
Talk about controvercial. When a carotid goes down, either there is a stroke or there is not. If not, then you keep it closed. Right? Usually yes. But not every time. Medicine is art and science — beware of doctors (and people in general) that will never do anything different as much as of those that never play by the rules.
History is a multi-year CTO presenting with a recent deterioration.
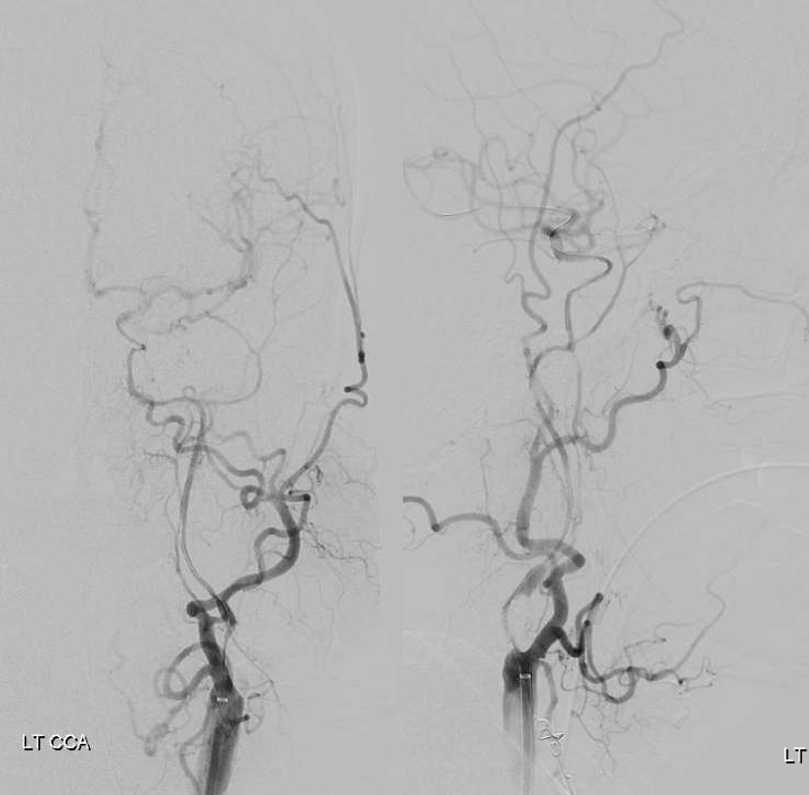
Angio — small ACOM, bad left A1. Delay of left ACA compared with right, and left MCA compared with PCA. Seems legit…
