
Adding to our collection of superselective fistula embolizations. The point is that many sigmoid fistulas, especially low grade ones, drain into a common channel in the wall of the sigmoid sinus (black arrow = common channel, black arrowhead = connection to sigmoid sinus proper), like this:
![]()
How to deal with this? The easiest thing is to take down the whole sinus, assuming the brain does not need it. Simple and usually safe, but needlessly sacrifices the sinus.
![]()
The other way is transarterial. Not very elegant, as it involves embolization of arteries not directly involved in the fistula, riskier, and often plagued by incomplete embolization if the common channel is not permeated.
![]()
When carried out to completion, this approach is successful, but on the whole riskier than transvenous embolization, and still involves unnecessary permeation of arteries far away from the fistula
![]()
The best approach is superselective transvenous embolization of the common collector channel. It combines low risk of transvenous approach with sinus preservation.
![]()
So, the question is — sledgehammer vs. stiletto…
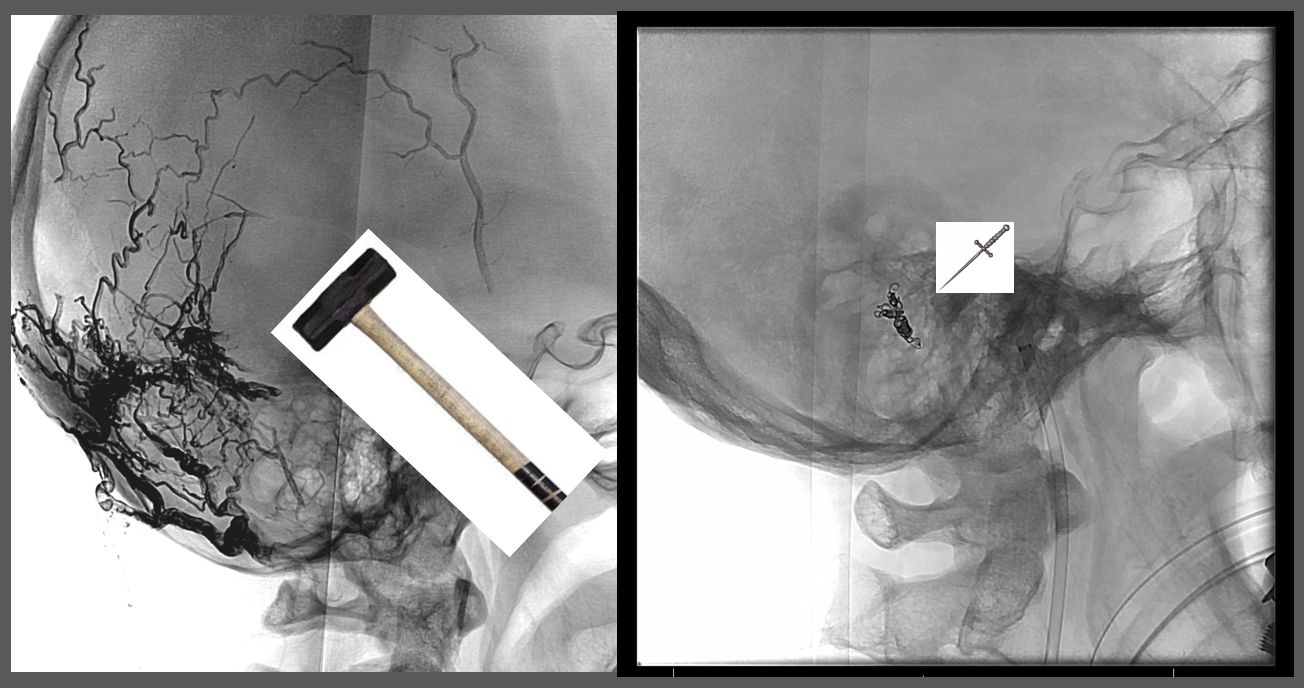
The answer is clear — keep the sledge in the baggage train — once in a while that’s the answer. But, carry the stiletto – it’s more comfortable, safer, and is usually plenty enough to get the job done.
Here is another example of this, in a patient presenting with pulsatile tinnitus
Angio shows some lateral tentorial arcade supply. The right sigmoid sinus is patent. Low grade.
ECA injection shows MMA and occipital supply, converging on a common channel (white arrows) that eventually empties into the very proximal sigmoid sinus, just beyond the jugular bulb. Notice how much thinner this channel is than the sinus itself.
