
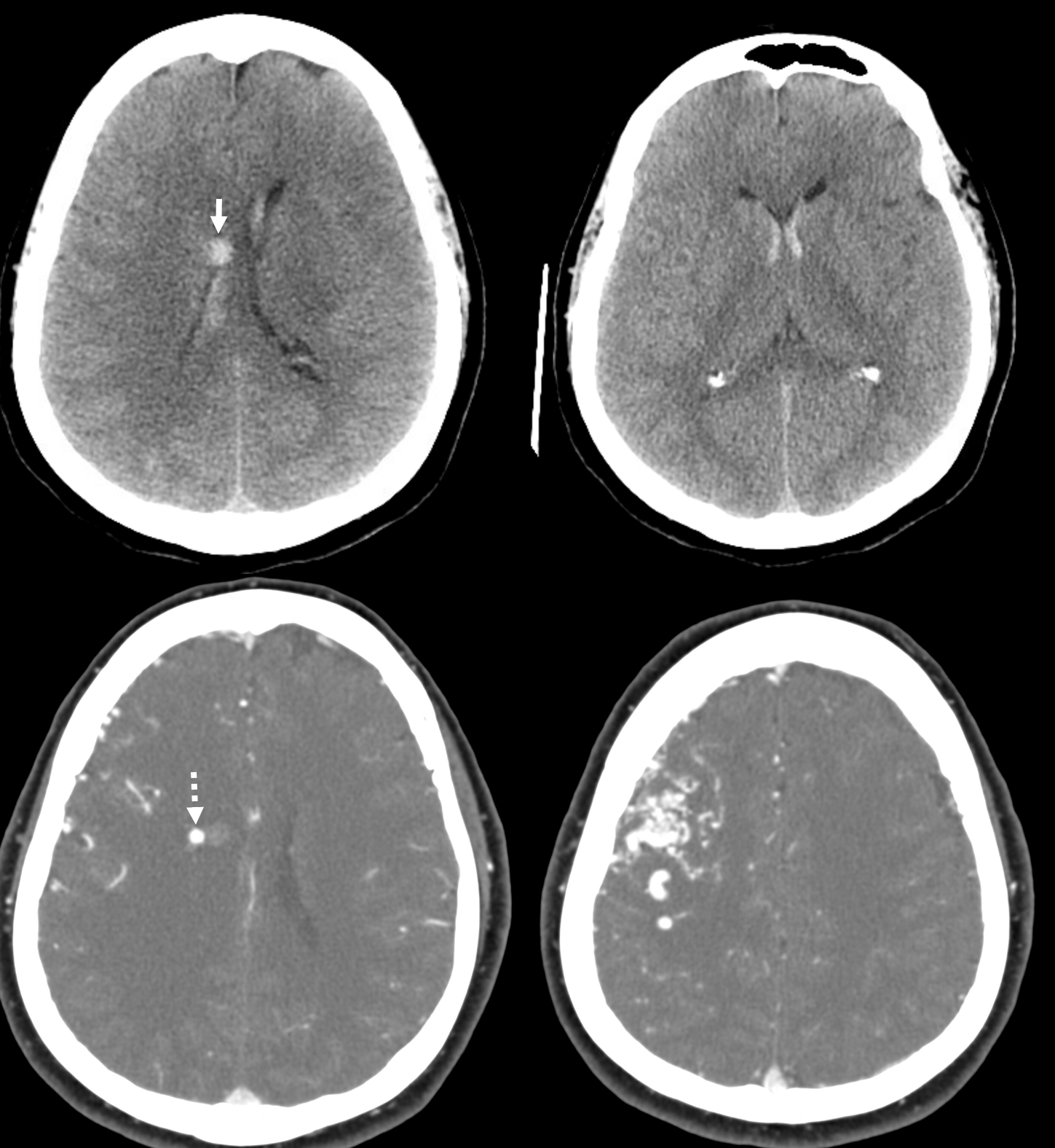
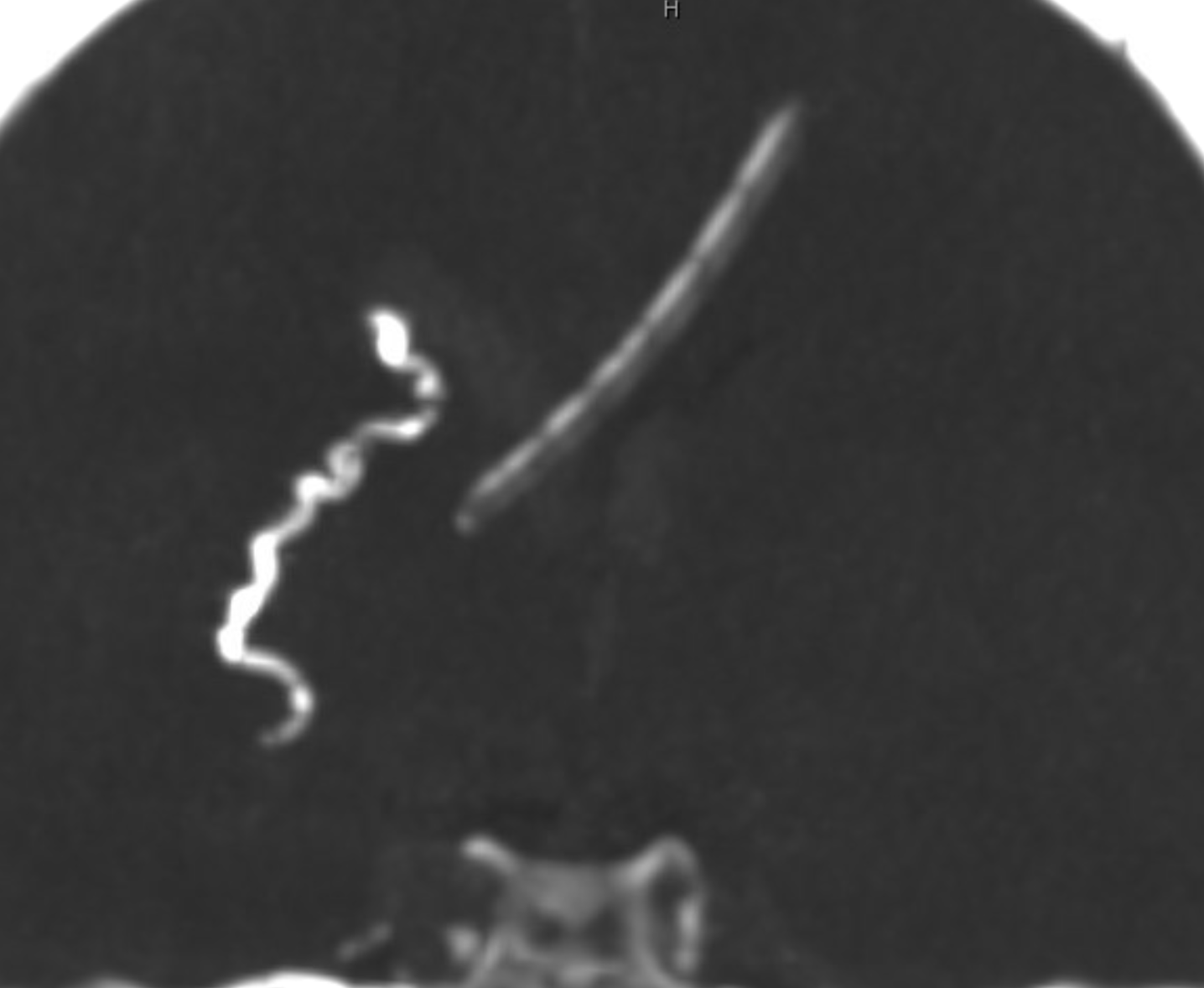
Presentation with right paraventricular hemorrhage with intraventricular extension. CTA shows culprit pseudoaneurysm, quite a distance from the mainly cortical AVM. This suggests high likelihood of lenticulostriate artery as source of supply to pseudoaneurysm and deep portion of AVM
