
Dealing with a variety of one-offs is an important part of any surgical / endovascular / invasive specialty. This is more about understanding vessels and flow, which can be applied to any situation.
Presentation is with progressive right upper extremity sensorimotor weakness. History of prior significant illnesses requiring central lines, etc. Direct fistulas in this spot you have to think of trauma such as stab wounds, lines, etc.
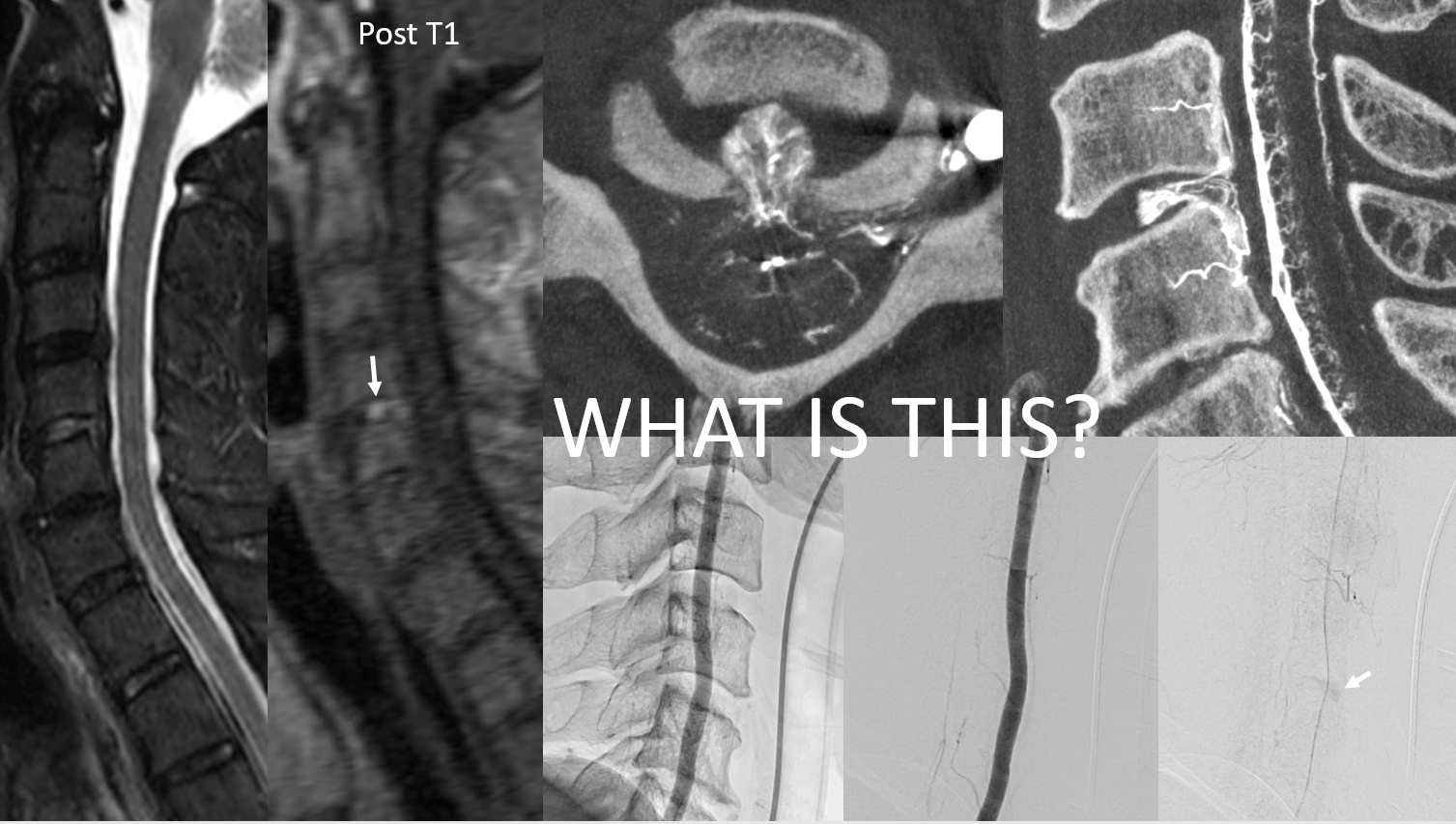
MRI pickup is prominence of epidural (right more than left) and cervical veins.
