
NEW! Click here for narrated version of this page on our youtube channel — www.youtube.com/neuroangio
Rare nice case — presentation is dizziness, followed by progressive obtundation and loss of consciousness. Intubate in ED. All toxicology negative. Extubated next day. Exam shows mild LUE weakness only.
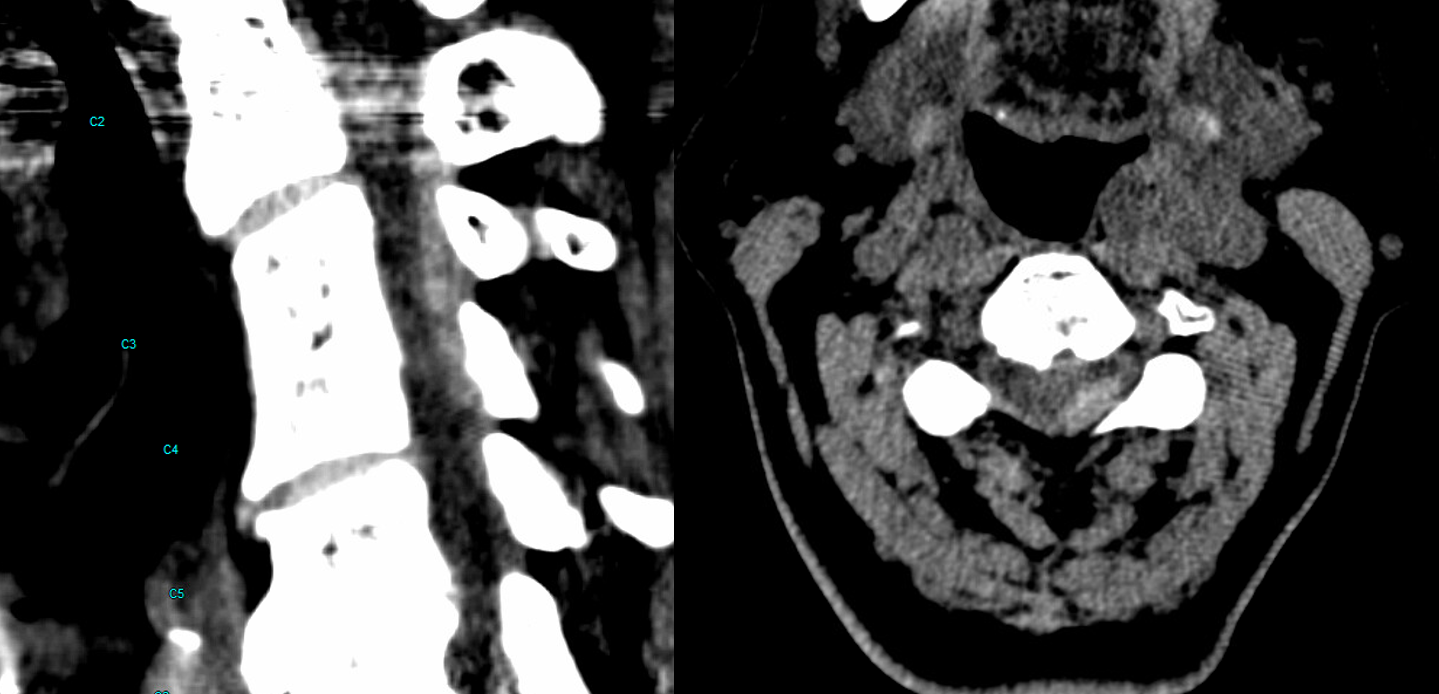
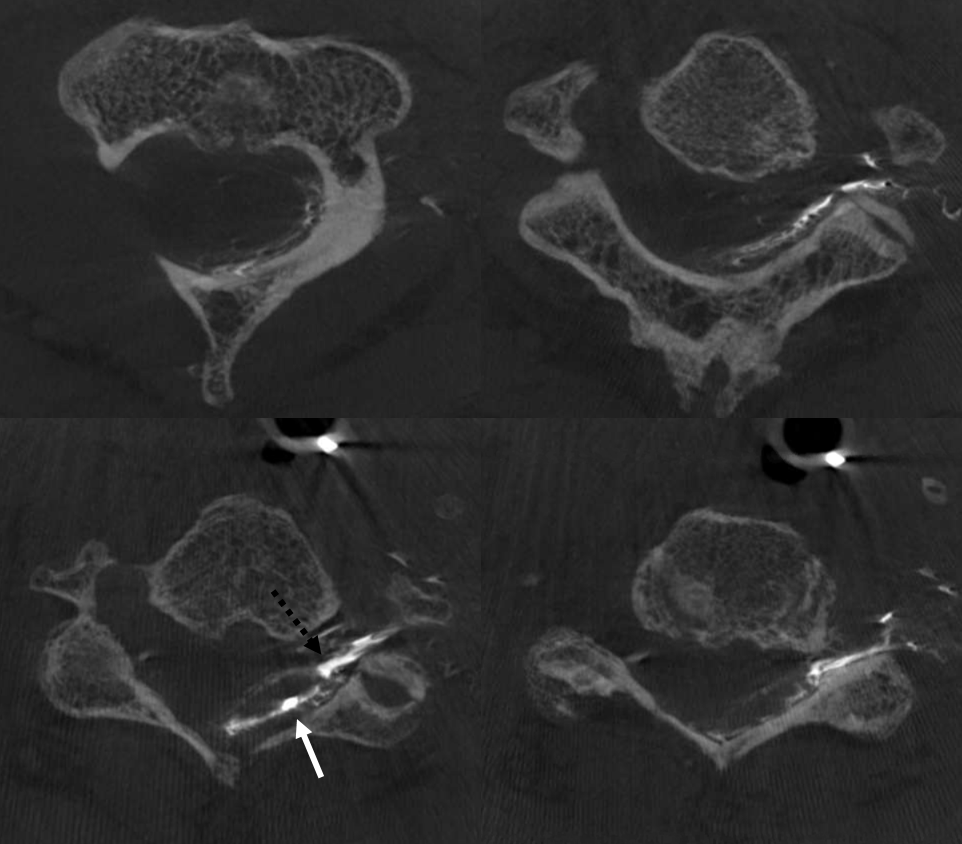
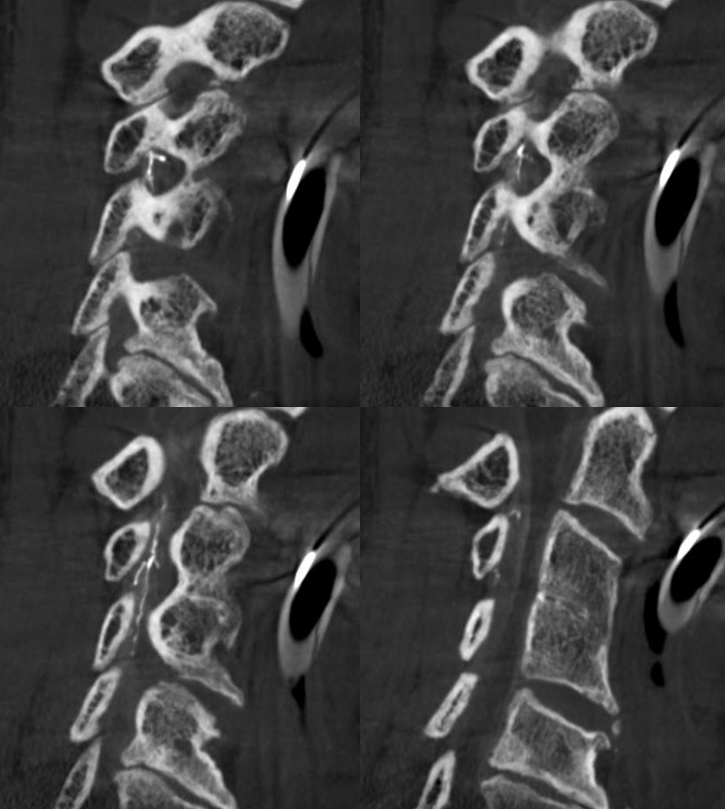