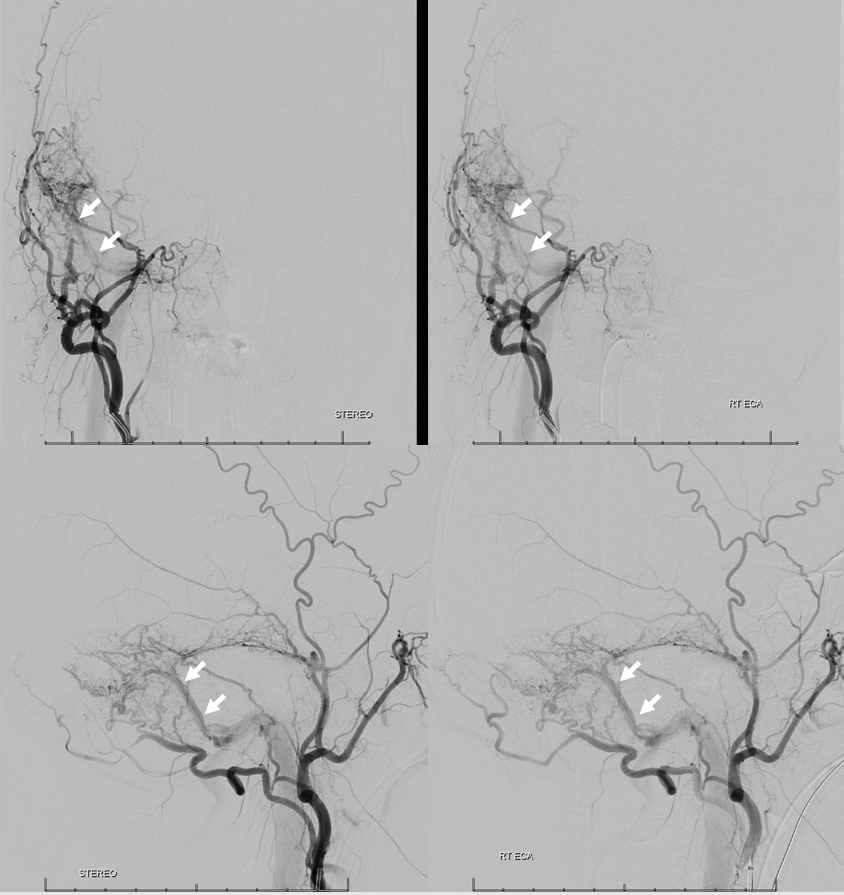
Selective occipital view, just for show
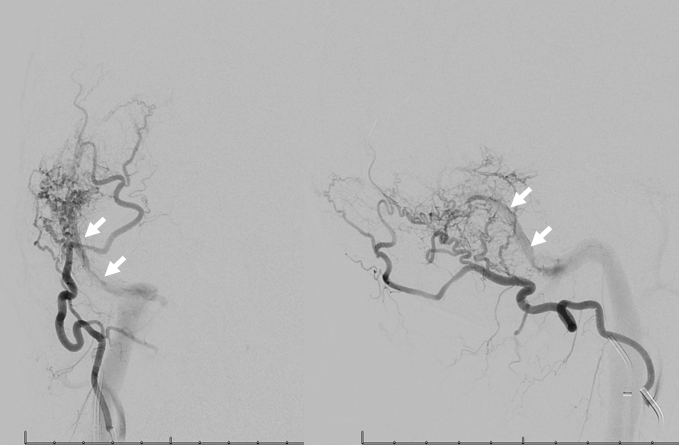
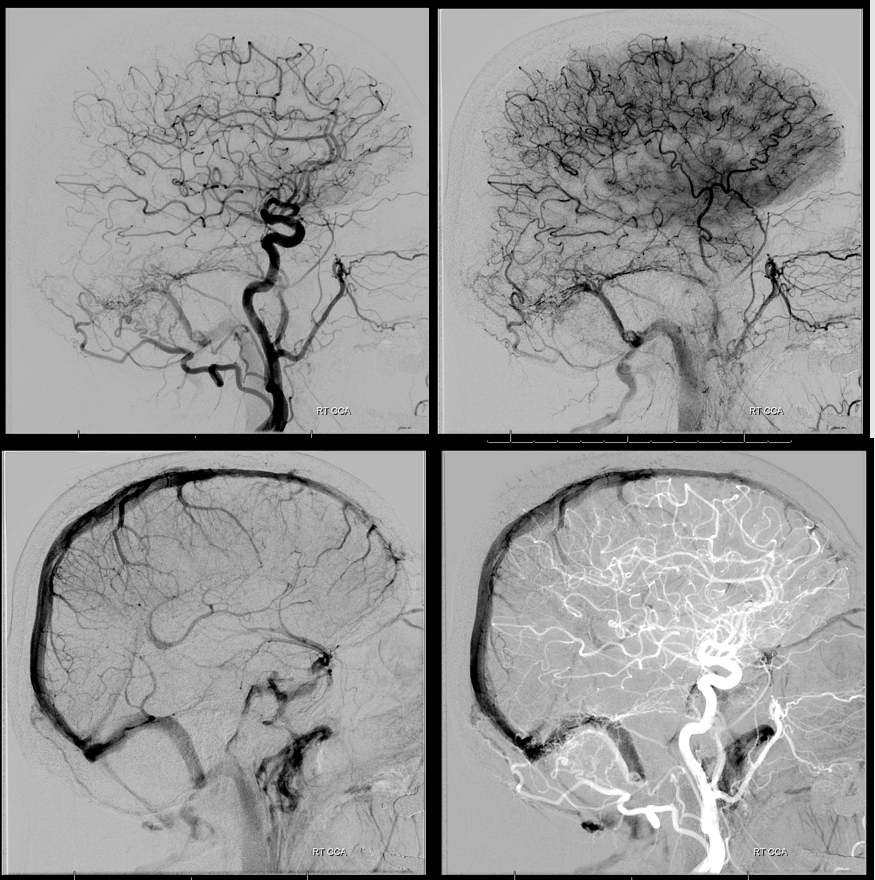
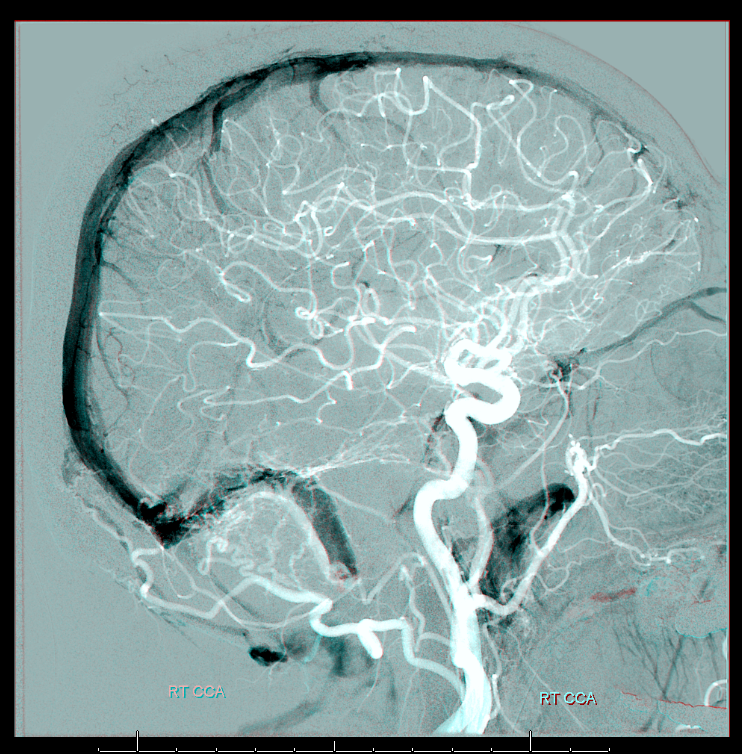
Common carotid injection, sequential images showing first opacification of the fistula channel (upper left image, arterial phase), sinus proper (lower left image, venous phase), and finally the double mask image with arterial phase mask, with channel is below sinus proper.
