
A beautiful and important illustration of hidden dangers in spinal dural fistula embolization. Don’t let a curable problem become a paralysis disaster — understand importance of spinal anatomy and high quality angiography!
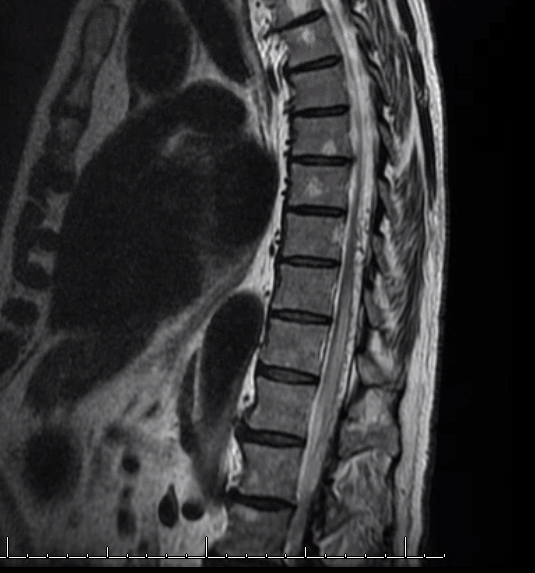
Patient presents with typical symptoms of progressive lower extremity sensorimotor dysfunction
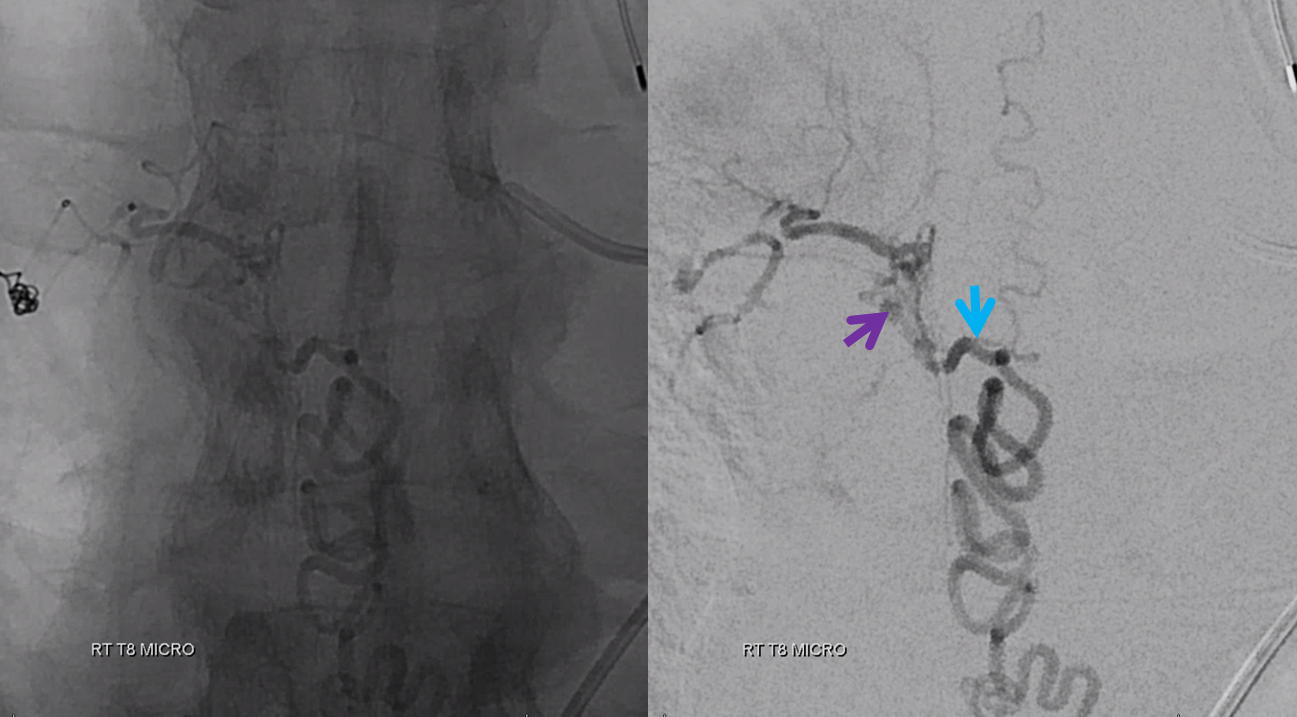
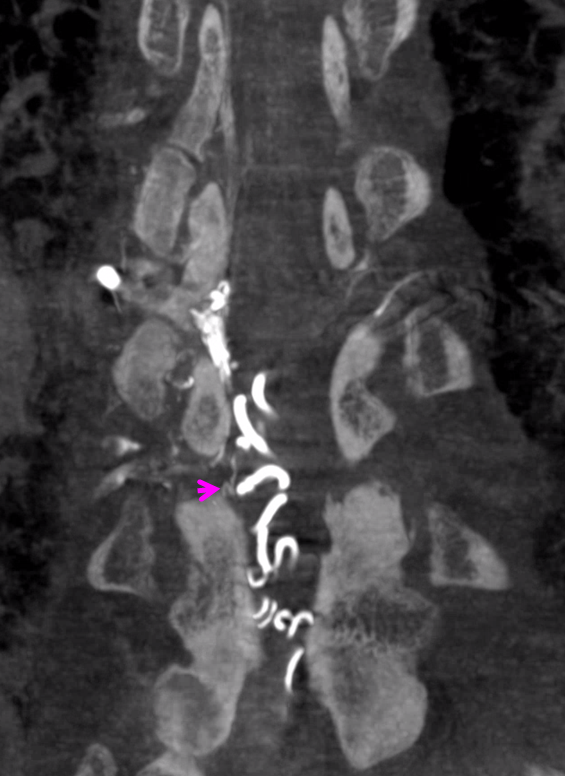
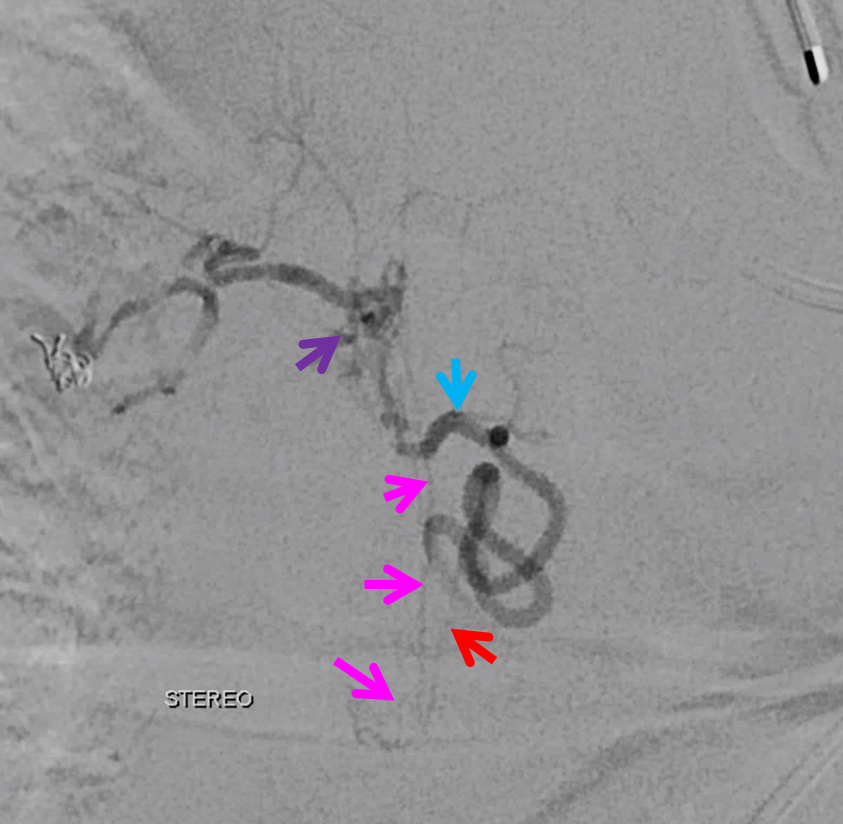
Fistula is at Right T8 level. Fistula is marked by purple arrow. Spinal draining vein proximal segment is blue. Classic appearance
Ready to embolize? Of course not. We need to find the anterior spinal artery. And, in this case, it happens to arise from Right T9 — directly one level below

This should already raise concern. Doesn’t seem like there is an obvious connection between right T8 and right T9 — but there always is. Question is where — prevertebral, paravertebral, intradural? See Spinal Arterial Anatomy page for some more info.
