
Case courtesy Dr. Erez Nossek.
What you don’t see leads to when patient can’t see.
Another example of the Network principle. There is a spectrum of meningeal-ophthalmic connections we cover extensively in MMA and ophthalmic artery pages. The point is that these connections are many, and their visualization is dependent on hemodynamic and technical factors — injection pressure, catheter position, vessel size, etc. Good angiographic technique and knowing anatomy is how you stay safe
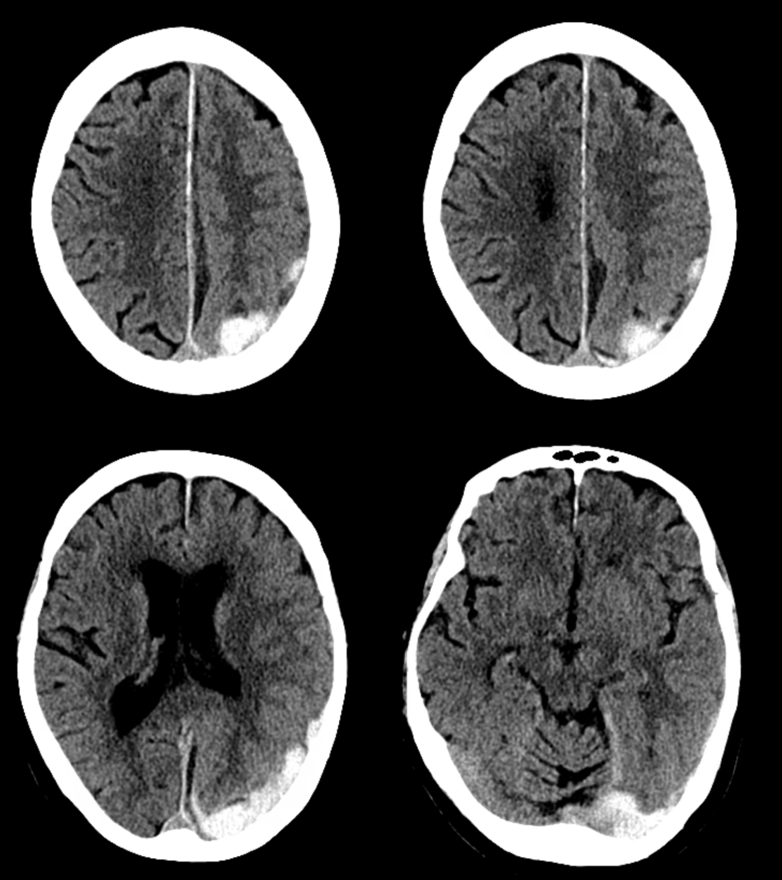
Subdural hematoma
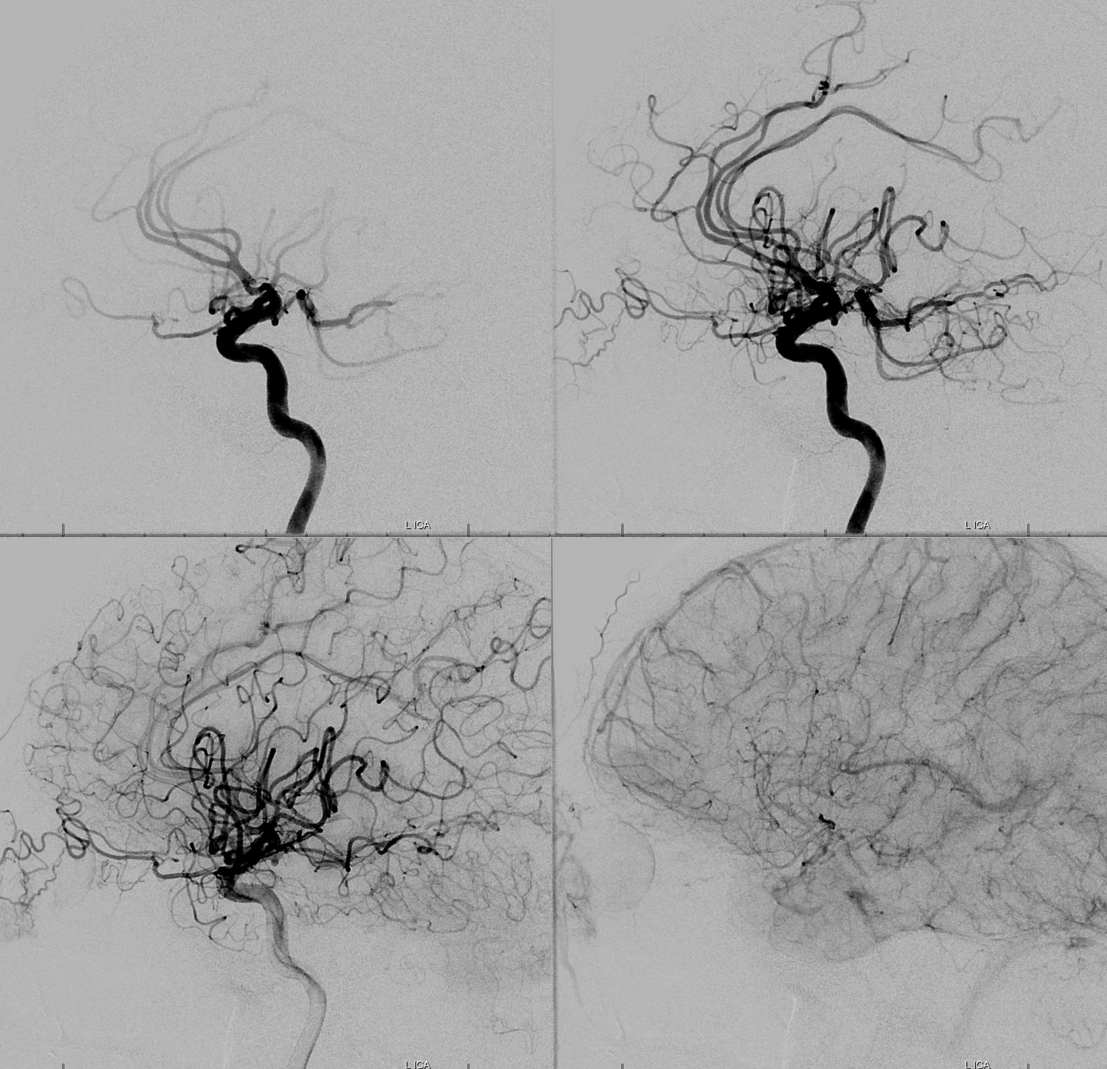
usual-appearing ophthalmic origin
Usual-appearing frontal ECA
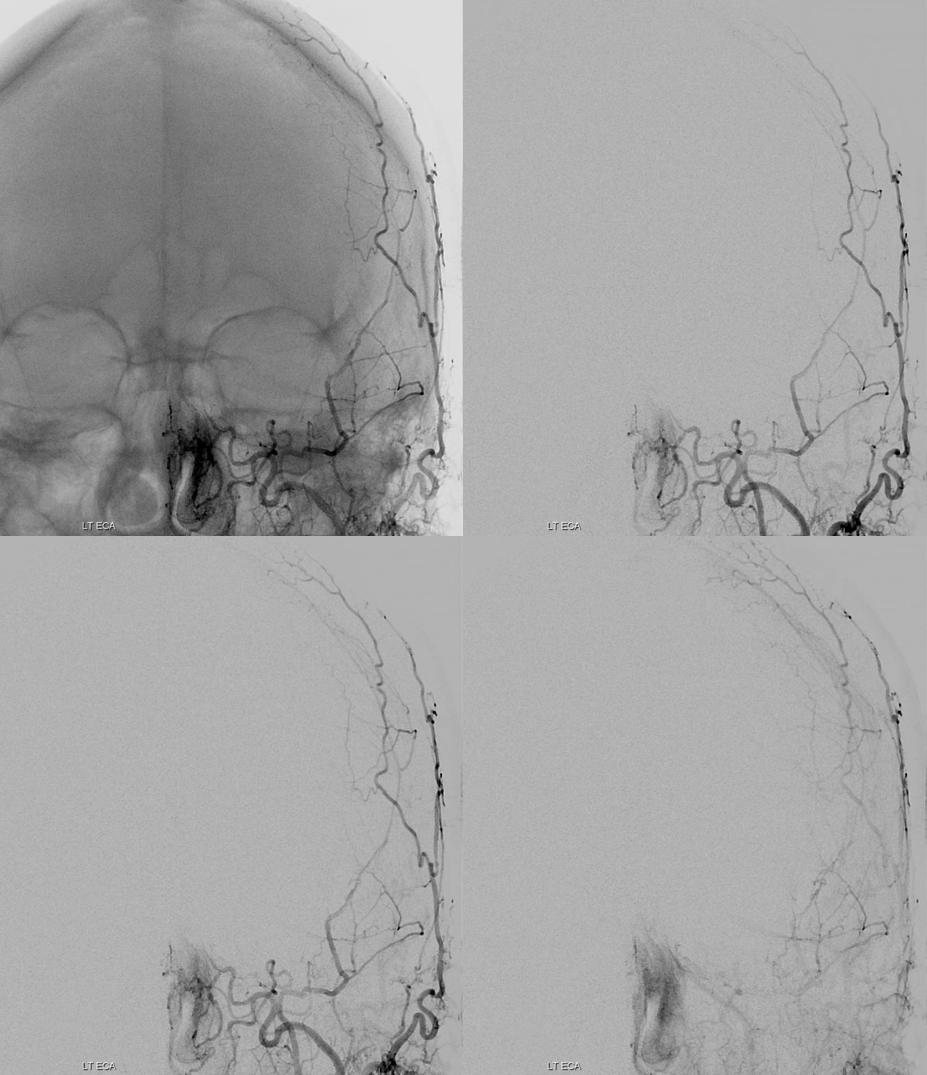
Usual-appearing lateral ECA