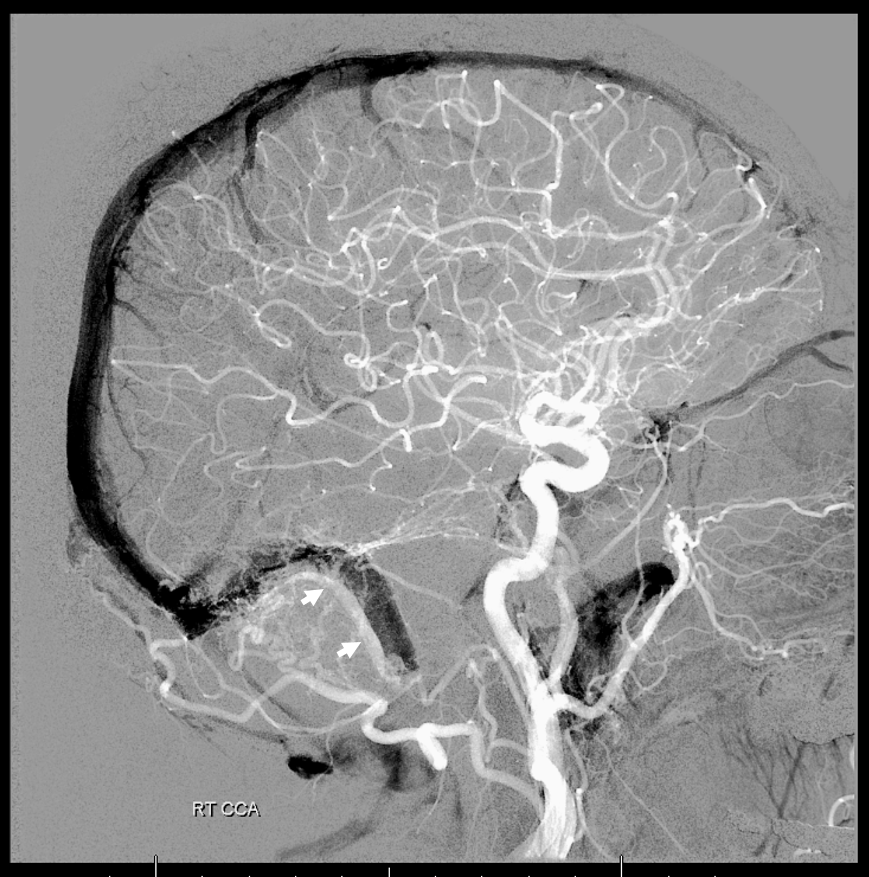
Magnified view, channel marked by white arrows
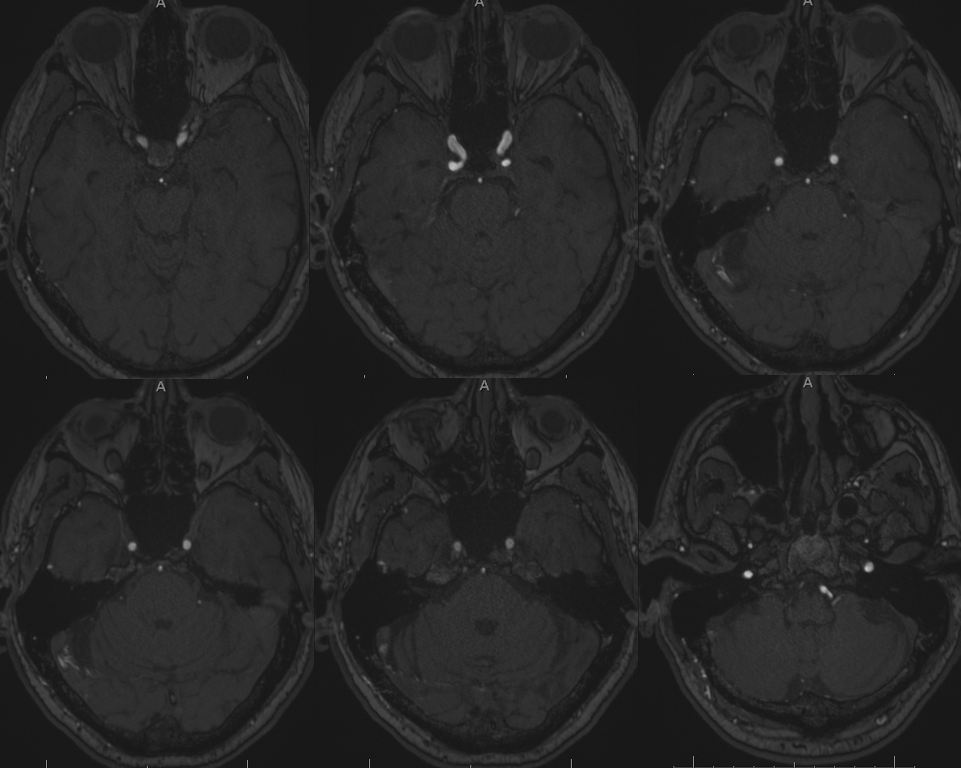
Dyna CT, same idea, face looking the other way
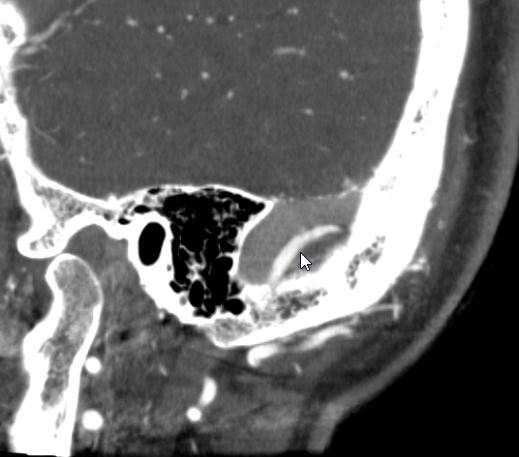
Scroll thru this DICOM set to see the channel
We place a Scepter balloon, from the venous side, into this channel.