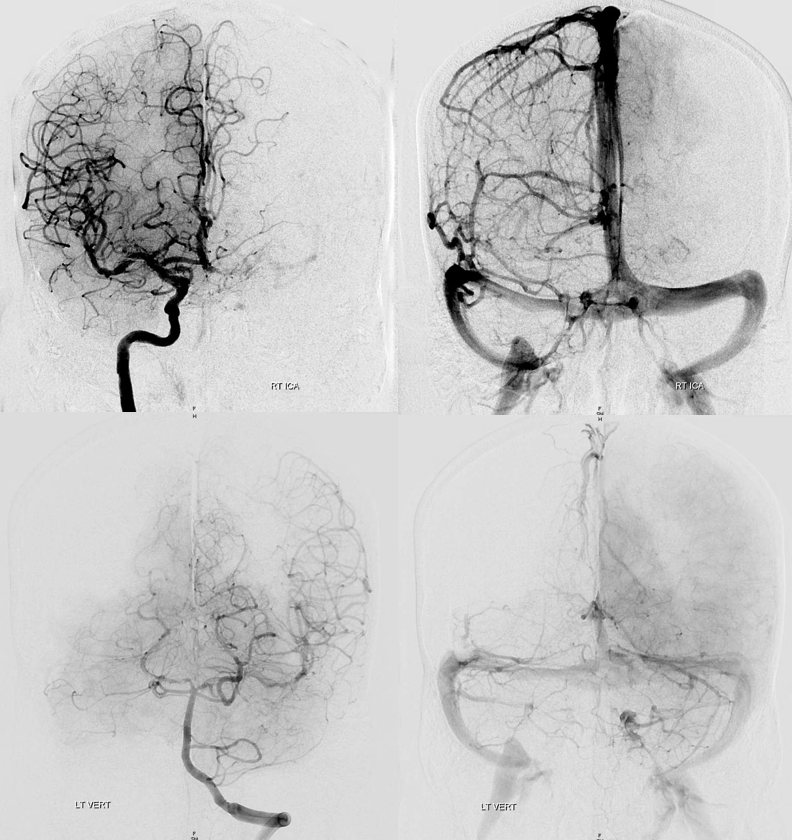
The problem is a stenosis of the main COW collateral at the P1 segment.
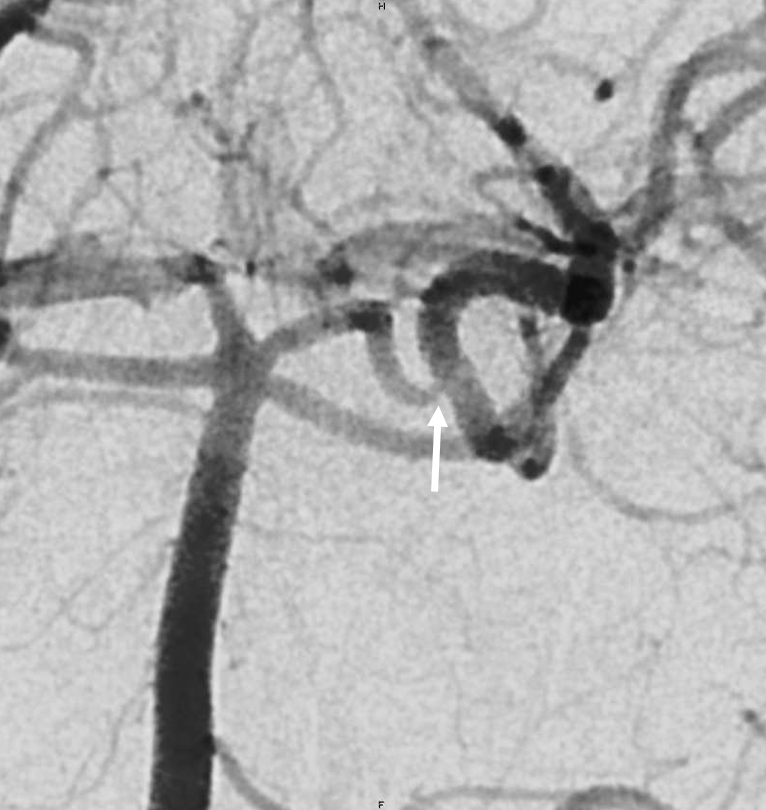
Usual ophthalmic reconstitution. But wait, is there more?
See something?
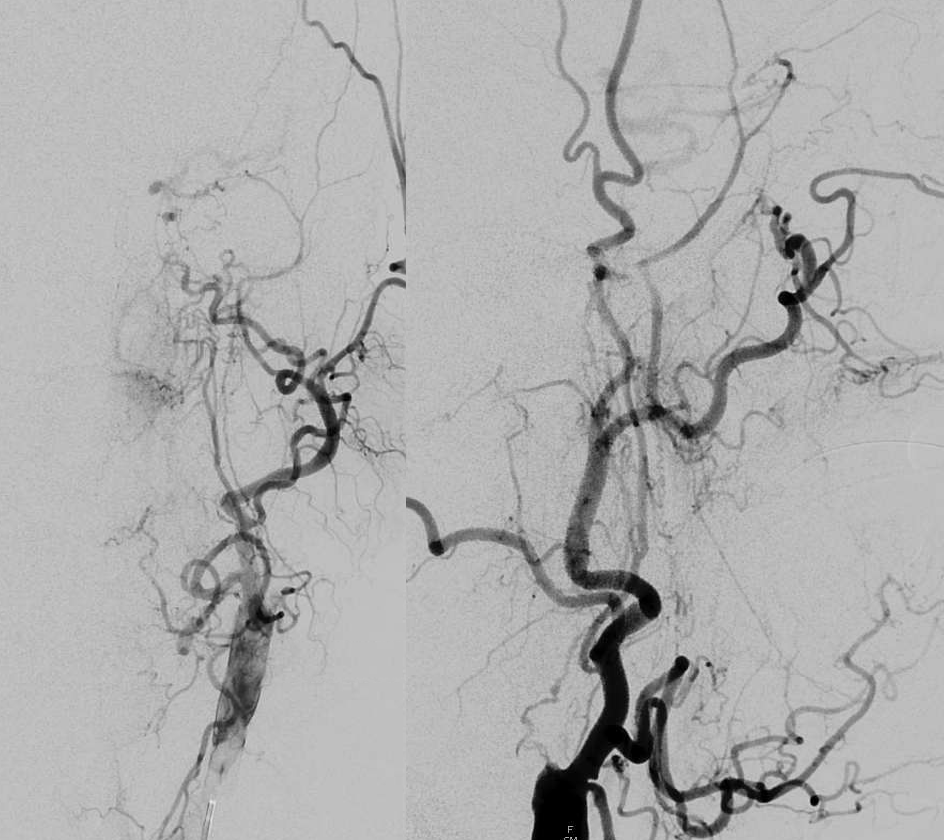
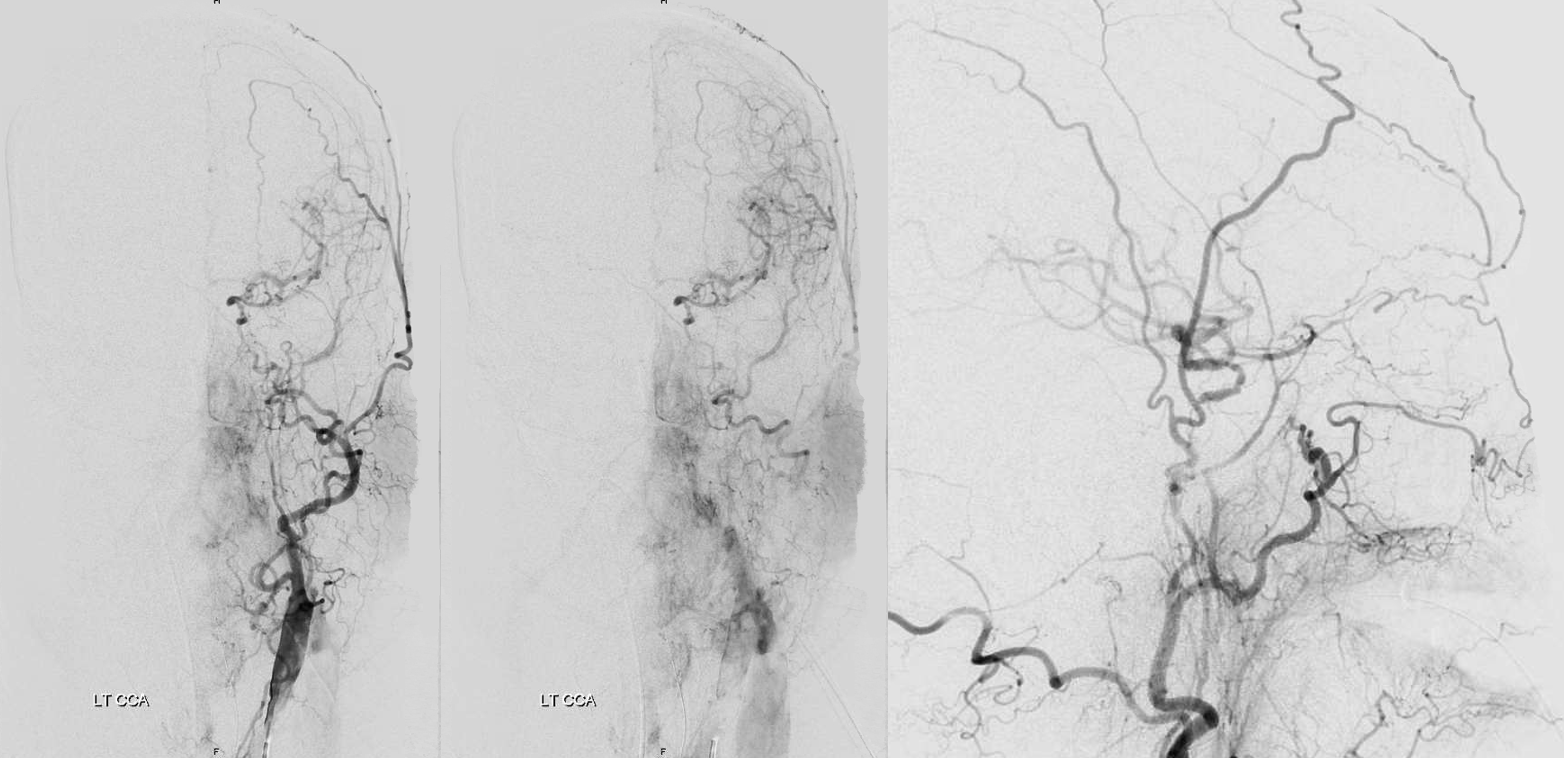
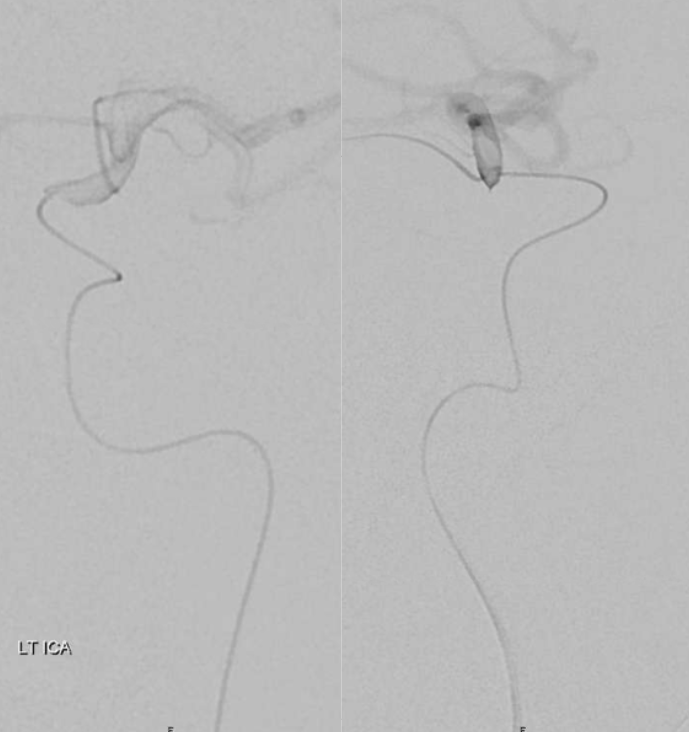
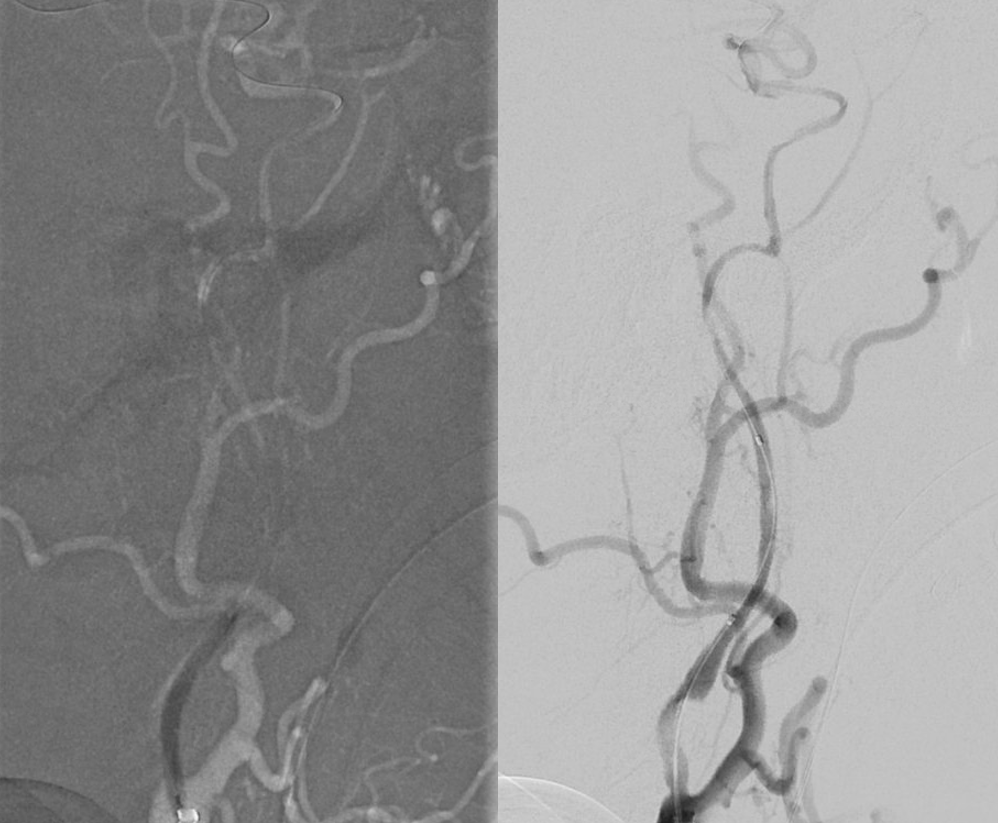
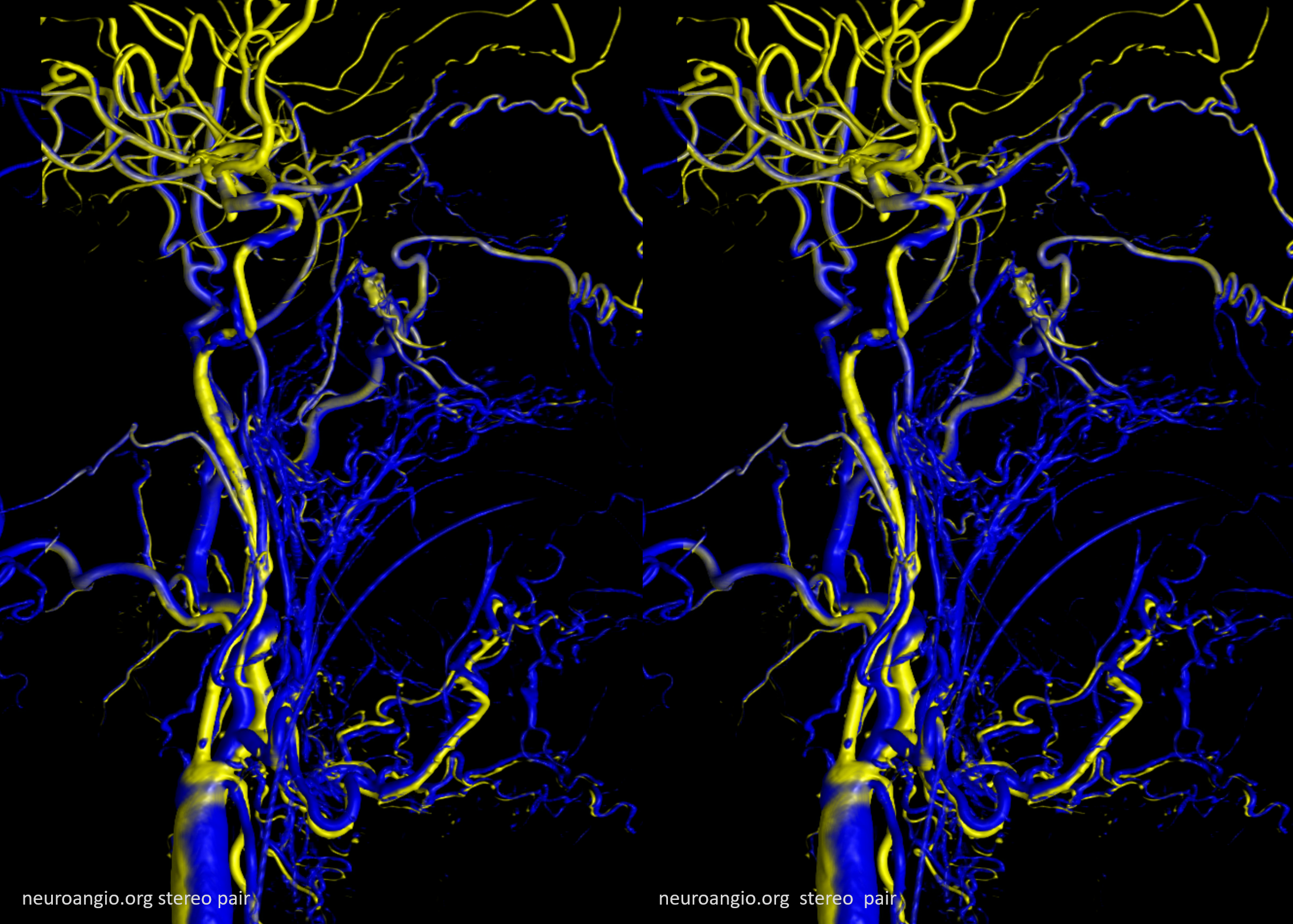
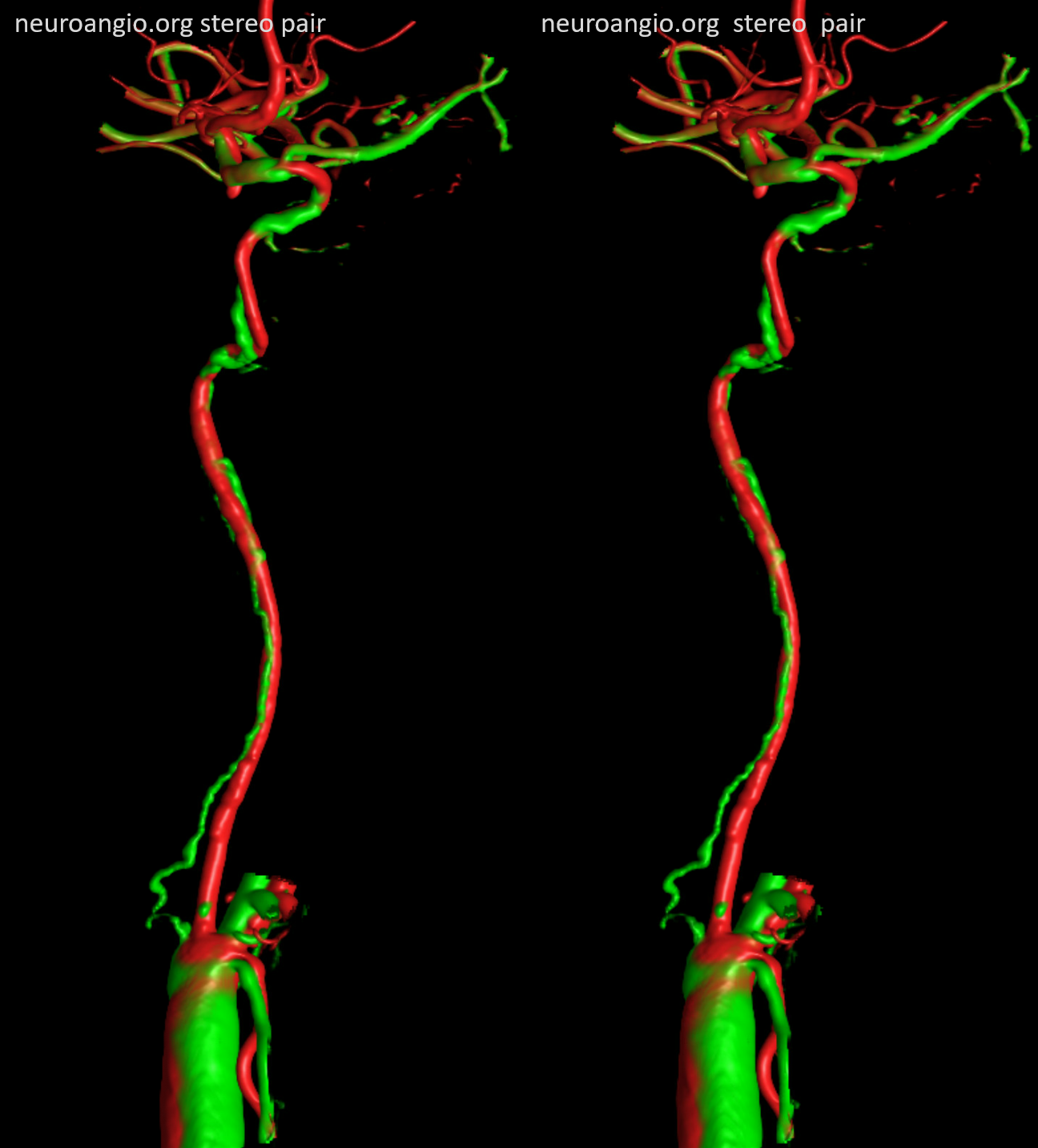
What is the tortuous artery following ICA from the stump?
