Case Courtesy Drs. Jan Karl Burkhardt and Patrick Karas of Baylor College of Medicine
What could be more critical than a top of basilar occlusion? How about basilar and ICA?
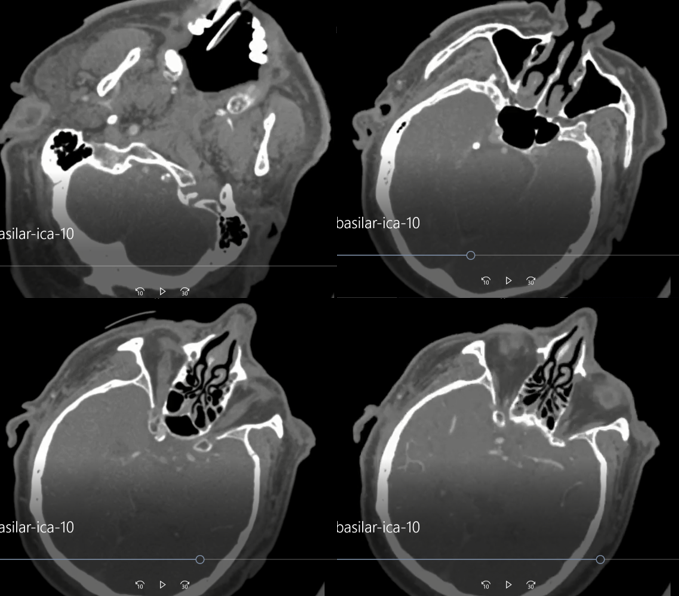
Presentation is coma with fixed and dilated left pupil. CTA is read as left carotid occlusion
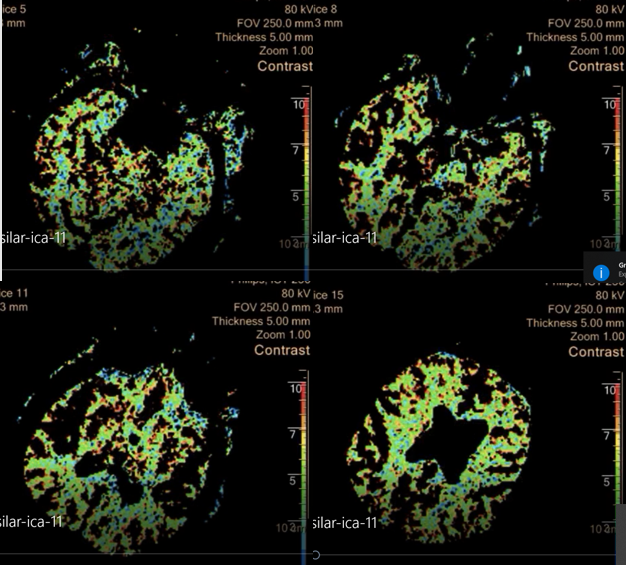
CTP CBF images show a different story. There is decreased flow in superior vermis, left midbrain, and left thalamus as well
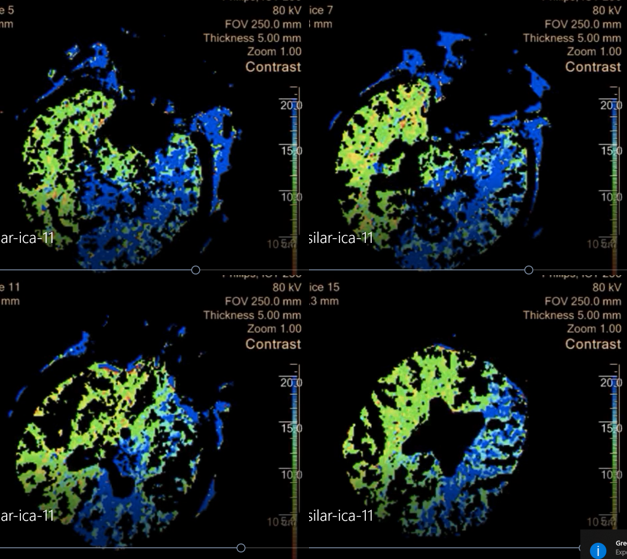
CBV is preserved
MP4 of CTA