CT — looks like acute left epidural hematoma
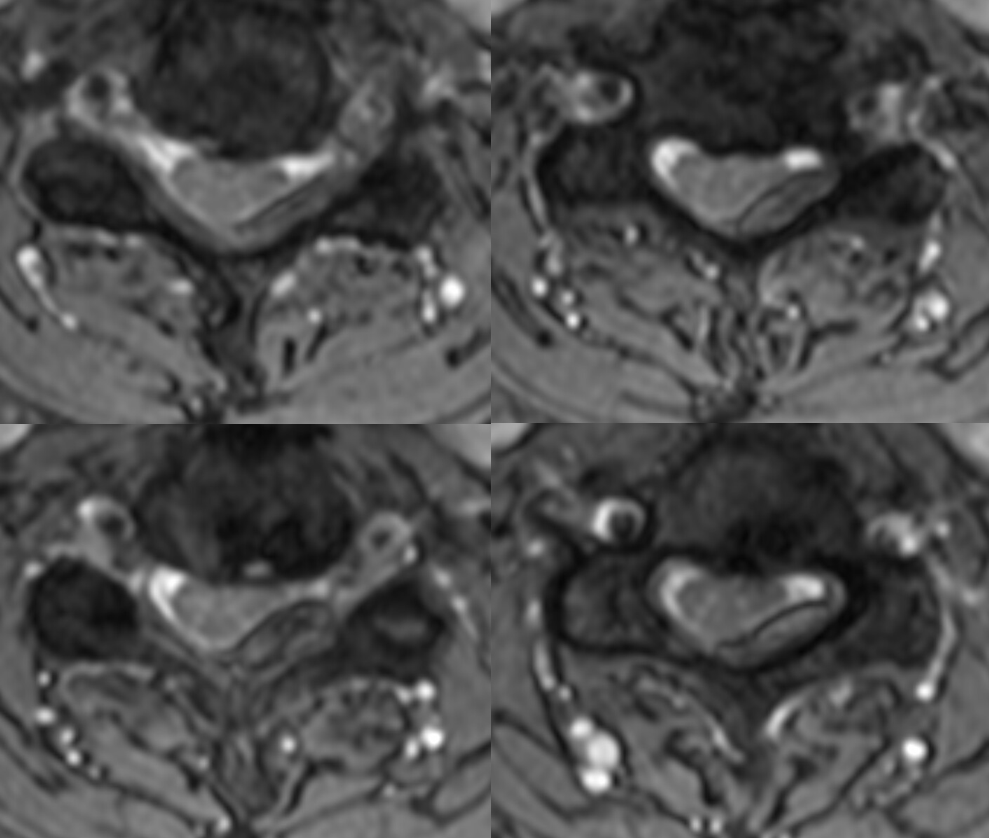
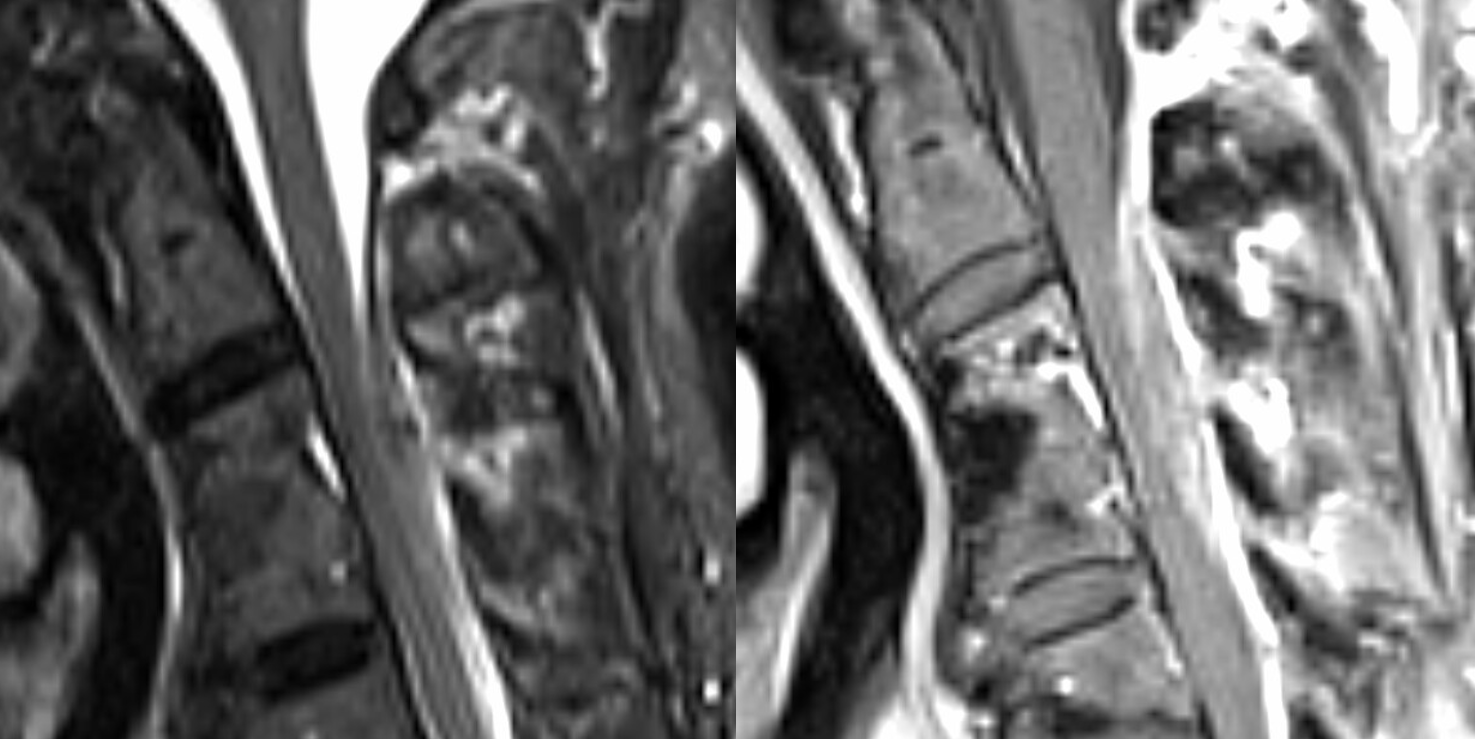
MRIs
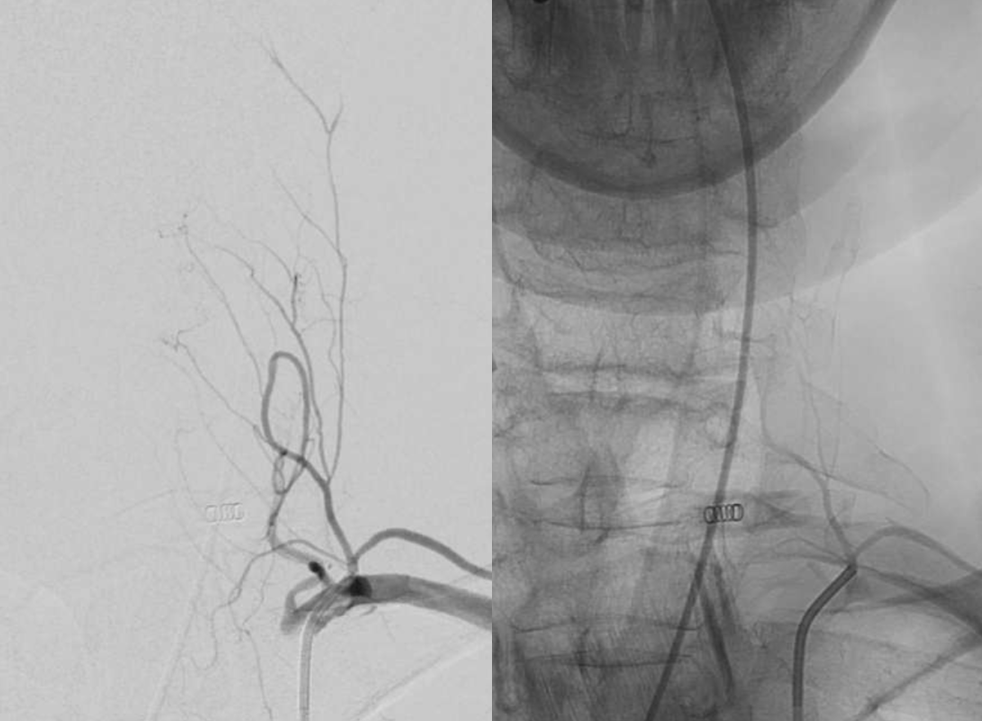
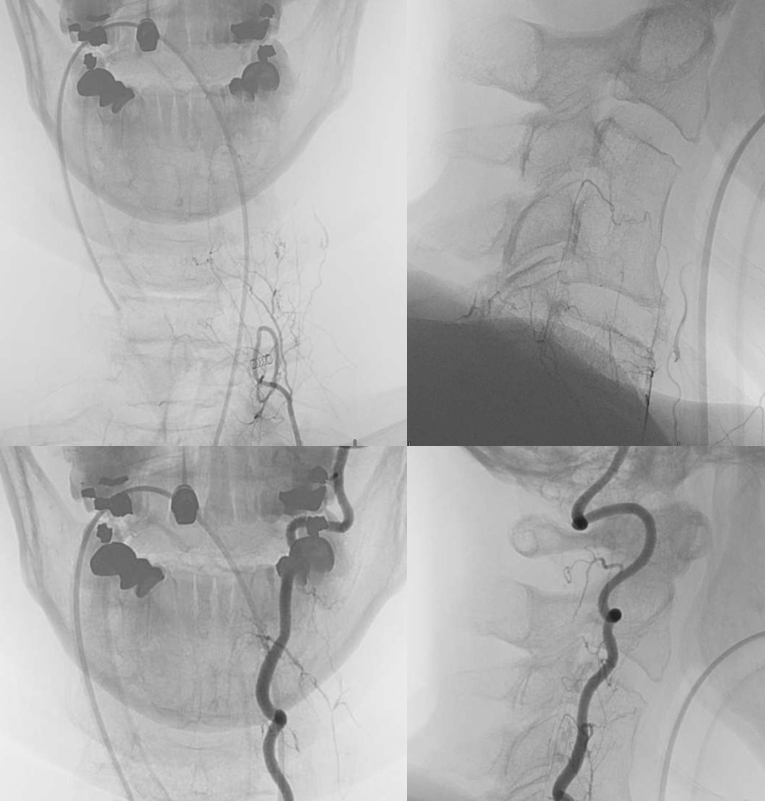
Angio — good technique is key to spine. Patient under GA. Pharmacologic paralysis and apnea. There is a suggestion of what looks like a pseudoaneurysm (white arrow) Vertebral injection

Ascending cervical (variant) injection — nothing to see?
