
What is that? It is a rare fistula between the epidural venous plexus and the epidural arterial arcade (also known as the retrocorporeal arterial arcade). The fistula drains retrogradely from the epidural venous pouch into spinal veins.
Many practitioners do not see a distinction between the supposedly very rare epidural spinal fistulas and the more common spinal dural fistulas. The difference, if in fact real, is mostly anatomic. Dural fistula shunt is located in the nerve root sleeve, while epidural one is in the epidural space. The end result however is the same — retrograde spinal venous congestion. Treatment options are also the same — endovascular or surgical.
In the end, we believe the distinction is real. Epidural fistulas do exist, and should be recognized as a distinct entity, even if practical management differences between the well-known dural type may be minimal.
Here is an example of one recently treated by Dr. Omar Tanweer
Gradient echo T2 MRI of patient with typical progressive lower extremity issues
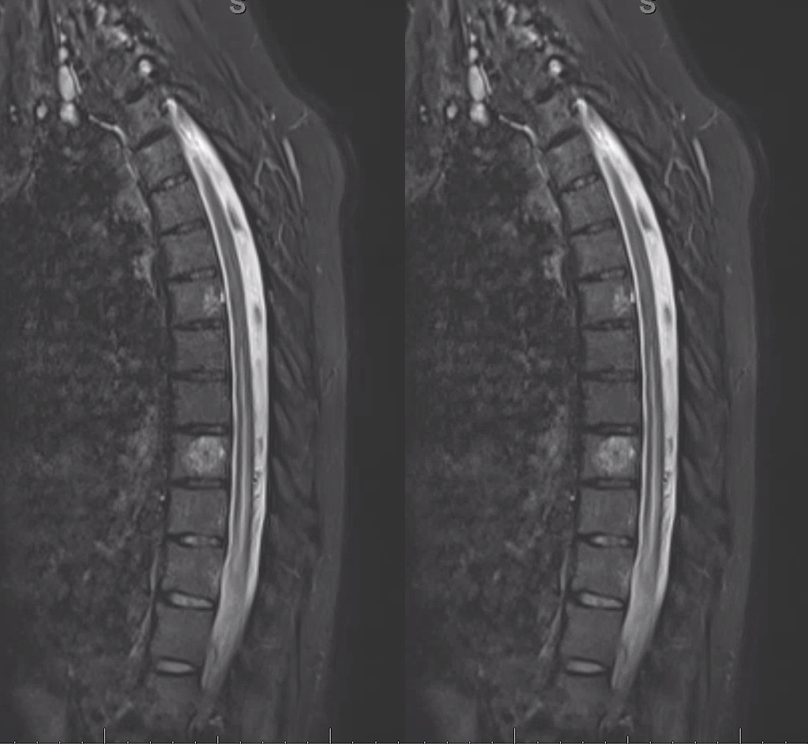
A volumetric SPACE T2 sequence is much better

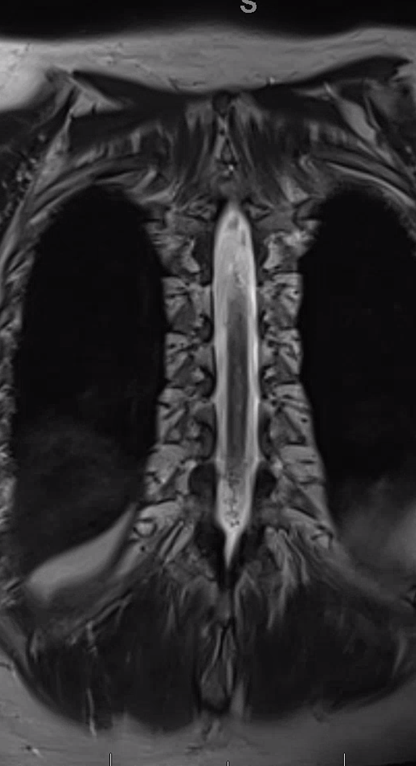
Coronal T2
Fistula predominantly supplied by left T2 segmental artery. Notice several unusual features. First, there is a rather unusual venous pouch present. Second, the fistula itself is at L3 level, while supply is from L2. Also unusual for a dural fistula
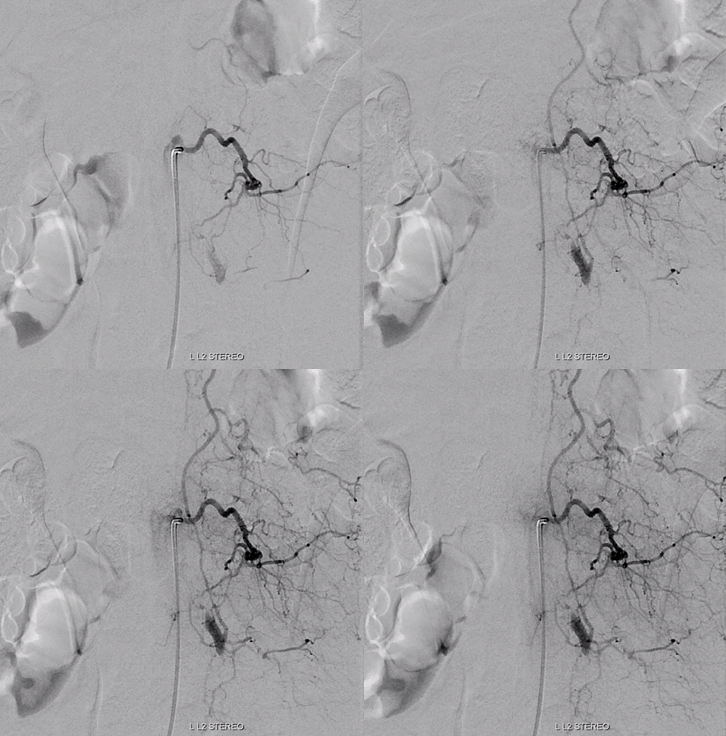
