
A case of spinal pial fistula looking very much like dural one… even though they are not the same
Pial fistula is a shunt on the surface of the cord. Whether pial fistula is just a really small spinal AVM is not exactly clear. Fistula-looking angiograms many times look more like an AVM in surgery. However, both are totally different from a dural fistula.
Patient presents with years of progressive low back and leg pain, lower extremity paresis, and bladder dysfunction. For several years relies of straight cath. Now using wheelchair. Co-morbidities include extensive peripheral vascular disease due to smoking
MRI looks completely indistinguishable from a dural fistula

A spinal angiogram was done — illustrating exactly how not to do it. Awake patient, tilted body, no labels, no venous phase

When catheter is not optimally engaged in the vessel, it does not count

In all, 5 levels were not injected and nothing was found. A high resolution MRI was done however 1 month later to look for fistula level. The images are very nice
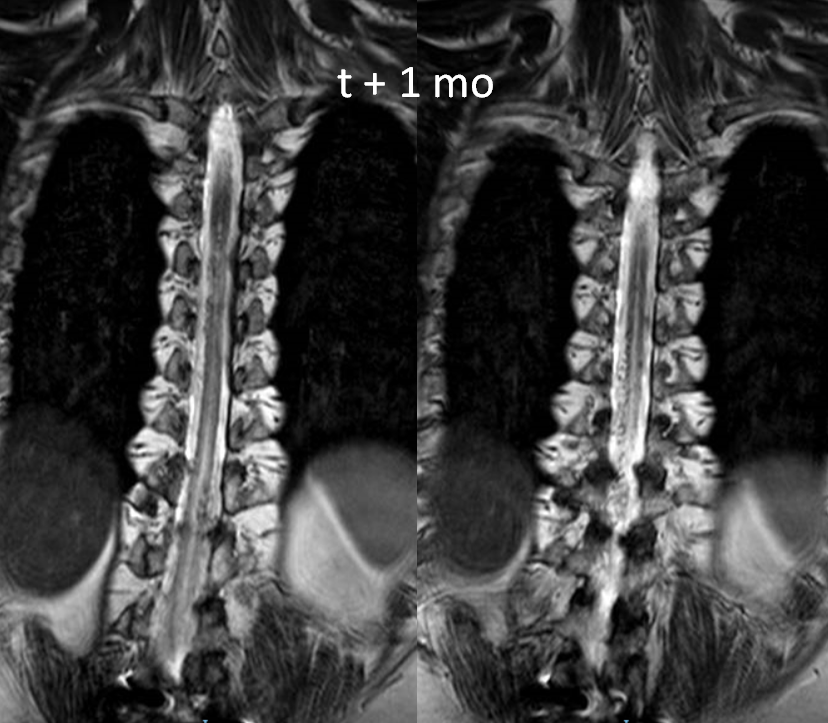
Sagittal shows extent of venous congestion

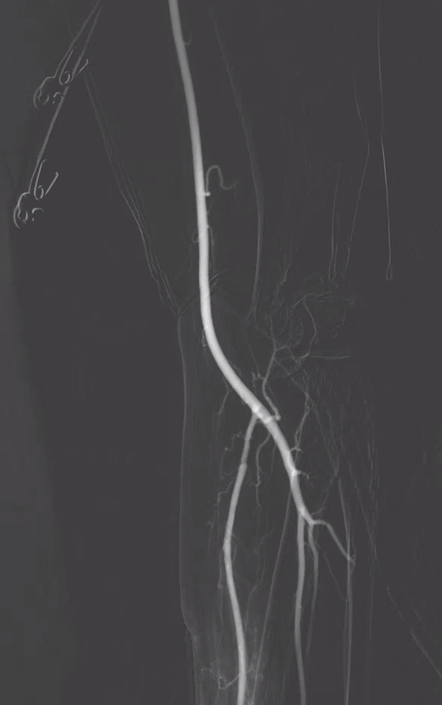
Another spinal angiogram was then done, and again nothing was found. The image below was correctly interpreted as anterior spinal artery. No venous phase images of this injection were done