A better injection — technique again. See now? Pseudoaneurysm (white arrow), supplied by distal pedicle (dashed white arrow). Note the frequently seen connection to the vert (black arrows)
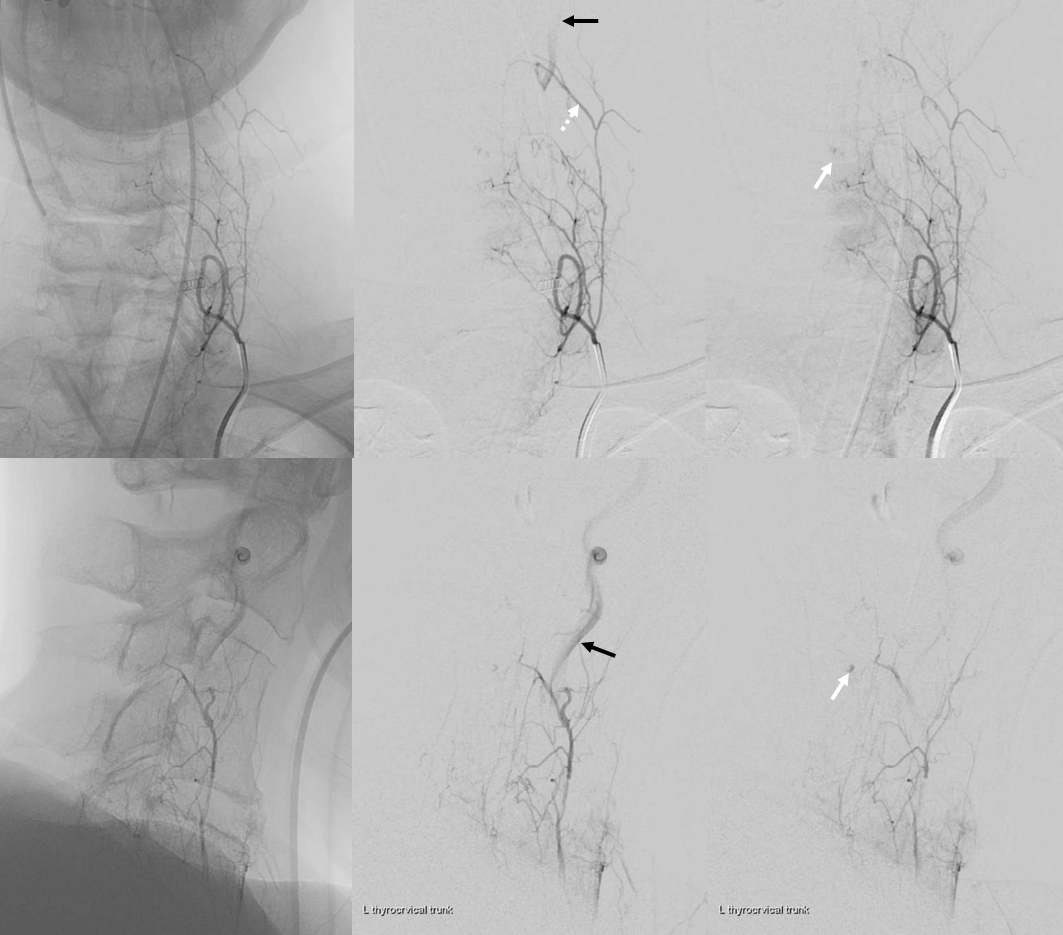
Coned down vert injection — target musculospinal branch origin is dashed arrow. Note retrograde visualization (reflux) into same ascending cervical branch we see above (dashed white arrows)

Single tip (dashed black arrows) headway duo in the musculospinal branch. There is no direct connection to the target — the pseudoaneurysm is seen via reflux into the ascending cervical branch (dashed white arrow)
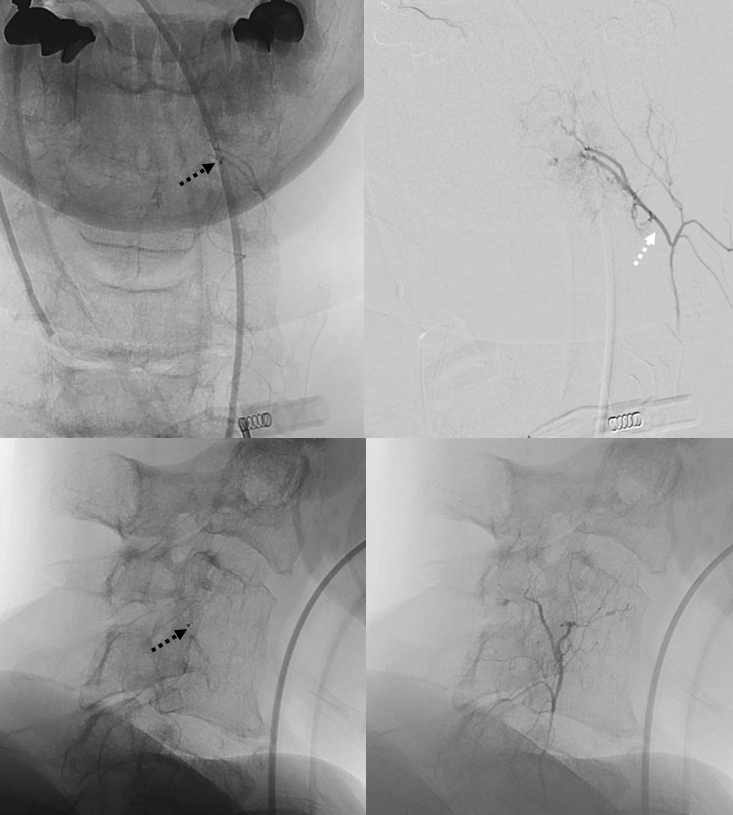
Headway duo moved to distal ascending cervical tributary to the pseudoaneurysm. Tip is marked with dashed black arrows. Lets give this “tributary” a better name — the C4 radicular branch. Why — because it supplies the dura via the C4 foramen.
