
The balanced, distributed nature of venous system is highlighted on multiple venous pages, including venous sinuses, superficial venous system, and deep venous system.
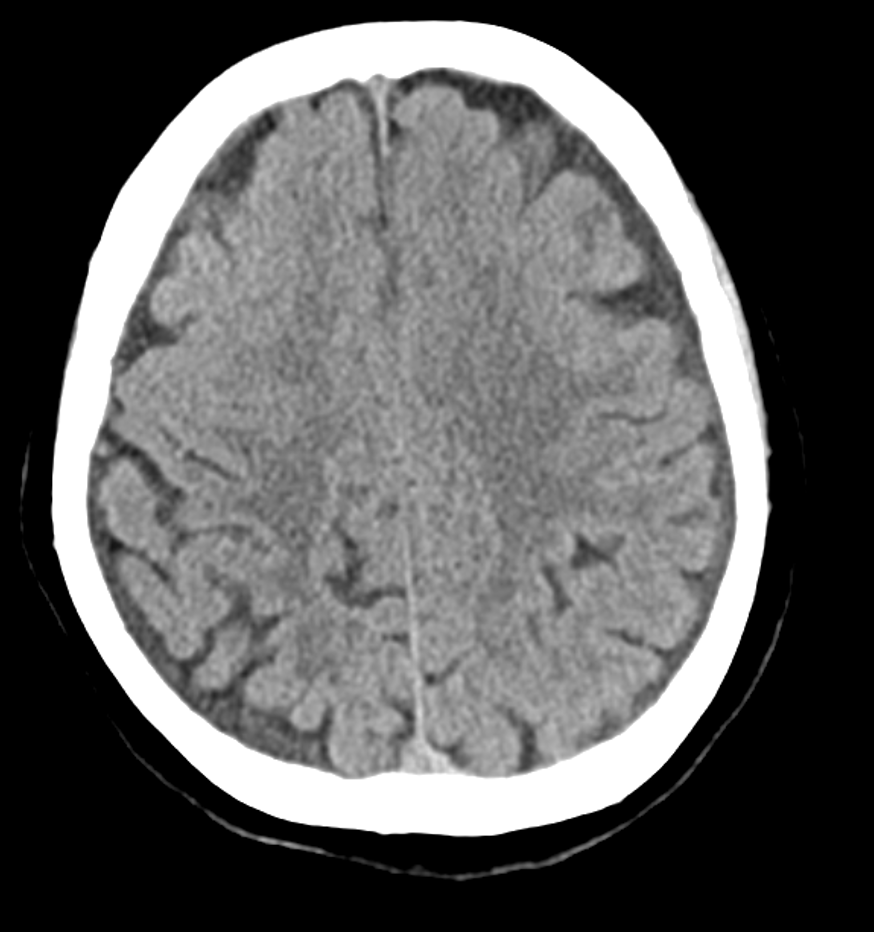
Here is a quick example, in a patient with venous sinus thrombosis. Why do some patients do well and others don’t. The answer is often in detailed, functional analysis of imaging — to understand collaterals and put everything togeher. Initial CT
