Several nice points in this case
First, SAMMPRIS does not apply in acute stroke. The goal in acute occlusion is to reopen the vessel now. There is nothing complicated about it — most things are simple once you understand them. This one sure is — an artery went down, the brain is not getting flow — solution is to open the artery. By whatever means — embolectomy or stenting.
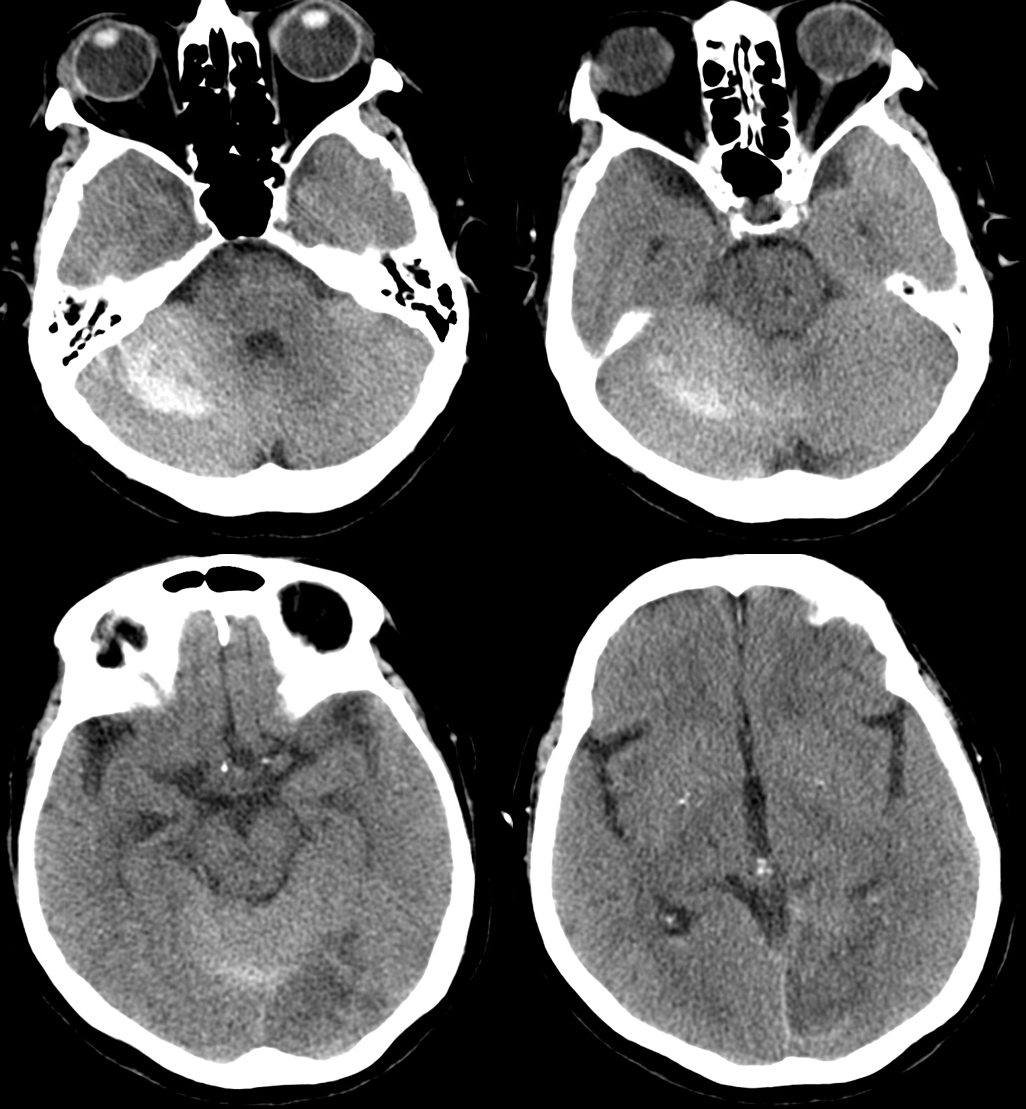
This patient presents with multiple recent smaller strokes, now with major symptoms.
