
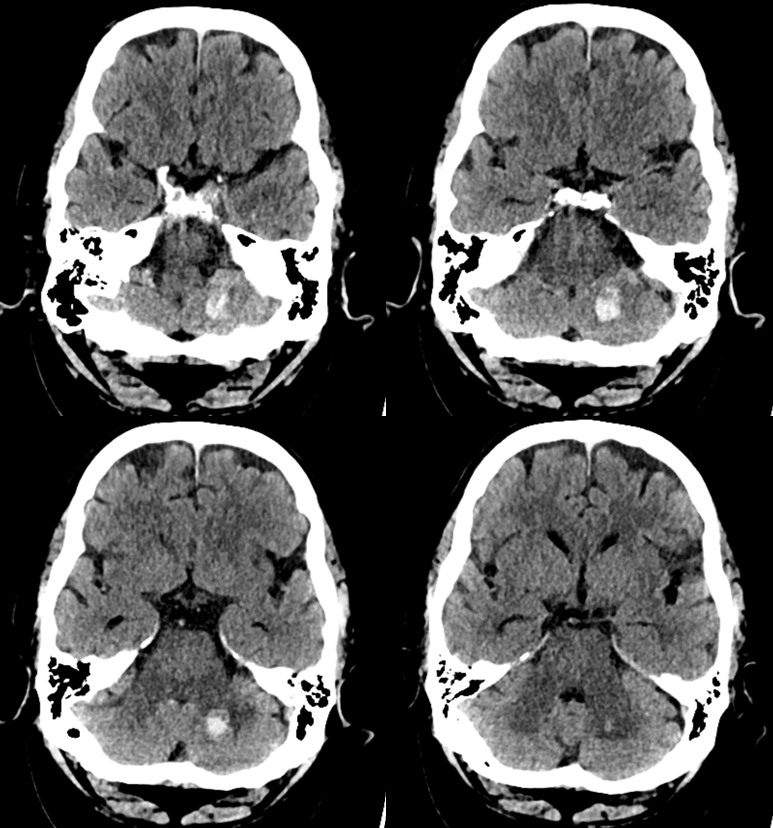
Another beautiful demonstration of dural fistula hemorrhagic pathology being related to venous congestion. The power of Cognard classification to predict hemorrhage as it relates to venous congestion has stood the test of time. These hemorrhages are overwhelmingly supratentorial, with infratentorial / posterior fossa ones being very rare. Why? Simply because posterior fossa veins are extremely redundant and even when ipsilateral dural sinuses are occluded there are usually plenty of alternative outflows. If the outflow is however compromised, the cerebellum will bleed just like any other part of brain. We came across one recently, presenting with headache and dysmetria