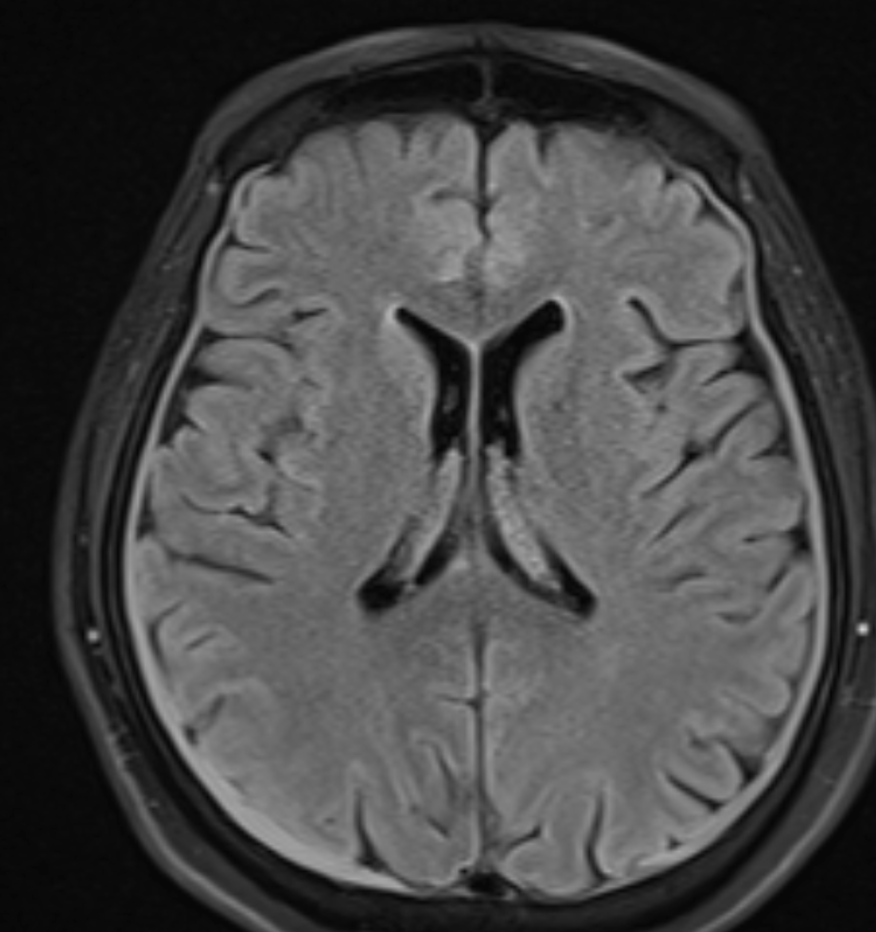
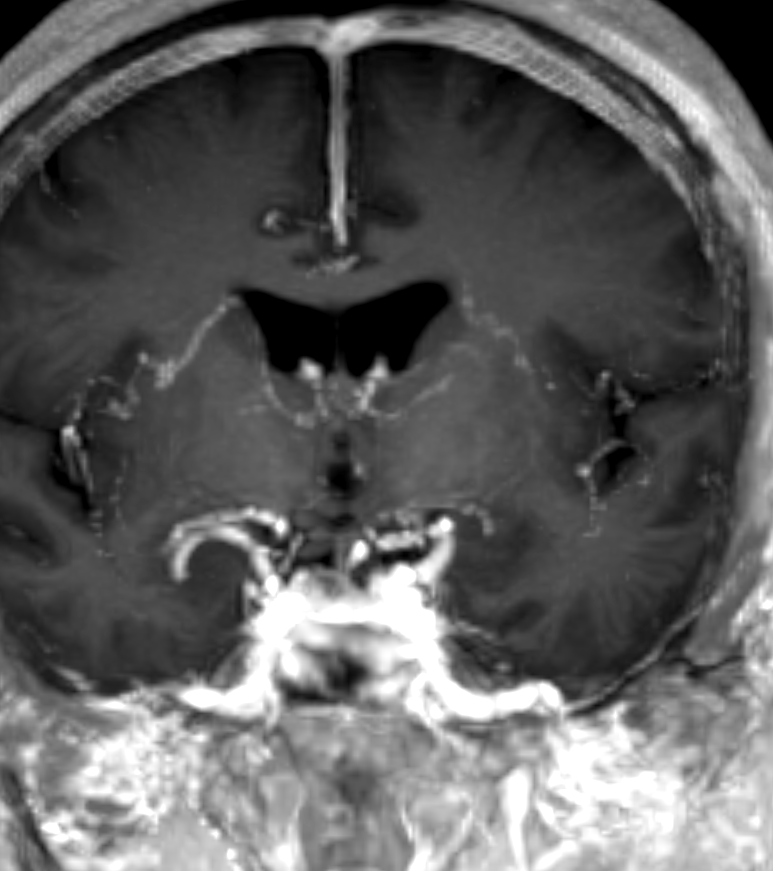
MRI. Apart from headache, patient is asymptomatic. Presumably, the headaches are from venous thrombosis.
MRV — important to analyze this in detail. Look where thrombus is — anterior and mid-SSS — a bit unusual. The proximal SSS is open. Plus right sigmoid sinus, left transverse and distal / mid-sigmoid sinuses. The proximal right sigmoid is open.