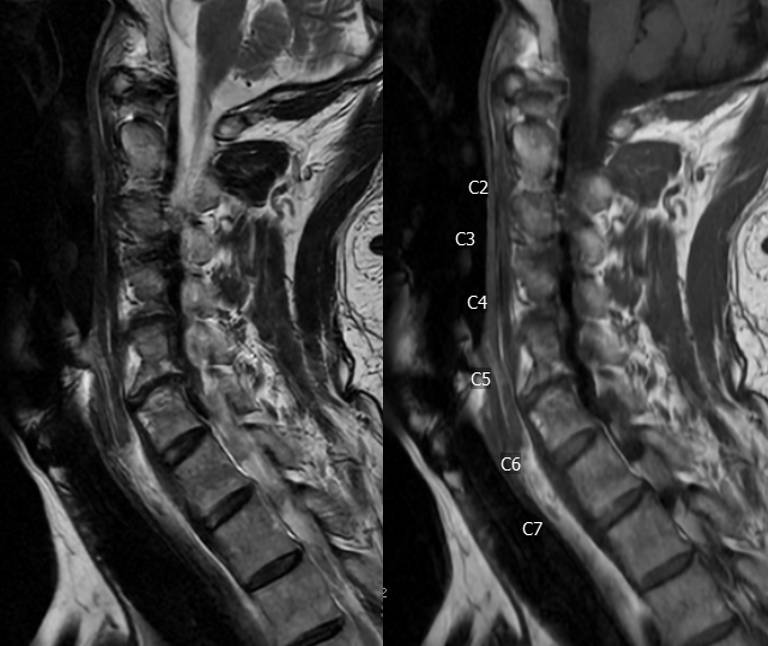

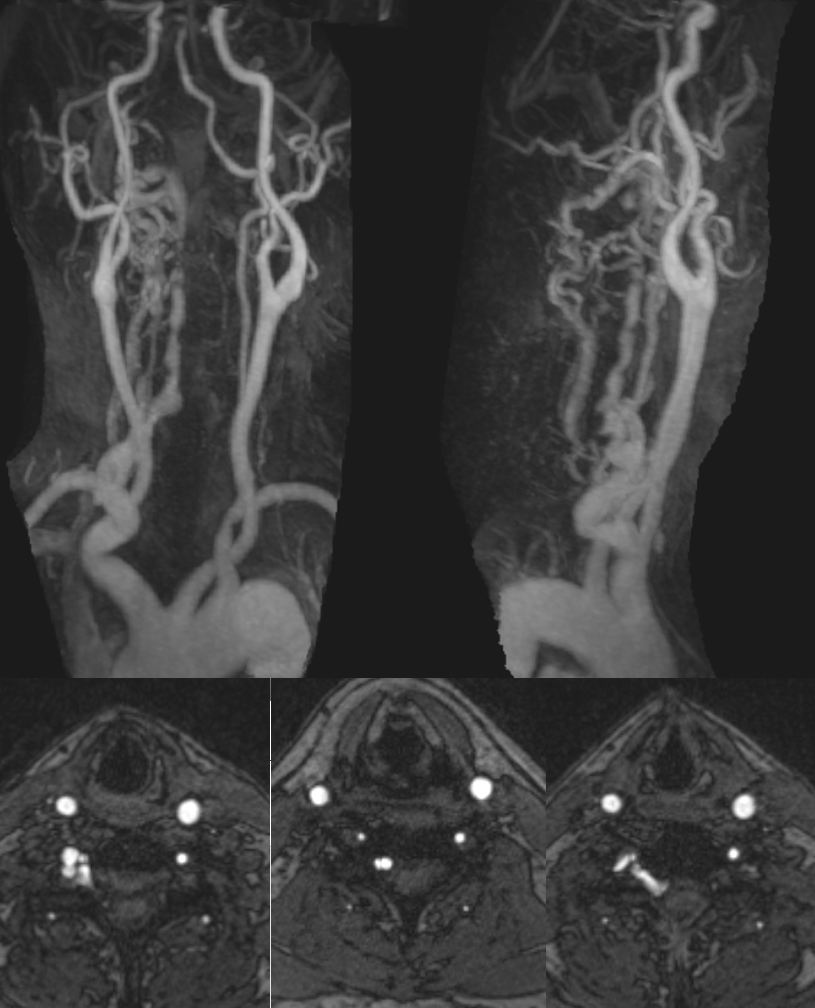
MRA also looks bad
Angio — subclavian injection