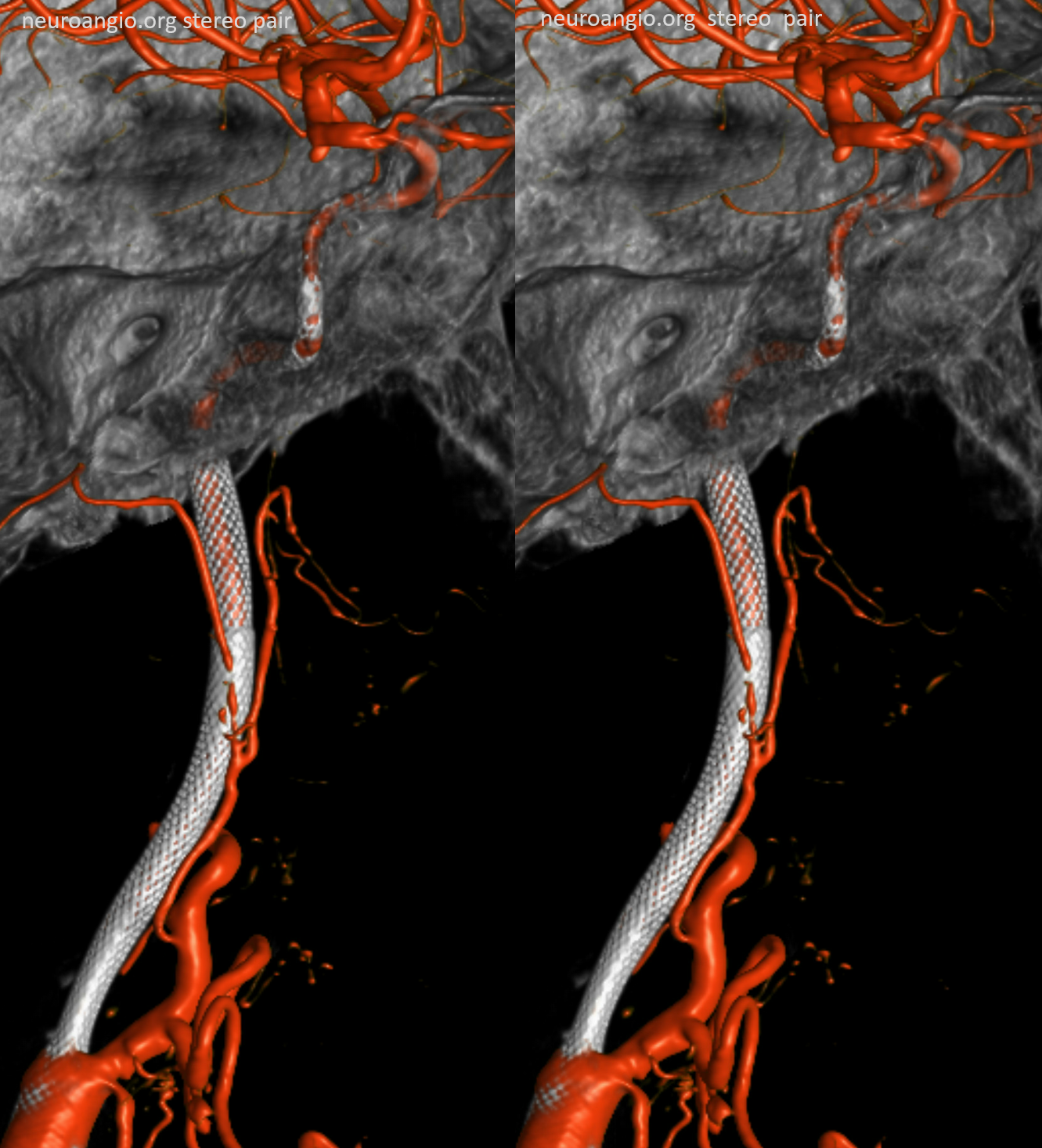
Vasa Vasorum — see CTA above. Channel in wall of the ex-ICA. Good thing is that it joins the ICA proper at the cavernous segment which is extradural. Safer to get there.
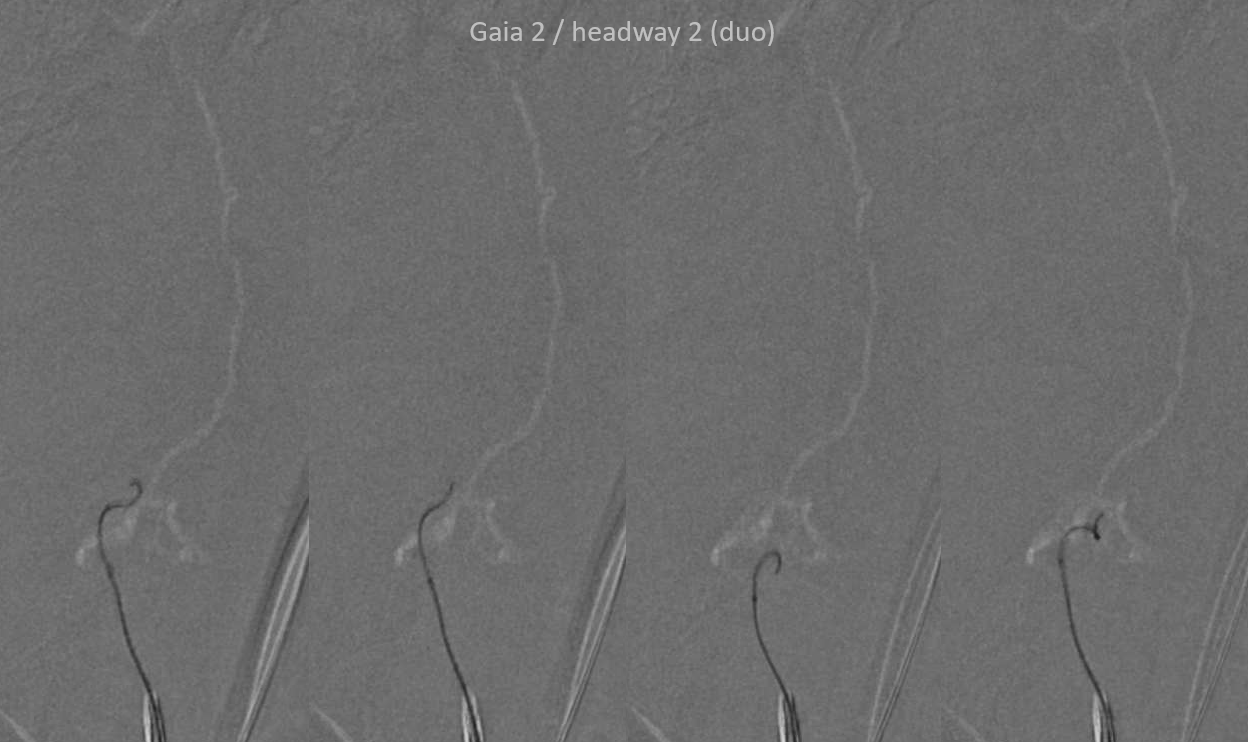
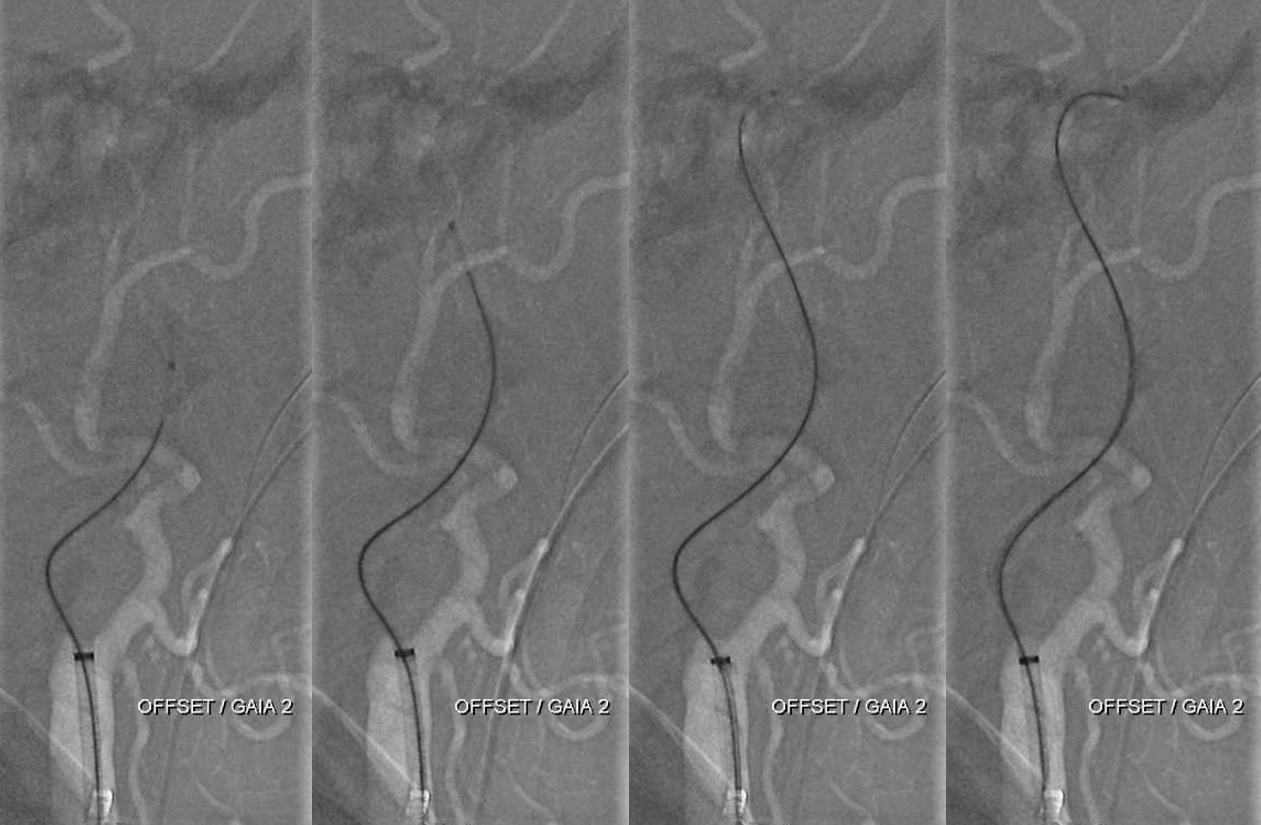
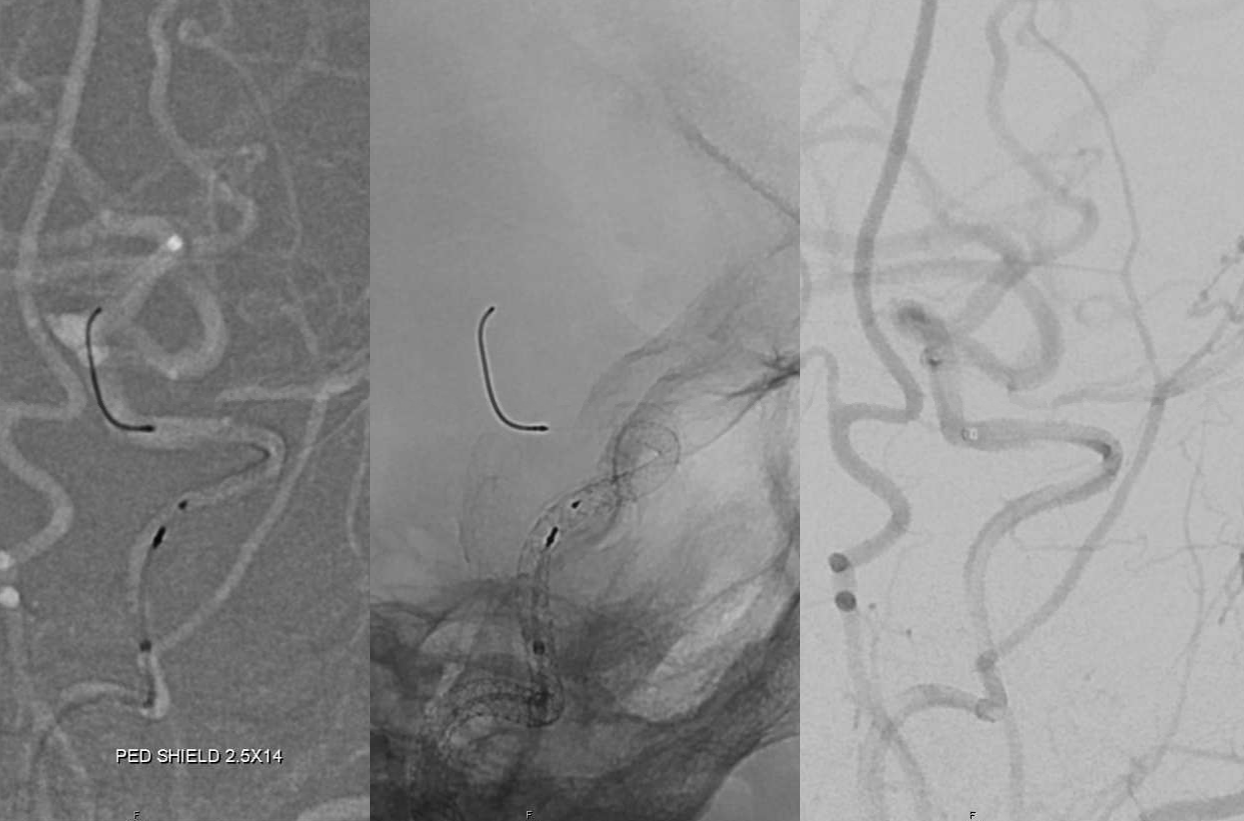
How did we get into the vasa vasorum. With help of the Gaia wire — specifically designed for CTOs, used in cardiology and peripheral work. This is Gaia 2
More Gaia work below…