Perfusion MP4s
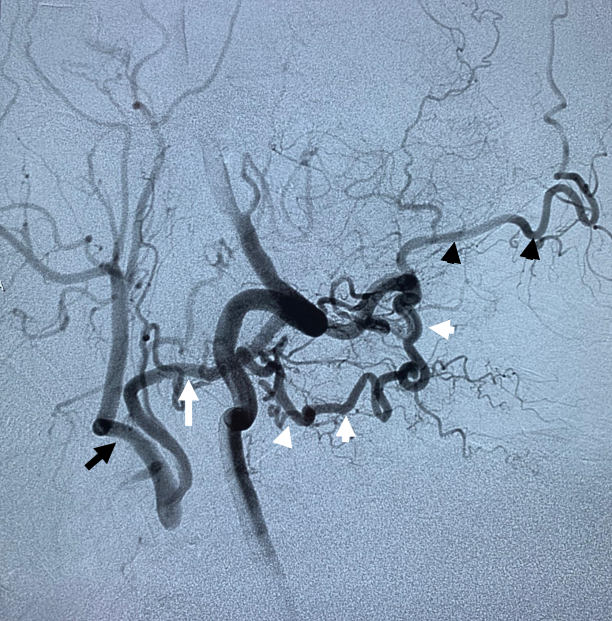
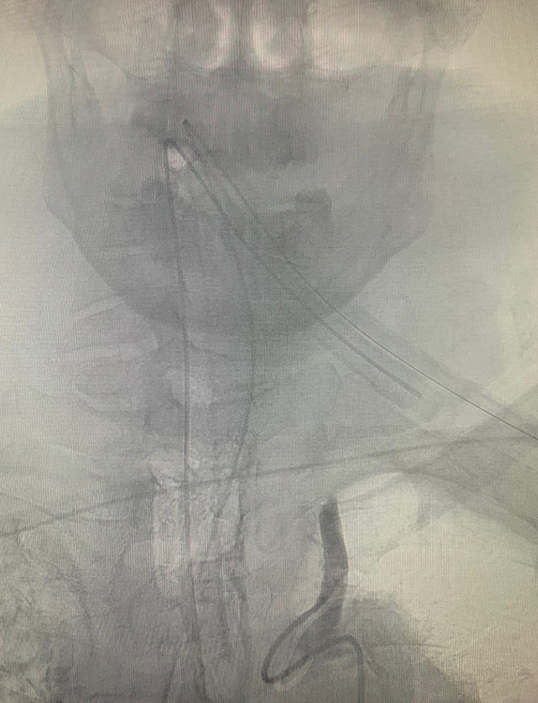
Left vert
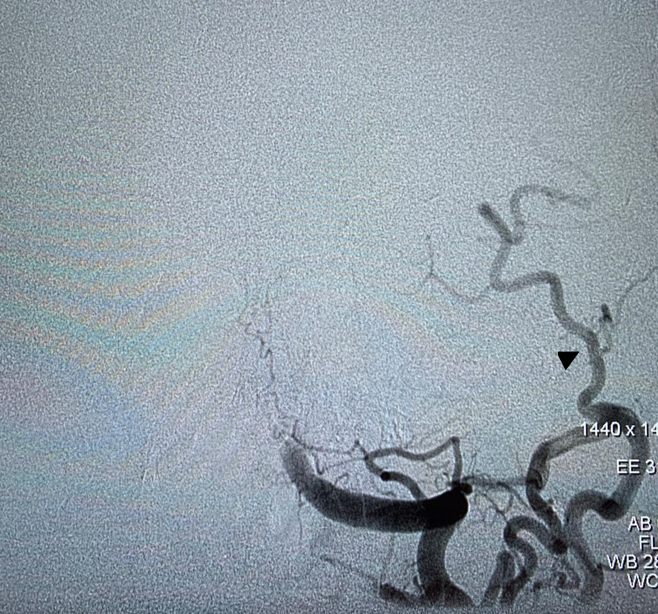
Lateral below. Notice C1 muscular branch of vert (white arrowheads) reconstituting the left external carotid artery (black arrow) via the occipital artery (proximal – white arrow, distal — black arrowheads)
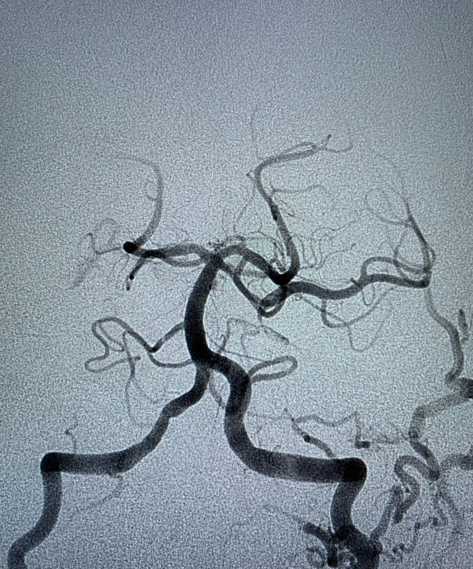
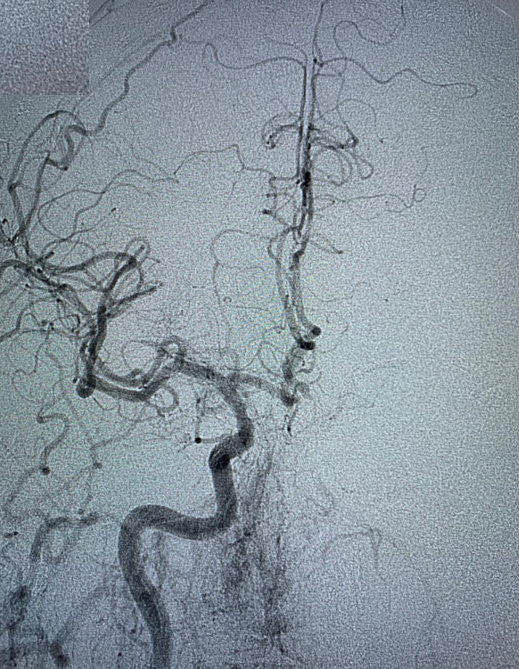
Post aspiration thrombectomy. Notice retrograde flow in left PCOM
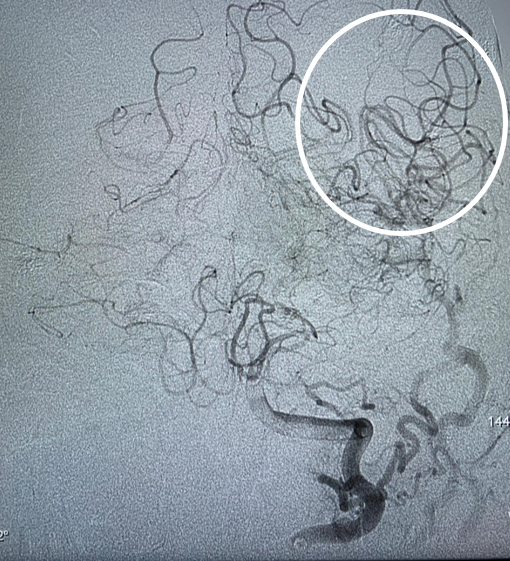
