
This young patient presented with multifocal extradural, extramedullary (epidural) and intradural extramedullary (subarachnoid) hemorrhages involving the cervicothoracic cord, with extensive cord signal changes that were ultimately given no better diagnosis than transverse myelitis. Spinal angiography identified a radiculopial spinal aneurysm arising from the right T9 segmental artery, like so:
An obligatory stereo pair, so useful in the spine:

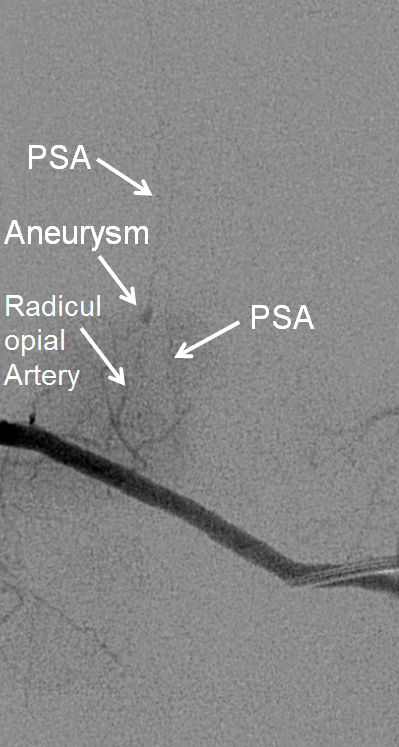
Microcatheter run, better showing the aneurysm and its off-midline relationship to the spinous processes. Notice unusually large size of the posterior spinal artery segment. In fact, prominent surface cord vessels, hyperemia, and arteriovenous shunting were seen throughout the cervical and thoracic spine, consistent with an acutely inflammatory process.

We felt that neither nBCA nor Onyx embolization were worth the risk; to durably chose this aneurysm the embolic must fill the aneurysm itself, and close the radiculopial artery, which is usually surprizingly well tolerated; in this case we felt that the prominent size of the PSA, and presence of major myelopathic symptoms, were too much to risk another hit. Coils were therefore placed in the intercostal artery (to mark the level of laminectomy) and into the proximal ventral division to slow down intra-aneurysmal flow. Our feeling was that proximal coils alone may achieve aneurysm thrombosis this case, which however did not turn out to be the case in surgery:
As suspected, the patient remains severely neurologically impaired from whatever it is we call “transverse myelitis.”
A similar case of radiculomedullary artery aneurysm was treated by proximal coil occlusion, without surgery. The patient recovered fully, and continues to be monitored without re-hemorrhage.