
How about some variety from neuroangio.org We do over 100 vertebral augmentation procedures annually. Mostly kyphoplasty. Here is a sacroplasty. Many ways to do this one. Fluoro-guided, CT-guided, fluoro-CT. Here is a CT case of a large unilateral fracture in a patient with severe left sacrum/pelvic pain exacerbated by standing/walking.
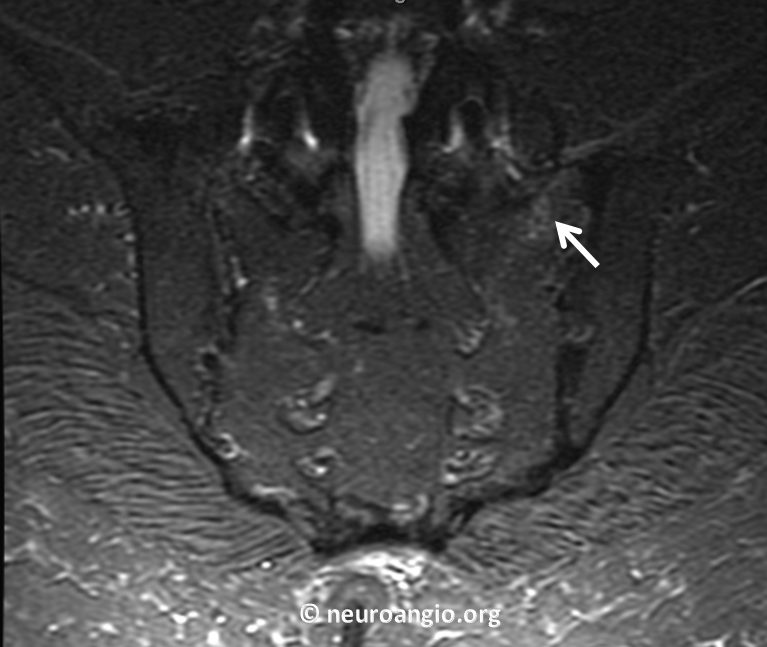
STIR MRI of pelvis in early stage shows beginnings of fracture (arrow)