A few days after heparin therapy

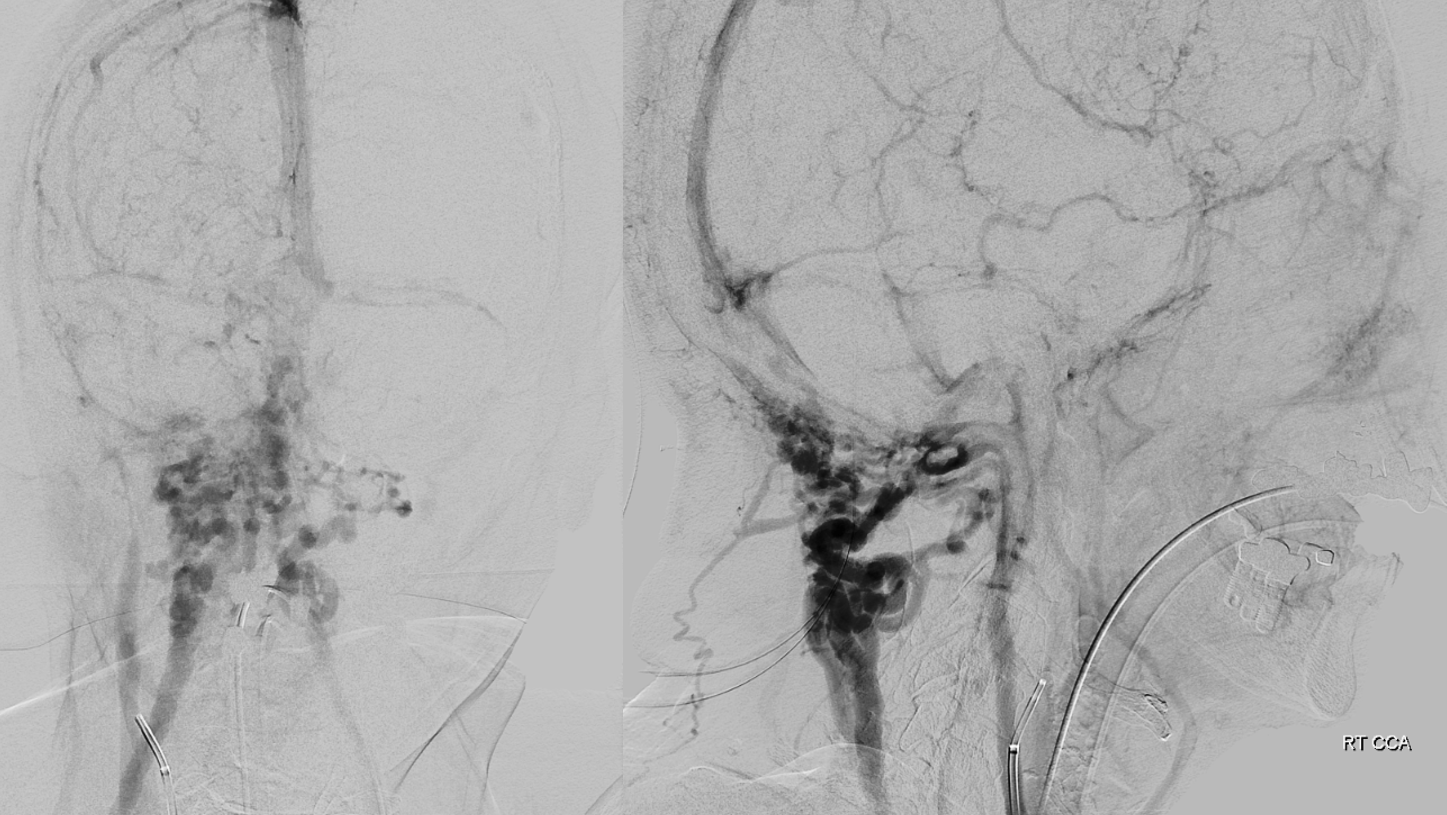
Angio in context of MMA embo — one of main imaging goals is to have all studies consistent, and to reflect clinical state. This is an example. Angio venous phase shows congestion of frontal lobe due to occlusion of anterior/mid SSS. Venous flow is routed via surface veins into the functional Trolard system draining into patent SSS. The bulk of SSS drains via a life-saving