
Case Courtesy Dr. Omar Kass Hout and Dr. Tibor Becske
Check out this highly skilled thrombectomy. A surfer with neck pain and dizziness, double vision, nausea/vomiting, left body numbness, mild weakness for for 3 days; prior episodes of neck pain/injury. Exam with left body and face mild weakness and right CN VI palsy
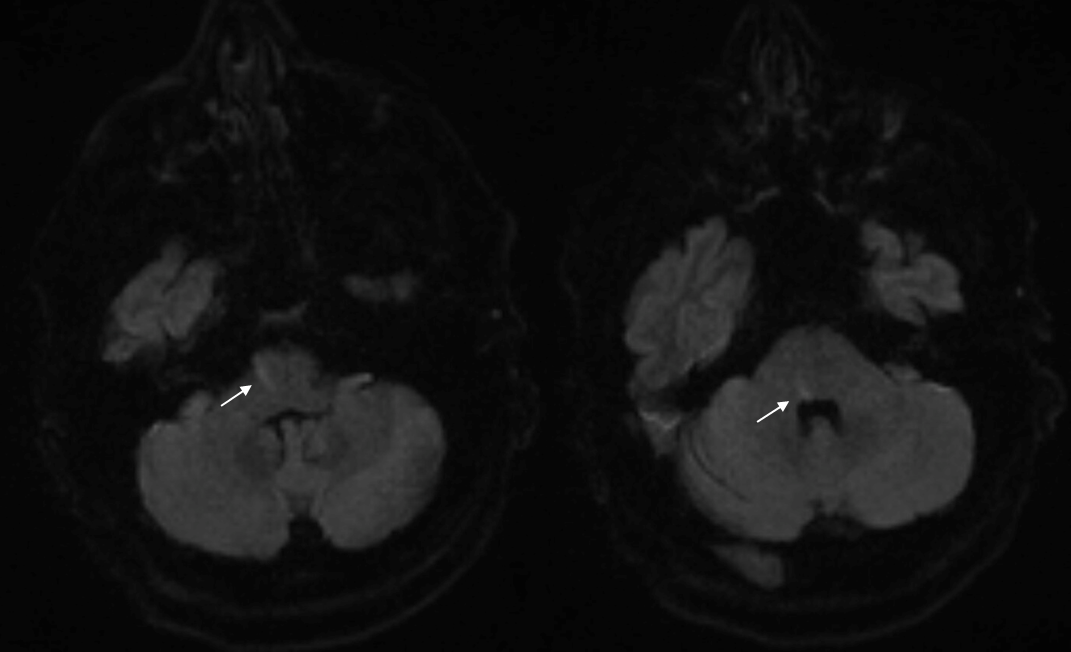
