
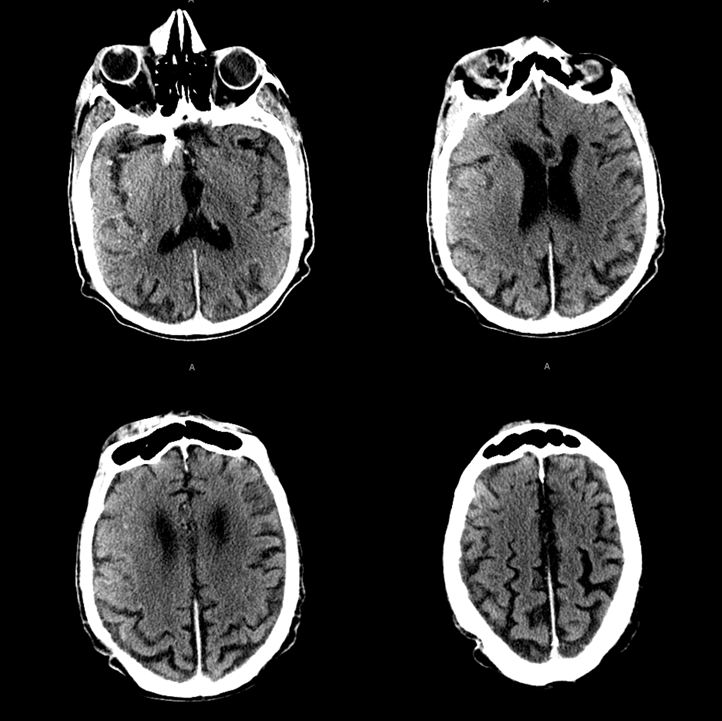
A nanogenerian presented with first time known seizure leading to status epilepticus. This CT was obtained
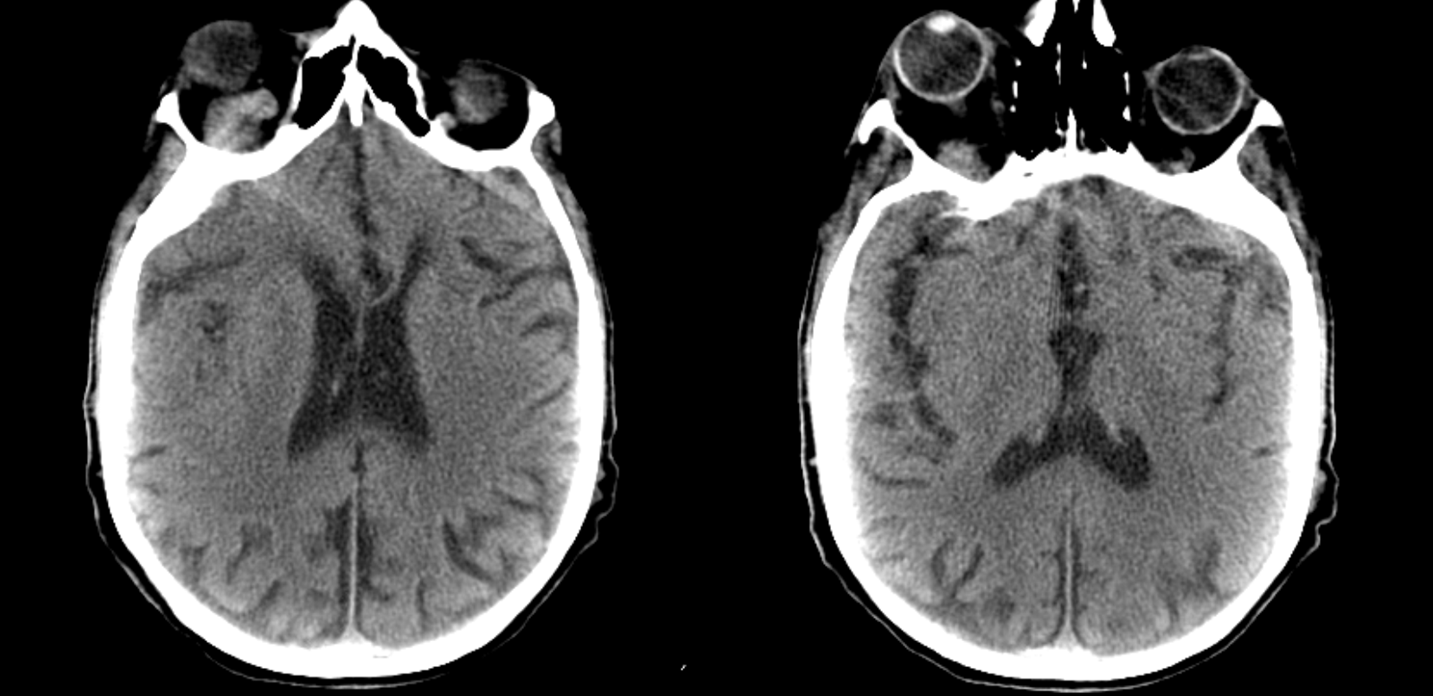
There is tremendous right proptosis and enlargement of the superior ophthalmic vein strongly suggestive of a right-sided carotid cavernous fistula. It was not known for how long he has had right proptosis / chemosis
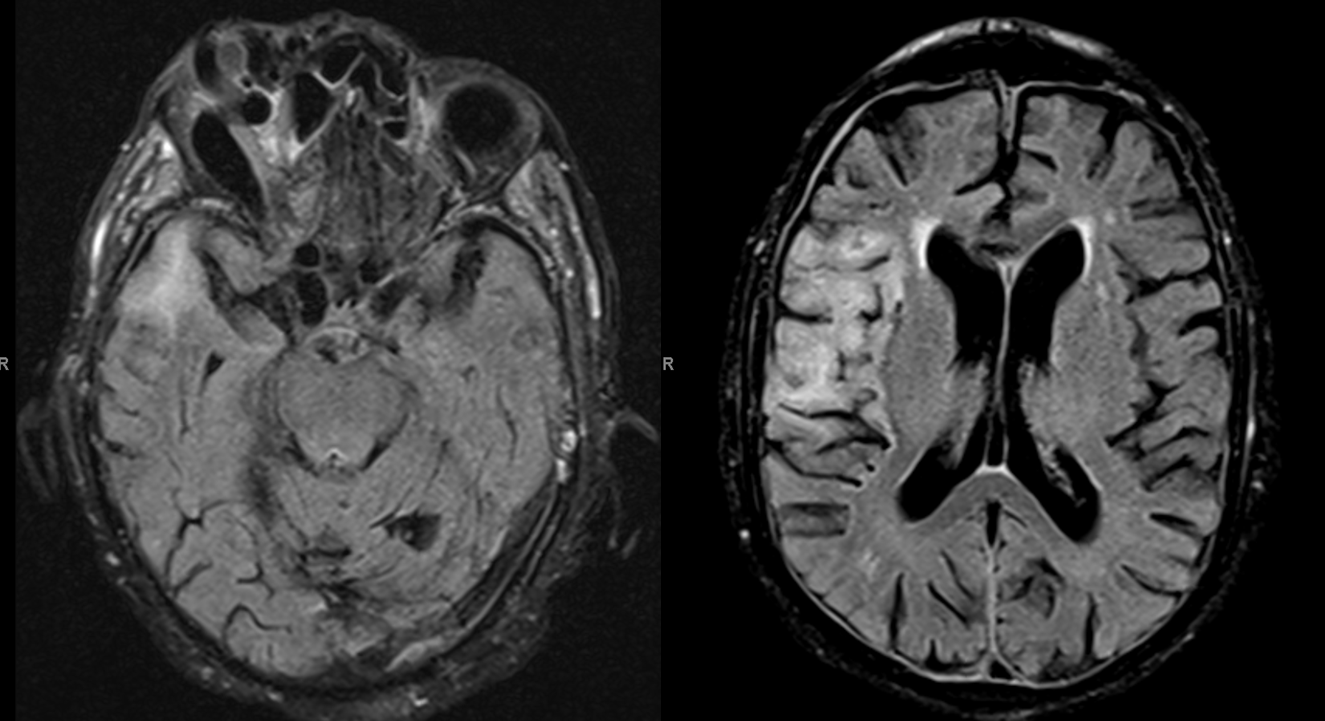