emissary vein (dashed arrow) below the torcular into the suboccipital venous plexus (solid arrows). The sylvian system is hypoplastic. The correspondingly dominant anterior part of the basal vein drains via the lateral mesencephalic vein into the superior petrosal sinus and then into the patent proximal sigmoid sinus (no arrows) — see Basal Vein page
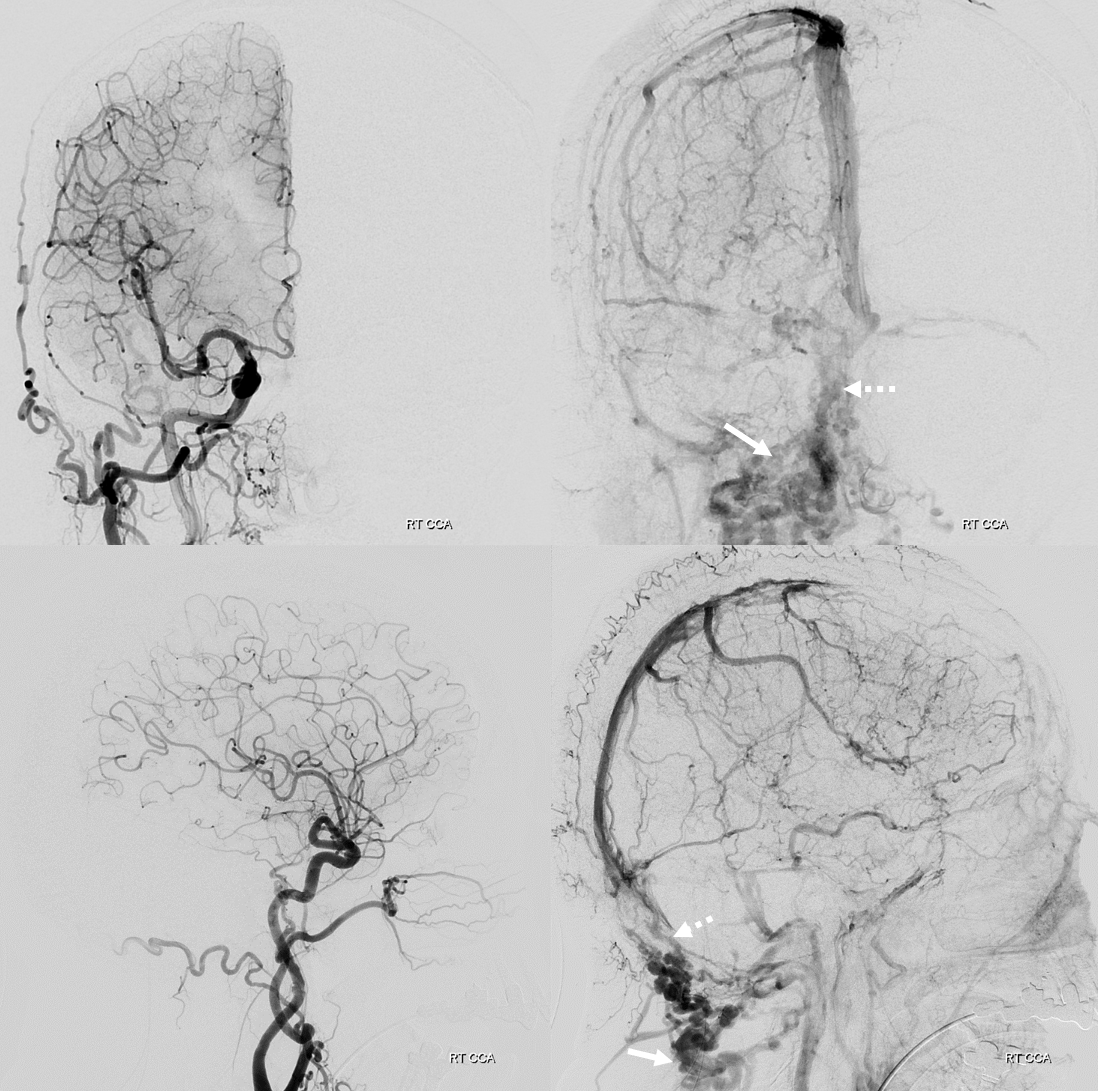
Better look at those suboccipital veins below.
