
We have come a long way in understanding of how to treat dural fistulas. This is particularly important in places like torcular, where sinus sacrifice is usually not an option, and effective transarterial embolization can be challenging. The superselective transvenous common collector / venous pouch embolization is the optimal strategy in the tocular — preserving the confluence with fairly high efficacy of occlusion. Certainly doesn’t work every time, but we believe its an excellent strategy.
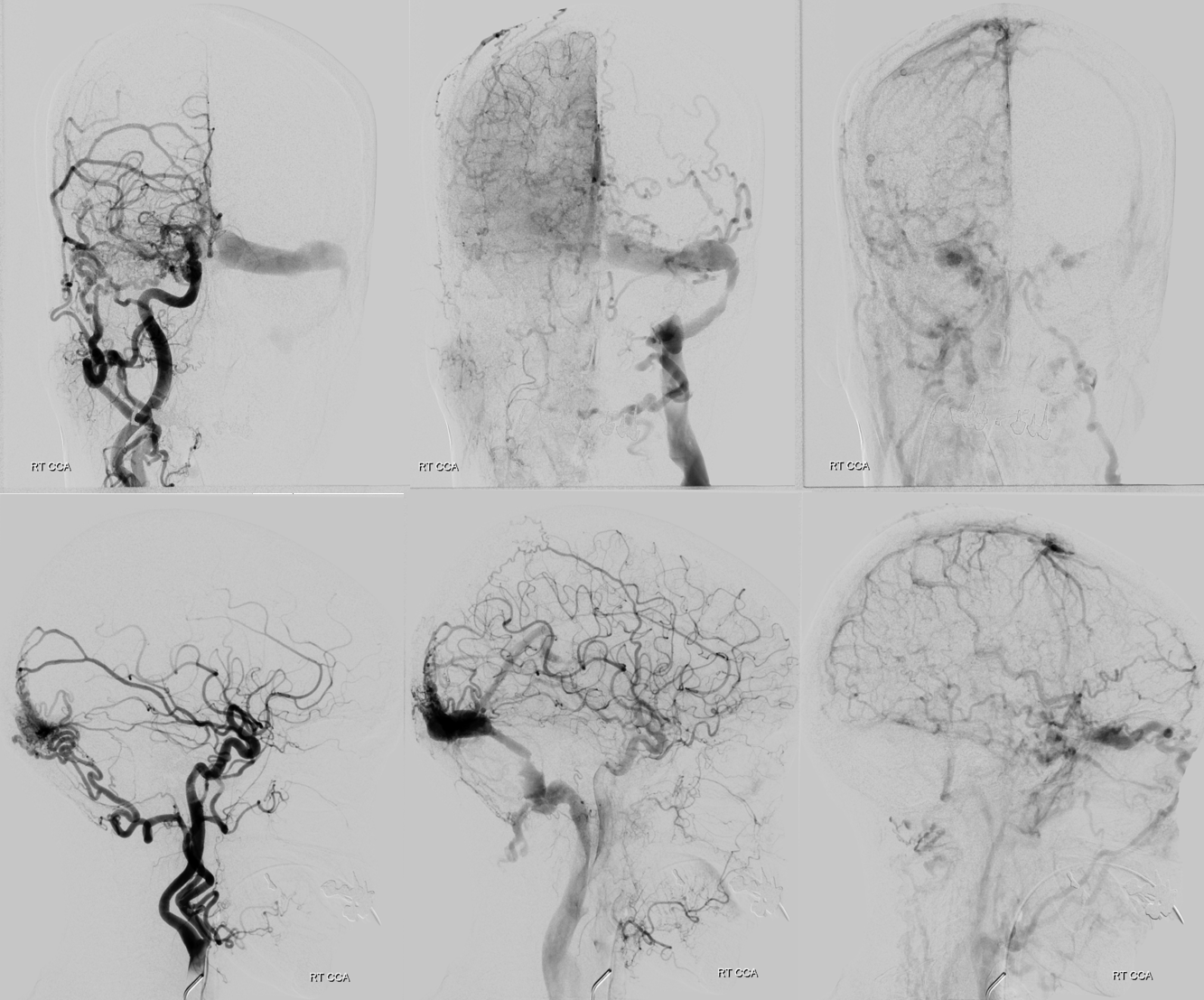
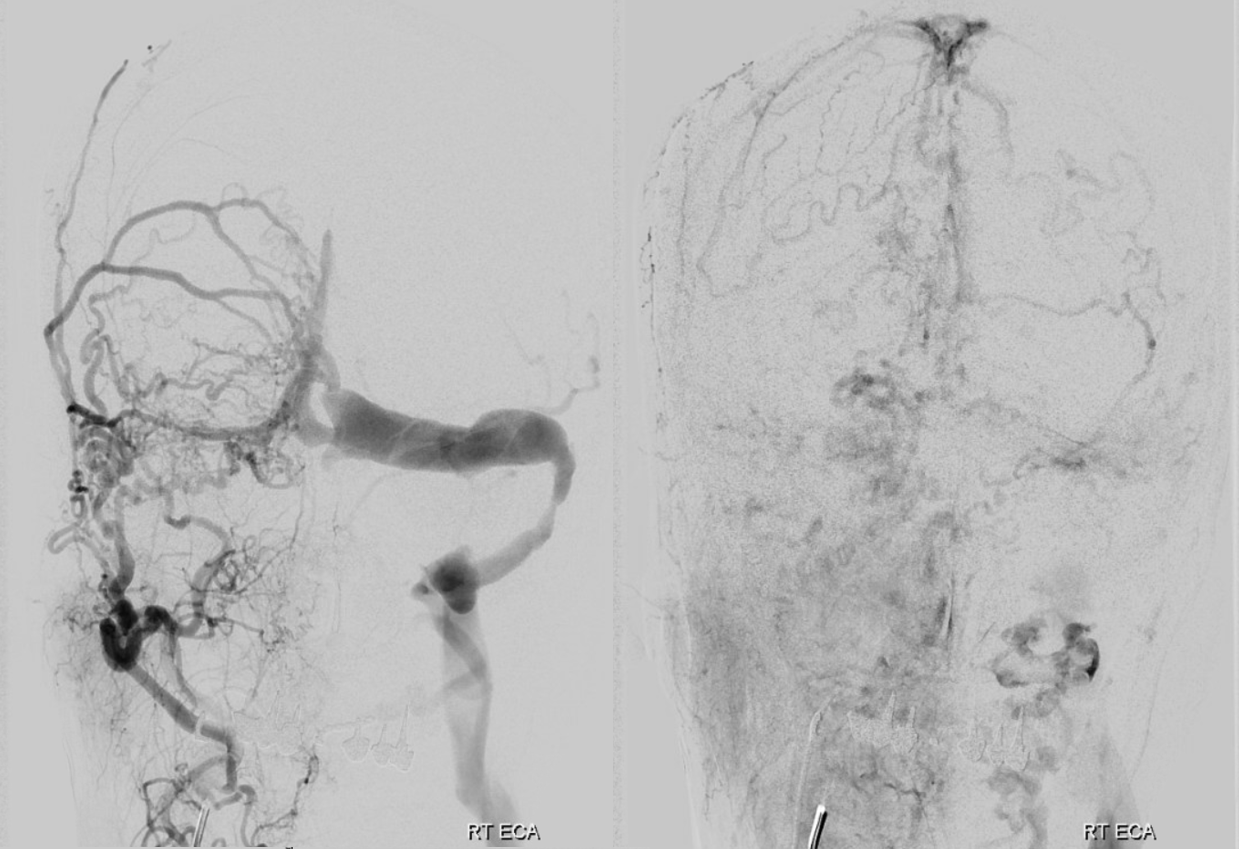
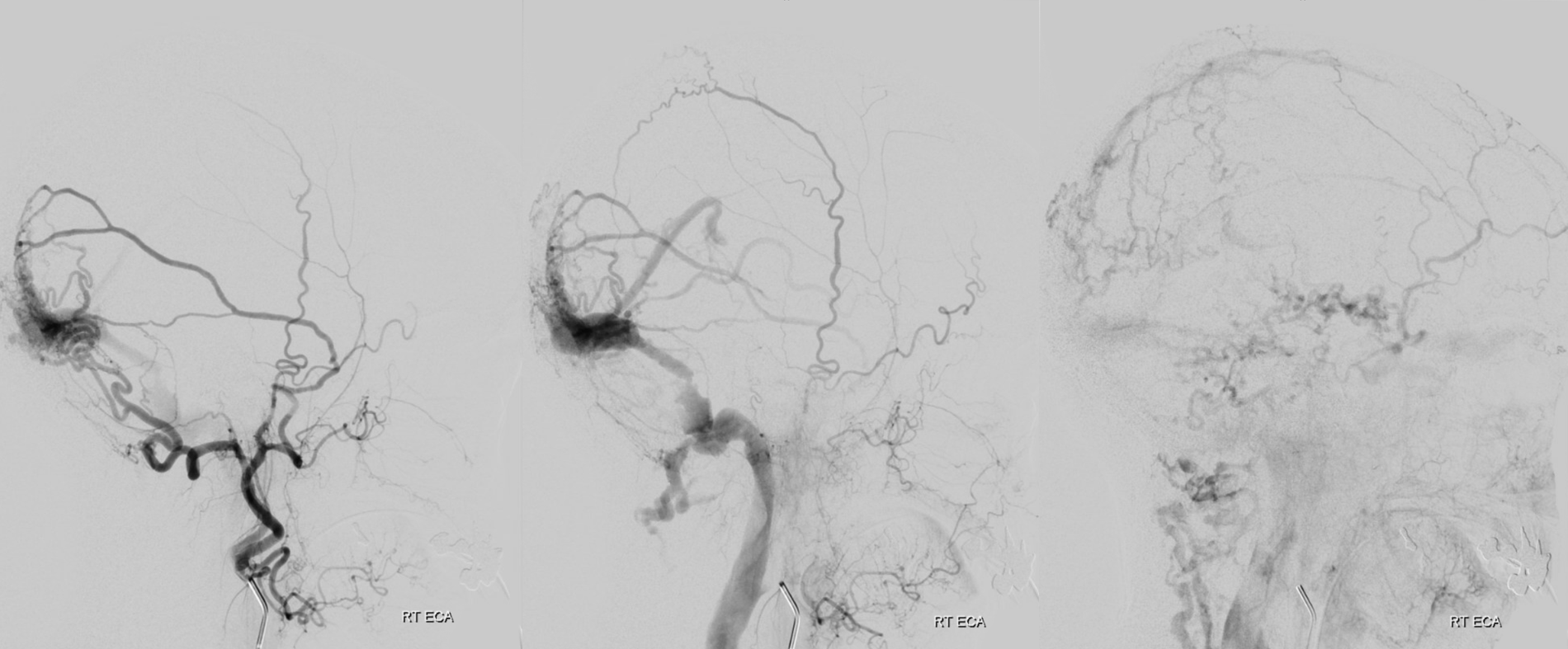
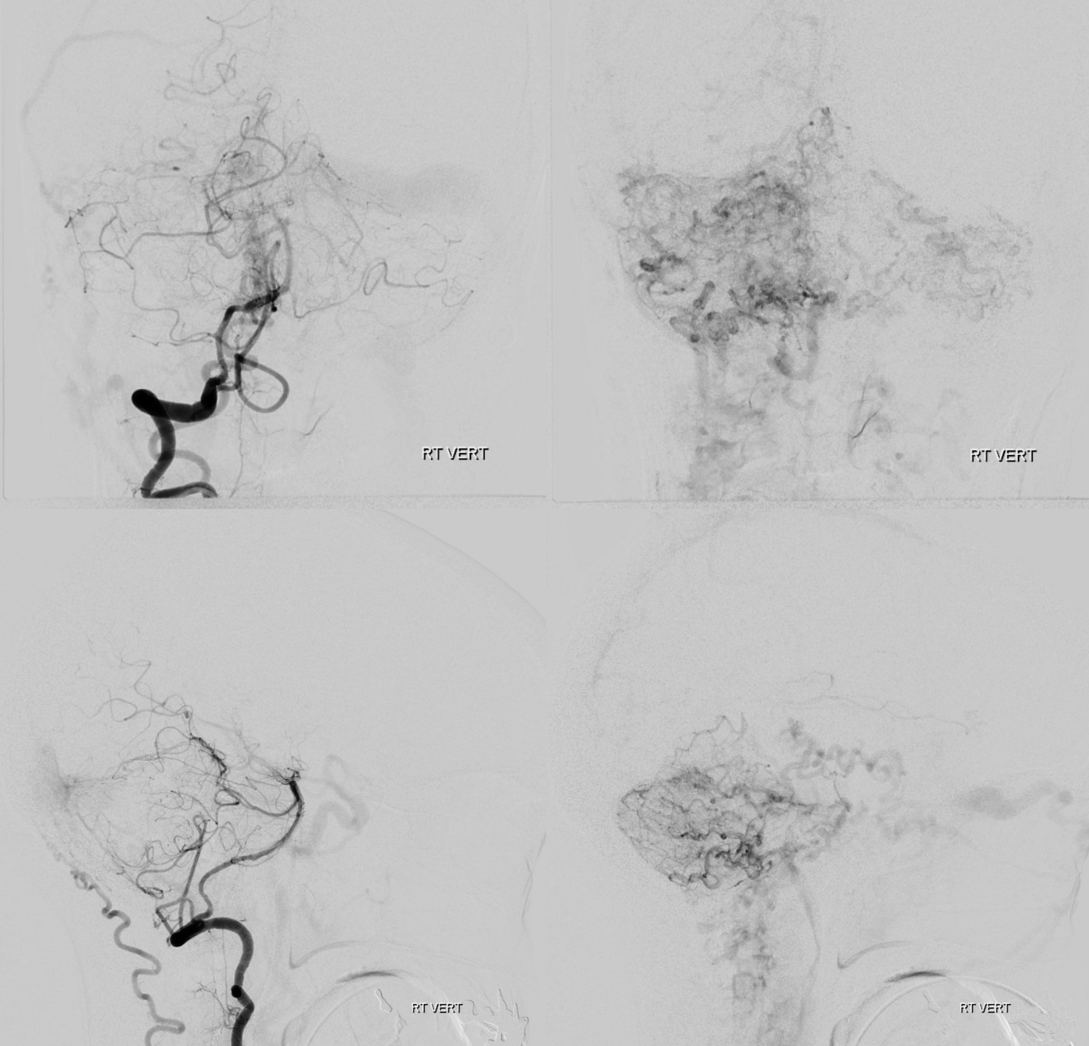
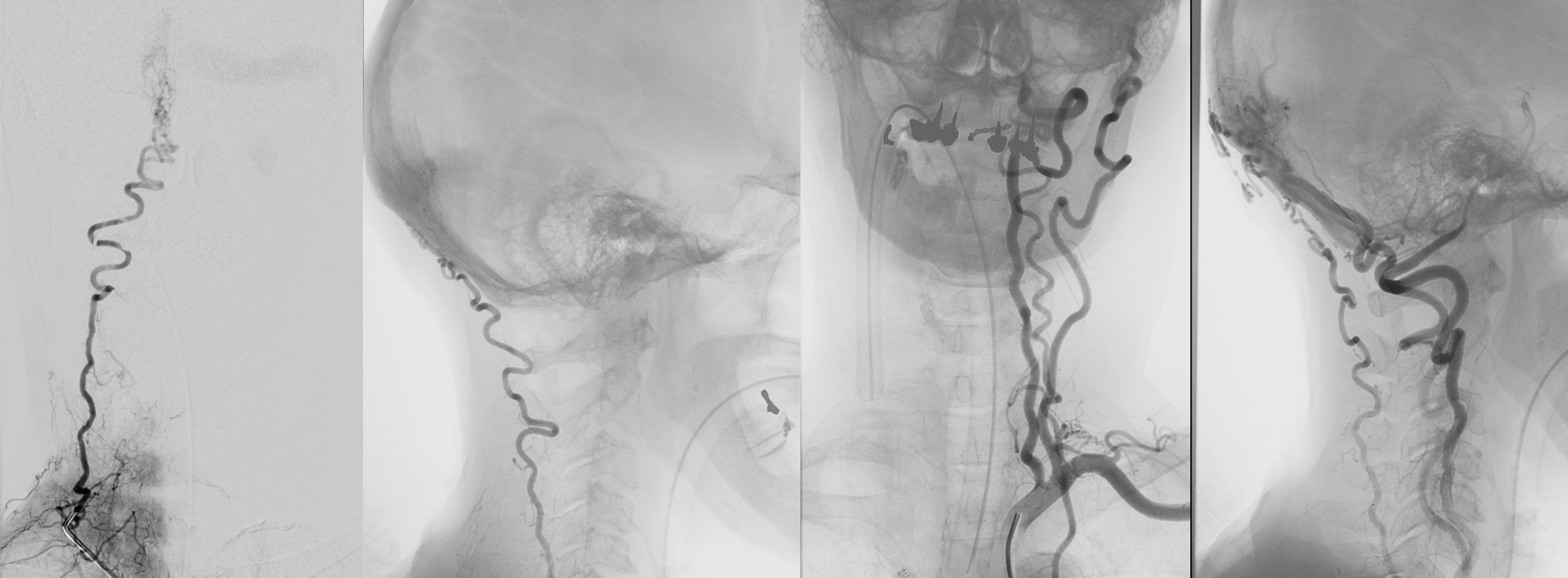
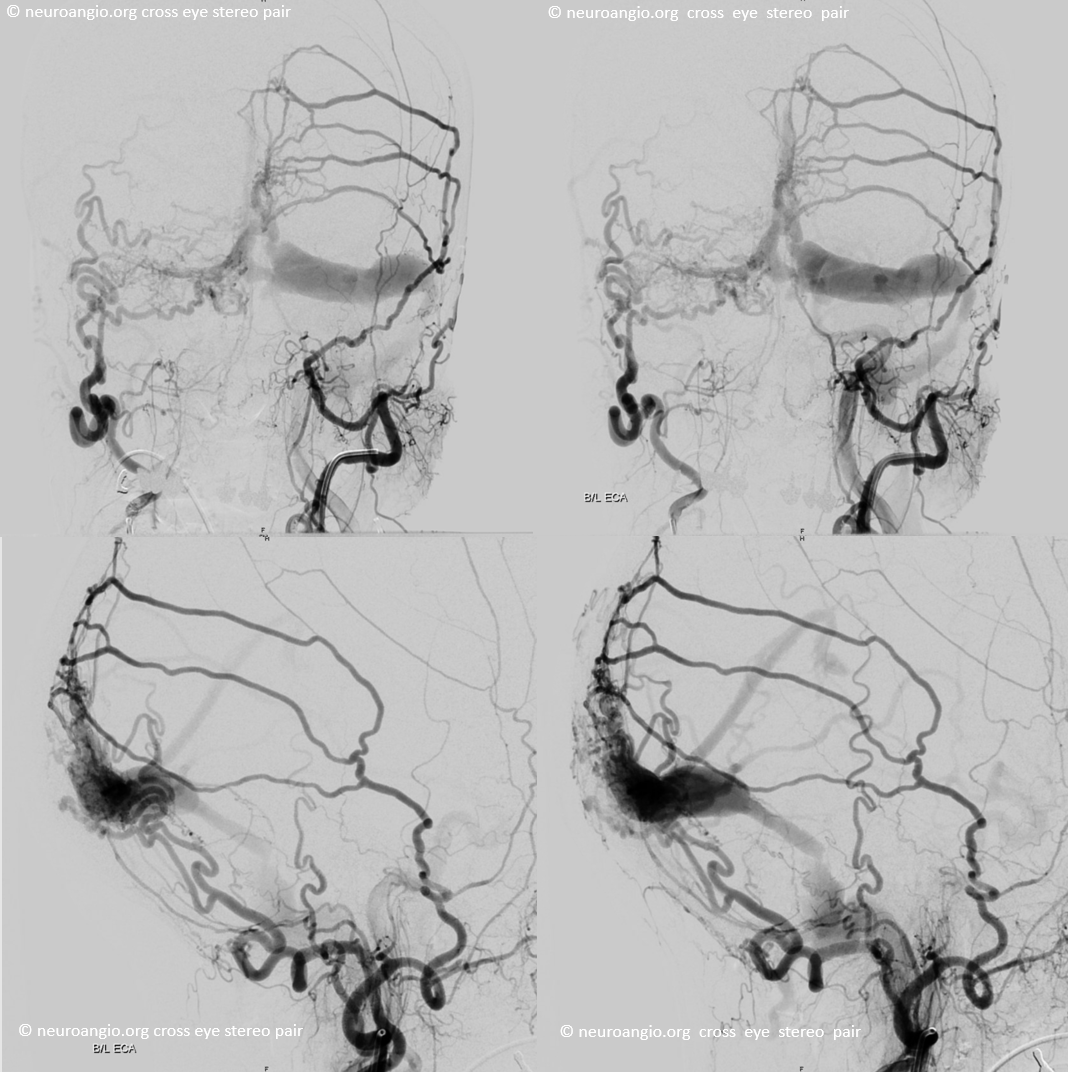
Presentation is confusion. No arrows — analyze this!