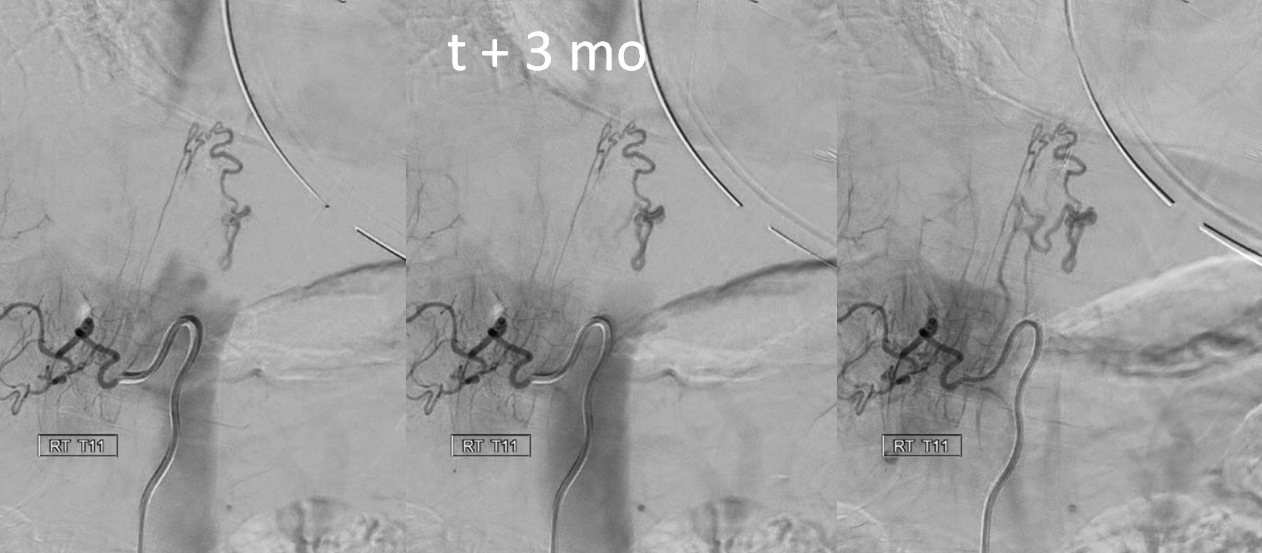
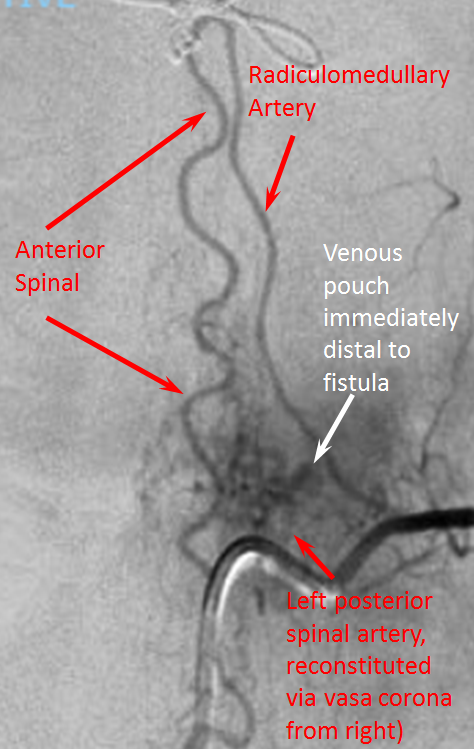
Finally, the patient came to a place that knows how to do spinal angiography, and very quickly a shunt is identified from right T11 level
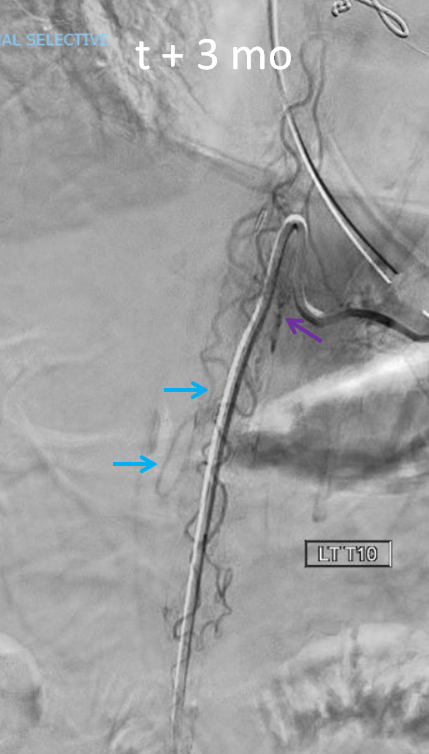
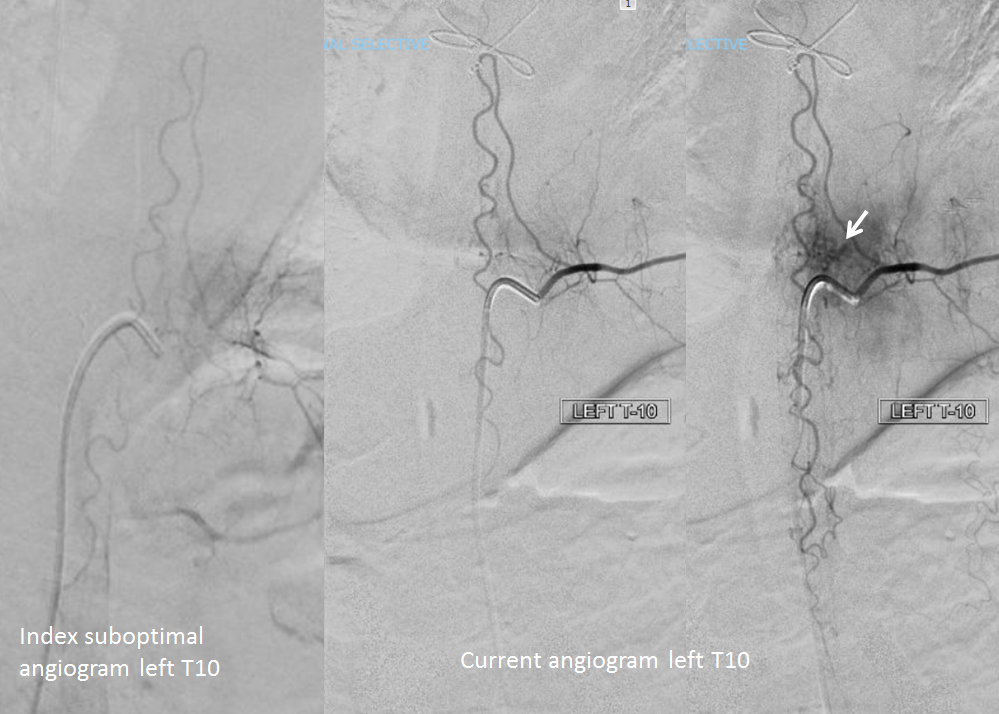
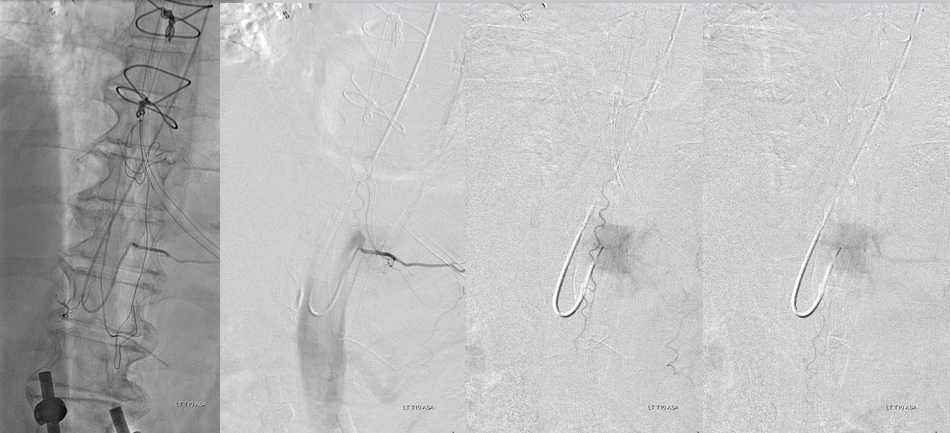
A better image of left T10 level shows that anterior spinal is in fact not normal. There is a shunt just medial to the catheter tip (purple arrow), and an early vein is visible (blue arrows).
An attempt is made to embolize from right T11 position (which supplies the fistula via radiculopial artery) using Onyx. It does not reach.