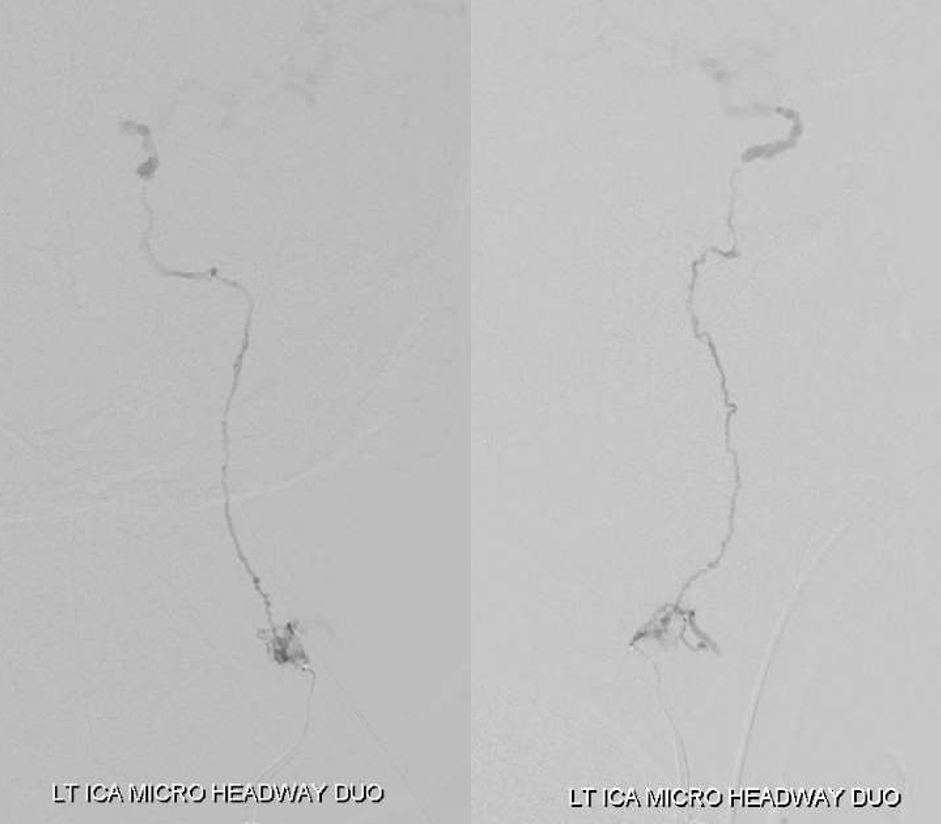
Great — now we lost the vasorum… Its not so simple

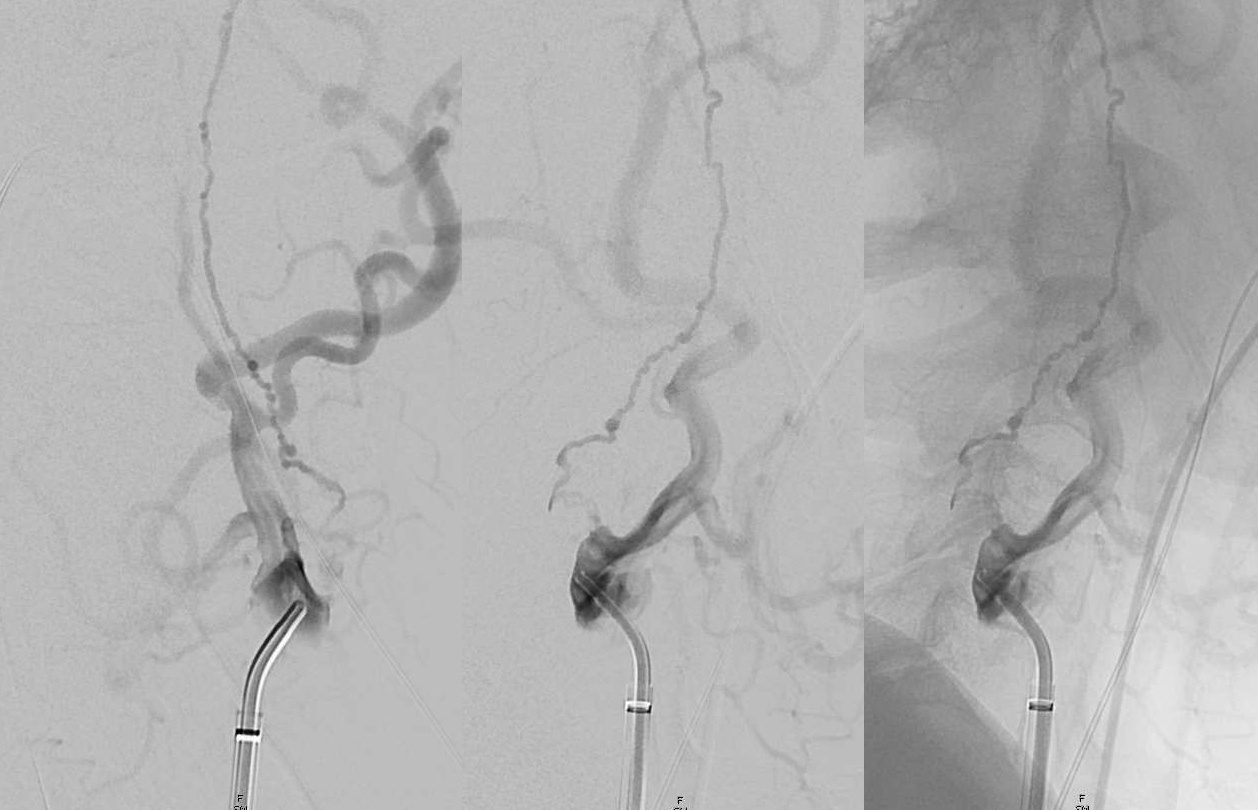
Some more looking — this is patient work. And unfruitful as it turned out with the headway duo

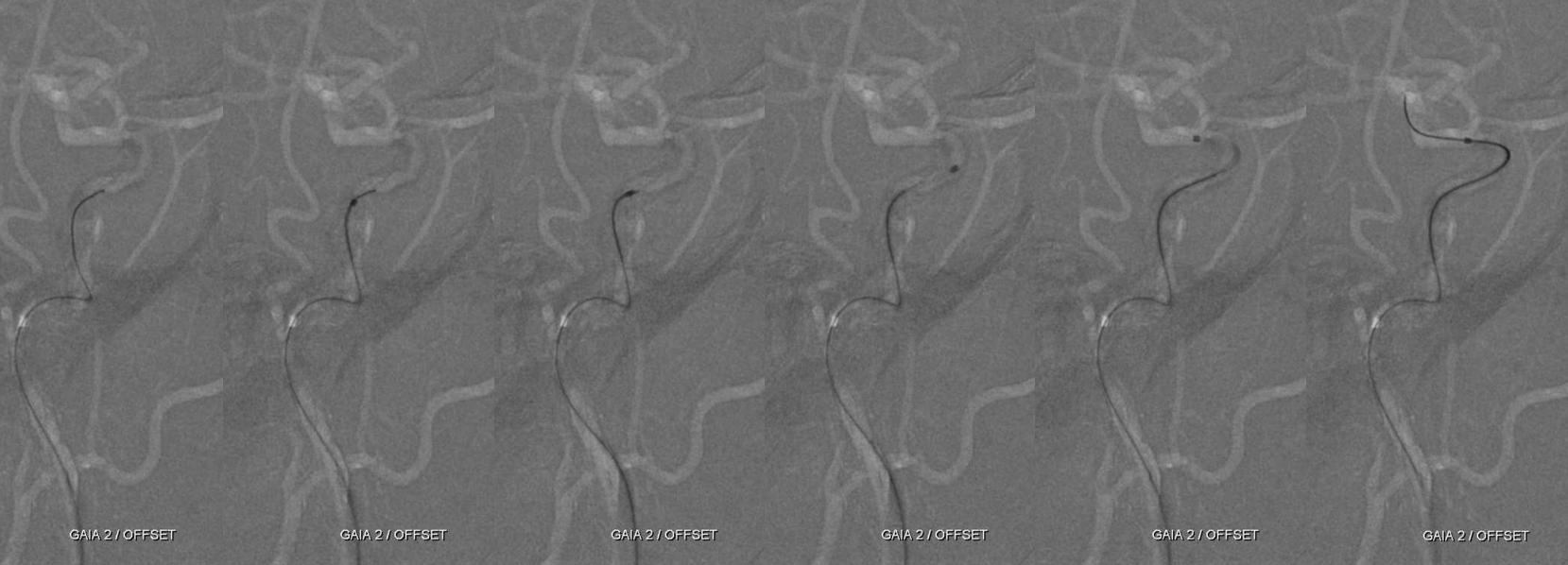
However, the Offset (a much underused tool in stroke) does the trick — Goia finds starting points, offset tip then goes up — its supportive enough to keep going but atraumatic enough to stay in the right place hopefully.

