
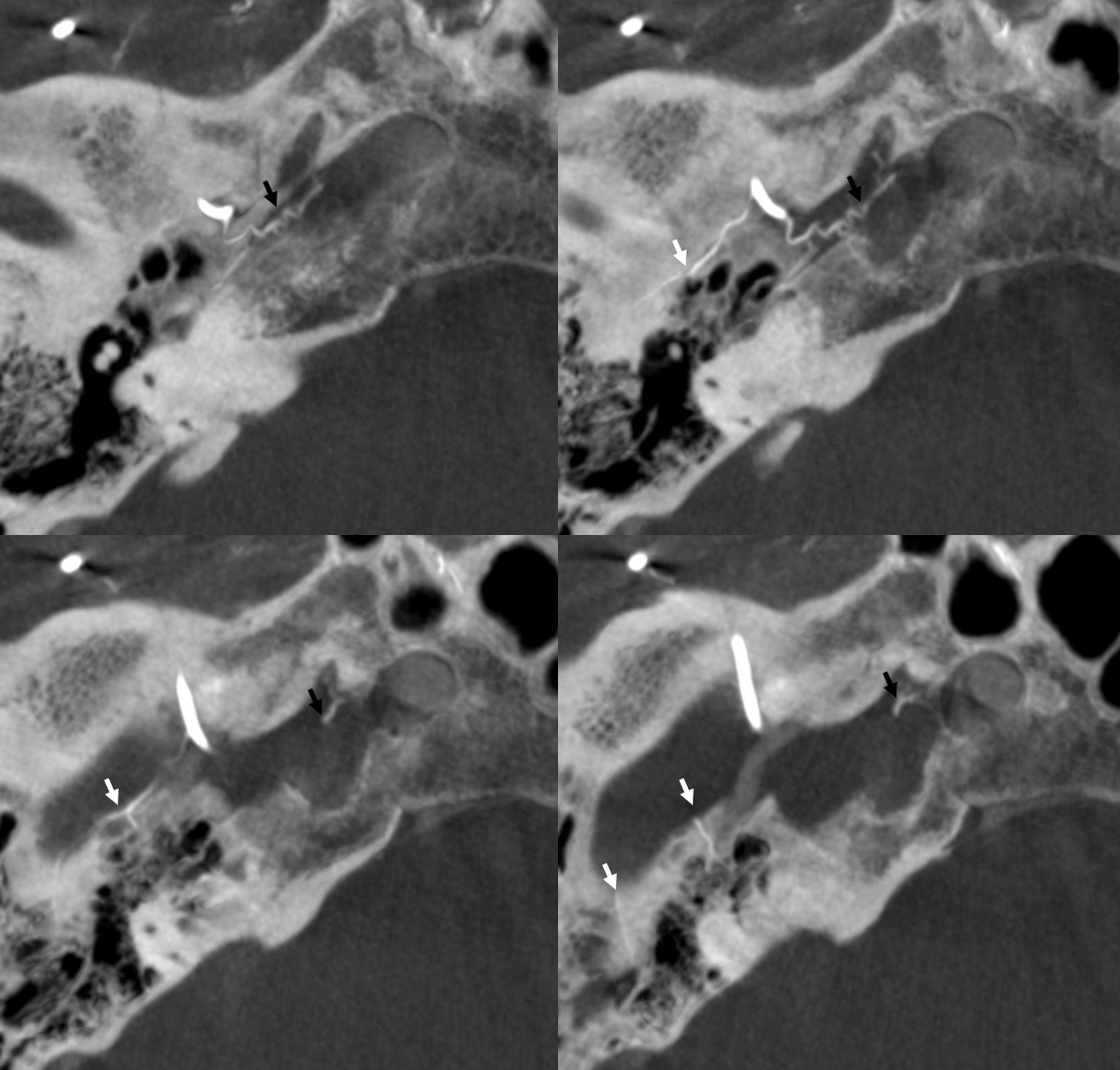
Number 35 above. Same as spinosum branch of ILT. Connects proximal MMA with ILT. Both can supply cranial nerves of the cavernous sinus and Meckel cave. Another reason not to embolize from a proximal MMA position. On angio projects medially, arising immediately