
Not your typical M1 TICI3. How many more of these do u really want to see anyway?
Case in collaboration with the uber-dedicated and uber-awesome Dr. Sara Rostanski of Bellevue HHC Stroke Center, New York City
Demographics withheld. Presentation is acute quadriparesis progressing to locked in
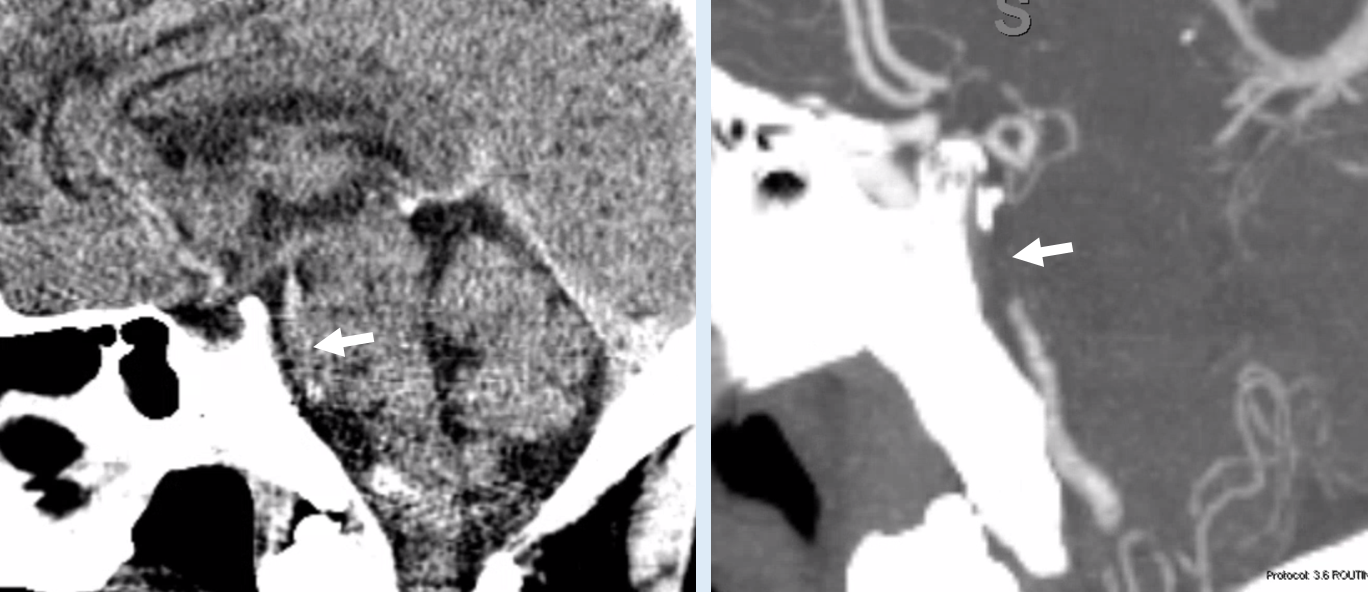
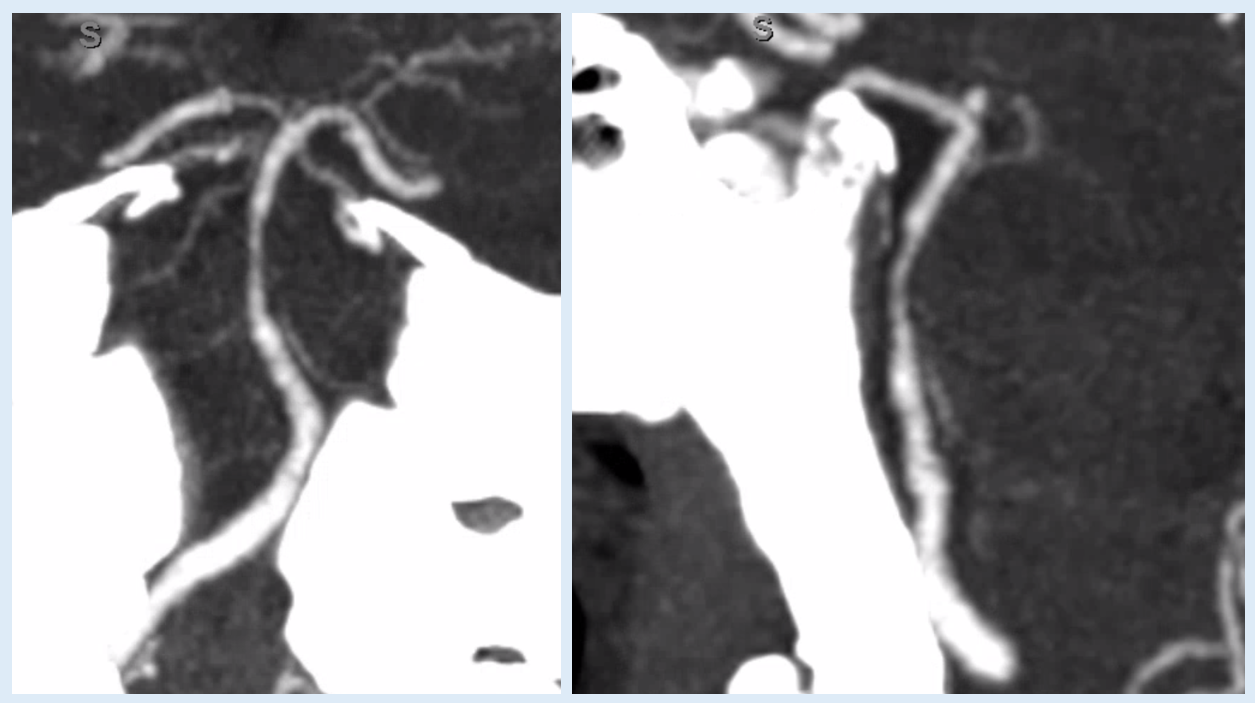
CT on left, CTA on right. CT shows a “hypodense basilar sign” — a relatively hypodense area (white arrow) compared to normal slightly higher density of blood in the upper basilar that is similar to that of straight