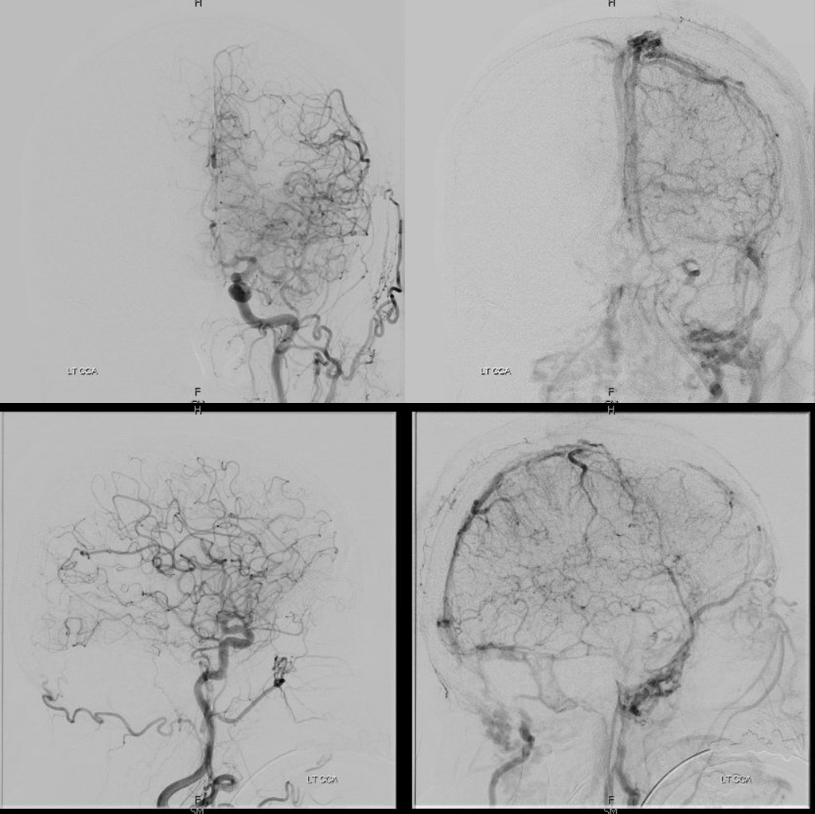
On the left, the superficial sylvian veins are well-developed, and drain into cavernous sinus. These dominant sylvian veins collect convexity outflow that cant reach the SSS — frontal lobe for example. There is reversed flow in the SOV, which is often the case with venous sinus thrombosis, as it helps drain brain also, and is often a large enough vein to carry significant flow. The sigmoid sinus, which is less filled with clot than on the right, continues to drain in antegrade fashion. Because the sylvian veins