
Part of neuroangio.org radial access collection. Perfusional status in a maximal medical management patient with severe intracranial left vertebral artery stenosis, occluded right intracranial vertebral, and hypoplastic posterior communicating arteries. Left radial artery is an excellent choice for left vertebral work. A 5F sheath works with any number of 5F distal support catheters, such as Navien, which is what we typically use. Our usual protocol is 4F VER for vert catheterization followed by exchange for the Navien. Primary Navien catheterization is also feasible. See video below
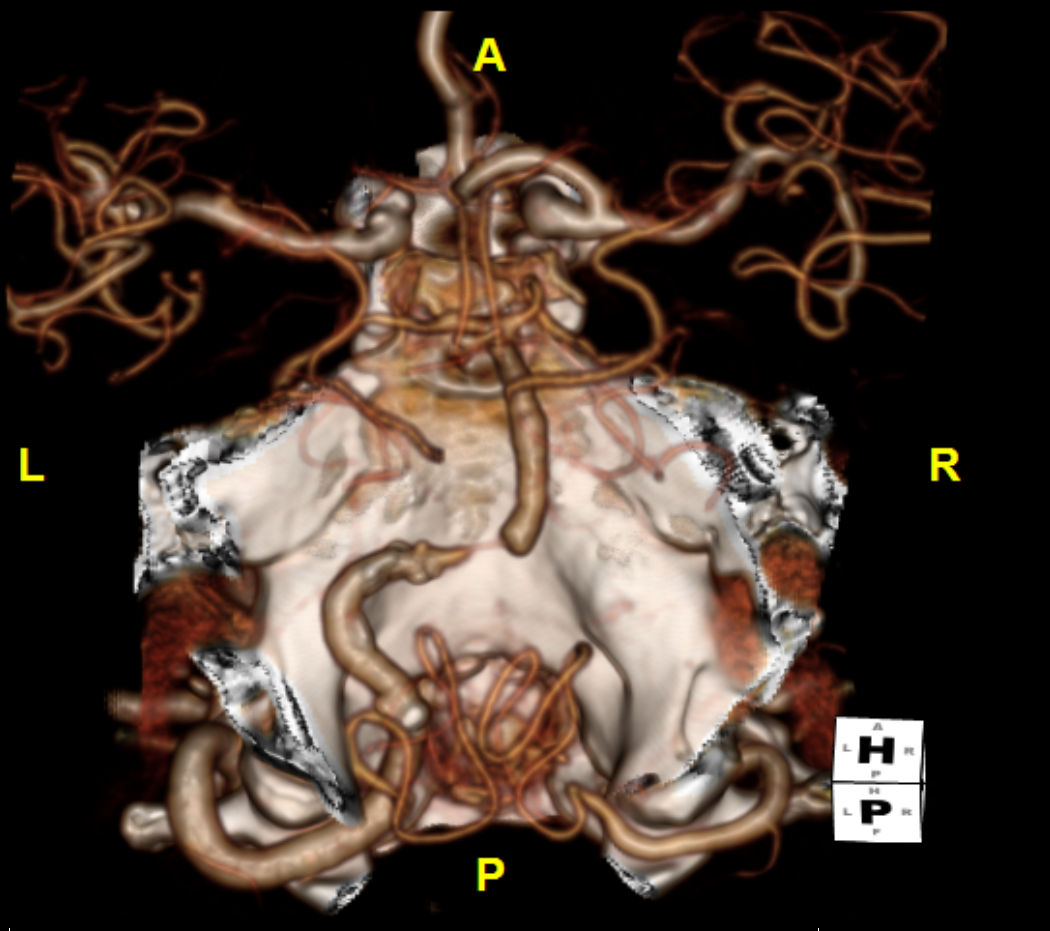
Here are some still images. CTA