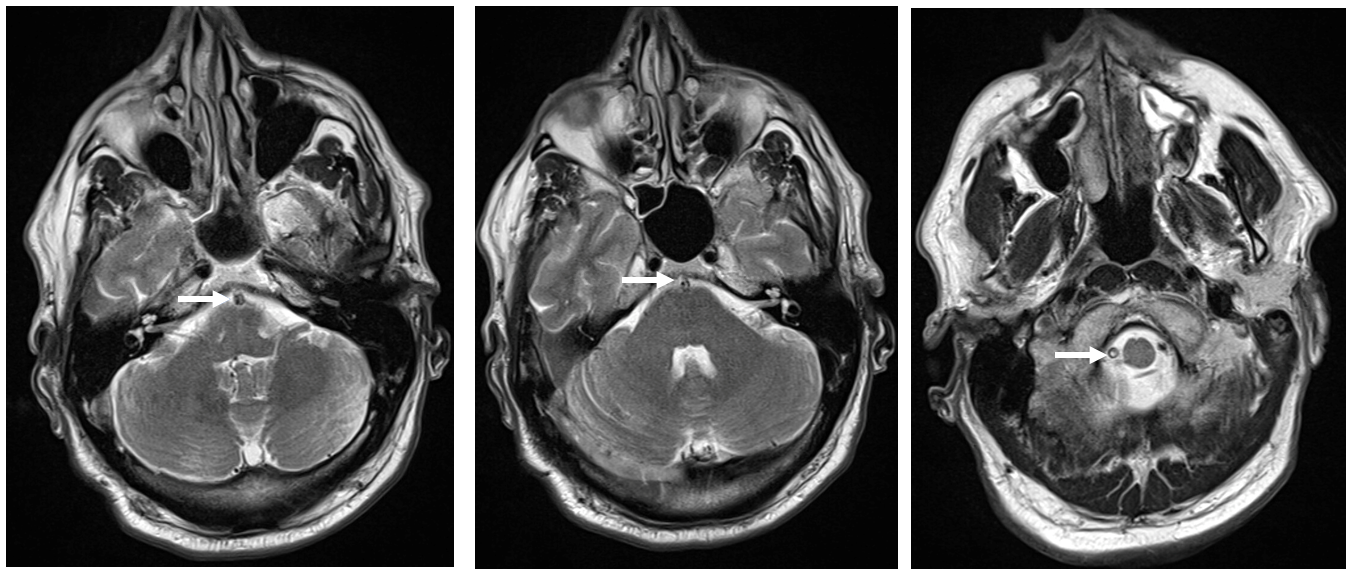
MRI
T2 with abnormal signal in vertebral artery and basilar
MRA; single vert supply to abnormal basilar artery
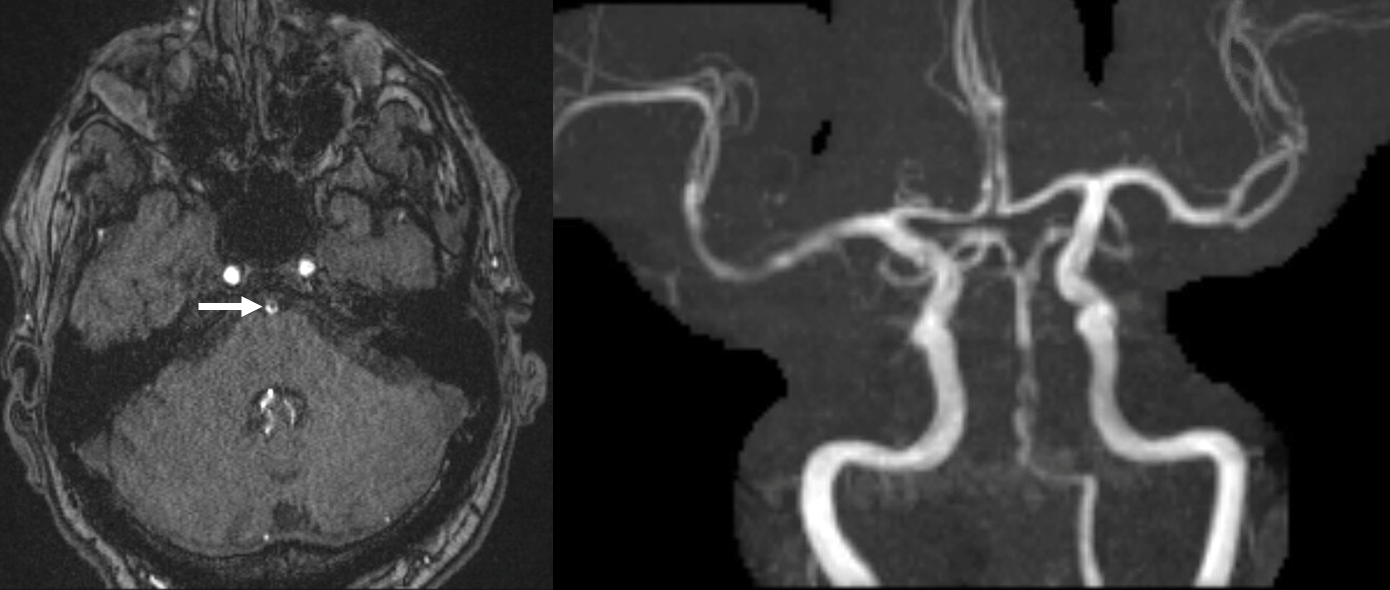
MRA neck. Both cervical verts look open

Not at all — these are not verts. Both cervical verts are closed. These are deep cervical arteries reconstituting the vertebrals at C1 level.