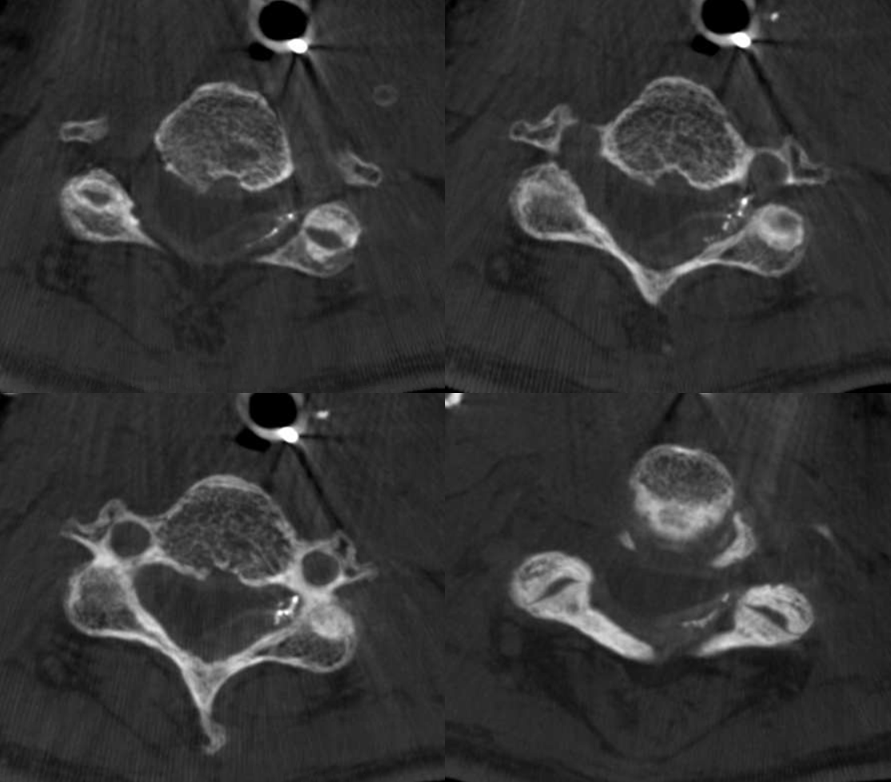
Micro injection. Note microcatheter tip location in the foramen area (unsubtracted images) and connection with the vert (black arrows). There do not seem to be obvious cord vessels present
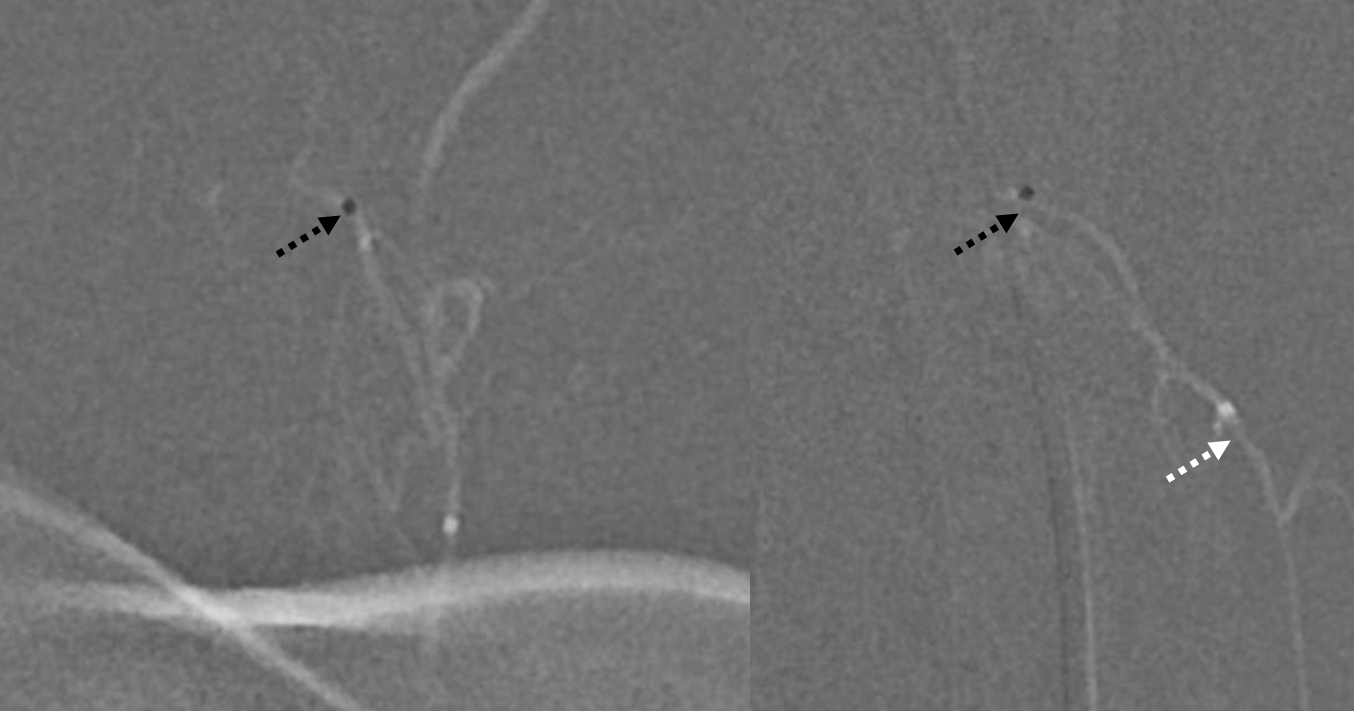
DYNA CT (20 second injection duration). Of course — how could we not do a DYNA? Also important