MRI came next. Notice FLAIR hyperintensity ni right temporal lobe
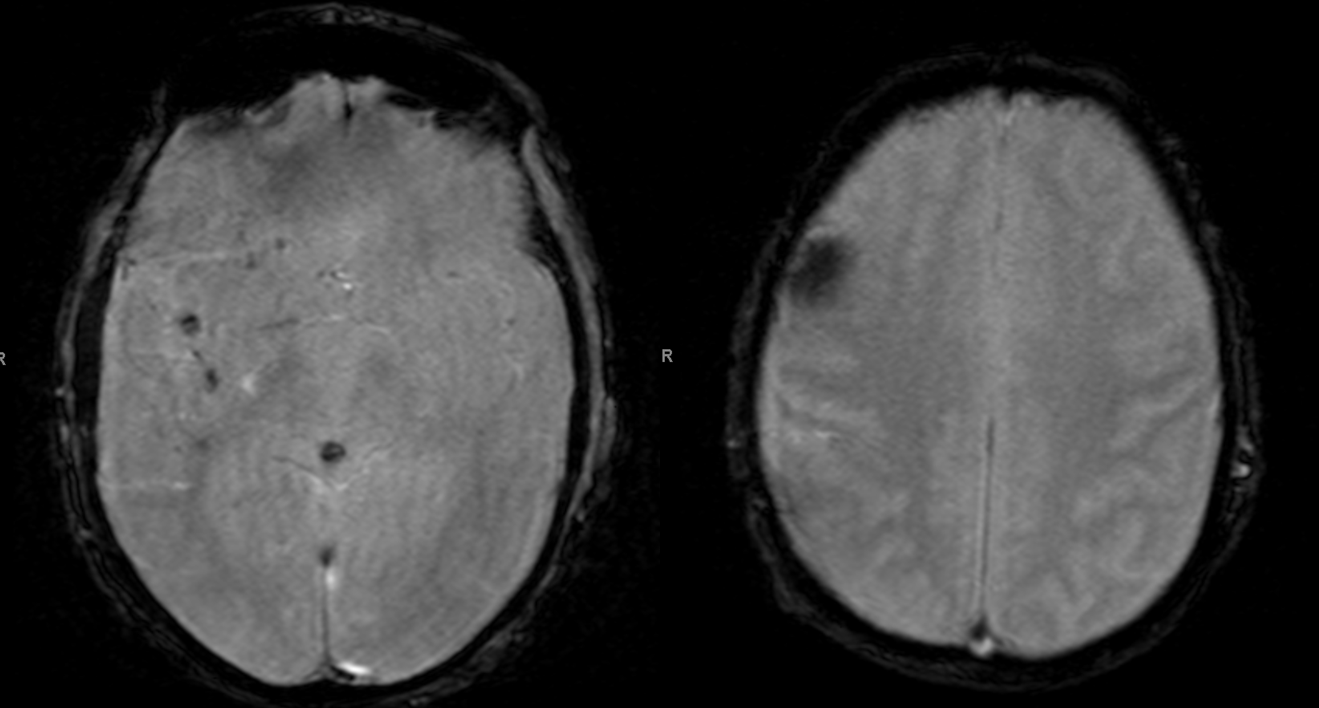
Scattered susceptibility areas, given suspected fistula-related venous congestion involving the sylvian veins
A characteristic venous congestion pattern on postcontrast T1

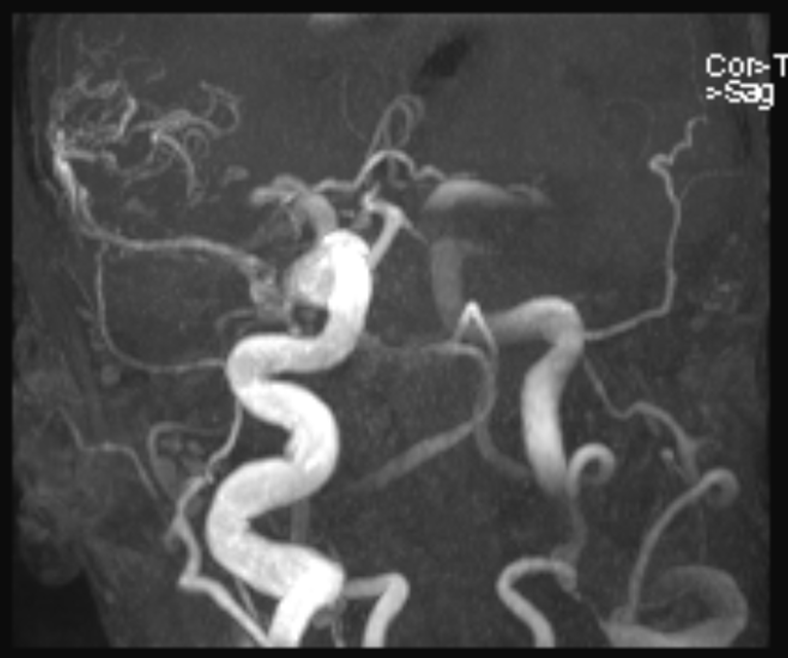
MRA shows an absolutely astounding size of the right ICA, related to extremely large size and long chronicity of fistula
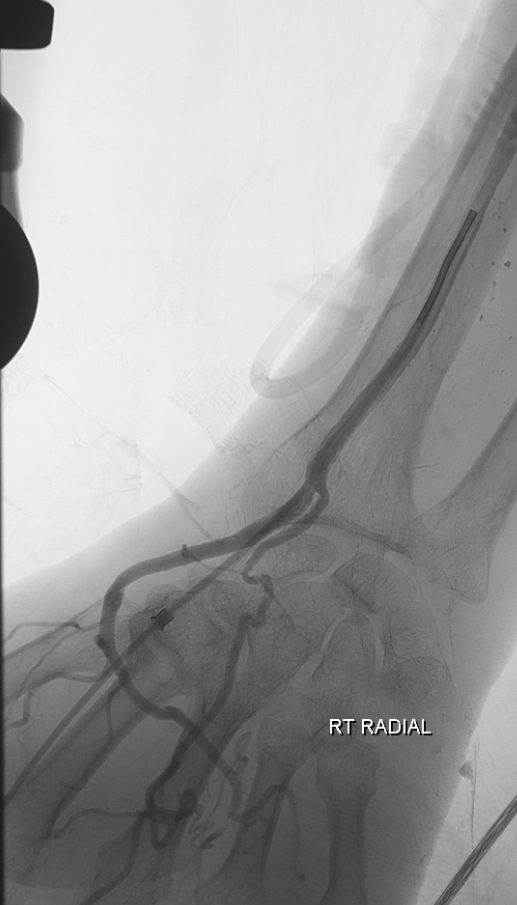