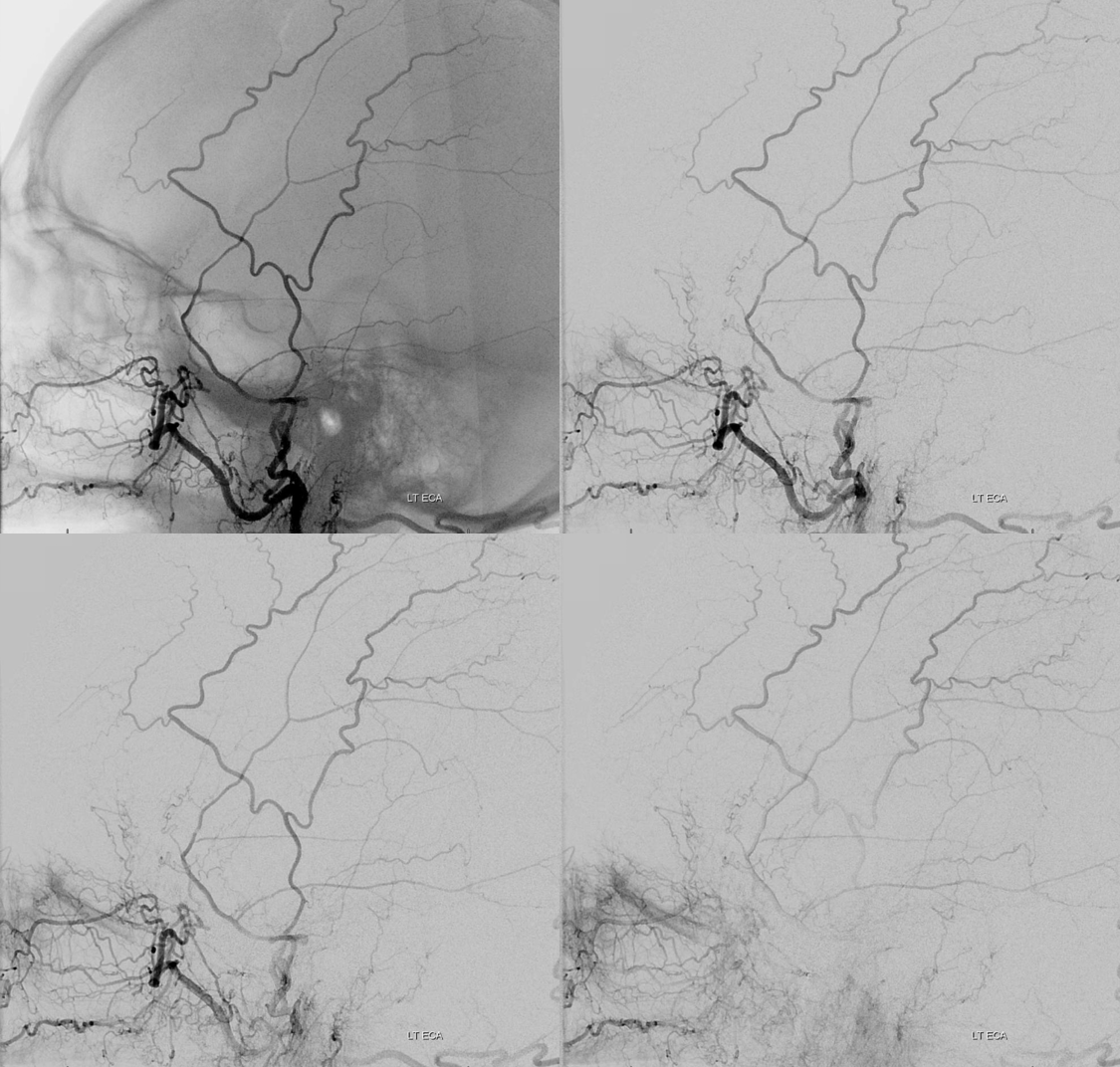
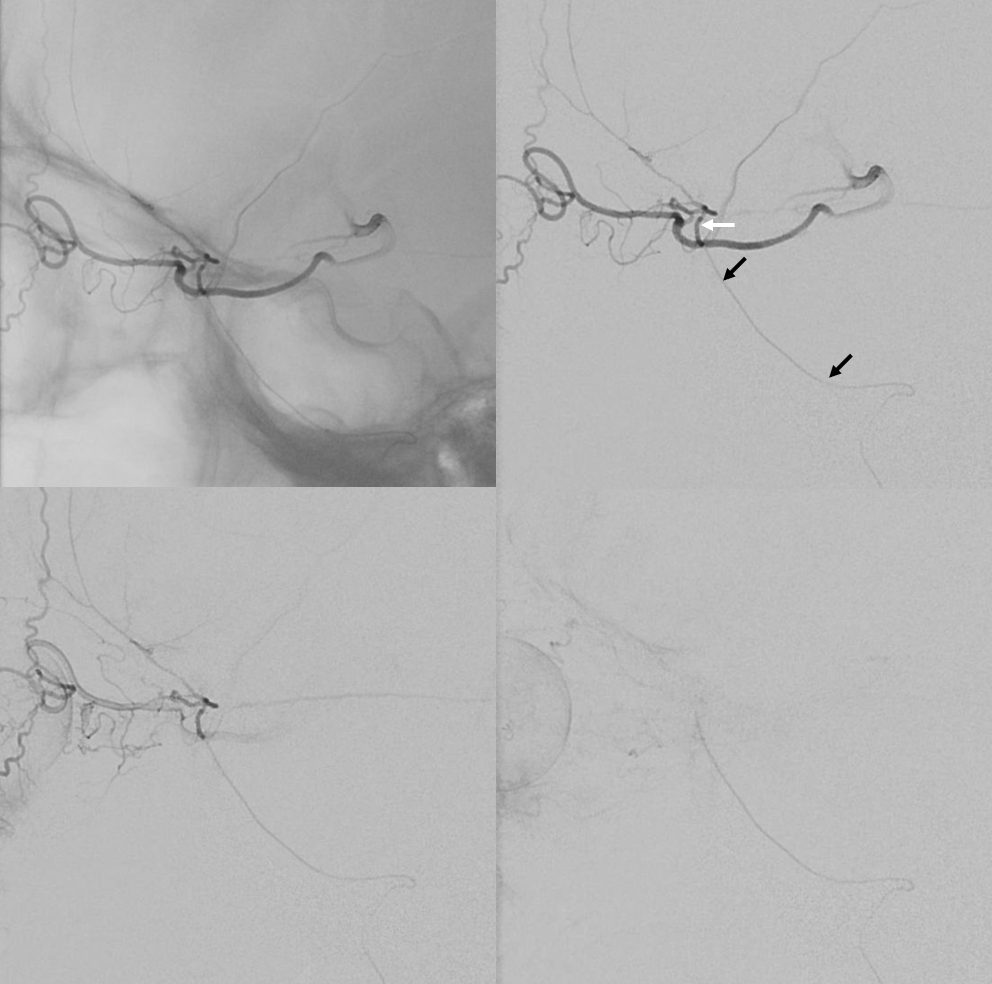
Proximal MMA injection. Catheter – black arrows, sphenoid ridge branch (40) — white arrow. The sphenoid ridge branch is the usual connection between the MMA and proximal