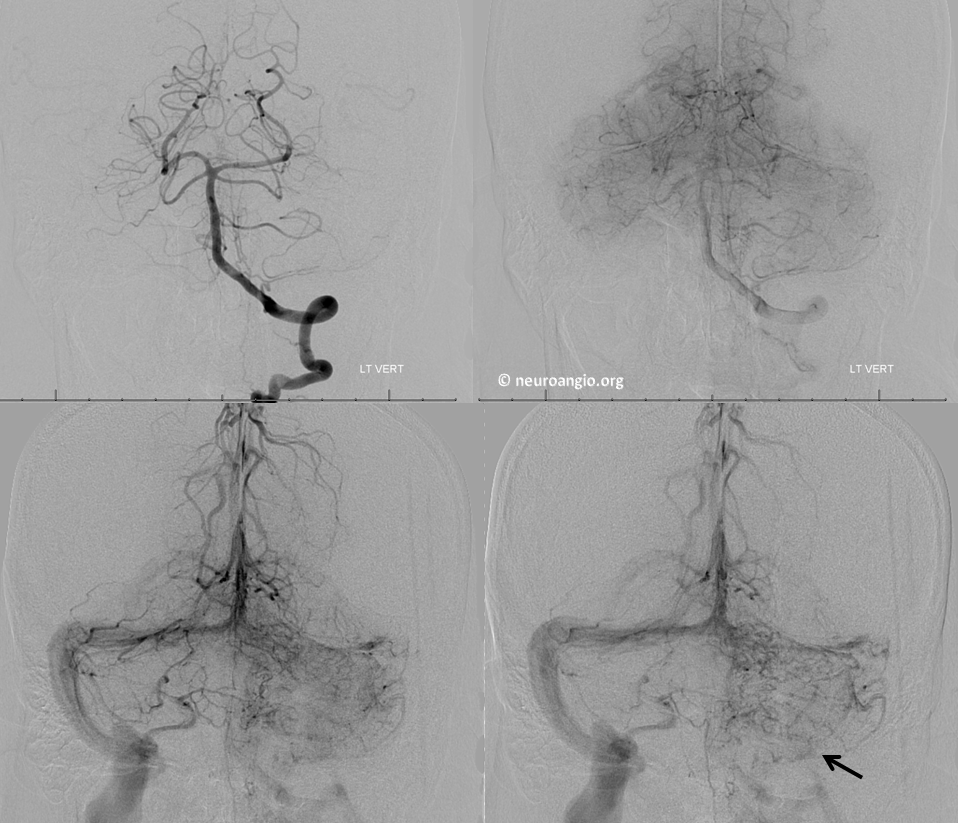
Vertebral injection, frontal views. The left transverse/sigmoid sinus is out and there is pretty impressive and equally rarely encountered venous congestion of the left cerebellum. A very faintly visible left inferior petrosal sinus is present (black arrow)
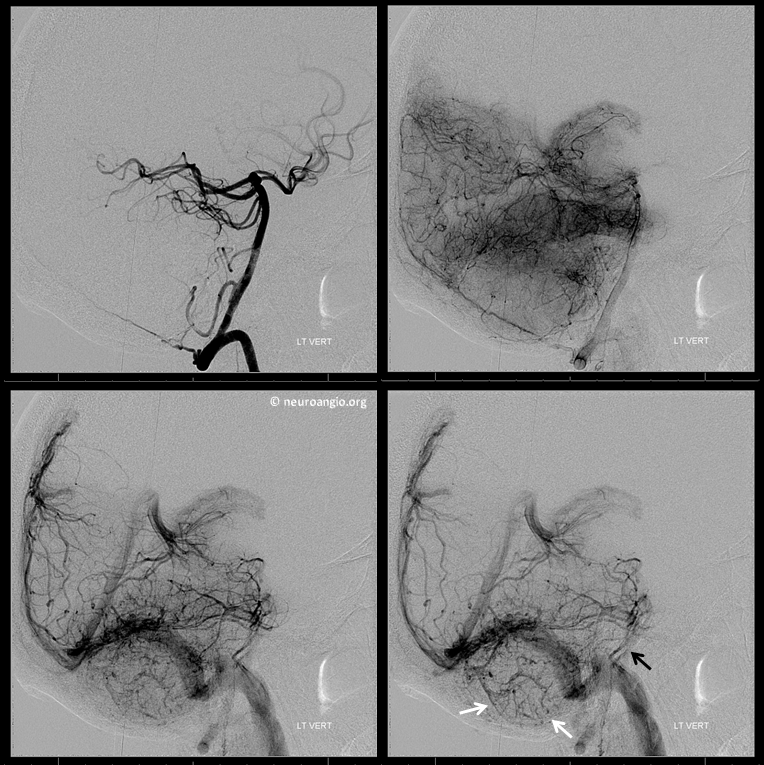
Lateral views. Notice ectasia of the cerebellar veins due to venous hypertension (white arrows). Paired petrosal sinuses (black arrow) speak to presence of left-sided one in case you did not believe me on the frontal view
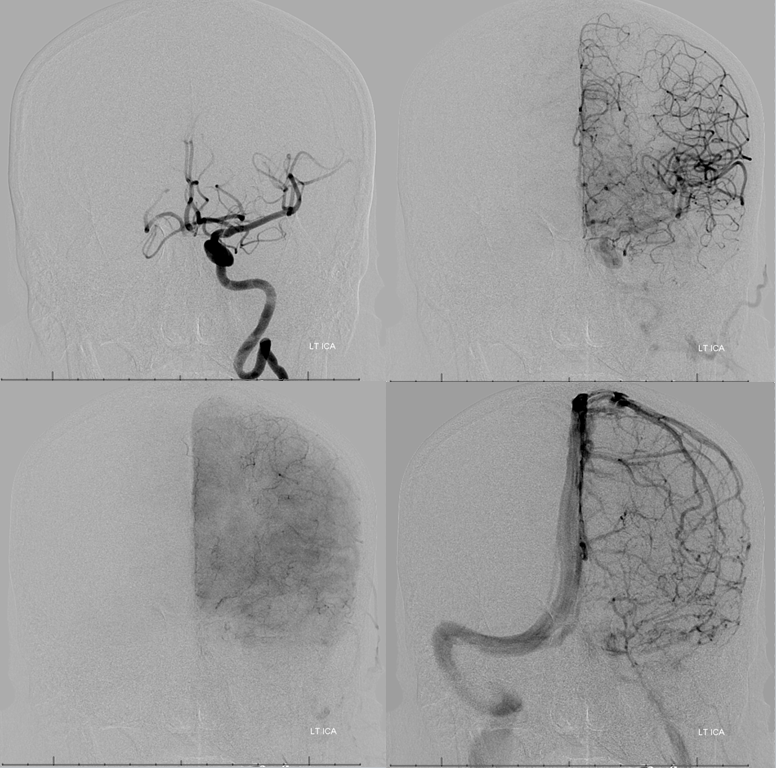
Left ICA also shows lack of left-sided sinuses. Notice lack of right inferior petrosal sinus opacification (of course its present as we see on vertebral injection). You can see the left petrosal sinus though.