sinus for example. The same hypodense area is not opacified on CTA. All of this suggests that the problem is not an embolus — atheromatous occlusion is common in the mid-basilar segment, whereas emboli tend to lodge at the top of basilar.
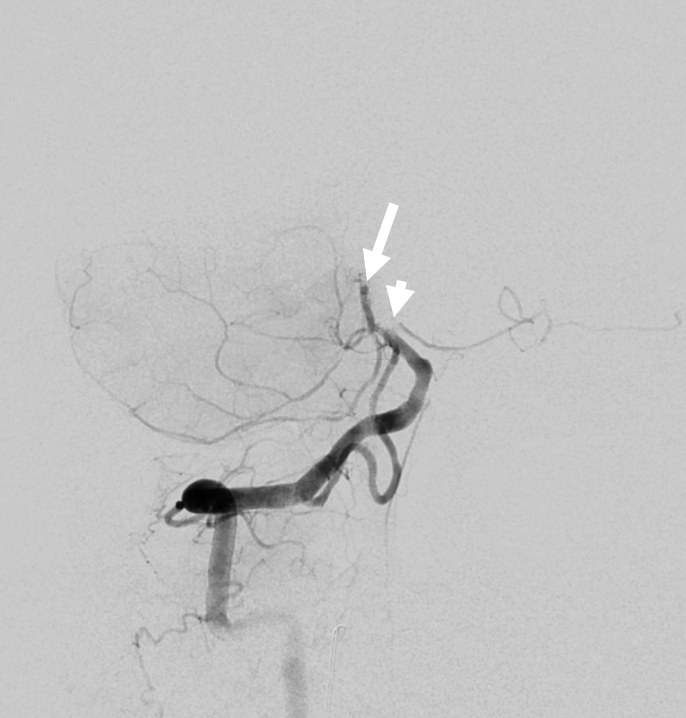
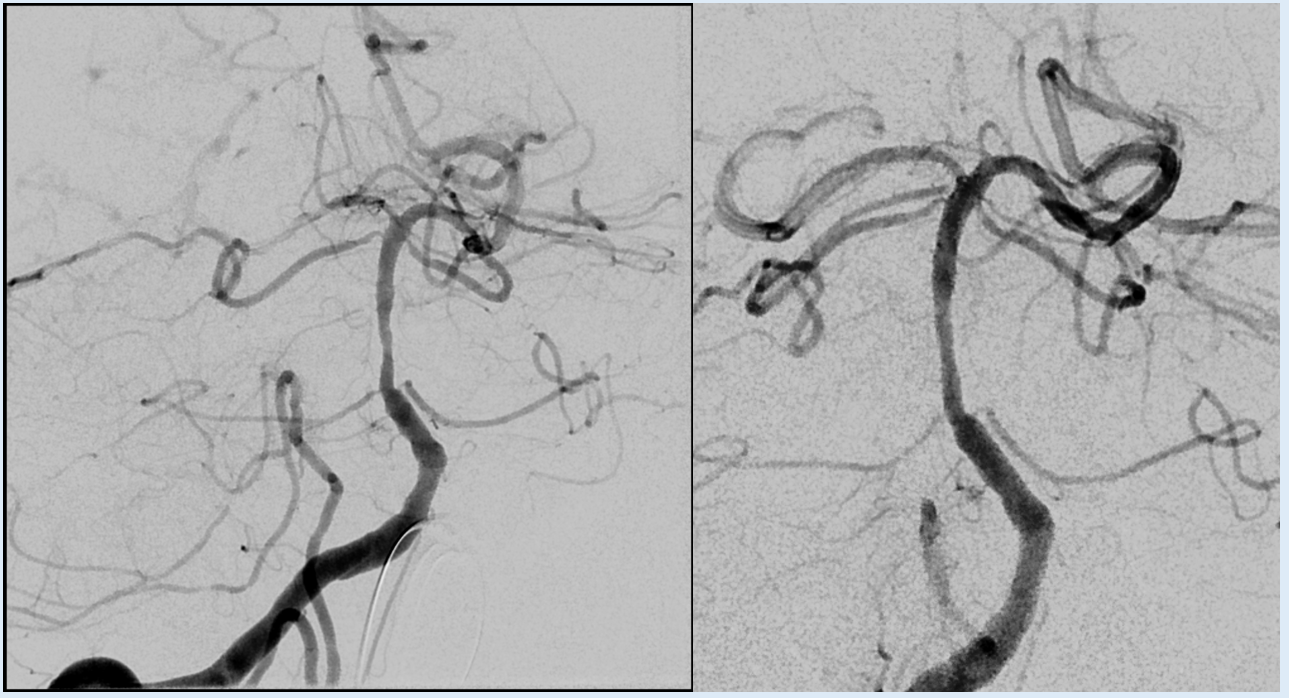
Angio. Notice that there is no sharp cutoff (white arrow) and that there is a stenosis at AICA origin (arrowhead). Both suggest atheromatous disease
The 6F Sofia is advanced under aspiration beyond the level of occlusion — our standard technique to “ingest” clot