after MMA enters cranial cavity. Often not well seen on lateral views due to foreshortening. Below both cavernous (black arrows) and petrous branches (white arrows) are seen
Here are some more examples
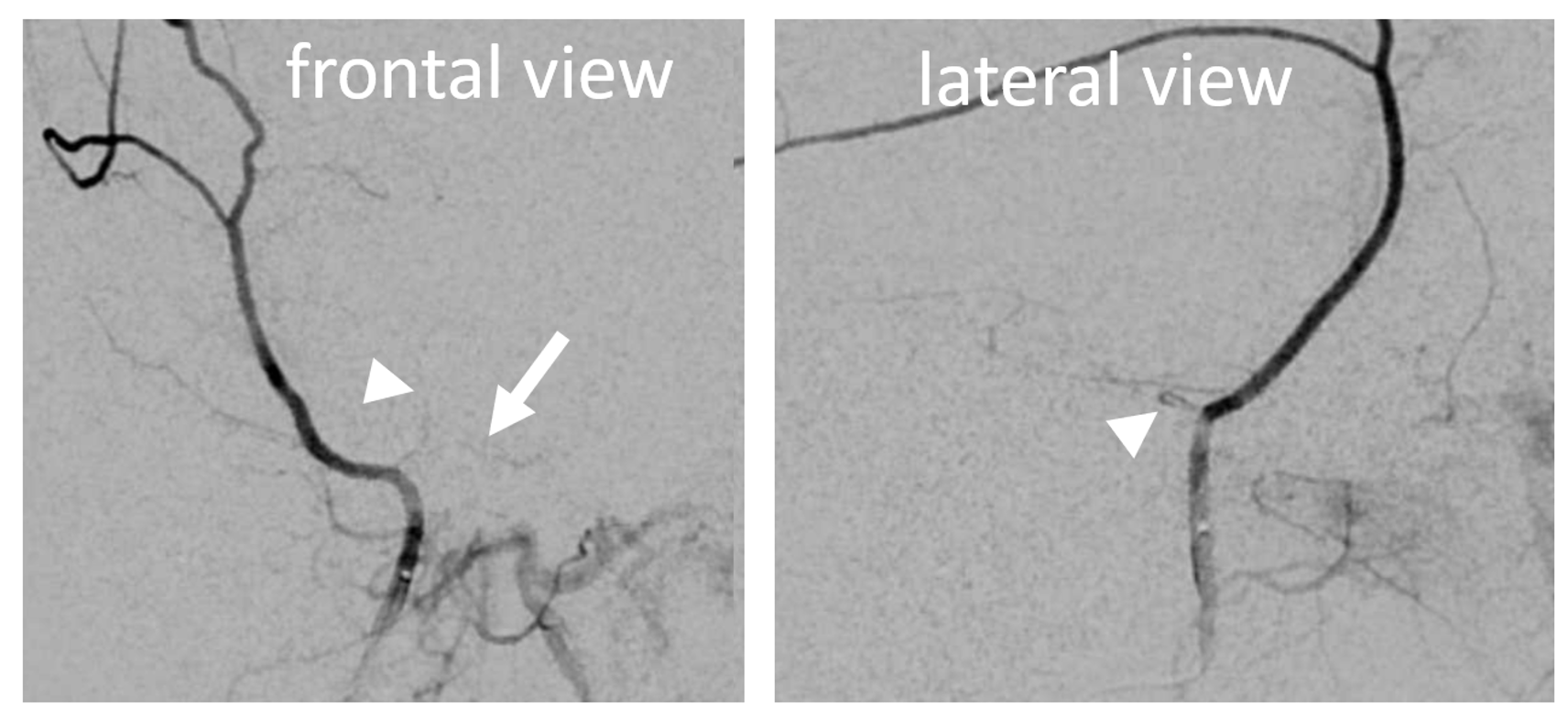
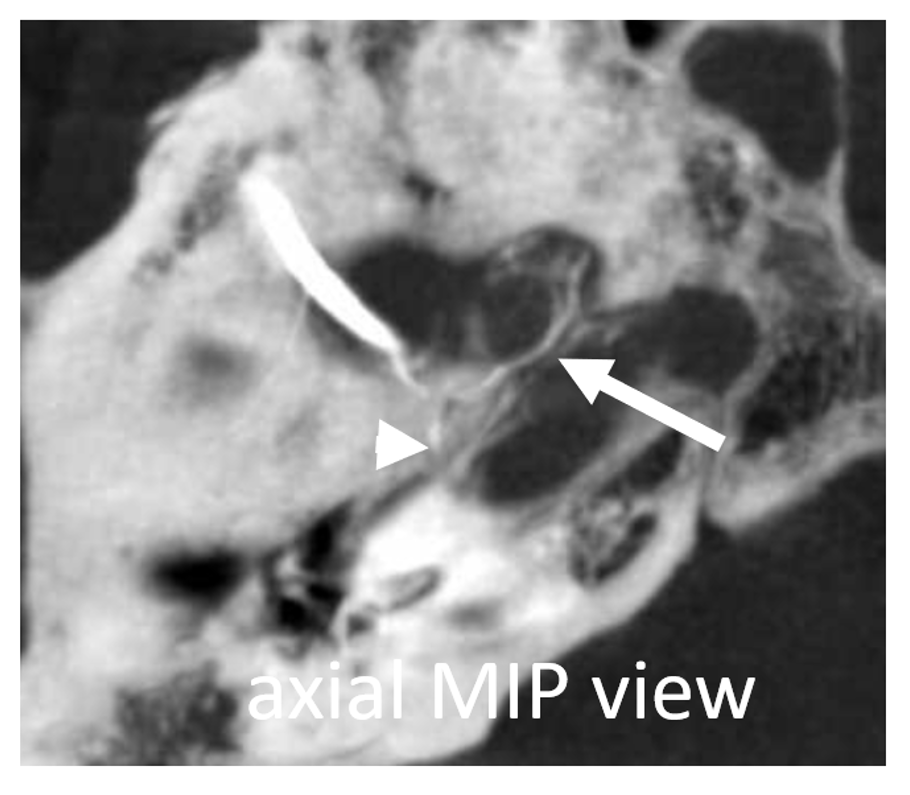