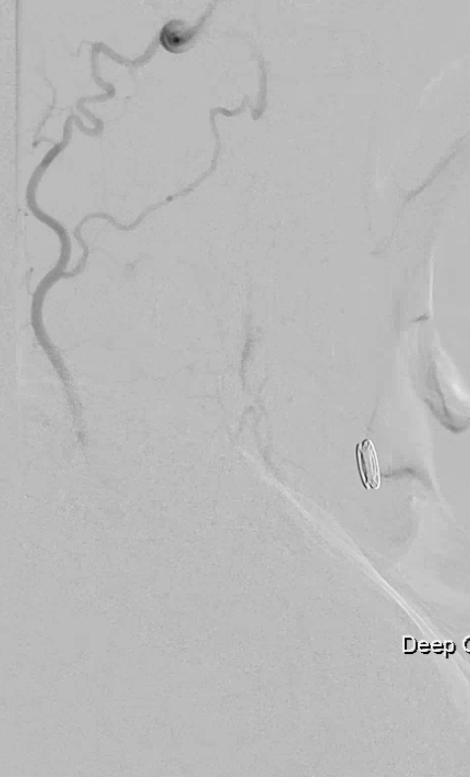
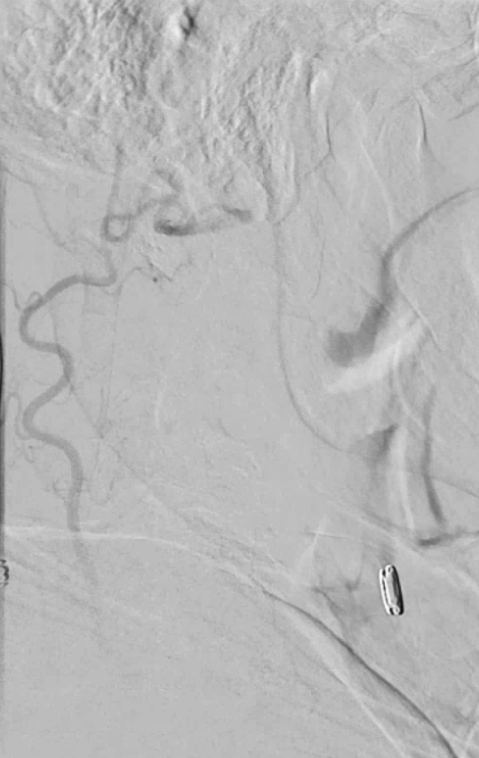
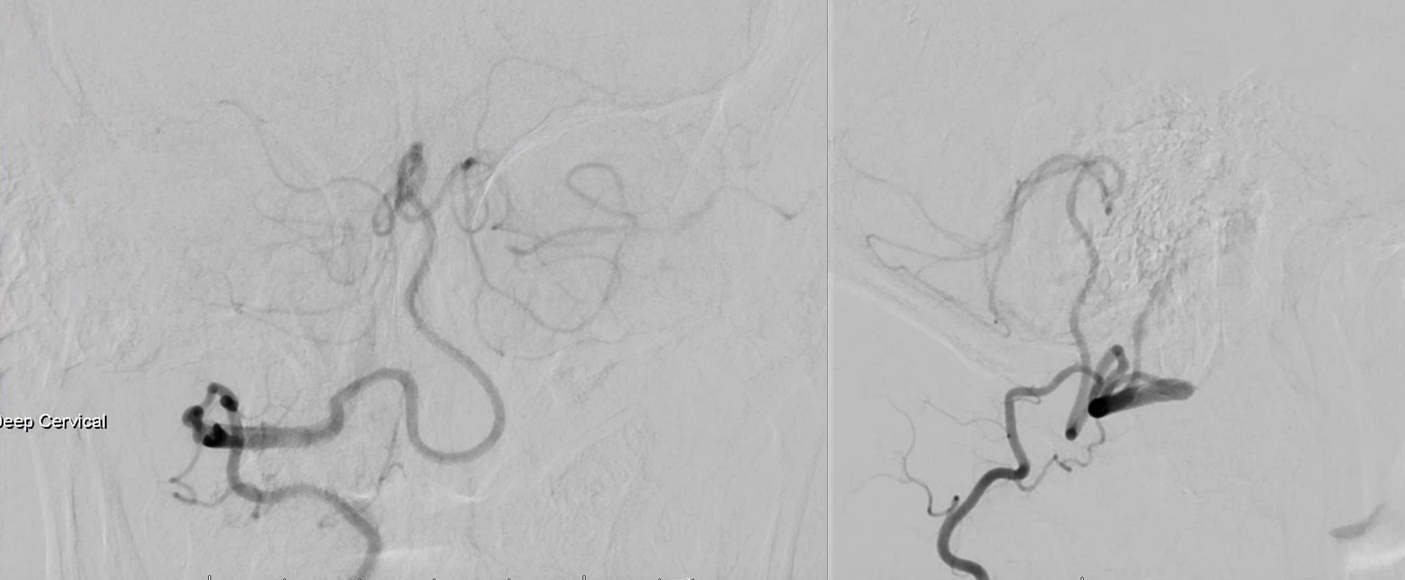
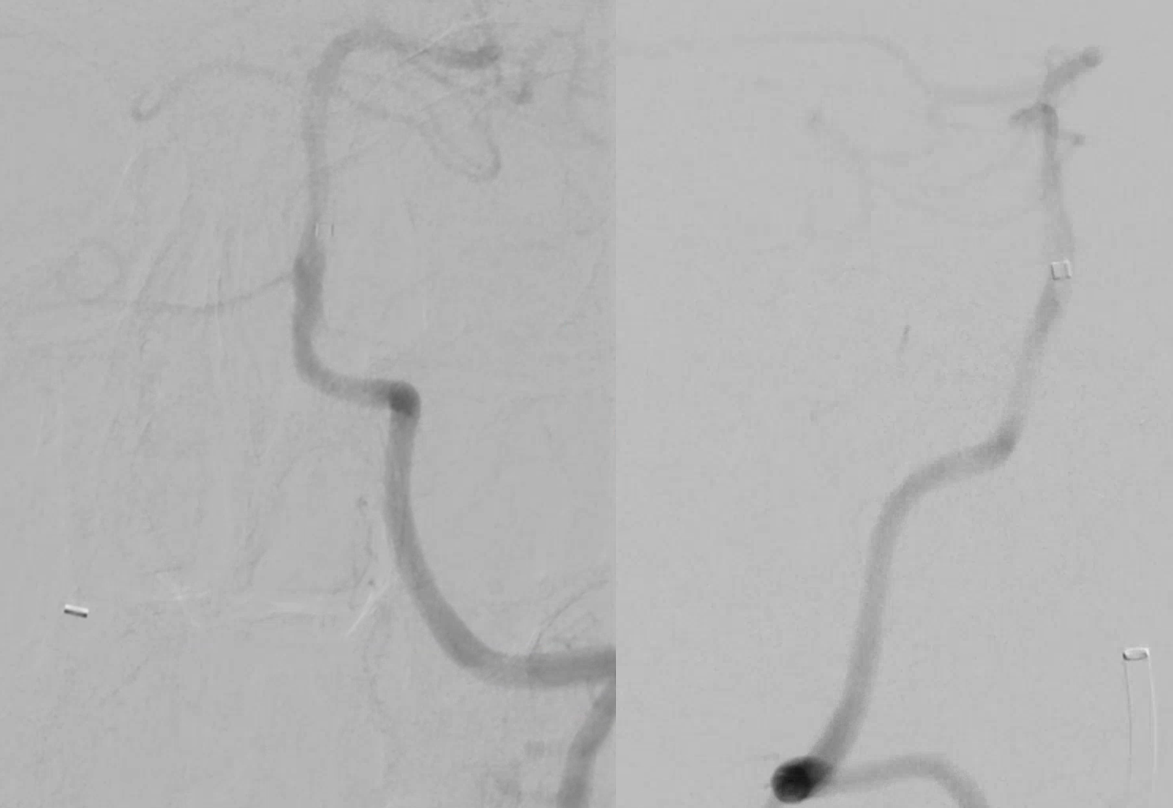
Angio left subclavian injection — left deep cervical reconstitution of vert at C1 level.
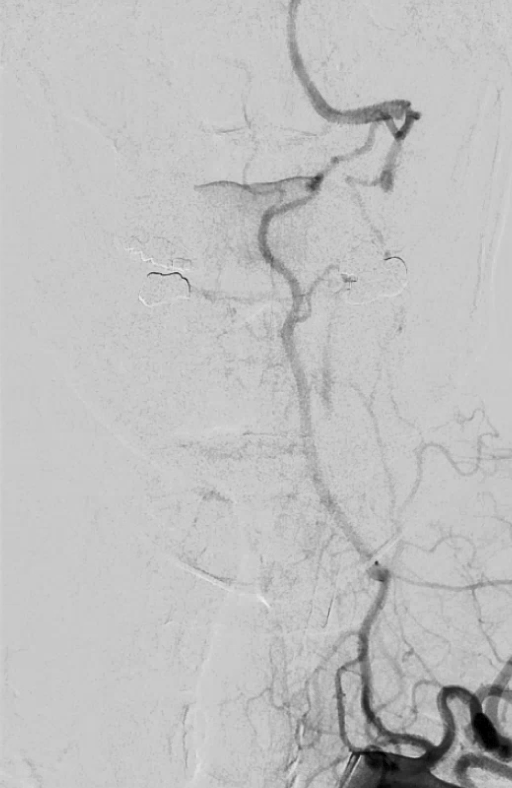
Lateral view
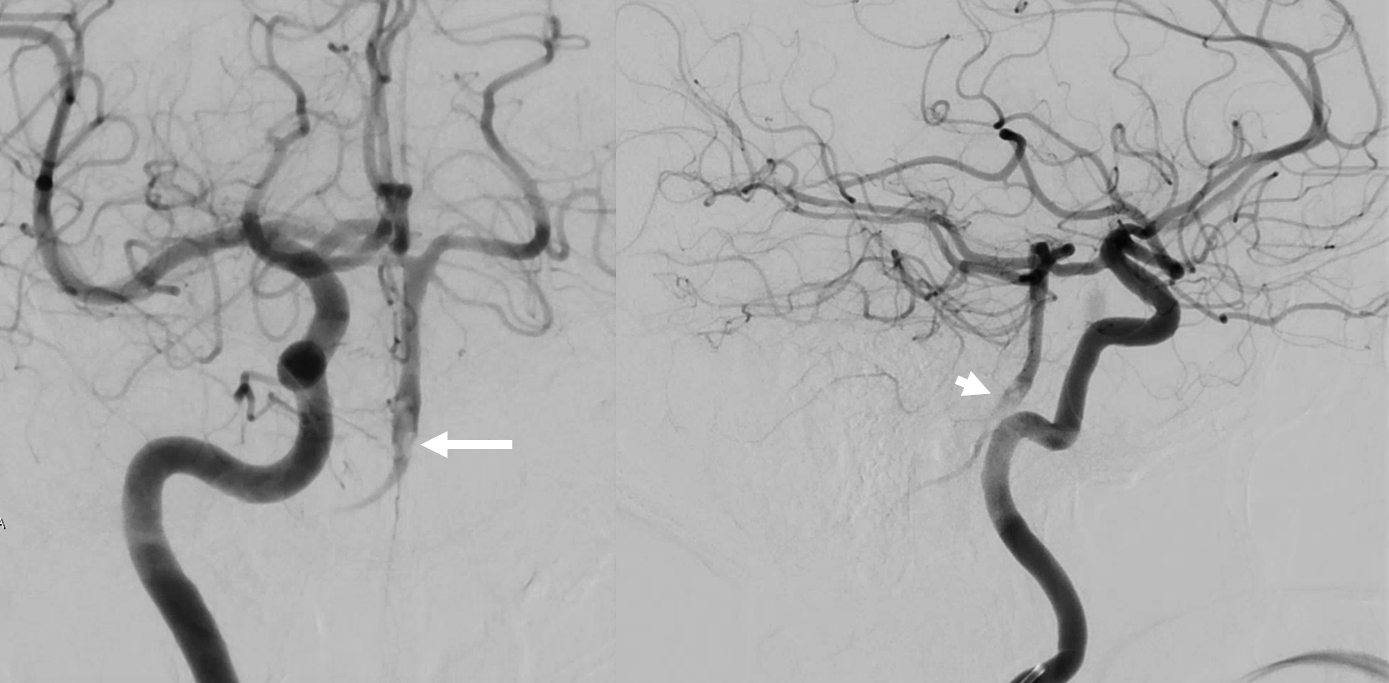
Cranial views show pieces of clot in the lower basilar