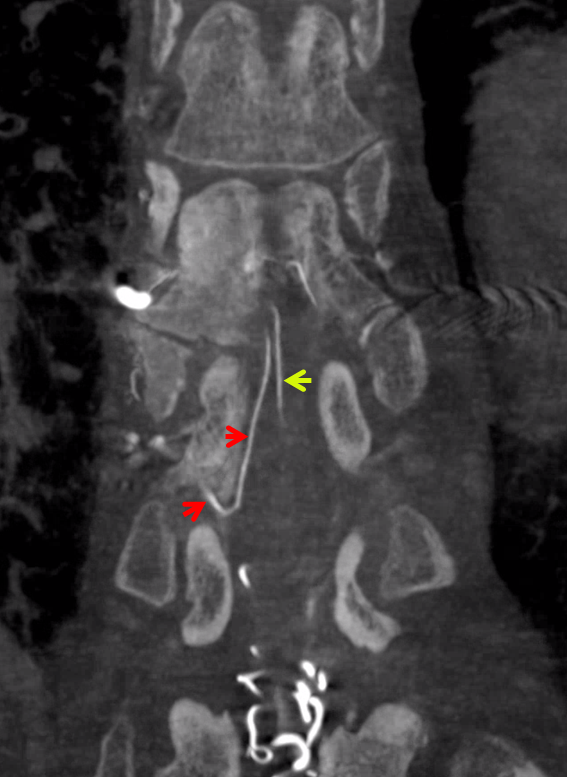
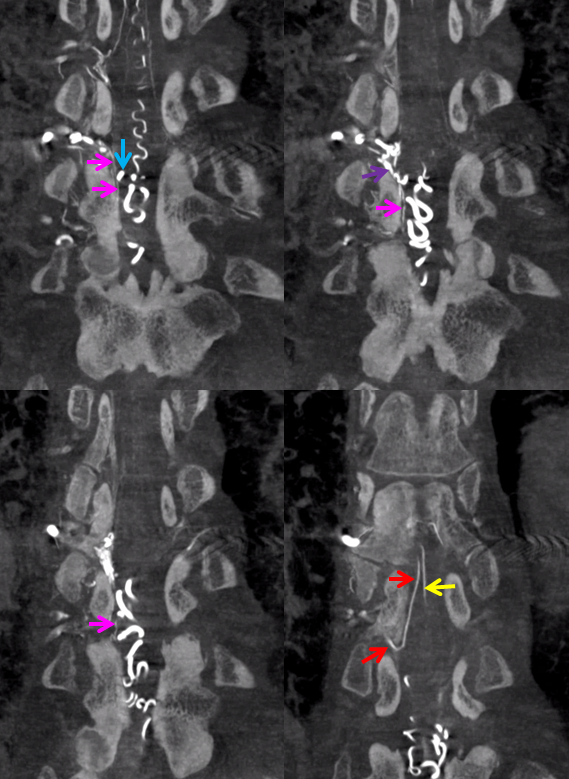
So, we do a DYNA CT — injecting from the right T8 fistula level. Guess what — the Adamkiewicz and anterior spinal artery are perfectly well seen now. Why — longer, stronger injection. What is the connection — a longitudinal vessel that runs in the lateral dura between the two nerve root sleeves. Fistula is purple arrow. Lateral dural connection is pink arrows. Adamkiewicz is red. ASA is yellow
