
Classic demonstration of “snowplow” during ICAD stenting
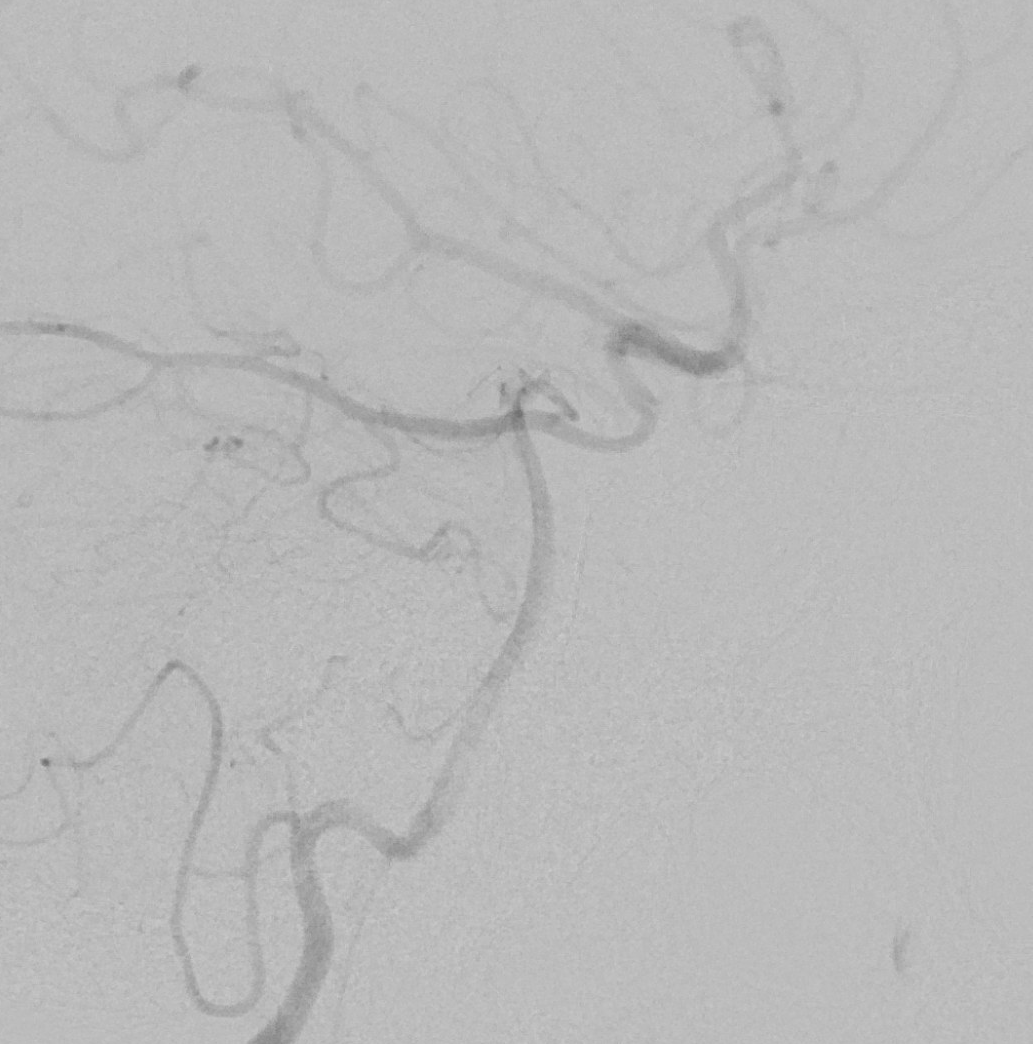
This is actually a SAMMPRIS case — failure of Max Med Management… Still happens sometimes. Stenosis is supraclinoid. Left subclavian injection shows a well-developed and quite useful P1–PCOM ICA reconstitution
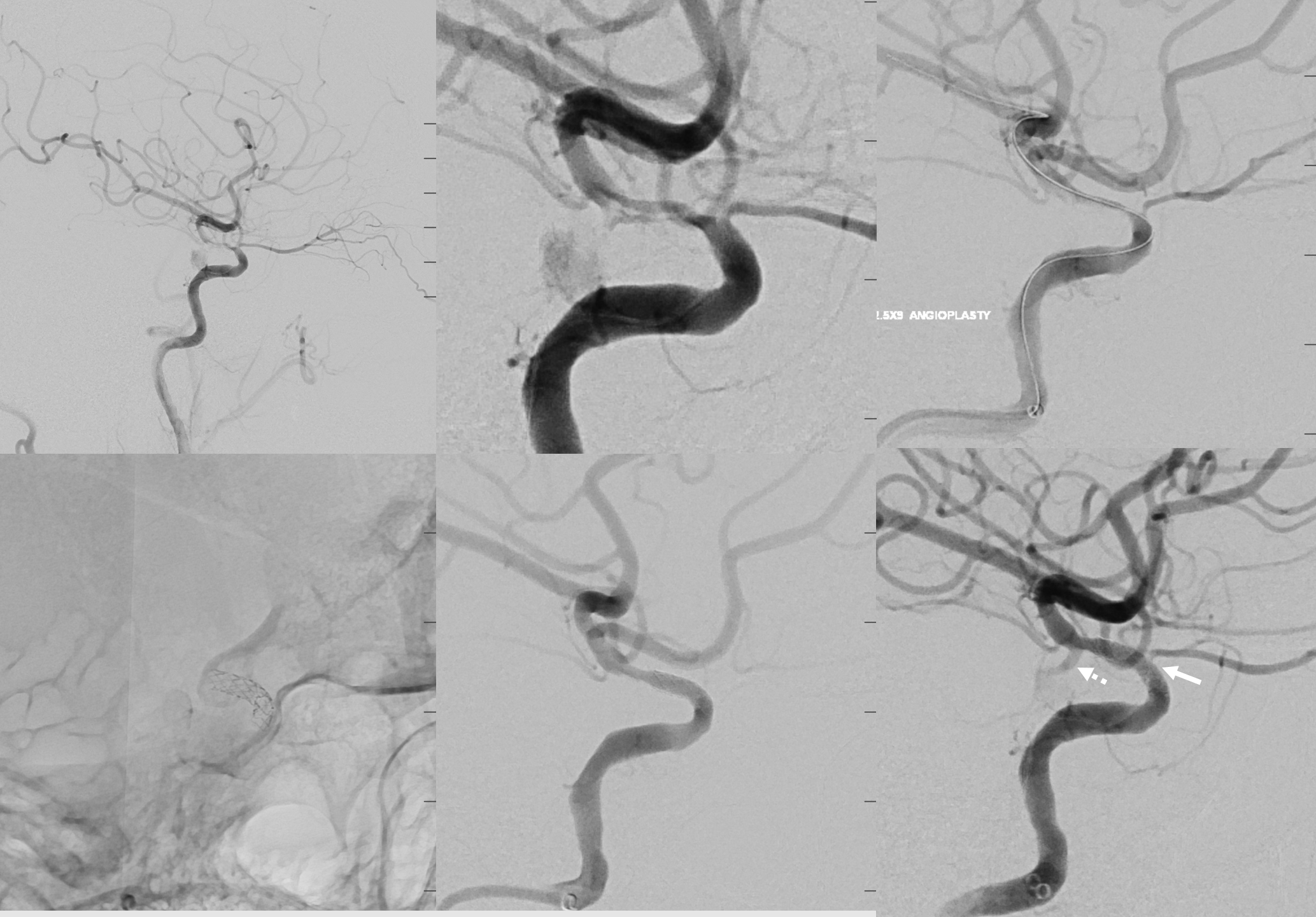
Angioplasty (top right image) done to better understand the relationship of the stenosis to the PCOM. The stent is deployed proximal to PCOM ostium. Even though there is a small stenosis between the distal edge of stent and PCOM , leaving PCOM uncovered is important for the future, should there be re-stenosis or occlusion.
