
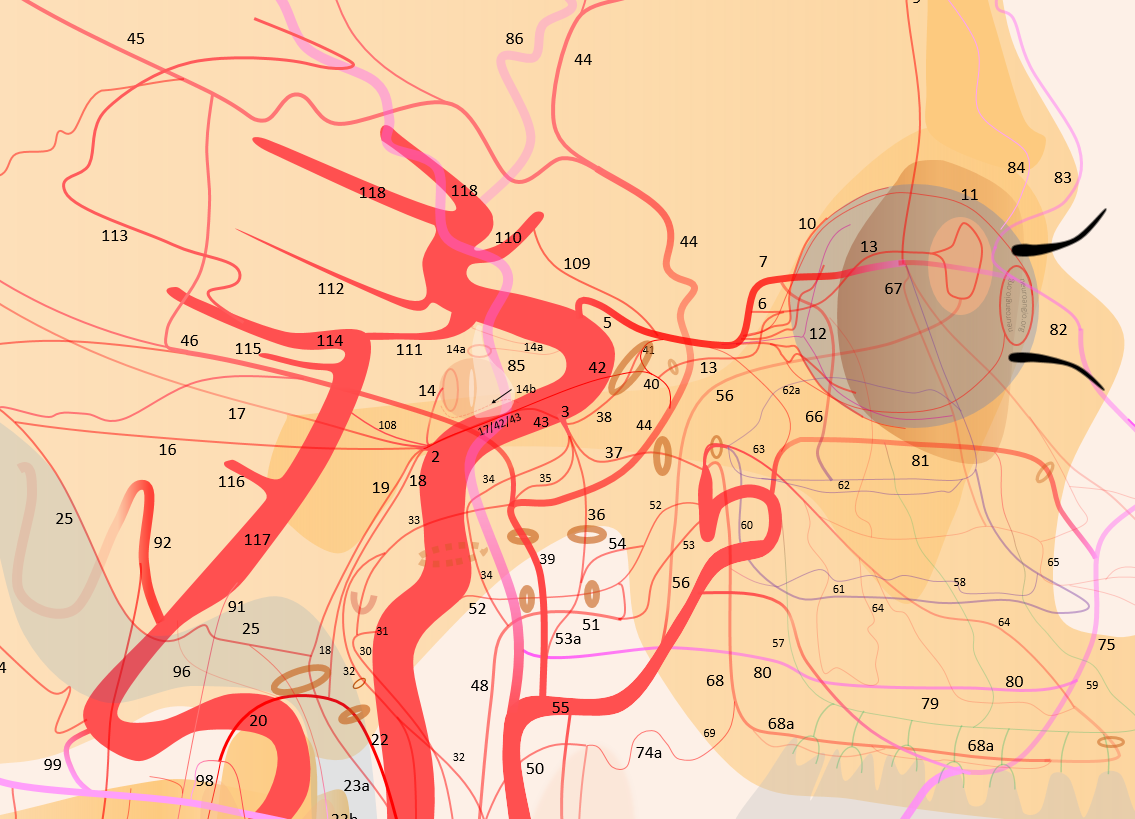
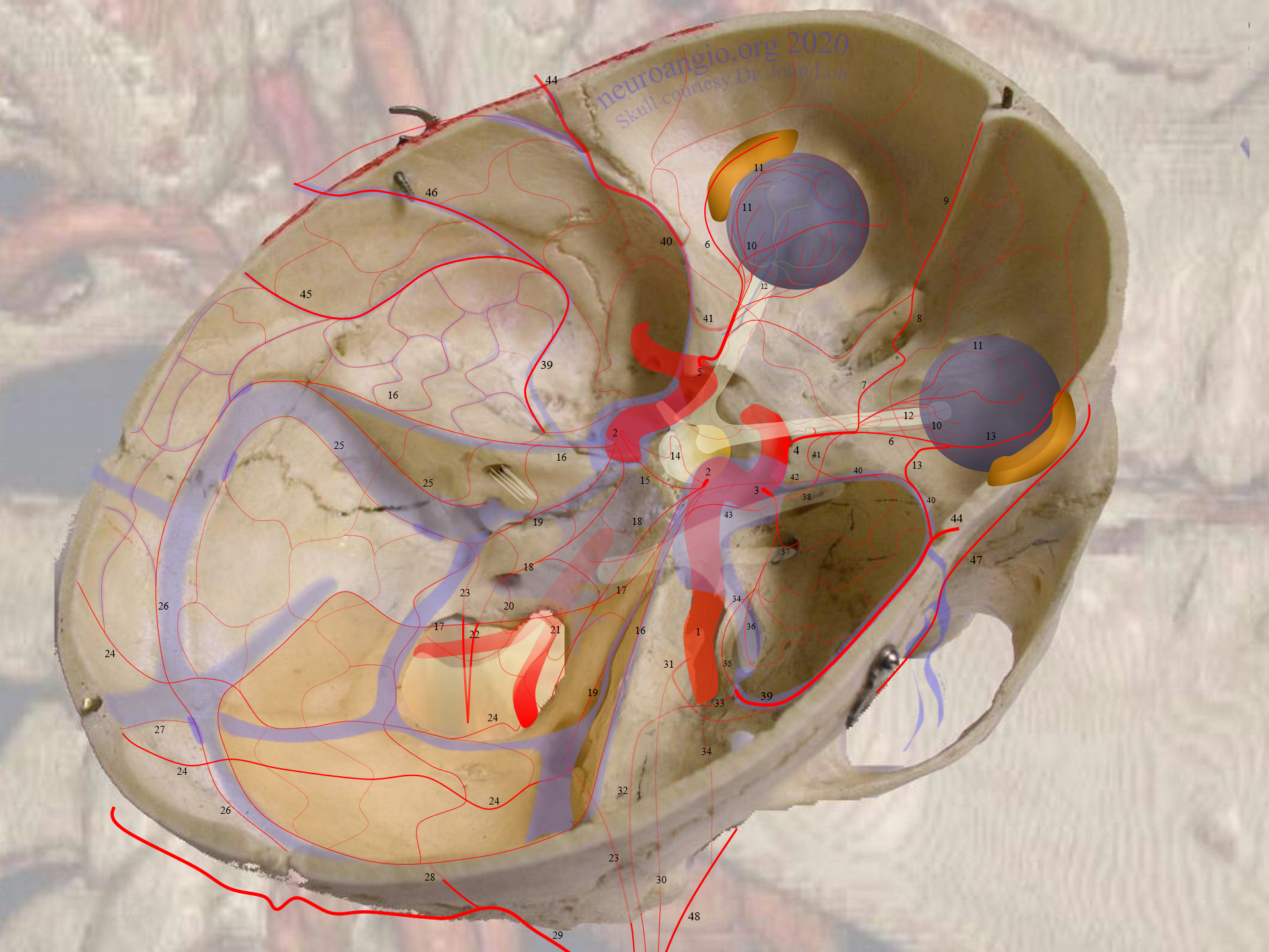
AMA — 53a. Soft tissue branch — 54. Meningeal branch — 36.
A real artery with serious cranial nerve and EC-IC anastomoses. Classically has extracranial and intracranial parts. Of course, everything varies tremendously.
The extracranial part is in the upper lateral nasopharynx. Supplies area around the Eustachian tube opening, to larger or smaller extent — in balance with the superior division of the ascending pharyngeal artery pharyngeal trunk, the pterygovaginal artery off the IMAX, the vidian. When large can take care of soft palate / pterygoid / posterior nasopharynx areas
The intracranial part classically enters to skull via foramen Ovale — hence its embolization endangers V3. Once inside, it can anastomose with all the usual suspects in the area — ILT, MMA — specifically the accessory meningeal can give rise to the petrous branch and its CNVII. So, be careful…
The classic Lasjaunias theory is in the relationship between the superficial and deep course of the IMAX, origins of middle and accessory meningeal arteries. The further an artery is from somewhere, the more likely it is that the arteries will come a common source. Common origin of MMA and AMA means the IMAX course is superficial.
