With Erez Nossek, MD
While the efficacy of spinal dural fistula embolization depends on permeating the “foot” of the vein associated with the fistula, safety is mainly a function of avoiding inadvertent embolization into arteries supplying the cord. Both anterior and posterior spinal arteries are important here — since liquid embolics are used. Proximal PSA occlusions can be well tolerated, however injection of liquid embolics into intrinsic cord arteries is likely to be problematic.
Identifying anterior and posterior spinal contribution to cord at or near fistula levels is key. Having one nearby doesn’t mean that embolization is impossible — see examples here and here. What it means is that we have optimal information to decide on treatment strategy.
Advanced Cone Beam CT / DYNA is extremely helpful in this task. Her is an example, presenting with typical dural fistula symptoms.
Adamkiewicz is from T10
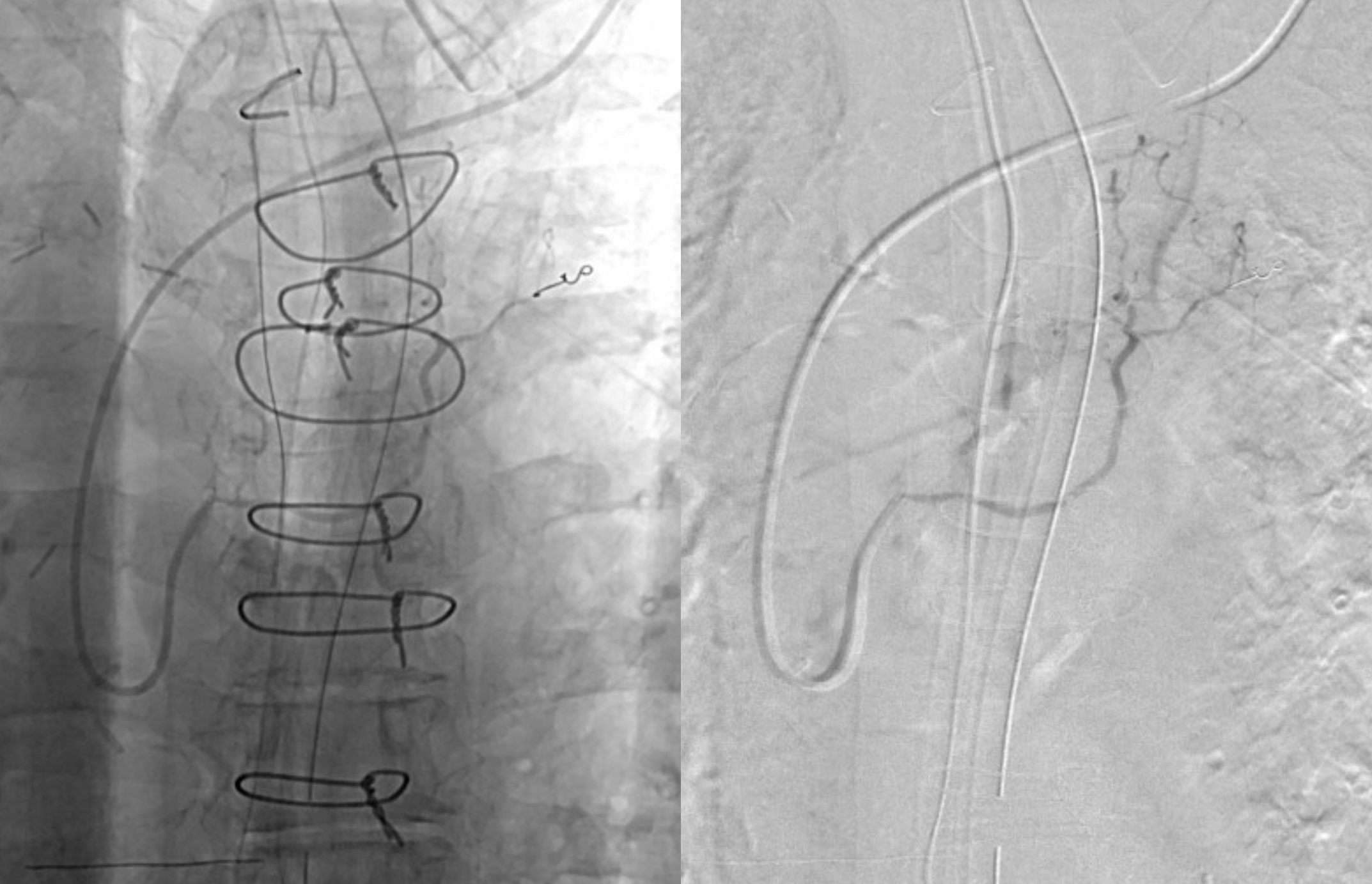
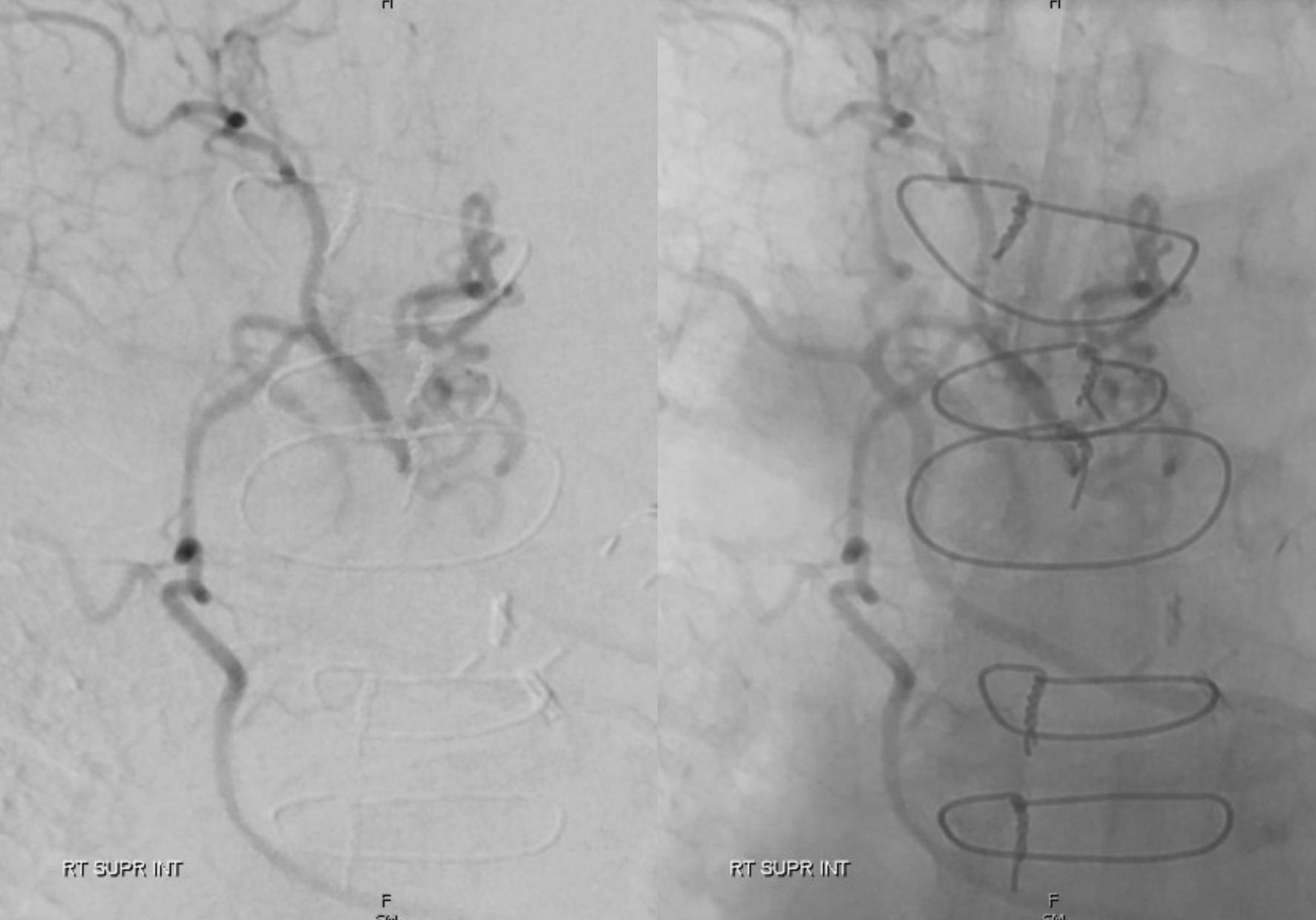
It turned out to be a quite technically difficult angiogram. The fistula was located from the right supreme intercostal artery, using a Sim 1 catheter in this case.
