A well known, uncommon but not “exceedingly rare” (as some literature wishfully believes) complication of LeFort Osteotomy. Either sphenopalatine or descending (also known as greater) palatine artery can be injured during surgical LeFort — as the maxilla is “broken” during surgery, the pterygoid plates or something else nearby can tear the artery. The location is deep and invisible surgically. Bleeding can be delayed and severe. For these reasons, some surgeons prefer to prophylactically embolize / close the IMAX — or specifically the greater and sphenopalatine arteries prior to a LeFort. There are tremendous collaterals to the downstream territories so closing bilateral IMAX is not a problem. Usually we do it with coils at the distal IMAX.
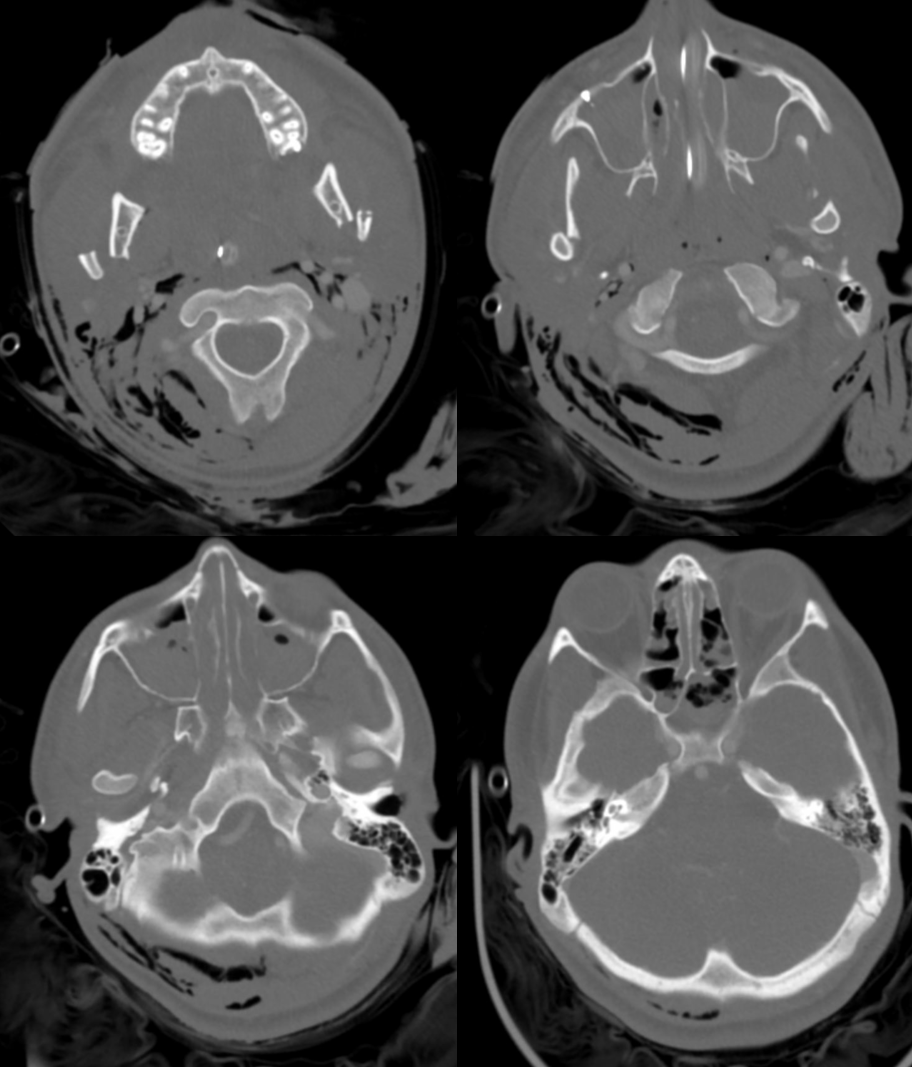
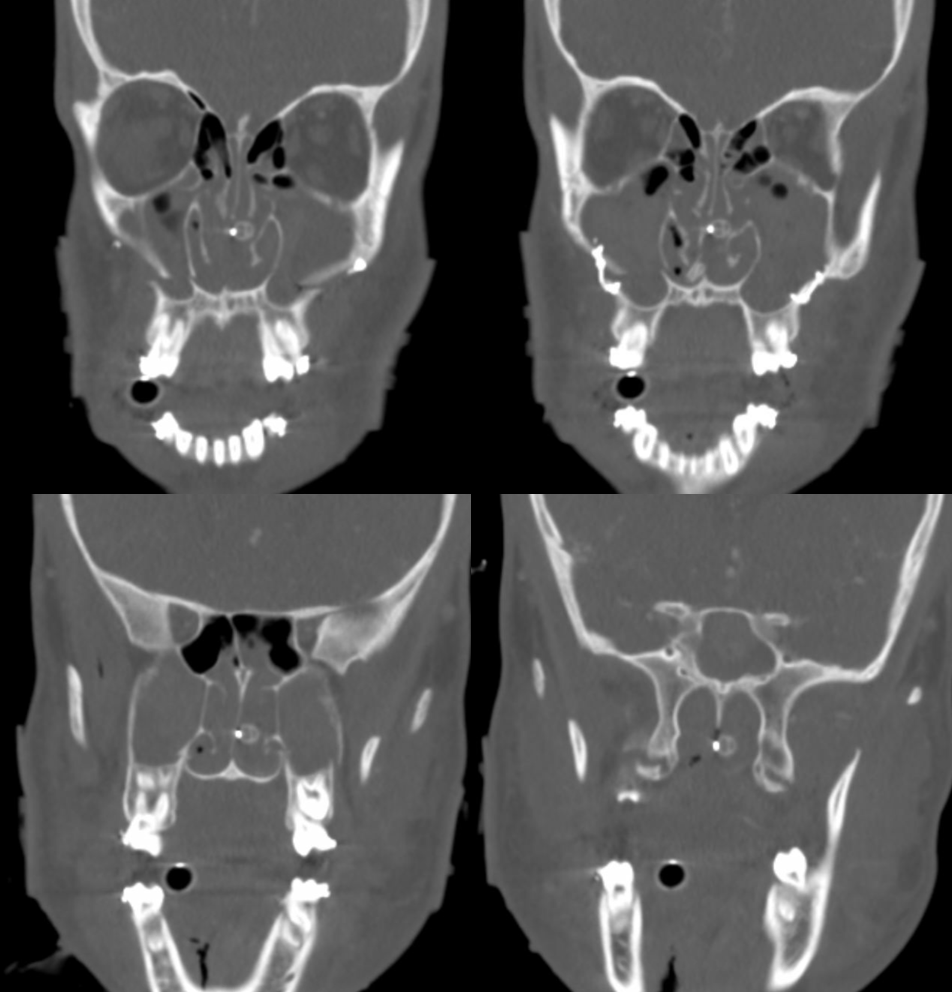
This patient presents with intermittent modest bleeding after LeFort. One week later, there is massive oral bleeding (can be either nasal or