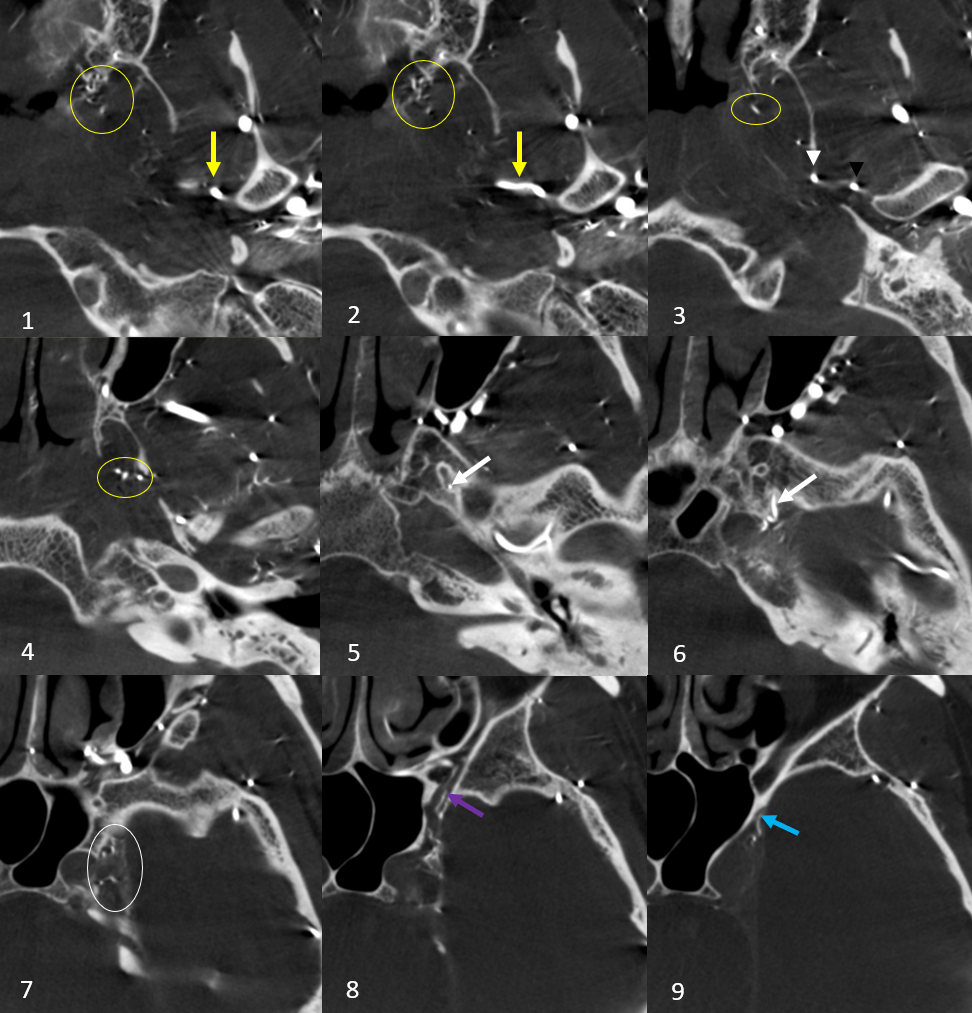