Fistulogram, with balloon deflated
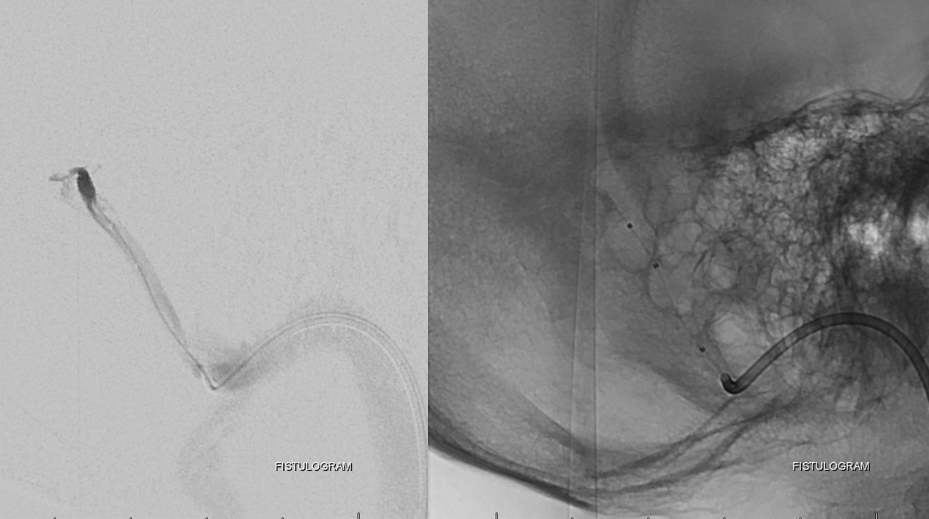
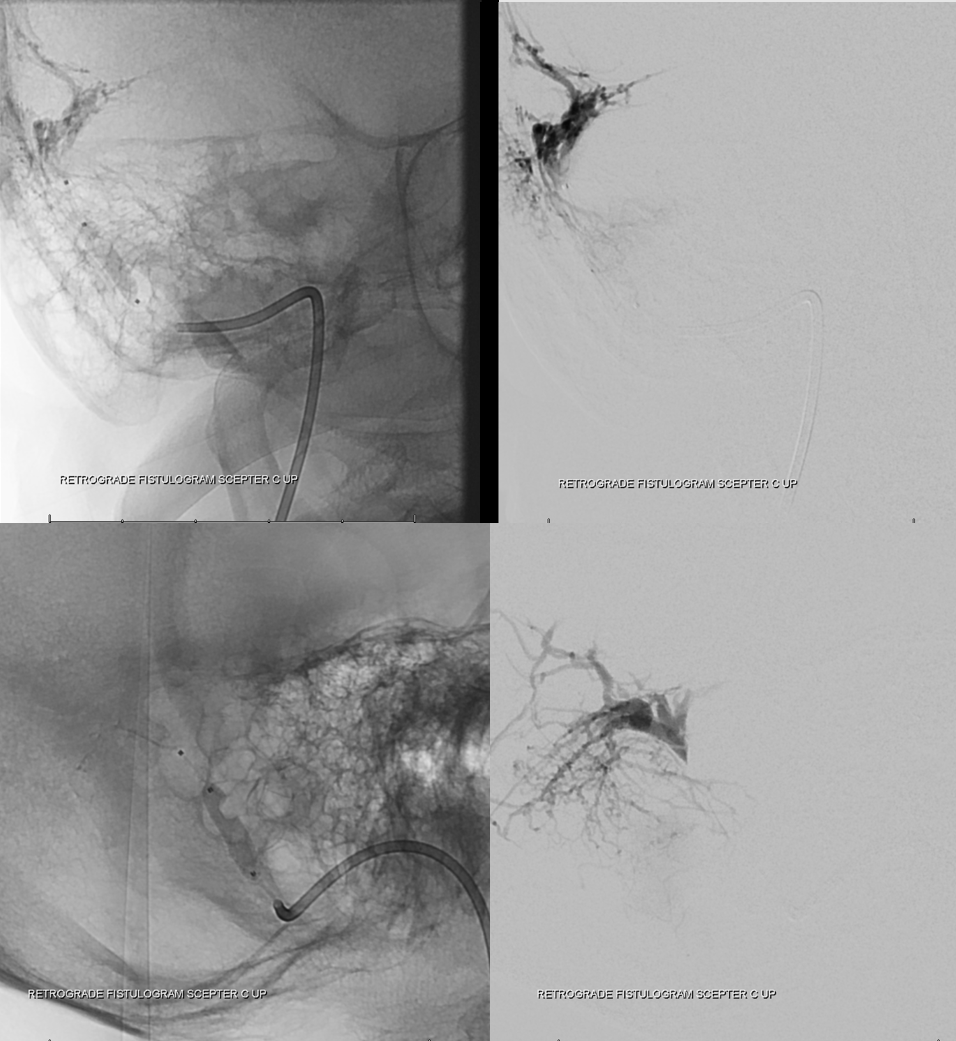
Balloon is inflated, occluding fistula outflow.

Injection of Scepter now retrogradely opacifies the myriad arteries feeding this fistula. See how many hundreds of tiny ones there are