Later phase views better show supply to left MCA territory (white oval)
Lateral — PCOM supply of entire left MCA and supraclinoid ICA, including ophthalmic

How to put it together? Left CCA is chronically occluded, with left vert reconstituting left supraclinoid ICA and left MCA via PCOM. Same left vert also supplies left ECA via C1/occipital anastomosis.
Then comes top of basilar embolism, which also takes out left MCA and supraclinoid ICA. Thrombectomy restores perfusion
Left CCA image below
Right CCA
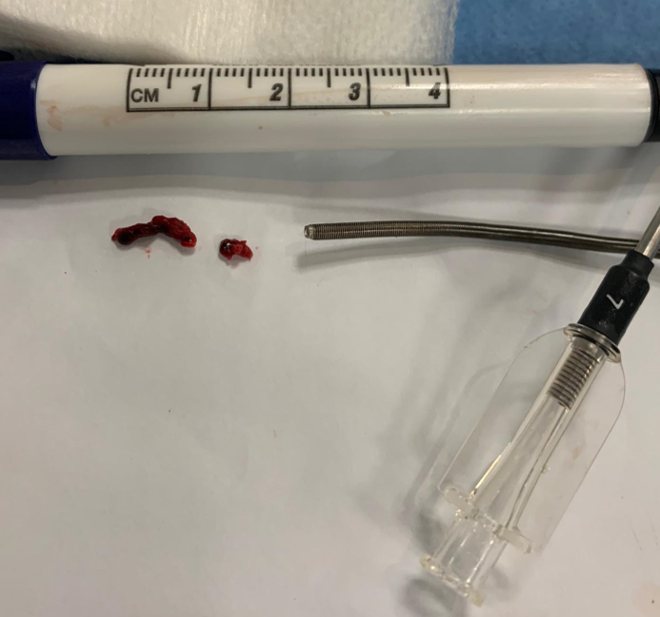
Emboli