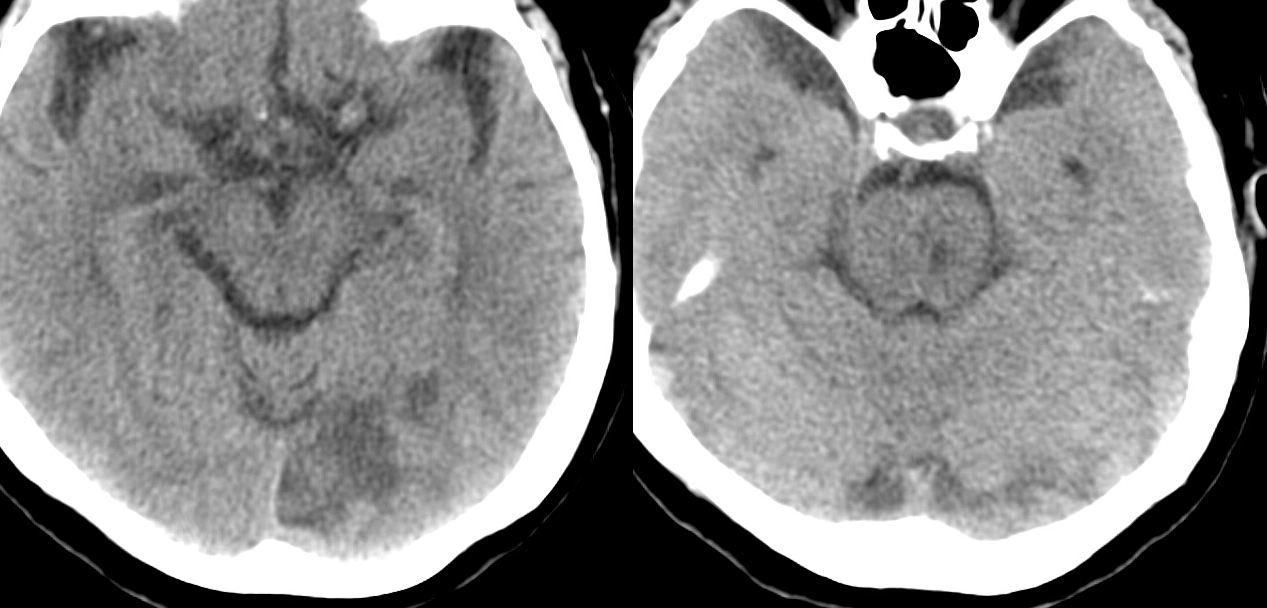
CT shows established infarcts in left pons and left PCA territory
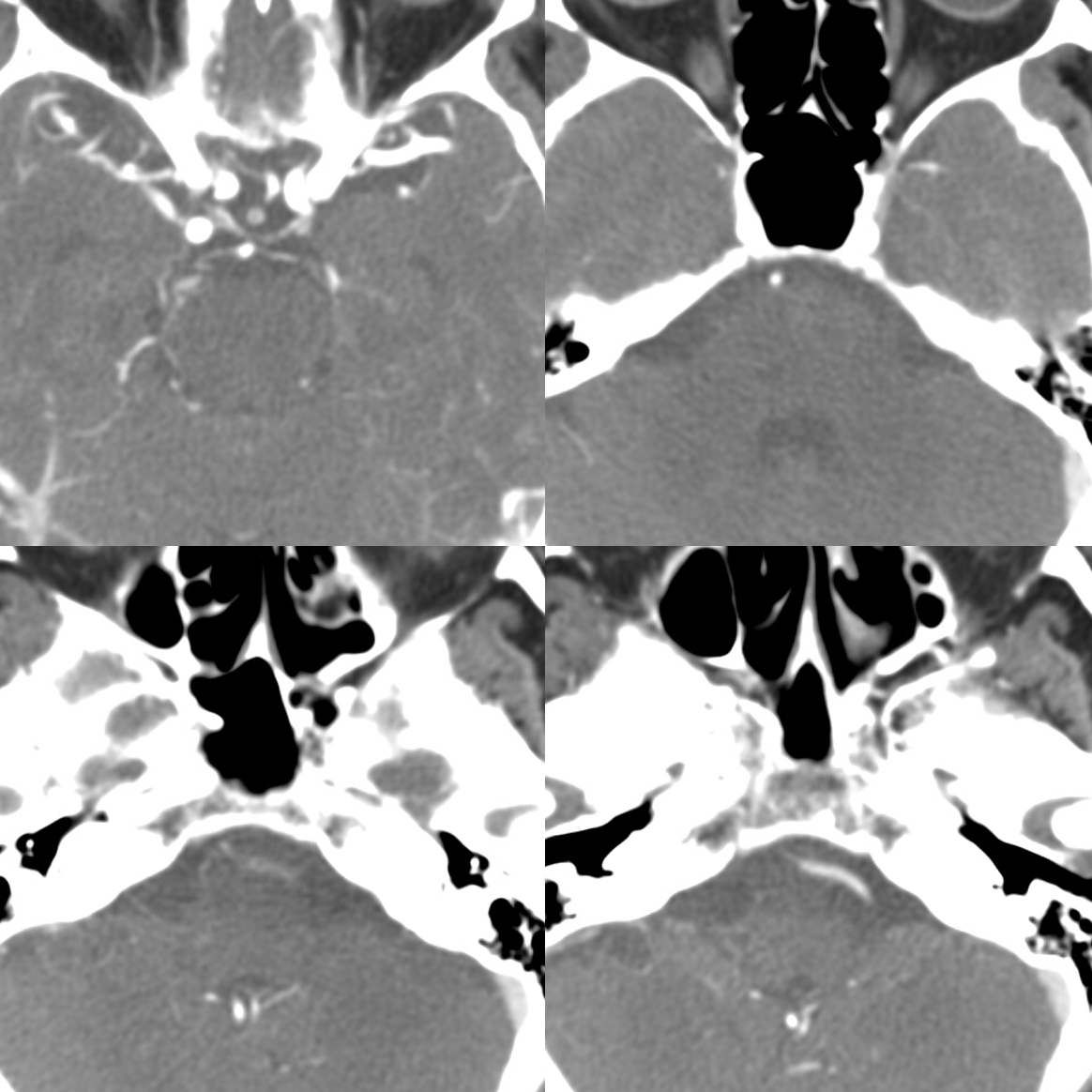
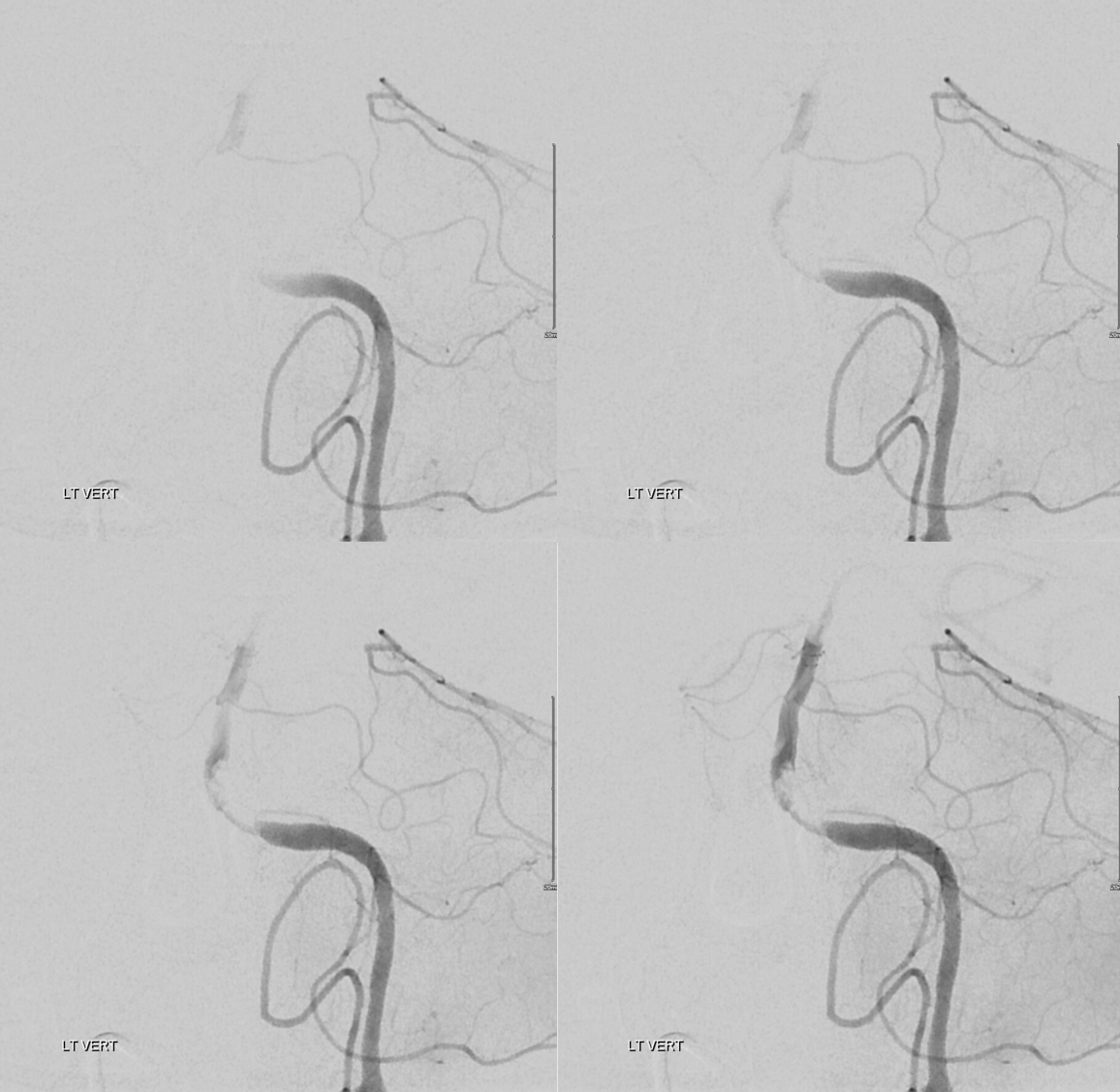
CTA — critical lower basilar stenosis vs. occlusion
Perfusion is a tool — its not some magic wand. The tool works when you know how to use it. A simple look at the automated maps — nothing wrong?