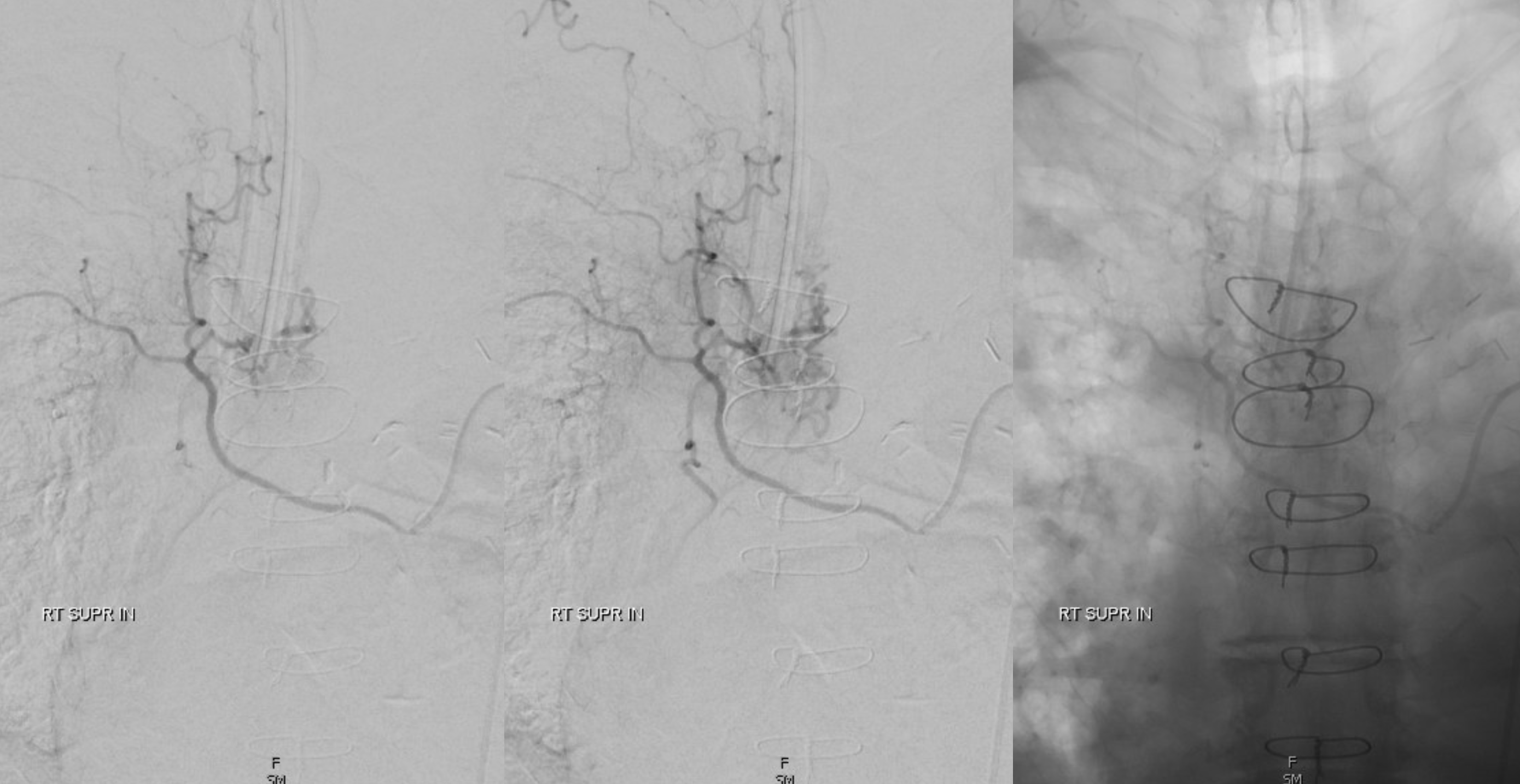
Wide window views
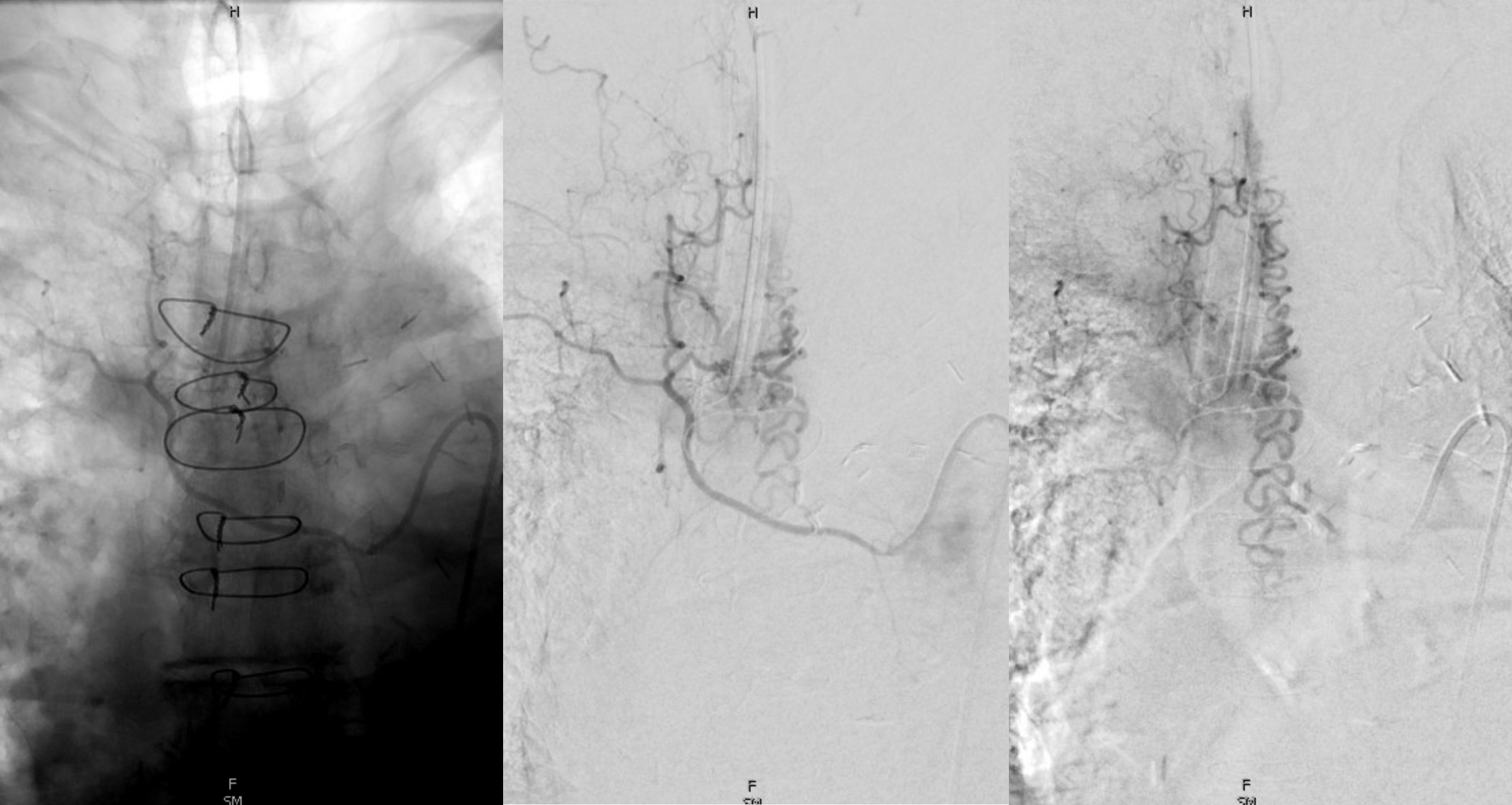
One of our requirements for endovascular treatment is being able to understand not just the fistula, but nearby supply to the spinal cord. Is it near the fistula? Could it be at the same level as the fistula, obscured ty things like ET tube, sternal wires, and suboptimally opacified due to additional fistula demand? You see where this is going. The fact that we do not see spinal arterial supply from nearby levels should give us pause. Magnified views do not seem alarming either.
Cone beam CT / DYNA helps a lot, and is part of our standard evaluation now. We no longer perform endovascular dural fistula treatment without at least 1 DYNA from — from the planned treatment level.
