Another frontier for Cone Beam applications. Gamma Knife Radiosurgery for AVMs. Targeting is usually done with MRI or MRI plus conventional angiography — acquired and co-registered in a stereotactic headframe. This is usually fine for big lesions. For small ones, things get tricky.
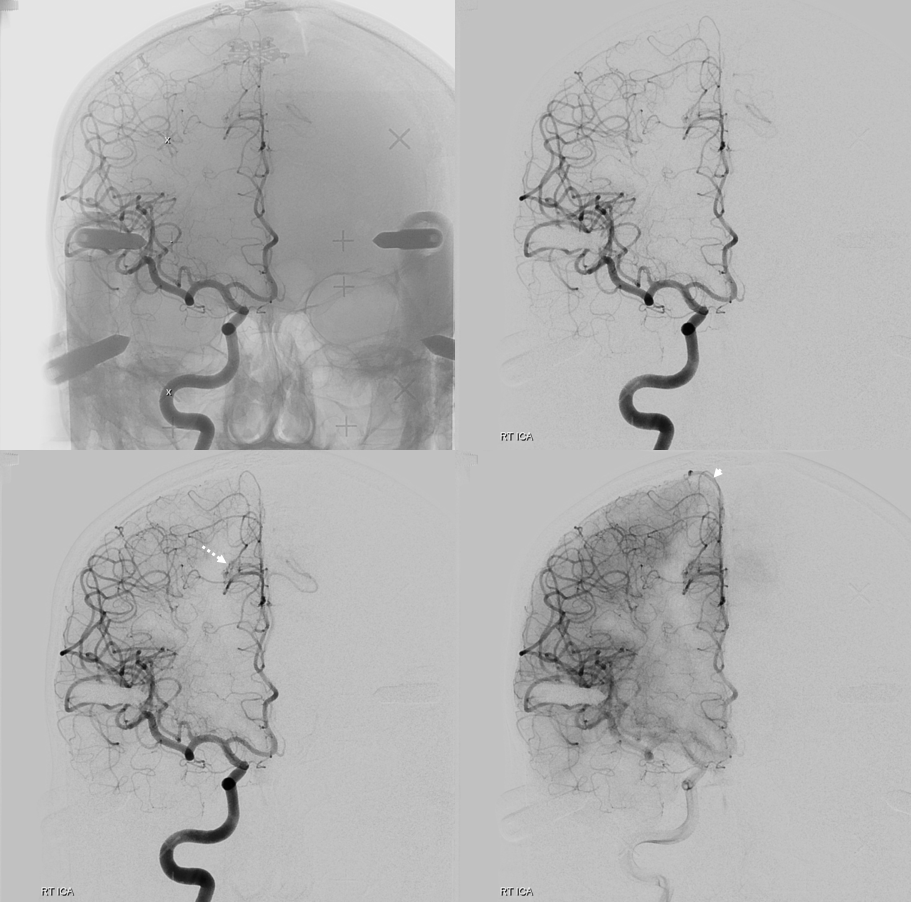
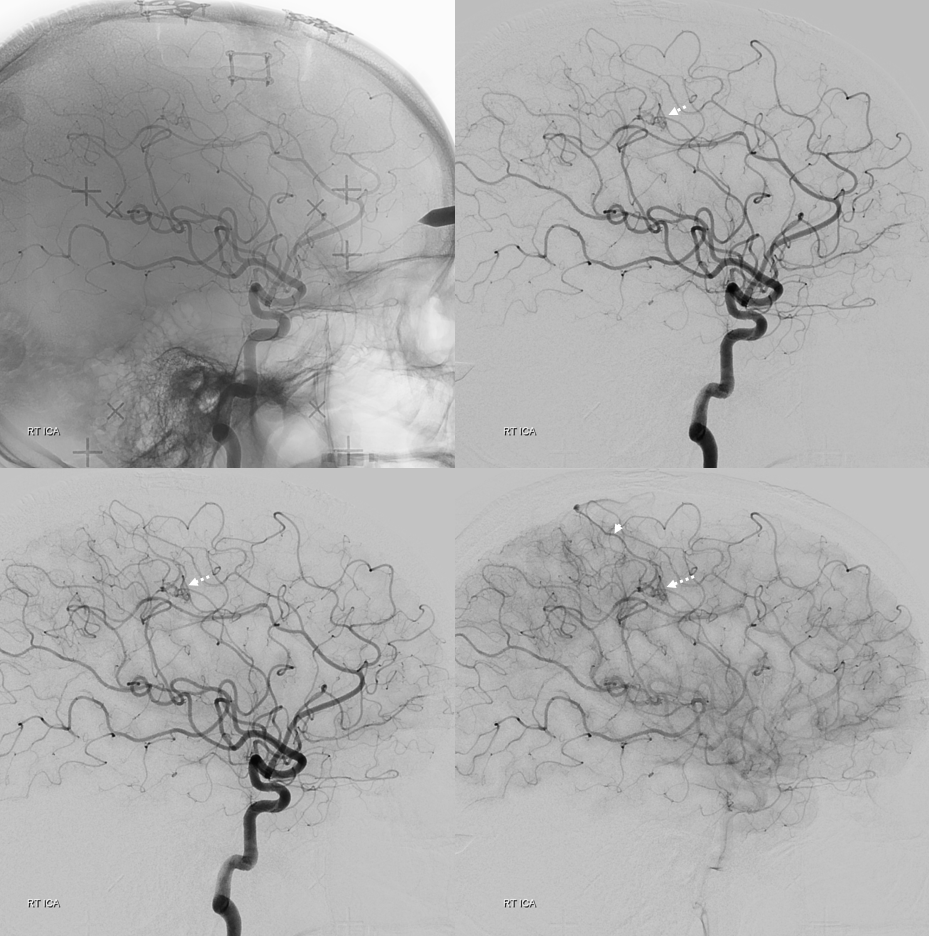