An emergency angiogram and embolization were requested. Because of suspected arch difficulty i this 90+ year old man, right radial access approach was chosen. This was also not very straightforward due to brachial artery tortuosity which was relatively easily straightened with an 035 Terumo glidewire and subsequent passage of a 5F VER catheter without an issue. This is why we prefer to visualize the arm fluoroscopically instead of blindly advancing a baby J or another wire. Just our preference
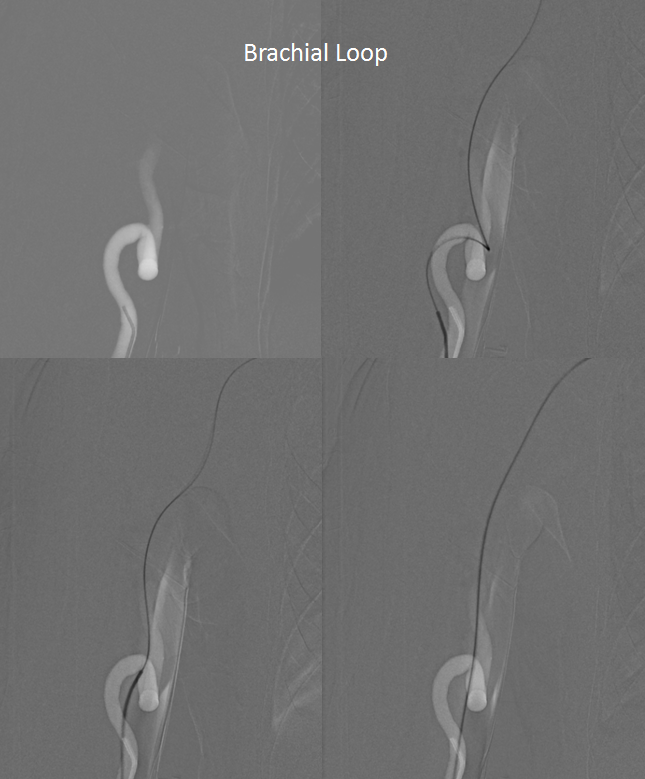
The subclavian looks impressive. There will be another loop at the right CCA origin, as you can see inferiorely

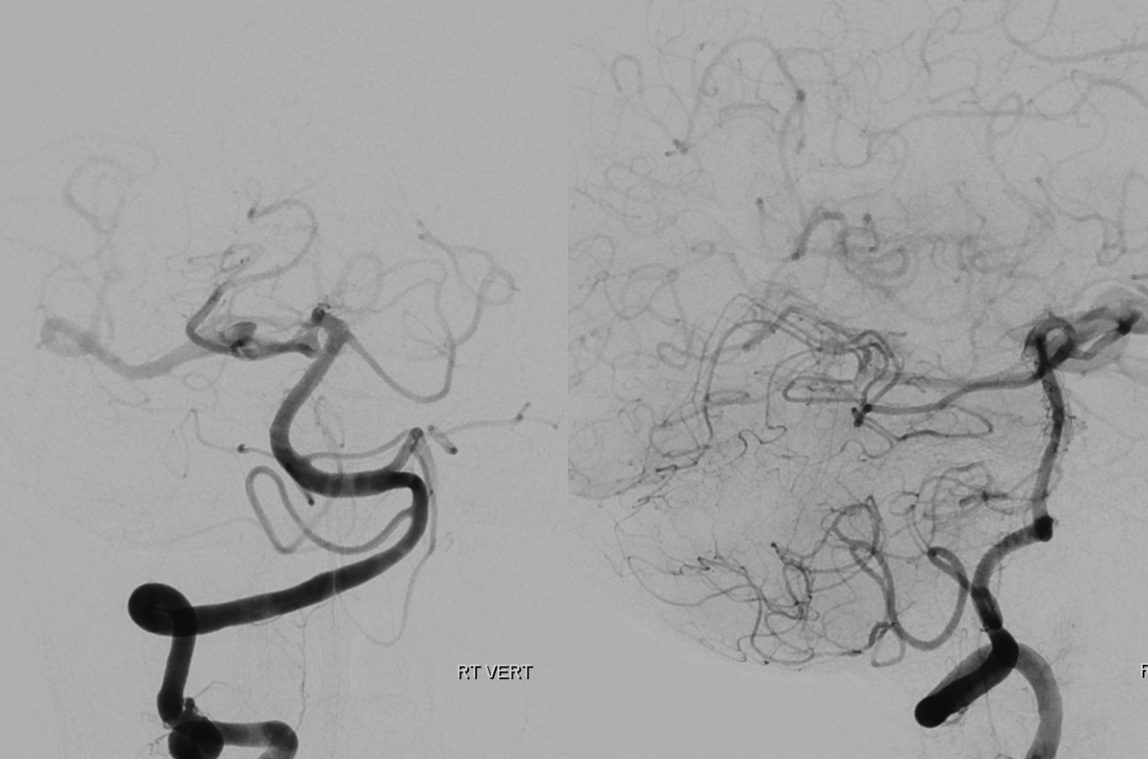
The vert shows retrograde supply of the right ICA via the PCOM
That was the arch. We were very glad to have gone radial
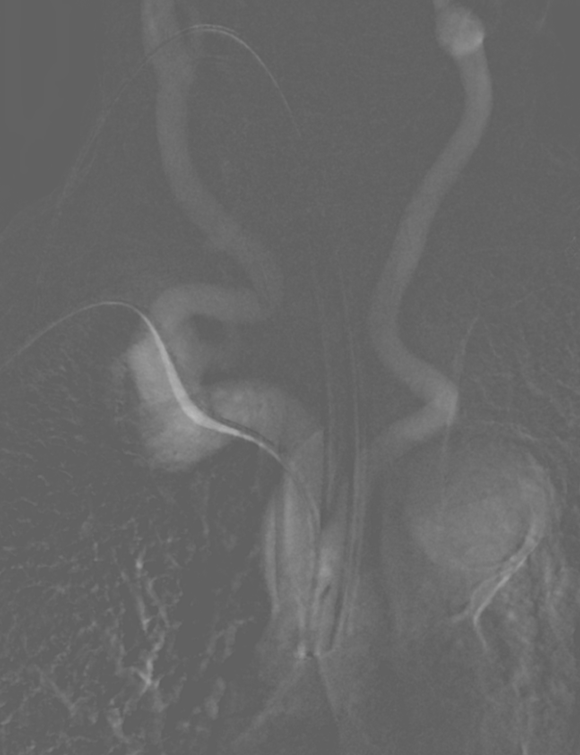
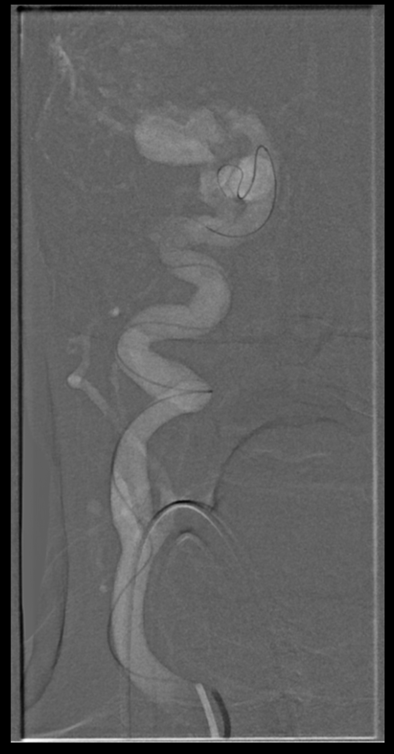
Look at the tremendous curve of the 5F vert has to take to get into the proximal right CCA.