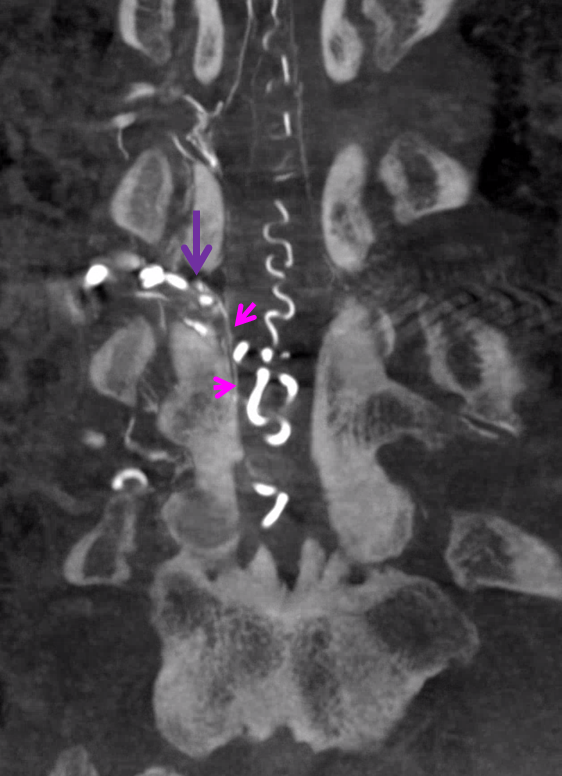
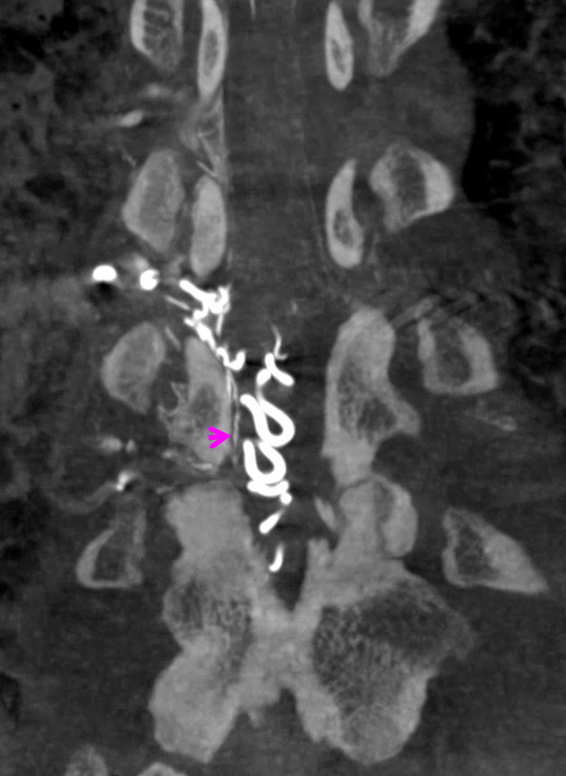
All in one
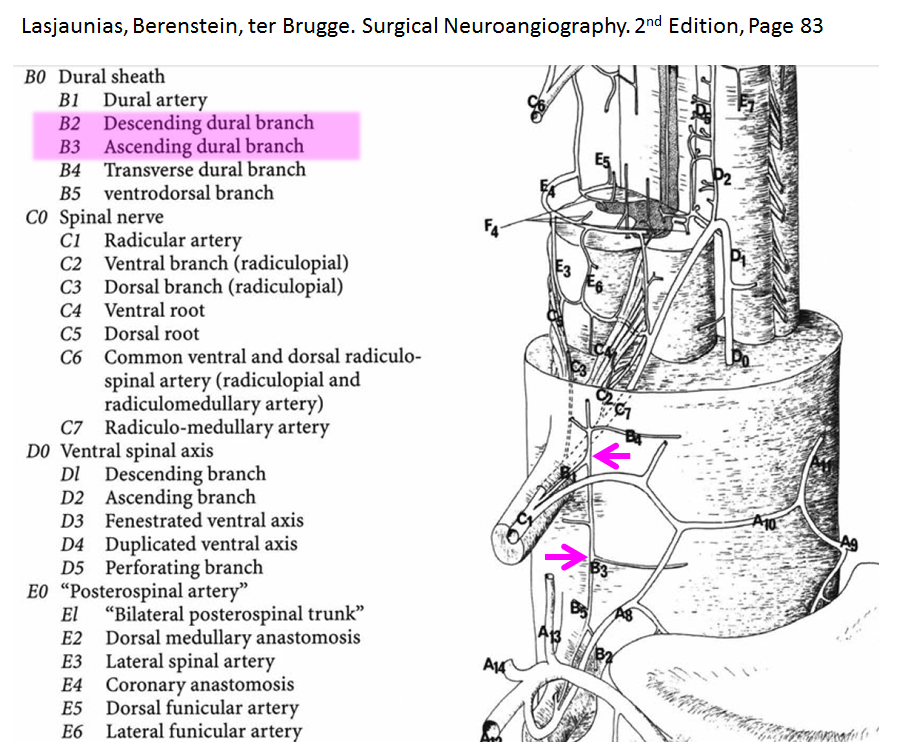
Here is the exact same branch in Lasjaunias/Berenstein/ter Brugge
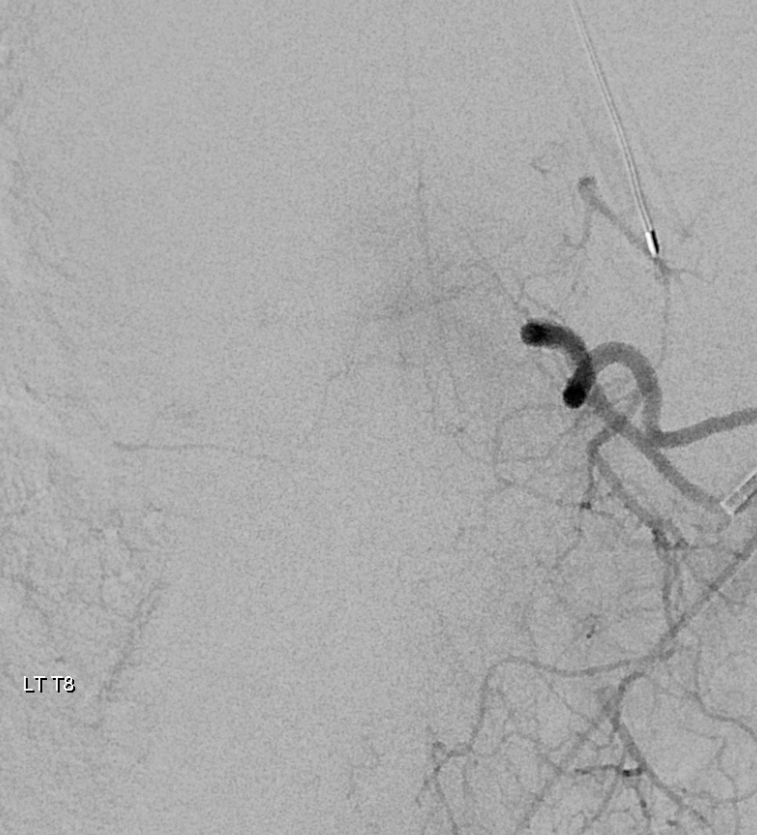
A stronger microcatheter injection of right T8 shows the same vessels on DSA
And, to boot, there is a large posterior spinal artery coming off from left T8, across from fistula.
Notice epidural arcade extending to the right (none are labeled). Posterior spinal of this size is also pretty important.
The fistula was disconnected surgically.
Conclusion: Know your anatomy and do a good quality angiogram.
Other cases:
- Check out the reverse — rational endovascular occlusion of dural fistula at SAME level as Adamkiewicz
- Check out how to protect adjacent level Adamkiewicz when its possible