Axial dataset
MIP images of original reconstruction
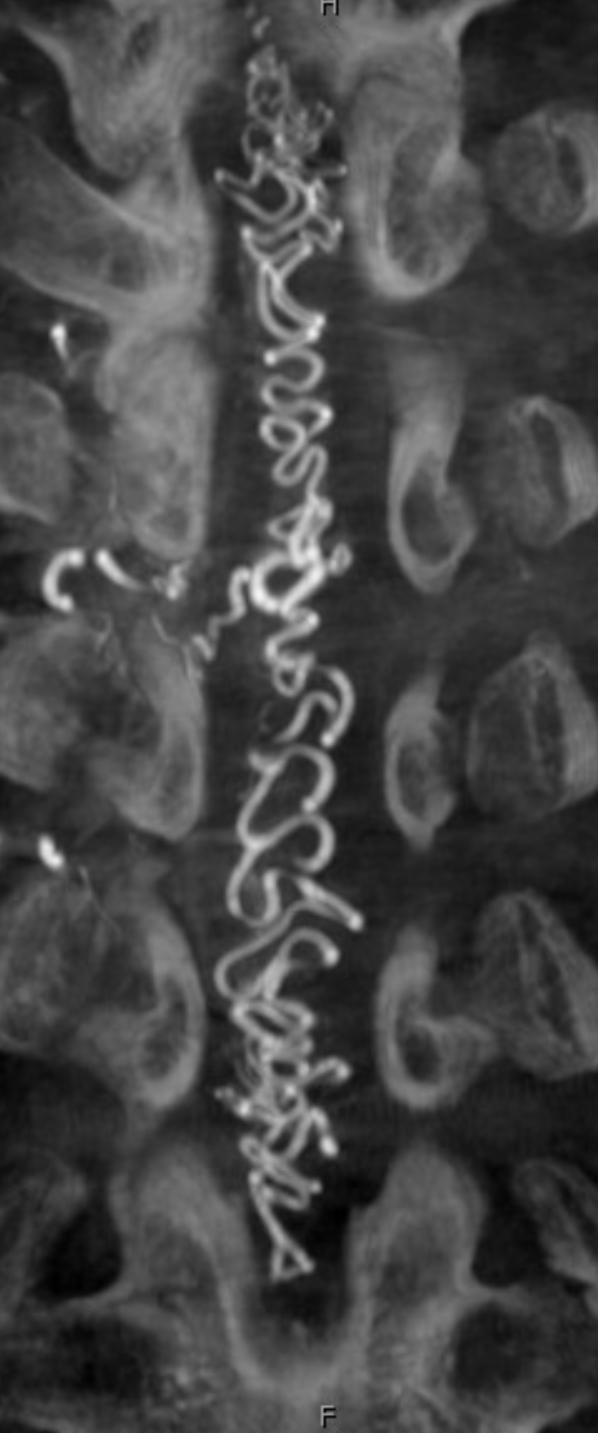
Volume rendered ones. Still nothing….

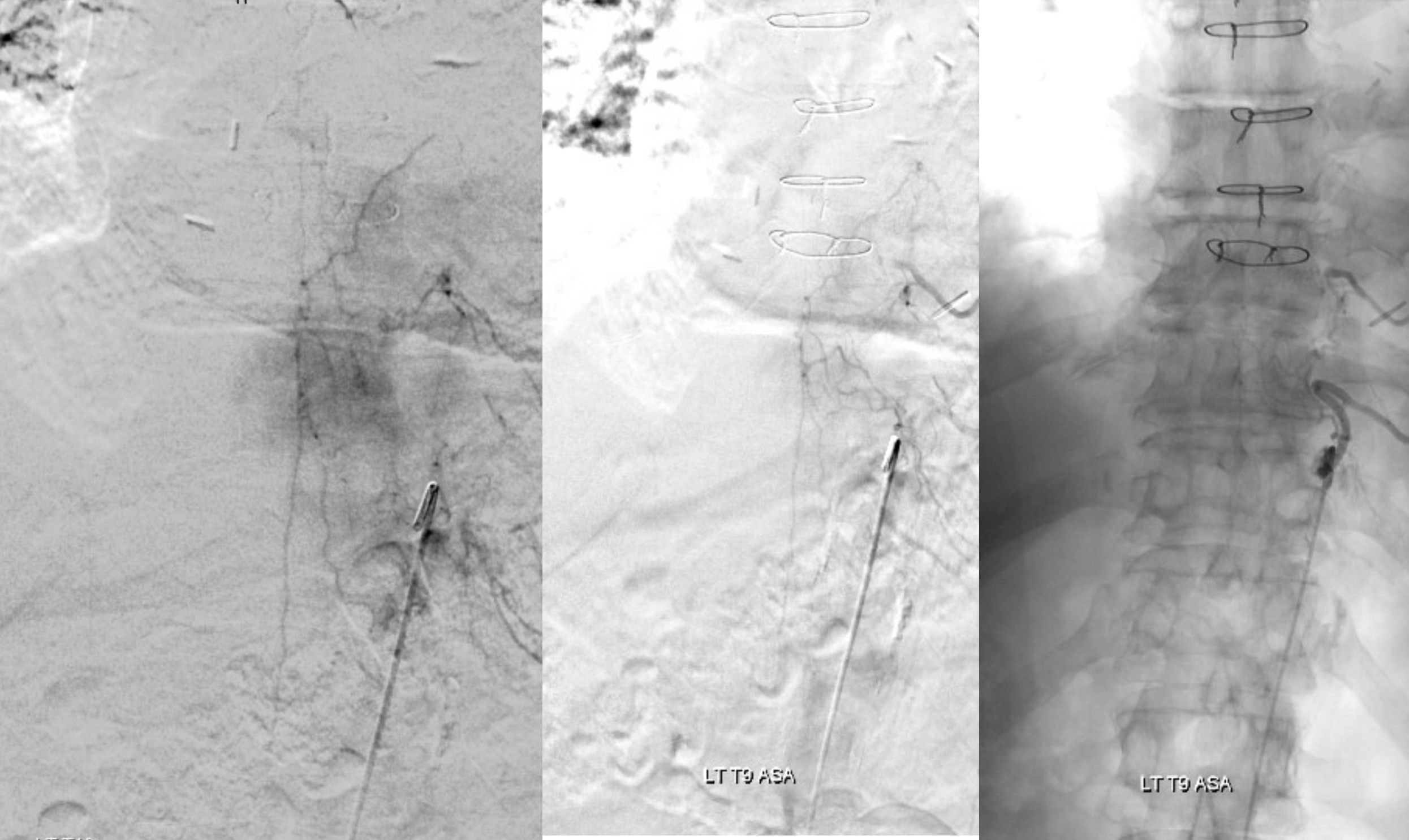
A more dedicated “small volume” high resolution however shows something important (arrows). What is this?