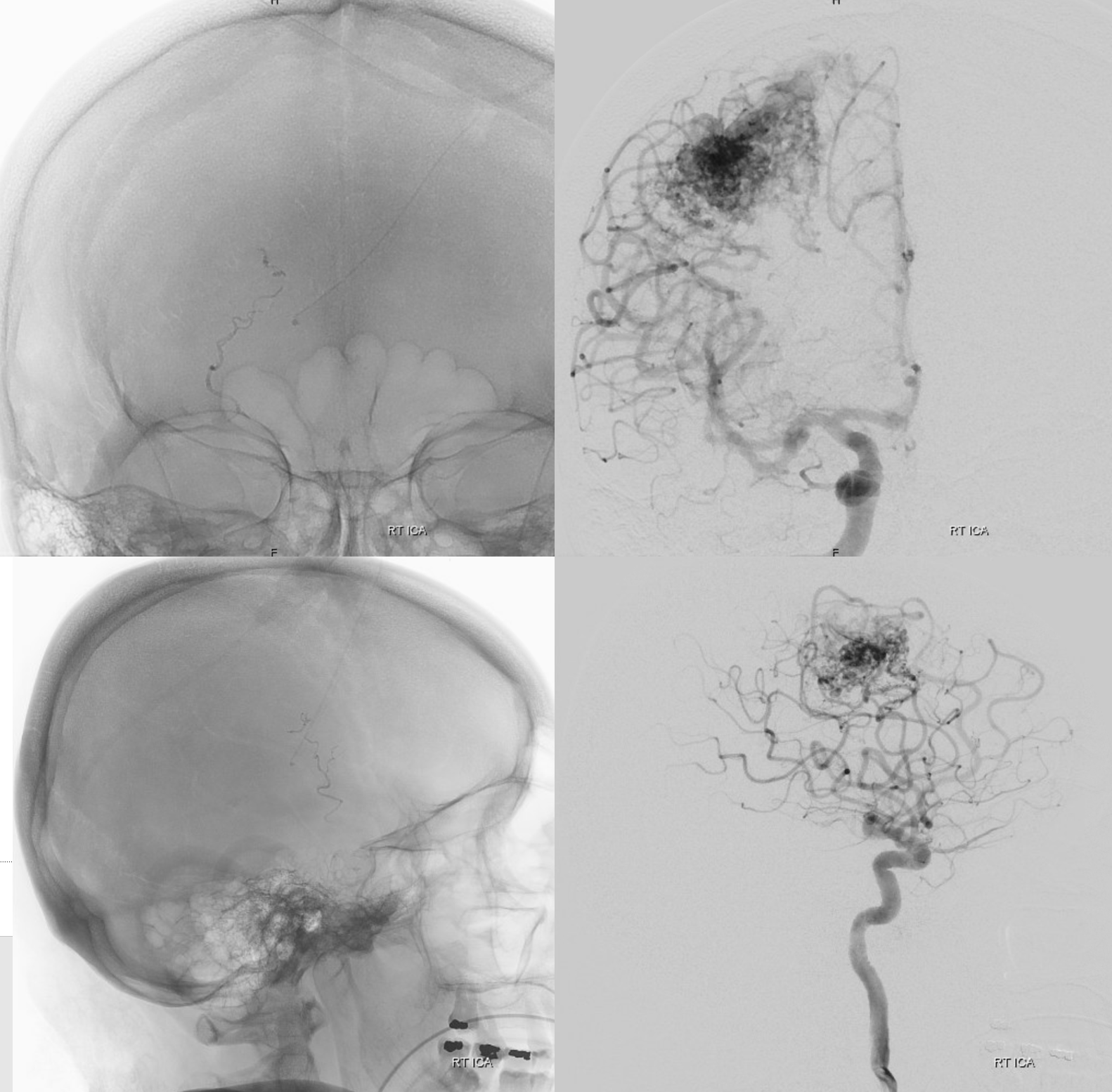
Indeed, this is confirmed angiographically. Notice a number of important features. The AVM is mainly cortical and superficial, yet it has deep supply which is also source of hemorrhage. Despite having deep supply the AVM has no discernable deep venous drainage, which is highly unusual.