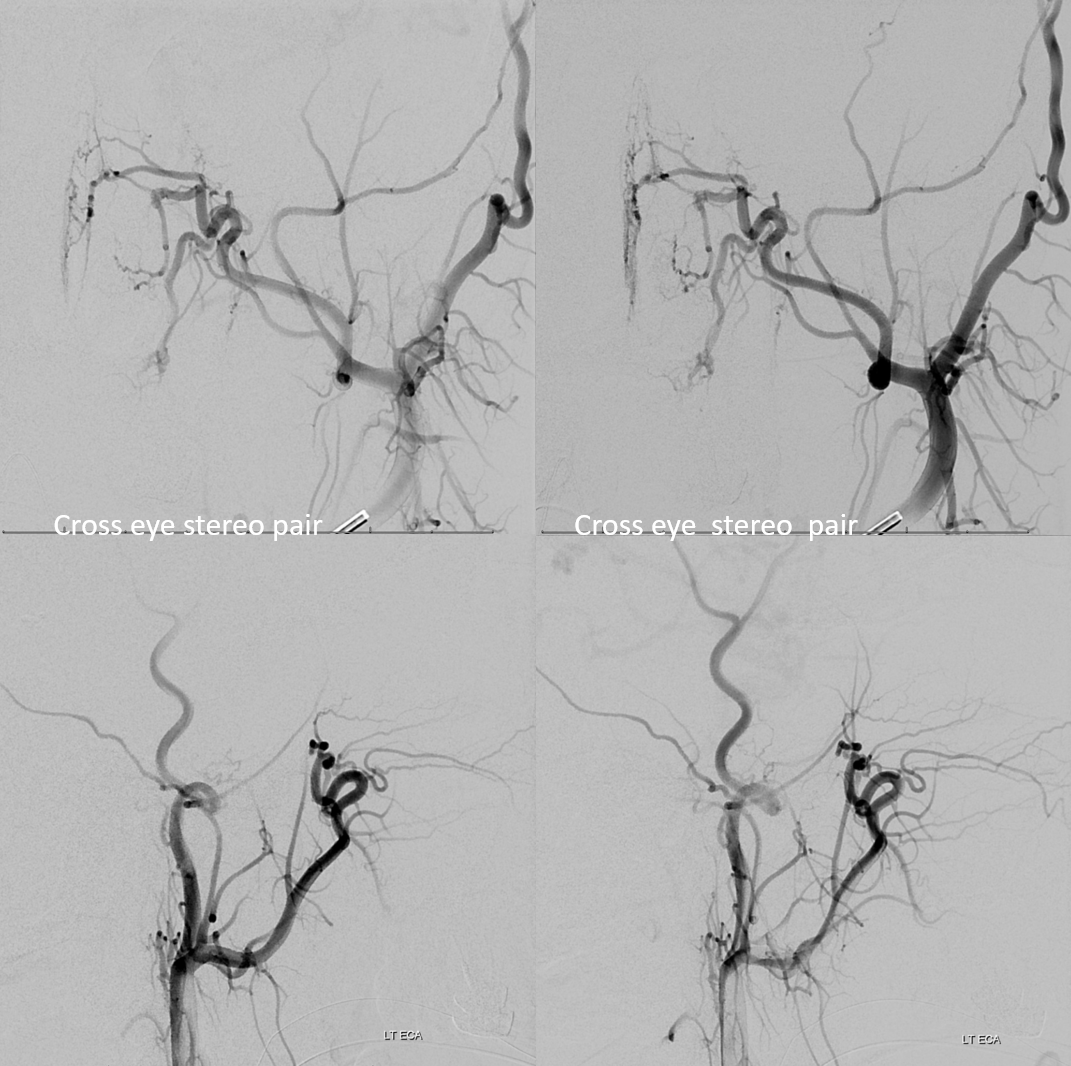