ophthalmic artery (via superior orbital fissure anastomosis [41])
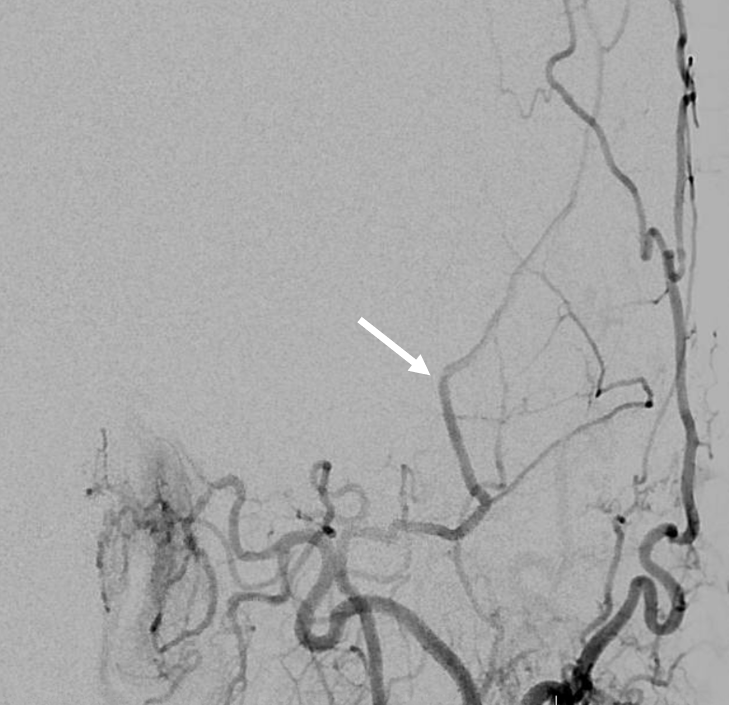
A detailed look at the preceeding ECA injection shows subtle unopacified inflow at the junction with the sphenoid ridge branch