Left L3 supply, though closer to fistula, is relatively minor
Congestion of anterior spinal system is evident For a large anterior spinal like that, we should see spinal veins in venous phase (rightmost image). Nonvisualization of spinal veins is diagnostic of cord venous congestion
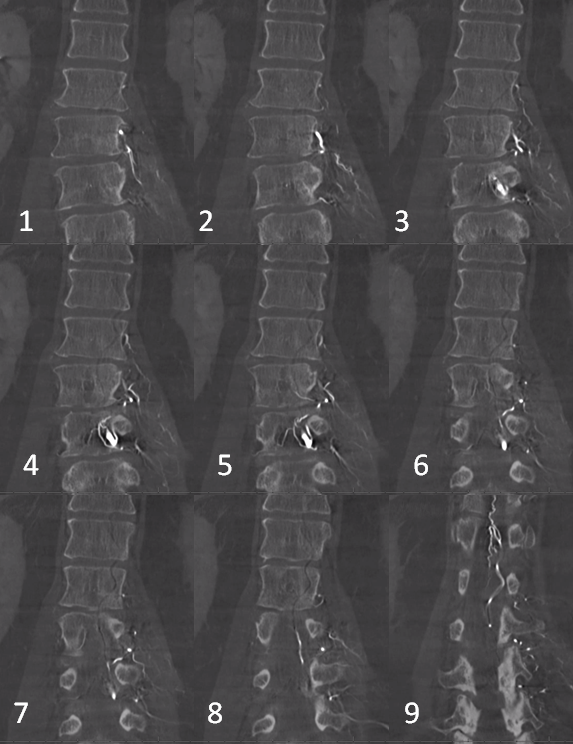
Dyna CT images
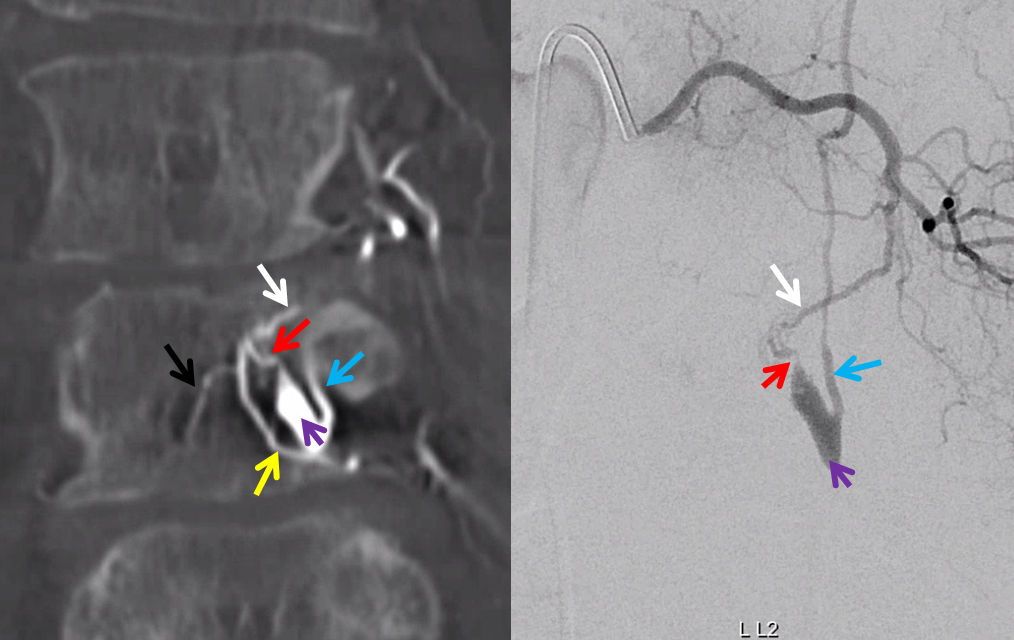
The angioarchitecture is not complicated. Fistula point (red arrow) is a hole between a branch of the ventral epidural arcade (retrocorporeal arcade) artery (white) and the epidural venous plexus (purple), with retrograde congestion of L2 radicular vein (blue) which then congests the spinal cord veins. See spinal arterial anatomy page