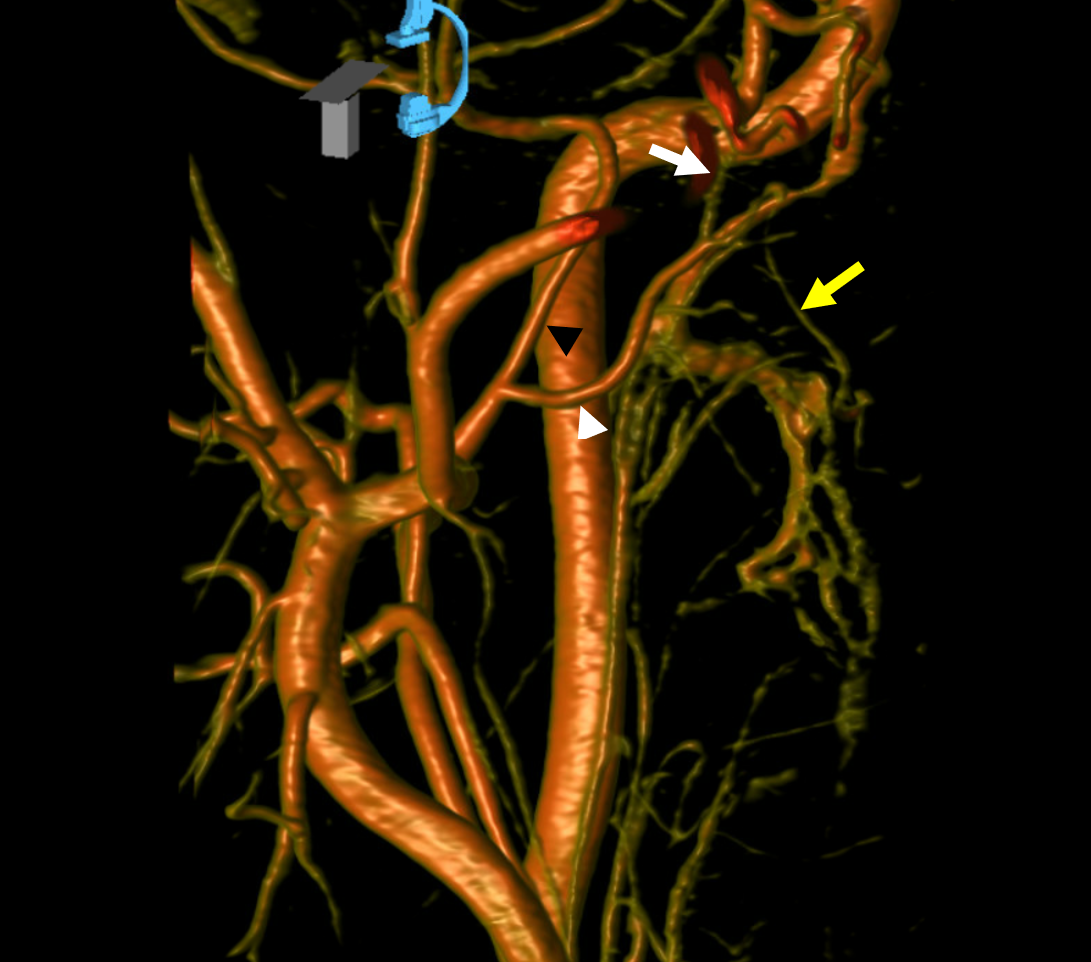
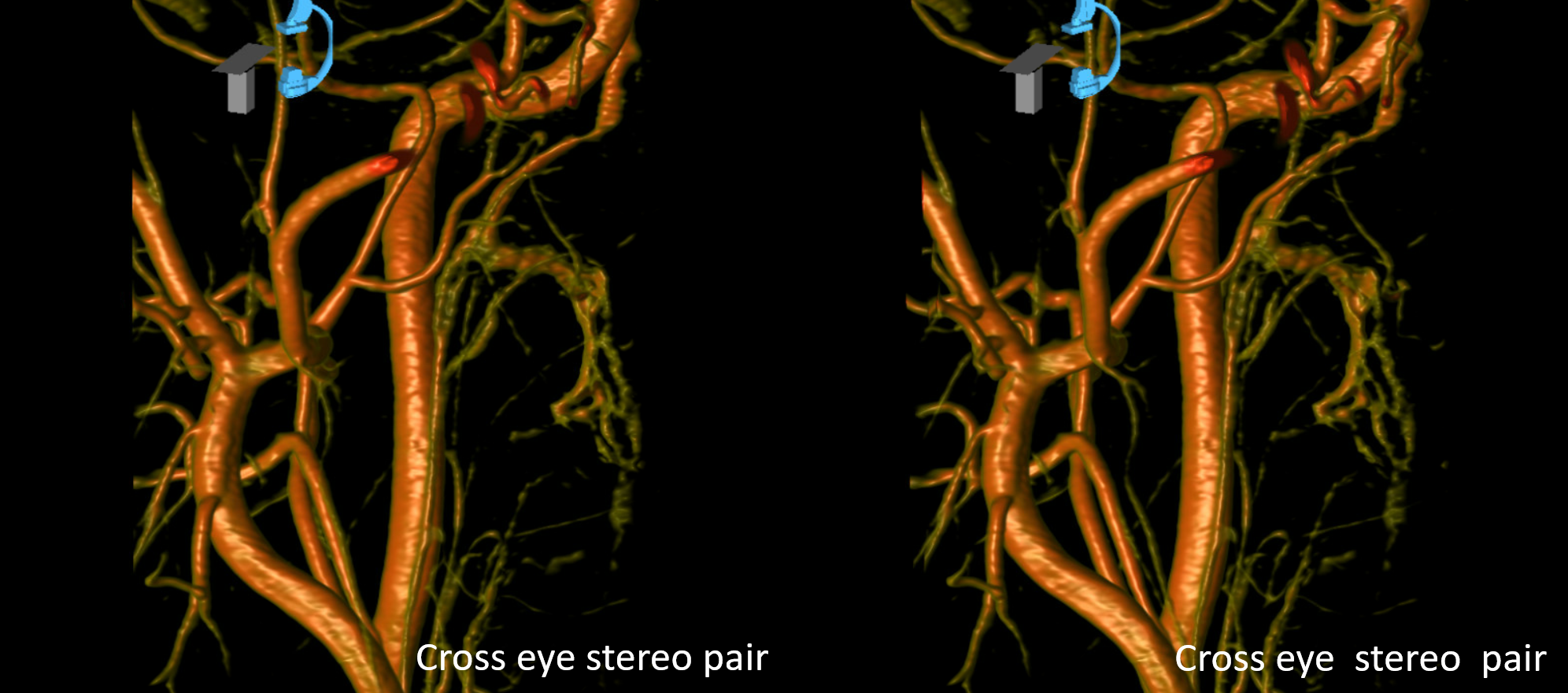