Note that after stenting the ophthalmic artery no longer fills well, with a critical stenosis (arrow). This is the “snowplow effect”. Note flash-filling of the PCOM (dashed arrow) — attesting to both its preservation and improved hemodynamics post stenting
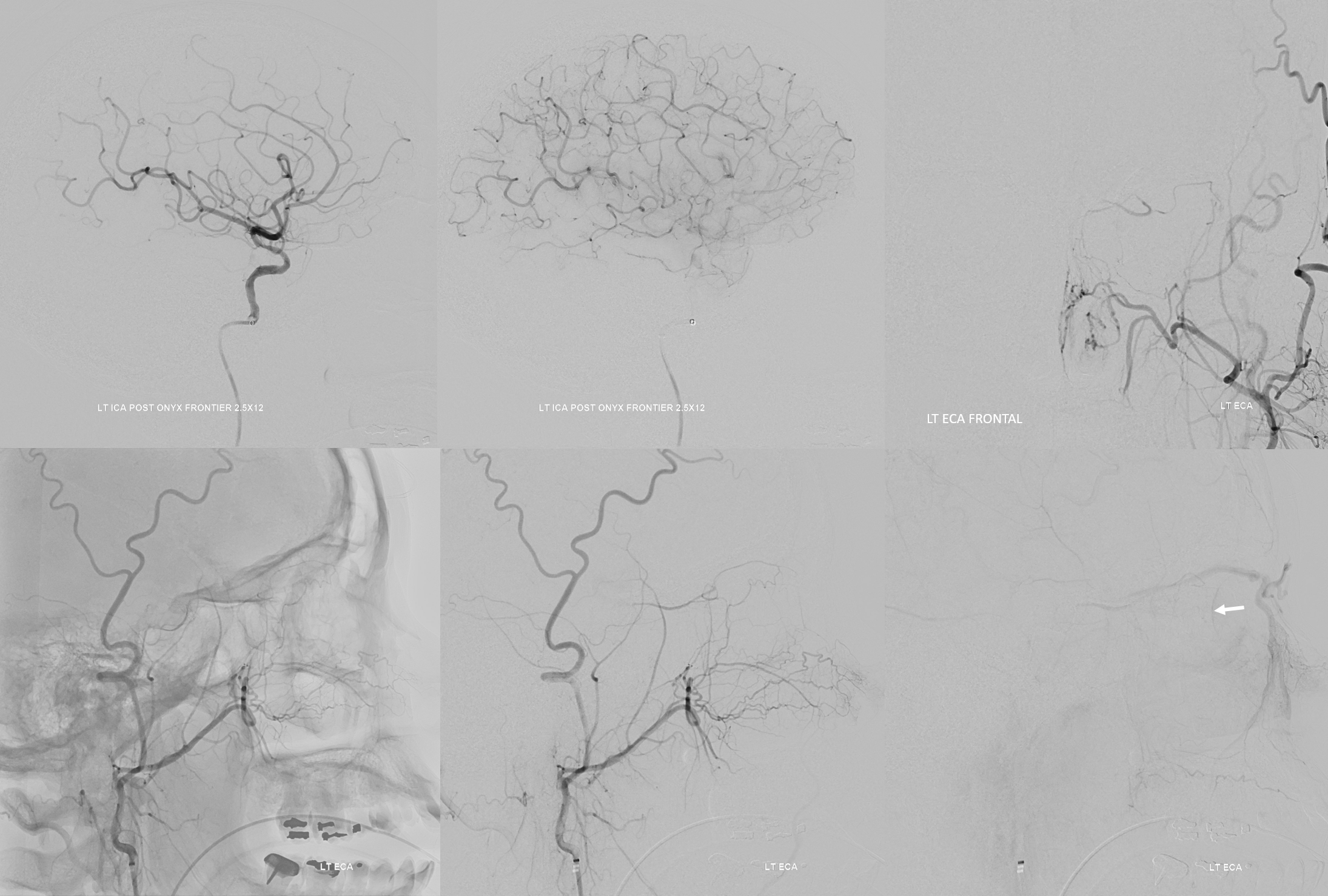
A few minutes later, during global ICA run, the ophthalmic artery is completely closed. However, ECA injection frontal (top right) and lateral (bottom row) shows robust reconstitution via ethmoidal and anterior deep temporal anastomoses. The choroidal blush is well seen (arrow) — which does NOT prove that patient can see.
