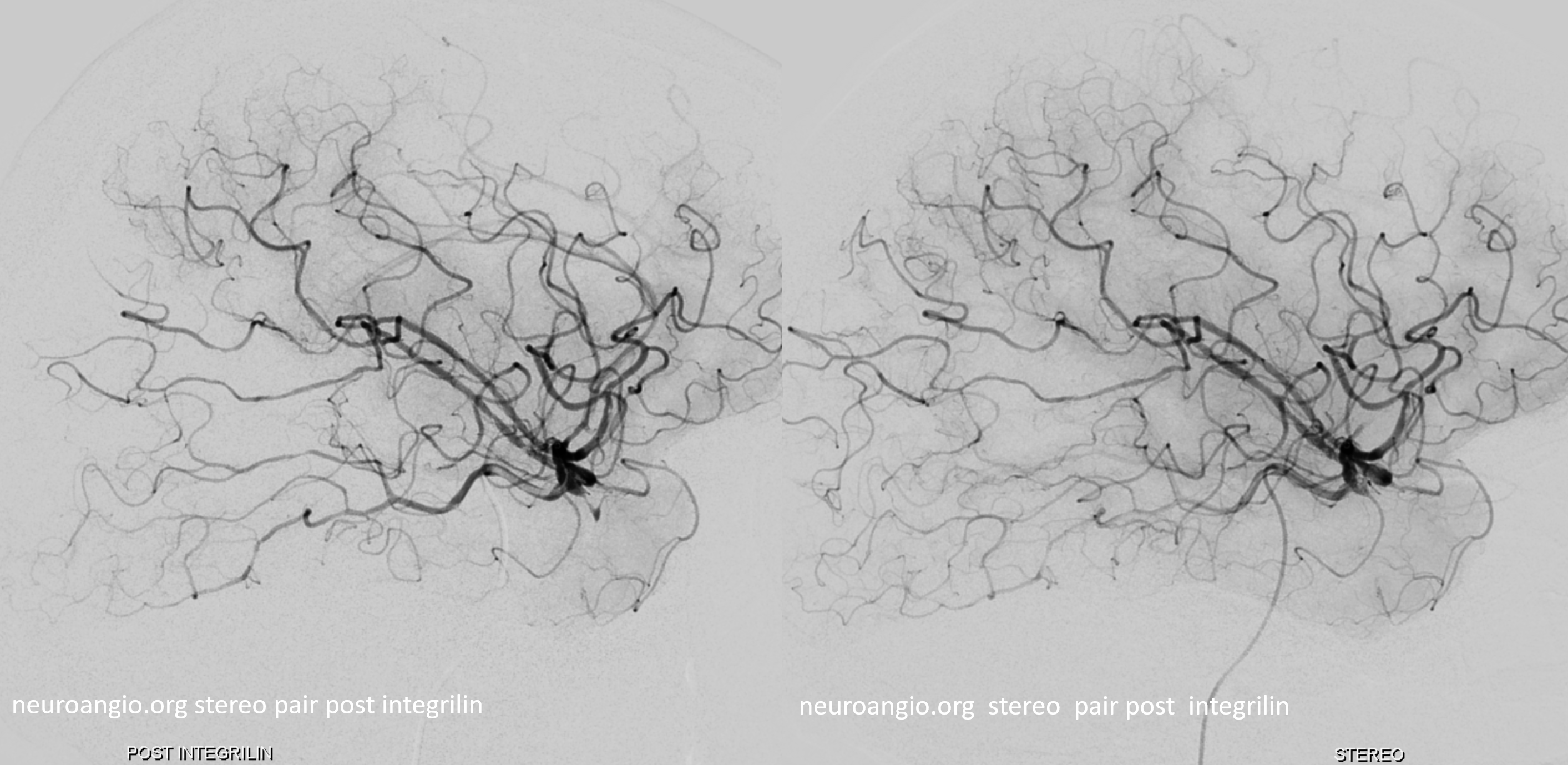