oral). A life and death situation results in an emergency tracheostomy. There is extensive air in all kinds of places air should not be…
Right side is fine, but has some good normal anatomy
con numeros — see Diagrams and Drawings
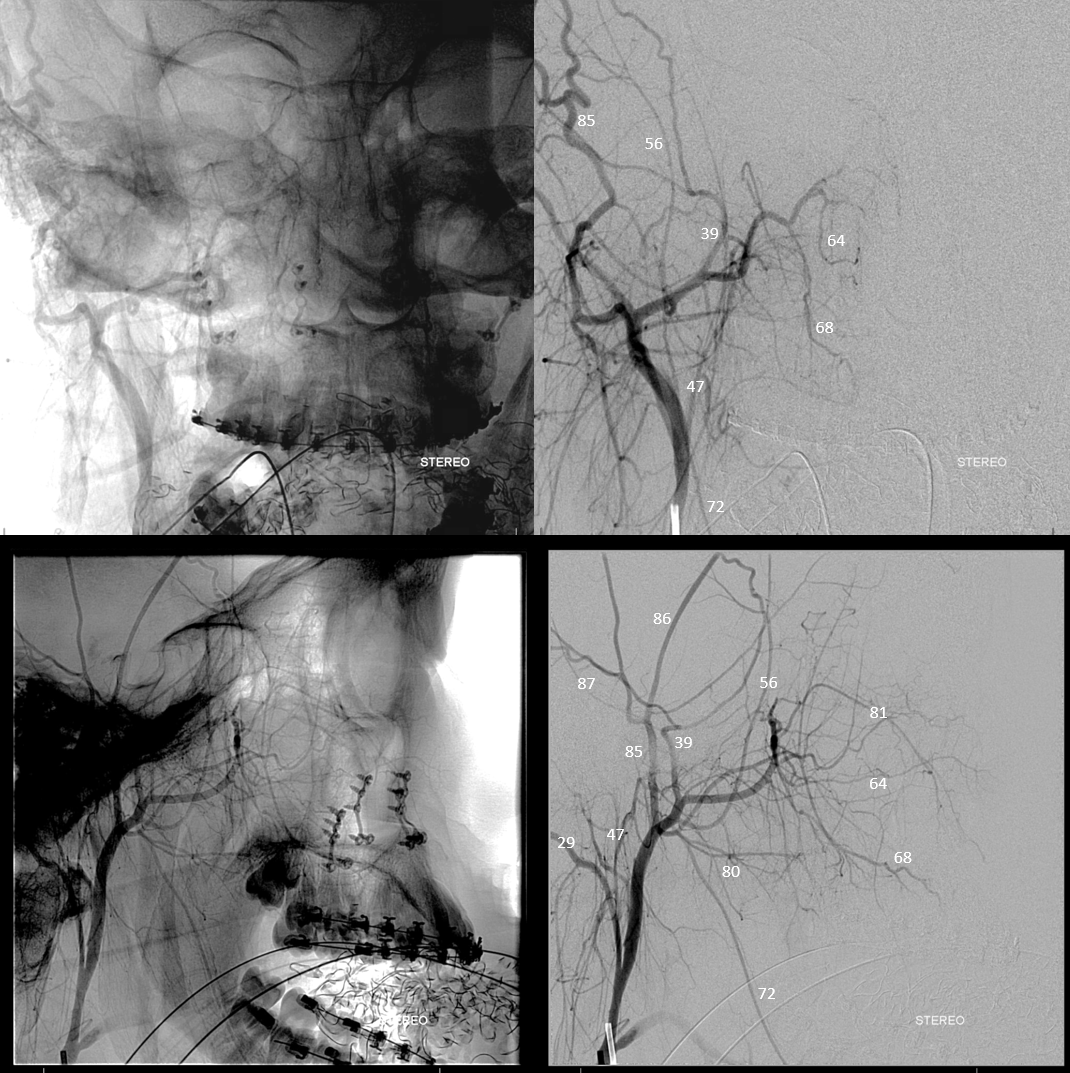
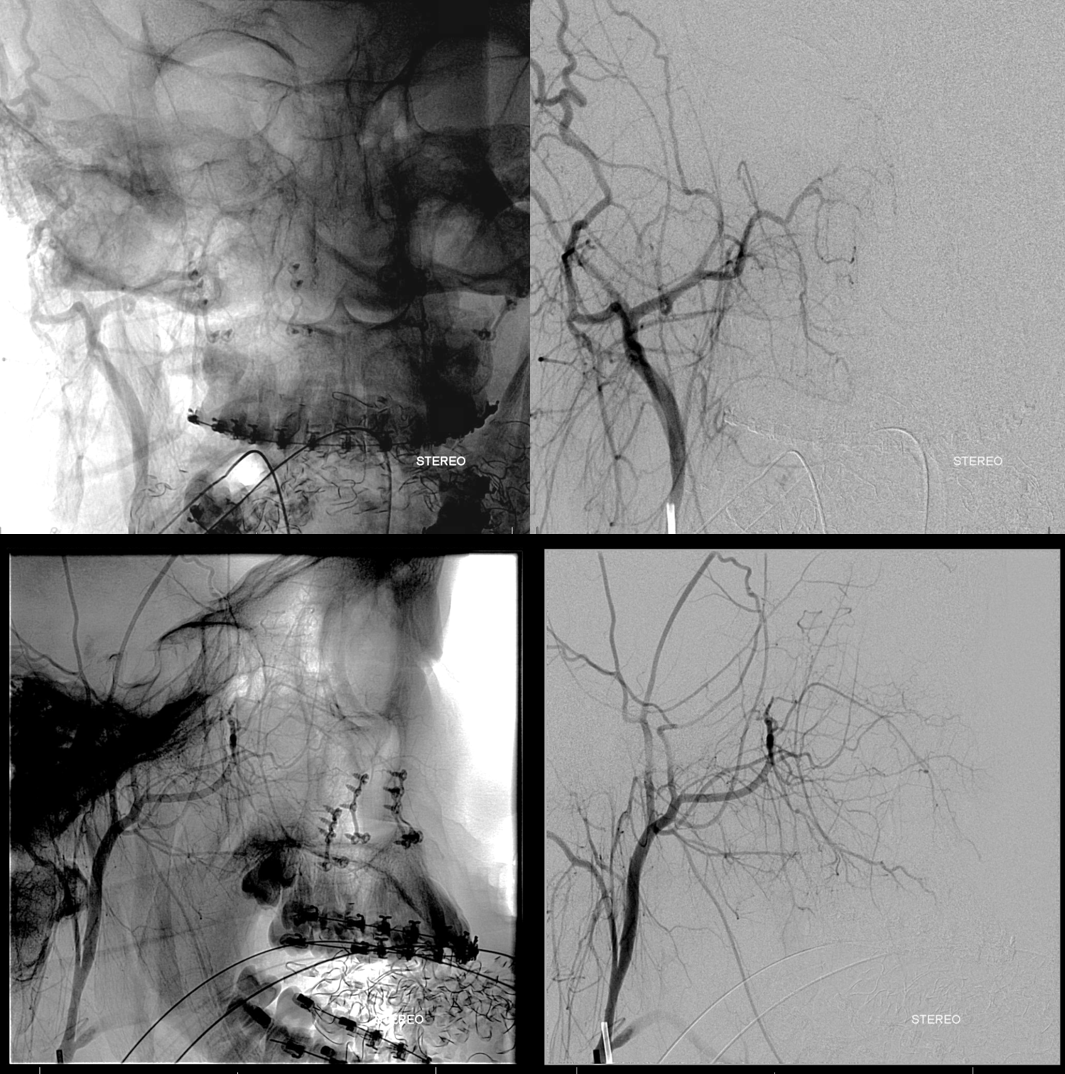
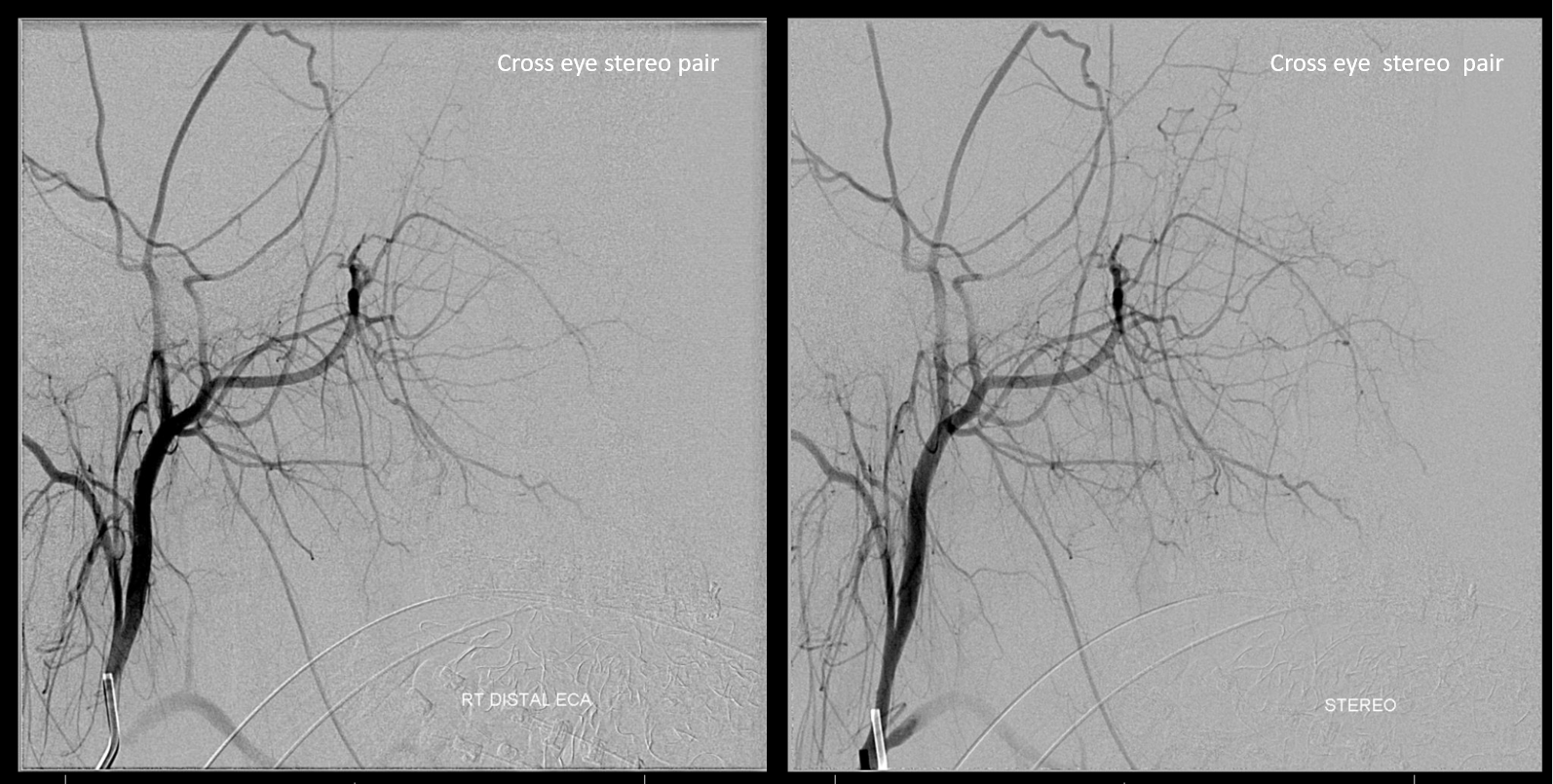
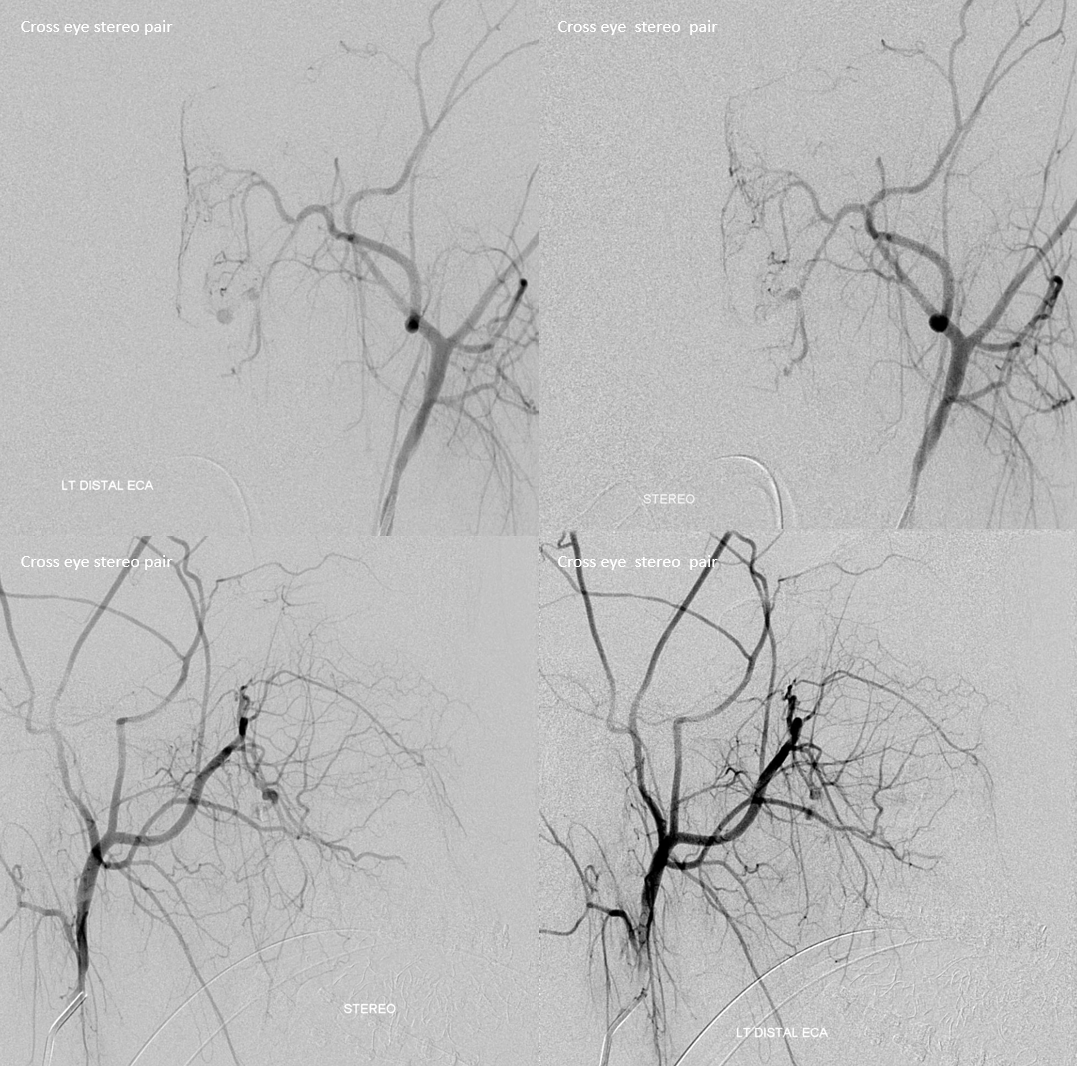
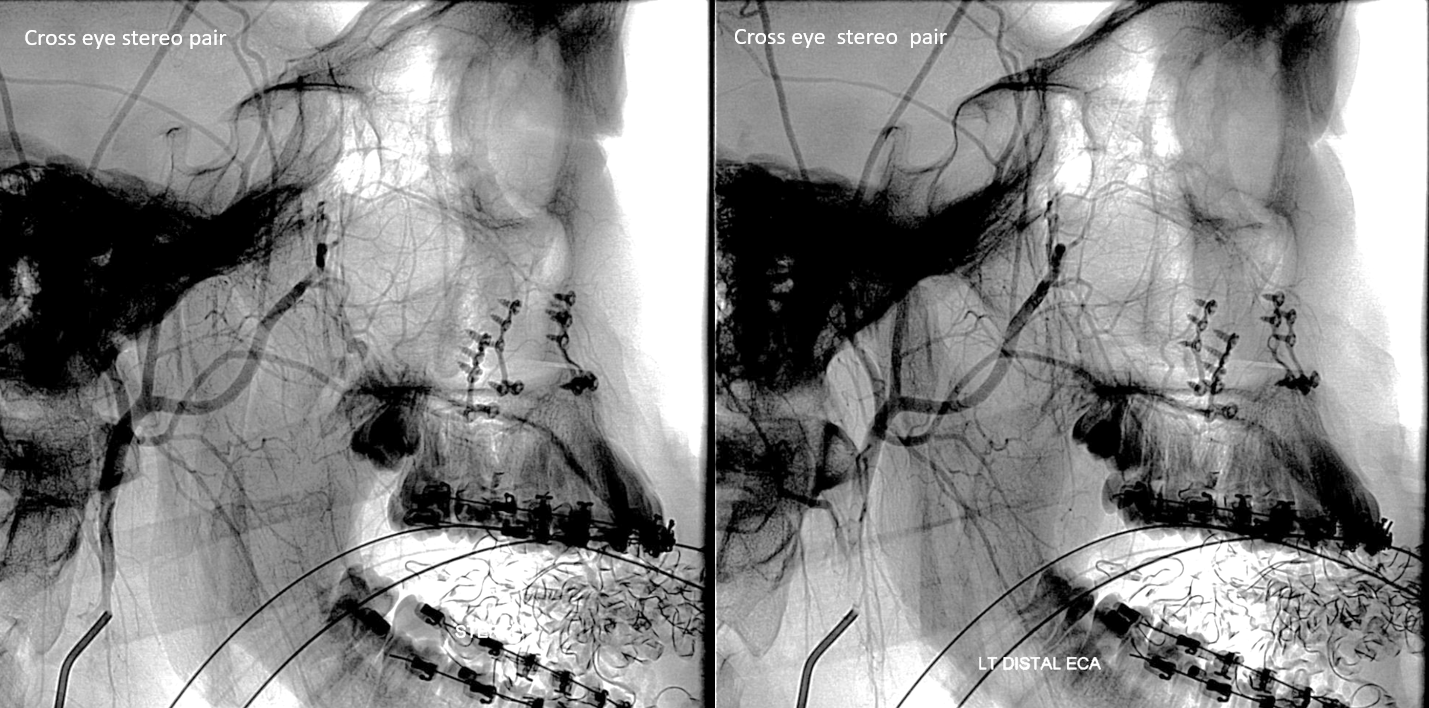
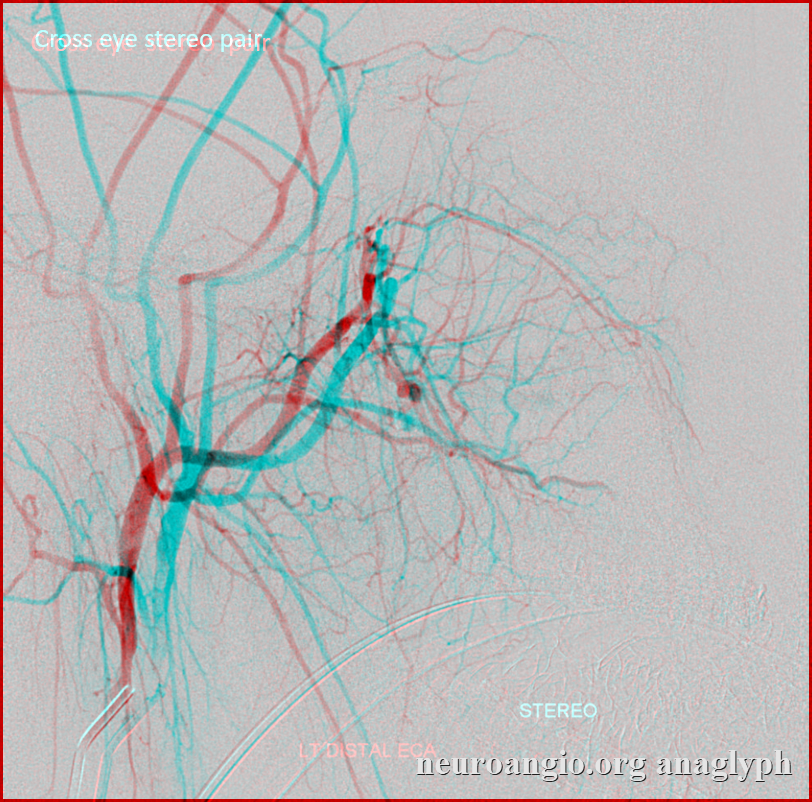
Cross-eye stereo