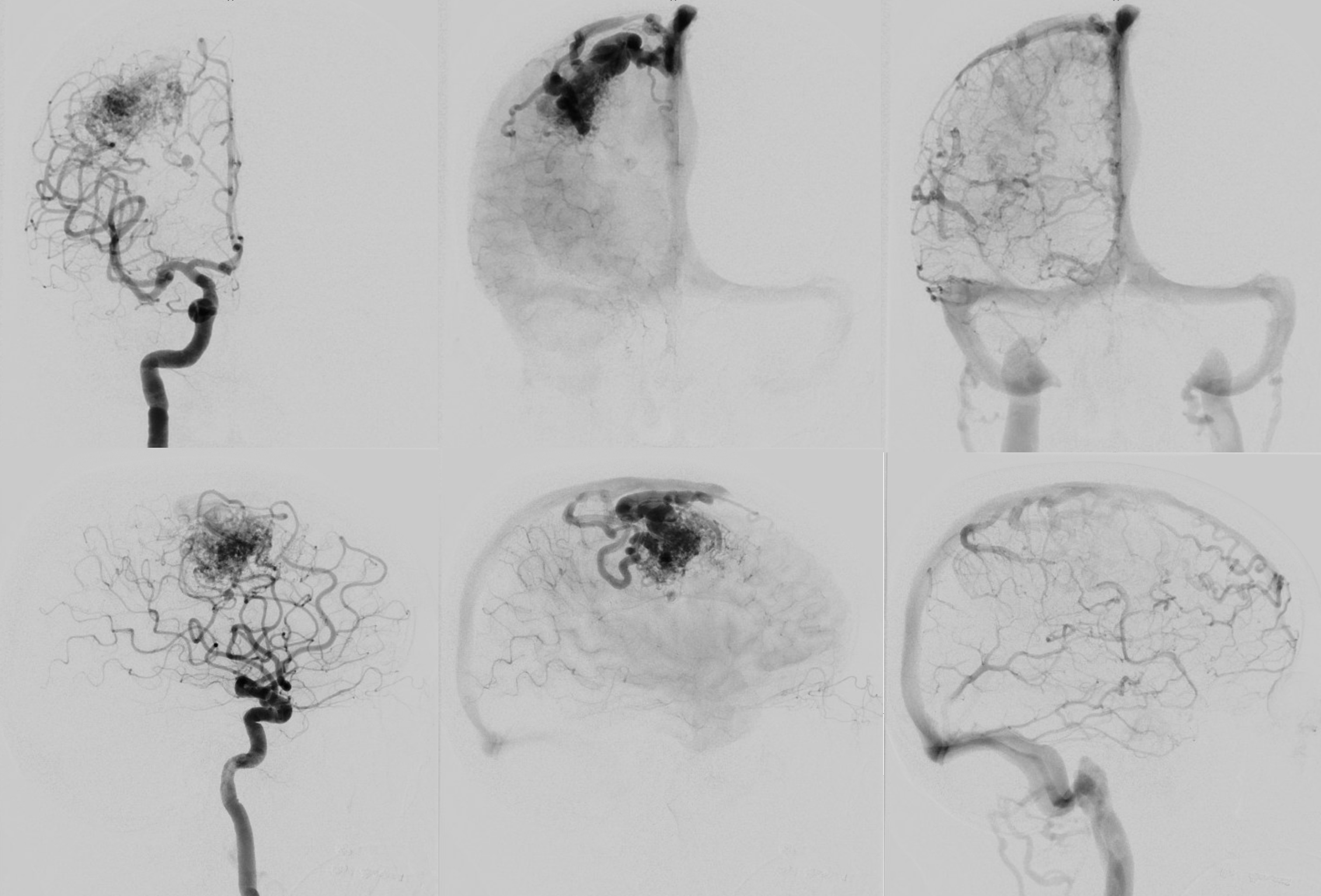
Deep supply to an AVM (whether lenticulostriate or choroidal) is at increased rupture risk, as these normally small vessels are subjected to massively larger flows than they were designed to handle
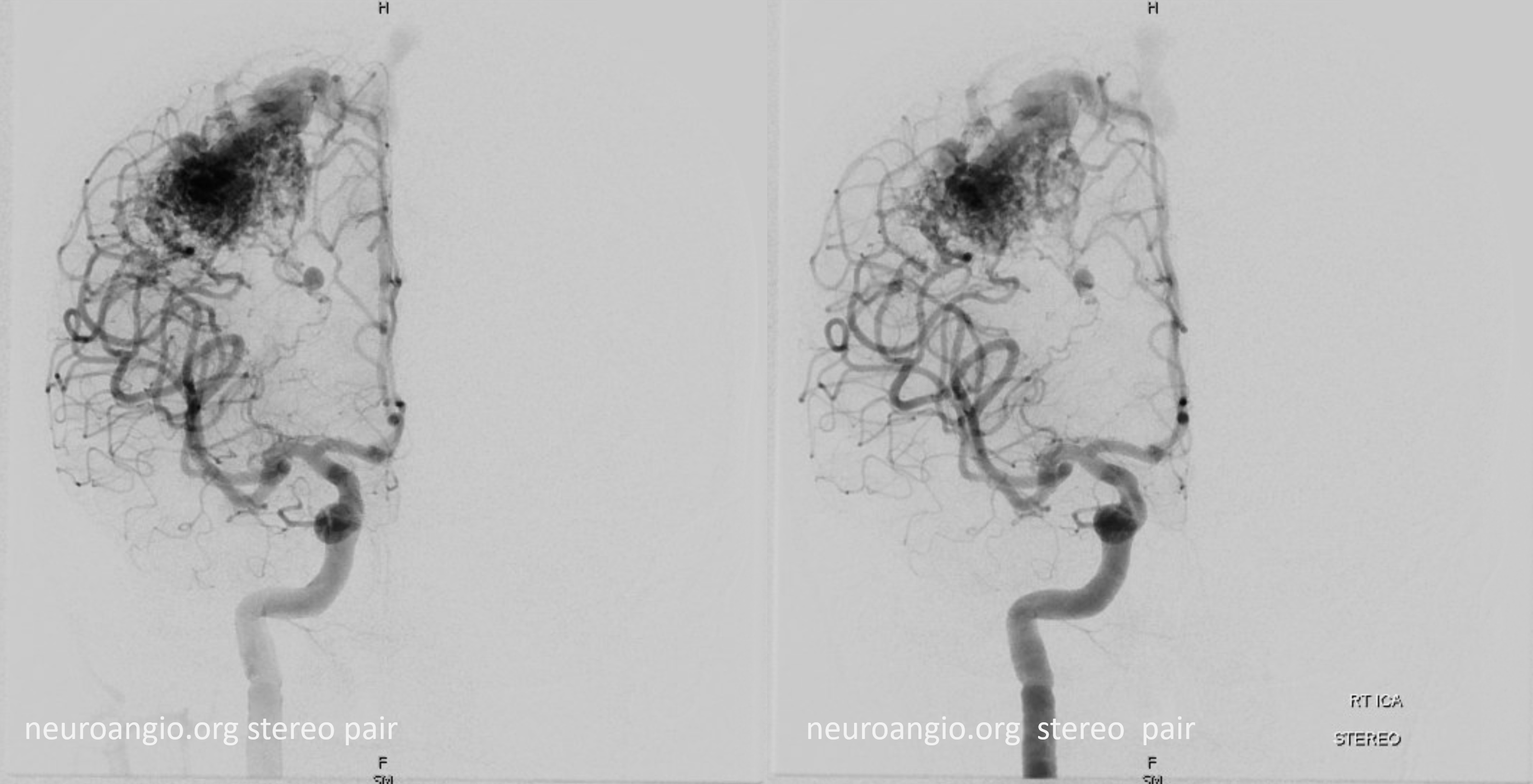
Stereo
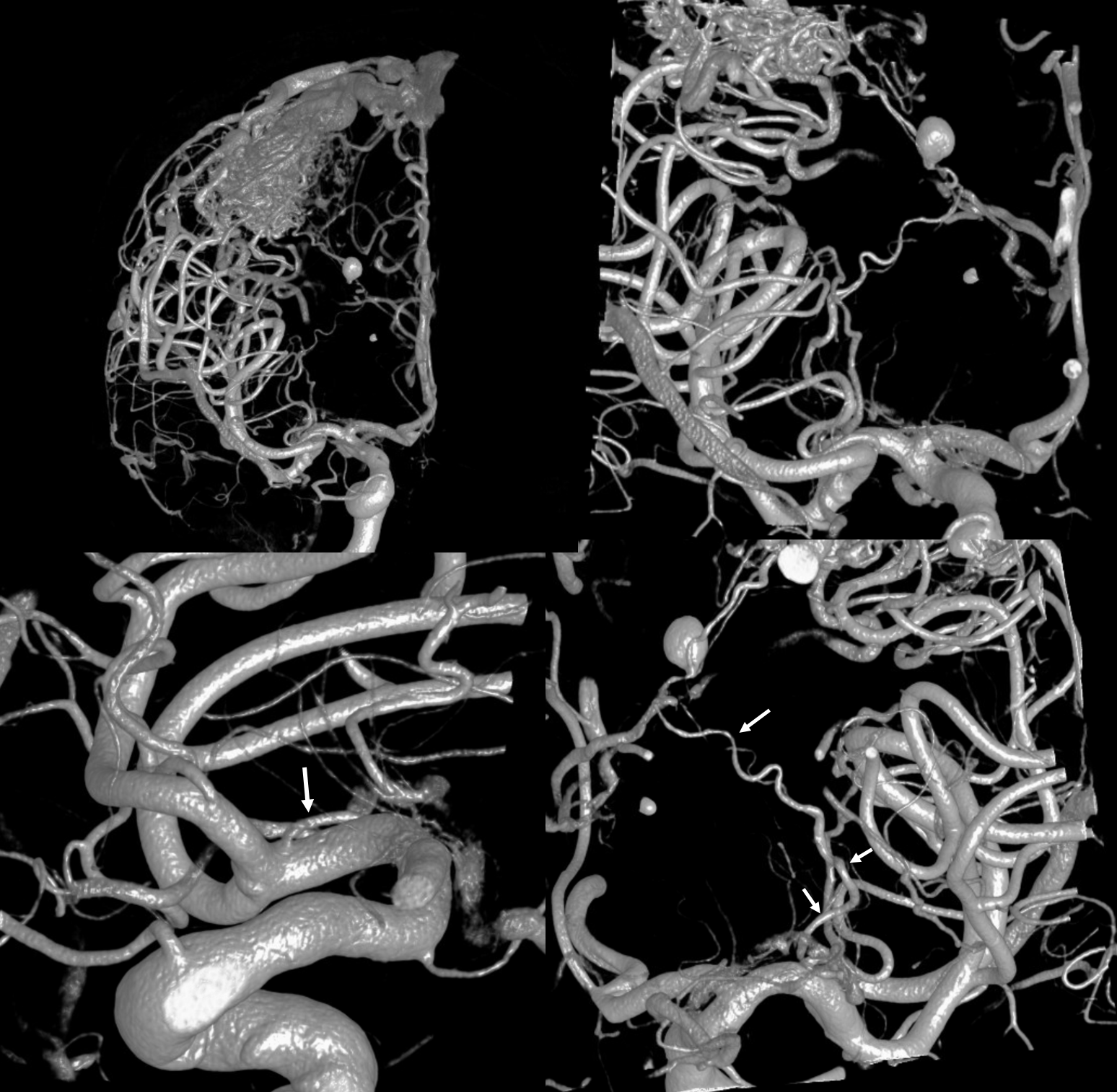