to verify there is no connection to cord — at least not one we can see. If there is, embolization would probably be a silly undertaking given that surgical cord morbidity would be minimal.
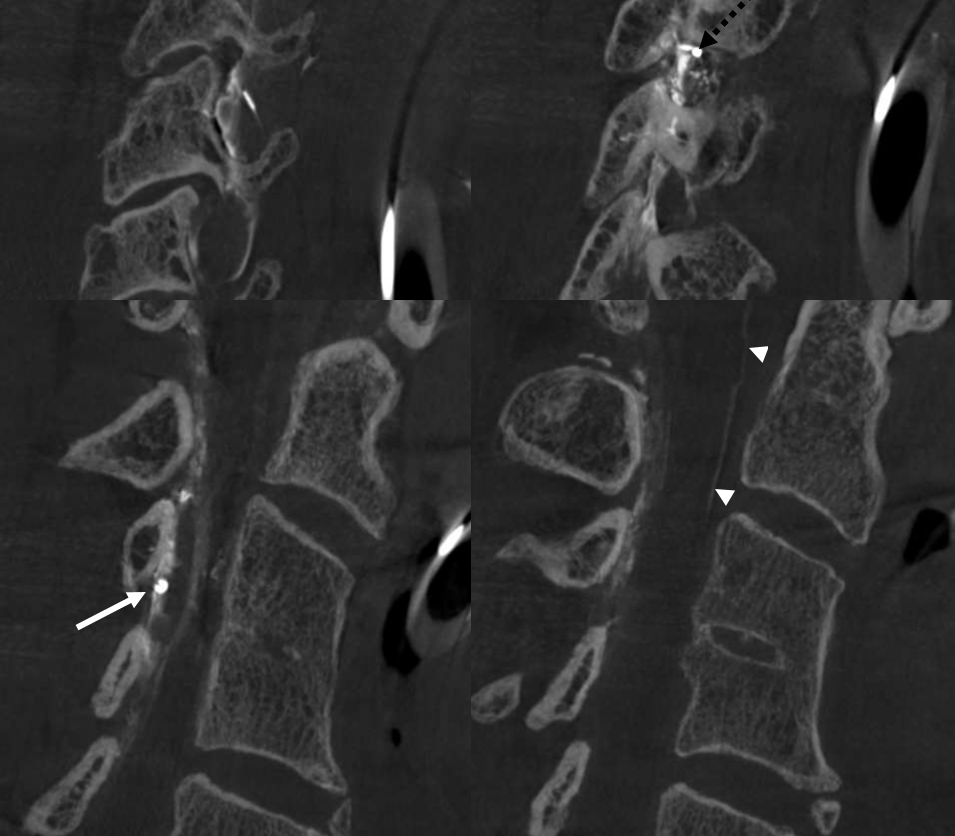
Catheter tip — dashed black arrow. Pseudoaneurysm — white arrow. Nice images huh? Look at that lens-shaped outline in lower left.
