
An example of preop embolization for JNA — a kind of tumor that is essentially inoperable without effective embolization.
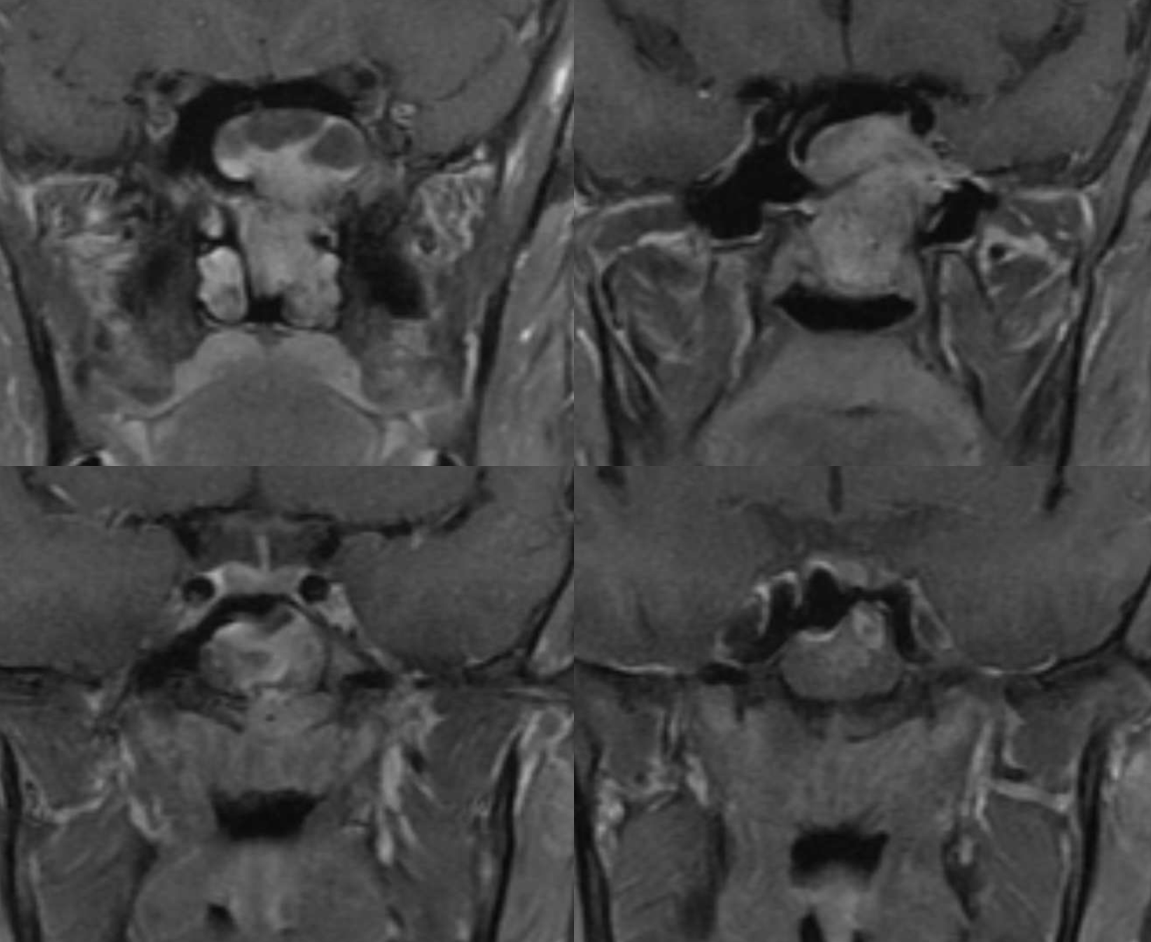
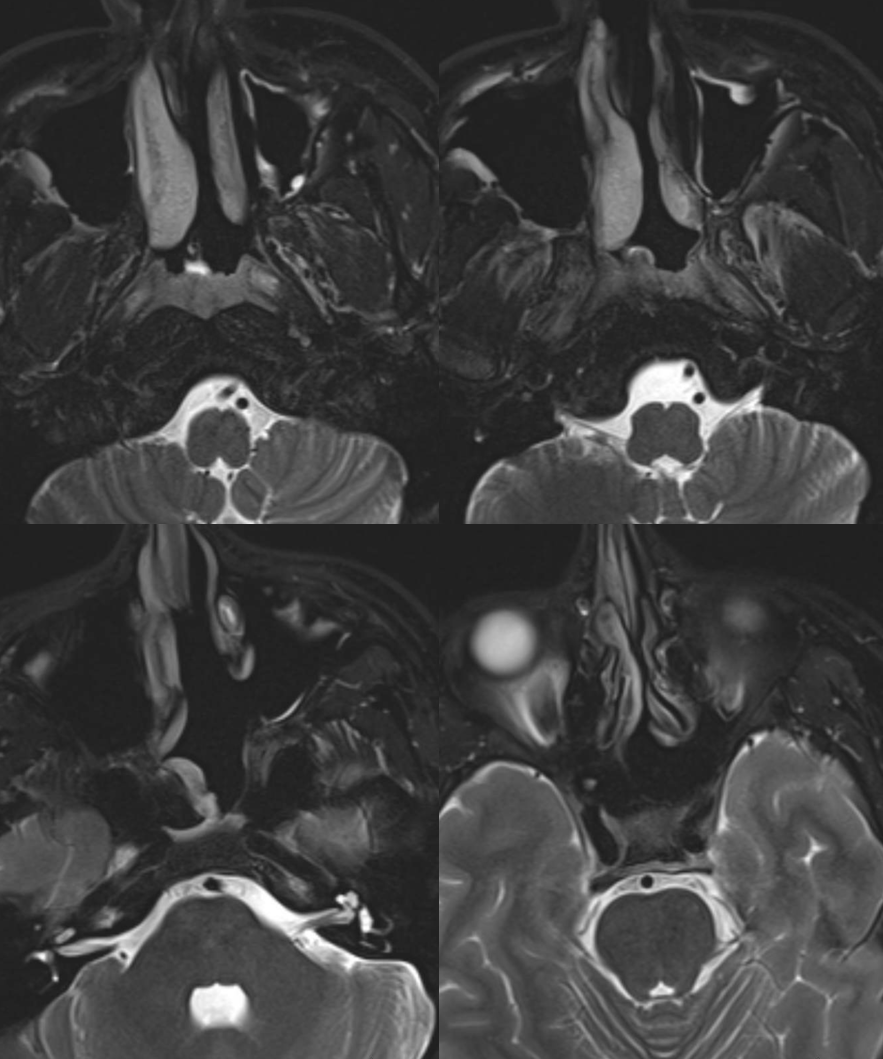
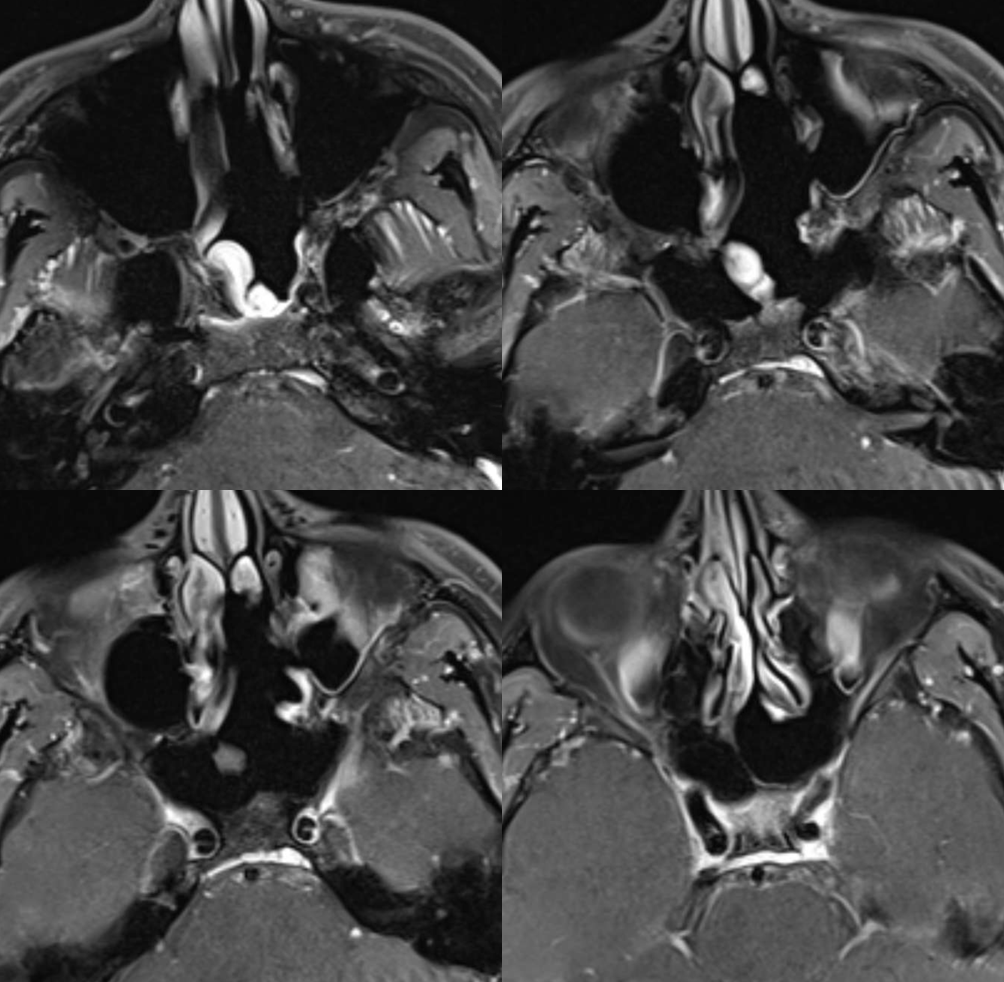
Typical MRI