Lateral views. Left petrosal sinus is marked by black arrow. Is this petrosal sinus business that important? Not really. But it is important to understand the anatomy completely to see why this patient hemorrhaged. Even this petrosal sinus the brain has to share flow with the left supratentorial brain (and the fistula, as we will see)

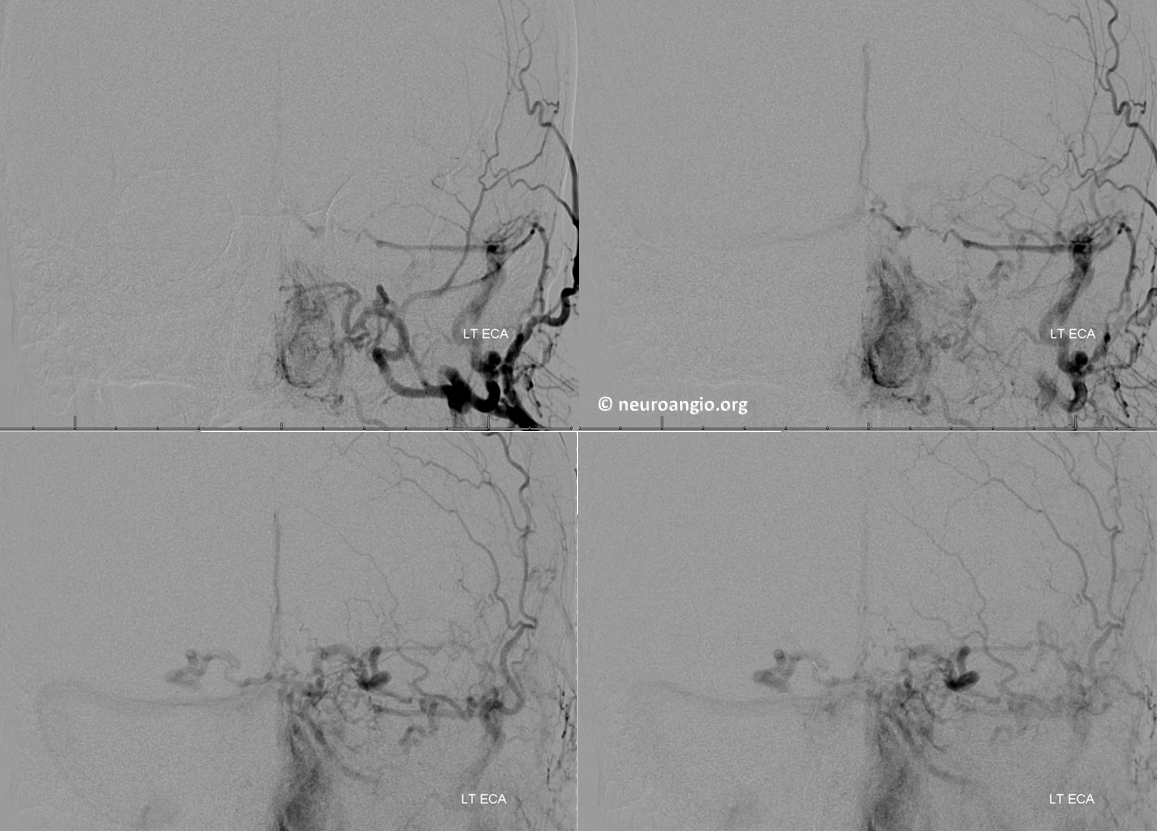
Left ECA injection, frontal view. There is a trapped sigmoid sinus dural arteriovenous fistula present. Drainage is difficult to assess here. For example, the superior ophthalmic veins are opacified in normal antegrade fashion from the IMAX, as will be seen on the lateral views.