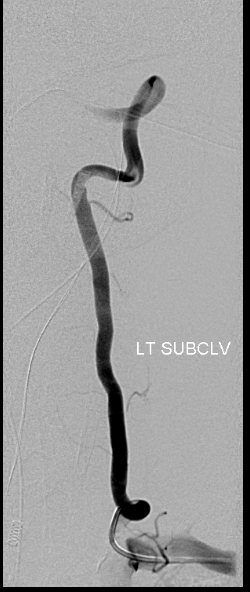
Typical arch. Catheter from left vert approach

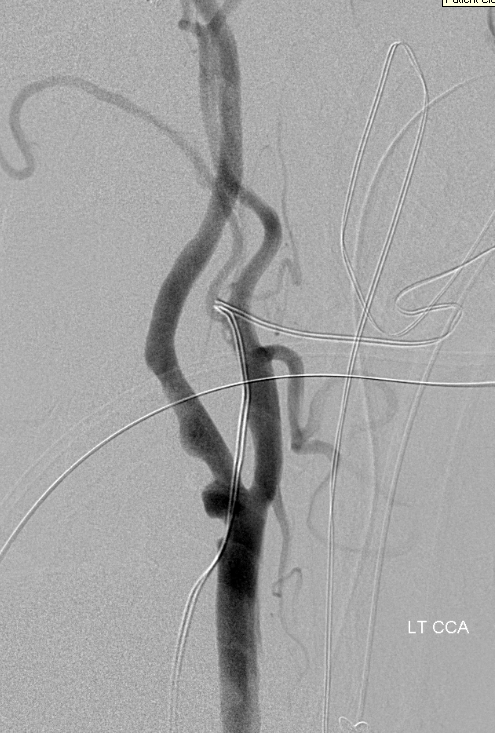
Left CCA. Catheterization of great vessels is more difficult from left vert approach and is not predictable in my view. Right vert is much better for that. Here however we dont need to inject everything
No PCOM. No A1

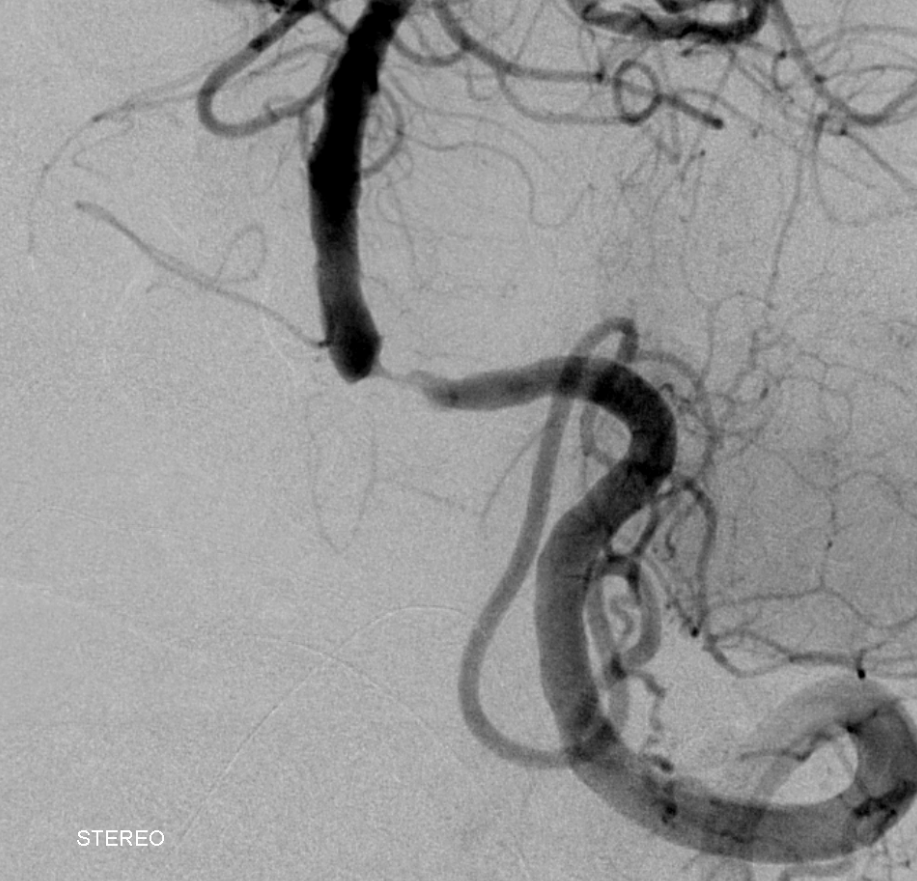
4F VER in left vert. There is a loop proximally that will be straightened out by access wire later
Lesion. A small pons perforator just distal to the stenosis is visible on the left as well as small right AICA. The anterior spinal is also coming from left vert but more proximally.