This patient’s AVM ruptured, followed by resection. Presentation is a small residual/recurrent AVM. Angiogram shows small right posterior frontal periventricular nidus (dashed arrows), draining via mesial frontal vein (arrowheads) into the SSS
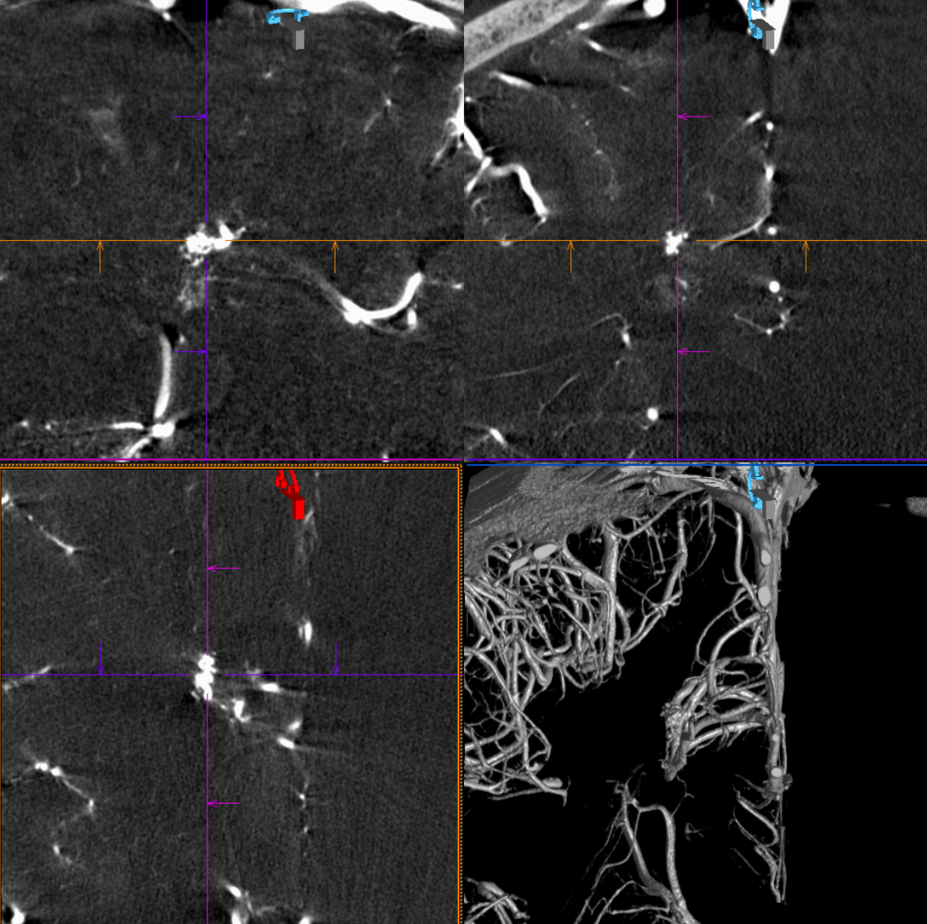
DYNA CT reconstructions show the nidus superbly well