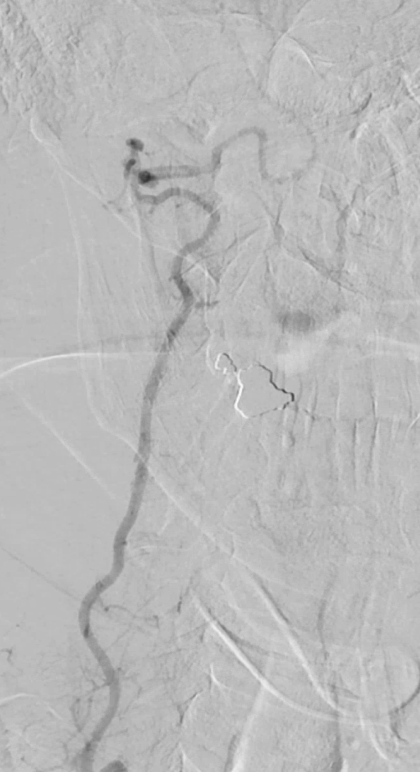
Right subclavian injection, deep cervical runoff

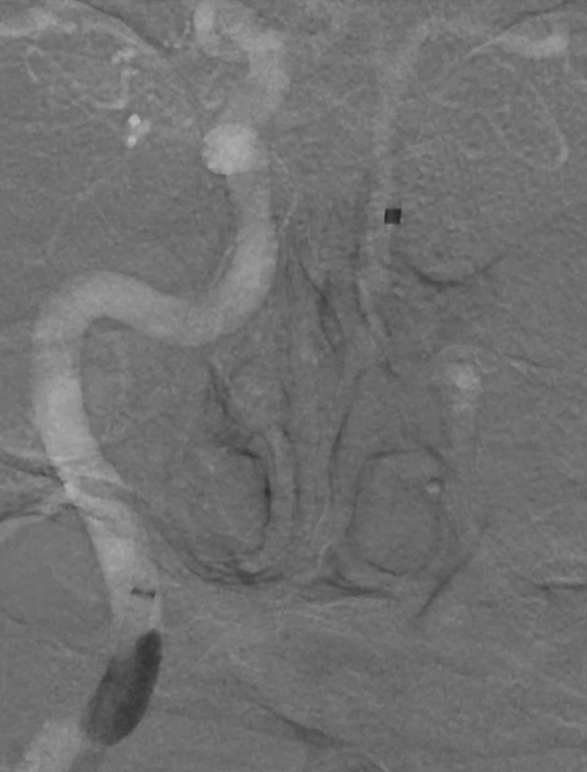
Right ICA — well-developed right PCOM retrogradely filling the basilar with same clot marked by arrows
Right deep cervical injections show same C1 level reconstitution of right vert, which terminates in the right PICA, as seen on MRA