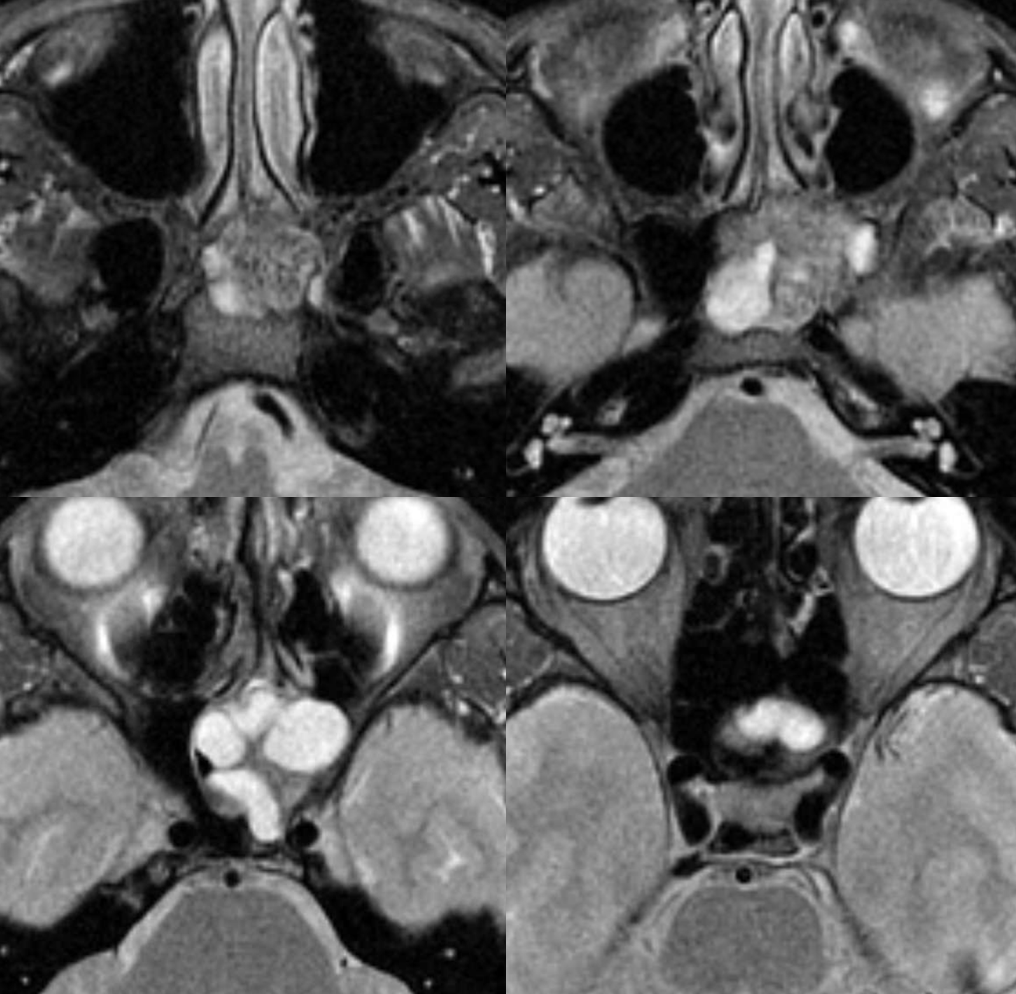
Axial T2s
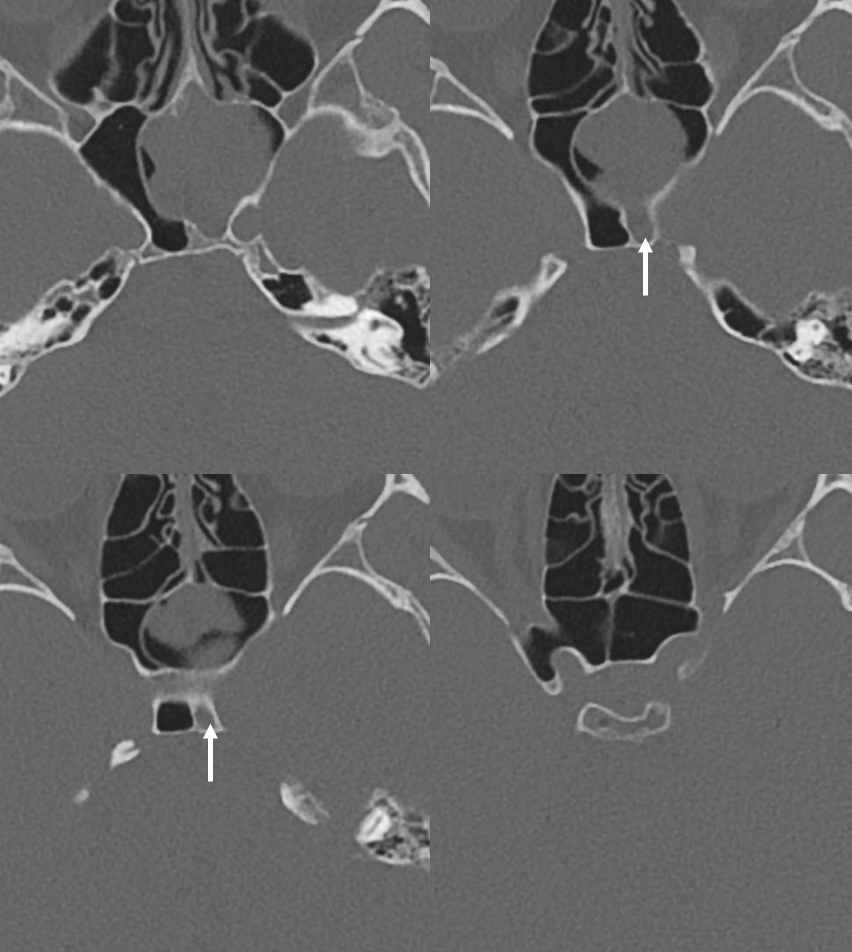
CT axials show particularly extension into sphenoid sinus
Coronals — notations made by ENT and diagnostic radiology team — careful presurg planning. Looking for intracranial extension (lower left image)