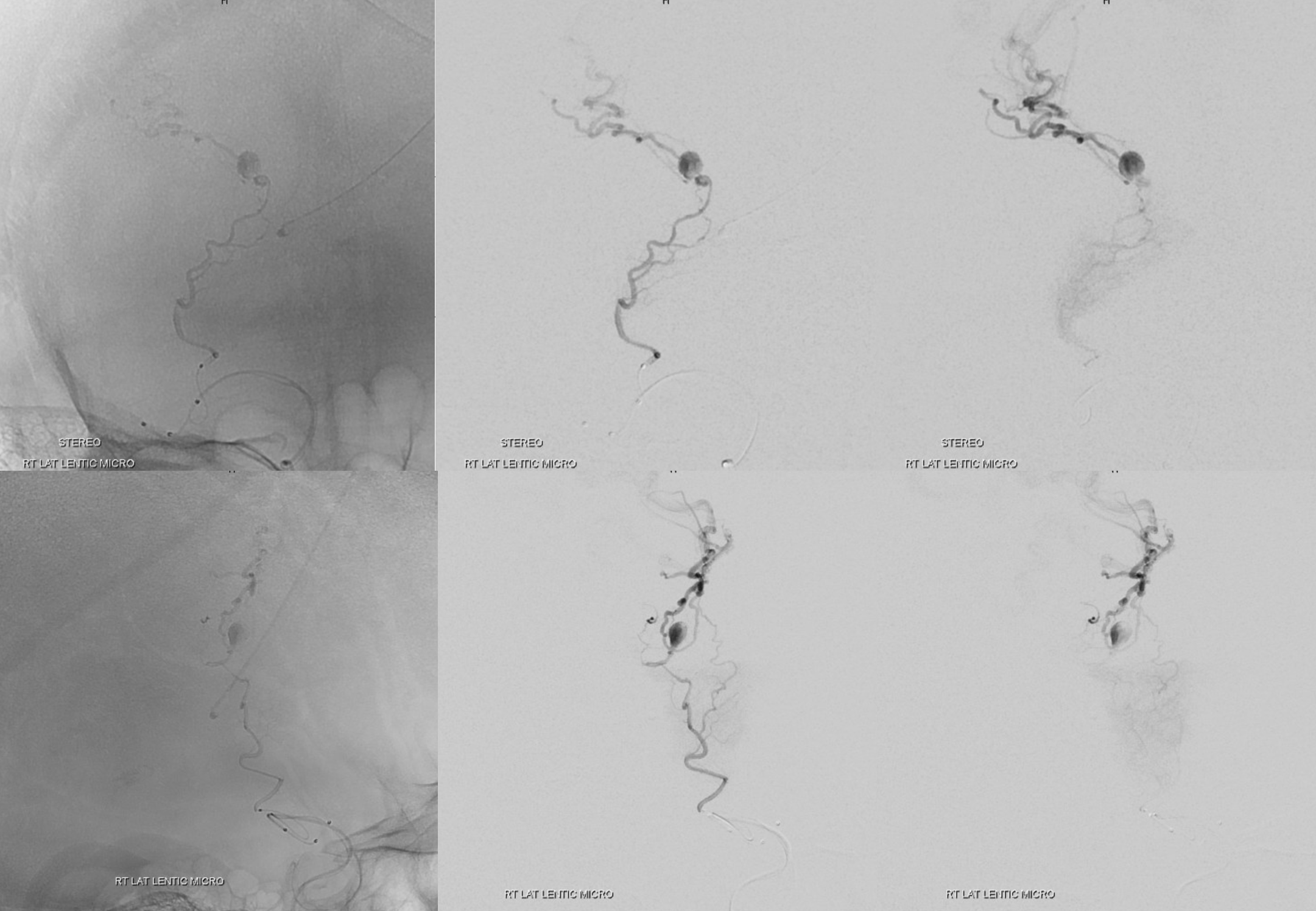
Catheterization of lateral lenticulostriates is extremely difficult due to their recurrent course. A flat panel / cone beam / DYNA CT is key to planning. The “regular” 3D images are usually of insufficient resolution to reliably see vessel origin. Here we have a global VR view, a magnified reconstructed VR view, and two