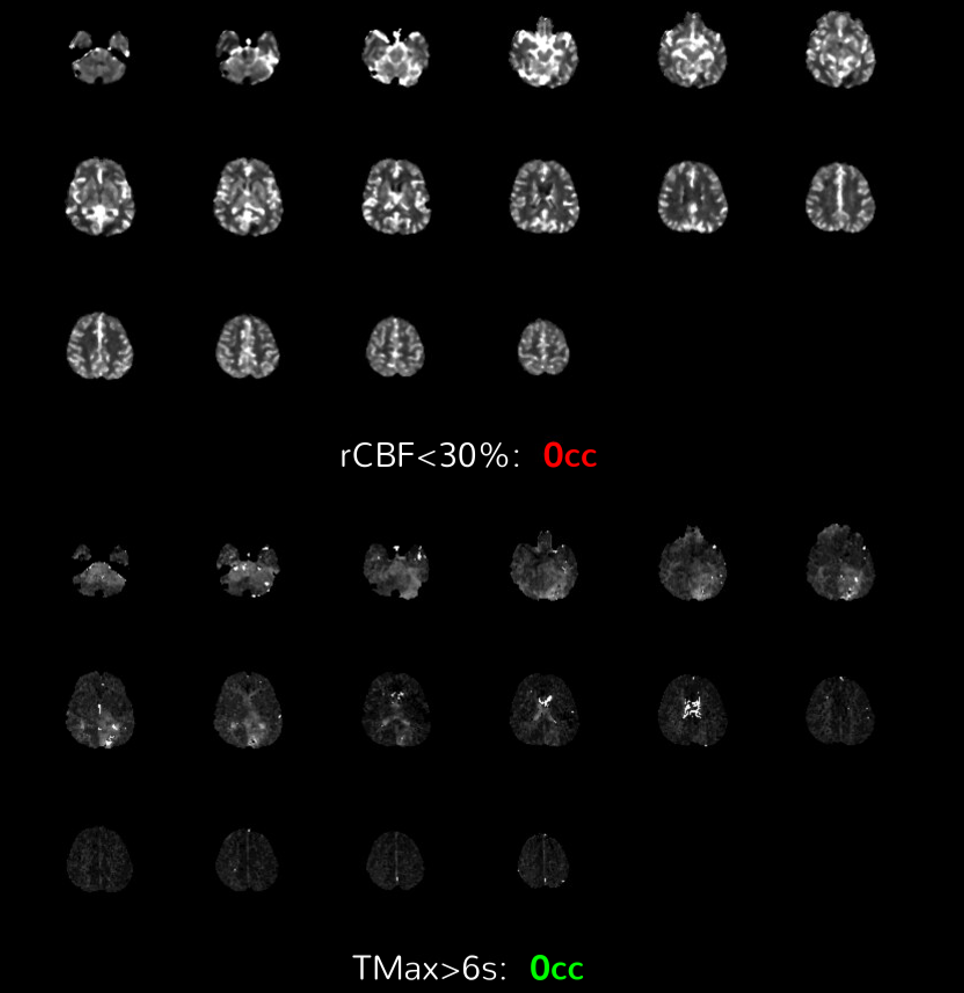
Of course there is something wrong. Need to look at everything. Tmax > 4 sec is delayed
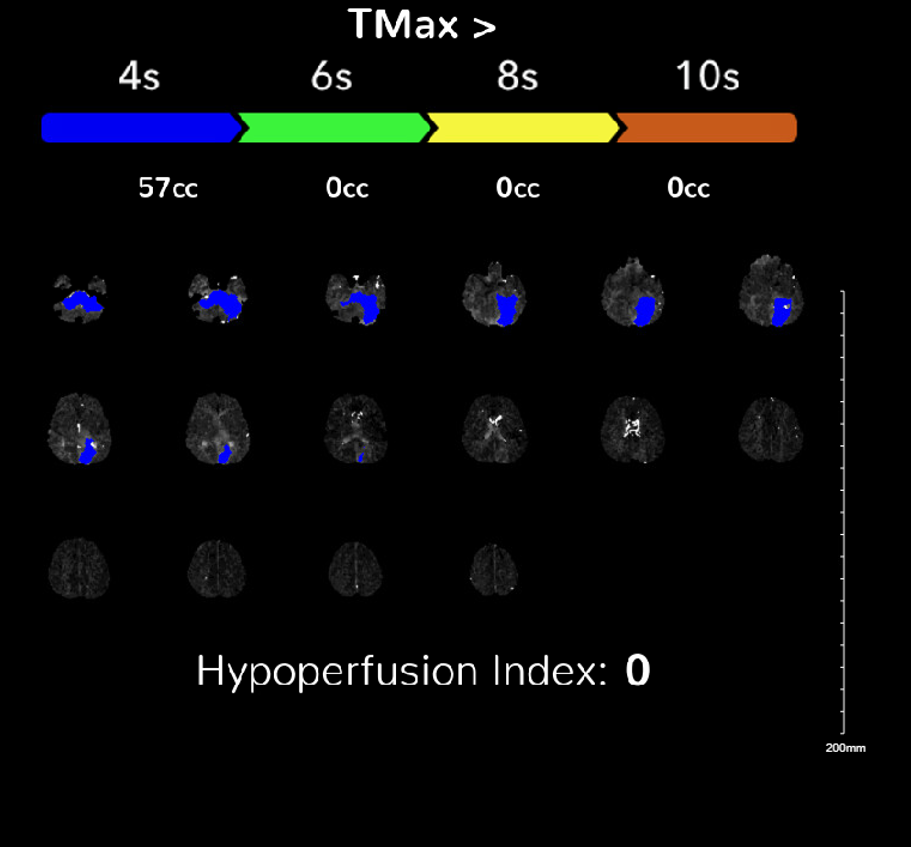