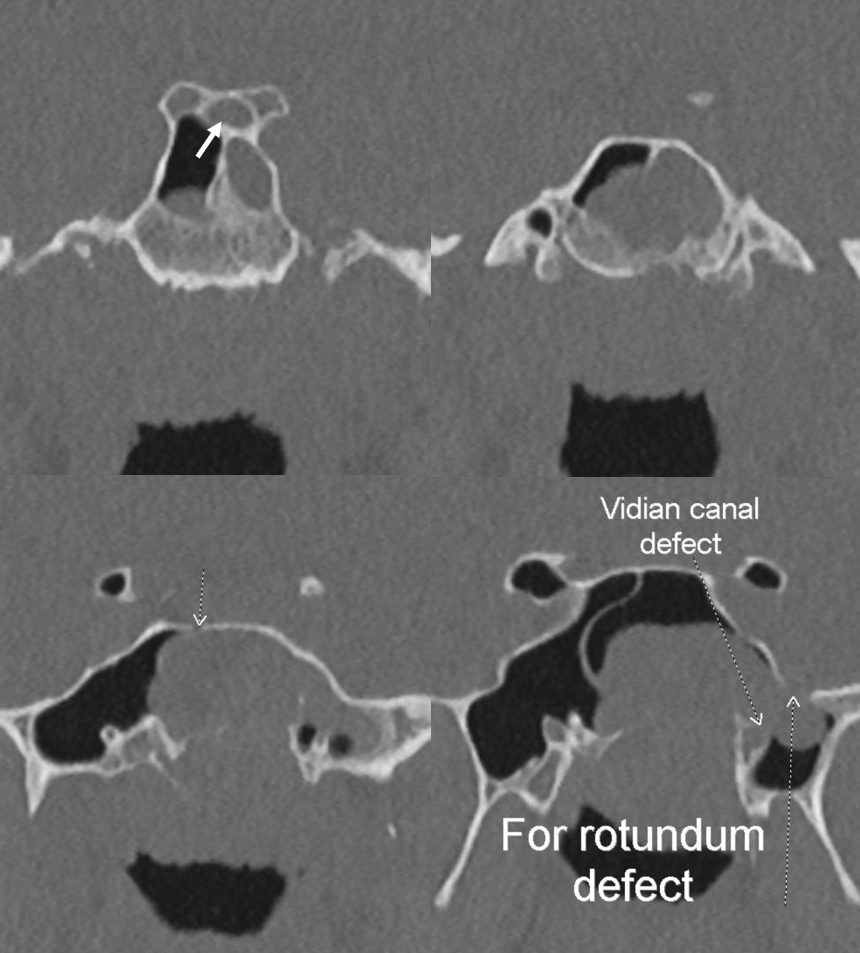
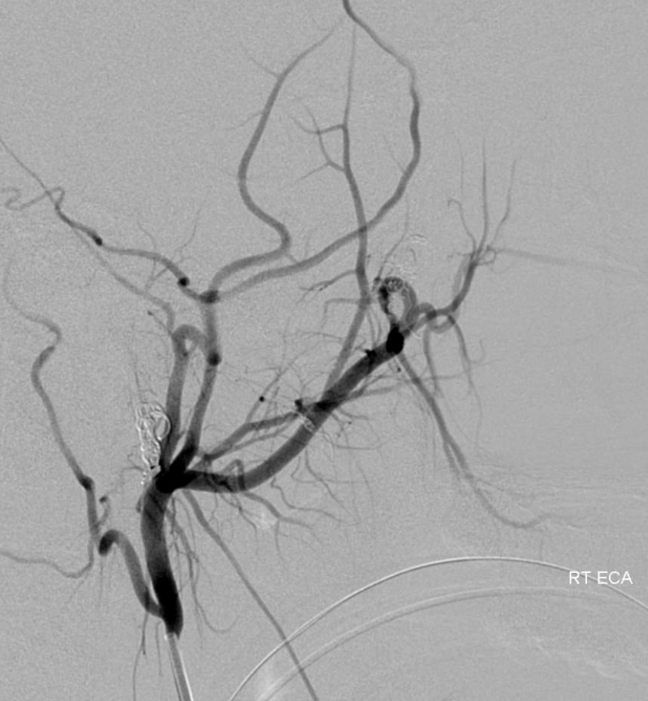
Classic supply in the pterygopalatine fossa — posteriorly projecting branches of the IMAX include, from top to bottom, foramen rotundum (37), vidian (52), and pterygovaginal (53) branches.