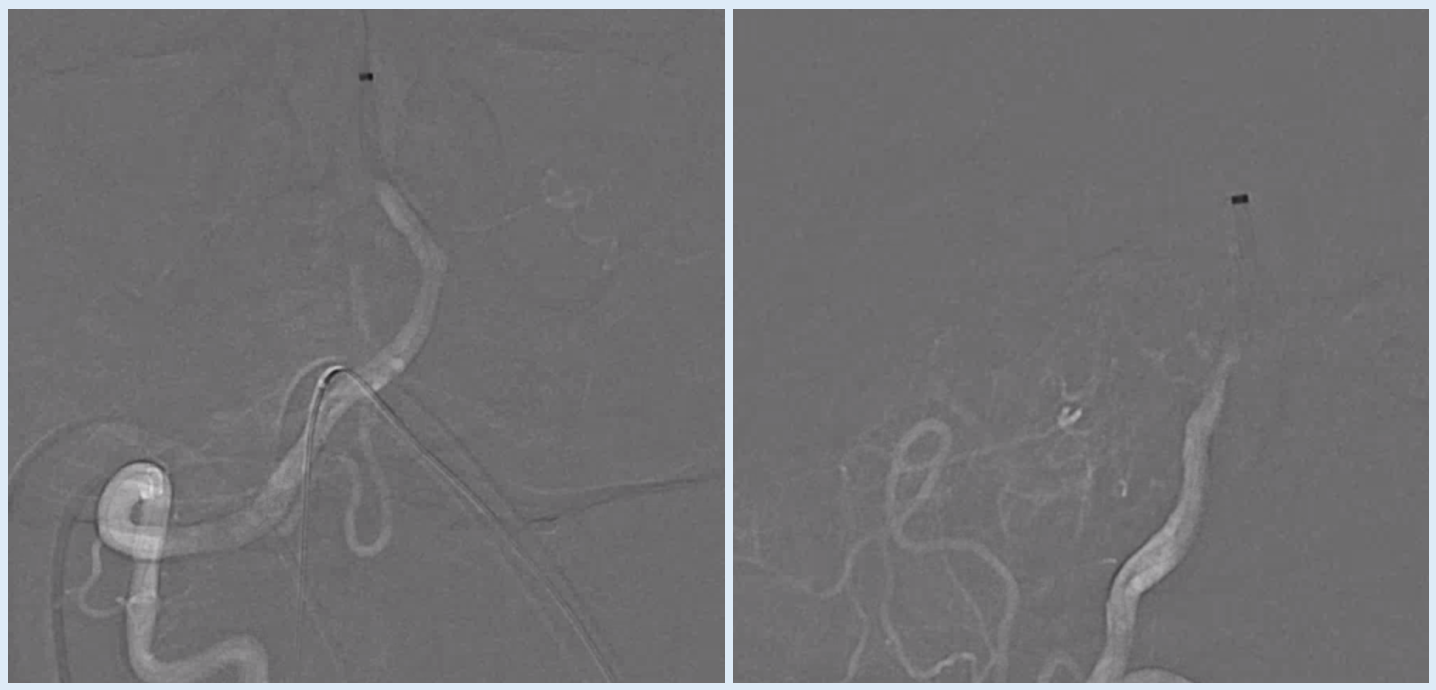
TICI 3
Look closely — notice how the mid-basilar is smaller in caliber — in fact the same caliber as the 6f Sofia (white arrows). This is what we call aspiration angioplasty — some plaque has been sucked up into the Sofia to create this tunnel. Hard to totally prove this is what happens but we think it does.
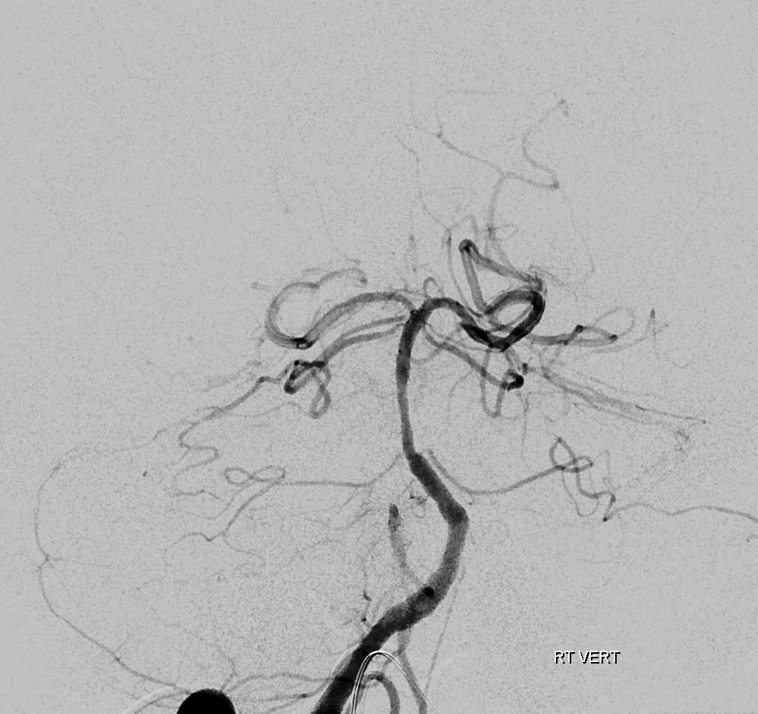
There are bilateral duplicated SCAs, with a tight stenosis of the right upper one (black arrowhead). Again seen is AICA ostium origin stenosis (black arrow)

When two AICAs are present, the lower one always goes to the hemisphere, and the upper one is the vermian one — also supplying top of midbrain, and often parts of quadrigeminal plate. It is typically much more eloquent than the lower SCAs. Normally, SCAs bifurcate into hemispheric and vermian branches anyway. The length of the SCA trunk before bifurcation varies — when there is no trunk at all, the two branches arise separately from the basilar. See SCA page for more info
All is well. Motor function is improving. Later same day, there is new diplopia and mental status decline. The astute Dr. Rostanski team calls another stroke code.