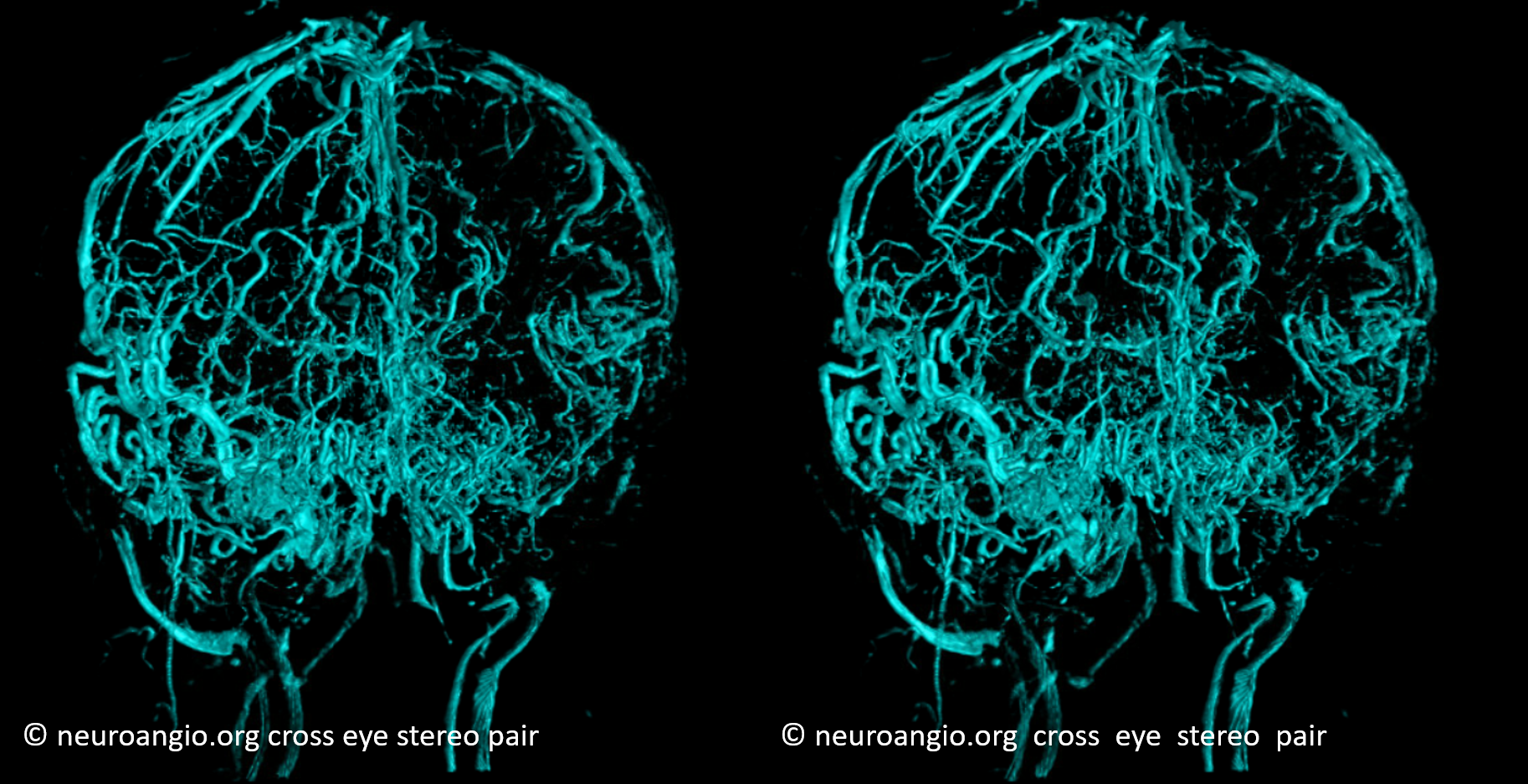
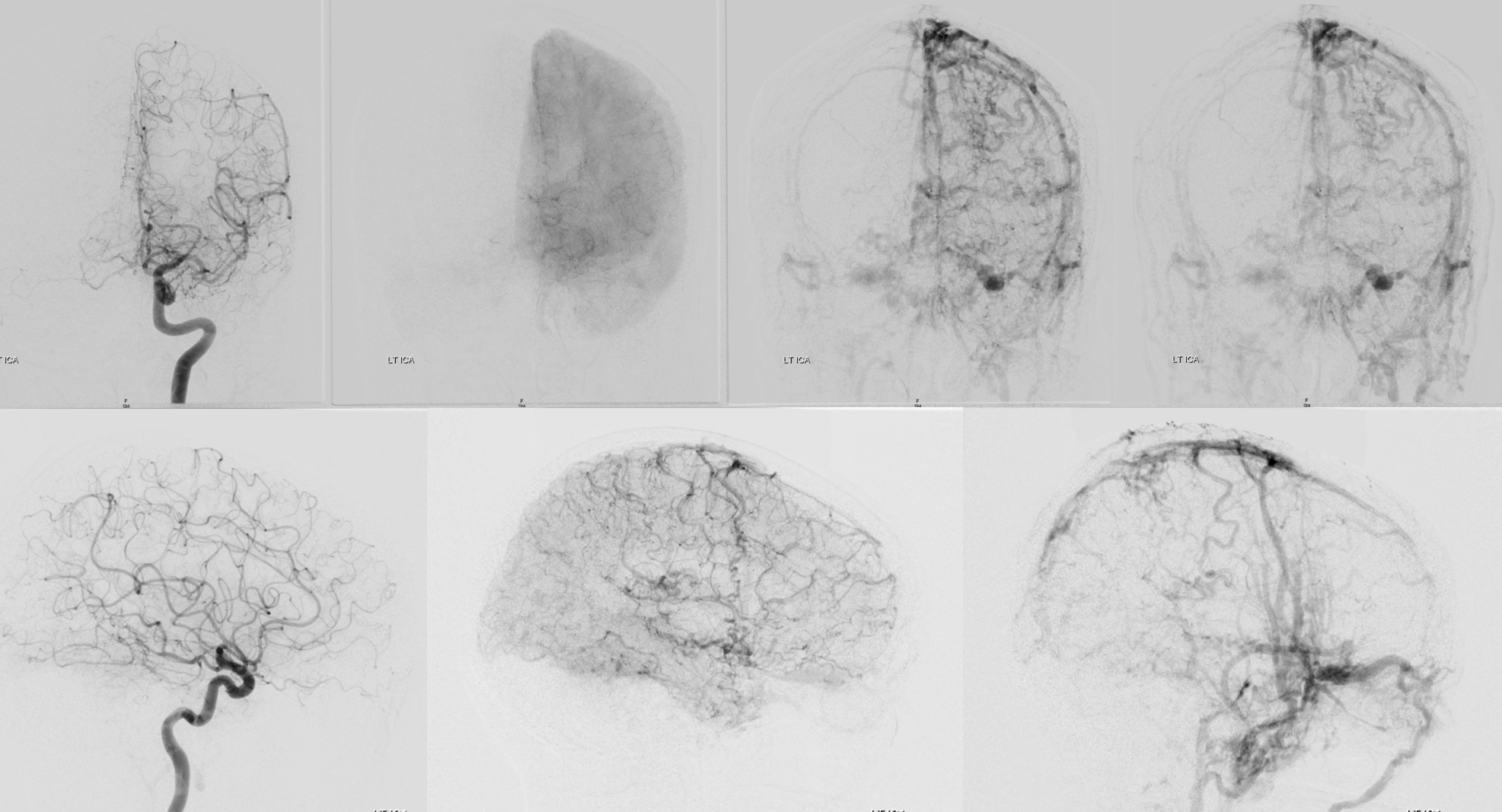
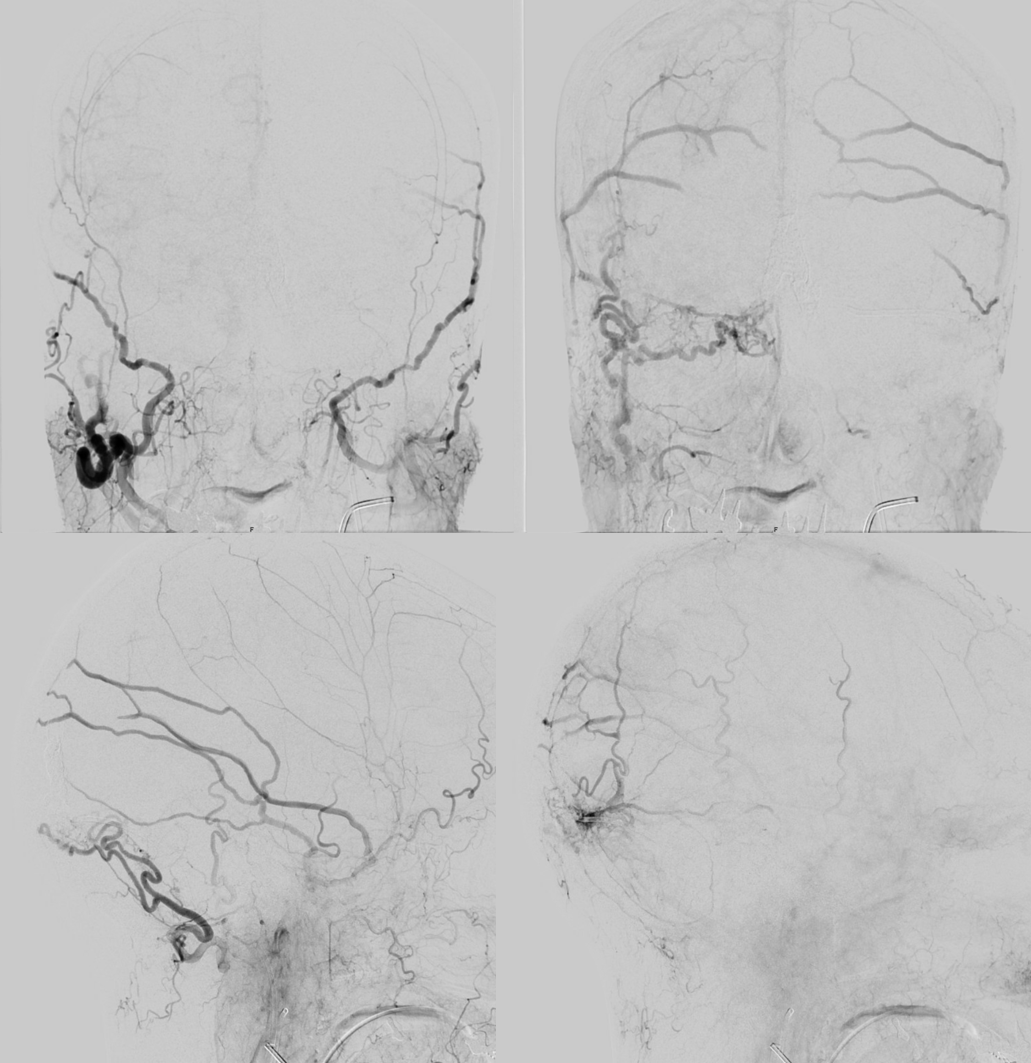
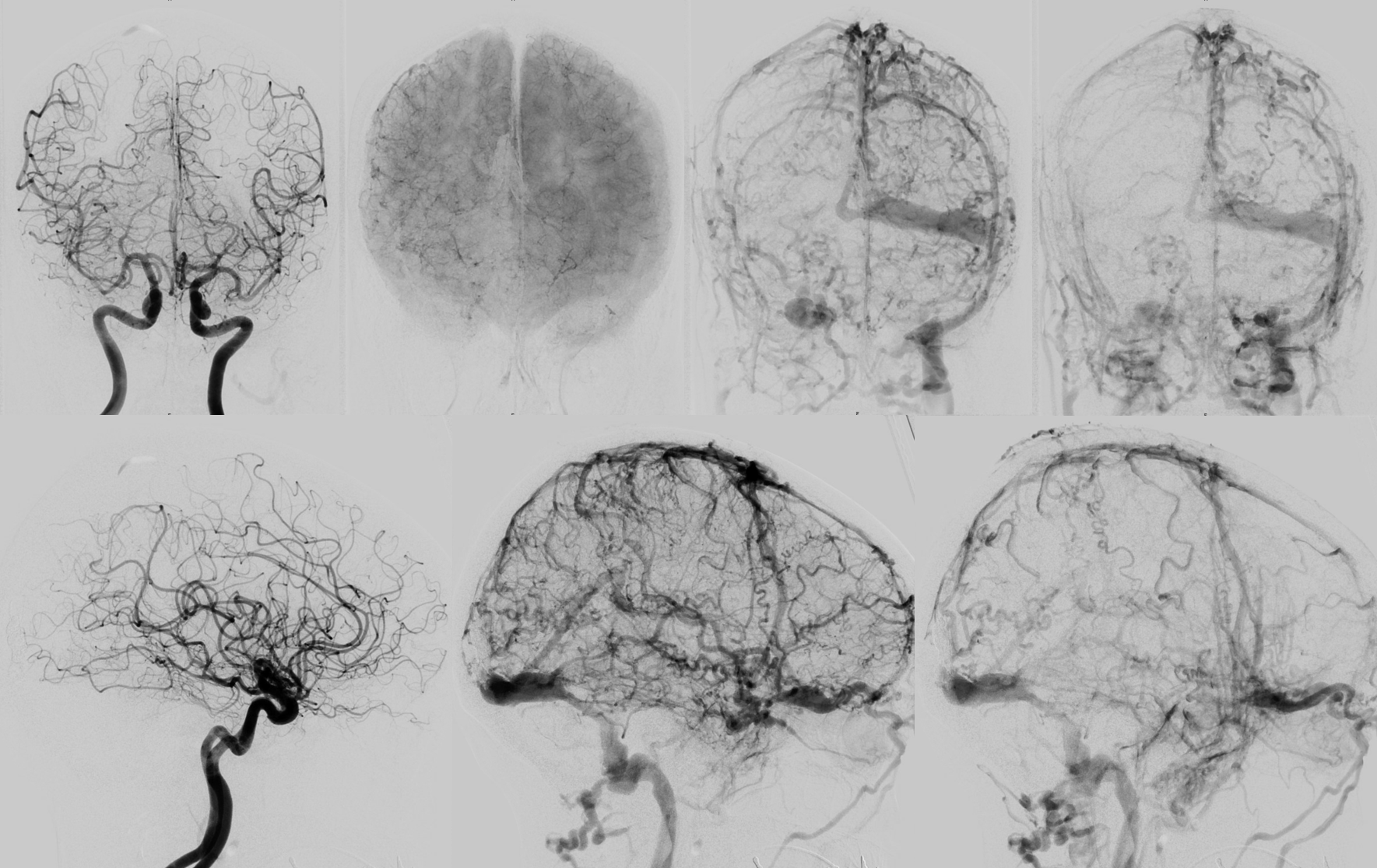
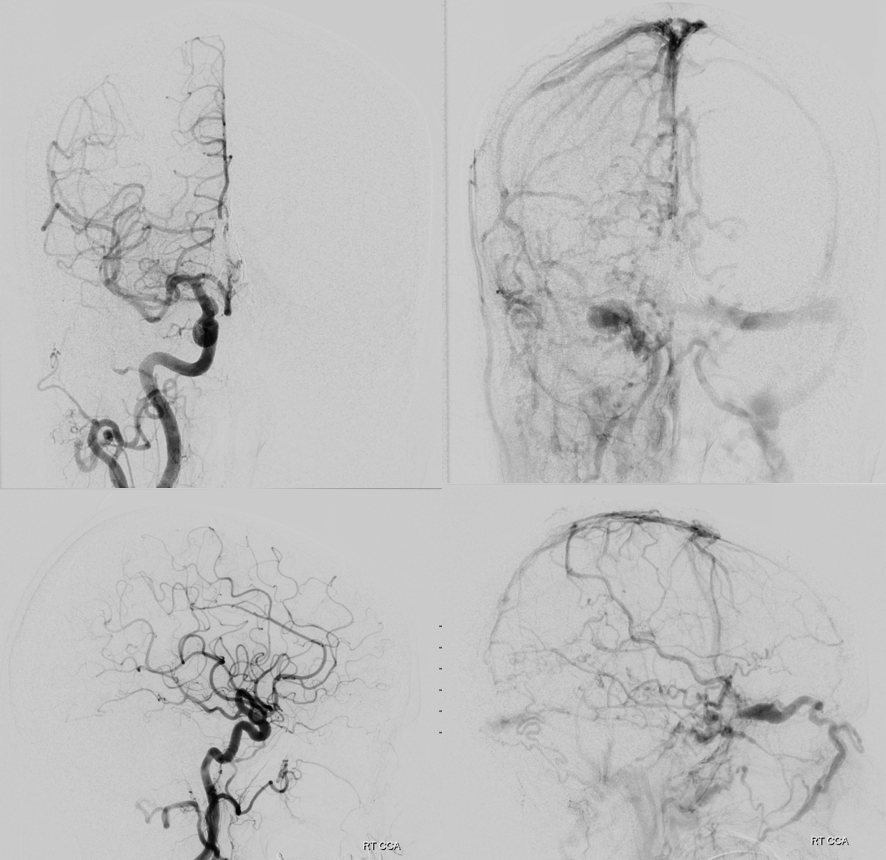
Right ICA (top row) and bilateral ICA injection venous phase axial MIPs of rotational angiography