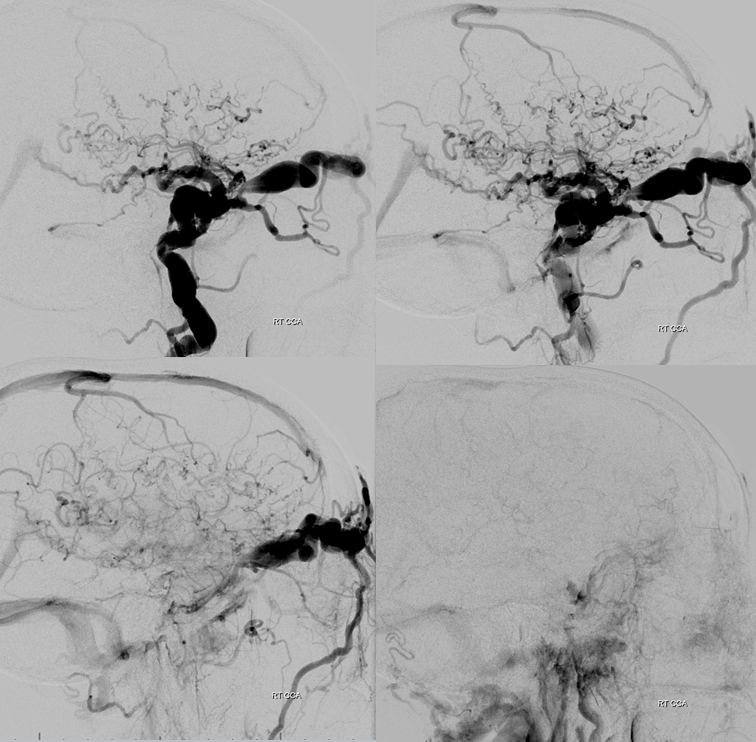
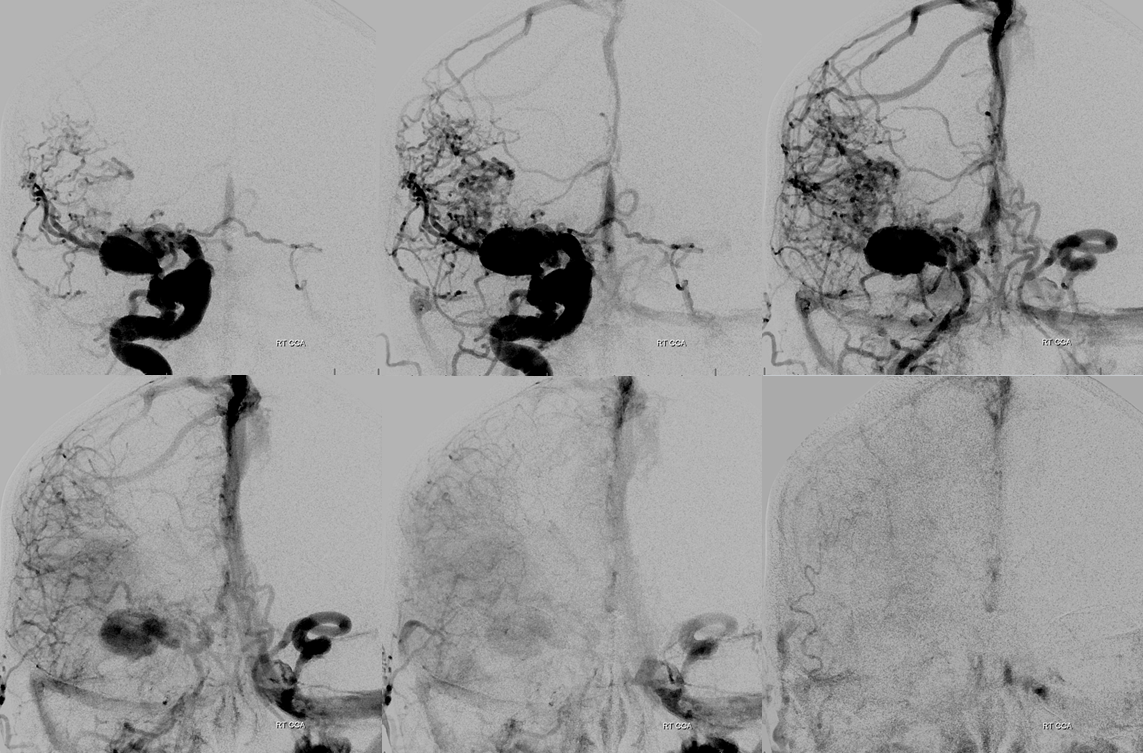
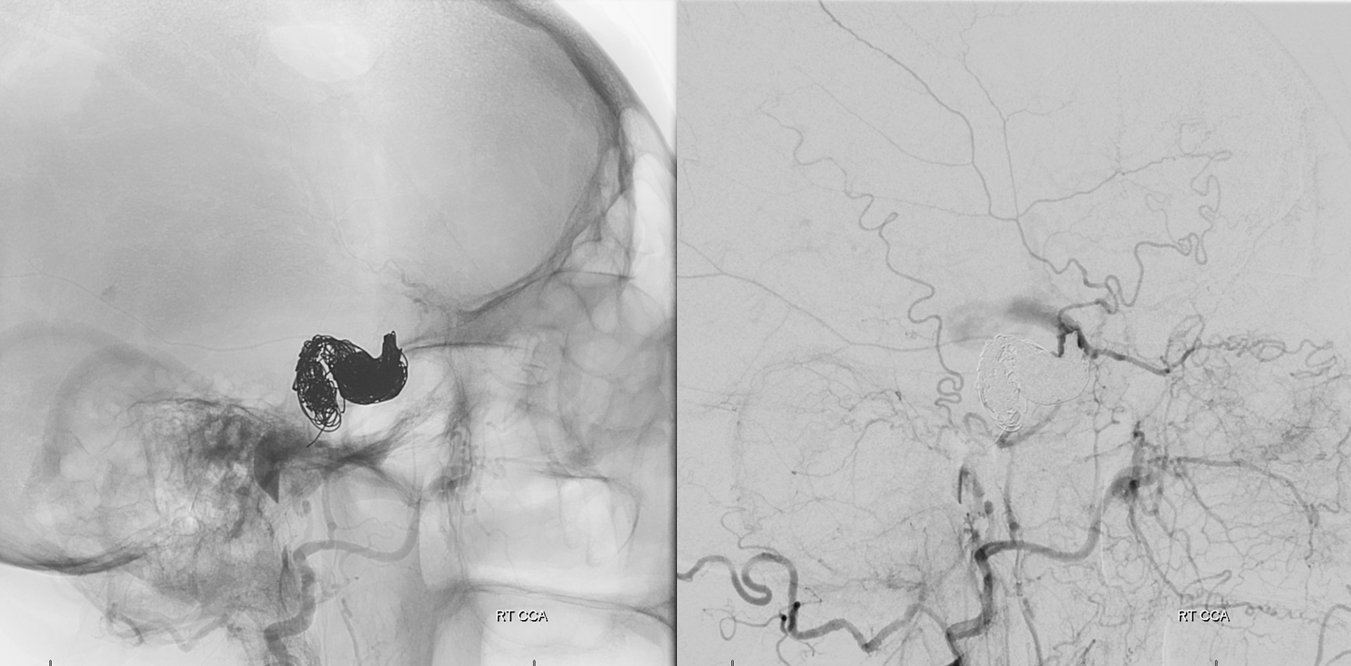
Right CCA injection shows a giant direct CC fistula. Aside from extensive superior and inferior ophthalmic vein engorgement (ocular pressure = 35) there is marked retrograde congestion of superficial sylvian and deep sylvian veins. The superficial congestion extends to the frontal operculum and