Summary — bilateral cervical vertebral occlusive dissections, with adaptive collateral reconstitution of both verts by deep cervical arteries, with acute nonocclusive thrombus in the basilar
What to do? Medical therapy (anticoagulation) vs intervention considered. Intervention setup: Flowgate in right ICA, then Jet D with Marksman and Synchro 2 — however did not allow for Jet D to cross PCOM due to step-off
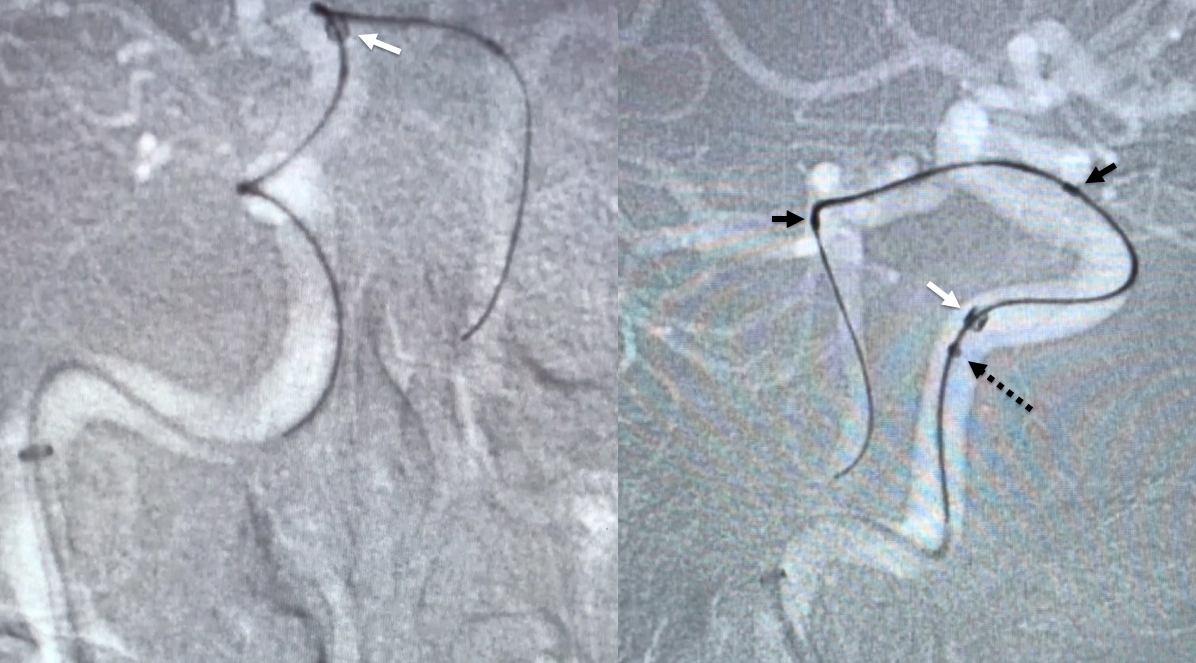