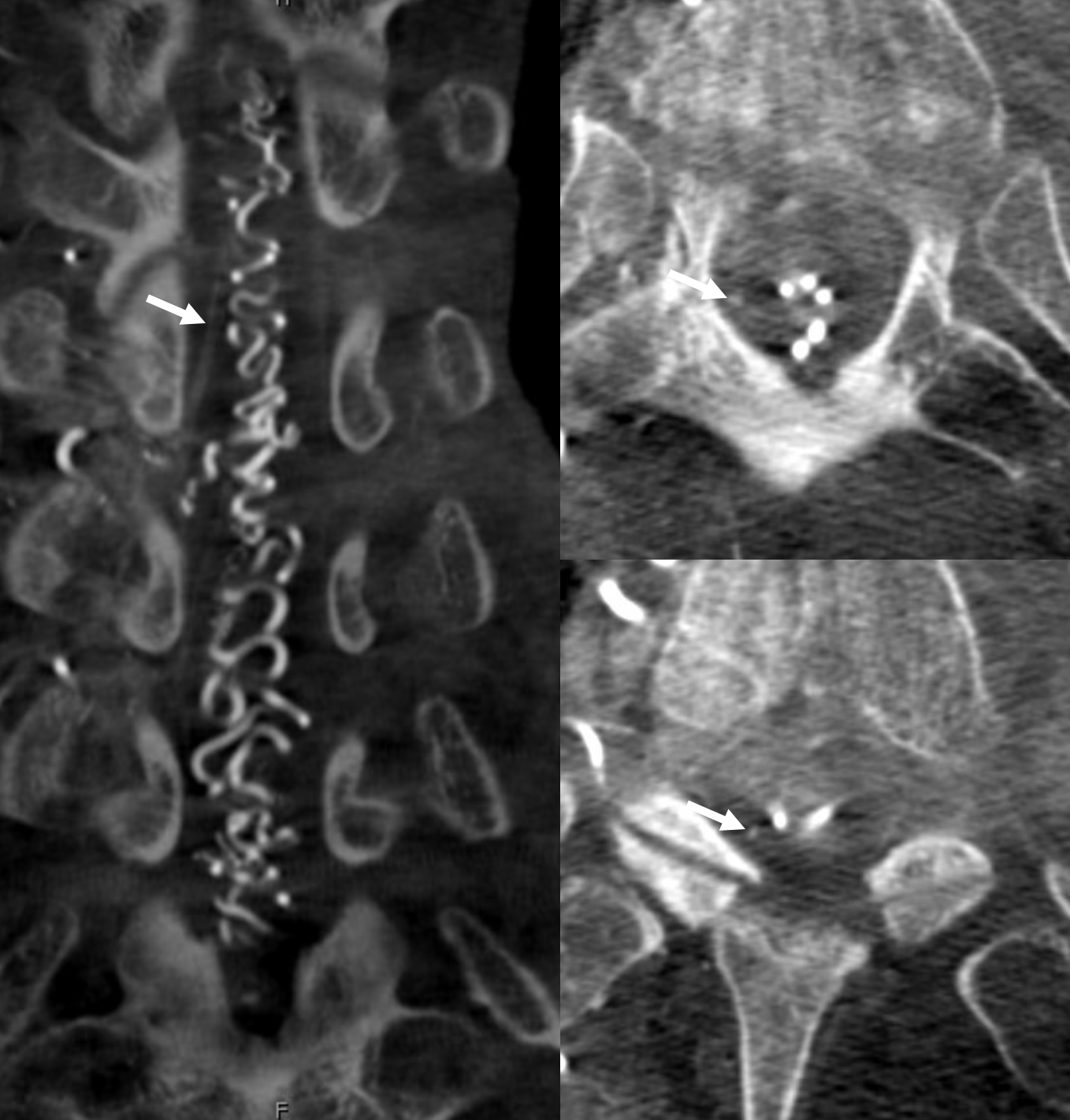
Micro injections — see it now? This is a prominent posterior spinal artery — when spinous processes are centered appropriately, the posterior spinal is lateral to midline. It can be quite prominent occasionally in the upper thoracic area, and indeed have anterior spinal-like significance.