 Angio appearance of cavernous (arrow) and petrous (arrowhead) branches. Both are usually very small. The cavernous branch is foreshortened on lateral views and not seen
Angio appearance of cavernous (arrow) and petrous (arrowhead) branches. Both are usually very small. The cavernous branch is foreshortened on lateral views and not seen
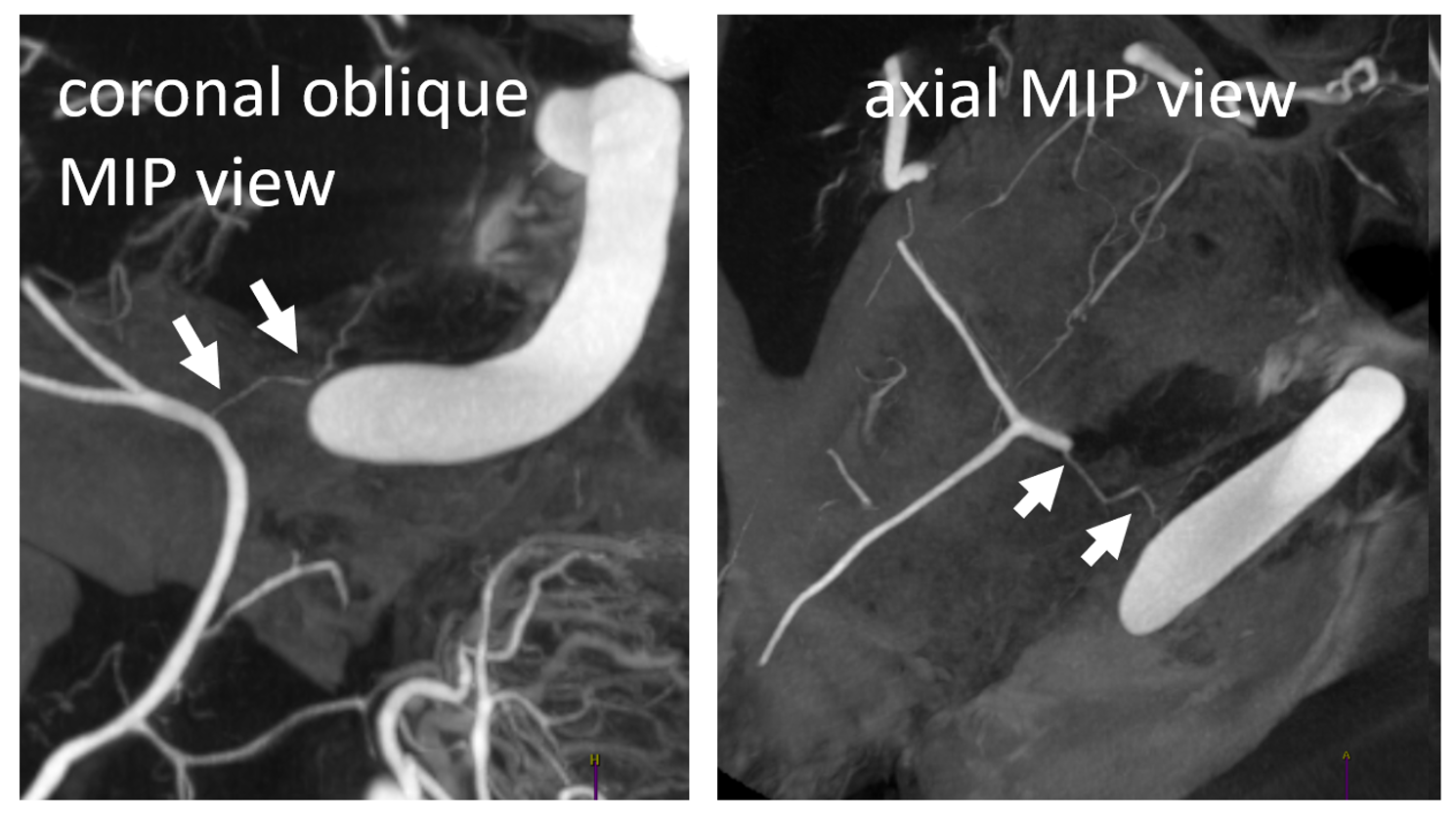
Same case on DYNA CT
Below is example of cavernous branch (black arrows) contributing to supply of cavernous sinus fistula
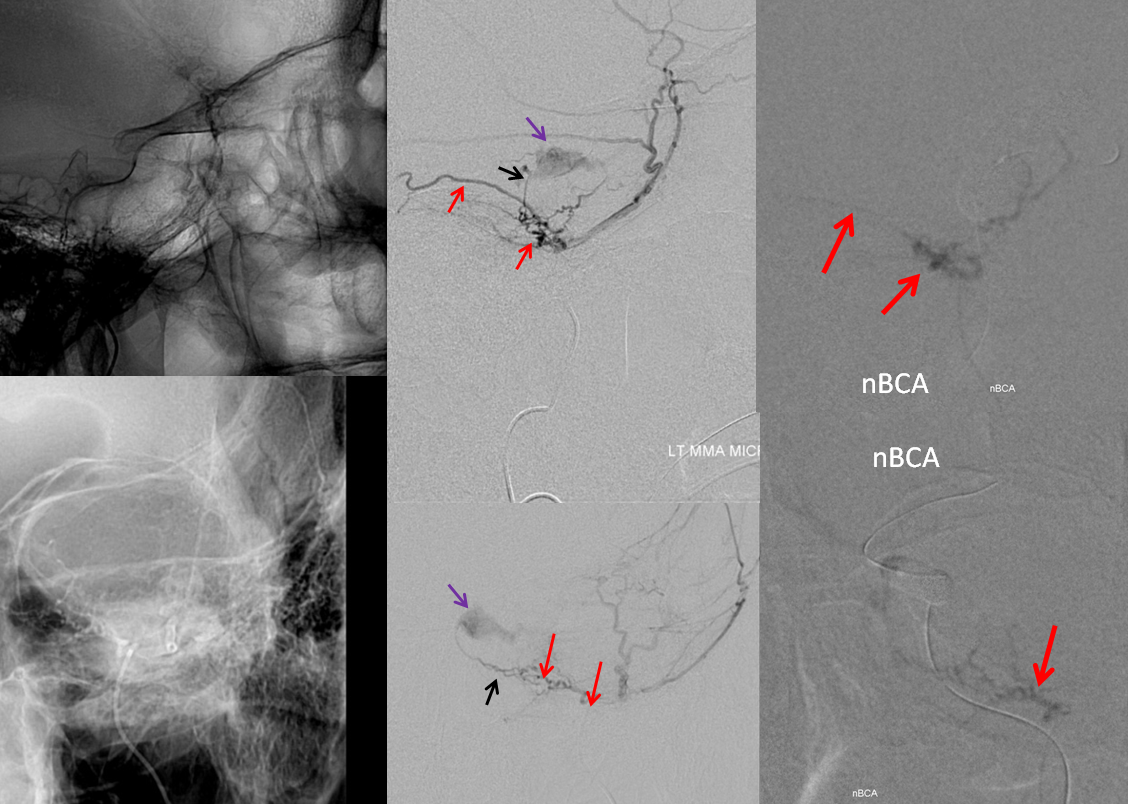
The whole case is here — and it shows why proximal MMA embolization is a a bad idea