basal vein as well as superior sagittal sinus are both visible as well. Venous phase image of brain (bottom right) shows extent of venous congestion.
Frontal views better show involvement of the left ophthalmic vein without ocular pressure elevation
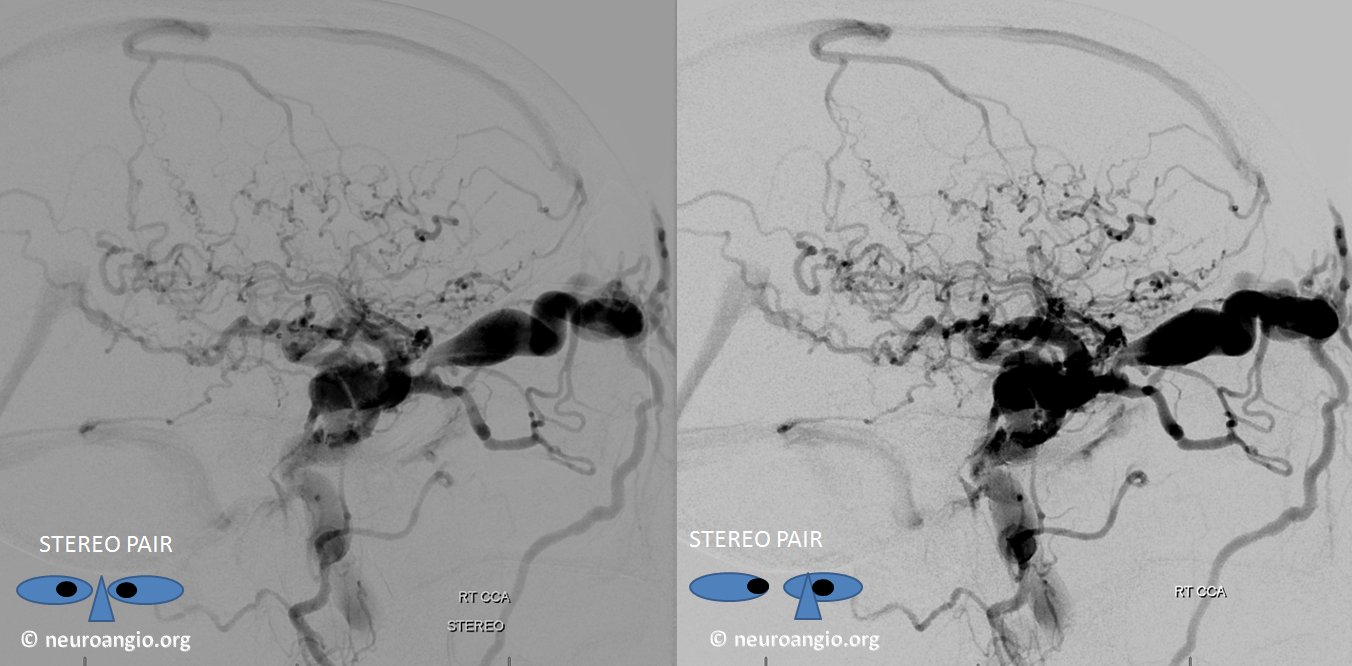
Stereo Views are particularly good for understanding cavernous sinus outflow and for venous drainage in general. Highly recommended.