there. Thats why proximal embolization does not work. You have to close the common channel
Now we inject the ECA. With balloon still inflated, the fistula is closed, confirming our hypothesis that this channel is the final common fistula drainage pathway.
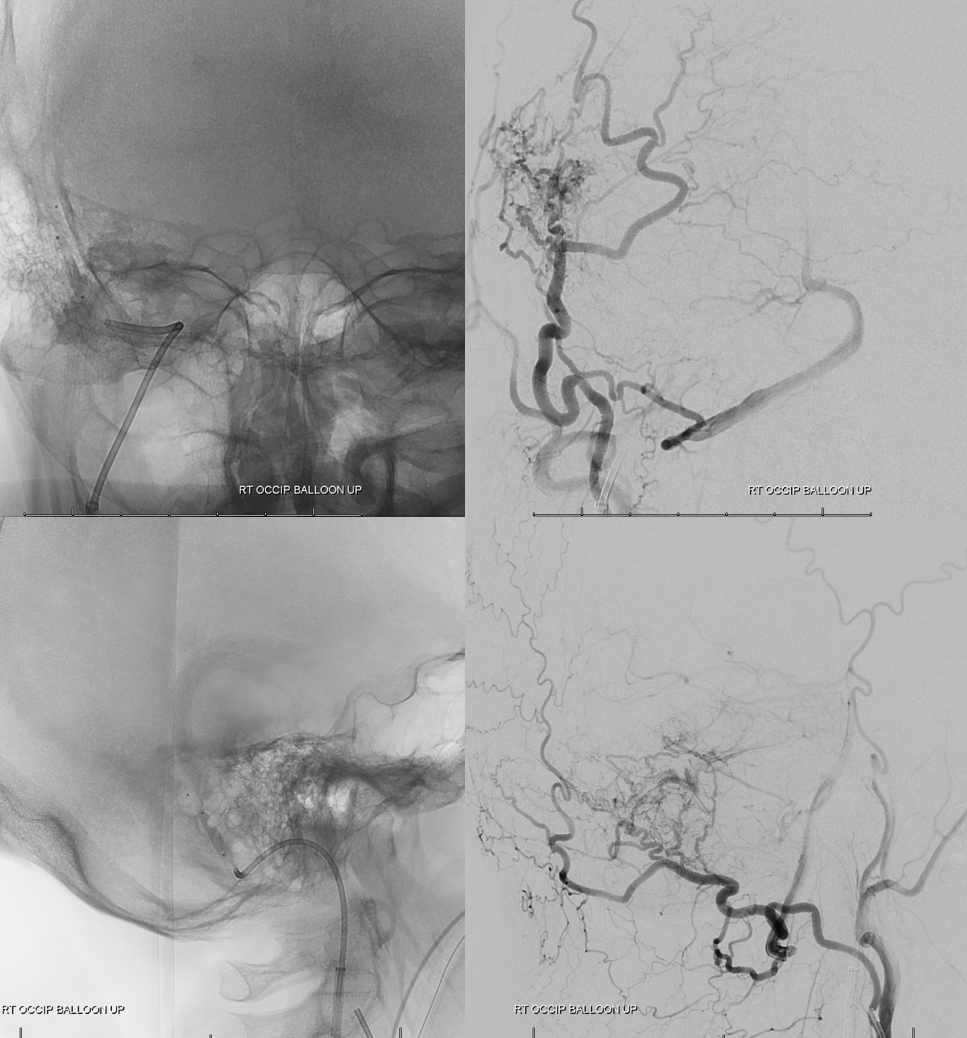