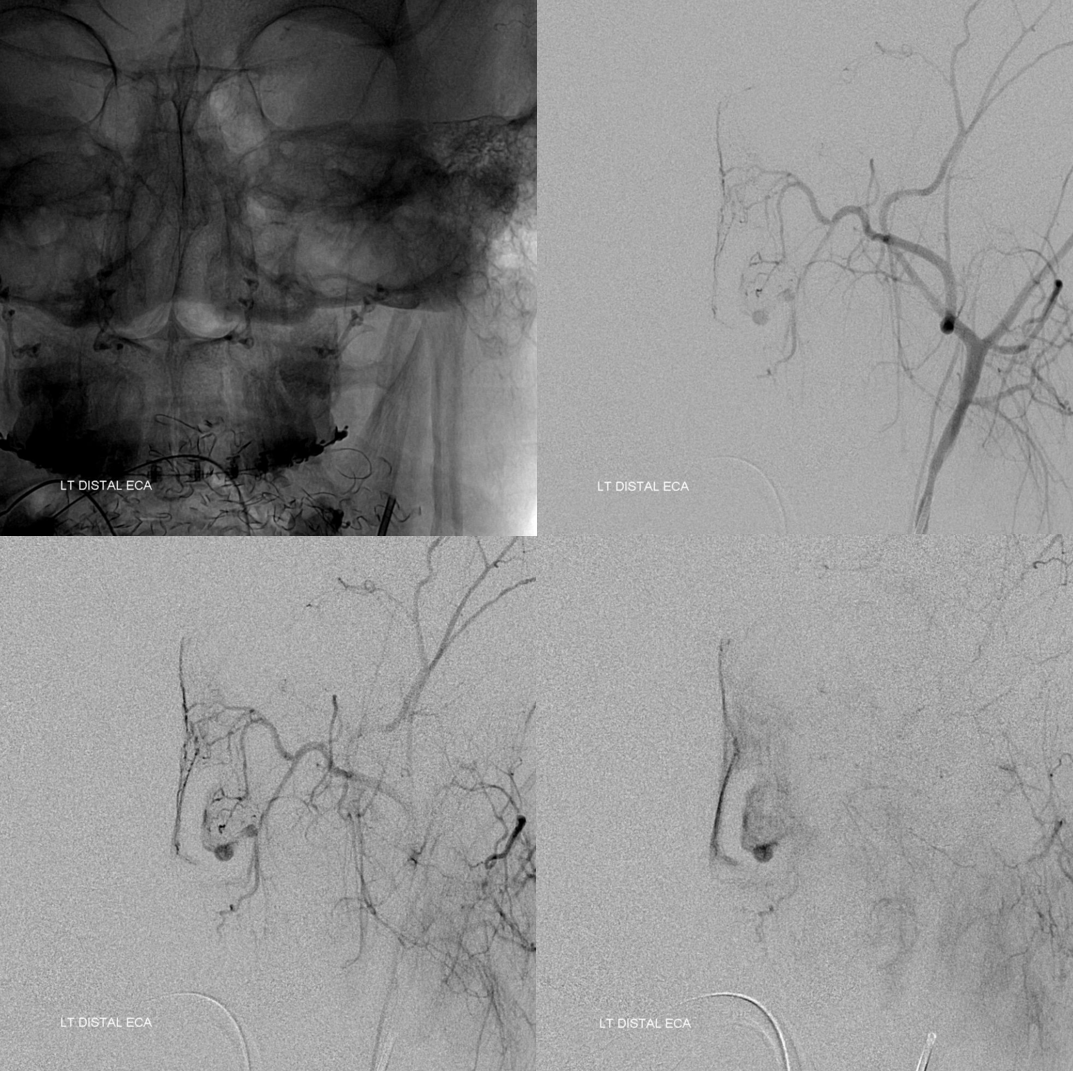
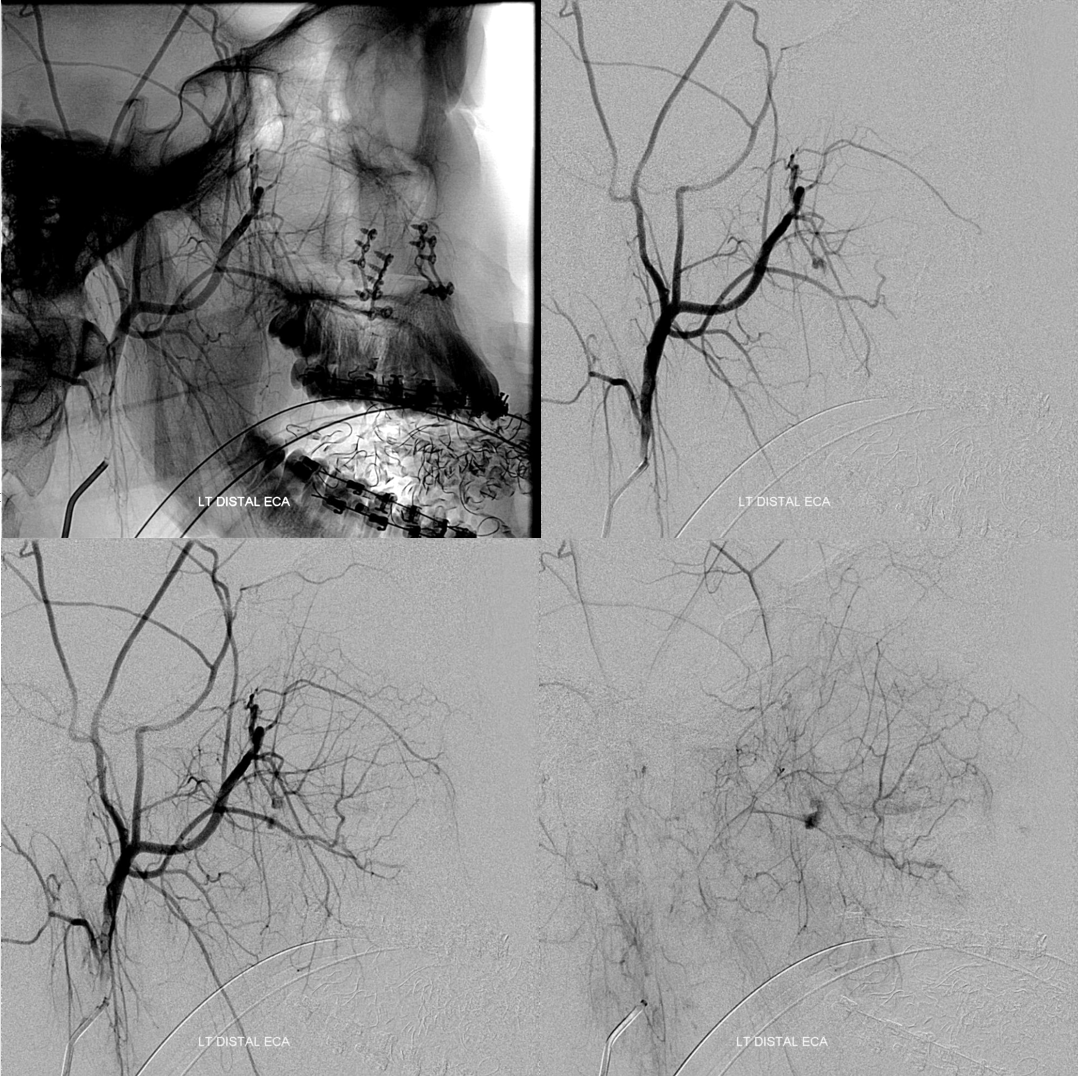
Left side is money shot — active extravasation from descending/greater palatine
Cross-eye stereos
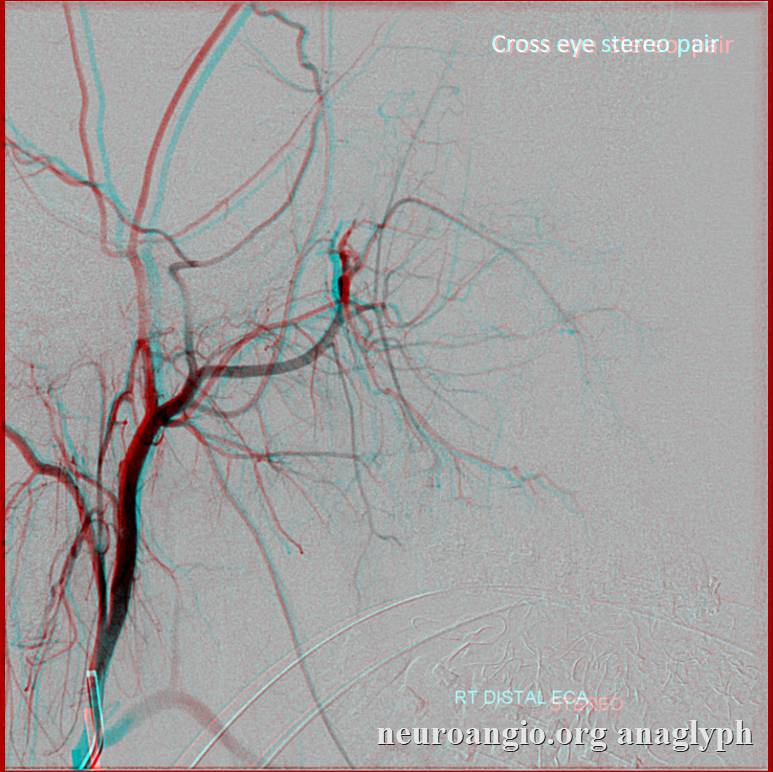
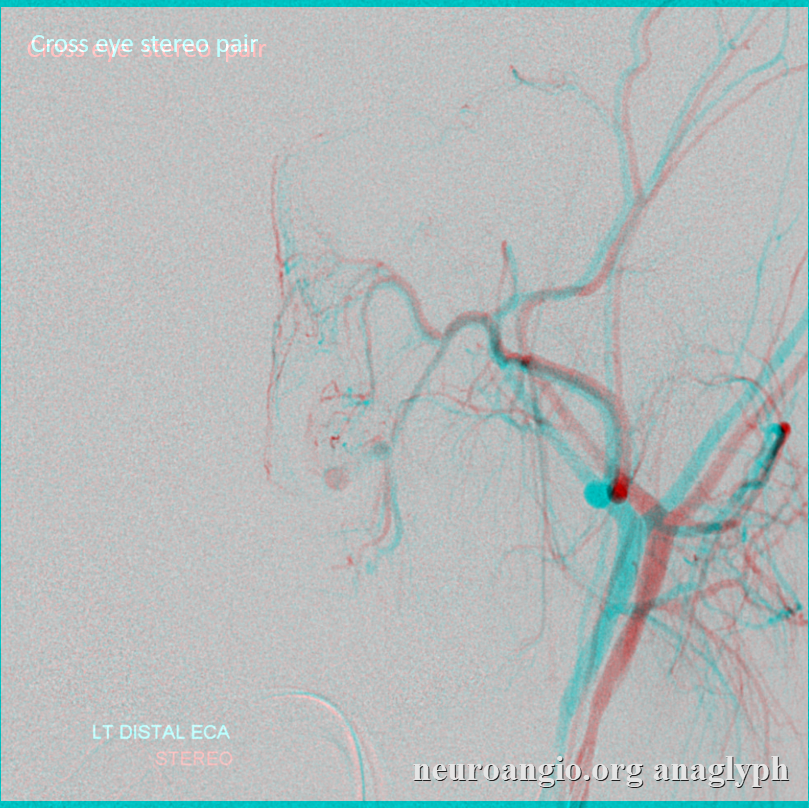
