
Difference in outcome of collateral embolization for frontal branch recurrent meningeal artery variant subdural hematoma. Figure from our JNIS publication on Dural Vascular Anatomy and Implications for Subdural Hematoma Embolization
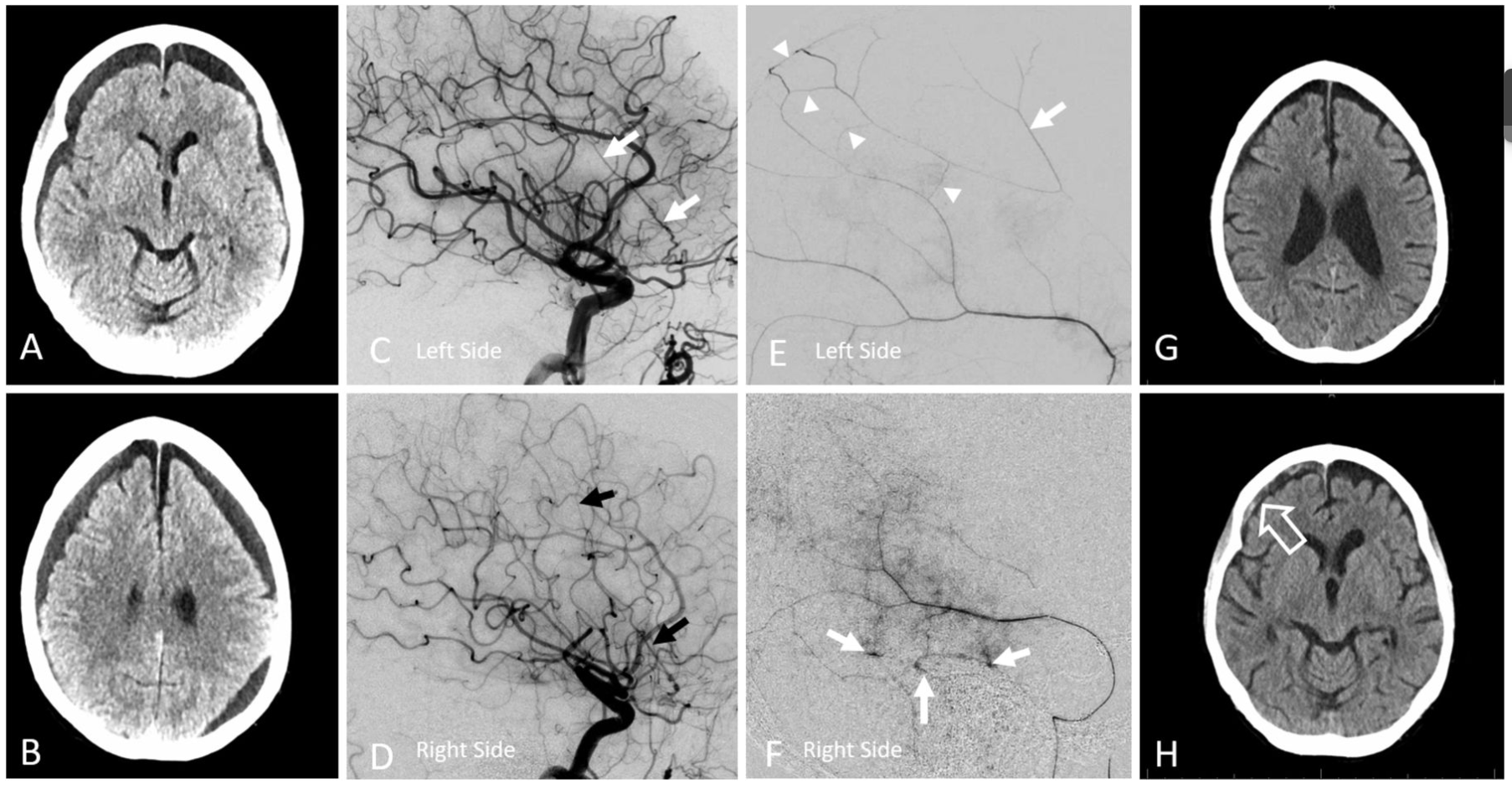
Figure 5
(A–H) Subdural embolization in the setting of bilateral recurrent meningeal artery dispositions. (A, B) Bilateral subdural collections. (C, D) Recurrent meningeal arteries supplying the frontal dura on the left (C, white arrow) and right (D, black arrow) sides (see figure 2A–D). (E) Left petrosquamosal branch ‘wedge position’ injection opacifying part of the frontal branch territory (white arrow) via several primary outer layer network anastomoses (arrowheads). This allows for partial embolization of territory principally supplied by the ophthalmic origin frontal branch. (F) On the right side, similar connections are not demonstrated and embolization is limited to the posterior middle meningeal artery territory. Note several venous lakes in the walls of the sigmoid and superior petrosal sinuses (arrows). (G, H) Delayed scan, showing complete resolution of left convexity collection, and persistent right frontal collection, with a small new hemorrhage (open arrow).