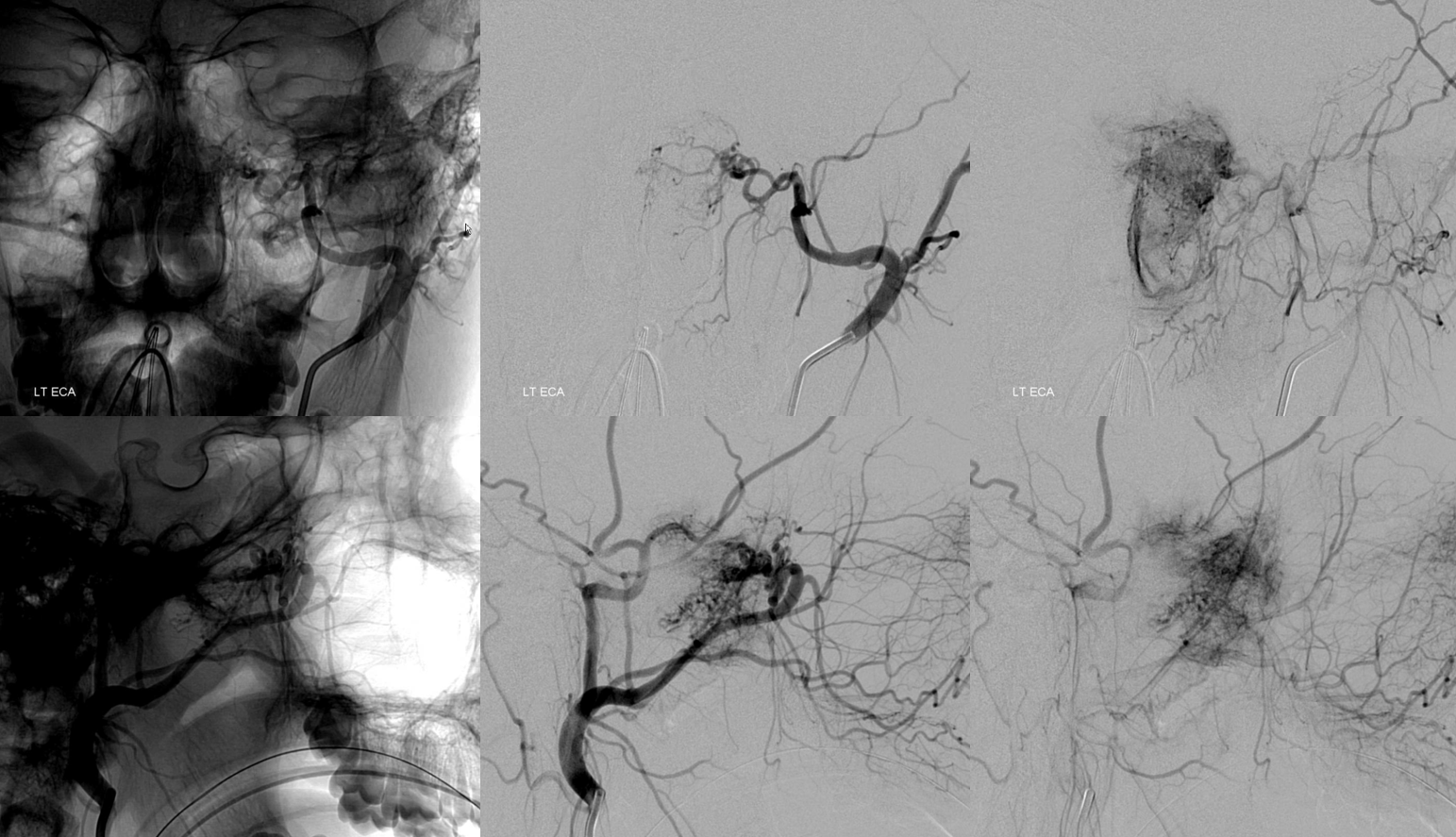
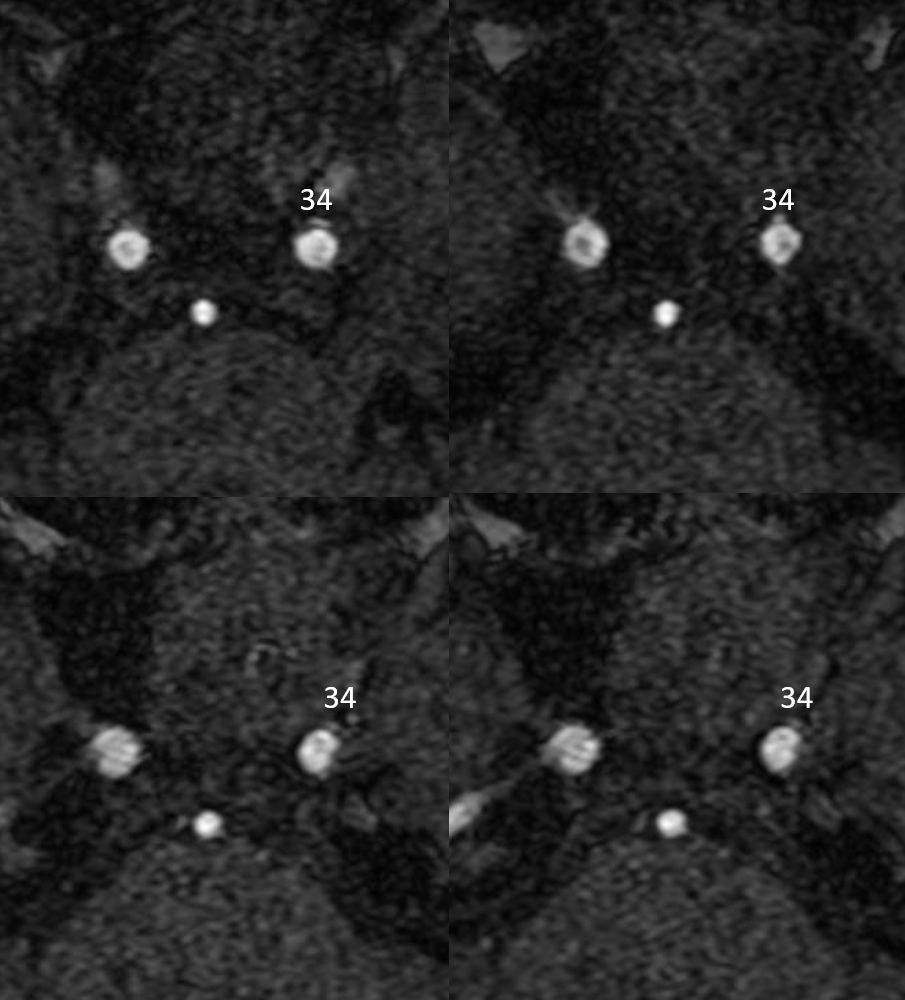
A rarely seen, except in JNA, foramen lacerum branch (34, master diagram) connecting the superior division of the ascending pharyngeal artery and the ICA — classically the ILT. As you can see, in this case the artery is opacified from the ICA, and originates proximal to the ILT. They don’t read books, you know…