Anaglyph stereos — very deep ones…
Descending palatine — pre embo — also see some normal septal arteries of the sphenopalatine branch
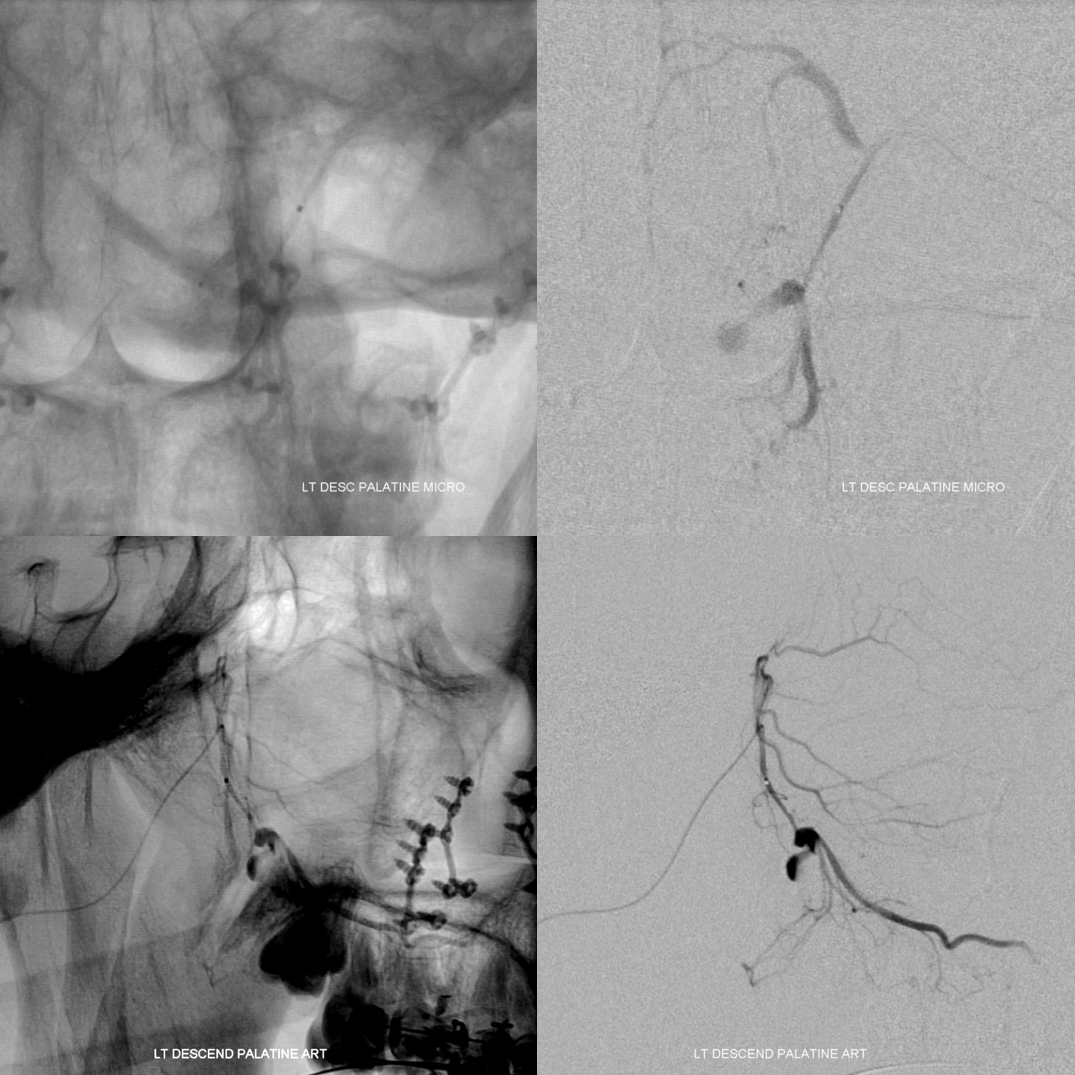
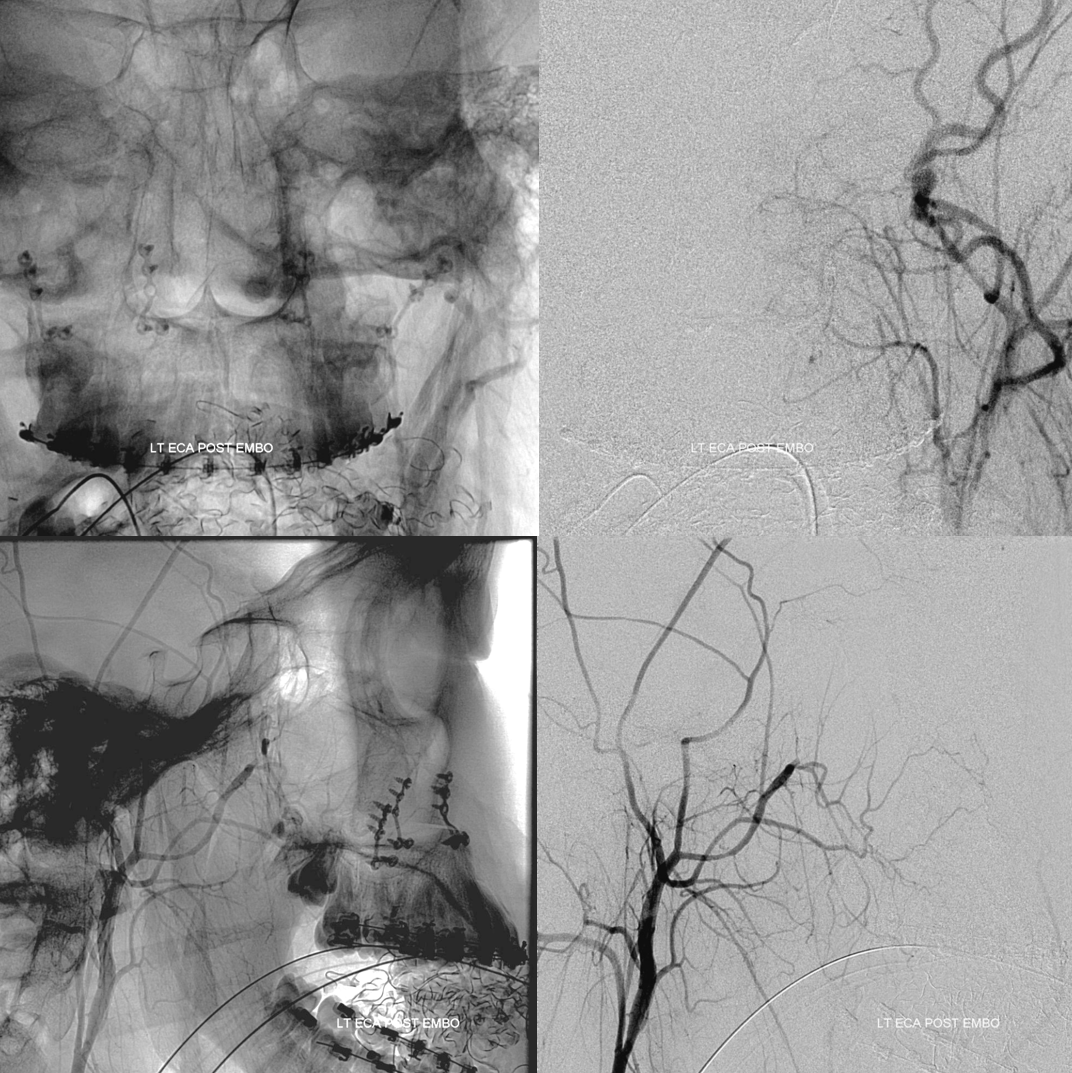
Post embo