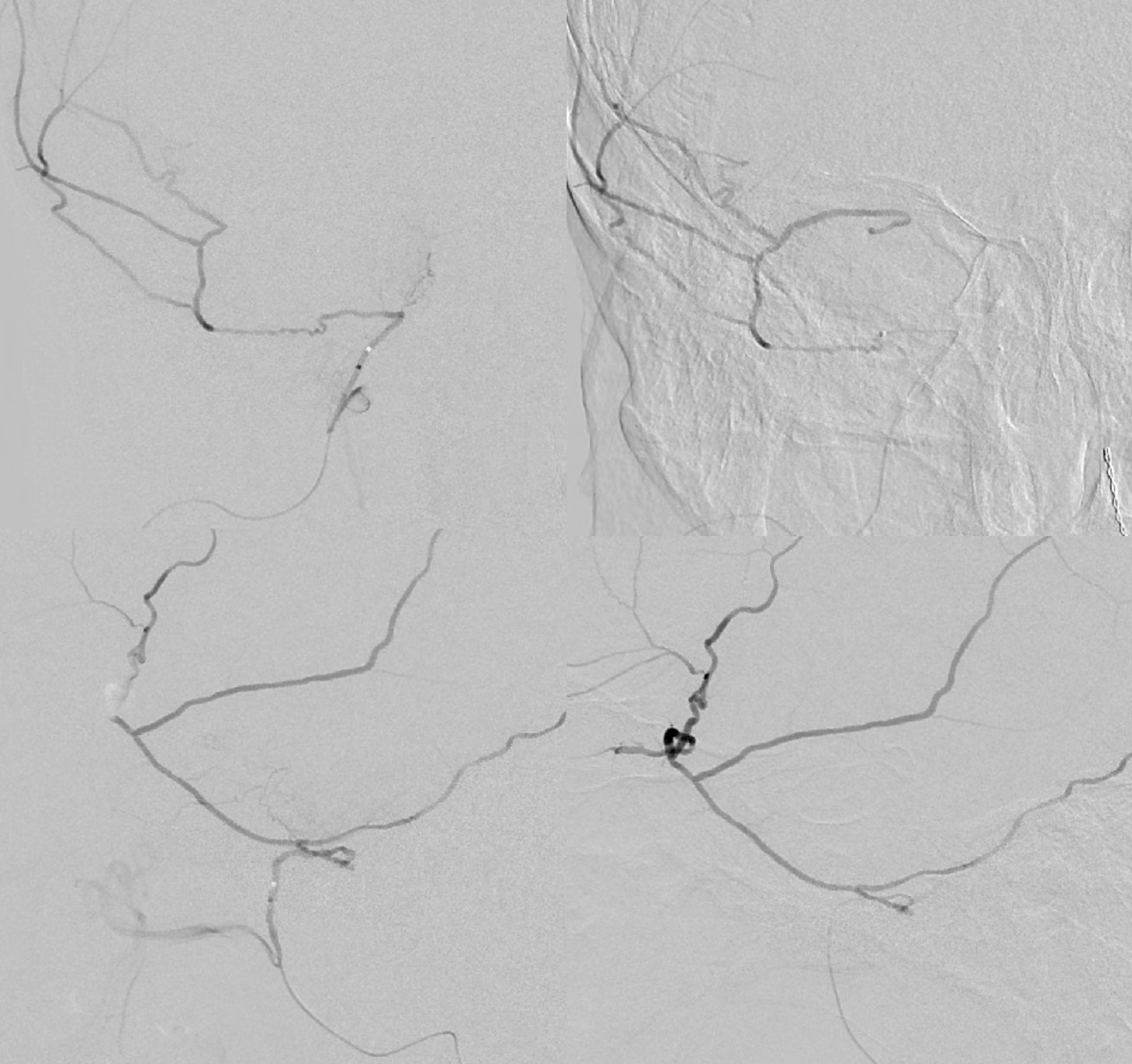