Next system: Jet D/ 3 Max / Prowler Select Plus 170 cm / Synchro 2 standard — minimizes step-off. Here it is below. Prowler markers are black arrows, 3 Max is dashed black arrow, Jet D is white arrow
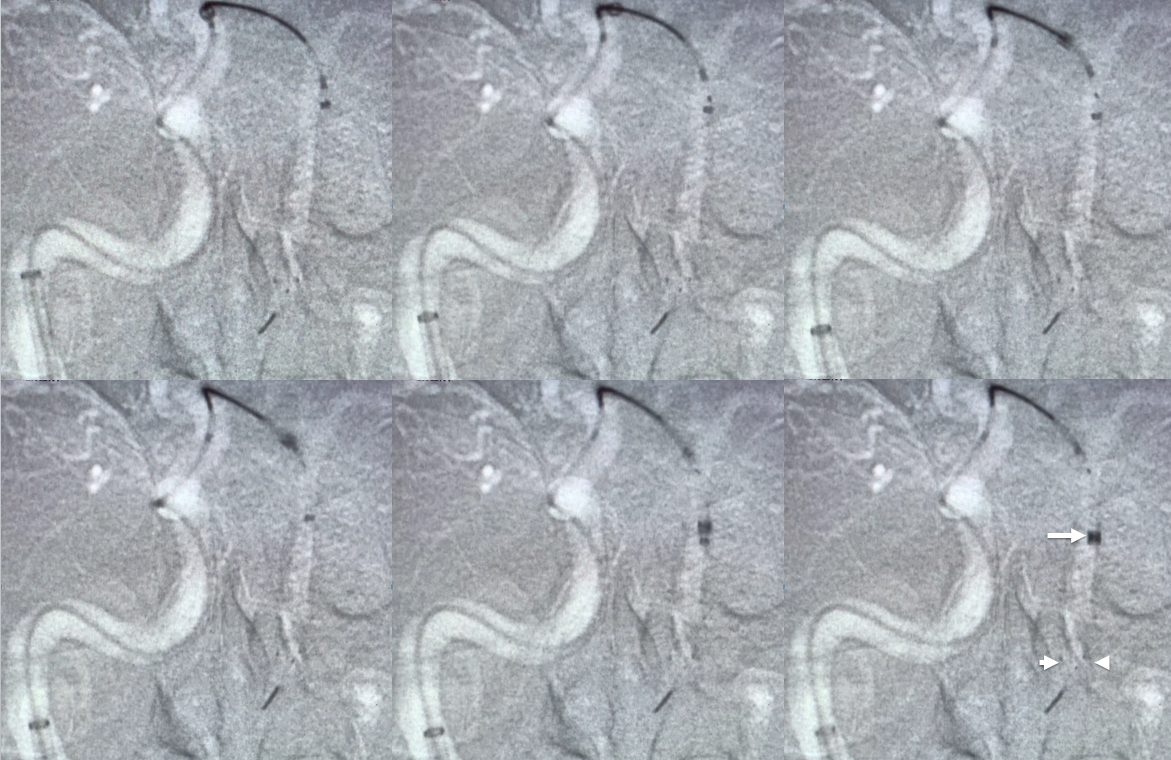
Frontal views. The basilar is catheterized with the Prowler, and an Embotrap 5×21 is deployed (white arrowheads in lower right image show markers) to help advance Jet D, with lower right image showing the Embotrap/JetD system in position