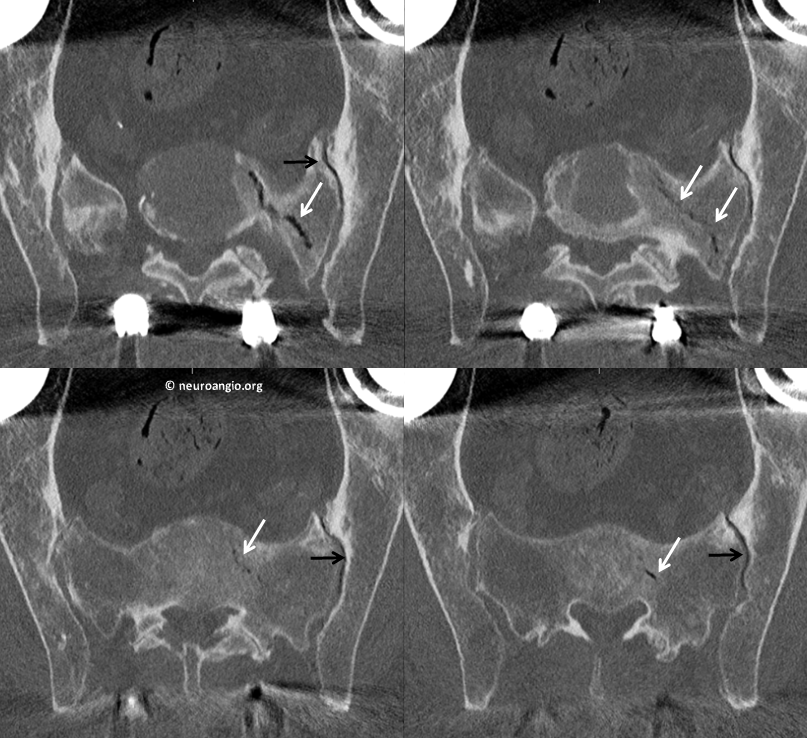
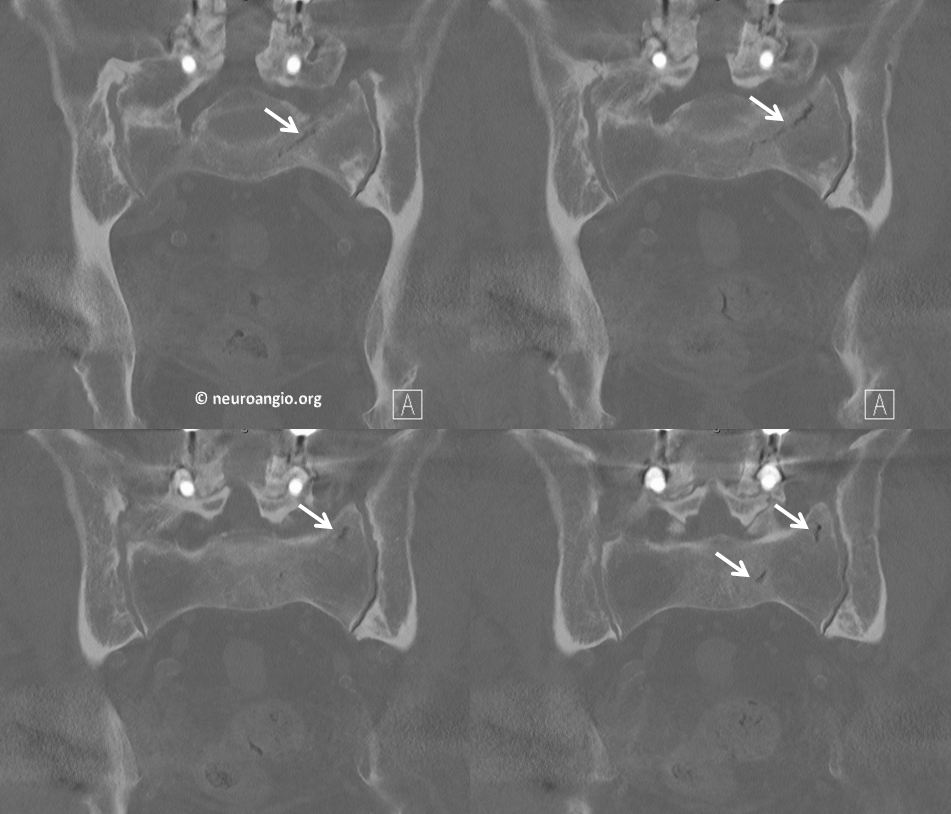
A few months later there is a gaping fracture with vacuum phenomenon (white arrows). There is also vacuum phenomenon in the SI joint (black arrows)
Coronal views
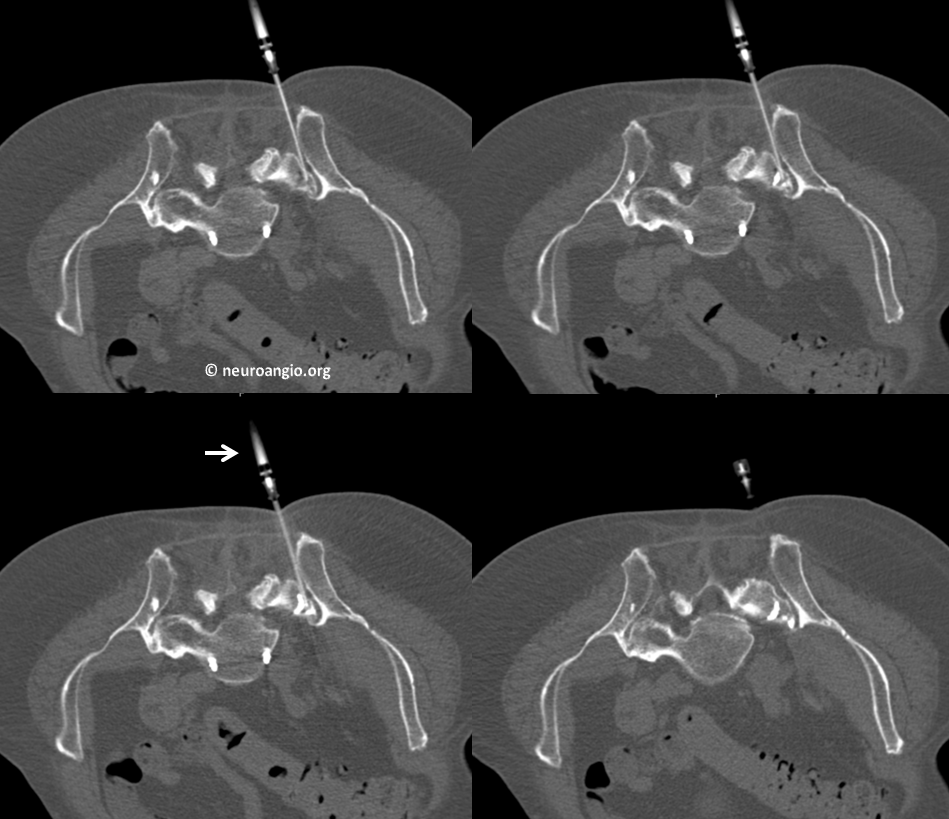
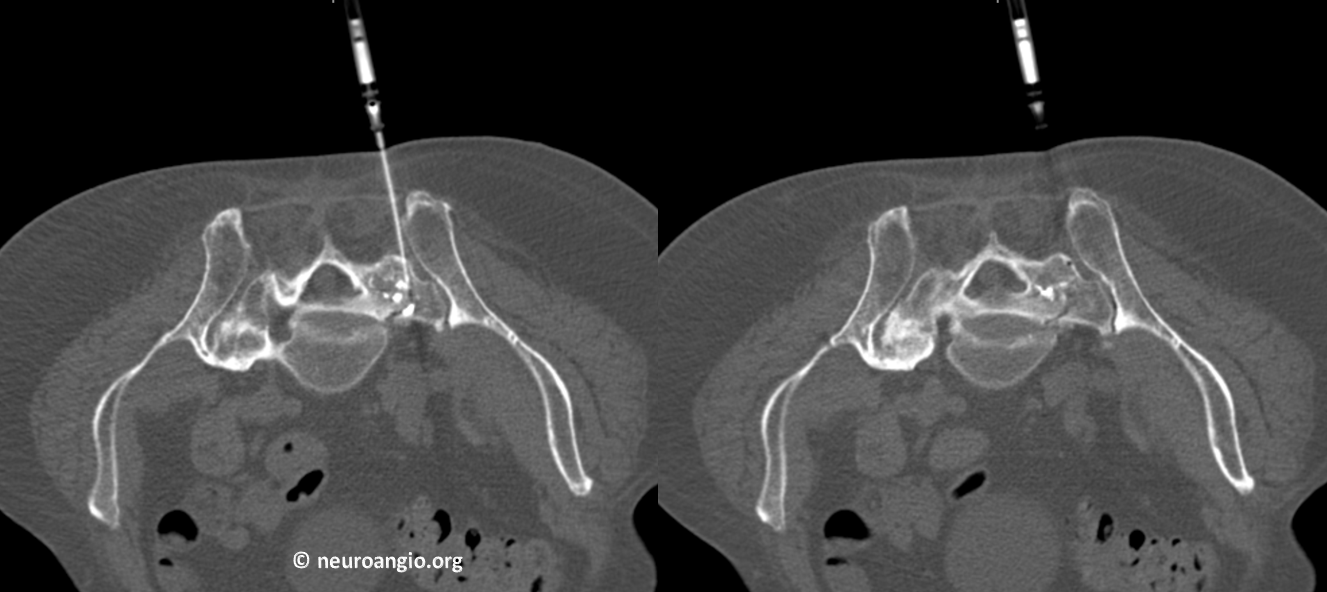
Poor quality bone facilitates easy access. This is a simple and very cheap Argon 17 Gauge, 7 cm coaxial needle. A push by hand is all it takes to get in. A 1 cc syringe full of very liquid methylmethacrylate cement is attached (arrow). In contrast to kyphoplasty, we prefer liquid, runny cement to penetrate cracks and fractures in sacroplasty. CT guidance helps of course. Small volume (0.3 cc or so) injections are followed by CT scans. There is about 5 minutes of work time available with a 17 gauge system like this.