highly detailed reconstructions (bottom row) showing in excellent detail the target artery. Note its extremely recurved proximal course, 180 degrees away from the M1.
Catheterization proved tricky indeed. Took about 1 hour, using a Magic 1.2F and Hybrid .08 straight. Ultimately was able to get about 2 cm into the vessel, with aid of a Scepter XC 4×11 balloon to help prevent wire/catheter herniation. Tip of Magic is arrow. Different time points of catheterization.
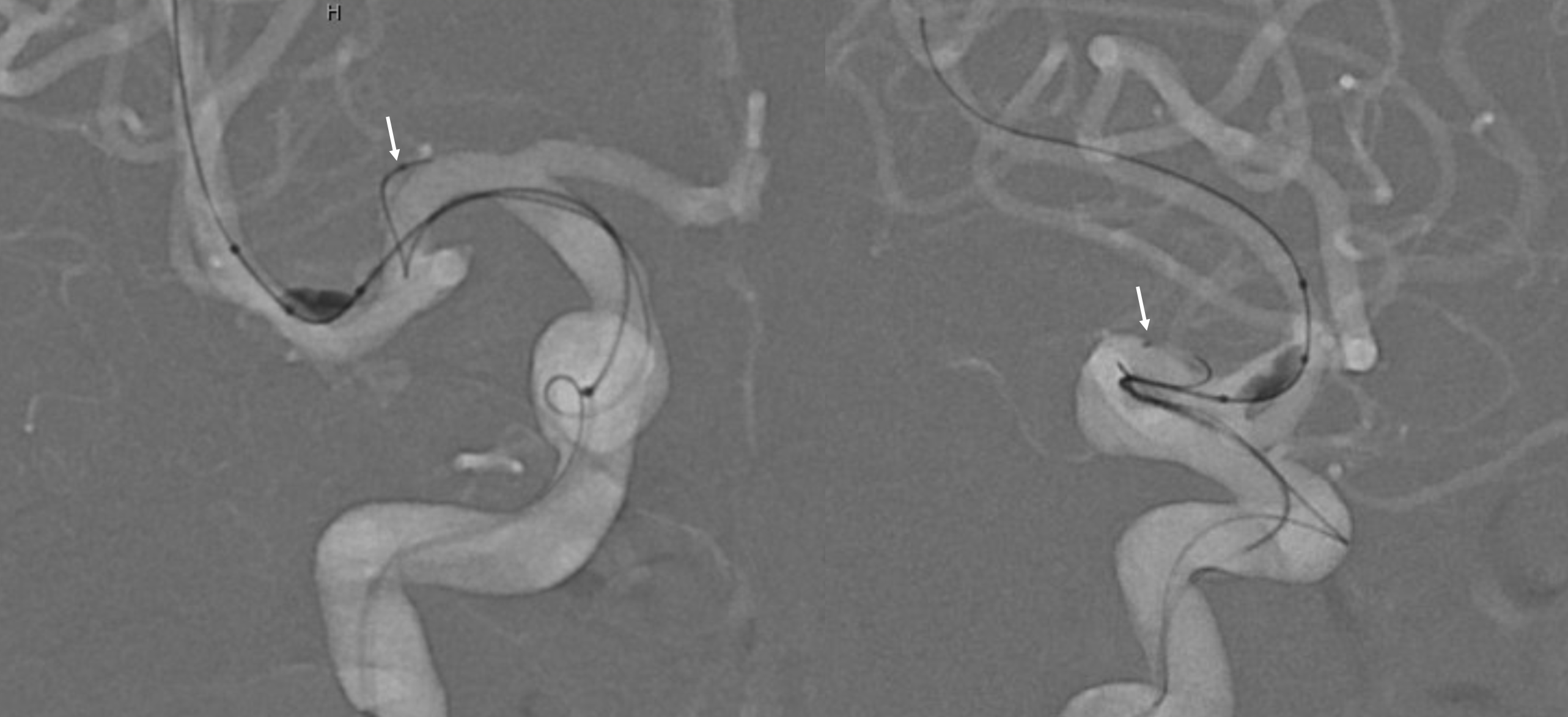
Beauty — selective lateral lenticulostriate injection. Notice a small medially projecting branch which supplies the majority of this vessels territory. The pseudoaneurysm is well seen.