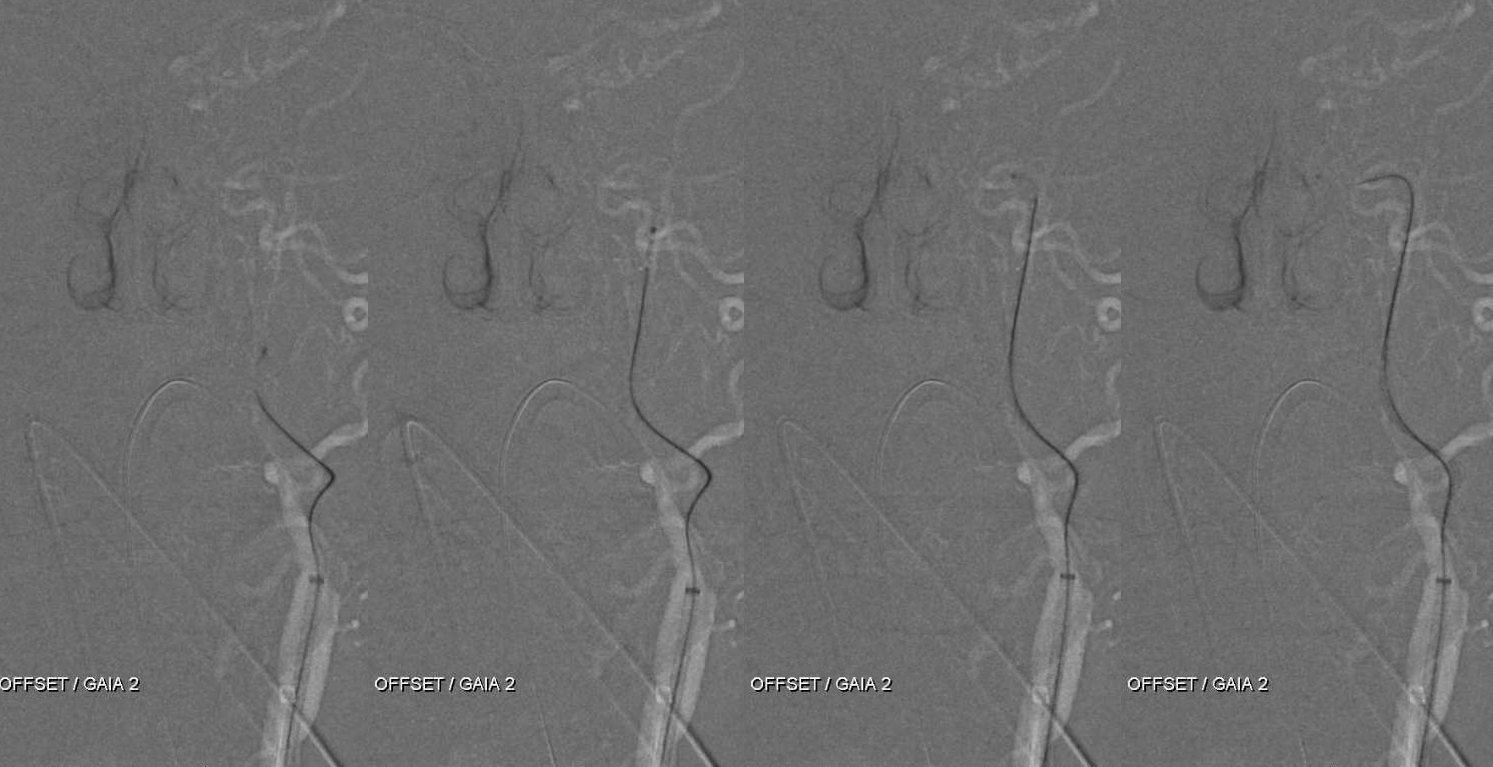
Keeps going
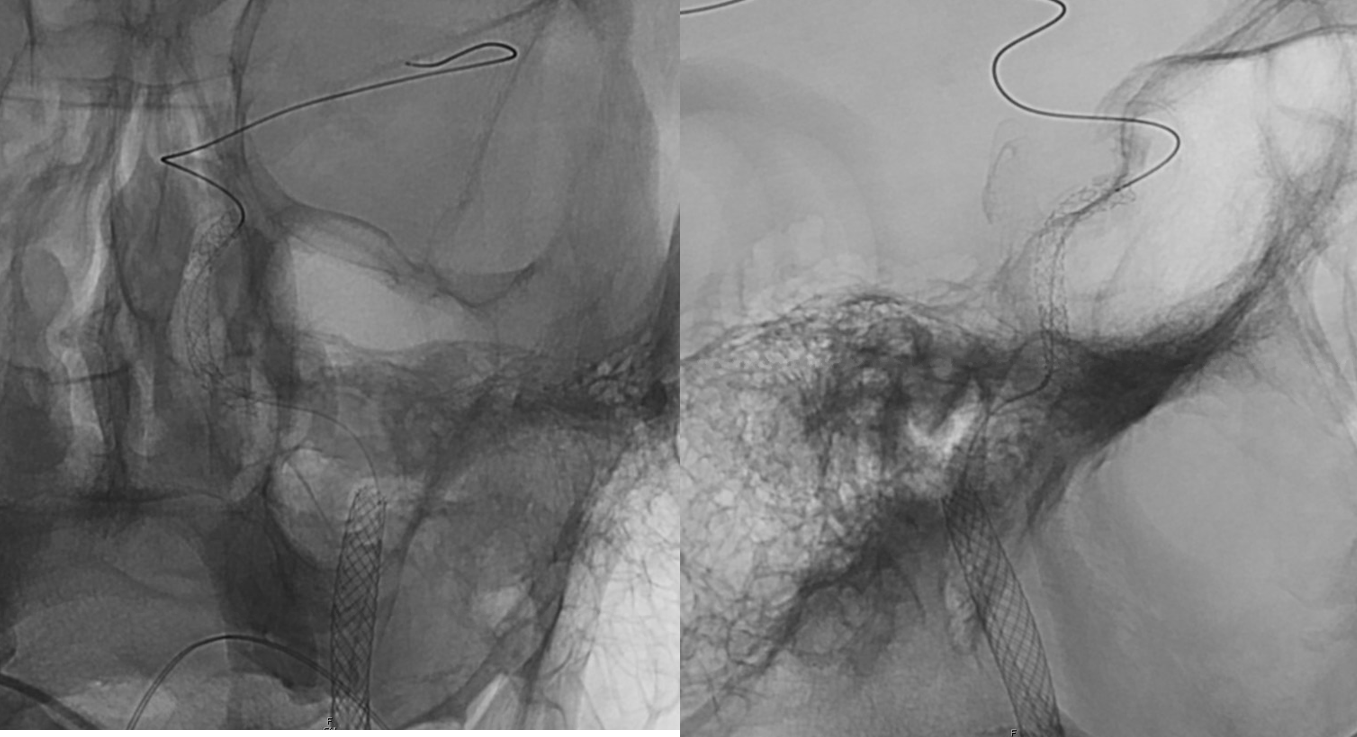
Until horizontal petrous segment where we stopped pushing and checked where we were. Probably should have kept pushing
Here is a movie of how this went
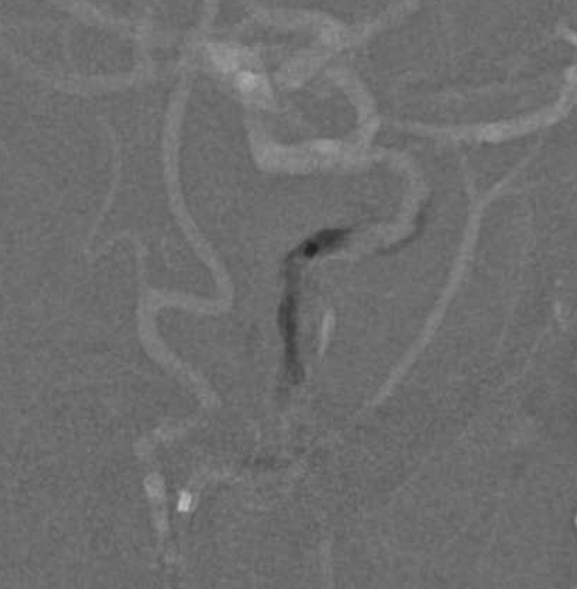
OK. no surprize here. we still arent in the cavernous segment…
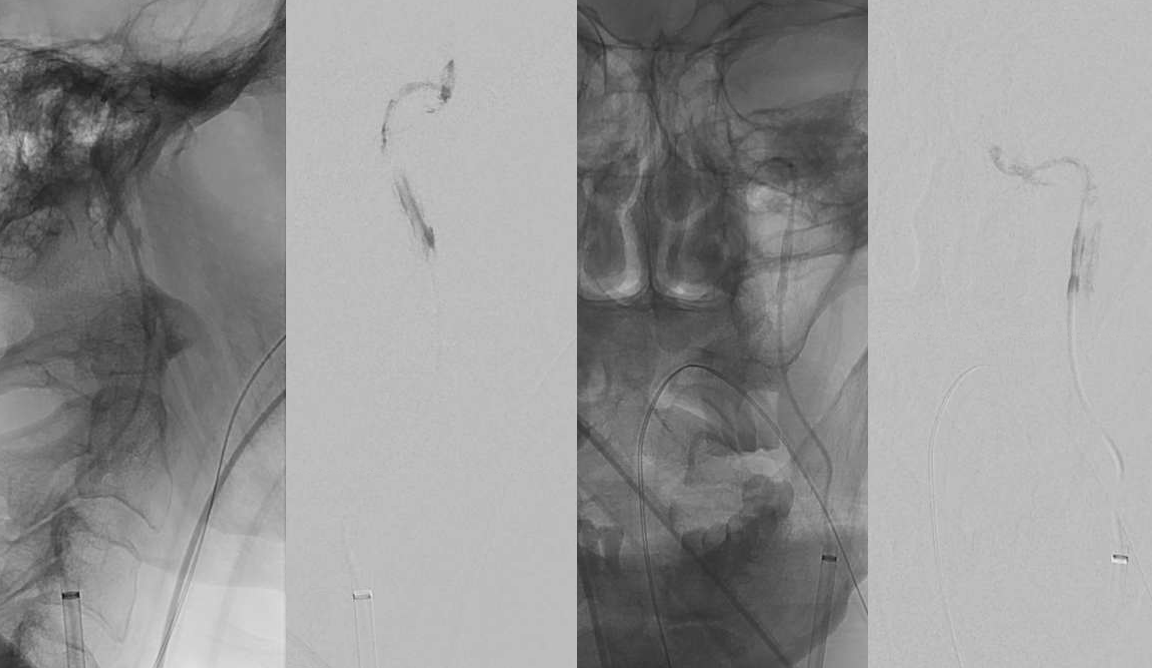
Despite advancing the Offset into the cavernous segment, see how it is not exactly in the right-looking place?