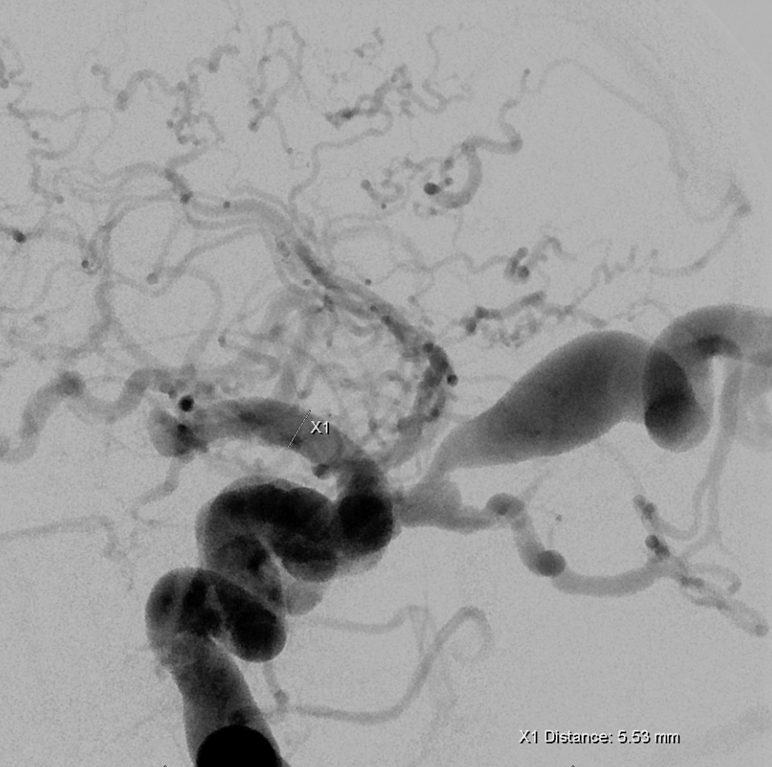
A better understanding of the fistula site. There is a pouch at the horizontal cavernous segment projecting inferiorly which likely represents a ruptured cavernous aneurysm with secondary fistula formation.
There are many ways to lose this kind of fistula The idea here is to close the carotid artery at the level of the fistula. The key is to prevent retrograde flow into the fistula and therefore to achieve a distal enough position with the catheter before using whatever it is u want to use to close this vessel. We typically prefer pushable firbercoils at some stage of occlusion due to their high efficacy and low cost. However due to access limitations we were only able to advance the guide (5F vert in this case was the best choice) we could only achieve distal enough position with an SL-10, necessitating use of detachable platinum coils.
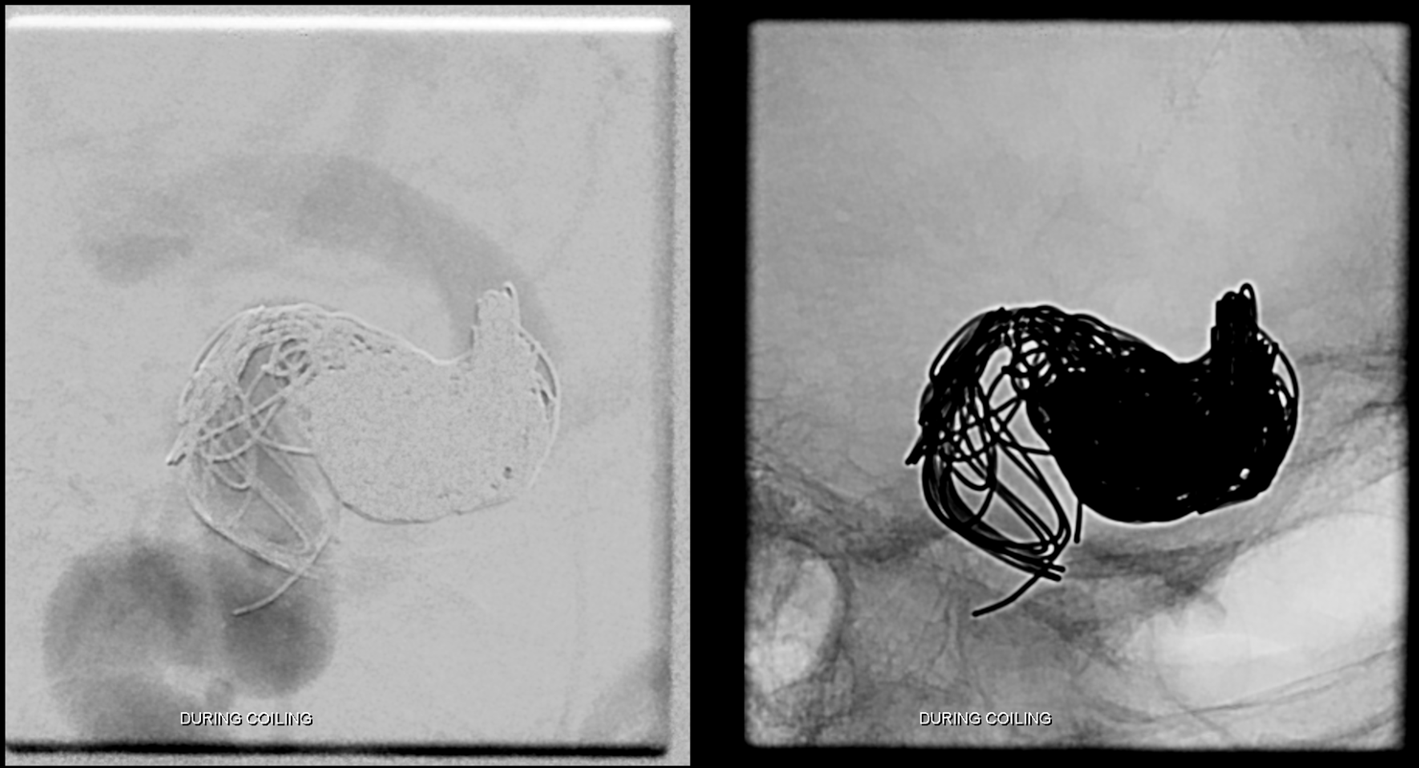
Distal position angiogram before occlusion

During coiling, There is filling of the anterior cavernous genu and cavernous sinus proper, with early filling of the proximal cavernous ICA. It takes a lot of bare platinum coils to close these, at very high expense, which is why we almost never do this, except in cases like this. Pushable fibercoils and even Amplatzer plug when u can get it up there are much more effective, much cheaper, and safe given experience.