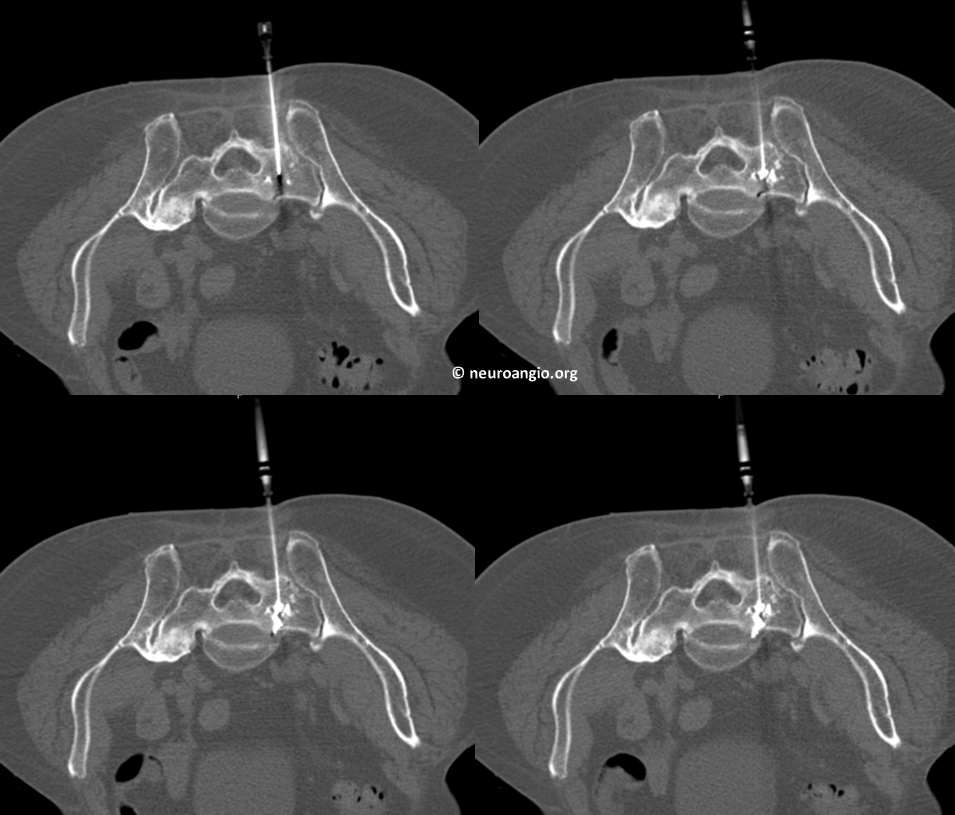
We keep 1 cc syringes on ice and reposition to a slightly lower location for additional cement. Still fracture is not well-penetrated throughout. The top part is, bottom not yet
Lower still third access. Small gauge needles compared to kyphoplasty