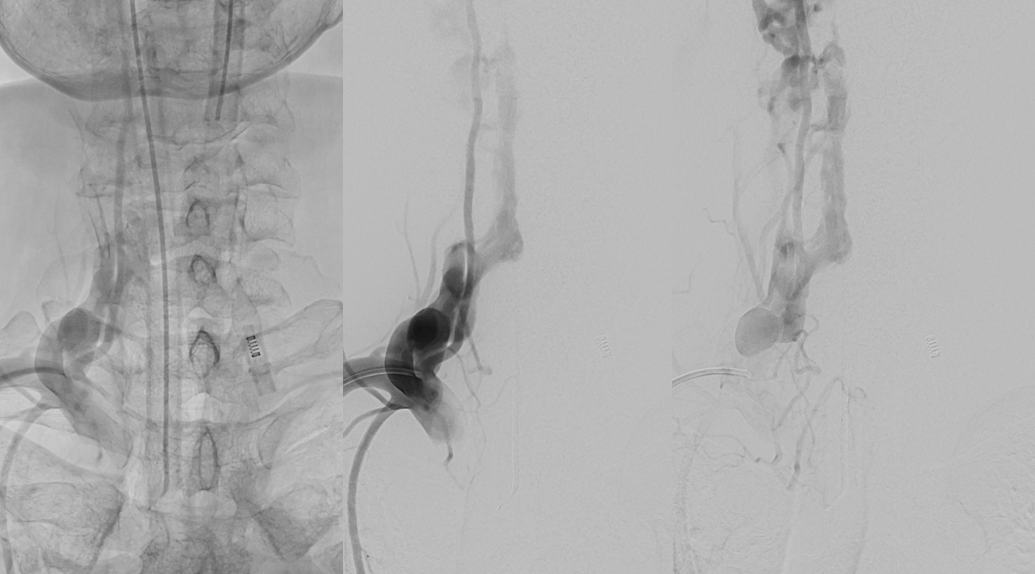
Nothing from the other usual suspects
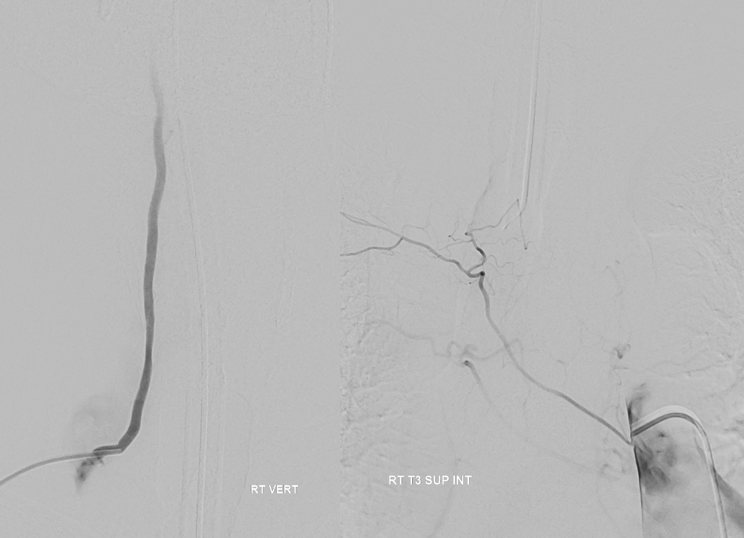
Critical to locate anterior spinal artery supply.