Individual maps are important — will see later
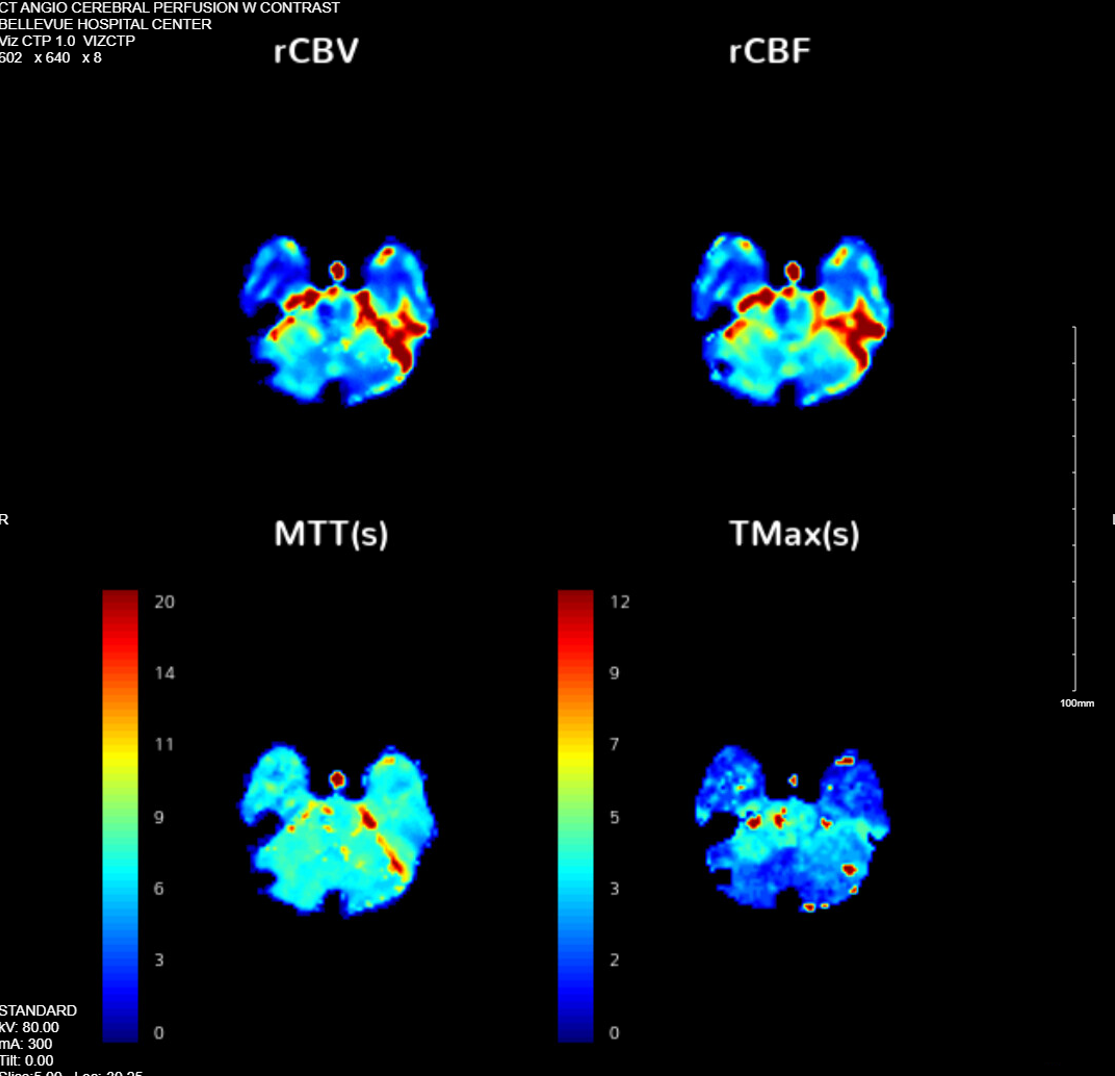
Point is that perfusion is not optimized for posterior fossa — but there is nothing magically different about it — looking at the data shows this perfusion not right. Does it help make decision — not in this case. But in others it does — check out this one for example
Angio — what kind of collateral do you see here? Is it important?

Magnified view — is this collateral important here?
Lateral views
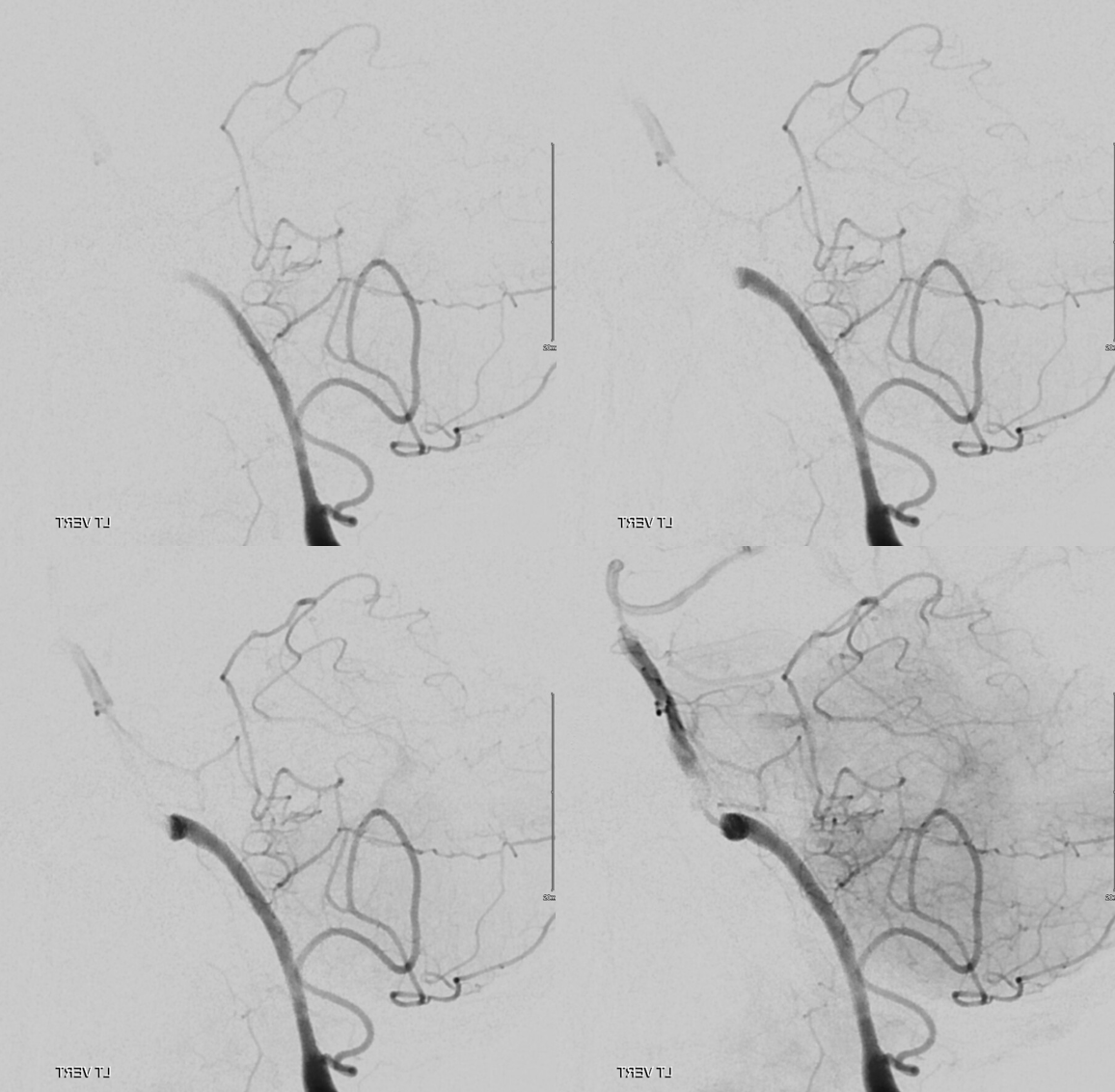
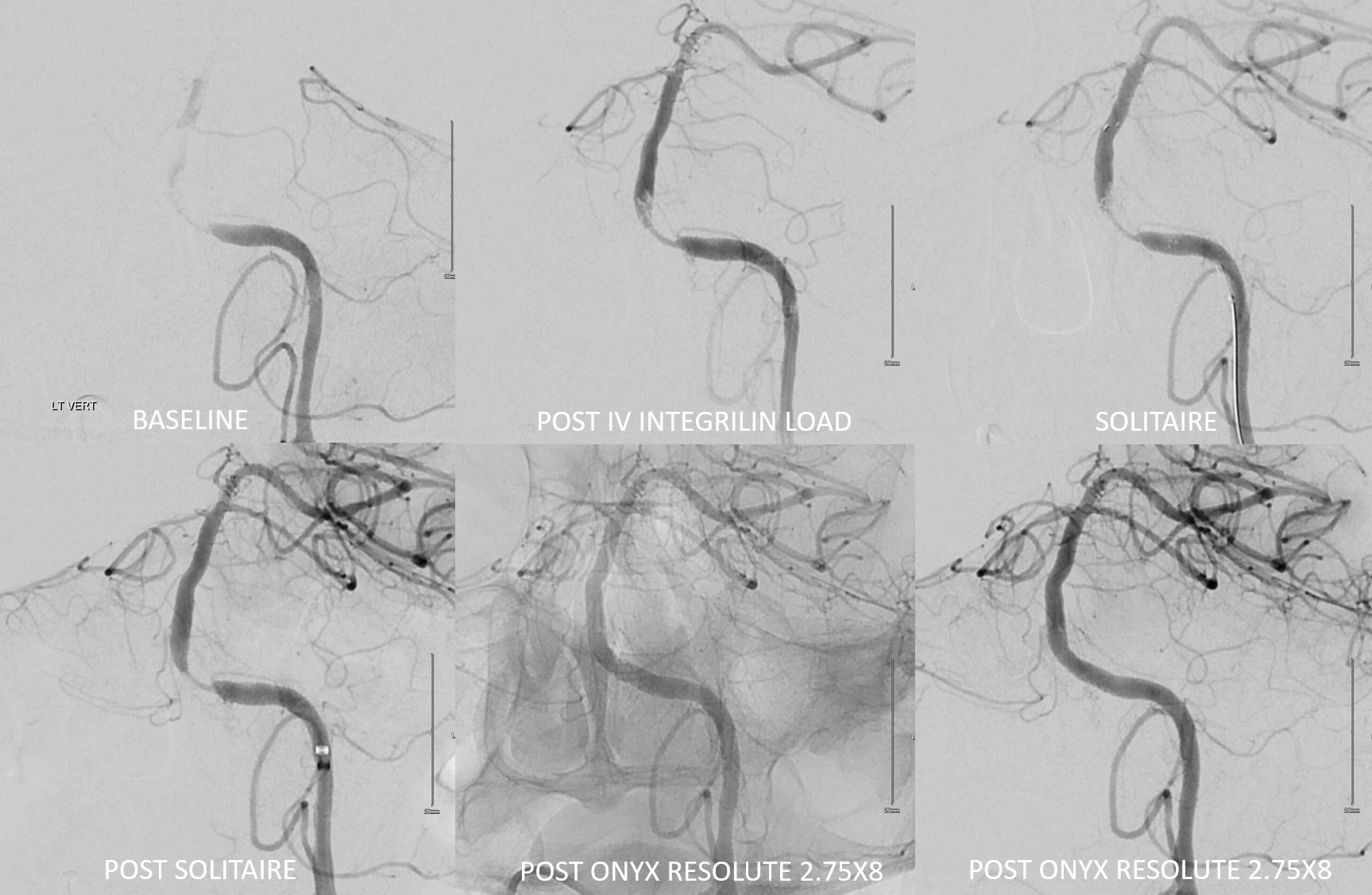