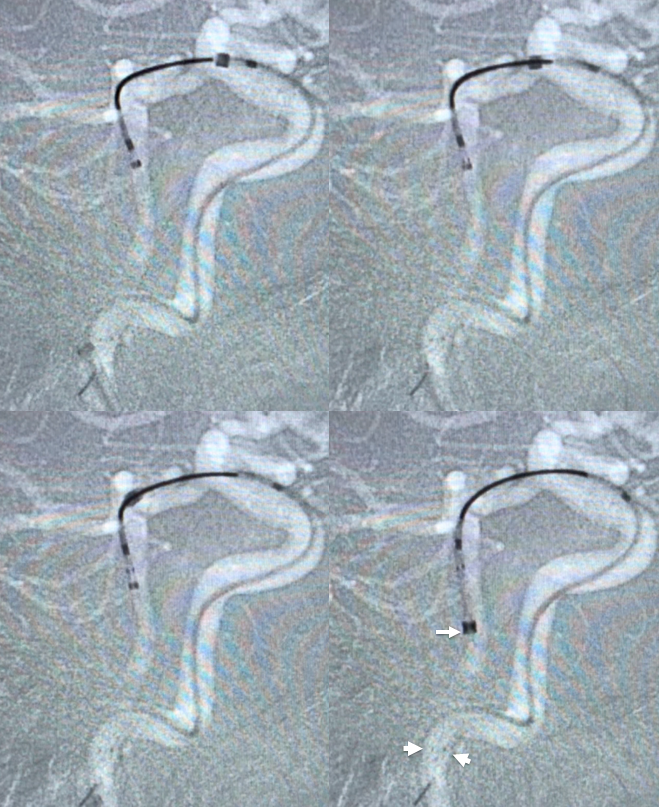
Lateral views of the same. Same arrows
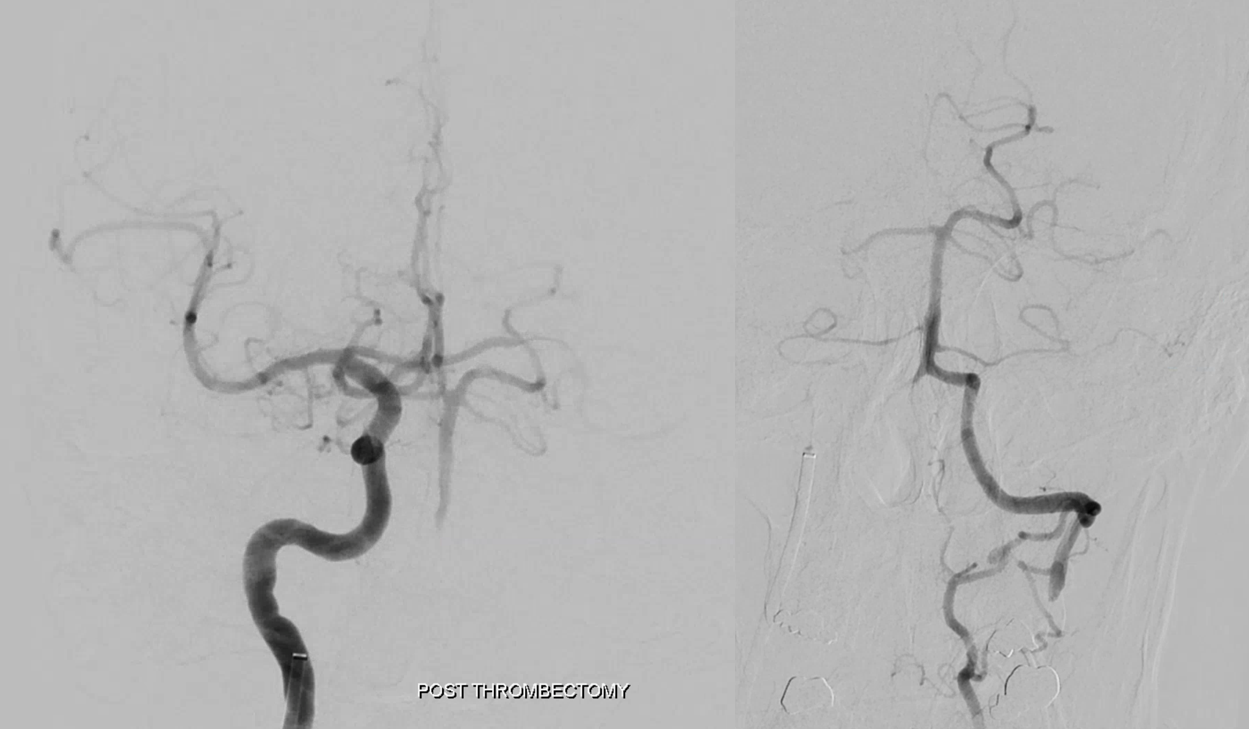
The Embotrap is retrieved into Jet D. Views post retrieval show successful clot removal
Finally, Jet D is removed, under aspiration of both Jet and Flowgate – belt and suspenders for sure
Post
Post delayed CT with small distal posterior inferior temporal branch infarct