The patient transiently improves, then worsens again. MRI 1 mo after embolization

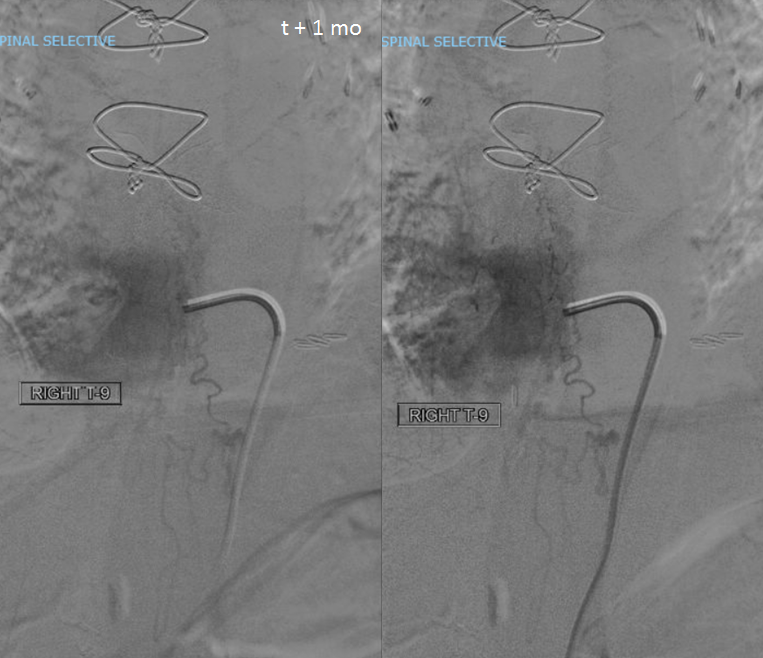
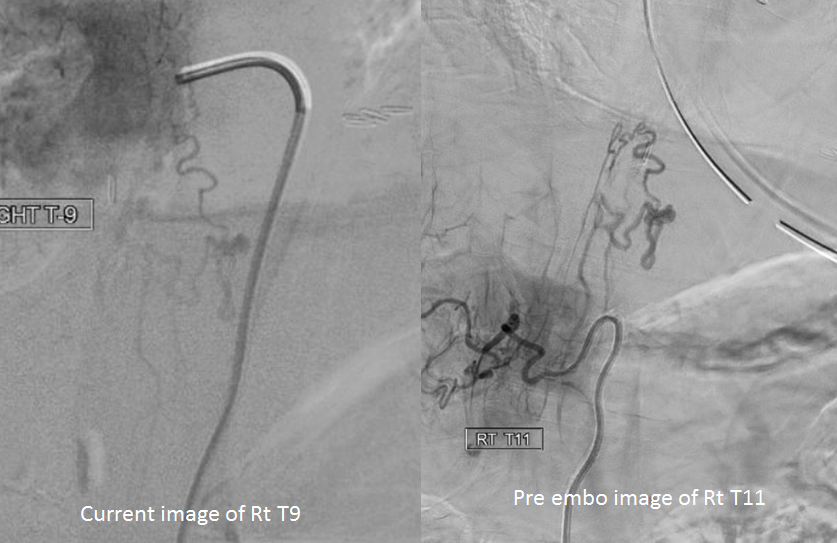
4th time is charm. A definitive spinal angiogram is done. The fistula is now reconstituted from Right T9 level (post prior proximal T11 embo)
Current and prior images for comparison
anterior spinal continues to supply fistula (arrow on proximal venous pouch)
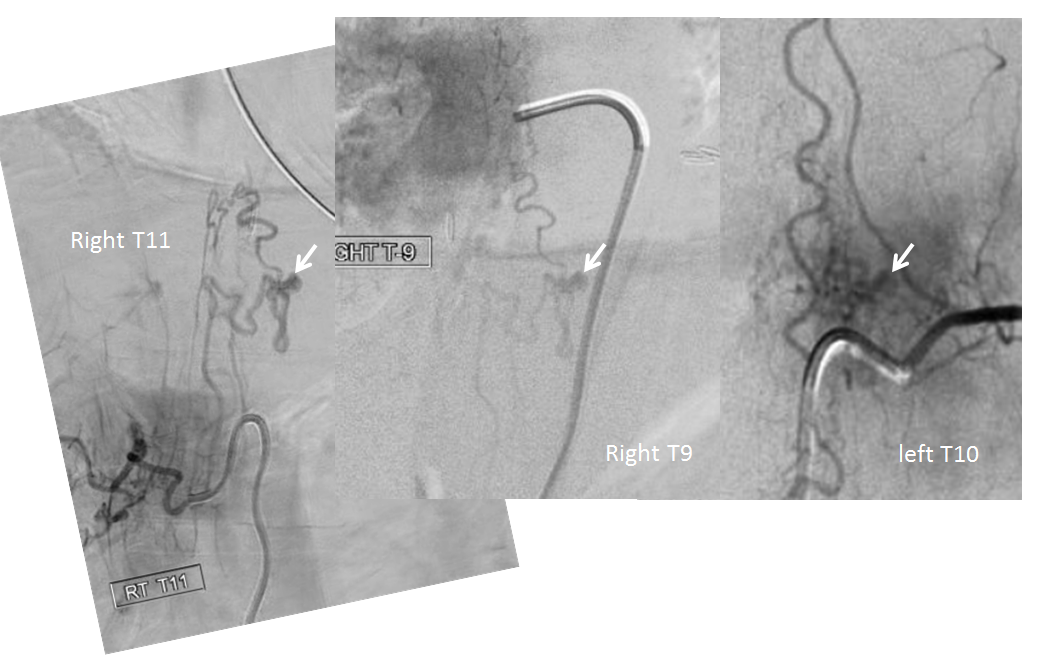
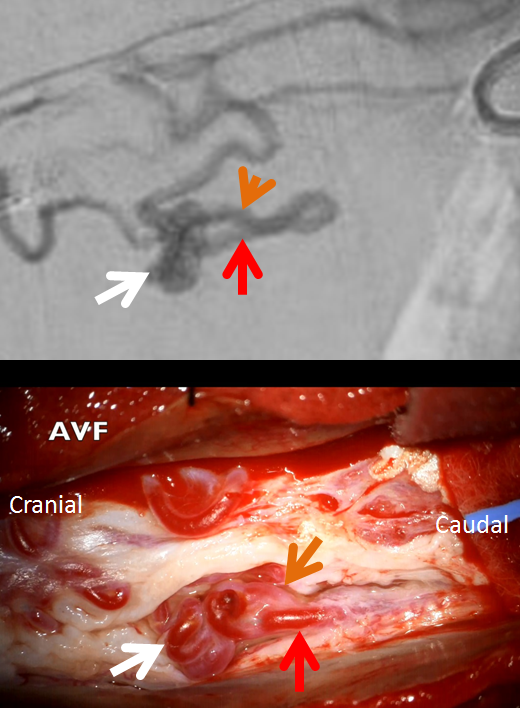
Putting it together — this is a pial fistula with predominant posterior spinal artery supply. Even though fistula is on left side, dominant supply is coming from right posterior spinal vessels — previously right T11, now right T9. The anterior spinal artery gives supply, also minor. Arrow points to venous pouch/aneurysm just distal to fistula.