CTA shows basilar still patient. What’s up?
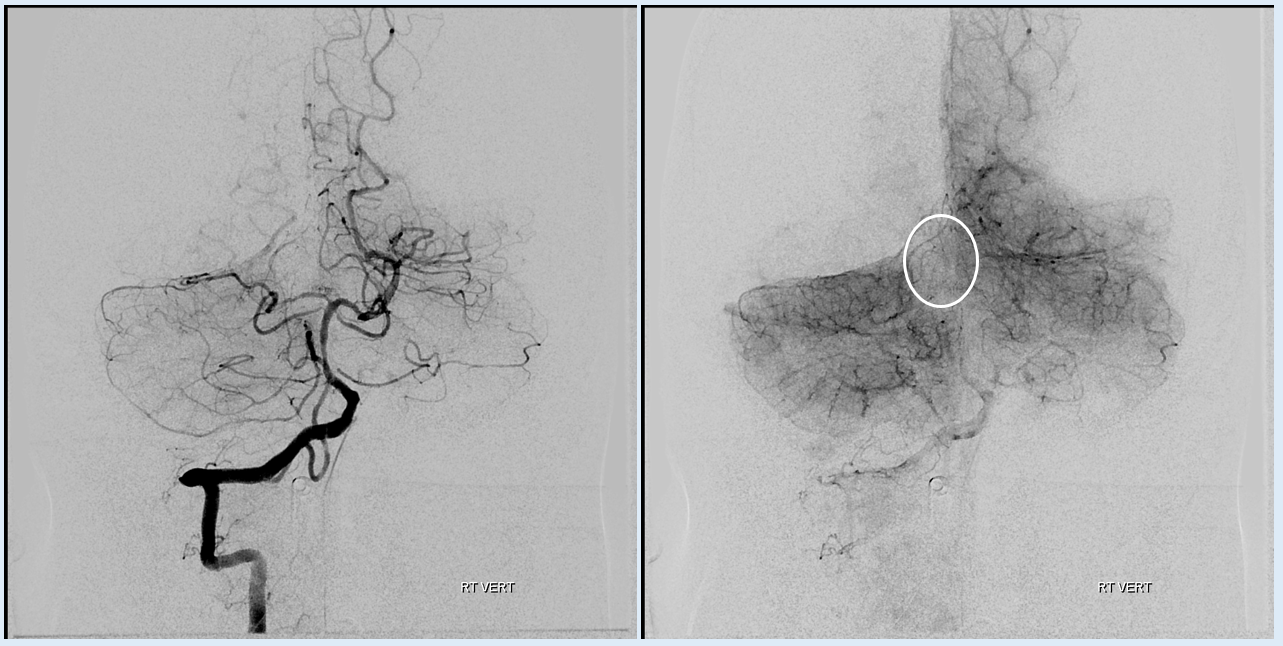
Look at the angio below carefully.