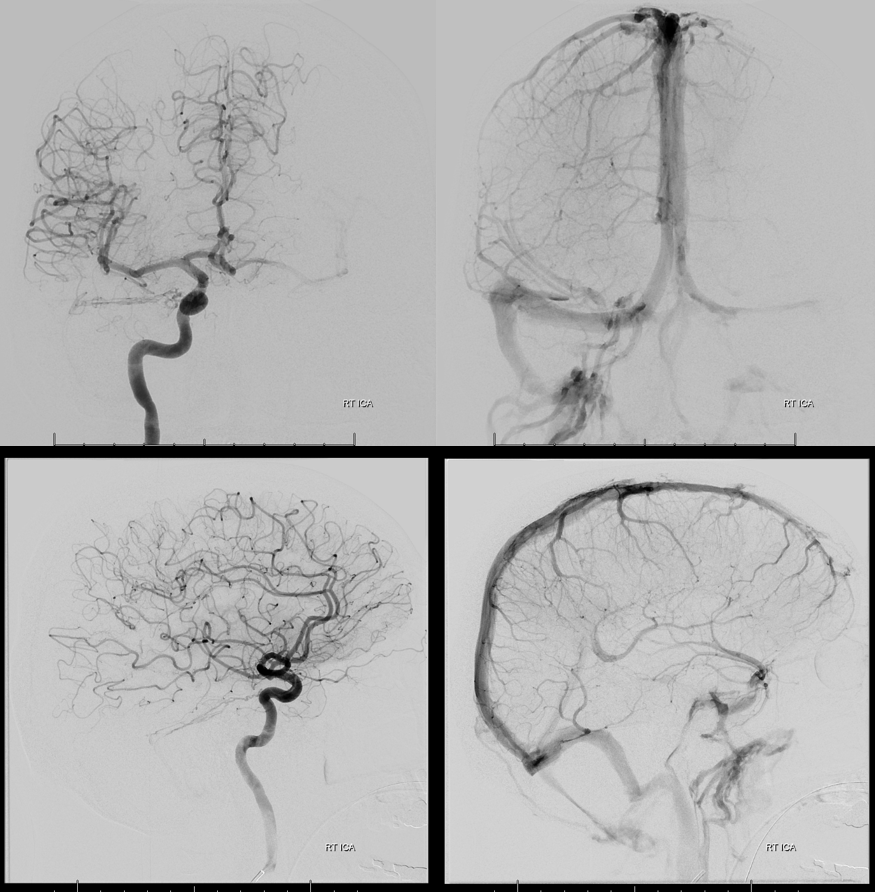
Now we keep the balloon inflated and fill the channel with Onyx. Post-embolization images below show no more fistula (ICA injection also showed no more lateral tentoral arcade supply). Why Onyx and not coils — why not? It works, and its cheaper than a few detachable coils.