So why this clinical presentation? Most pial fistulas and spinal AVMs do not cause global cord venous congestion. The outflow is usually directed into some nearby radicular vein and out of the spinal canal. Most of them present with either hemorrhage, some kind of steal phenomenon, or mass effect.
In this case, all venous outflow was directed into spinal cord veins with no nearby outlet — exactly like a dural fistula. This, combined with surface location of fistula and lack of MR-identifiable nidus led to initial misdiagnosis.
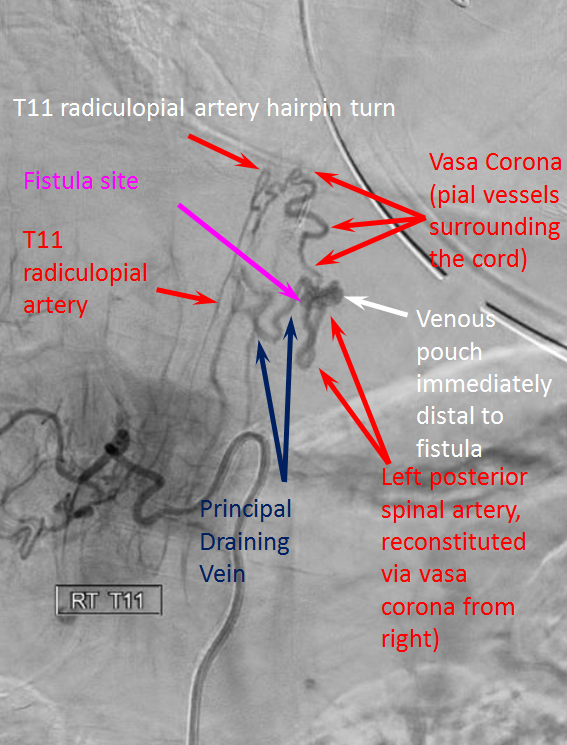
No safe endovascular route is available. Fistula was treated by surgical resection. Image below shows corresponding structures
Intraoperative angiogram (and neuro monitoring) are must-haves. Angio can be done via radial approach

Conclusions: Excellent case to show importance of good angiographic technique and appreciation of spinal vascular anatomy
See Spinal Pial Fistula Page for more