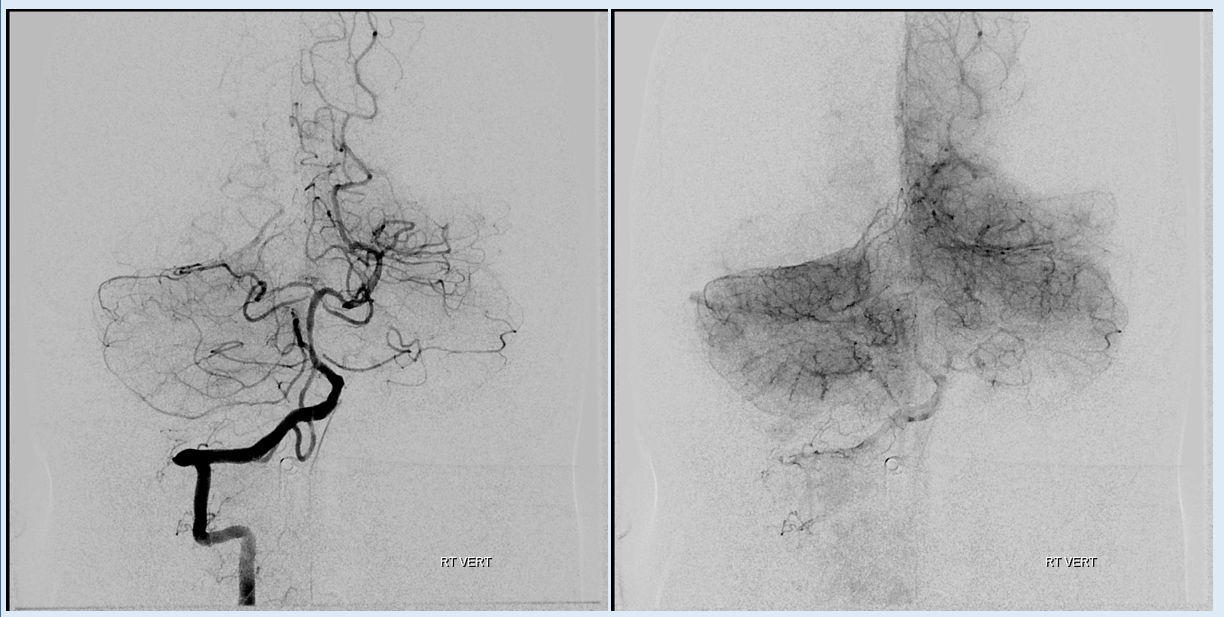
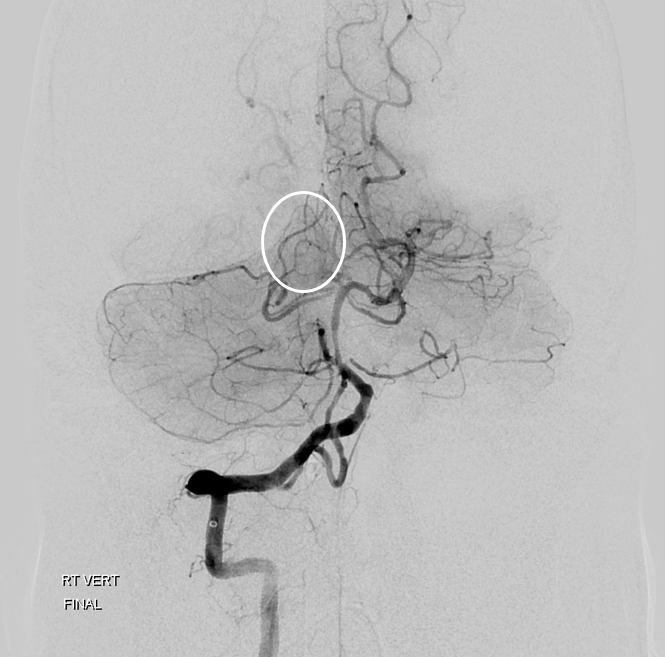
The upper right SCA (vermian branch is missing). There is corresponding hypodensity in the right midbrain (white oval)
New on left, old on right
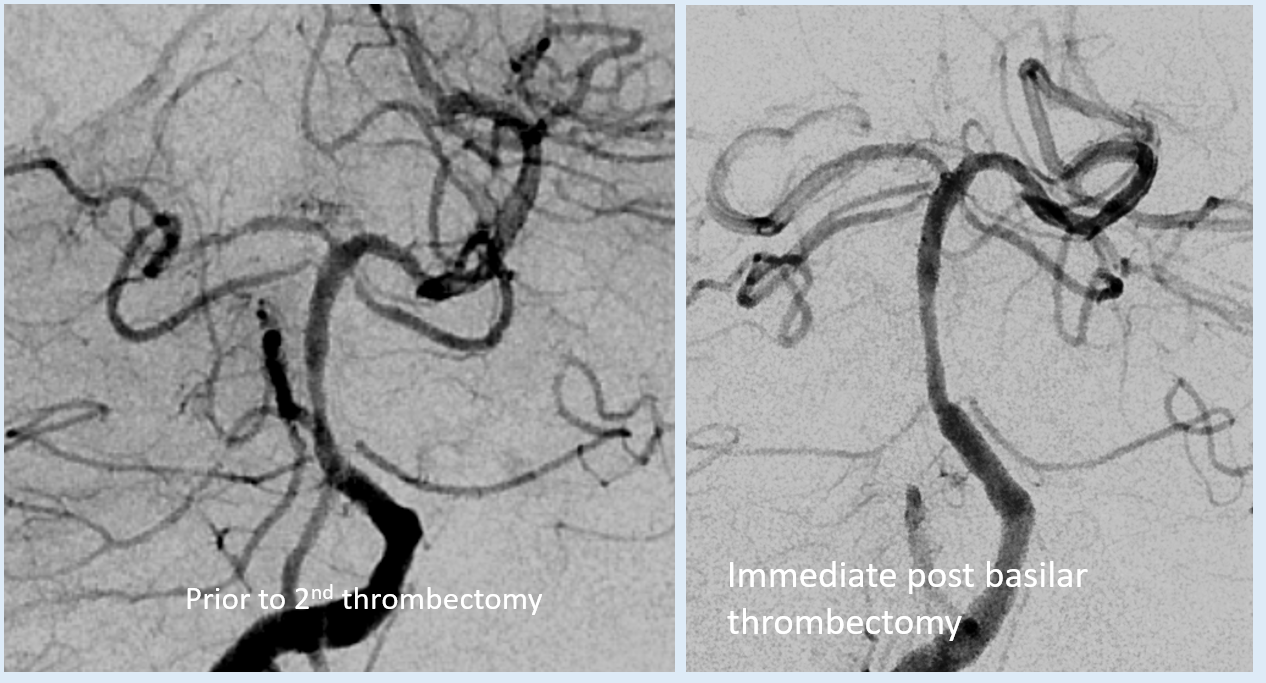
comparable angles. notice also how the mid-basilar is a bit more irregular — atheromatous disease.