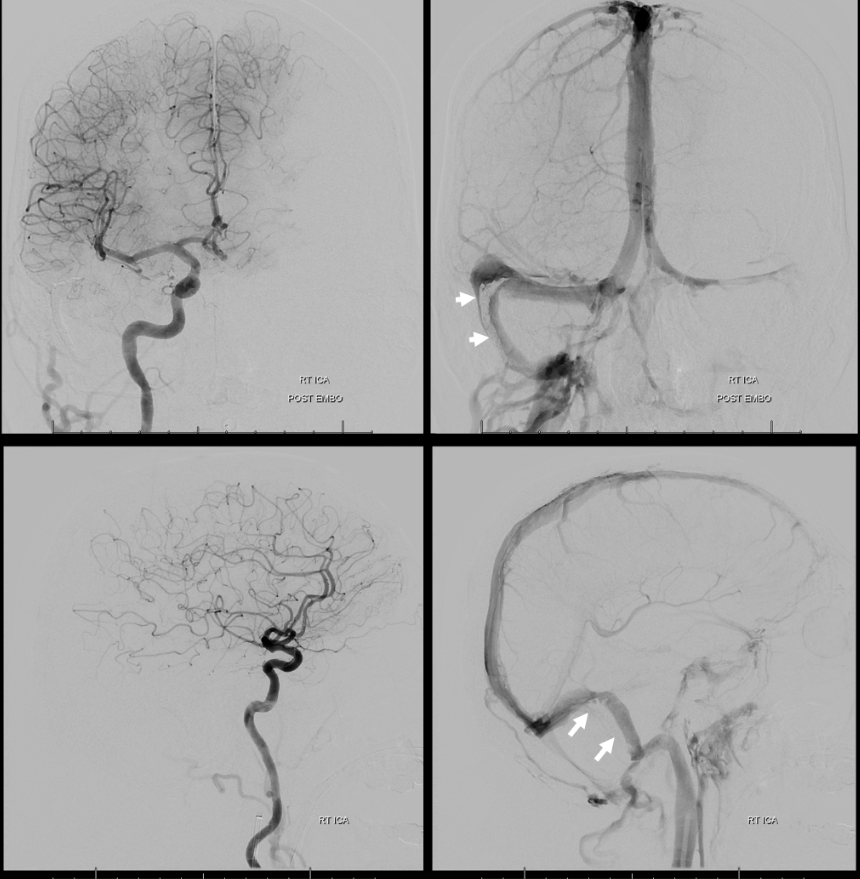
Post embo ICA injection, showing no supply from lateral tentorial arcade. Venous phase images show patent true right sigmoid sinus, with superimposed Onyx cast in frontal and lateral views (white arrows).
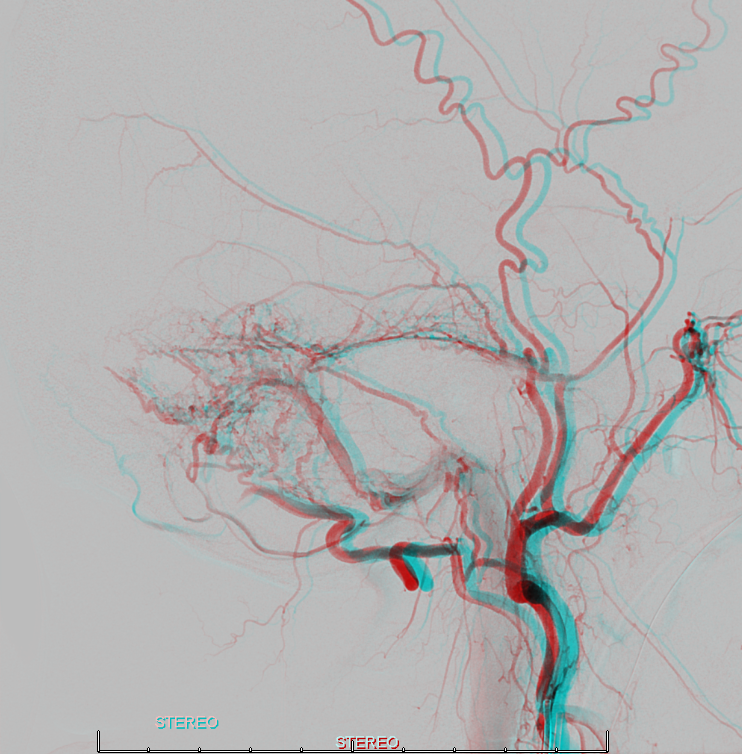
Anaglyphs!!!!


See other cases here:
Literature:
Mironov A. Selective transvenous embolization of dural fistulas without occlusion of the dural sinus. AJNR American journal of neuroradiology 1998;19:389-391
Piske RL, Campos CM, Chaves JB, et al. Dural sinus compartment in dural arteriovenous shunts: a new angioarchitectural feature allowing superselective transvenous dural sinus occlusion treatment.
Caragine LP, Halbach VV, Dowd CF, et al. Parallel venous channel as the recipient pouch in transverse/sigmoid sinus dural fistulae. Neurosurgery 2003;53:1261-1266; discussion 1266-1267
Shapiro M, Raz E, Litao M, Becske T, Riina H, Nelson PK. Toward a Better Understanding of Dural Arteriovenous Fistula Angioarchitecture: Superselective Transvenous Embolization of a Sigmoid Common Arterial Collector. AJNR Am J Neuroradiol. 2018 Sep;39(9):1682-1688