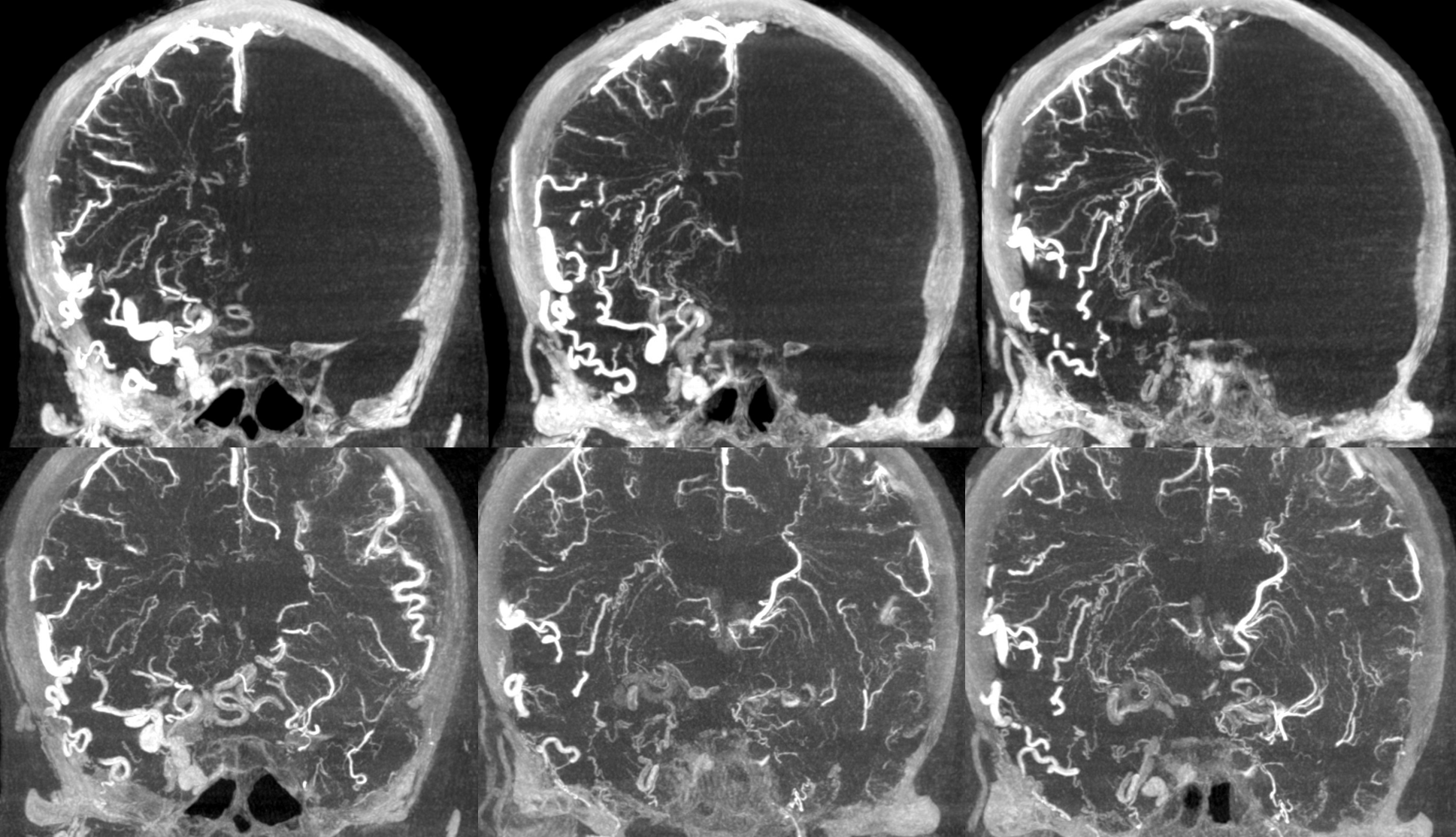
Source bilateral ICA injection venous phase dataset

Transverse sinus pressure = 68 mm Hg
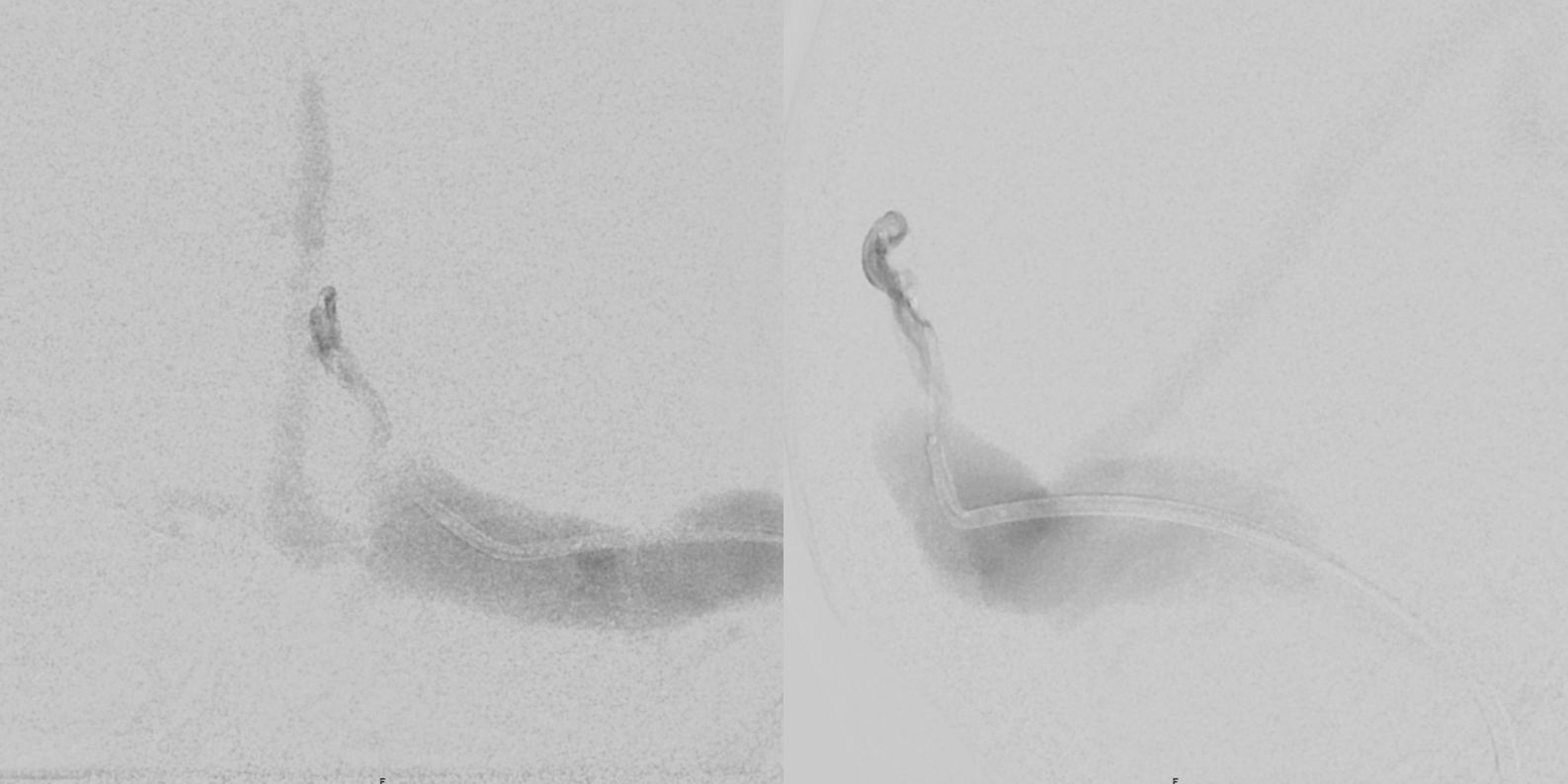
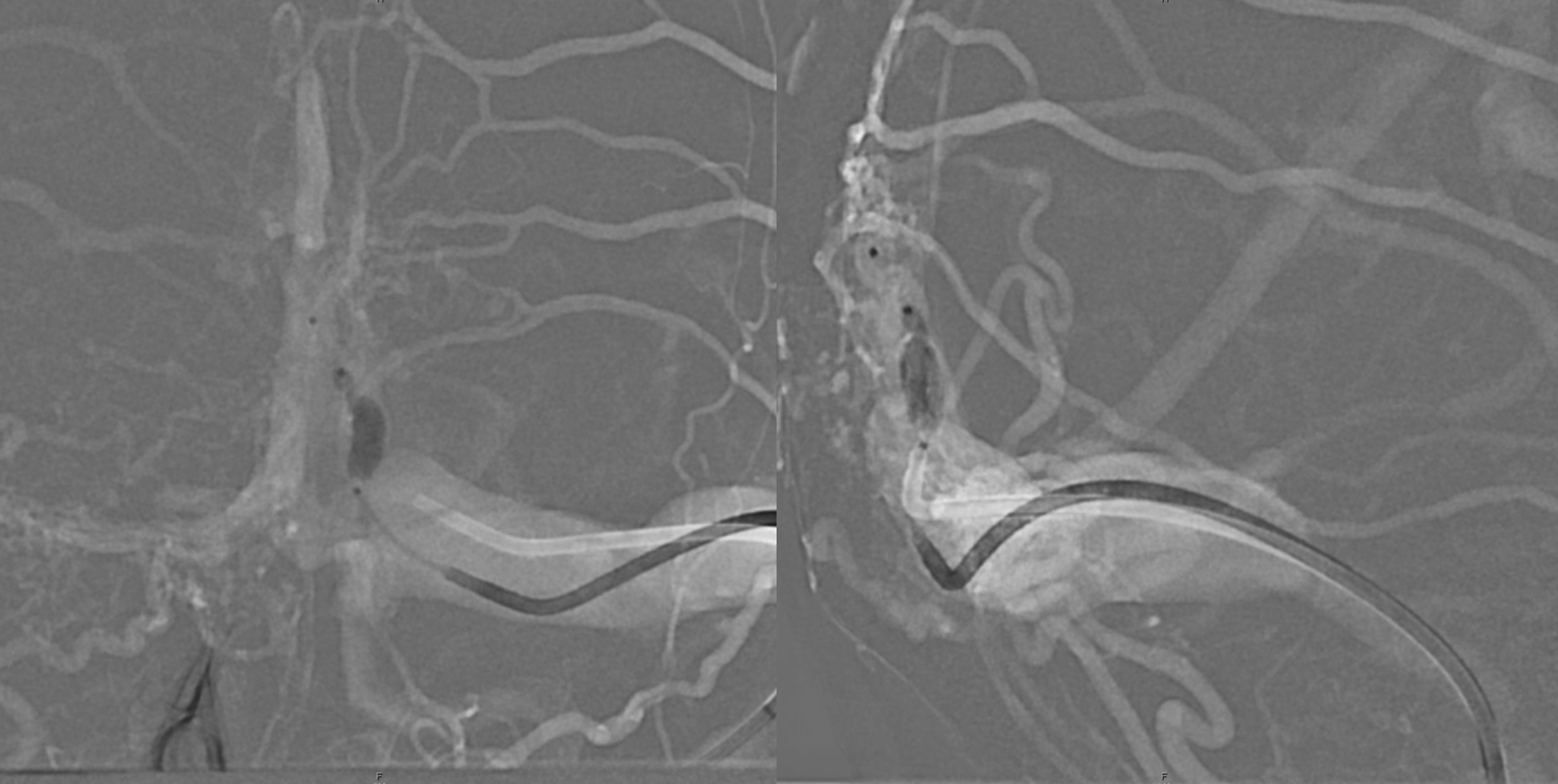
Image 8 is post-embolization transverse sinus injection to check patency of connection with straight sinus. Transverse