Why did the SCA go down? Snow plow effect? Probably the most likely reason
What are the options? IA lytics seem unlikely to work. Vessel too small for aspiration, even with an 027 catheter (see cases of that under the stroke section here). Too small for balloon angioplasty.
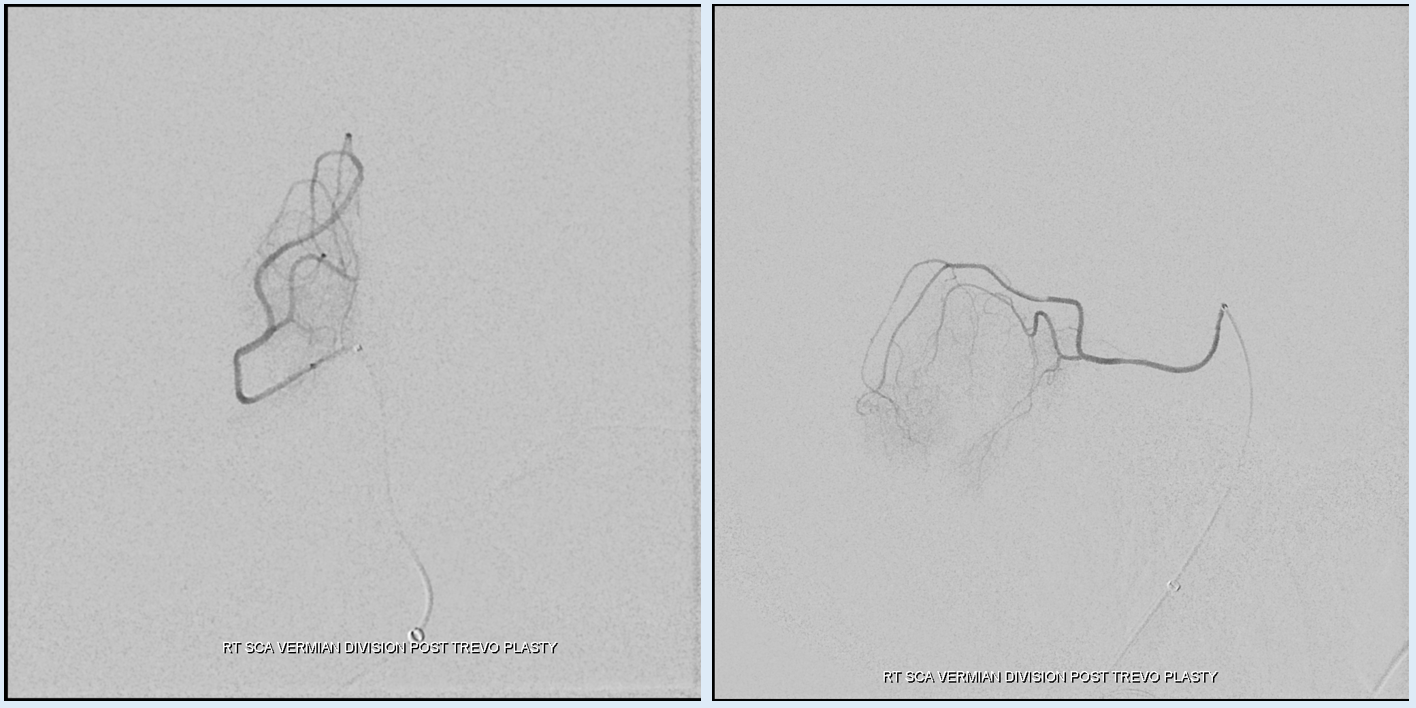