Still subintimal
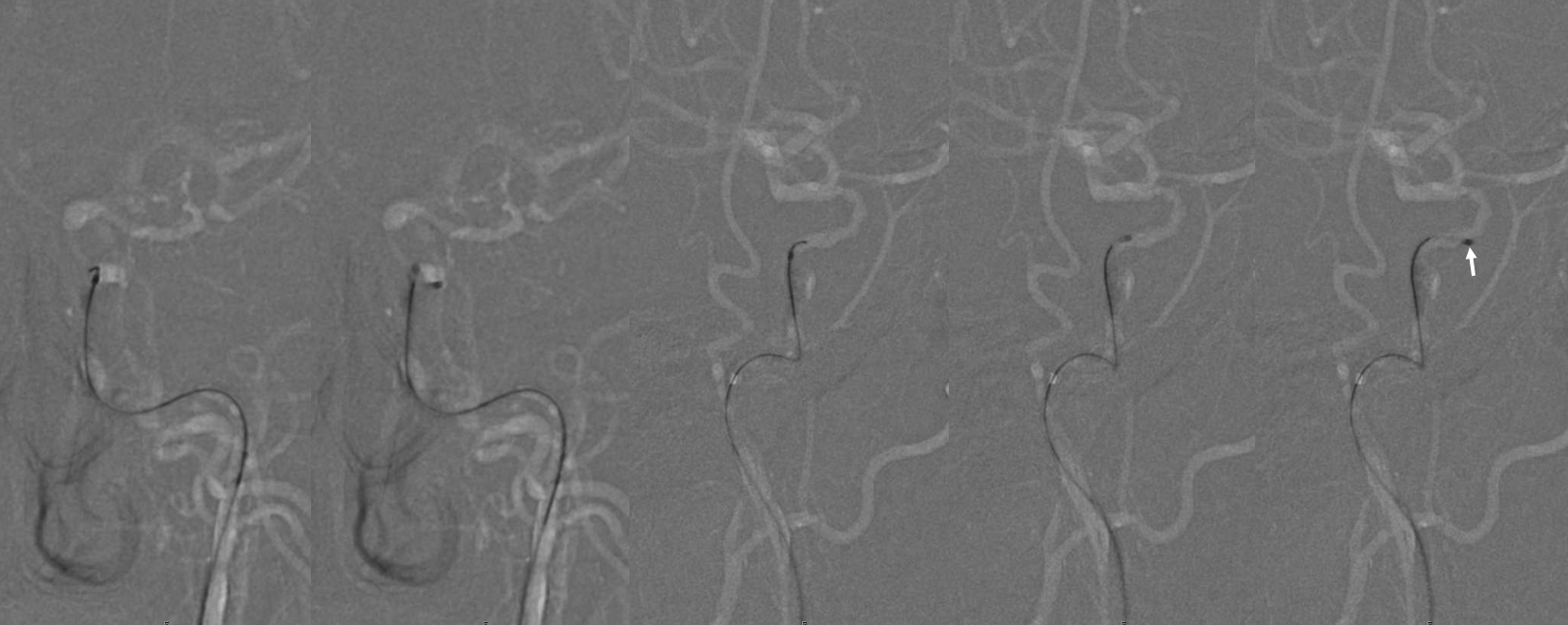
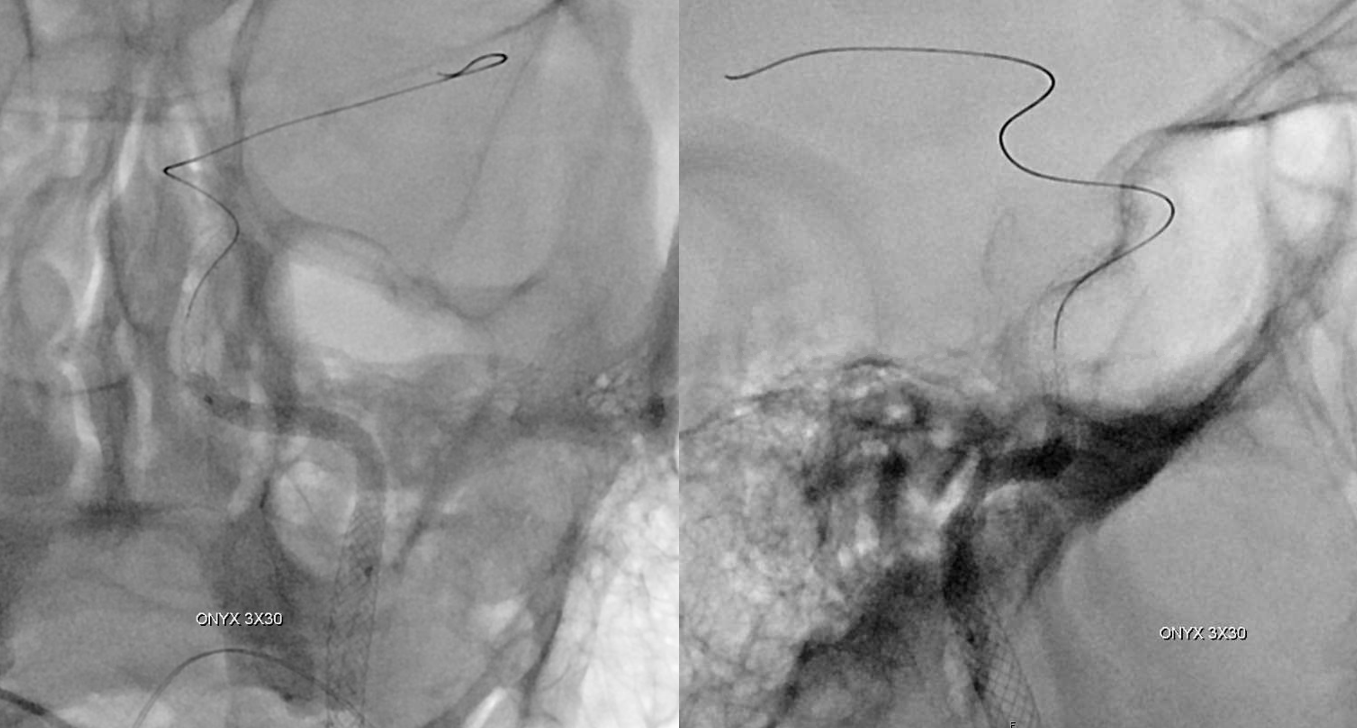
Takes patience to find the right road — Gaia gain found another channel and offset followed
Movie
Right place all right
Another nice thing about the offset — it kind of angioplastied a path already
Too early to selebrate way too early… An exachange 014 300 cm wire is needed here. A lot more work to do here. Starting with angioplasty.
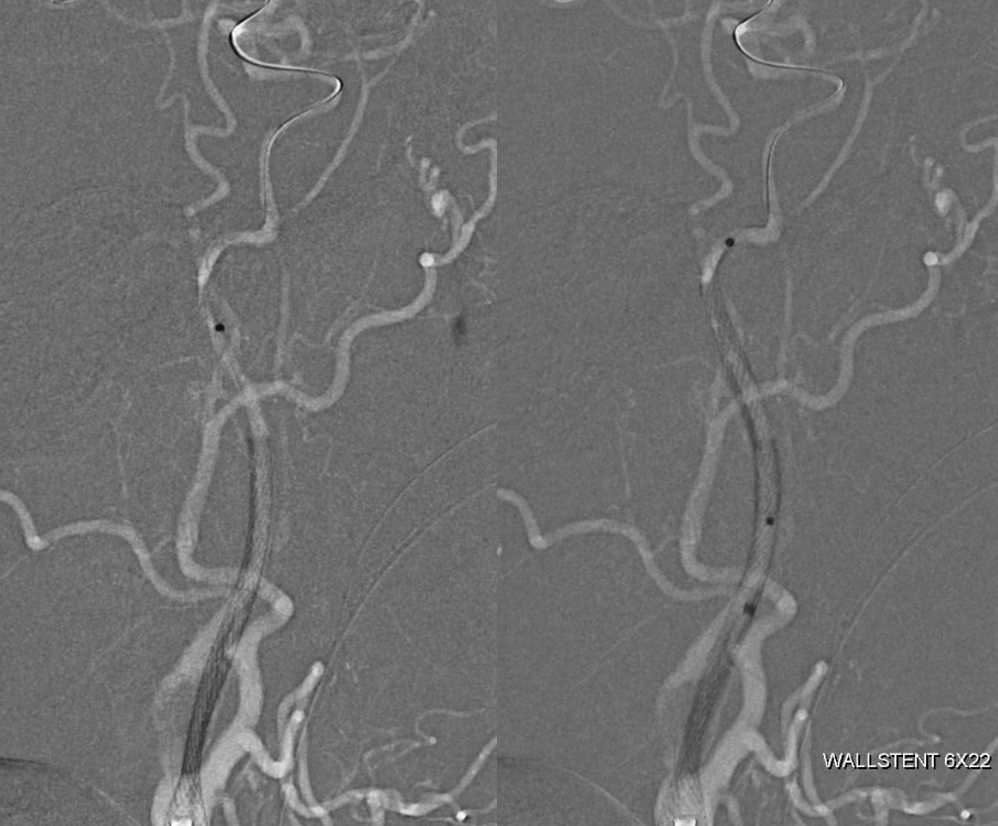
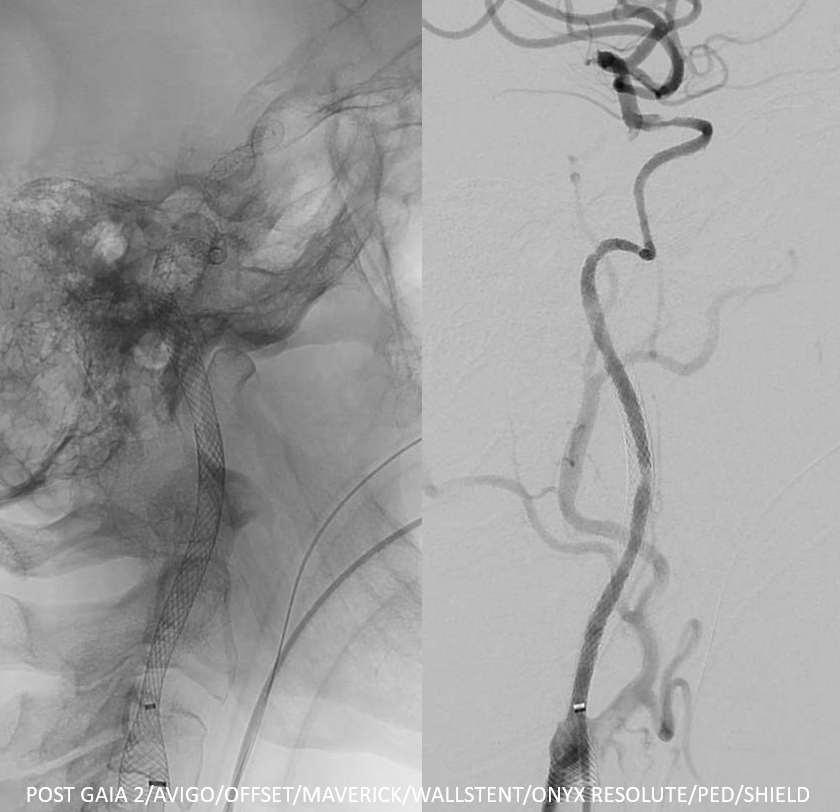
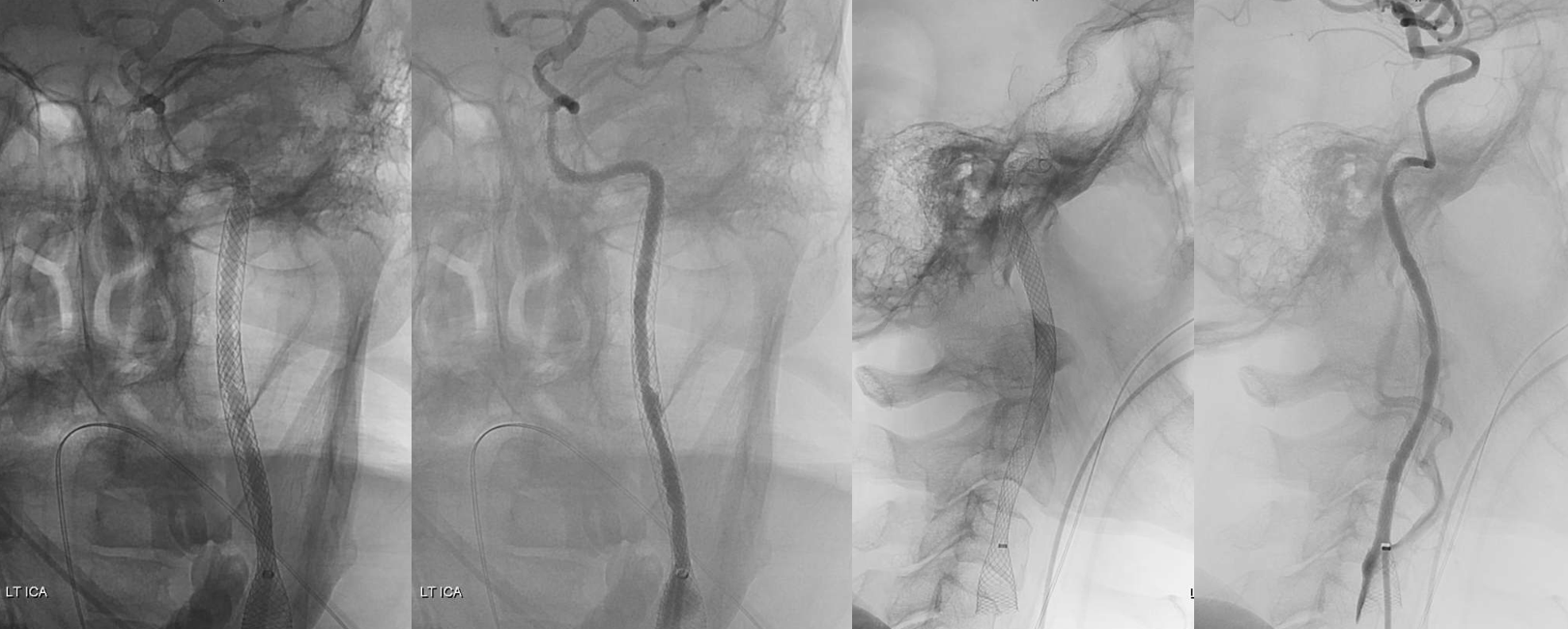
Proximal to distal is the way to build it. Starting with a few wallstents.