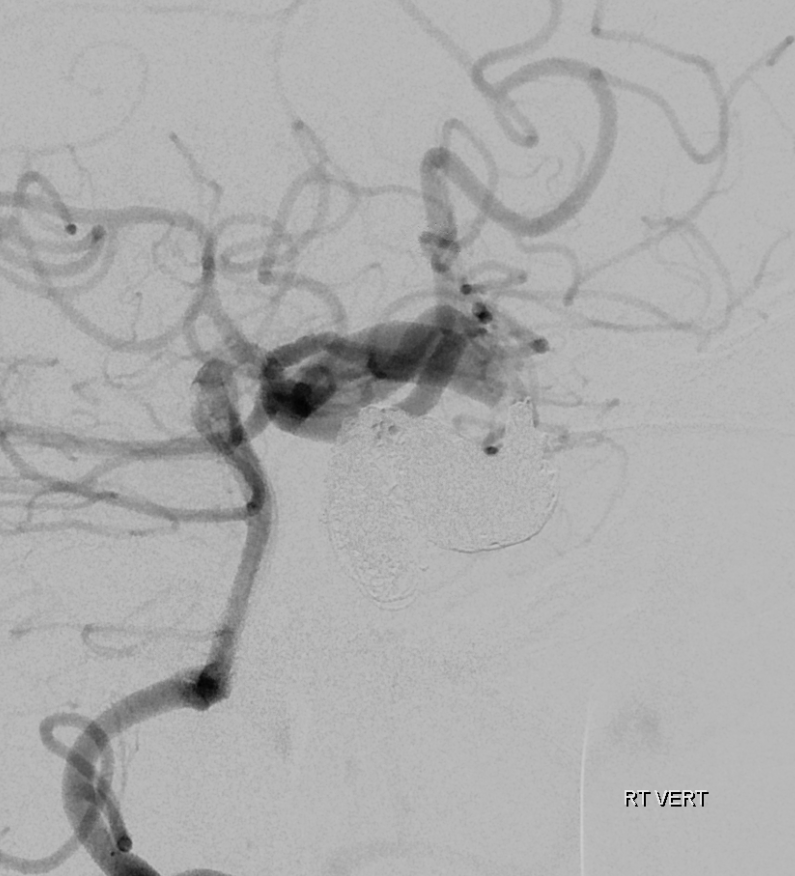
Post occlusion, external ophthalmic artery show retrograde ICA reconstitution distal to the fistula with no retrograde flow into the fistula, confirming its complete occlusion.
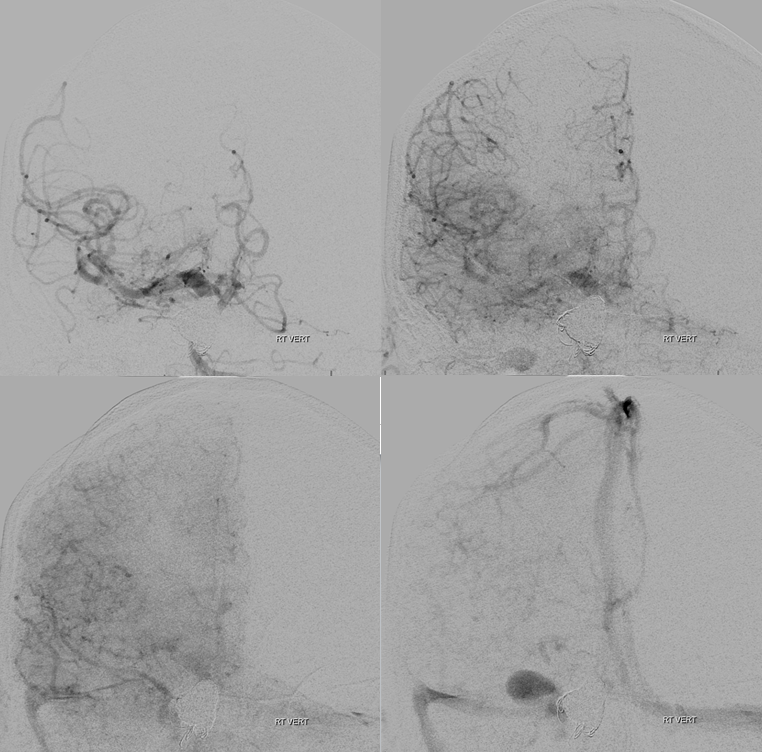
Right vert injection demonstrating PCOM support of right ICA territory
Frontal views of right vert injections
Radial sheath injection following embolization. There is antegrade flow in the patient’s large radial artery.
CT scan post treatment
From the technical perspective another option would have been direct carotid puncture, especially as the artery would have been sacrificed anyway.
Unfortunately the patient did badly due to issues related to status epilepticus. The status was precipitated by venous congestion of the temporal lobe. So, in the end, this is a technically instructive but disappointing case.
Other pages