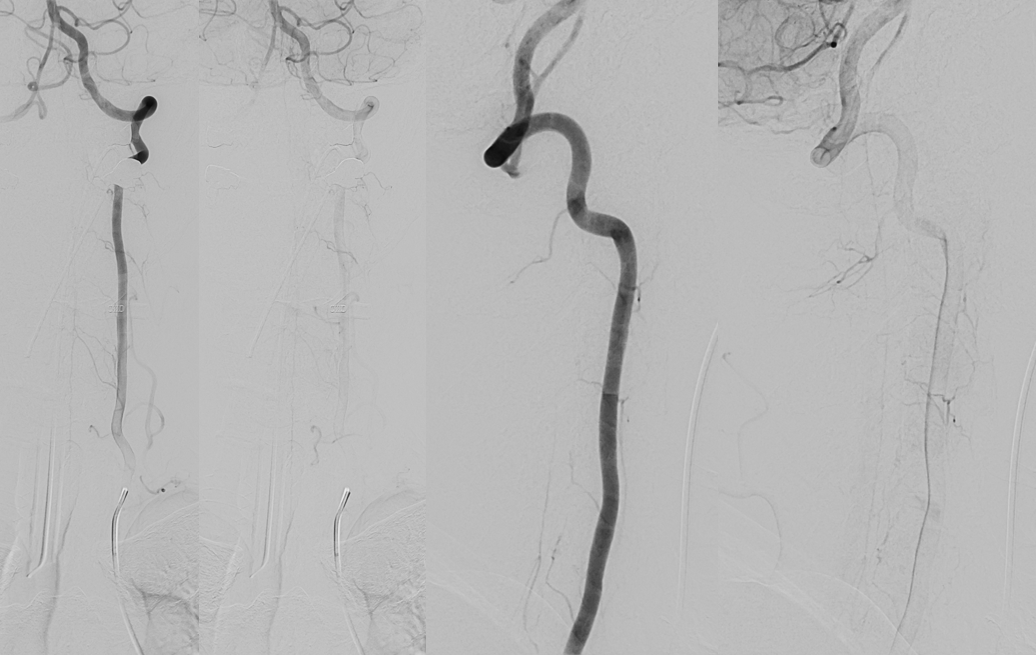
Venous drainage of the cord is only to the left side — right is congested by fistula
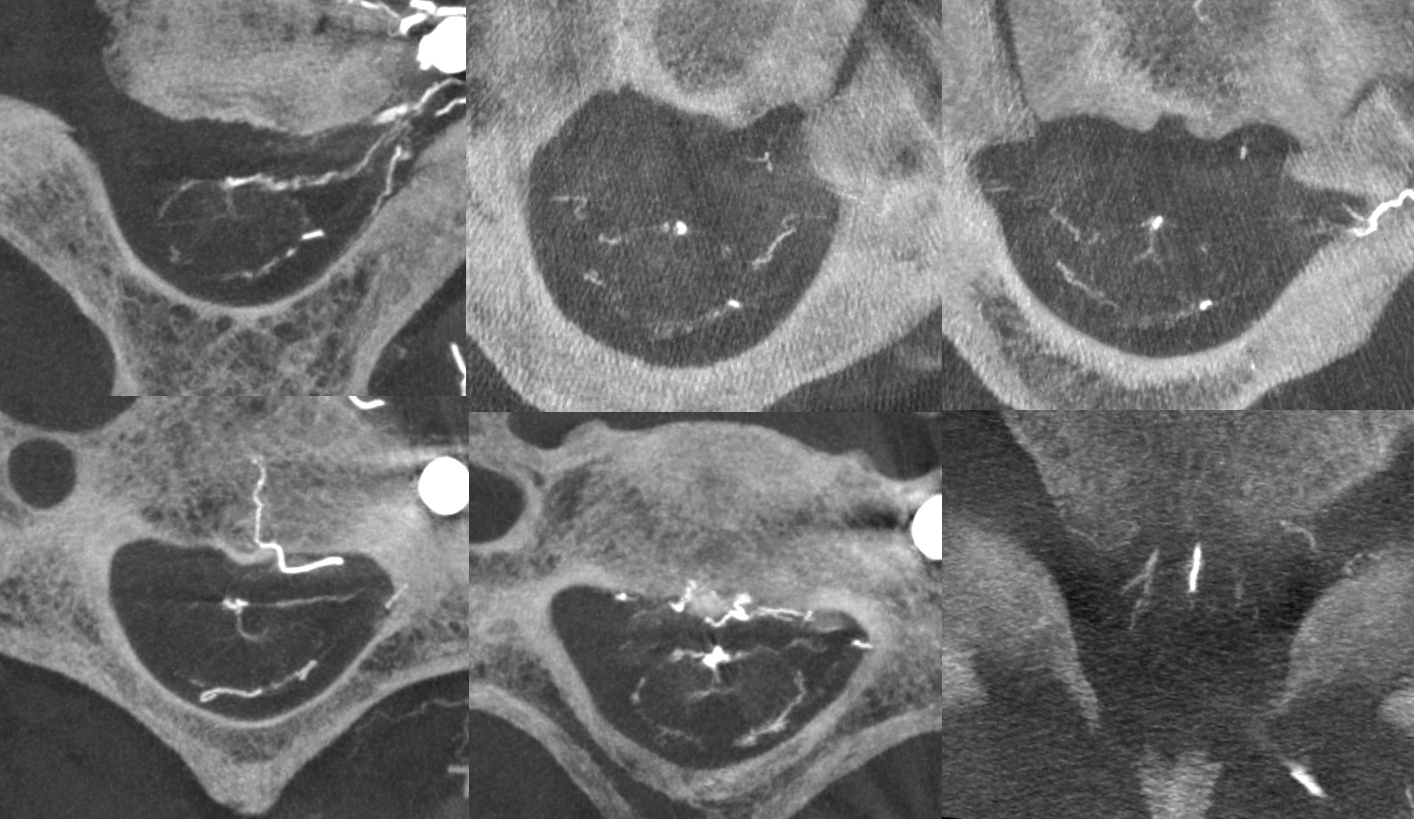
Axials
Interesting disk enhacement seen on both MRI and angio. Anyone know what this is? We do…
Back to our case… Rotational angio/DYNA CT is super helpful. This is an injection of the thyrocervical trunk. There is a direct fistula between the trunk and supraclavicular veins, which primarily drains retrogradely into the