In retrospect, foramen lacerum branch (34, master diagram figure) is seen on the MRA
Distal IMAX (likely pterygovaginal) branch supply. Notice extension into upper sphenoid sinus (projects very high on lateral views, just below the sella — as it should, and medial on frontal views

Small particle Contour 45-150 um are best for good devascularization in our opinion
During Embo
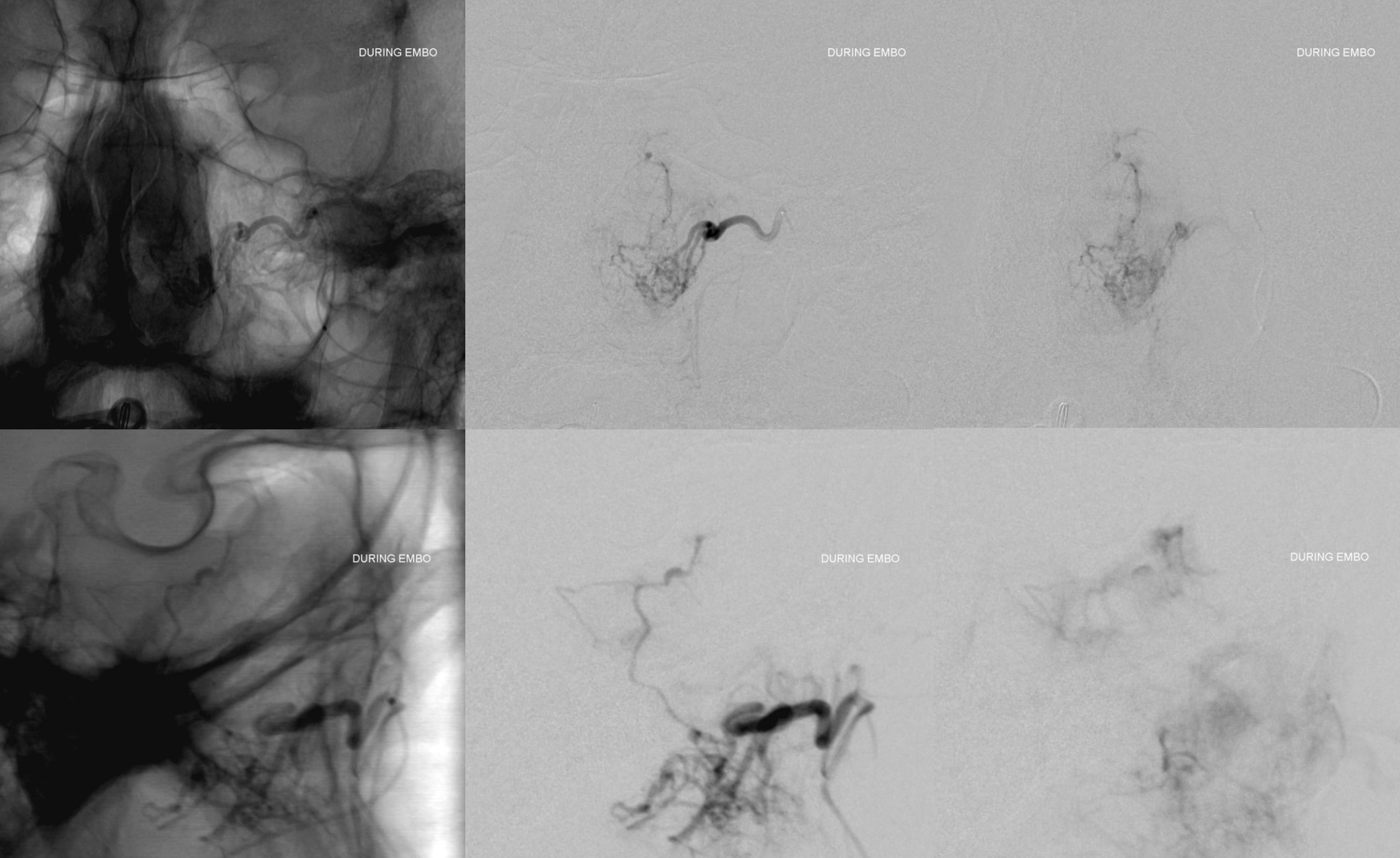
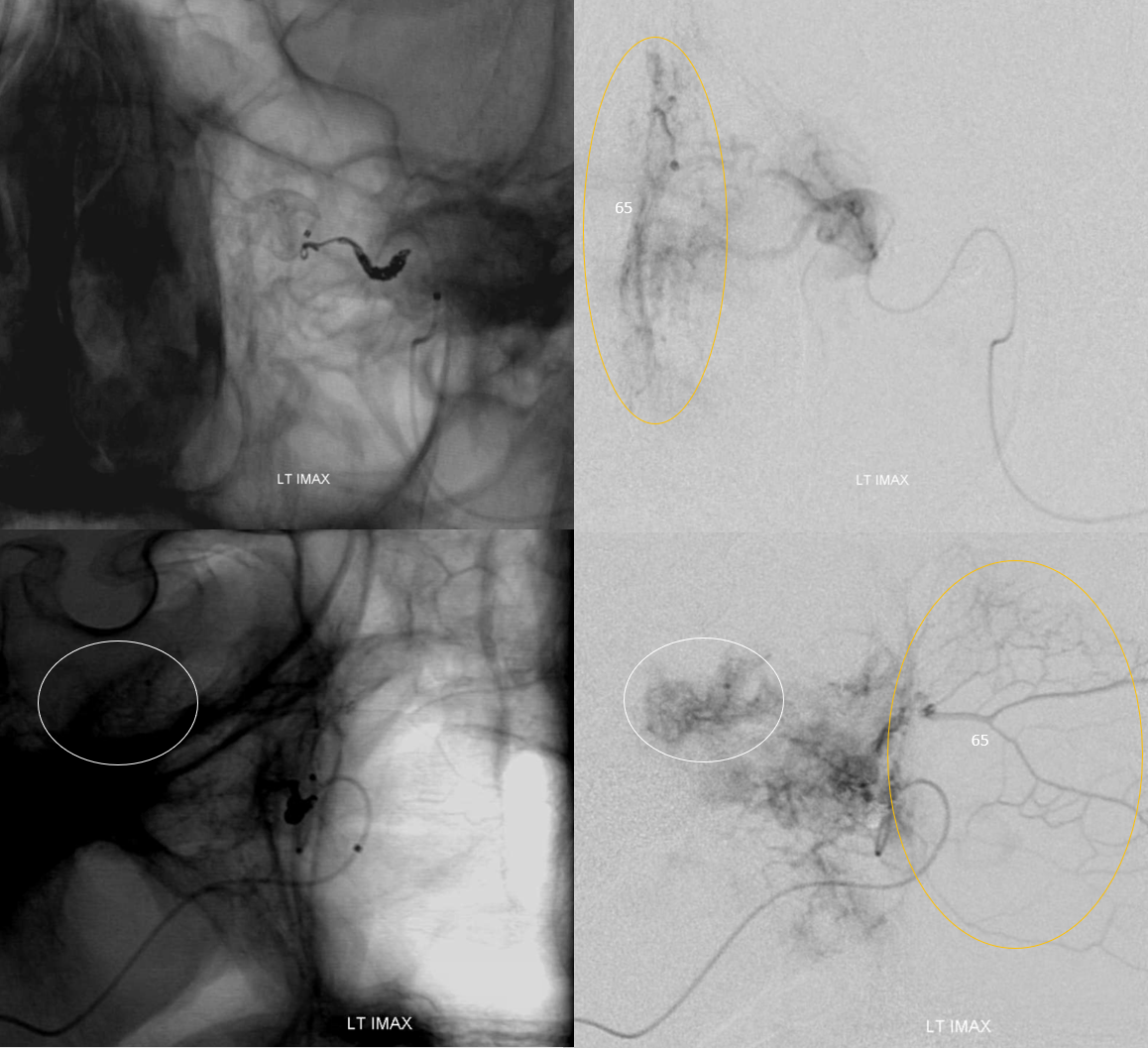
Additional supply from distal IMAX — notice nice demonstration of septal network (oval, 65 in master figure)
Post left distal ECA. Done? Of course not
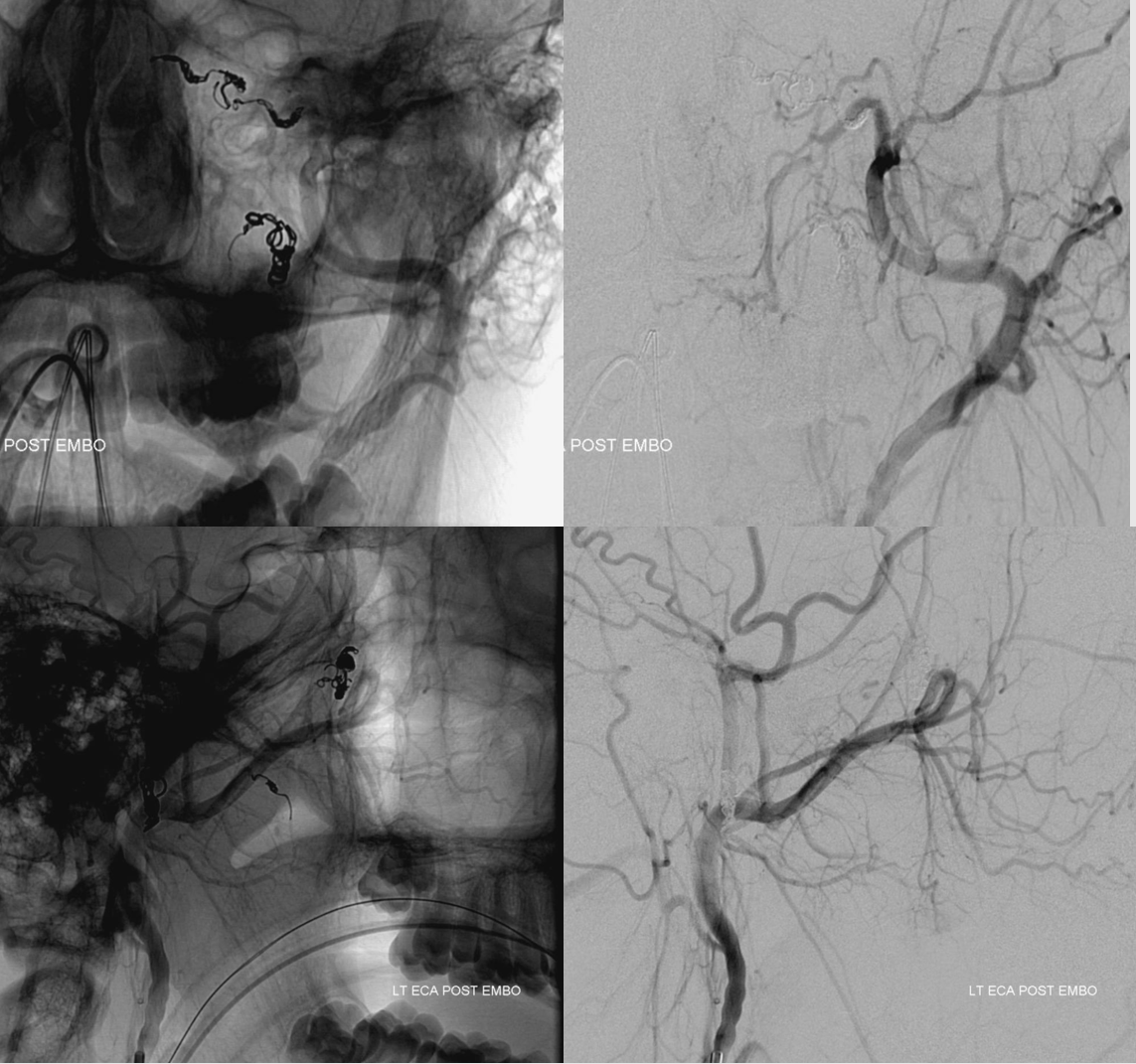
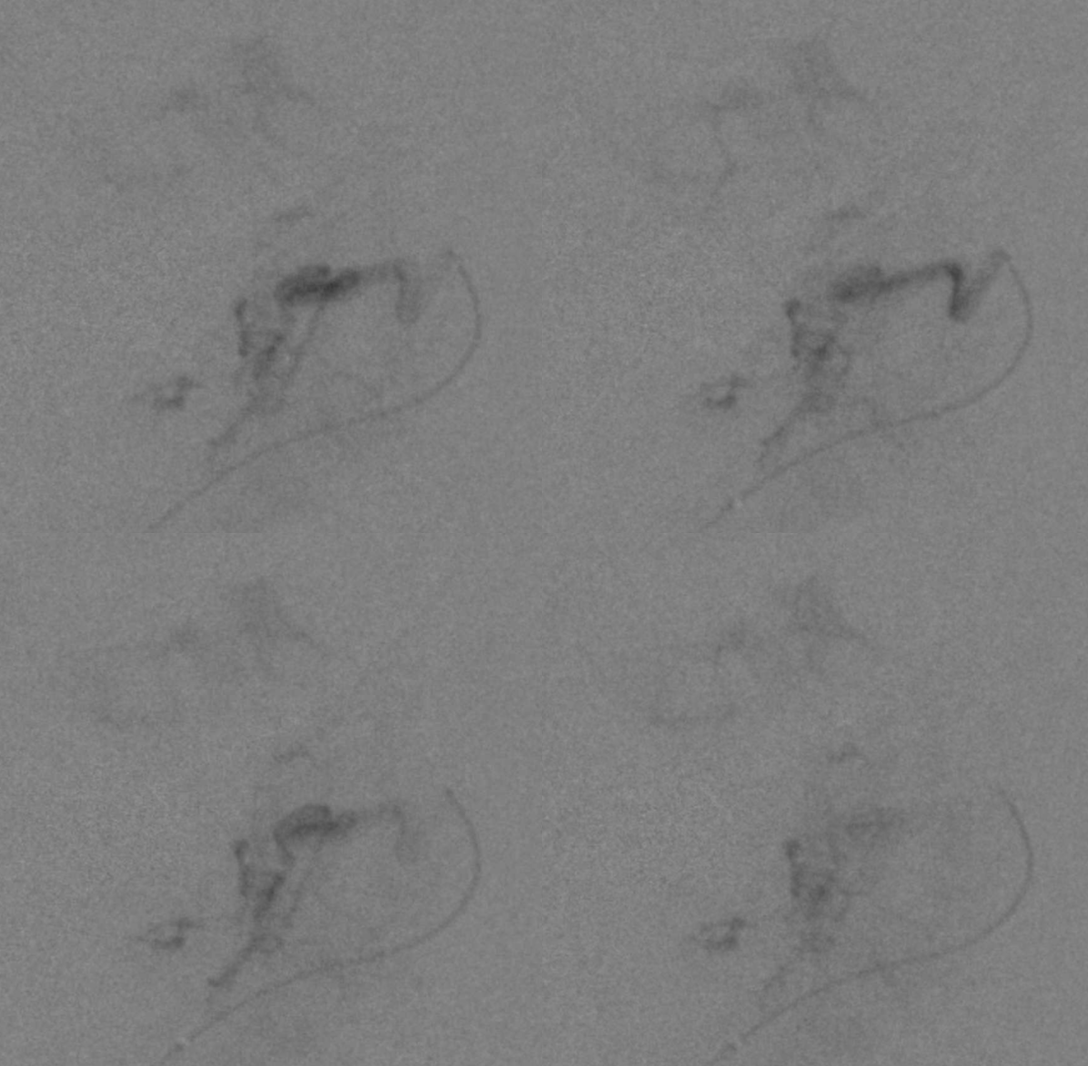