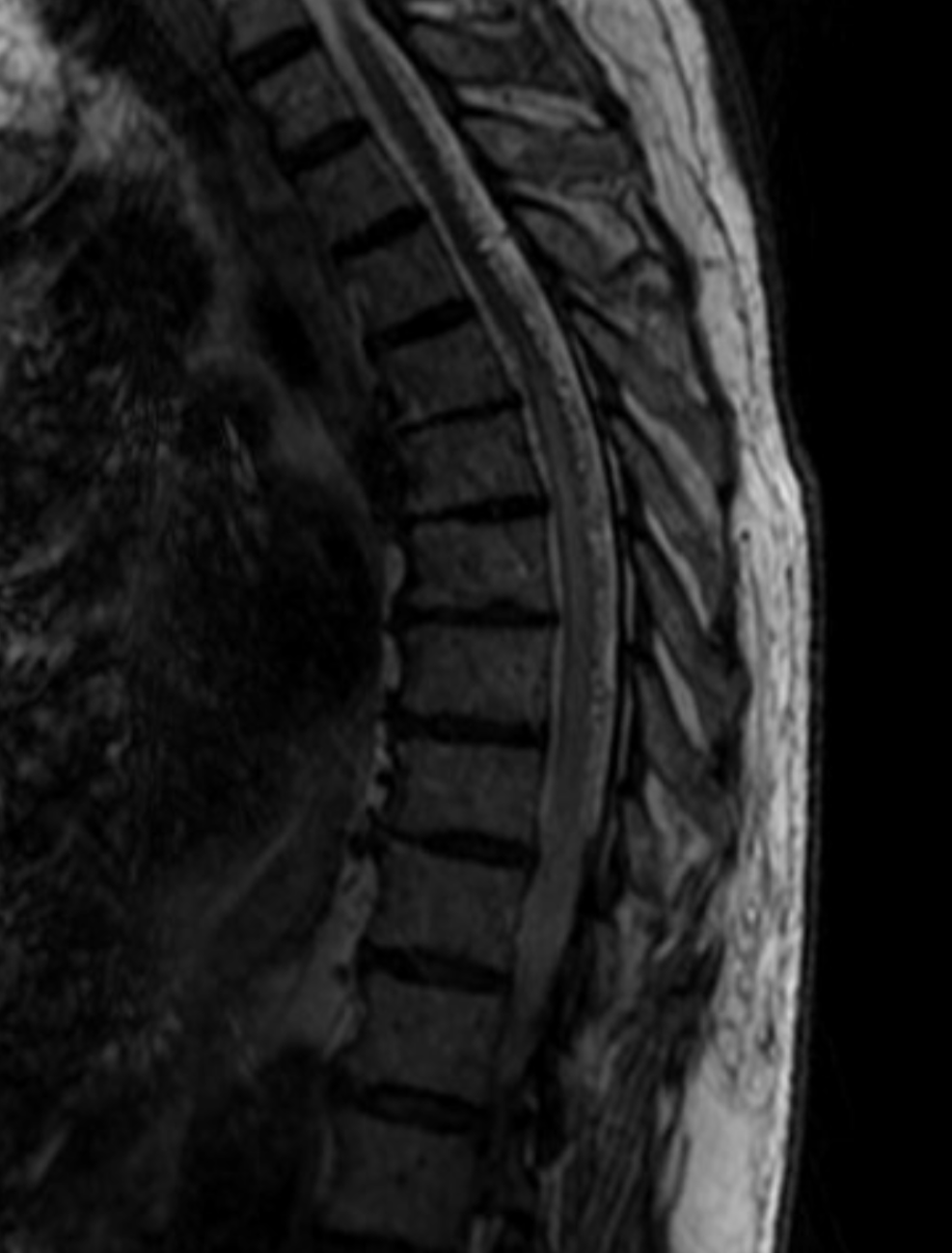
Dedicated micro injection DYNA CT — see location of artery in relation to spinal cord
This is the case for surgery.