epidural plexus. There is no connection with the jugular or subclavian veins (normally there is). Presumably, the patient became symptomatic when this antegrade connection closed, rerouting drainage into the epidural veins.
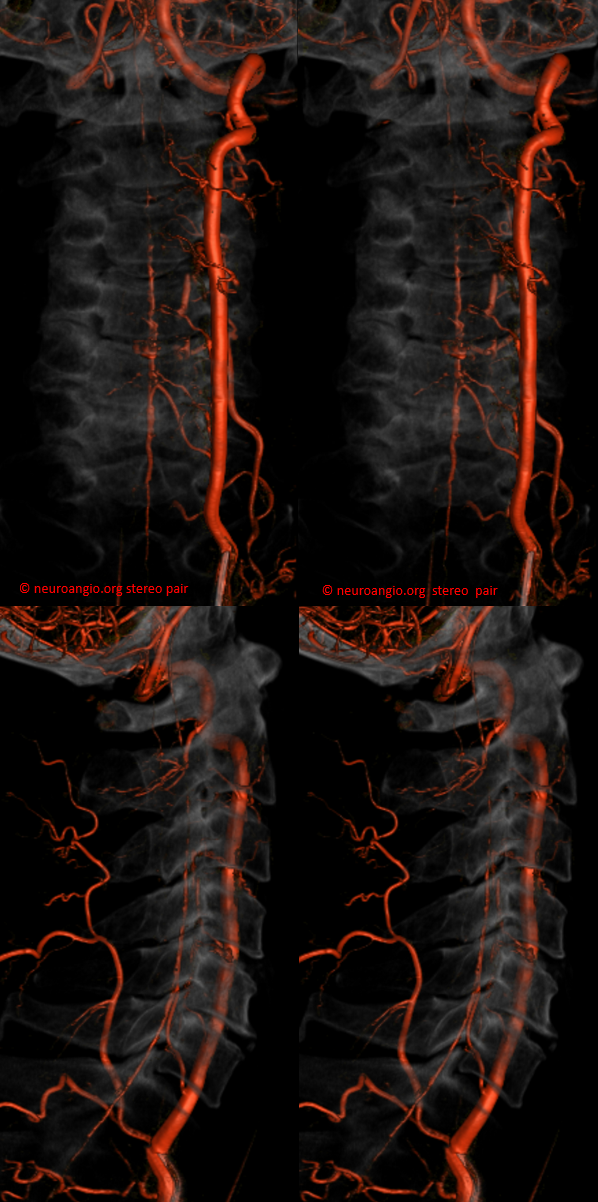
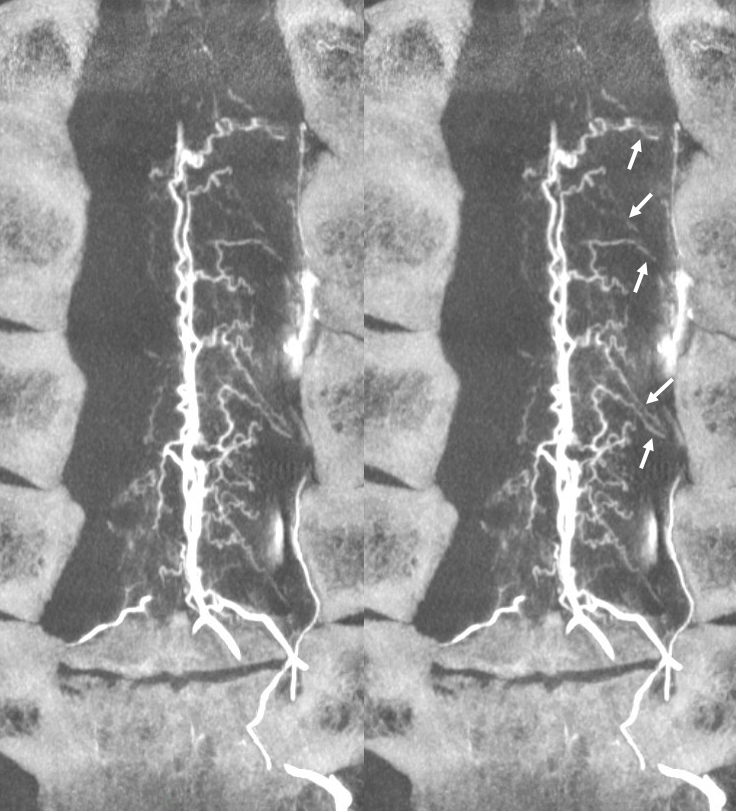
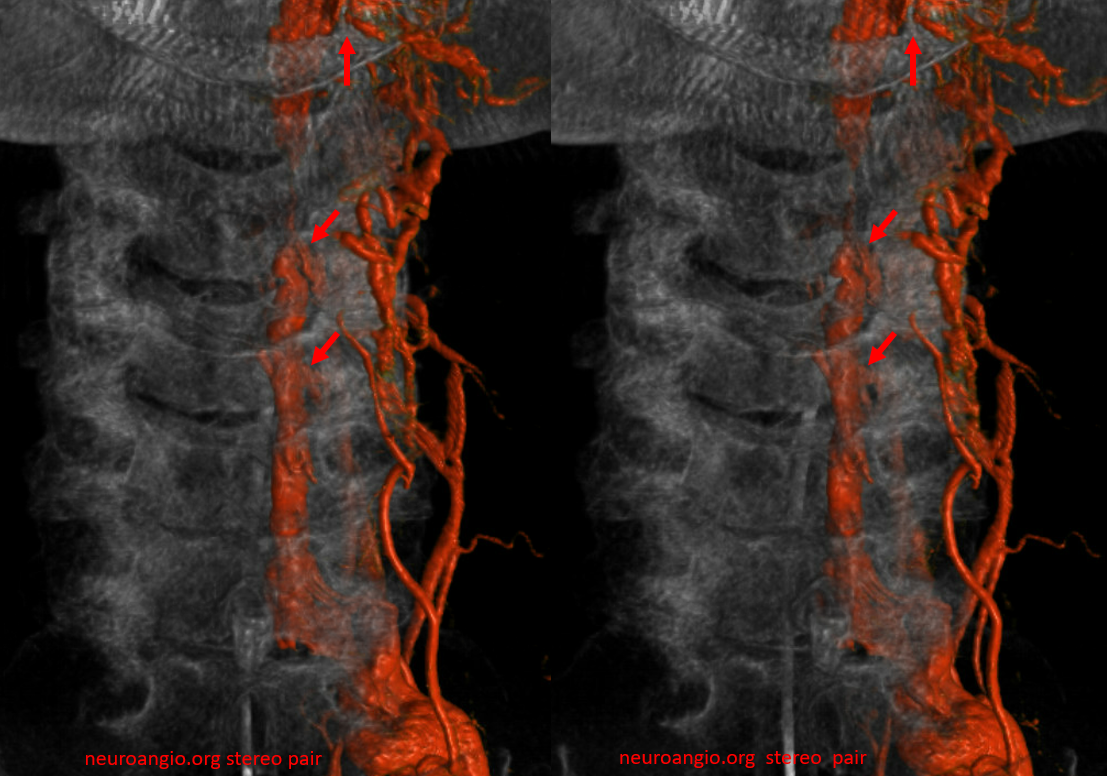
Below is a DYNA CT MIP Set, The reason for presentation (arm weakness/sensory deficit) is because the extraspinal veins for some reason do