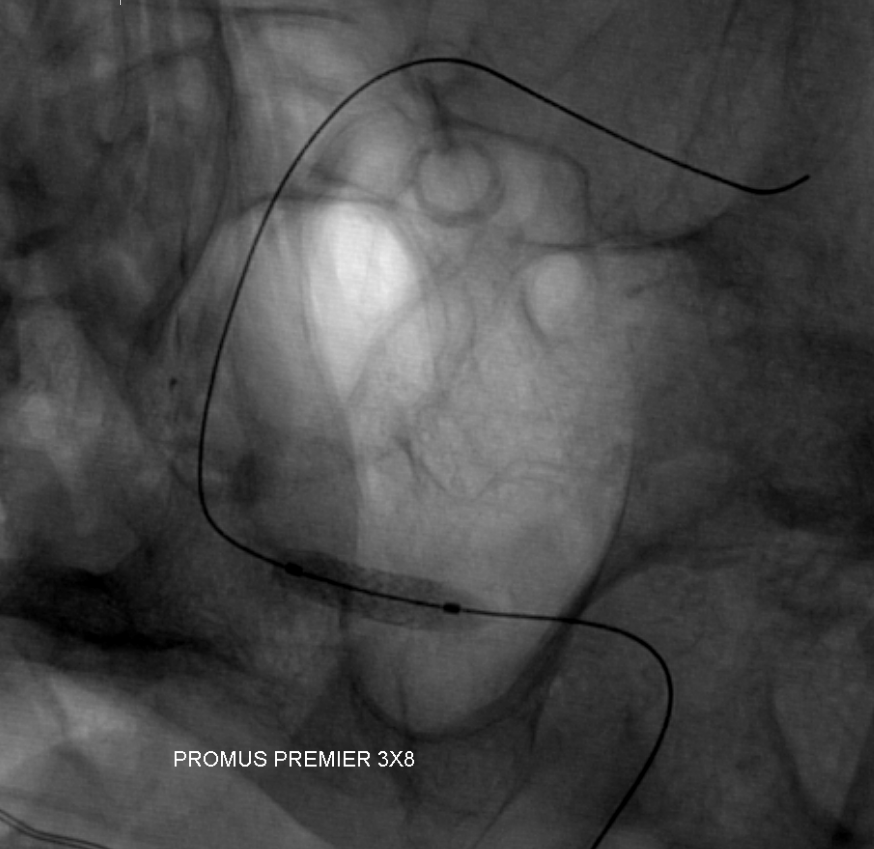
Promus Everolimus eluting stent 3×8 in place. The 4F VERT was exchanged for a 5F 058 Navien 115 cm which was brought into the C1 vert segment. Promus delivery system is a bit short (its designed as a coronary