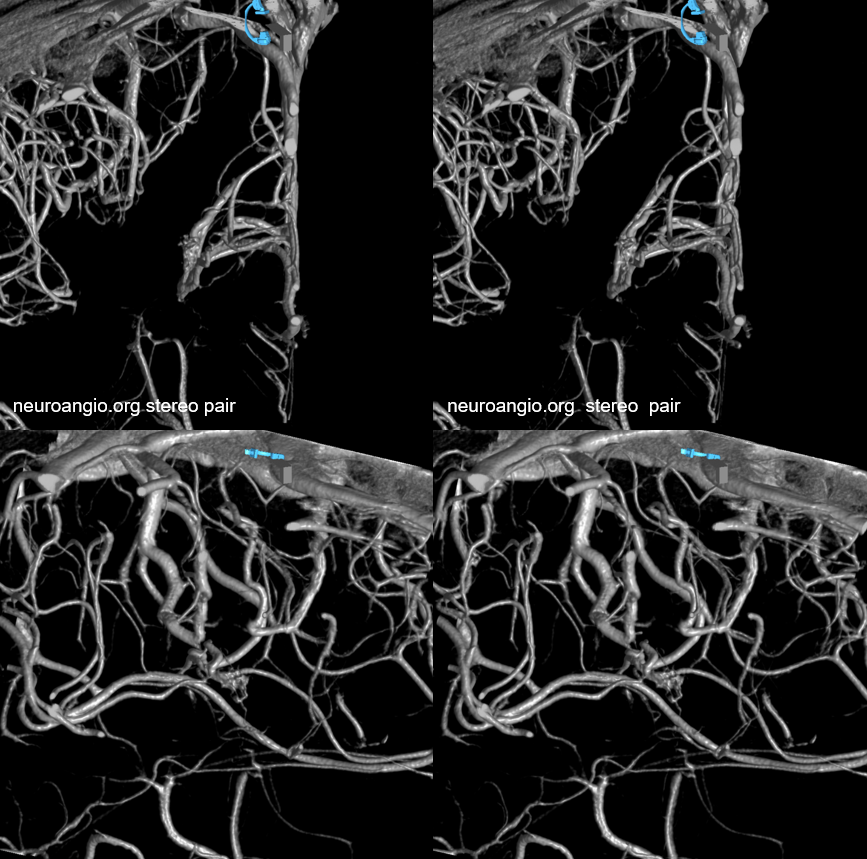
Cross-sectional imaging and VRs
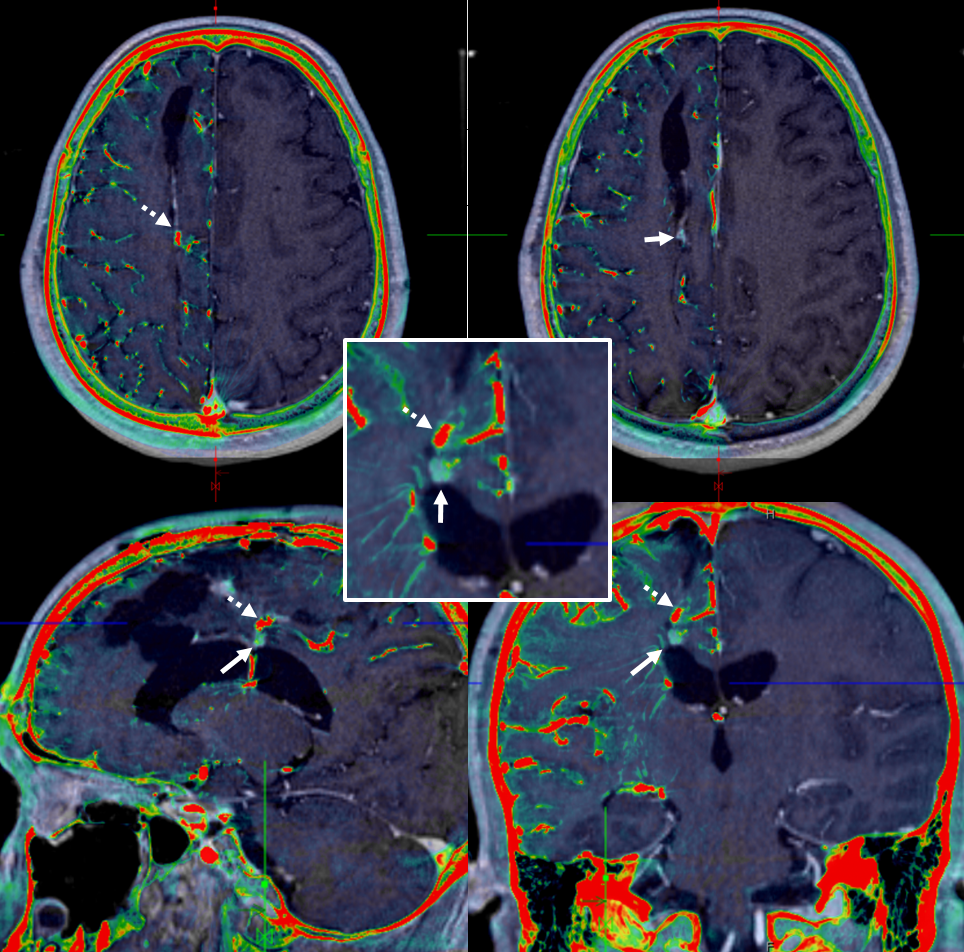
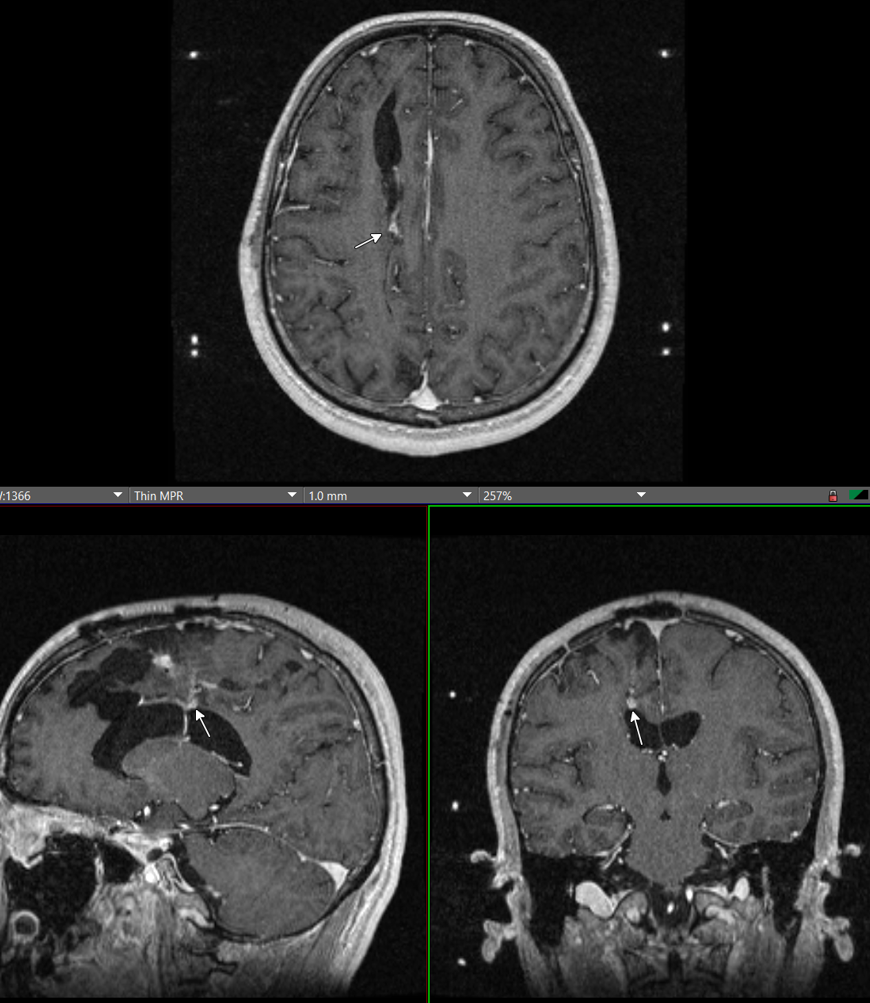
MRI — cavity and nodule of enhancement (arrows) — looks to be the same location as angiographic nidus
So, what’s the catch? Co-registration of DYNA cross-sectional and MRI imaging below. As it happens, the MRI nodule and angiographic / DYNA nidus are in different locations — close but definitely not the same. The co-registration is perfect. So, using MRI alone would have resulted in mistargeting. And, without DYNA, 2-D angiographic co-registration may be questioned also. With the DYNA, its extremely clear what the target should be.