not drain antegradely into the subclavian or jugular systems. Instead the proximal post-fistulous vein (dashed arrow) drains via the C6 foramen (open arrow) retrogradely into the epidural space. Thanks to multiple patent foraminal venous outflows higher up (arrows), the congested epidural space can decompress into the paravertebral cervical veins, so that symptoms are mostly of nerve root congestion, and not (yet) cord congestion. See details here.

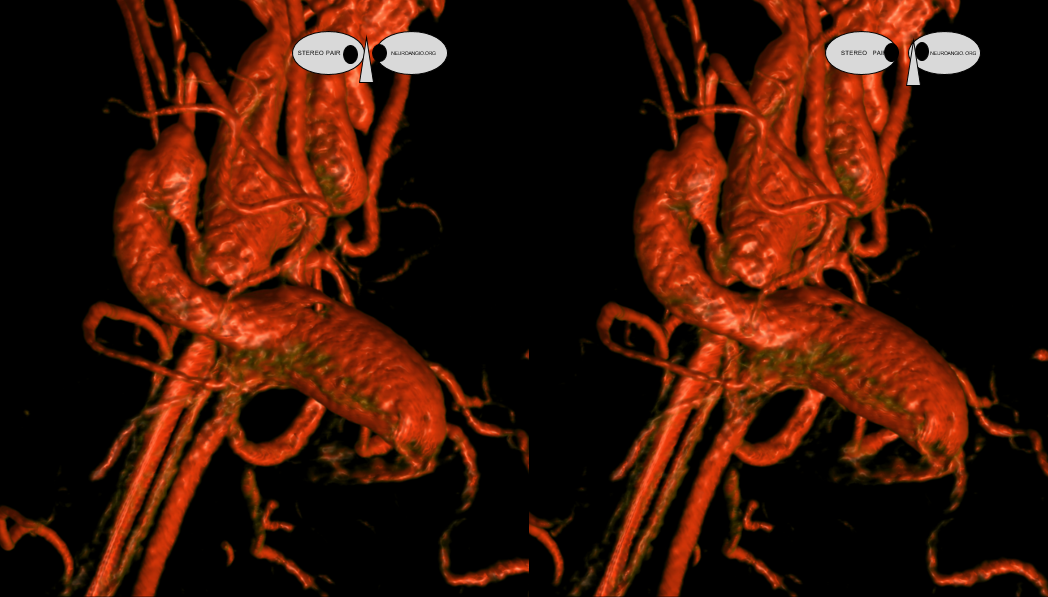
Stereo VR set. Foraminal veins marked by arrows
The strategy is to close the arterioenous connection. It is easier said than done.
Trying to close the connection selectively with small coil or two was not feasible due to high low. Scepter C did not help. A second balloon in the thyrocervical trunk (not shown) did not help either. So we ended up putting some coils into the proximal venous pouch to allow for subsequent coiling of the fistula region (middle and lower images)

Post