sinus pressure post fistula closure = 44 mm Hg
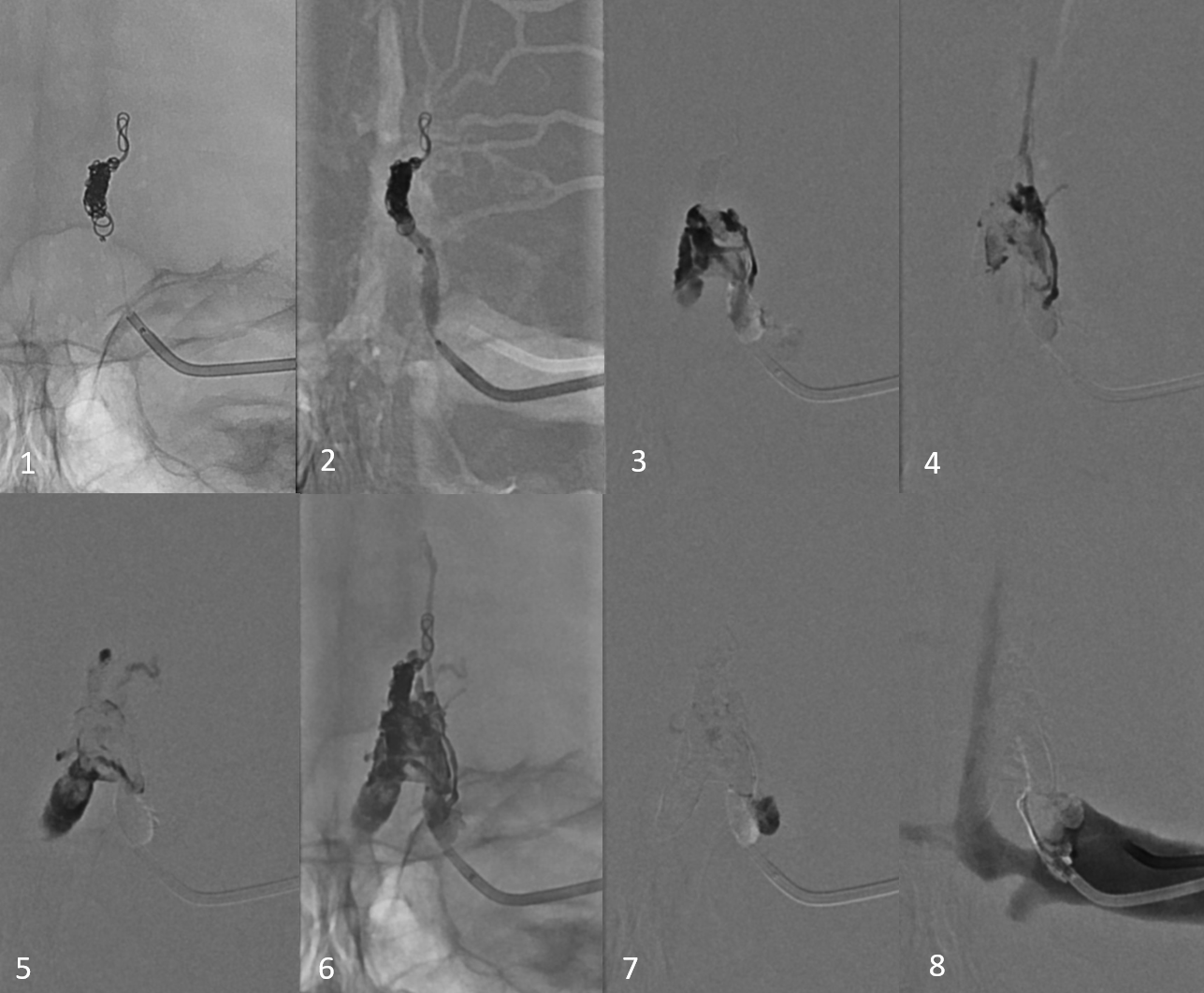

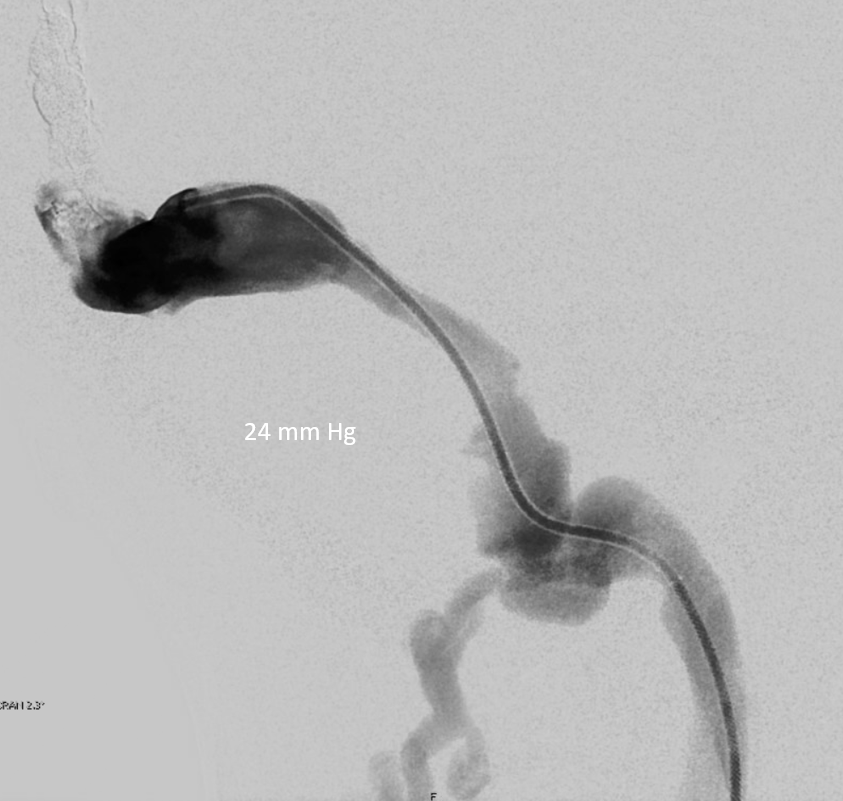
Transverse sinus pressure post sigmoid sinus angioplasty = 24 mm Hg
Deep cervicals were also negative
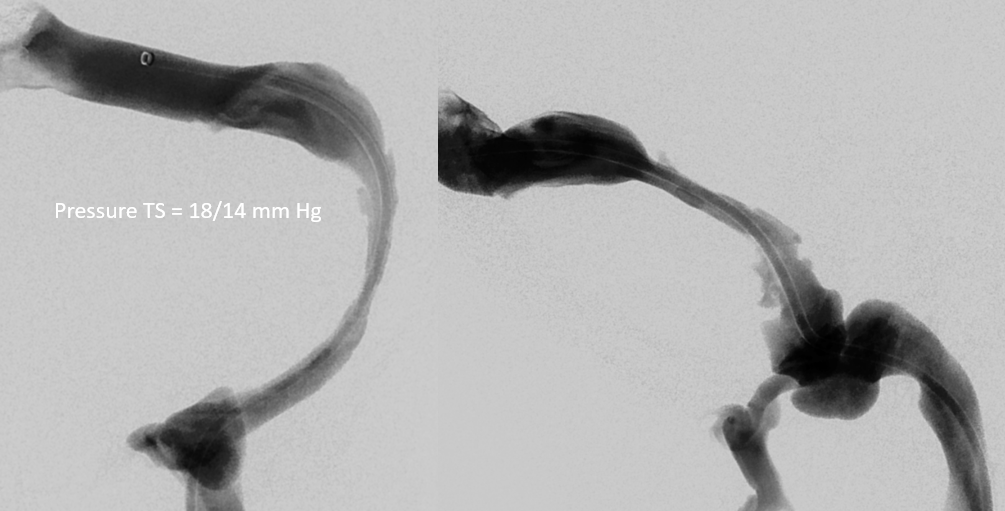