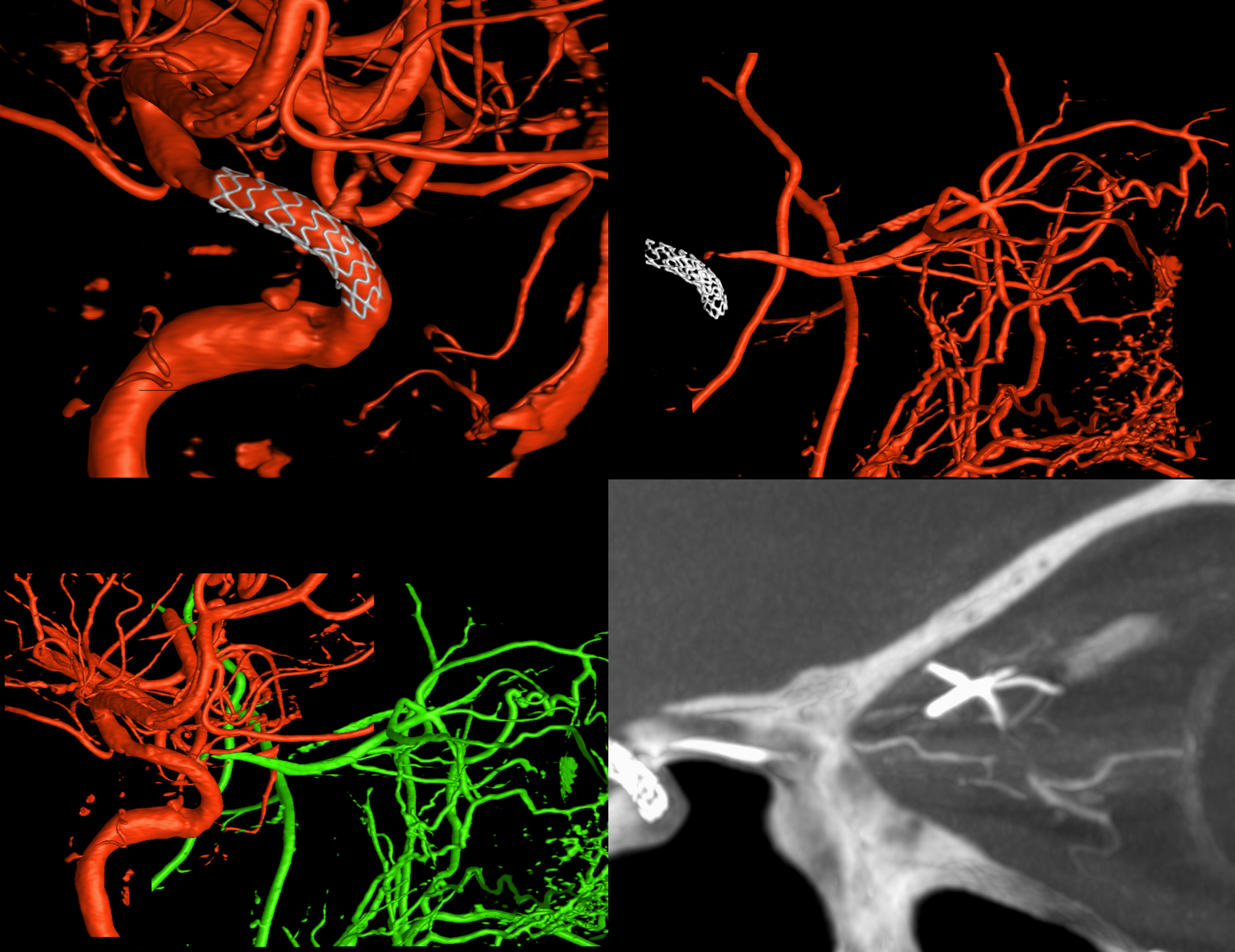
DYNA CT images. Note excellent reconstitution during ECA injection (top right, bottom left fusion), and demonstration of central retinal patency on MIP image (bottom right)
Less noted are effects on other vessels, such as the Superior Hypophyseal Artery (arrows, image below), which in fact supplies part of the optic nerve (middle right coronal image, arrow).
Bottom row snowplow occlusion of the superior Hypophyseal. Despite this, vision was preserved.
Stenting is a limited control procedure. Snowplow may or may not happen. It may or may not be clinically important. These factors contribute to the higher risk of ICAD stenting.