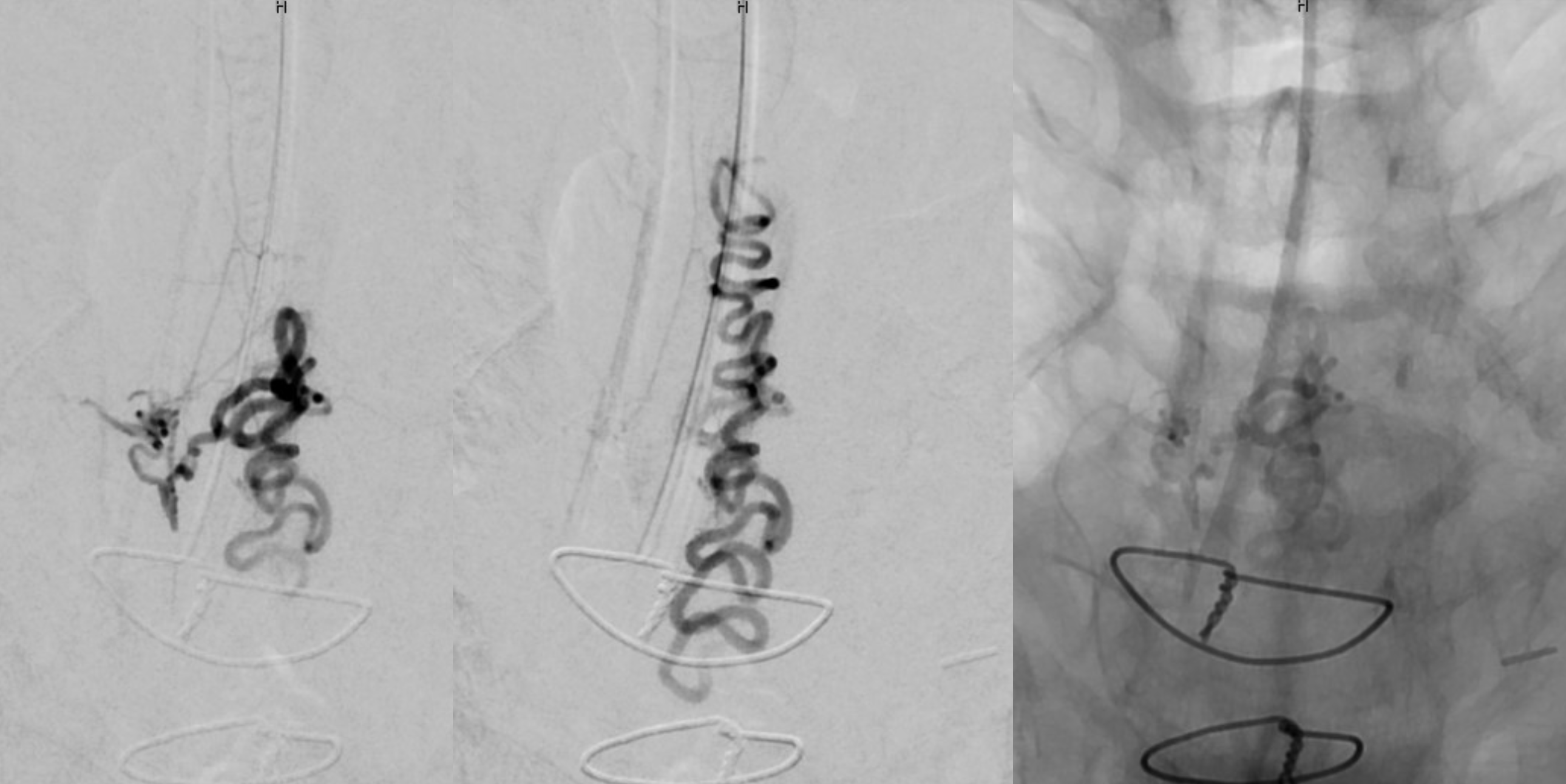
One other thing we do sometimes is intraoperative spinal angio using radial access. Its tricky also, and a recurved catheter such as simmons 1 is good for upper thoracic aorta.

Intraop image with fistula occluded. Resolution is not sufficient to see the posterior spinal artery. Since it was visualized intraoperatively we did do a DYNA. Note coil maker and mirror image appearance in prone position.