One week later — clinically improved dramatically awake alert had a long talk — turns out there is history of long-standing very bad trigeminal neuralgia, and most recently confusion / memory issues, before acute deterioration. Now back to baseline. The trigeminal neuralgia is likely to improve also. Now checking to see how the sigmoid sinus stenosis is doing
Doesn’t look so good. Pressure is ok, but pulsatile flow which is a soft sign of relatively higher pressure than should be the case
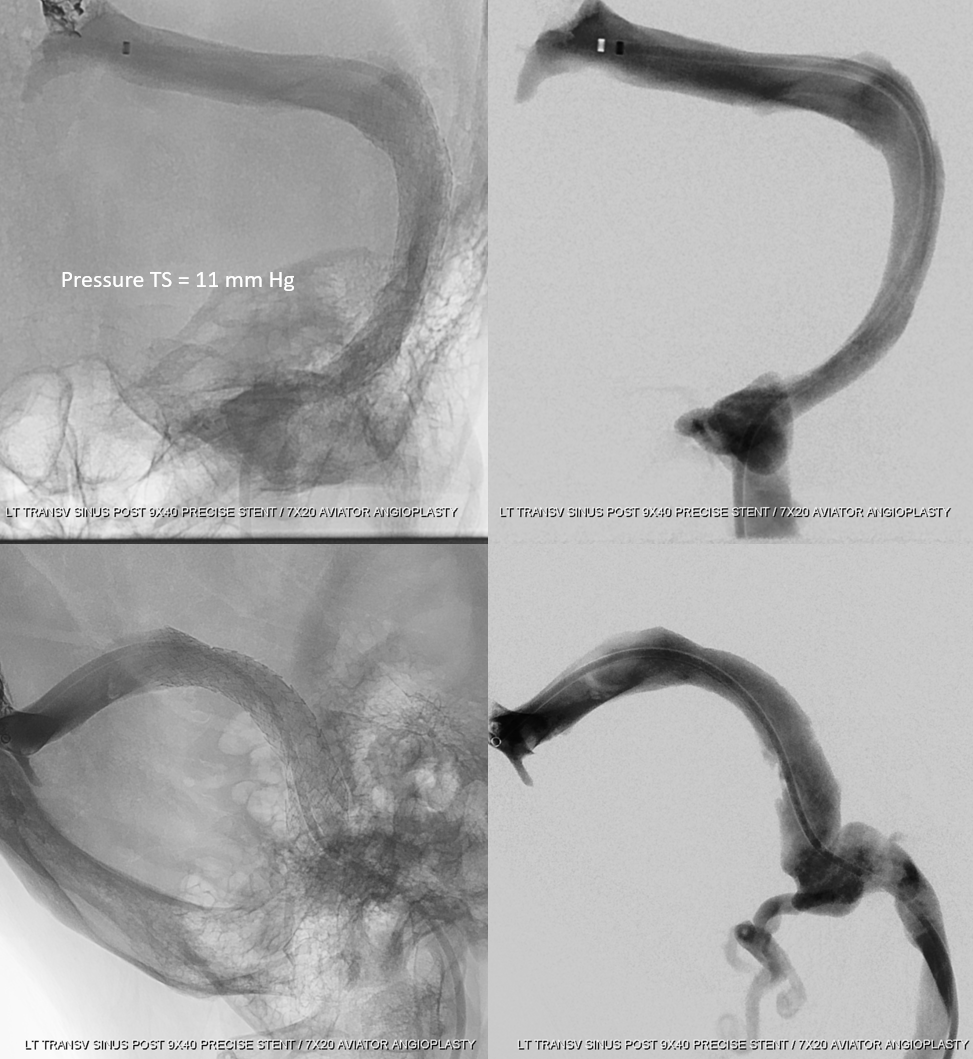
Pressure drops further after stenting. Which means that 18/14 was not a normal pressure for this person, even though it is “within normal limits”