The main collateral to the region of pterygopalatine fossa is the Ascending Pharyngeal — superior division (51) of the pharyngeal trunk
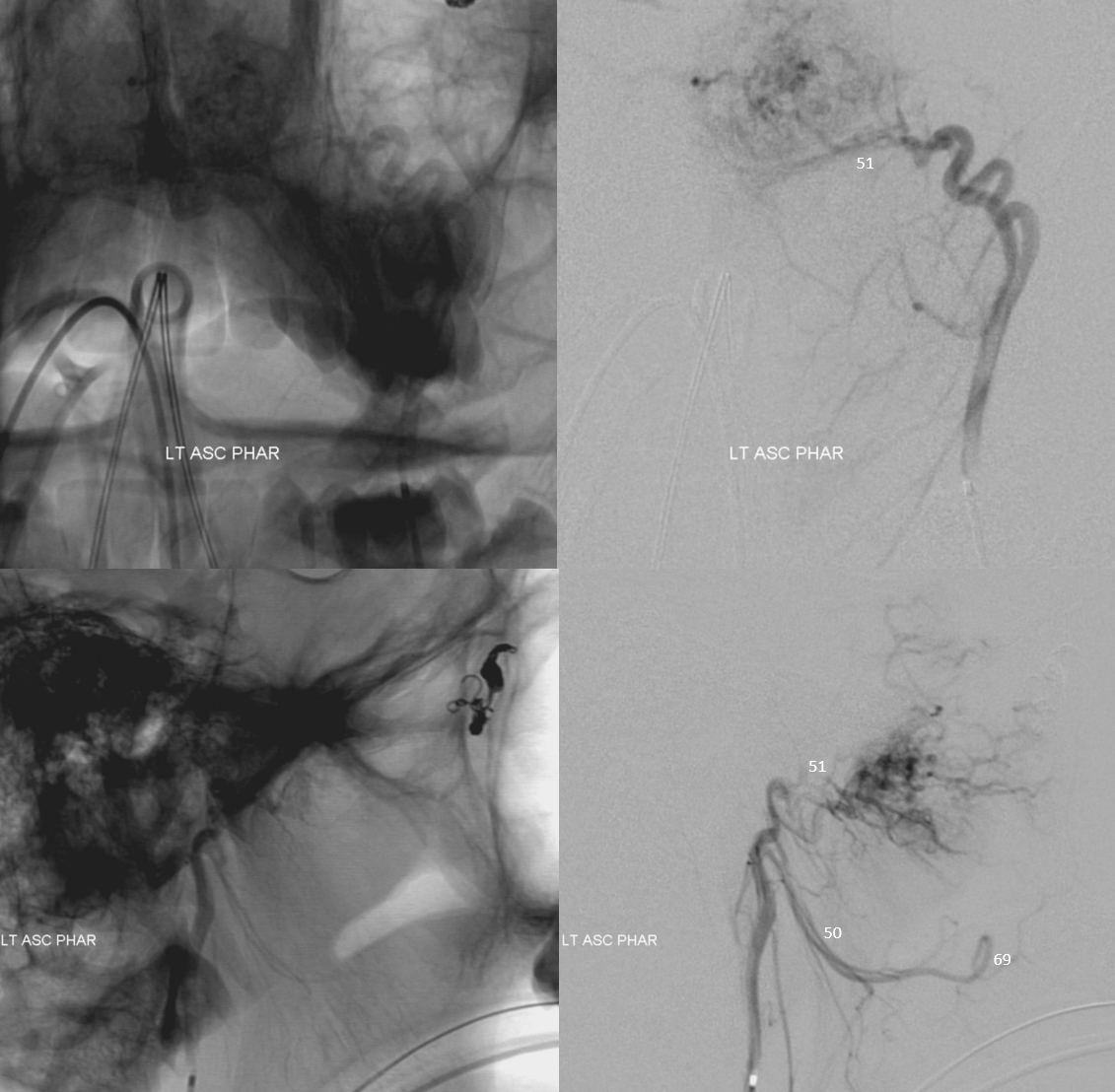
After AP embo, the lacerum branch (34) remains. It proved resistant to catheterization and was the only branch not embolized

Done? of course not. Contralateral AP is not doing much — but nice normal anatomy with superior division (51) supplying