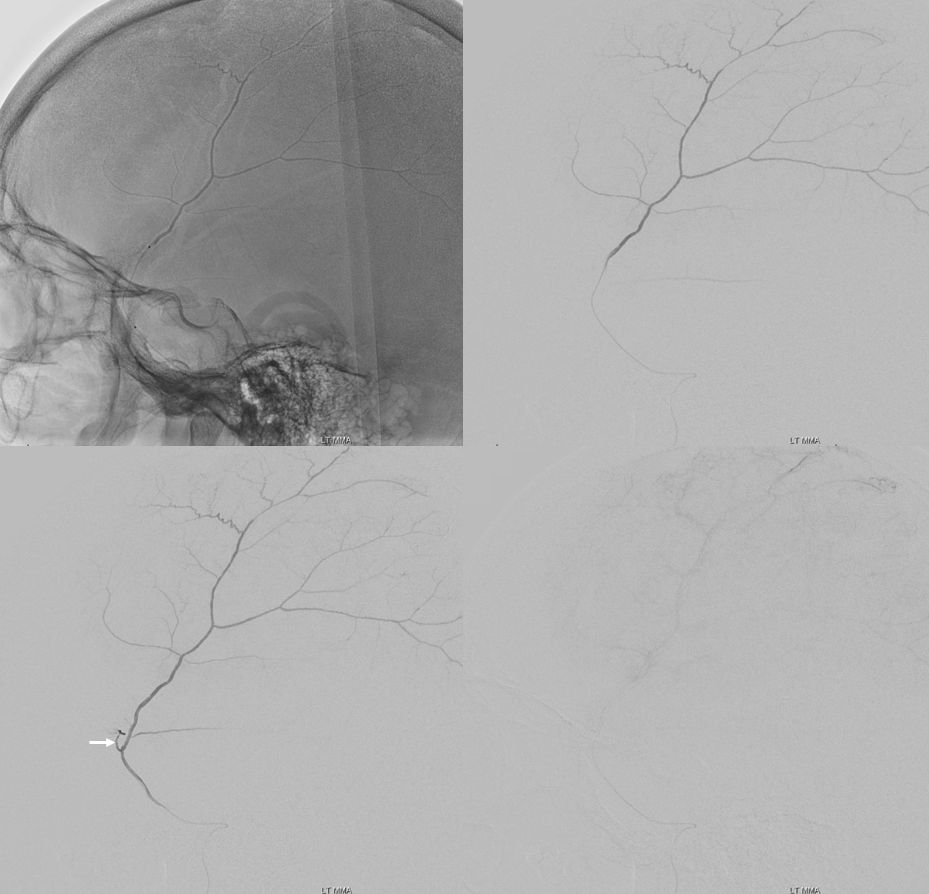
A more distal position in the MMA. Reflux into proximal sphenoid ridge branch — white arrow
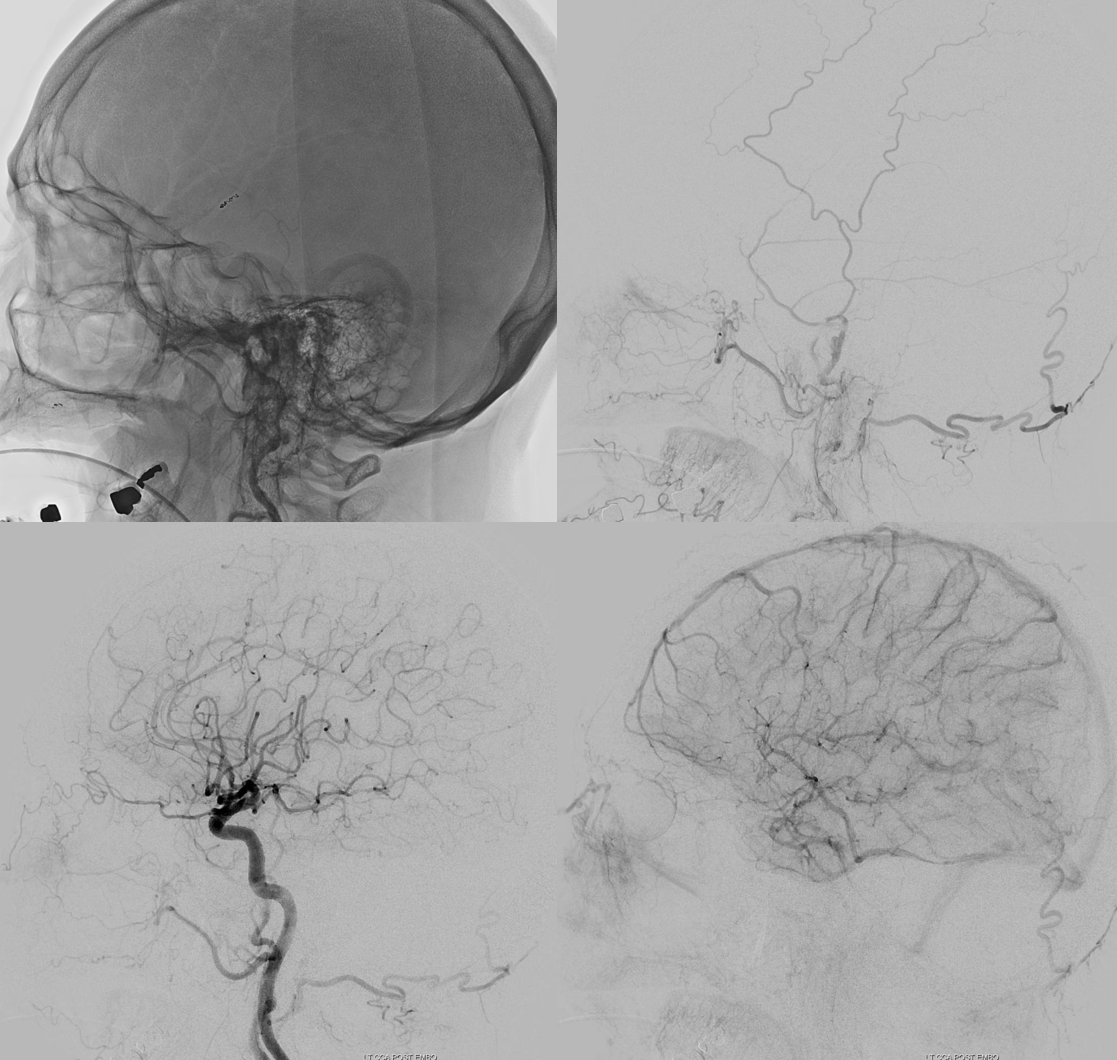
Post embo with PVA and coils — avoiding reflux
Schematic of how this happens