are so dominant, there is less reliance on SSS for the left hemisphere, and we see those suboccipital veins less here.
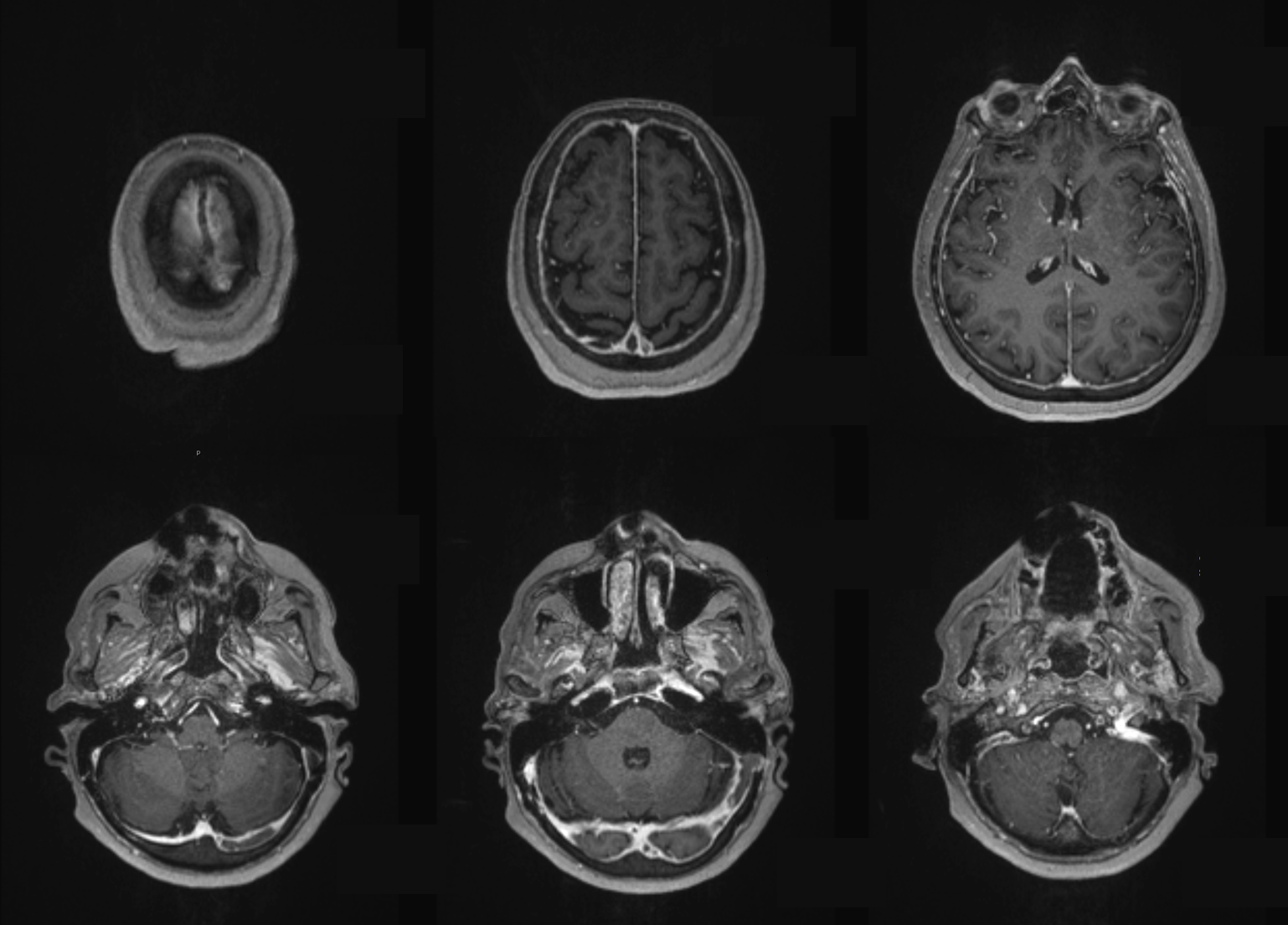
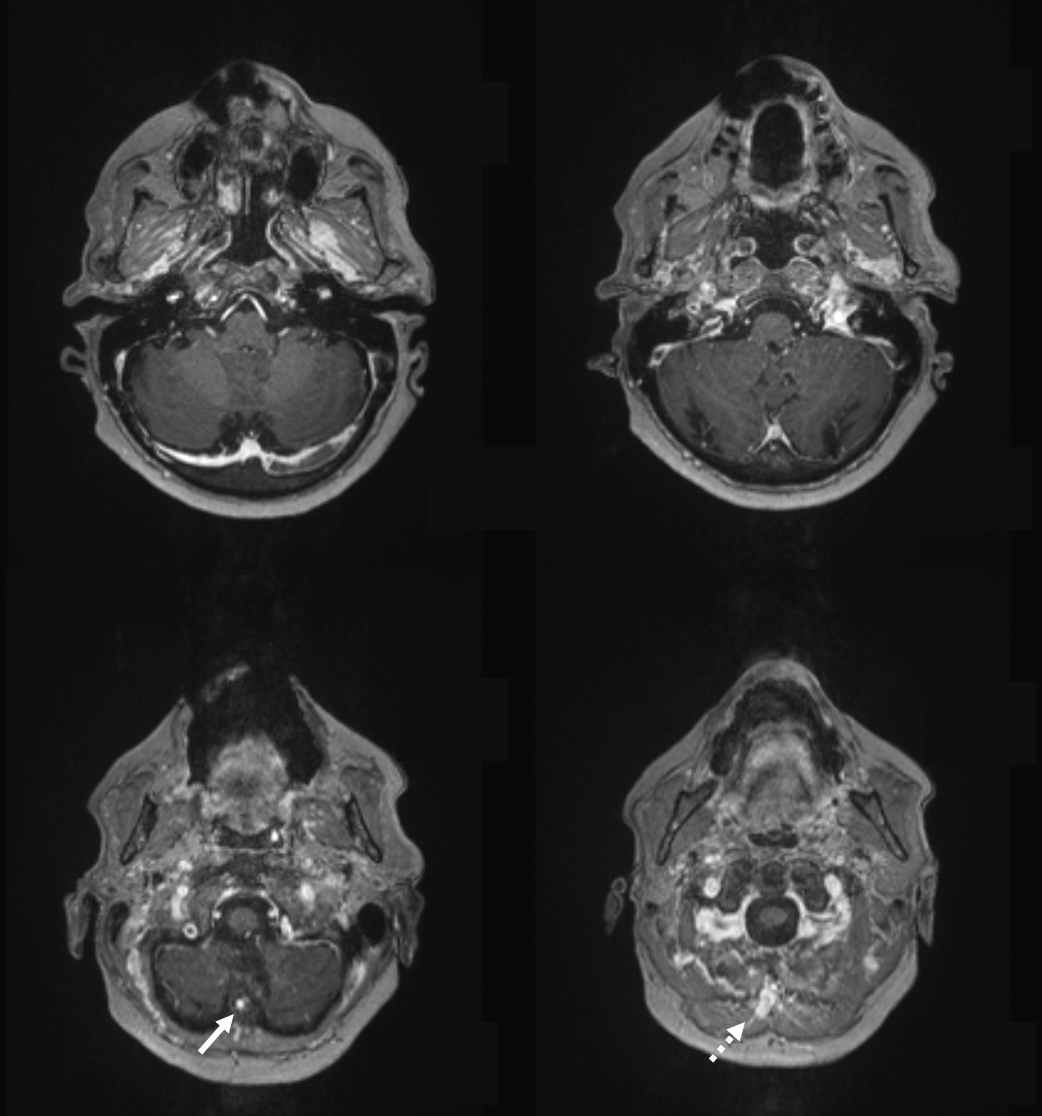
Retrospectively, looking at MRV again, once can see the same emissary venous channel and suboccipital veins on MR. It is important to appreciate how small emissary veins can serve important roles, draining very large volumes of venous egress, and how inconspicuous they might be.