allow for safe multiple access. Here we hit the fracture well with lots of good cement penetration
Post-procedure, lower half of sacrum. Nice cement cast in fracture. Notice extension to the foramen (black arrow) without penetration into it. Good time to stop
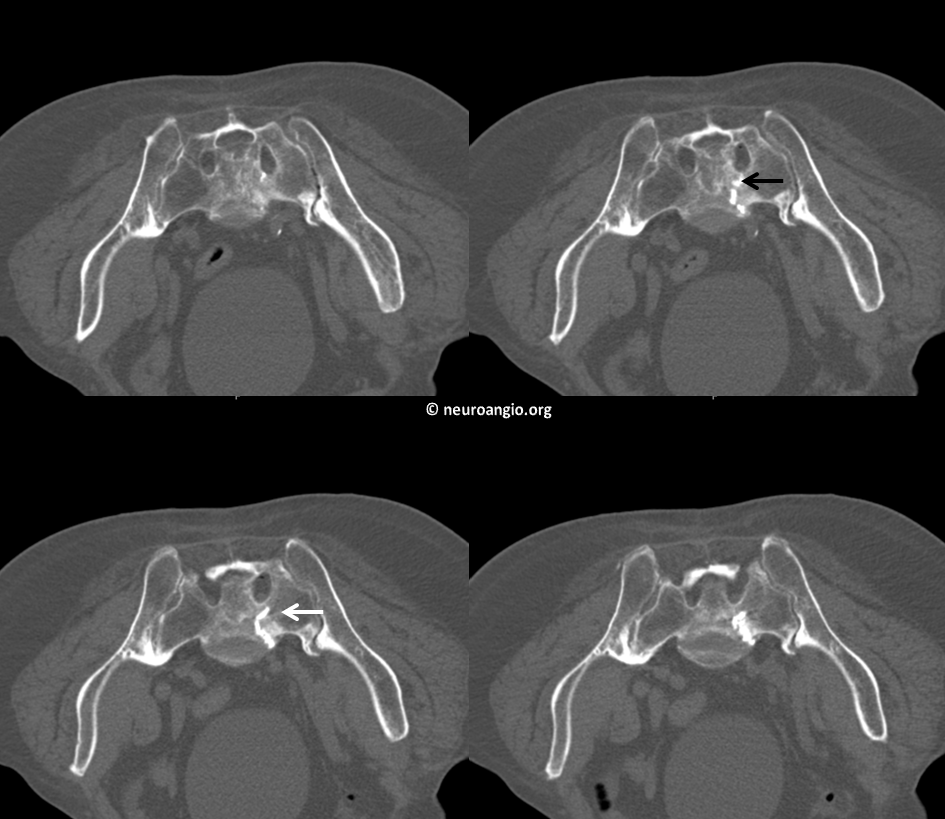