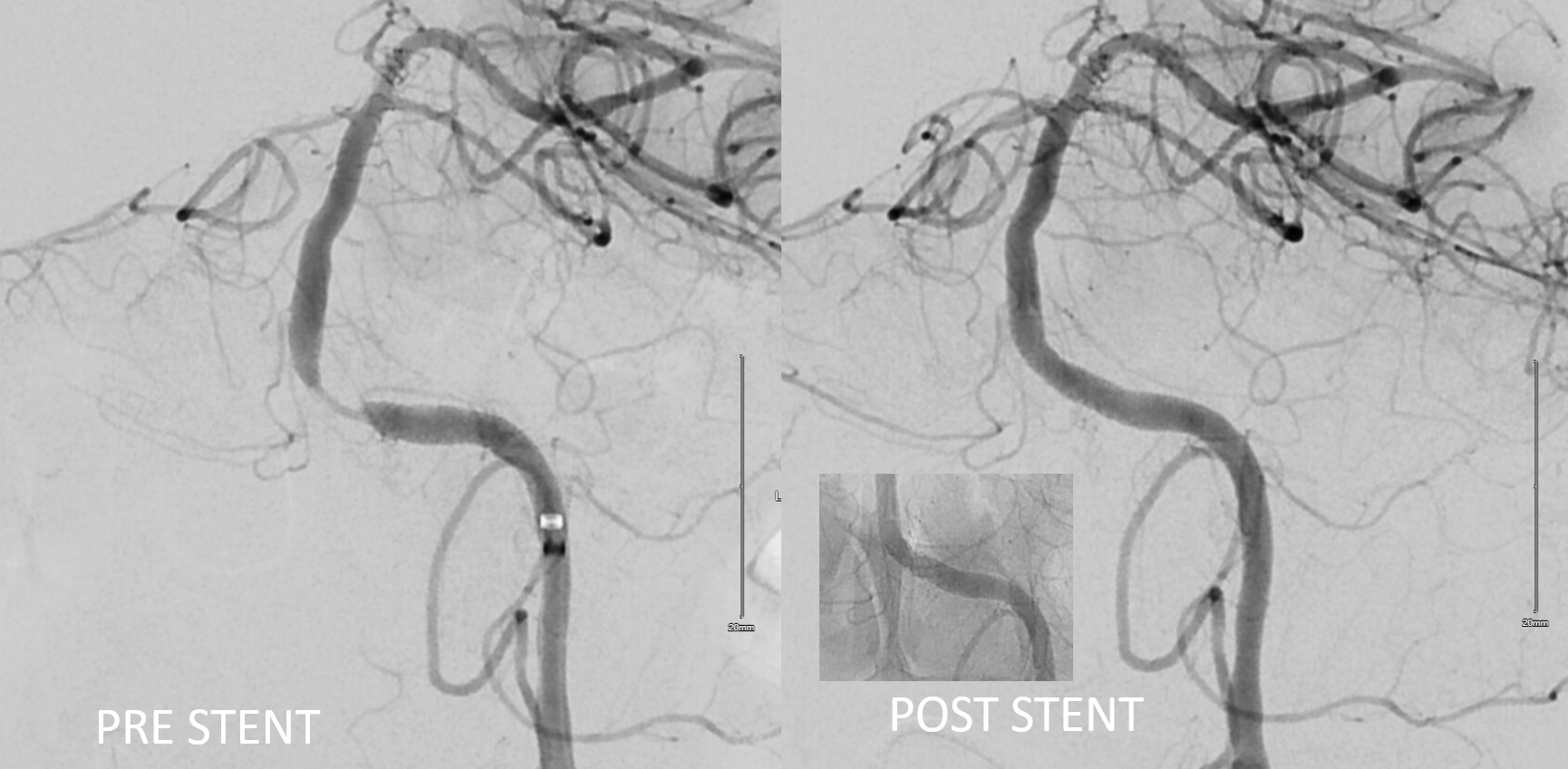
Sequence of treatment — each step contributes to reopening of the artery
Extra credit question — what is missing on the post-stent image?
CT 3 days later