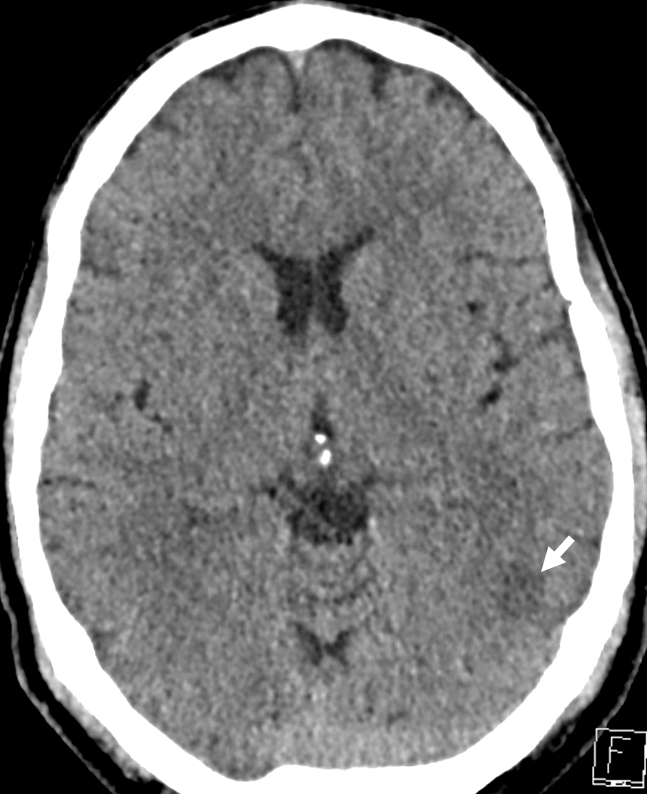
Final NIHSS = 0 with resolution of ophthalmoplegia and dizziness
Final etiology: acute vert dissection with emboli vs chronic dissection with stasis. Overall clinical and angiographic picture favors acute dissection. Discharged on Apixiban and Surfingban. Great example of difficult and successful thrombectomy, and very nice cervical anatomy also