Upper half

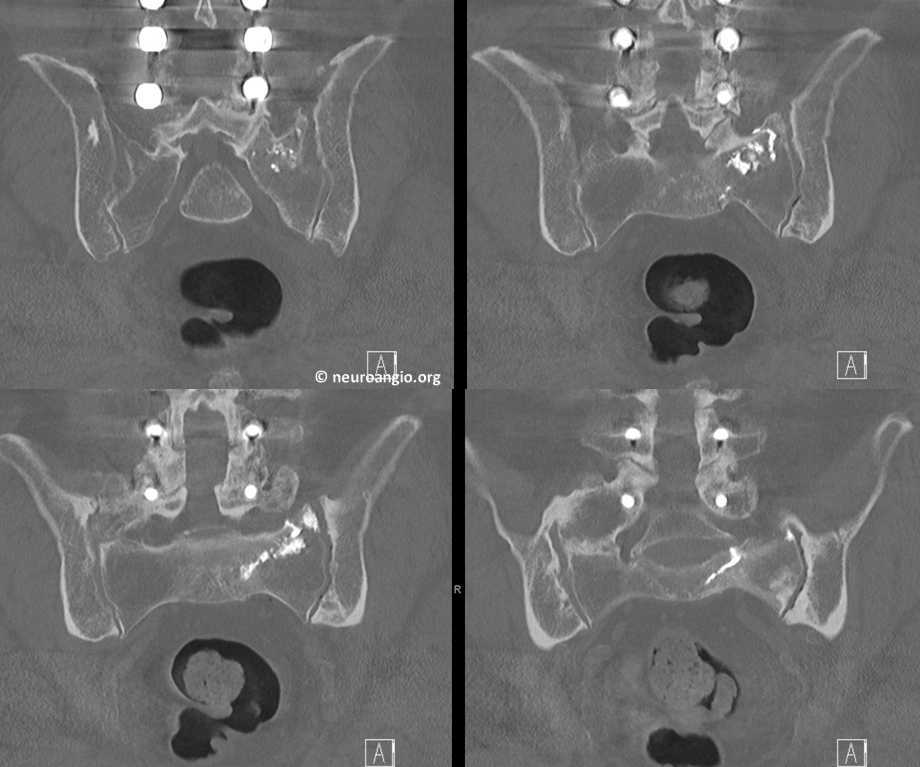
Coronal post views
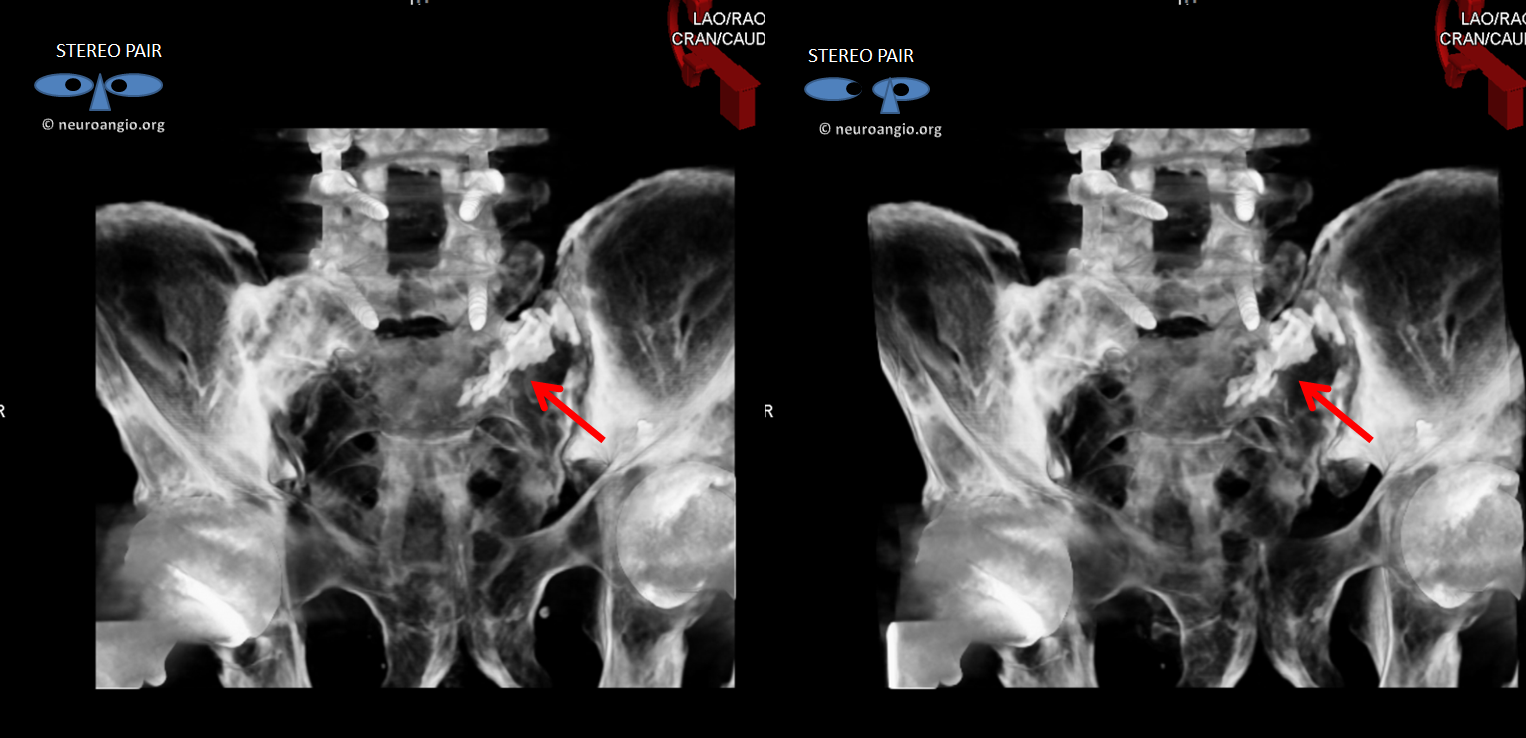
How about these stereoscopic volume rendered images! Cement marked by red arrows
Even fancier! Color thesholding applied. Look at this image in stereo!