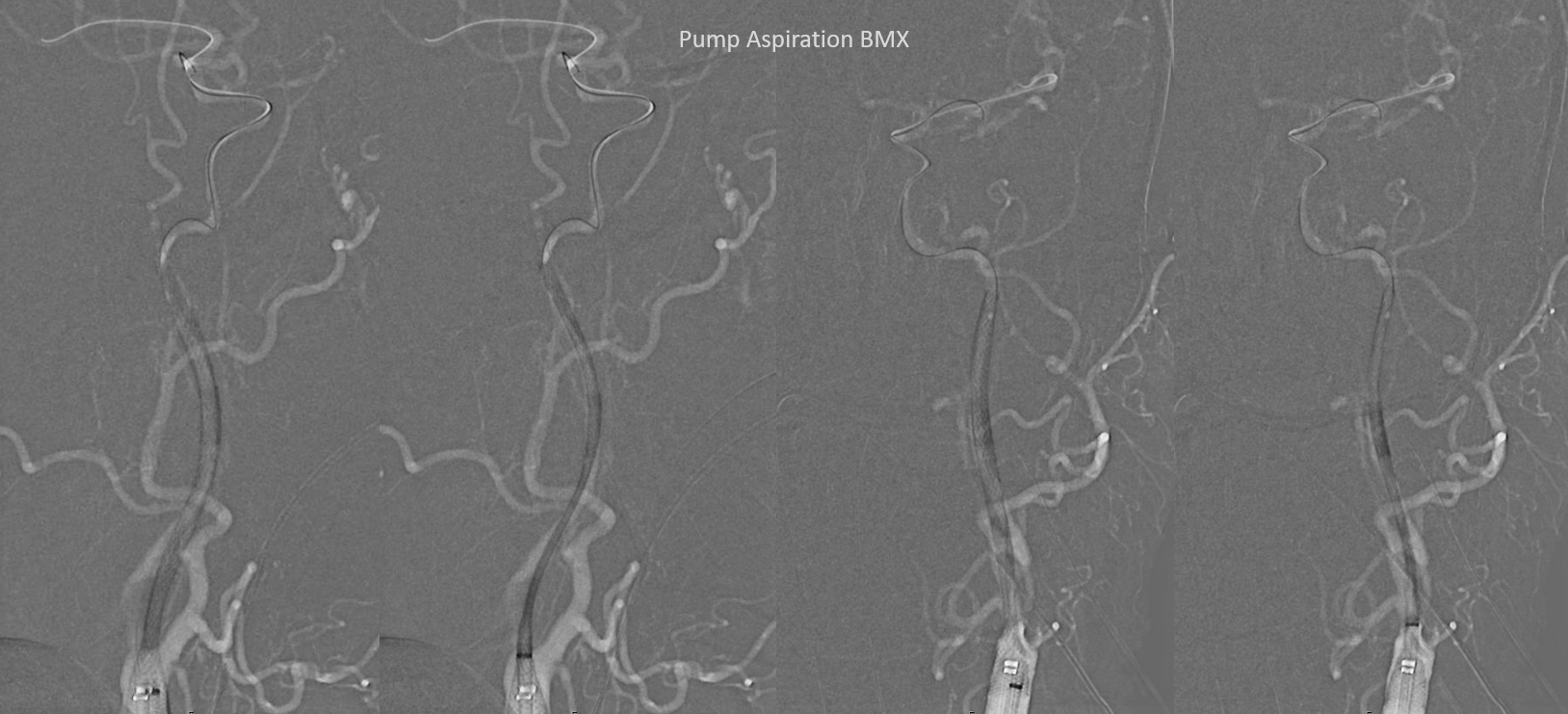
Notice something… Despite full dose integrilin the neo-ICA is closed again. See, there has not been an RBC in that lumen for years, and we are not even in the true lumen… its a bit thrombogenic…
How about what happens when aspiration is applied to the BMX… to heck for new thrombus
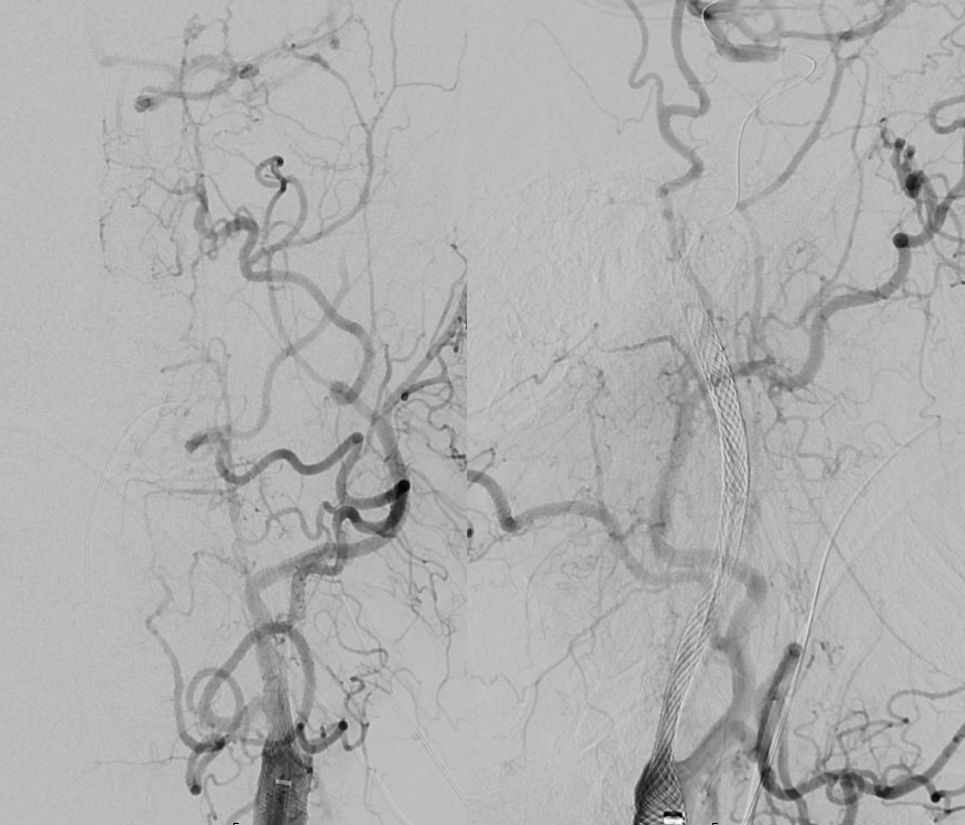
Now for the rest of the construct. Thats a job for Onyx Resolute. Or maybe 10 other untested things. So we like the Onyx…
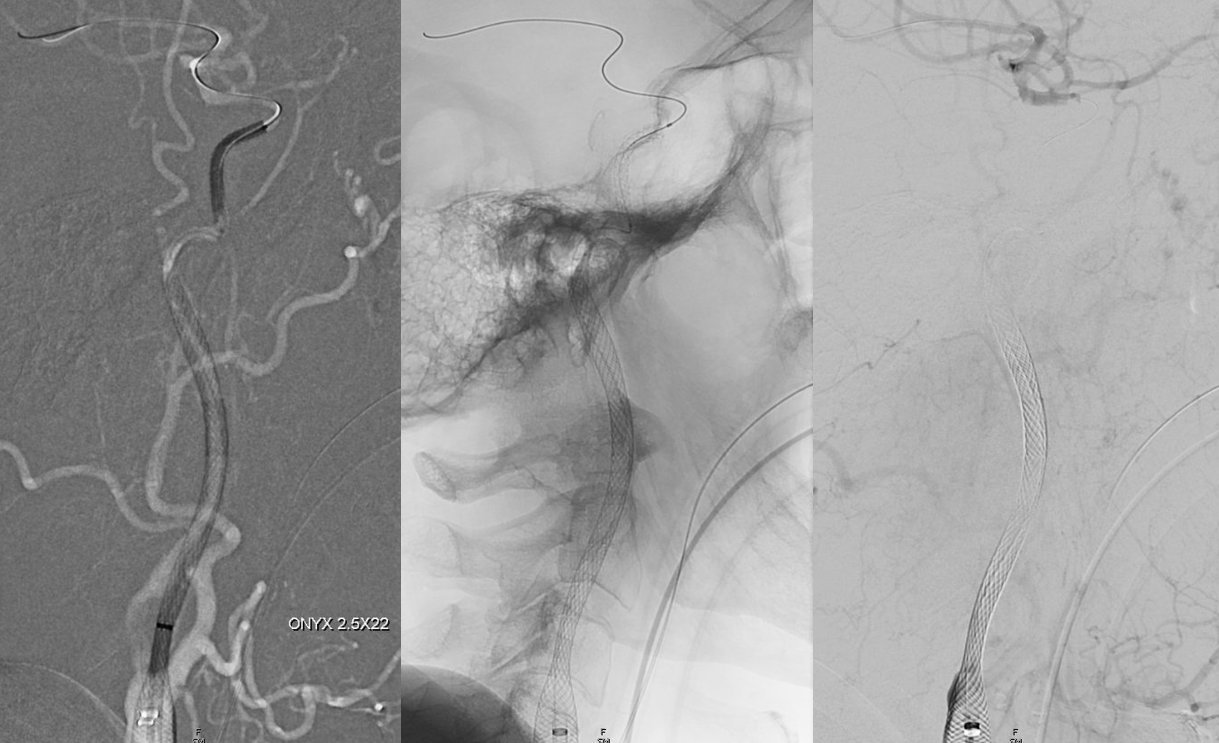
A few telescoping ones. Long ones cant make all the turns
Total of 3
Victory…
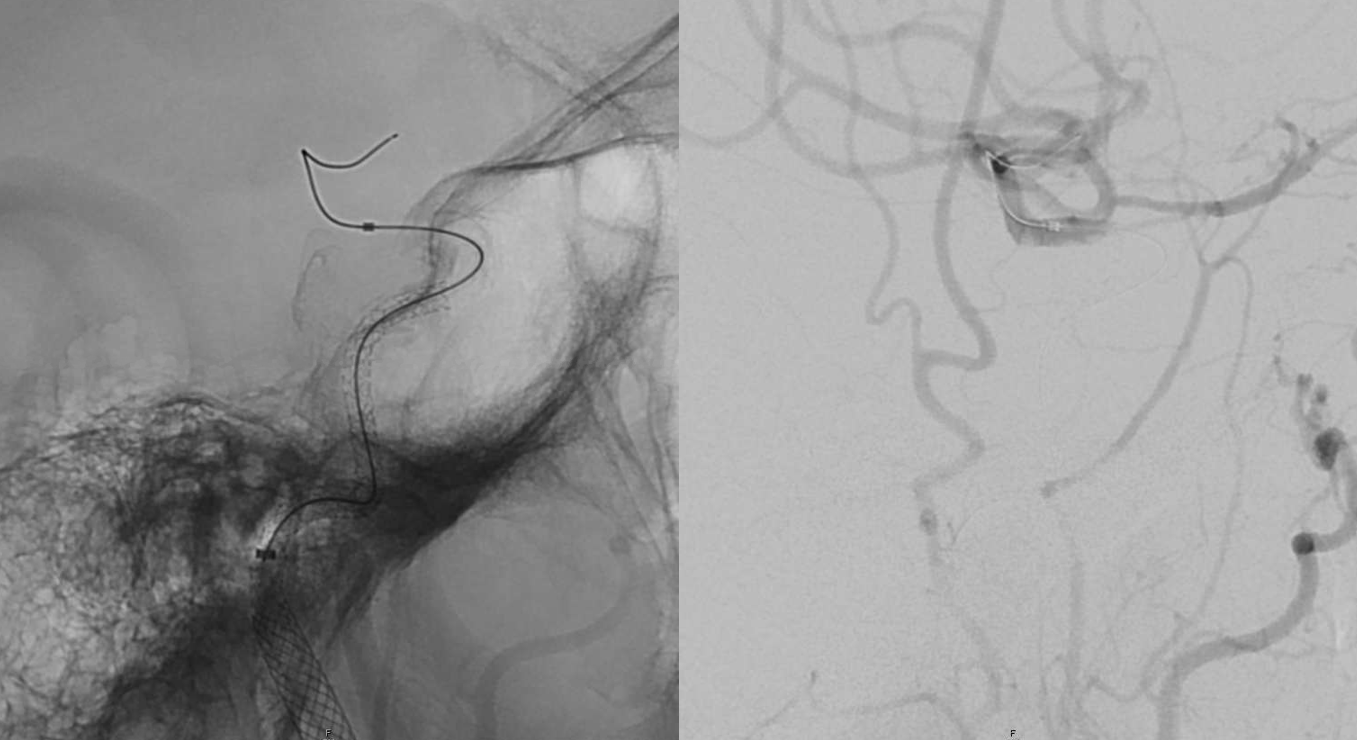
See why you need that 300 wire… Its not an easy thing to do. And its not done yet.