stent) so access has to accommodate for that
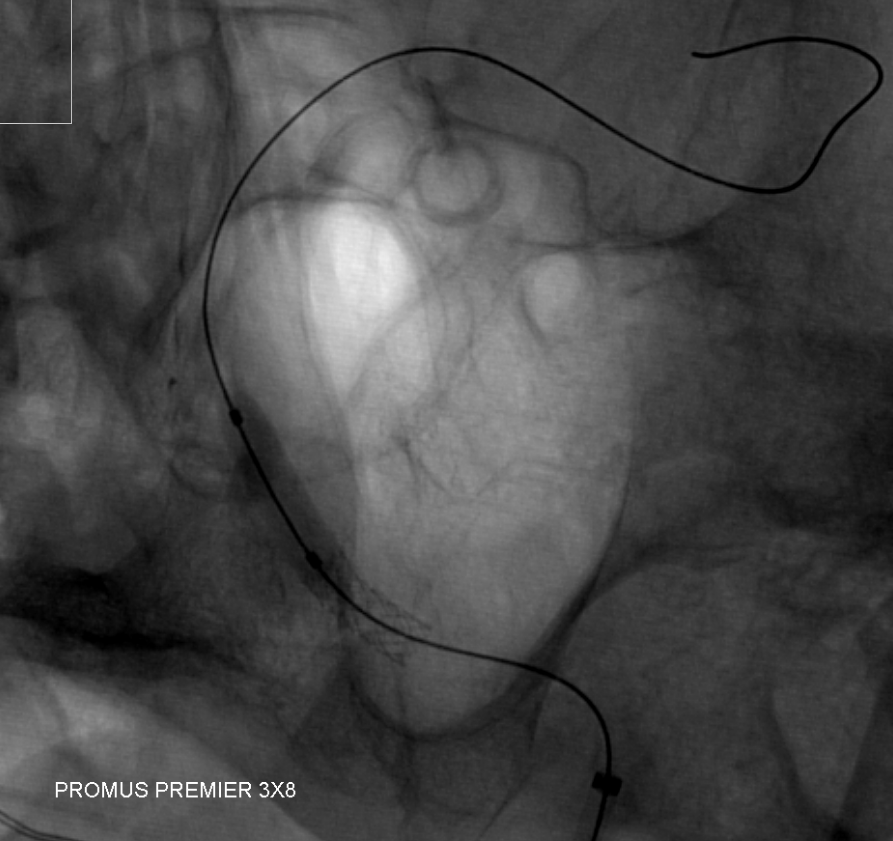
Inflating balloon a bit more distally to better match vessel size discrepancy between proximal and distal
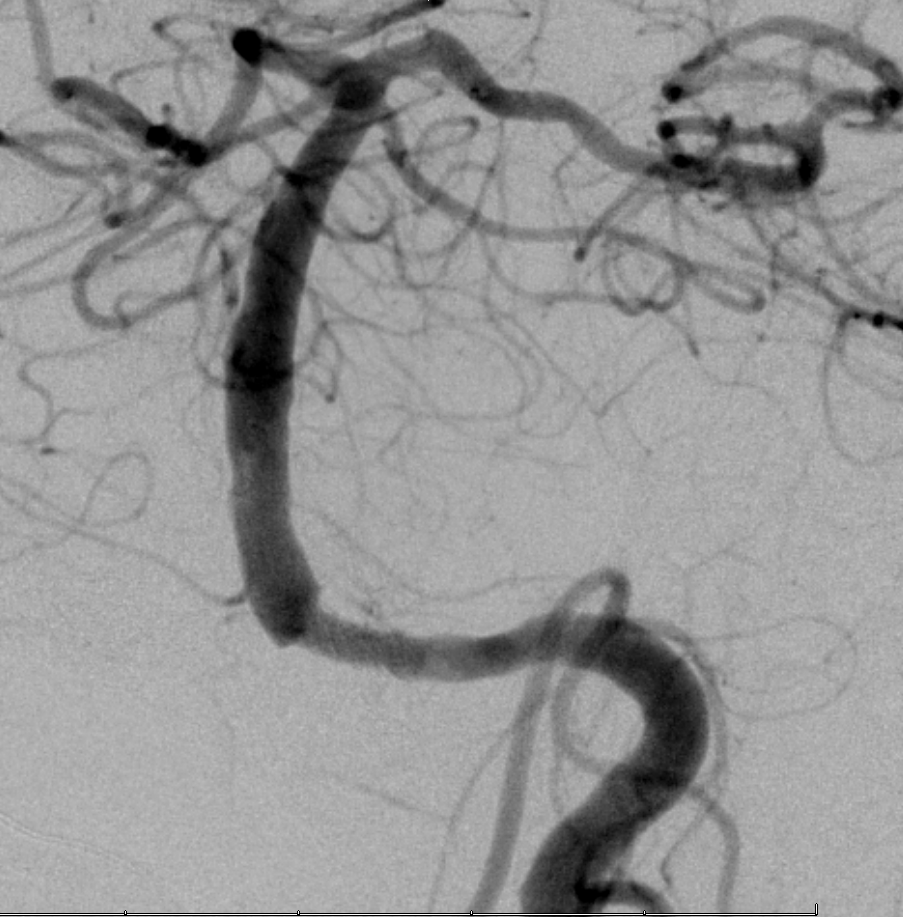
Post
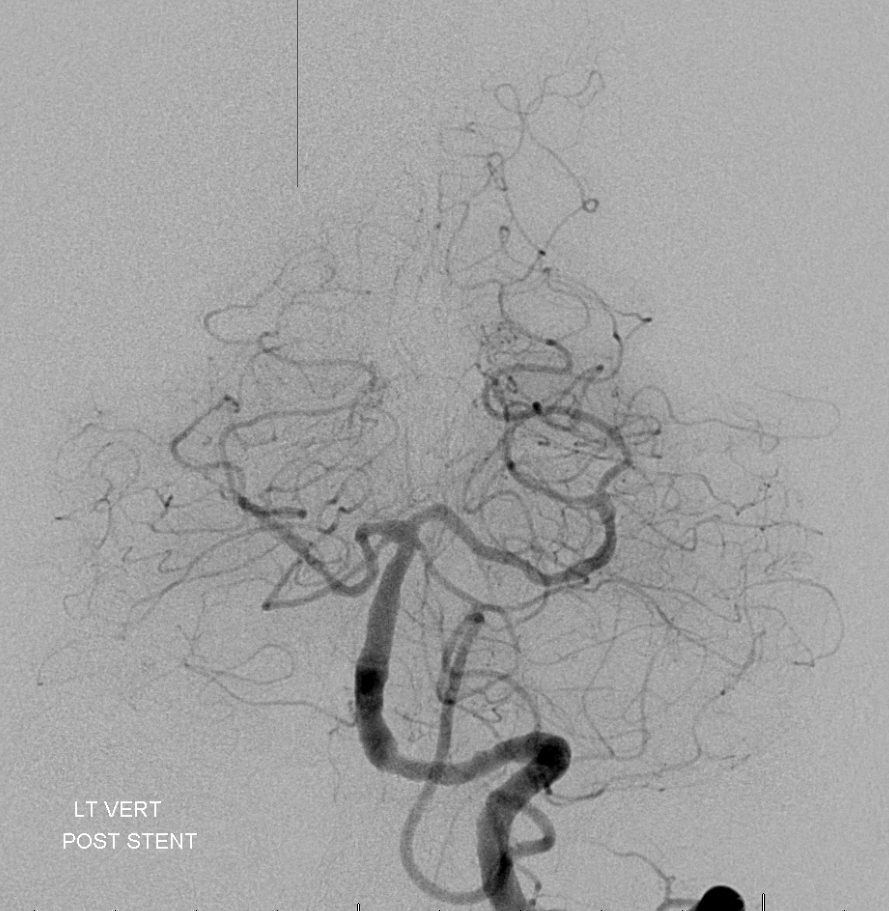
Global post
Radial shot on way out. We like doing that. There is antegrade flow in both radial and ulnar. We do a strong short injection so reflux into ulnar does not mean spasm.

Check out other Radial Access Cases on the “Cases” page