for more info on epidural arcade — a diamond-like network of arteries bridging adjacent radicular arteries, both side to side and up-down. The portion heading to the left is marked by black arrow. The left L3 epidural arcade branch is yellow — the one that supplies fistula from L3 injection.
The hallmark of epidural fistula is that big venous pouch in the epidural space. What is strange is that normally epidural venous plexus, like any plexus, is extremely well connected (like Batson’s venous plexus). So how does this otherwise isolated sac drains just into a spinal vein? Unknown.
What is known is how to treat them — endovascular is just like dural fistula. In fact its easier since the catherizations are more straightforward and fistula location is not immediately near a possible radiculomedullary artery.
Here is a volume rendered image of the above Dyna CT. Same arrow colors
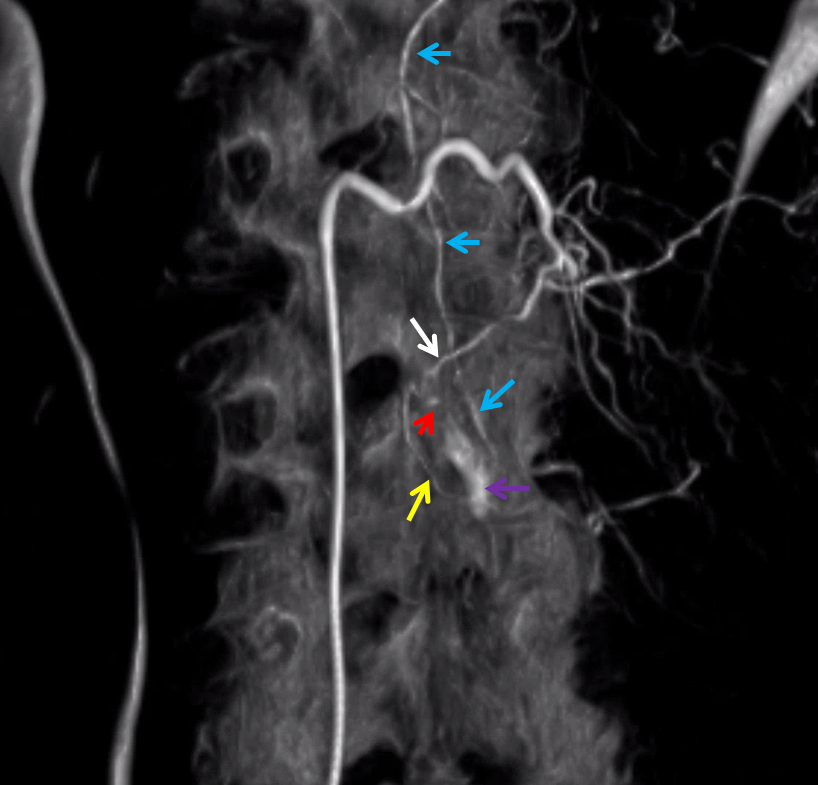
Cross-eye stereo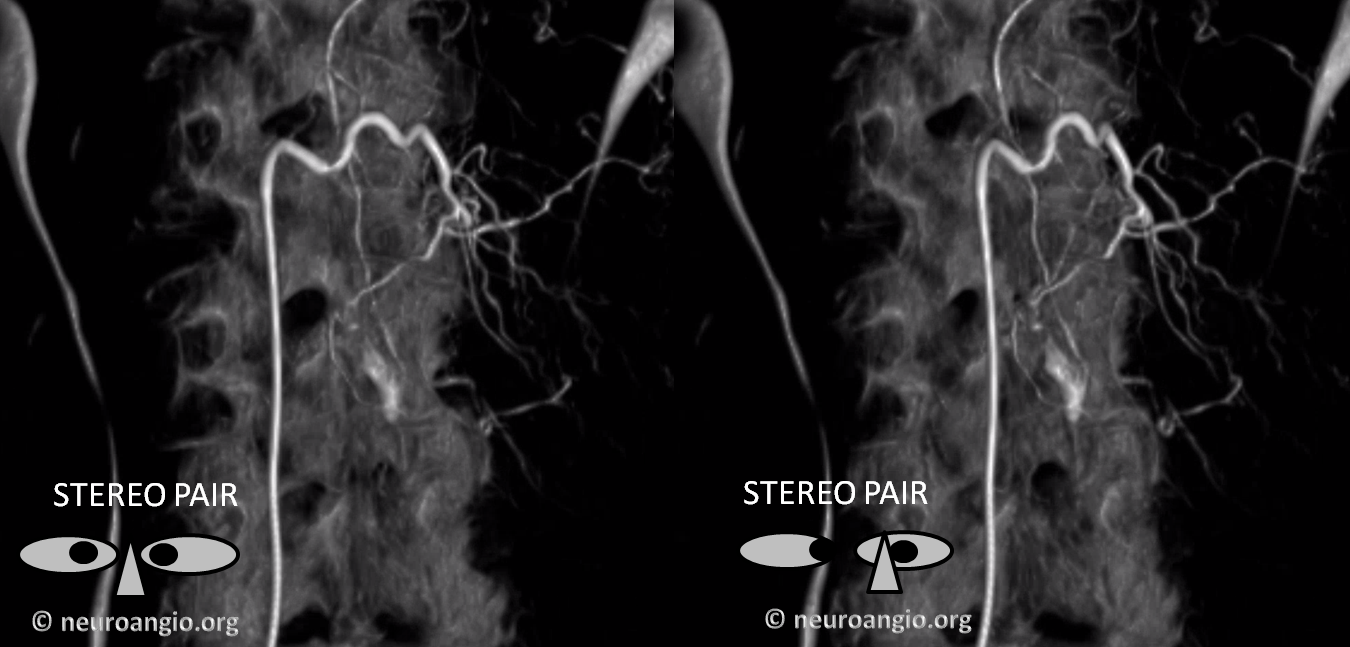
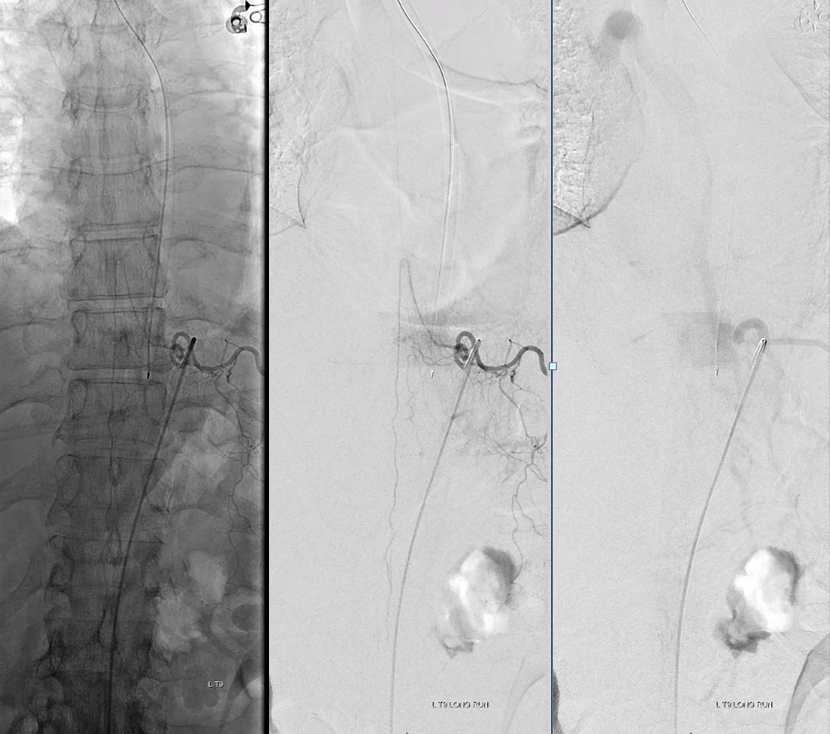
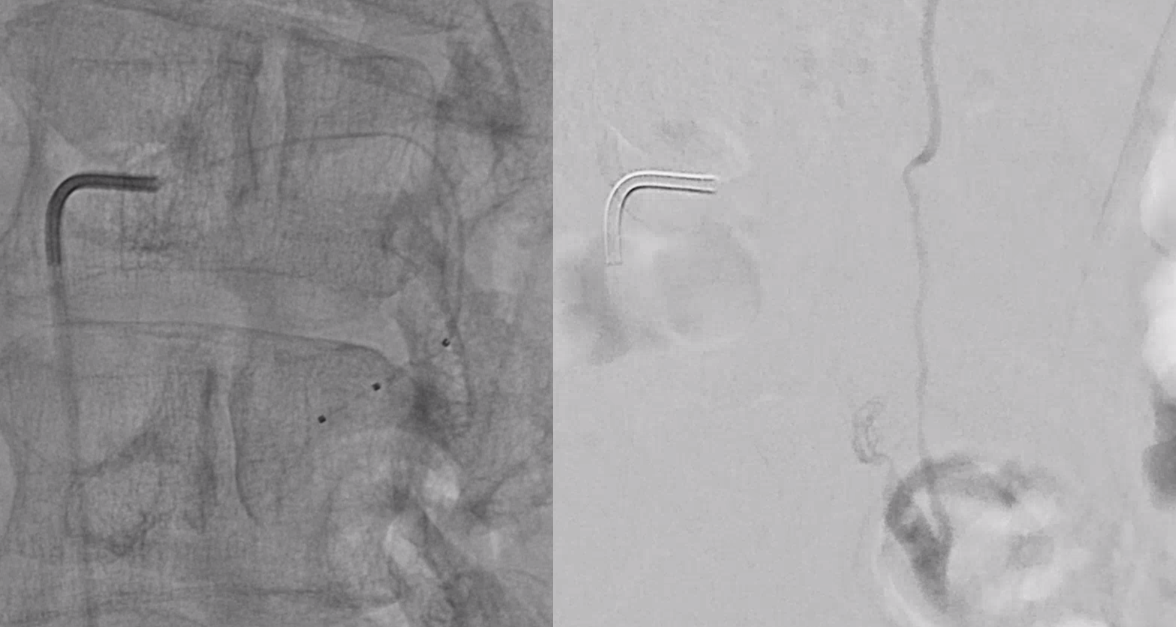
Scepter C microcatherization (see that Scepter in the characteristic 45 degree incline of the arcade. Scepter is inflated to make sure there is flow arrest.
Onyx fills the pouch and proximal spinal vein. Probably some of it extended into the nearby plexus more medially or ruptured into the epidural space — not a problem at all. Excellent Onyx penetration is due to use of Scepter.