Our strategy is Trevo plasty — open a baby trevo across the stenosis, then re-sheath (do not pull — too stiff, angle may dissect SCA) and see

 Stenosis at ostium
Stenosis at ostium

Post – resheathing beautiful image of vermian division SCA
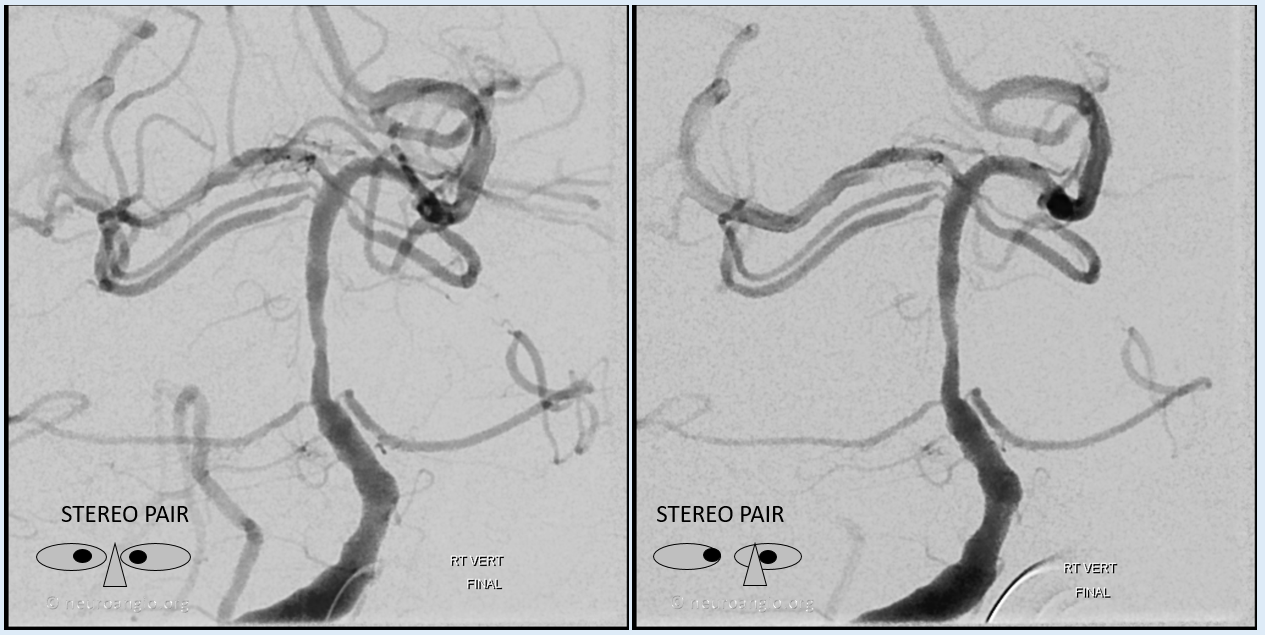
Post stereo pair
Global post. Notice restoration of normal blush
Interesting, huh? Better than watching another M1 TICI3, agree?