
Beyond the M1 “bread and butter” cases, there is a good variety of excellent and more unusual scenarios that are very instructive and helpful to the patient as well.
This woman presented with diplopia and decreased level of consciousness. Irregular heart rate was noted, previously unknown. IV t-PA was given. Noncontrast head CT is normal
CT perfusion maps are beautiful, showing penumbral pattern in the ventral midbrain and bilateral thalami

CT angiogram with thrombus in the right P1

Bilateral CCA injections demonstrating patency of the PCAs, with unopacified inflow as well, demonstrating that the basilar is also antegrade

Angiogram — a partially occlusive thromboembolus in the right P1 segment — there is excellent antegrade flow distal to the lesion, and even transient reflux into the right P1. The posterior thalamic perforating branches are absent

Post 3 Max Ace thrombectomy. Notice bunny ear hyperemia arising from the now re-opened P1 Percheron perforators.

Pre-(top) and post-thrombectomy (bottom) set of images

24-hour post MRI, by which time the patient is back to full normal. Notice how diffusion is less bright in the thalami than in the superior vermian branch territory. ADC values were in low 600s.

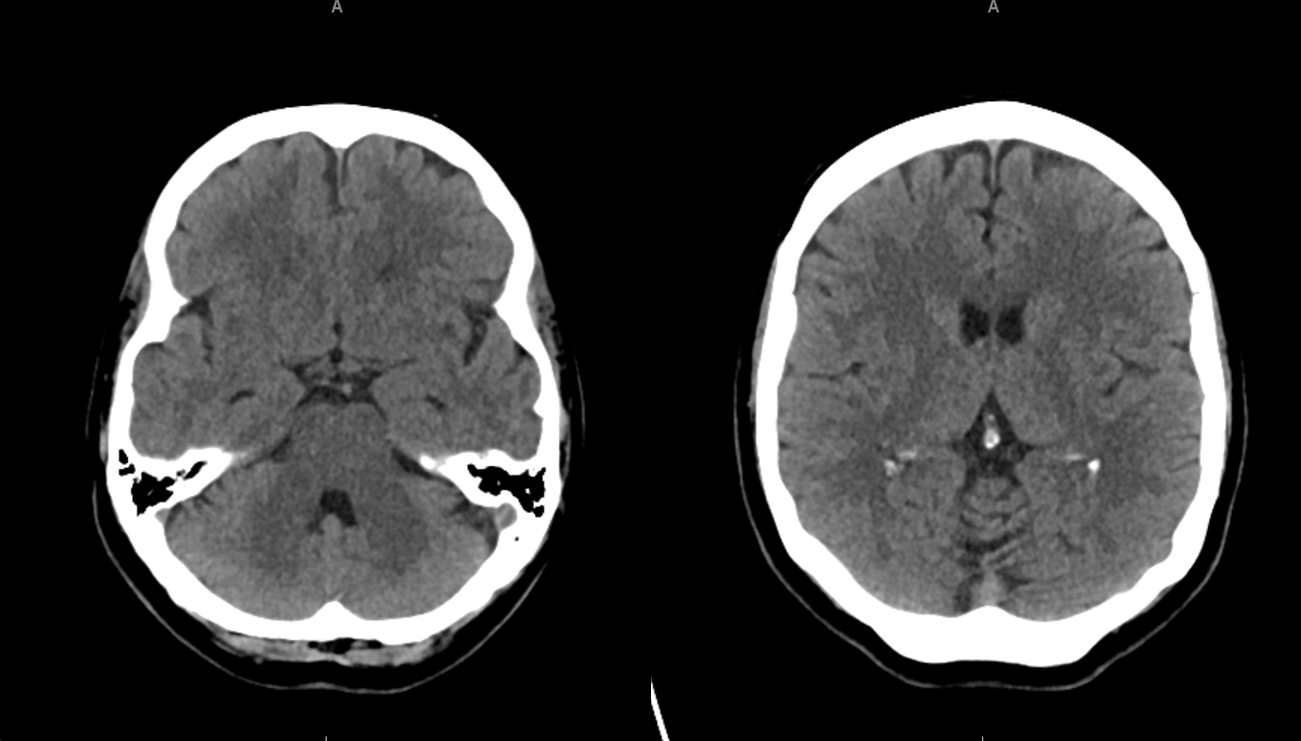
CT scan another 24 hours later

Further Reading
http://www.ajnr.org/content/31/7/1283.full
CT vs. CT Perfusion Stroke case, and classic CT Perfusion Primer
Back to Case Archives