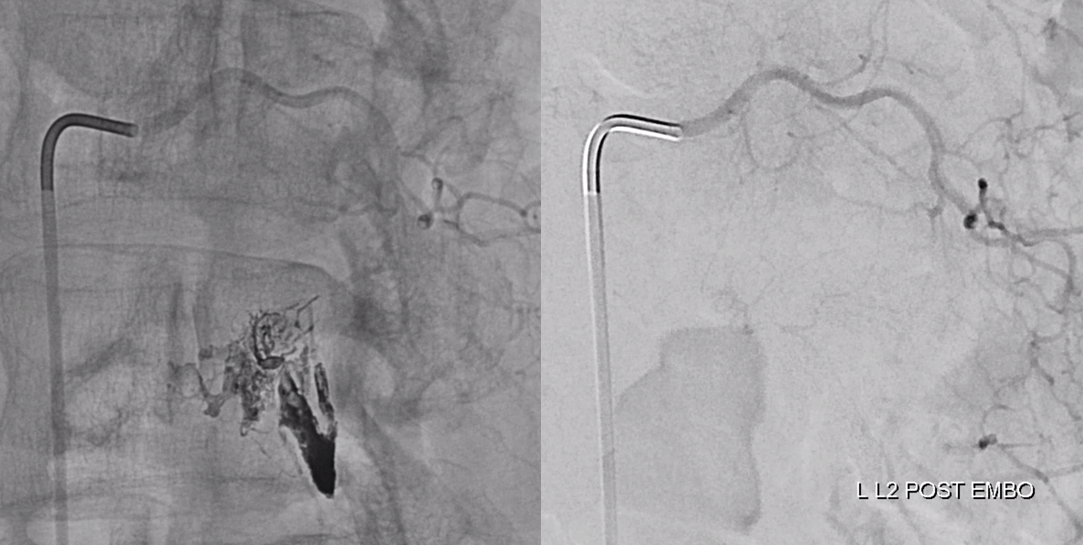
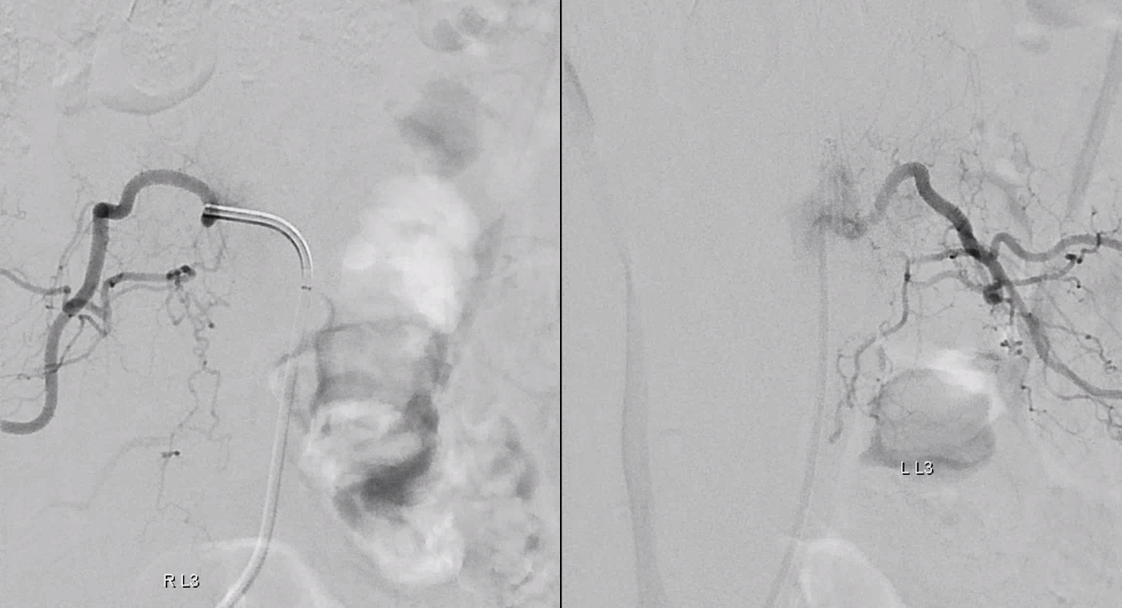
Control injections require looking at nearby levels for possible reconstitution. Especially left L3
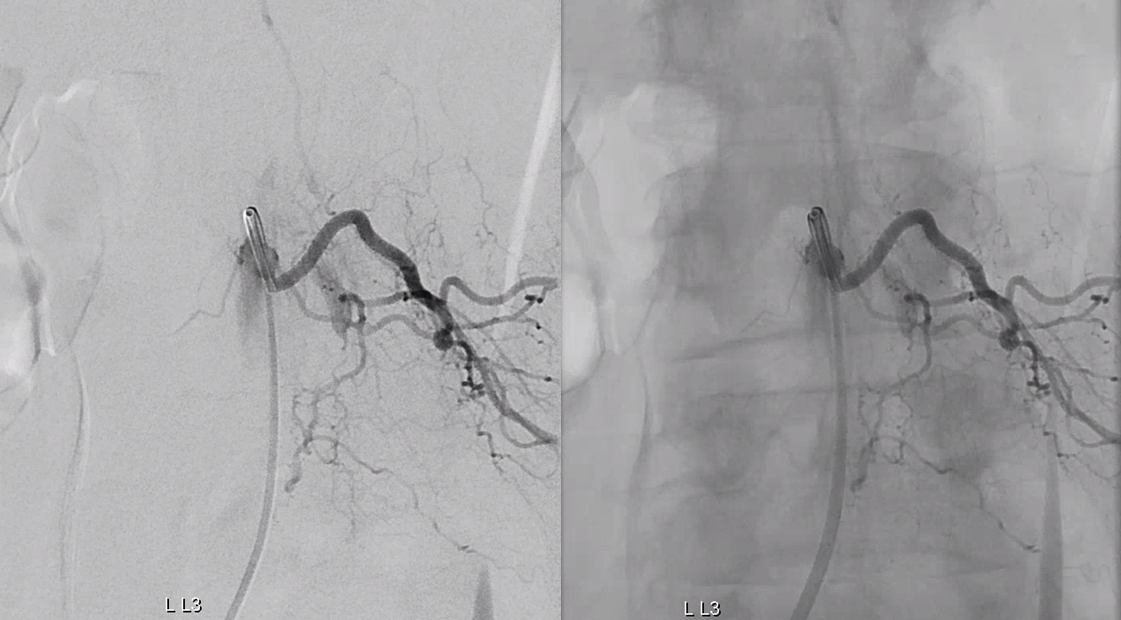
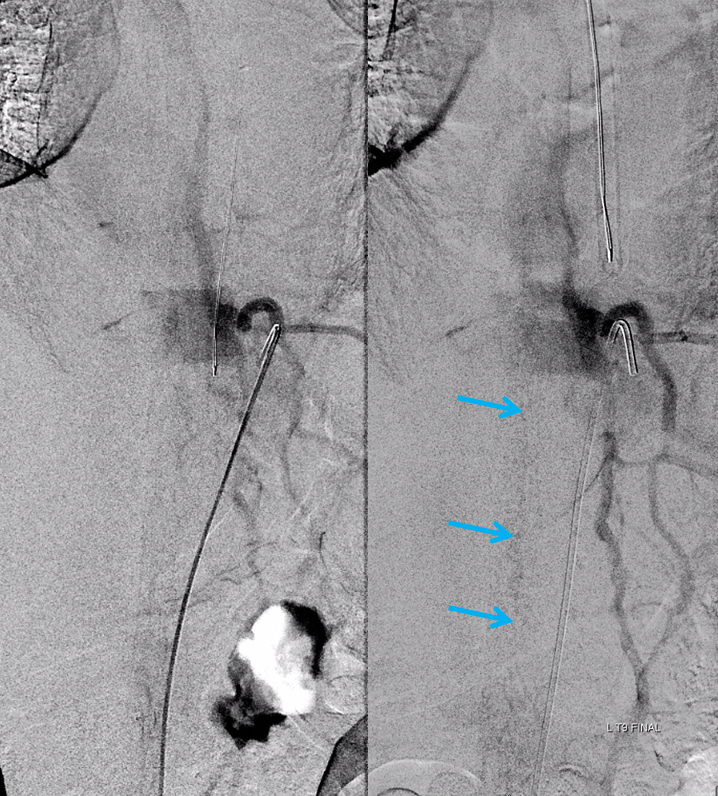
Finally, nice example of improved venous congestion. Now the spinal veins can be seen in the venous phase of Adamkiewicz injection. Can u see them?

Pre-embo on left, post on right. Veins are back in venous phase of anterior spinal injection.
See Spinal Epidural Fistula Page for more info