A Pipeline to top it off. Another option is to use the Pipes for the whole intracranial segment instead of the Onyxes. But we like it our way
Well, all it took is GAIA 2/AVIGO/OFFSET/MAVERICK/WALLSTENT/ONYX RESOLUTE/PED/SHIELD — not to mention BMX, and Transcend 300, and the Celt that is still to come when this all ends well…

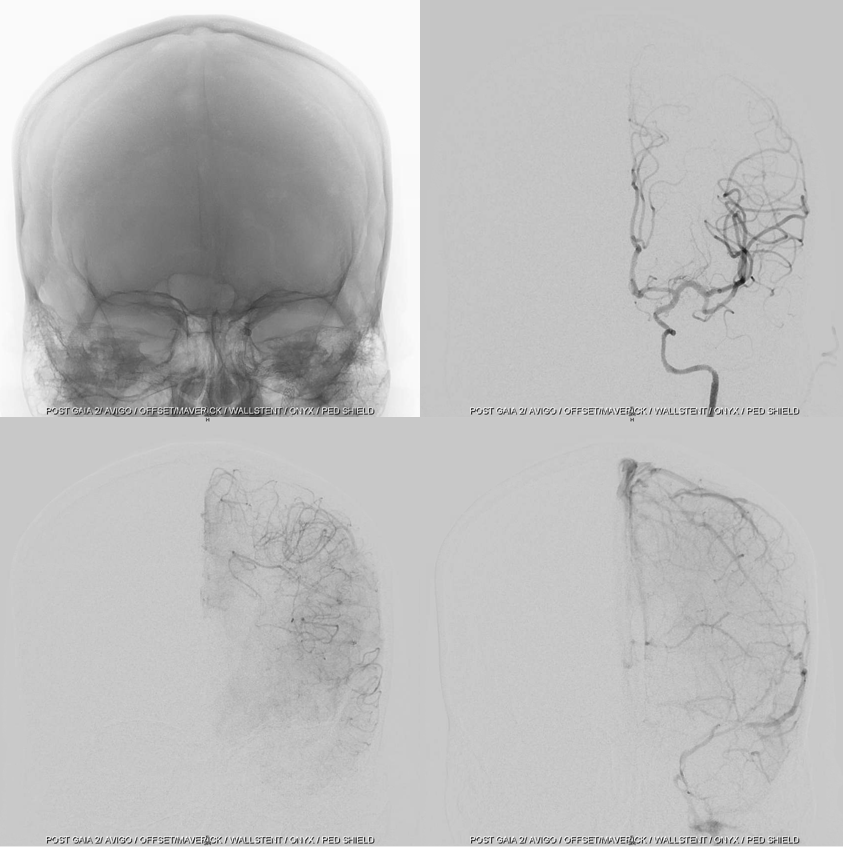
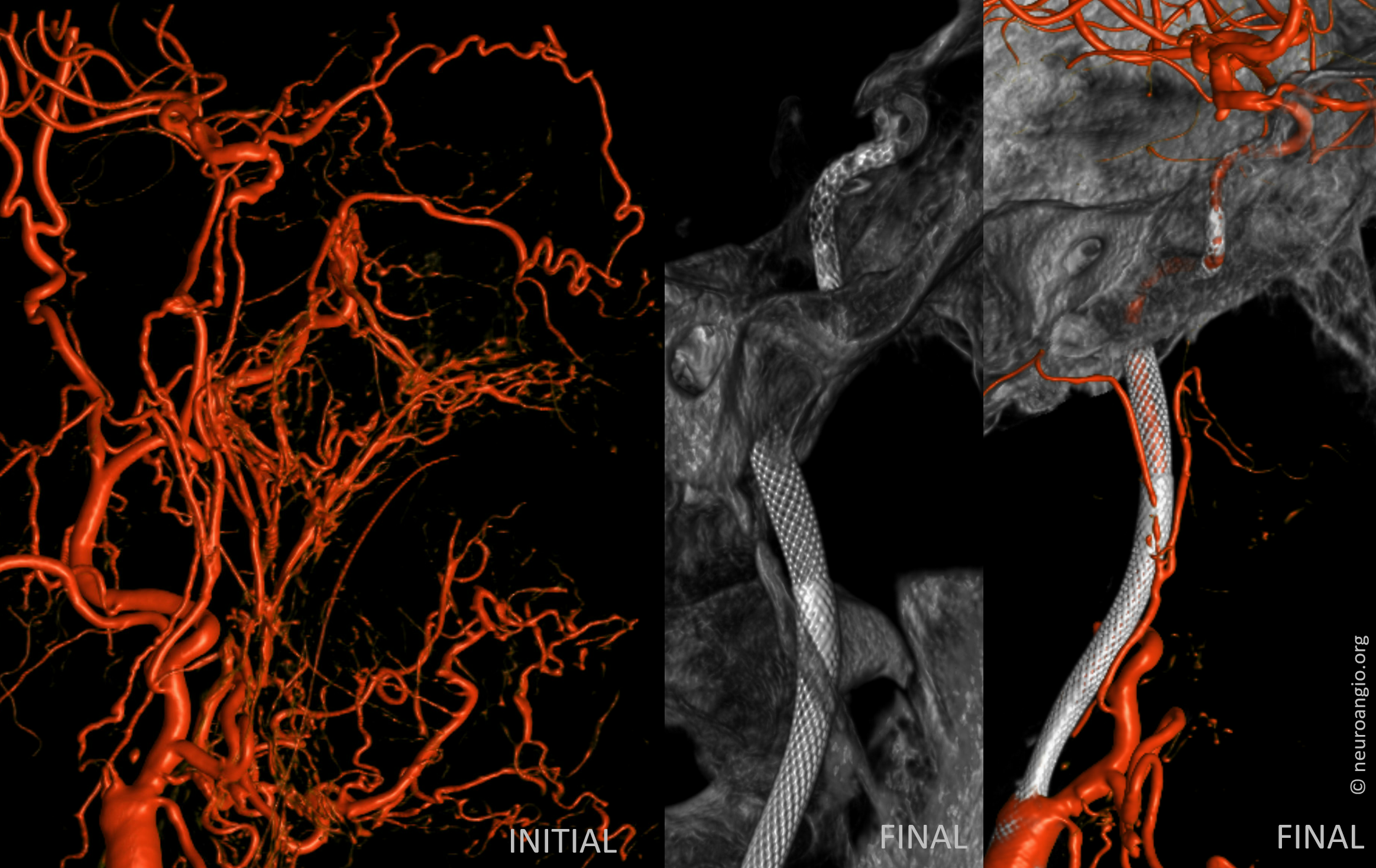
Now for some beautiful images
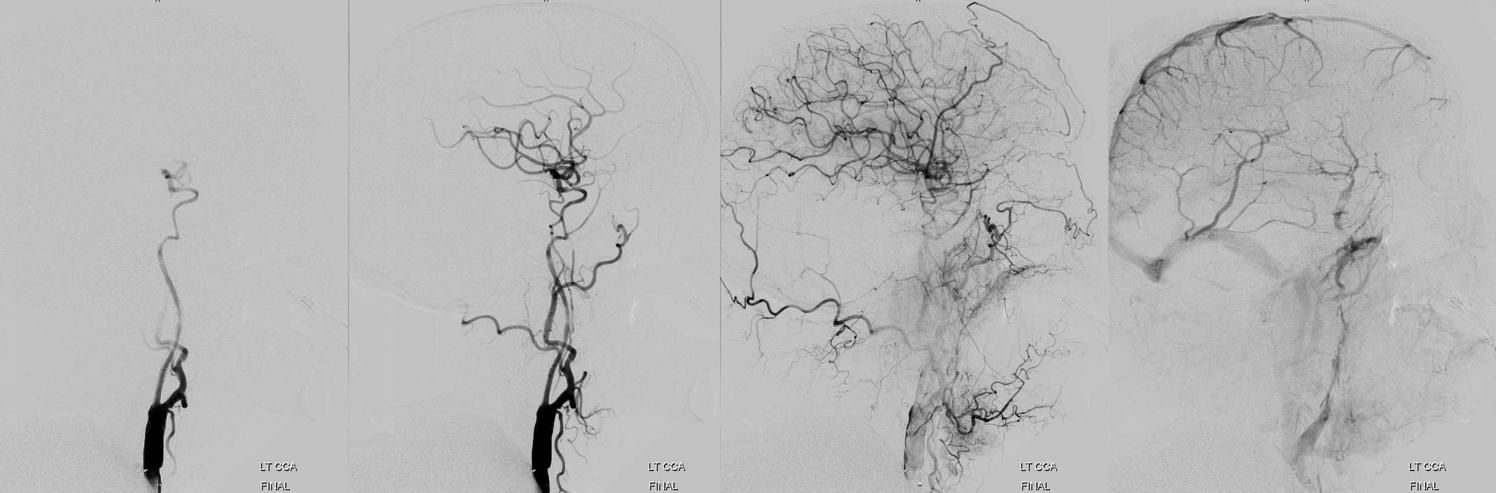
Before
Final — See how the vasa vasorum is not the same path as the revascularized carotid

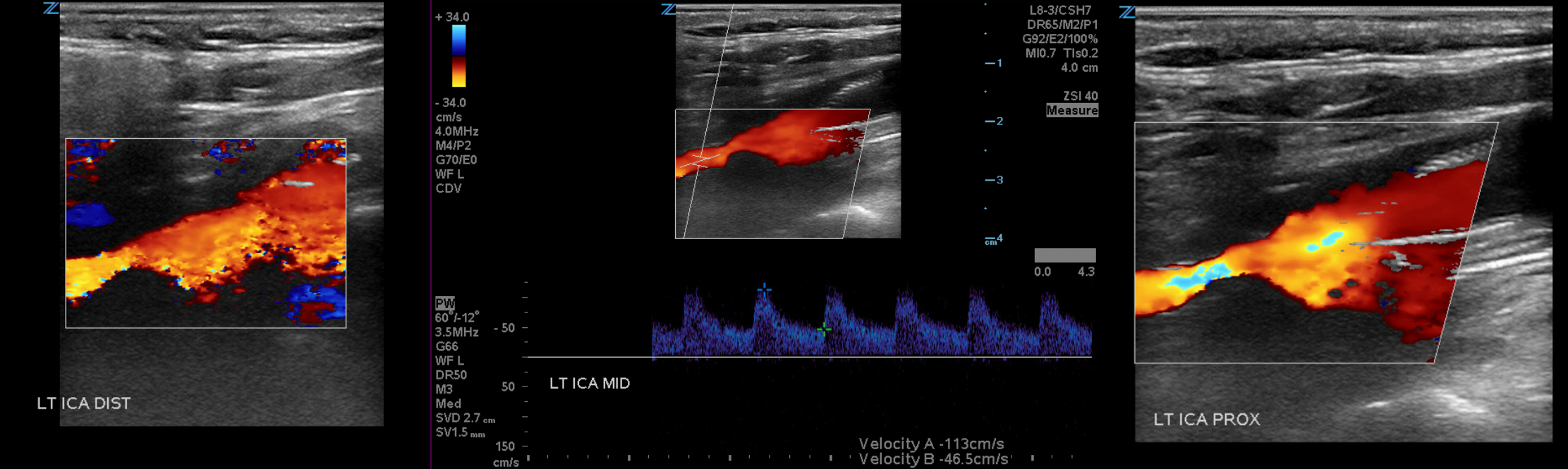
Patency can be followed by ultrasound
Angio 3 days later