upper nasopharynx and middle division (50) suppling artery to soft palate (69)
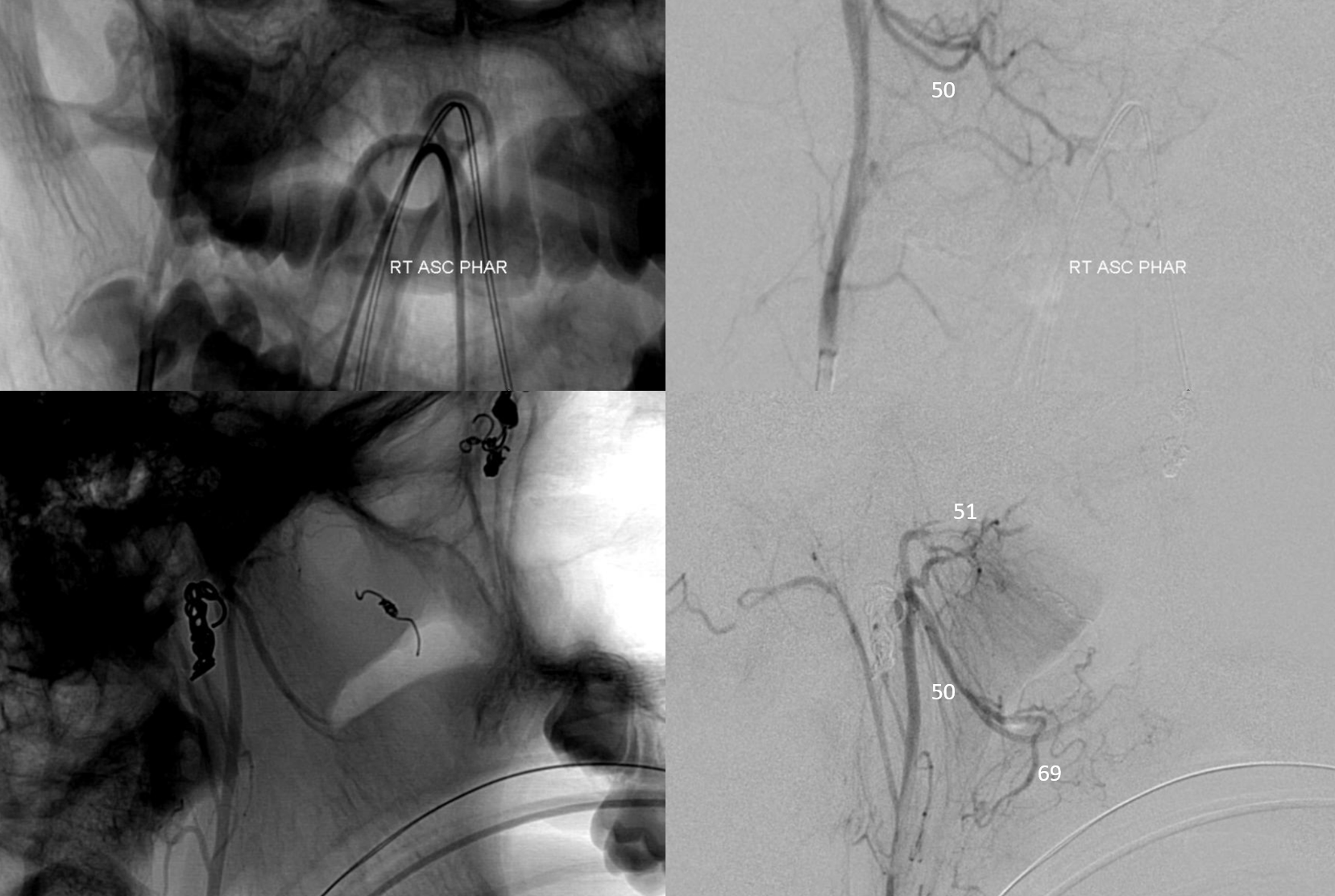
However, the right IMAX does — typically supply is bilateral. Notice coils in embolized branches — we usually put some afterward to prevent short-term recanalization

Post rt ECA
Delayed post resection MRI
Questions/comments: neuroangio@neuroangio.org