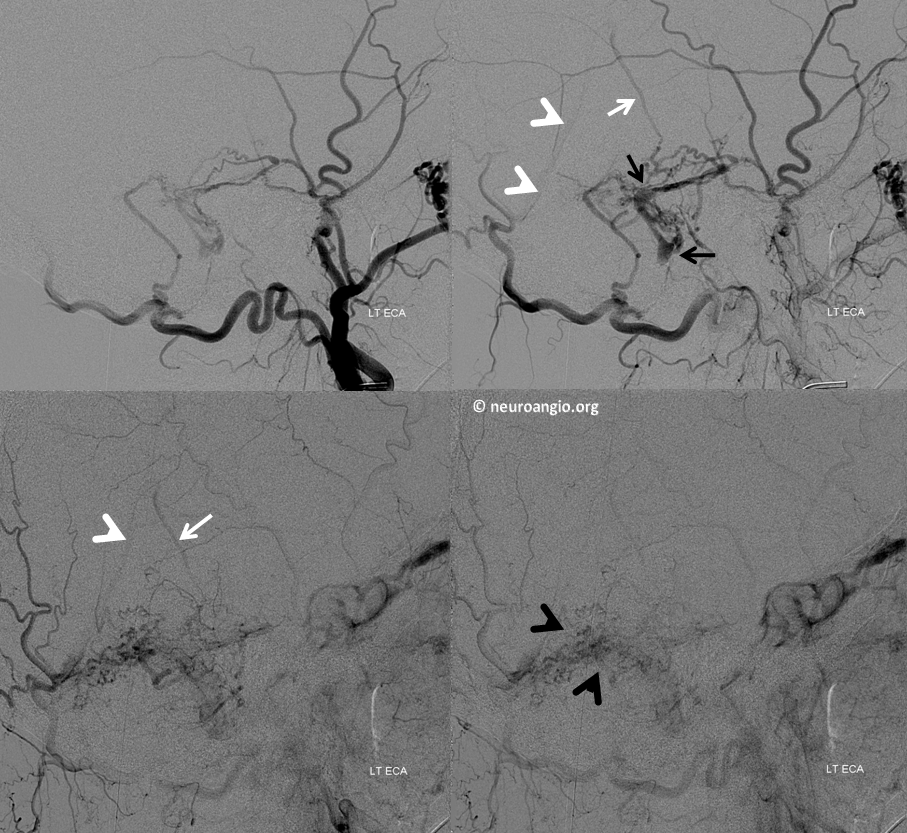
Lateral ECA view is the money shot. The fistula is supplied by the occipital and the MMA (not labeled, you should know by now). The sigmoid sinus is occluded proximally and distally (black arrows). What is exceptional here is lack of adequate venous drainage, causing tremendous (relatively speaking, for the size) cerebellar venous congestion (black arrowheads). The superior petrosal sinus is also trapped (not labeled). The only drainage proceeds via the precentral cerebellar vein (white arrow) into the straight sinus (white arrowheads).
Conclusions: So, as usual, location of venous congestion dictates location of pathology — hemorrhage in this case. There is nothing magical about posterior fossa “resistance” to venous congestion — it is only resistant to the extent that its venous system is highly distributive. When it fails, symptoms will arise just like anywhere else
See also Techniques Dural Fistula Ebolization Page and many other dural fistulas on the Cases page
Further reading: Satoh, et al. Five cases of posterior fossa DAVF related hemorrhage
https://www.ncbi.nlm.nih.gov/pubmed/11235946