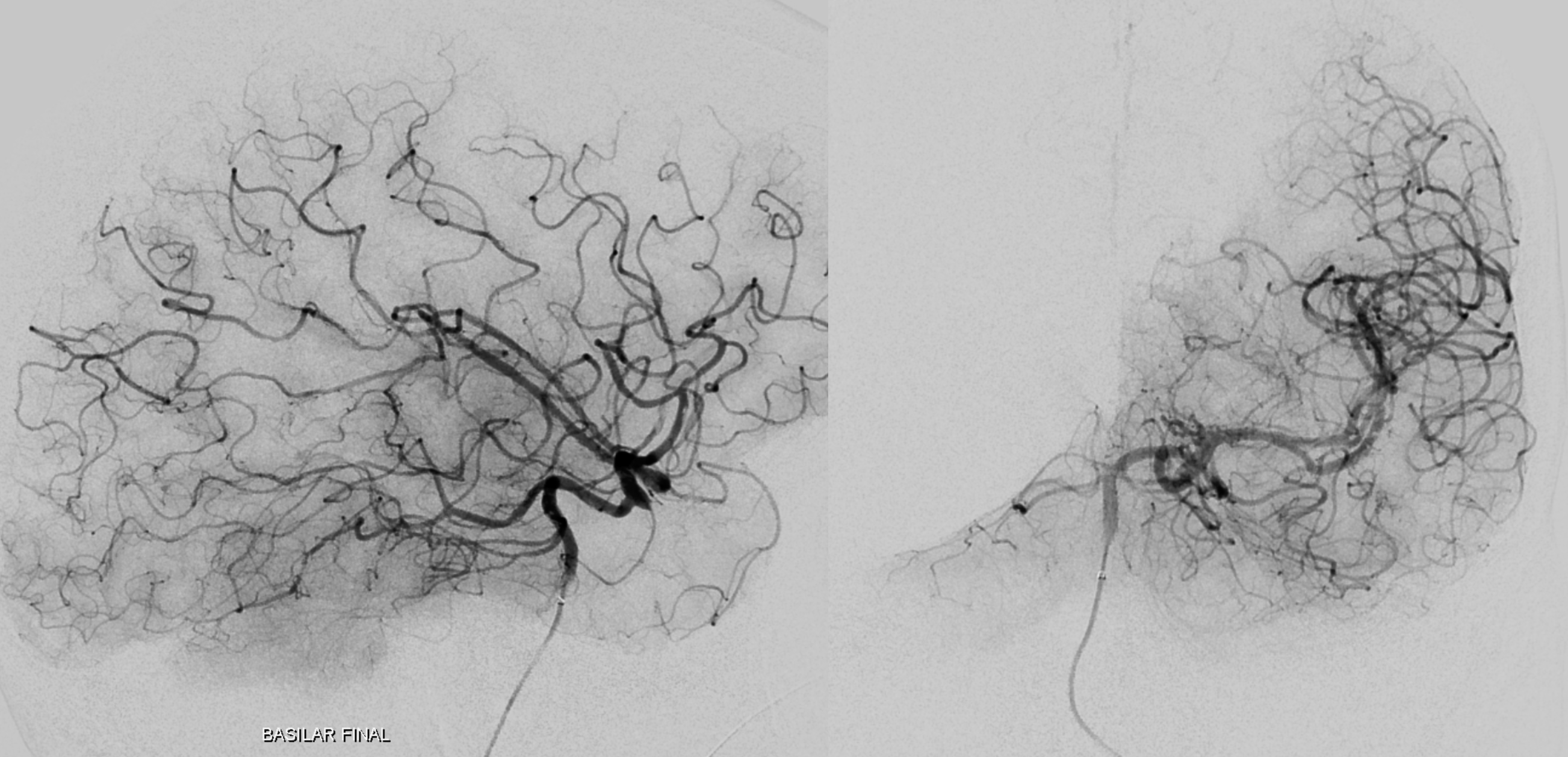
Final post