The same on non-contrast head CT — it is indeed a small opening — compared to the ones frequently seen at sigmoid level — small but look at what it can do…

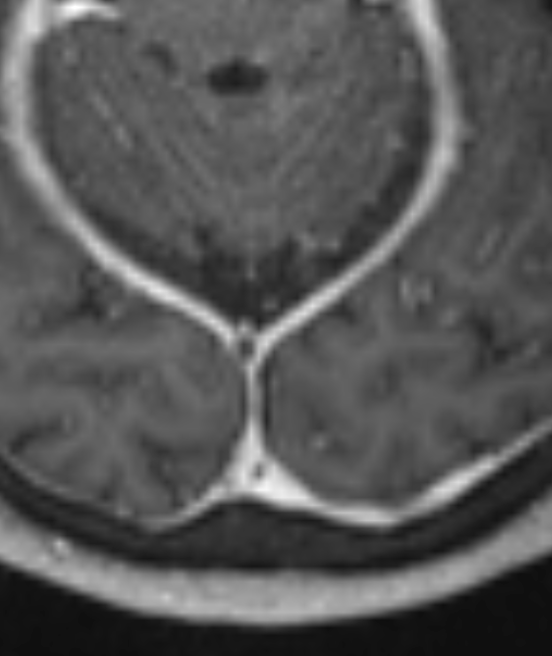
Now, gets even better. Two months later, patient is doing great. Follow up MRA shows resolution of most clots, with subocclusive residuals in SSS and left sigmoid sinus — happens often, it becomes a scar-like structure. However, look at these transmedullary veins —
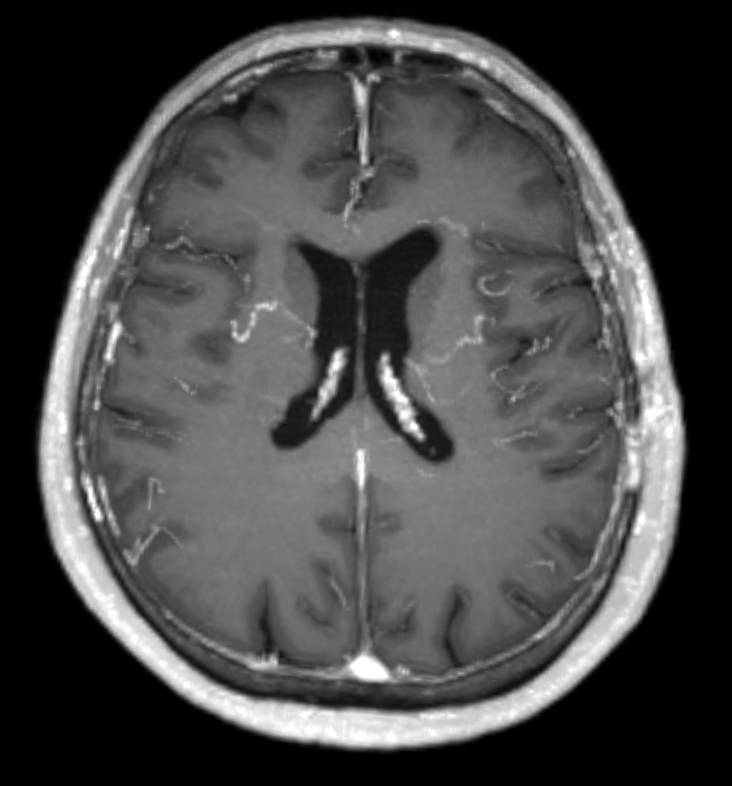
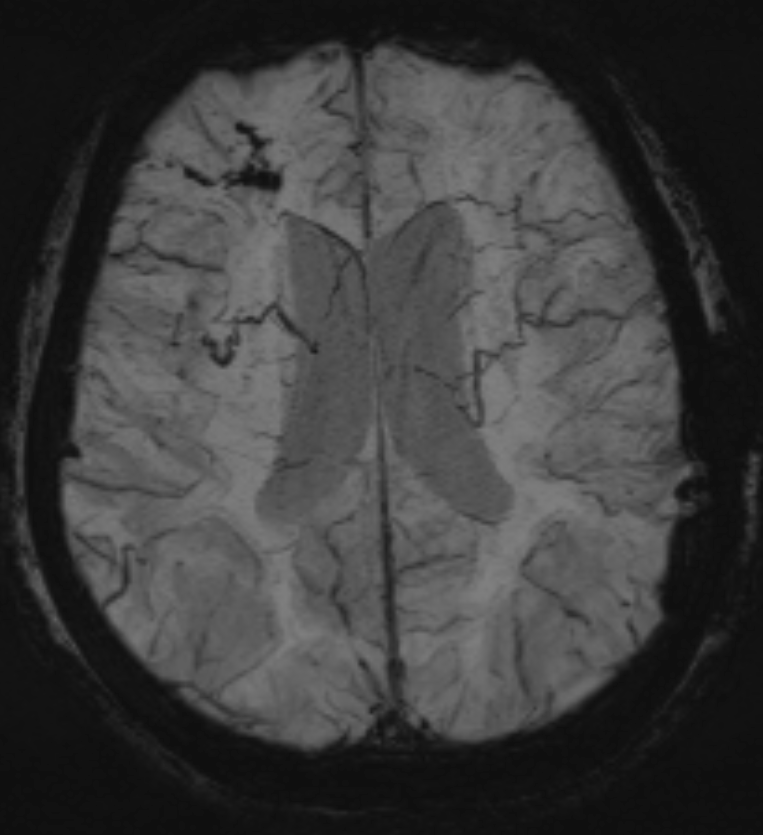
Why are they like this? Excellent example of venous collateral development — there was occlusion of the straight sinus also — see angio images above — transmedullary veins are important collateral route for the deep system. the image below is from time of thrombosis.
Conclusion: Even without fancy imaging one can make a lot of conclusions and correlations. It all makes sense — and its not just cute — its important to understand why some patients with SSS do well and others don’t. It all has to do with availability of alternative outflow.
Check out those venous pages, including venous sinuses, superficial venous system, and deep venous system.