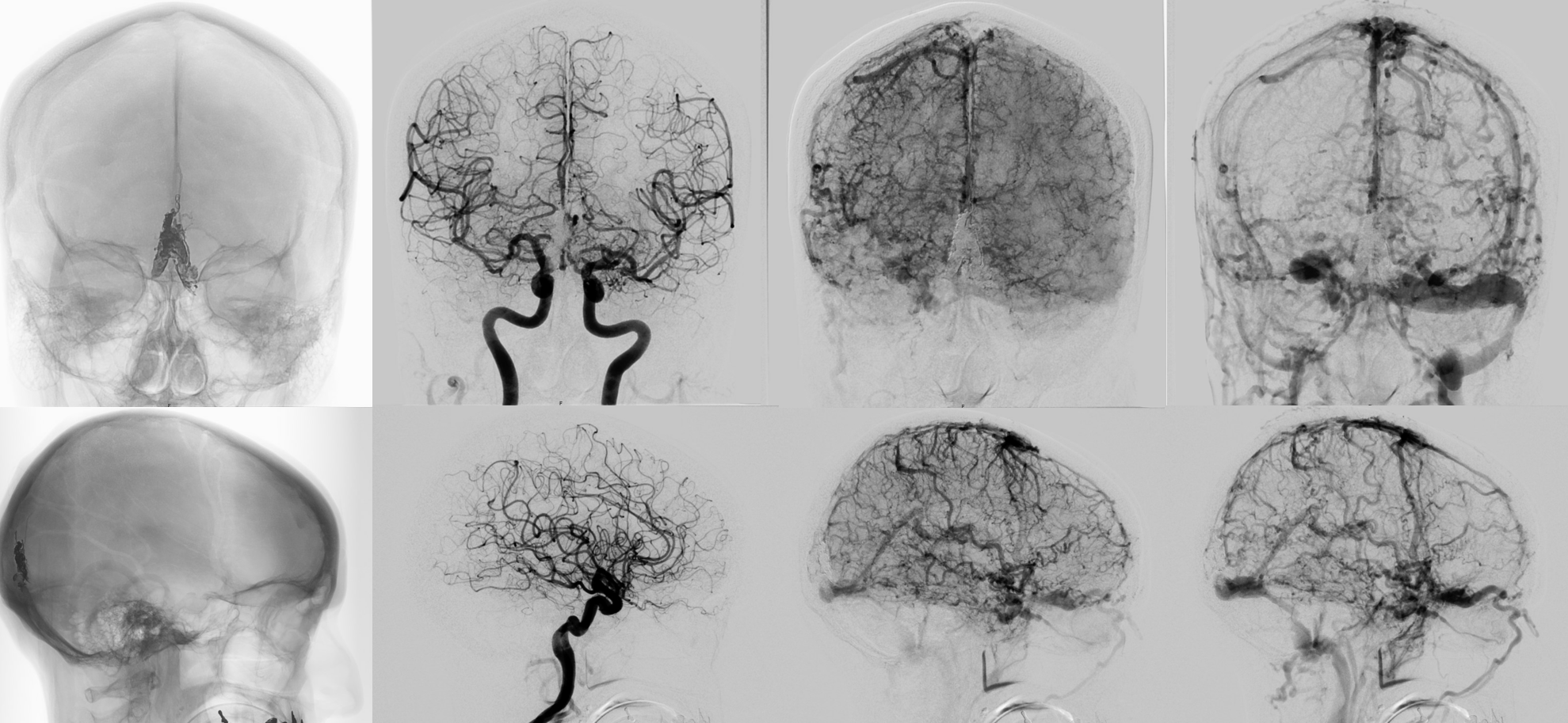
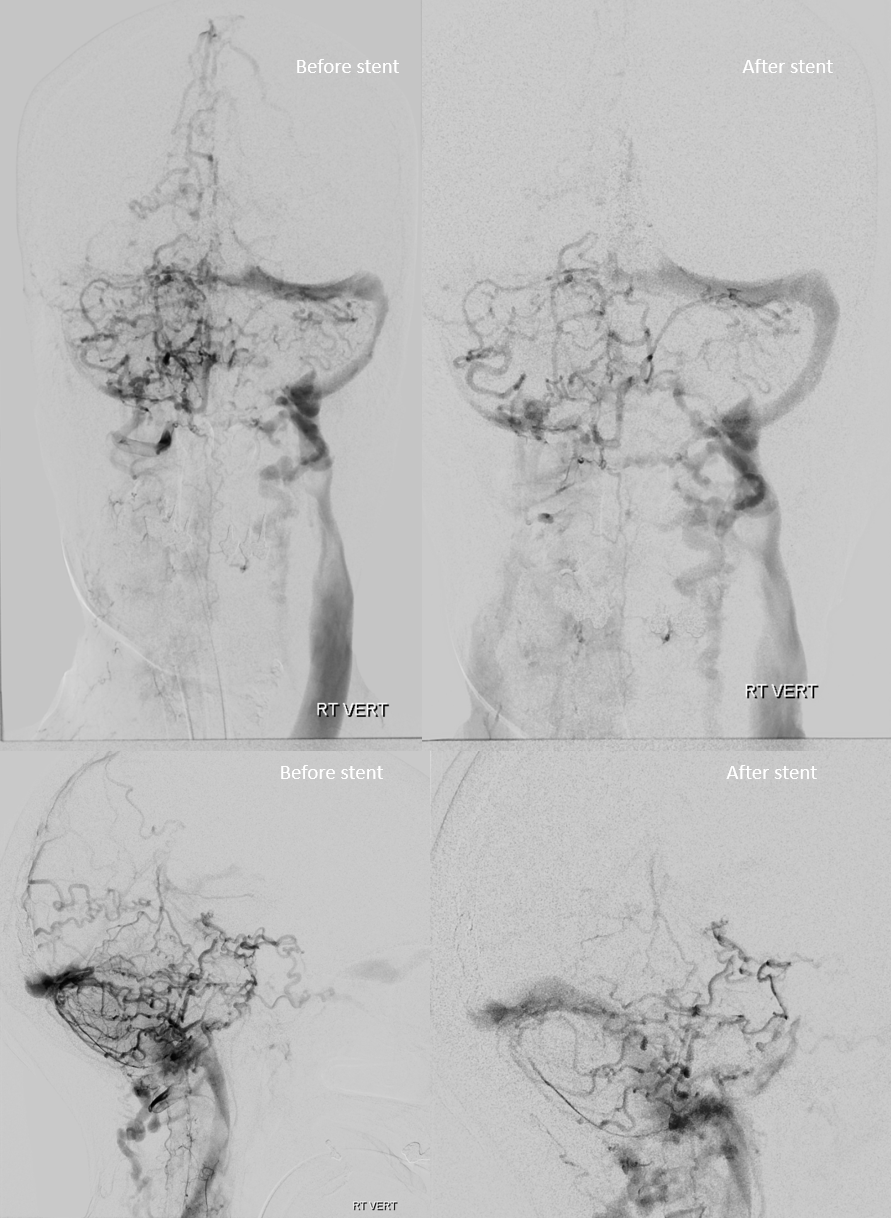
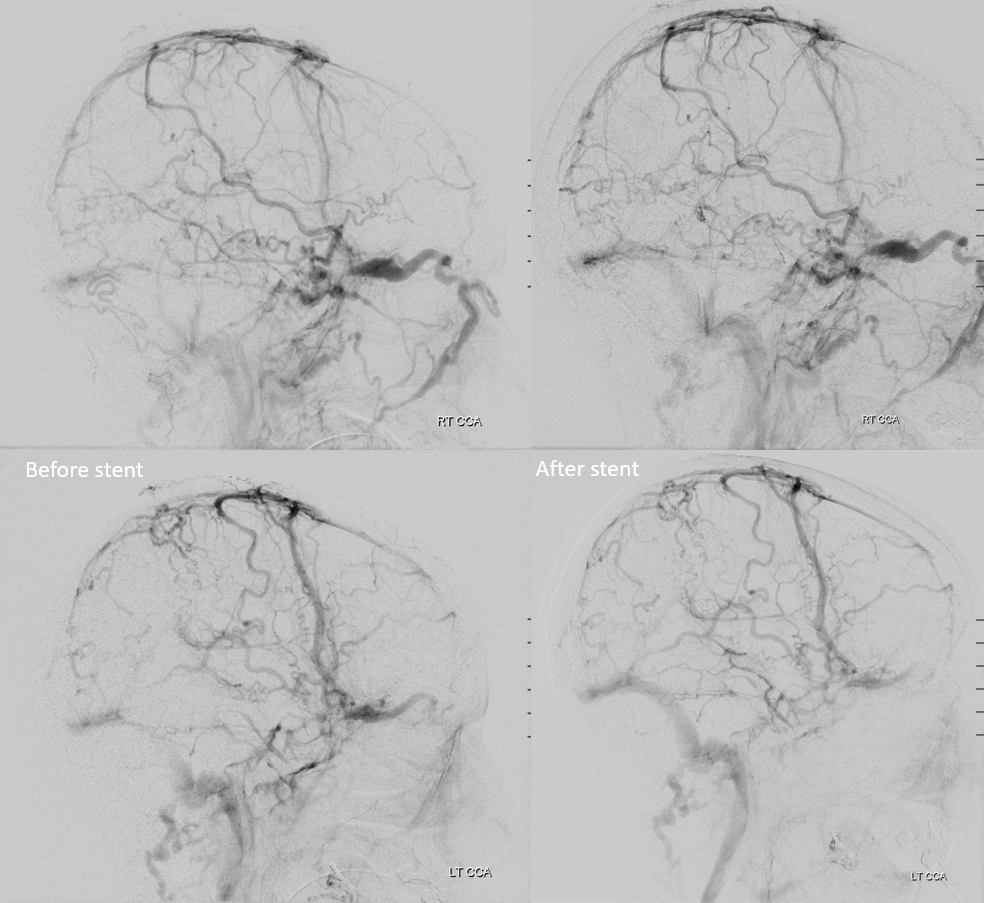
Post stent venous phases
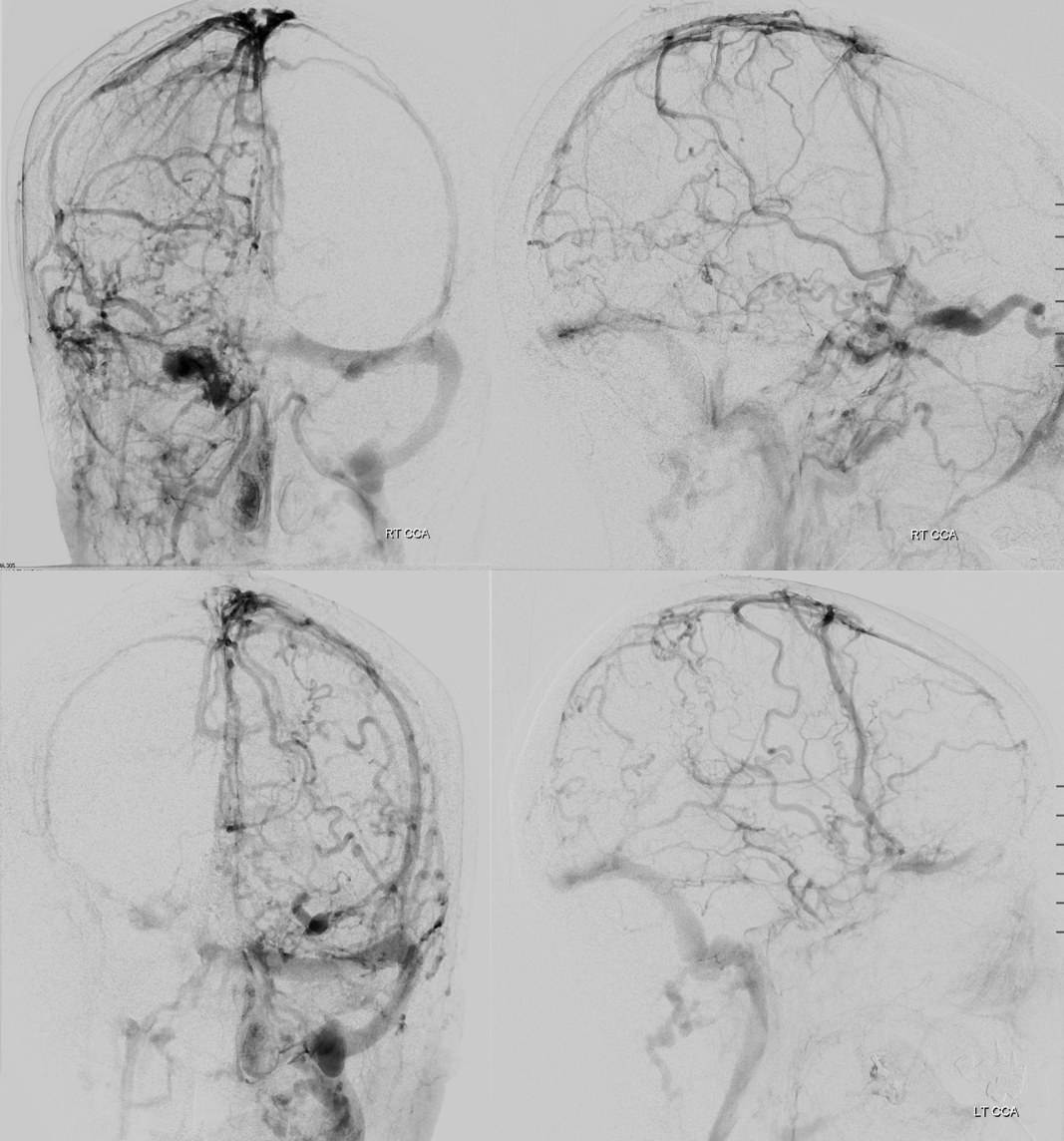
Before and after side by side — see the difference?
See Case Library page for other superselective embolization cases