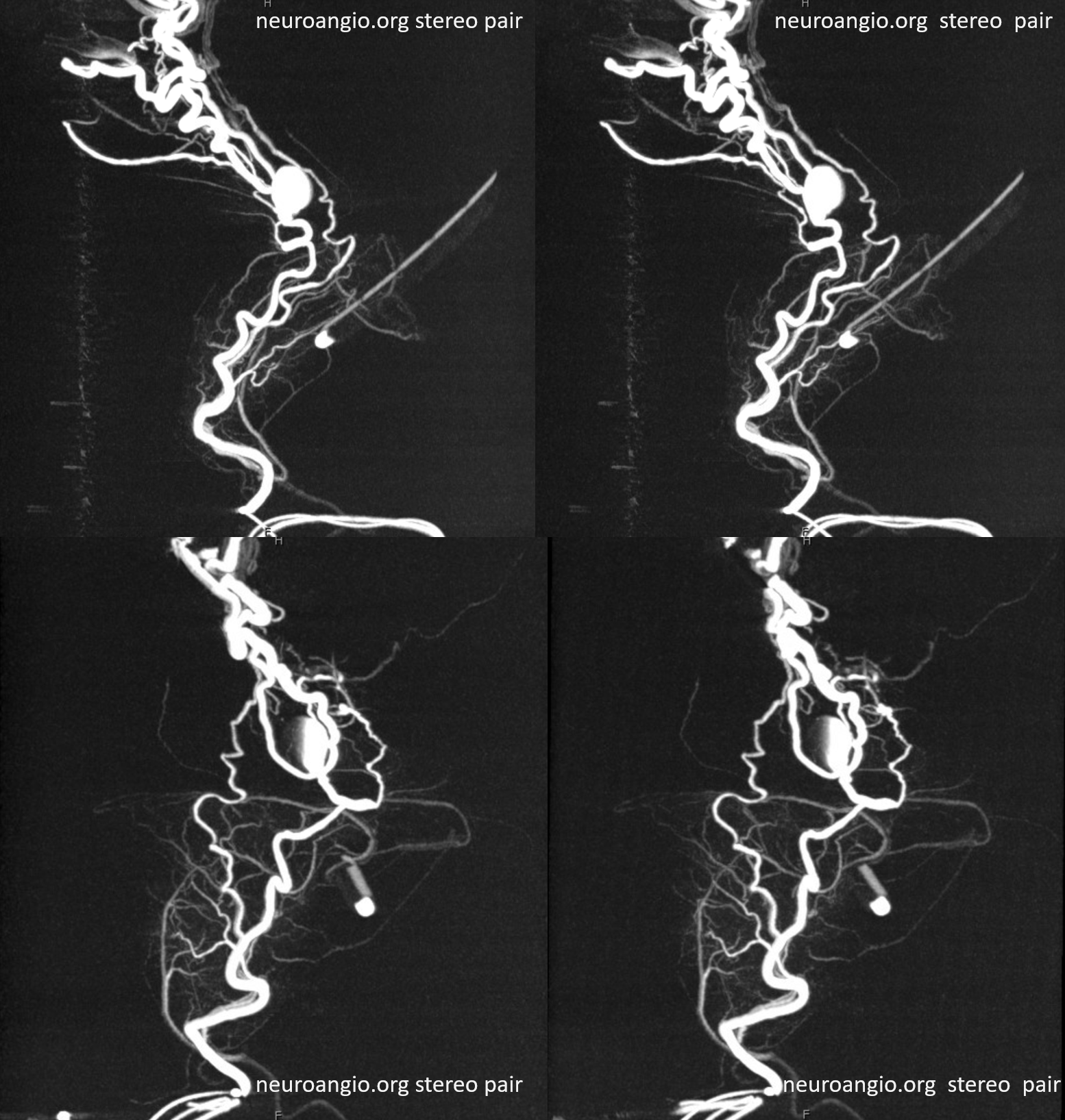
Stereo MIP images of DYNA CT — how cool is that…
VR movie
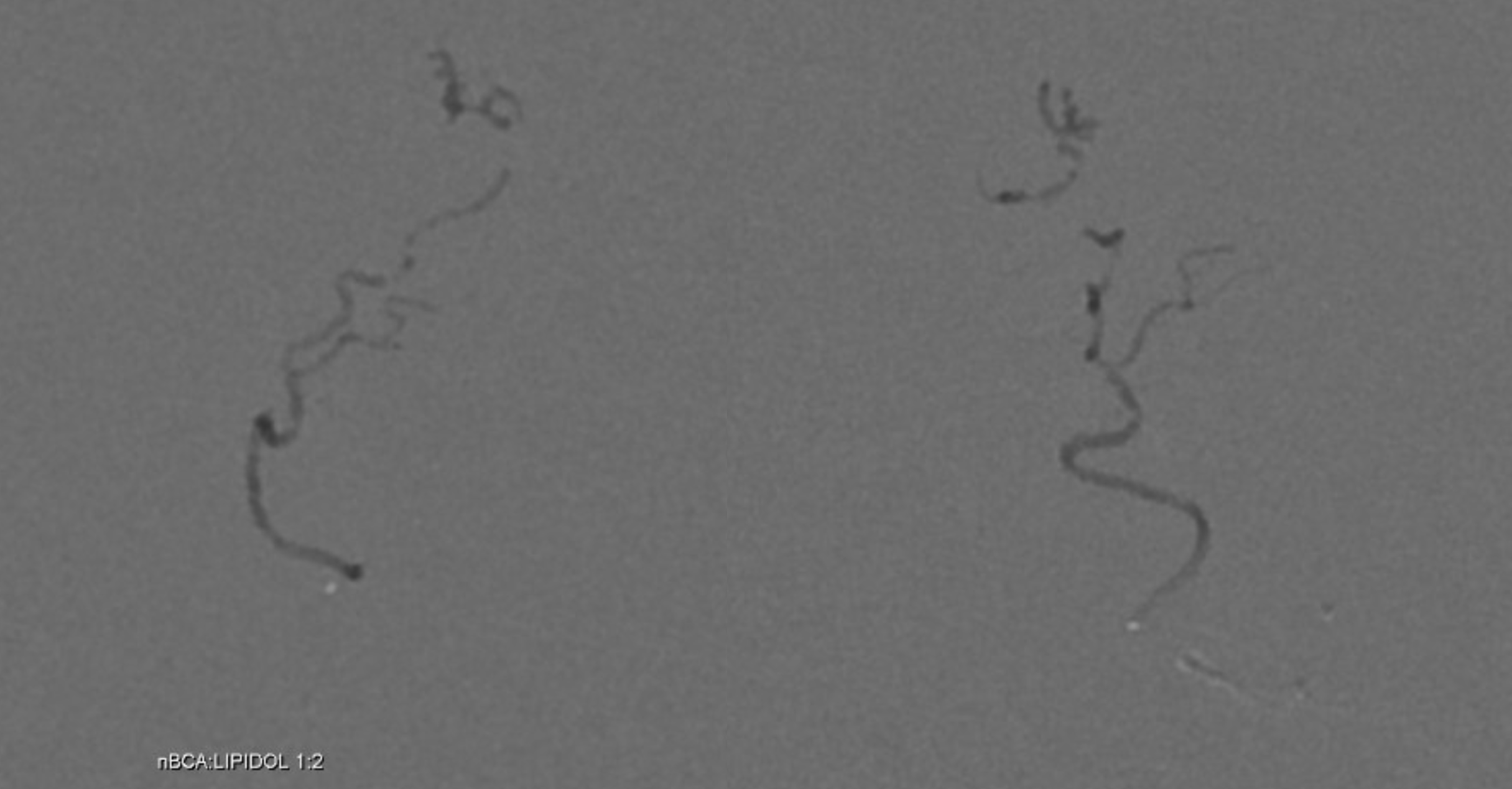
nBCA:Lipidol 1:2 cast. This was pushed as a torpedo (sandwich) technique, given long distance from catheter position to the target, and lack of flow control / wedge position. The very small volume of the vessel was smaller than the volume of “torpedo”; nevertheless, the technique allowed for sufficient penetration to reach the aneurysm. A more proximal occlusion would have been sufficient also, but it is nice and even more helpful to nail the aneurysm.
Torpedo / sandwich injections (both terms are used) are fast and particularly tricky. Below is a real time movie of the injection.
Post DSA
Just like in setting of acute thromboembolic occlusion/thrombectomy, infarcts in lateral lenticulostriate territory, especially on the right, are extremely well-tolerated. Post CT
The existence of marked variation in relationship between AVM location and extent of deep venous drainage is discussed in our JNIS paper on Cerebral Venous Drainage.
Also see MCA page for some lenticulostriate variation discussions