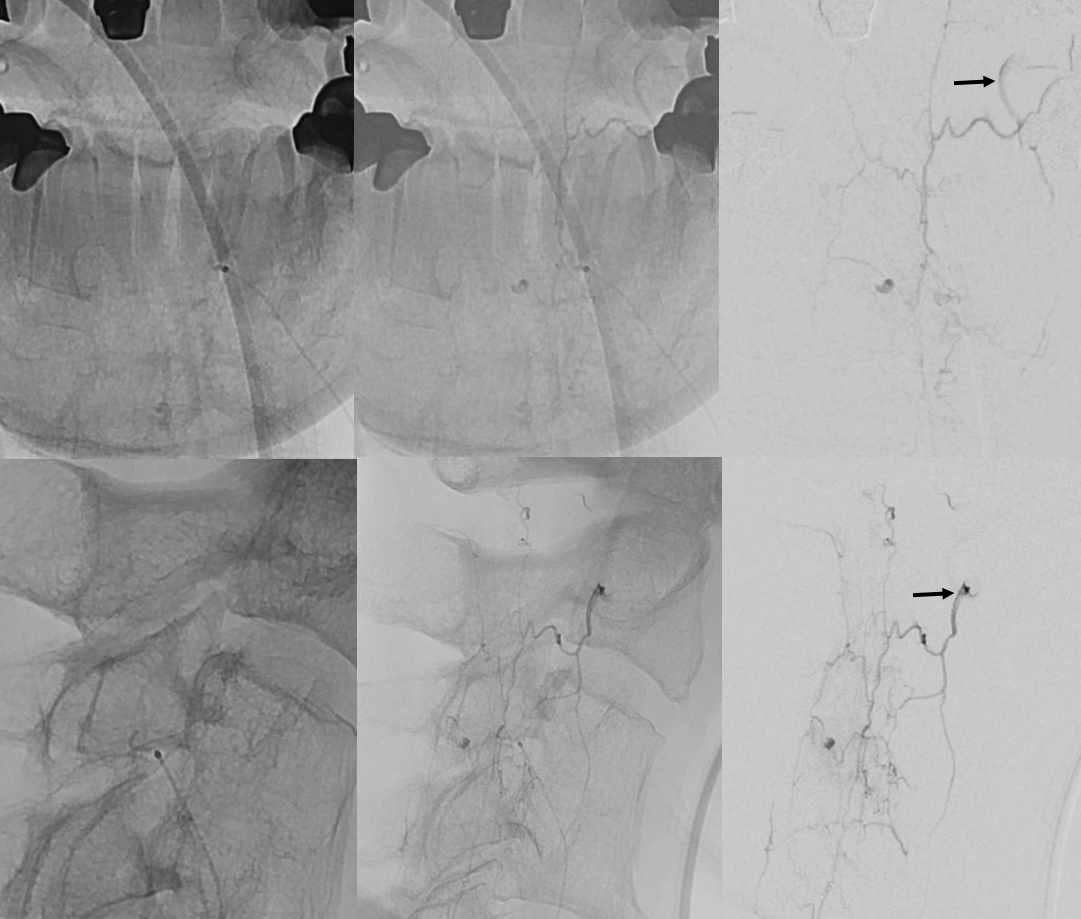
Sagittals — what is this curious vessel shown by white arrowheads?
nBCA cast — it was a 3:2 nBCA:Lipidol mix with some tantalum added. The idea is to make nBCA polymerise relatively quickly — before reaching the vert connection — and easier to see with tantalum addition. However, the tantalum was a mistake — injection became very difficult about half way through the catheter length — probably due to tantalum clumping. Pushed anyway as guide was in ascending cervical distal to vert, but there is a risk of catheter rupture. thankfully that did not happen. We did not fill the pseudoaneurysm, but in this case it was felt to be a success anyway — a rebleed is very unlikely.
Dyna of nBCA cast — always more than meets the eye during injection
Sagittals — beautiful images of the lateral epidural anastomosis extending up and down the dura
Complete occlusion is confirmed on post DSA
How common are arterial pseudoaneurysms in epidural hematomas? Very rare. Are they worth angiographically looking for in an apparently spontaneous epidural bleed (no anticoagulation, trauma etc) — yes, we believe so. Very few places angio these — so the true incidence is likely higher
https://link.springer.com/article/10.1007/s00701-016-2806-4