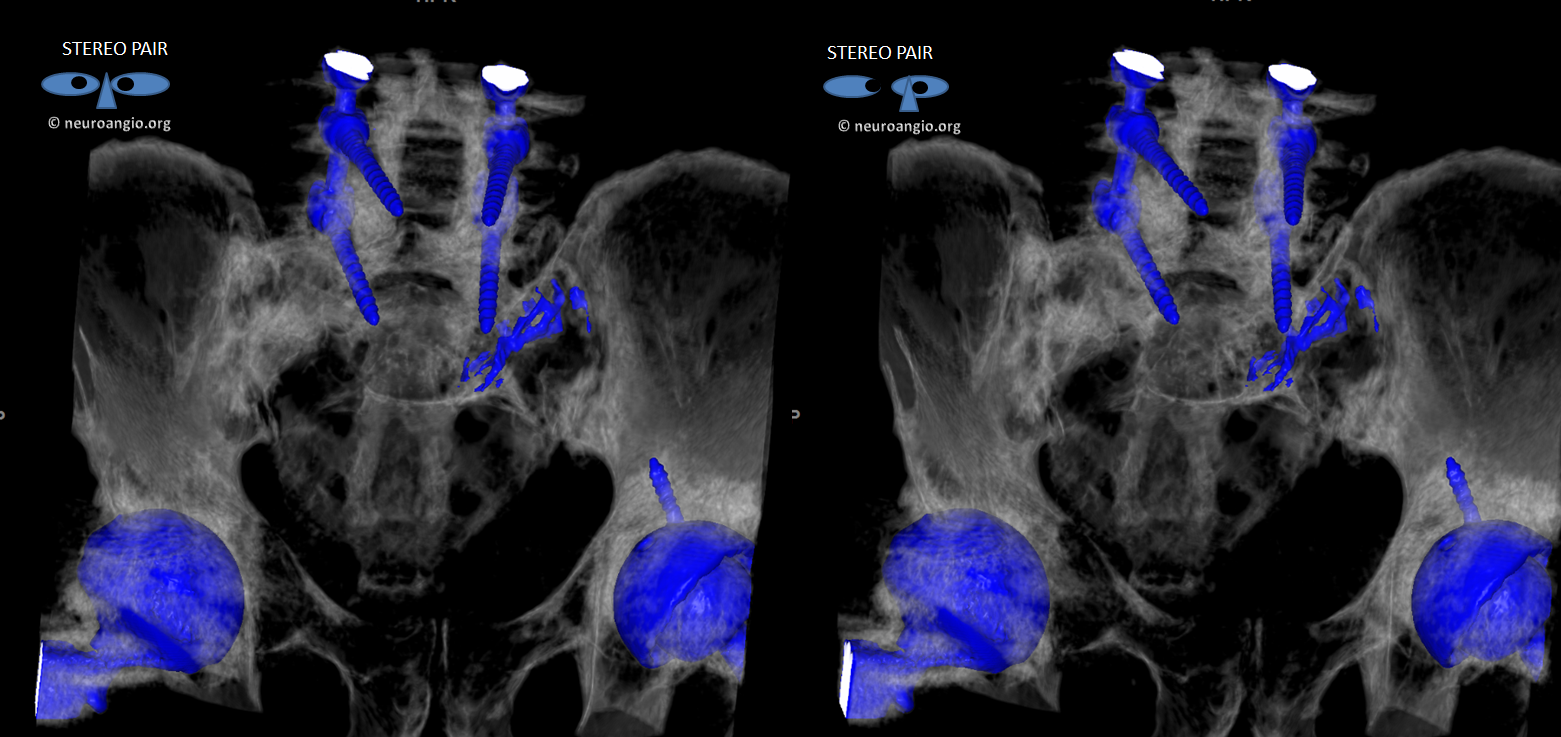
This is as good a sacroplasty as they come. No pain post procedure either. Hope that SI joint holds up