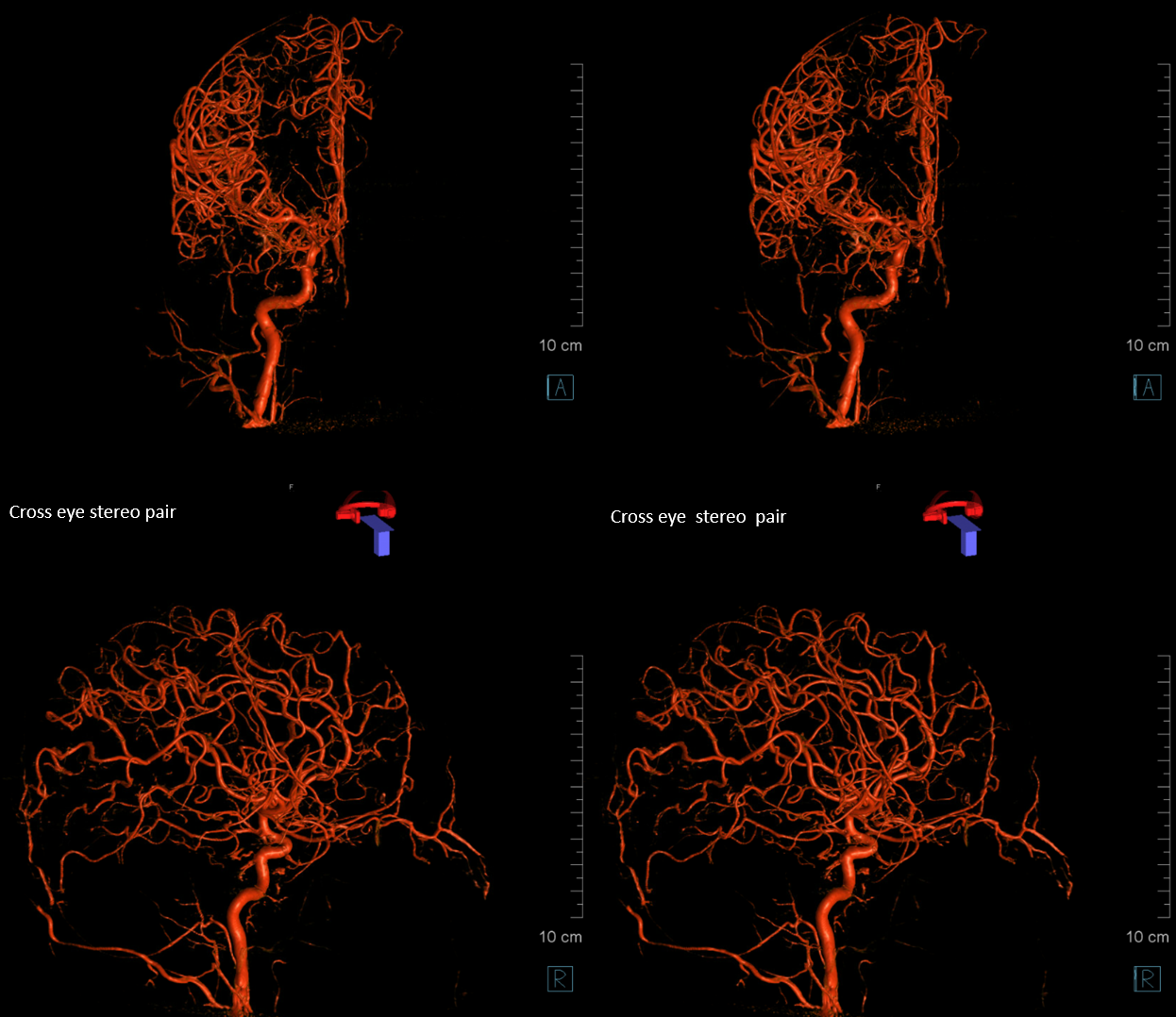
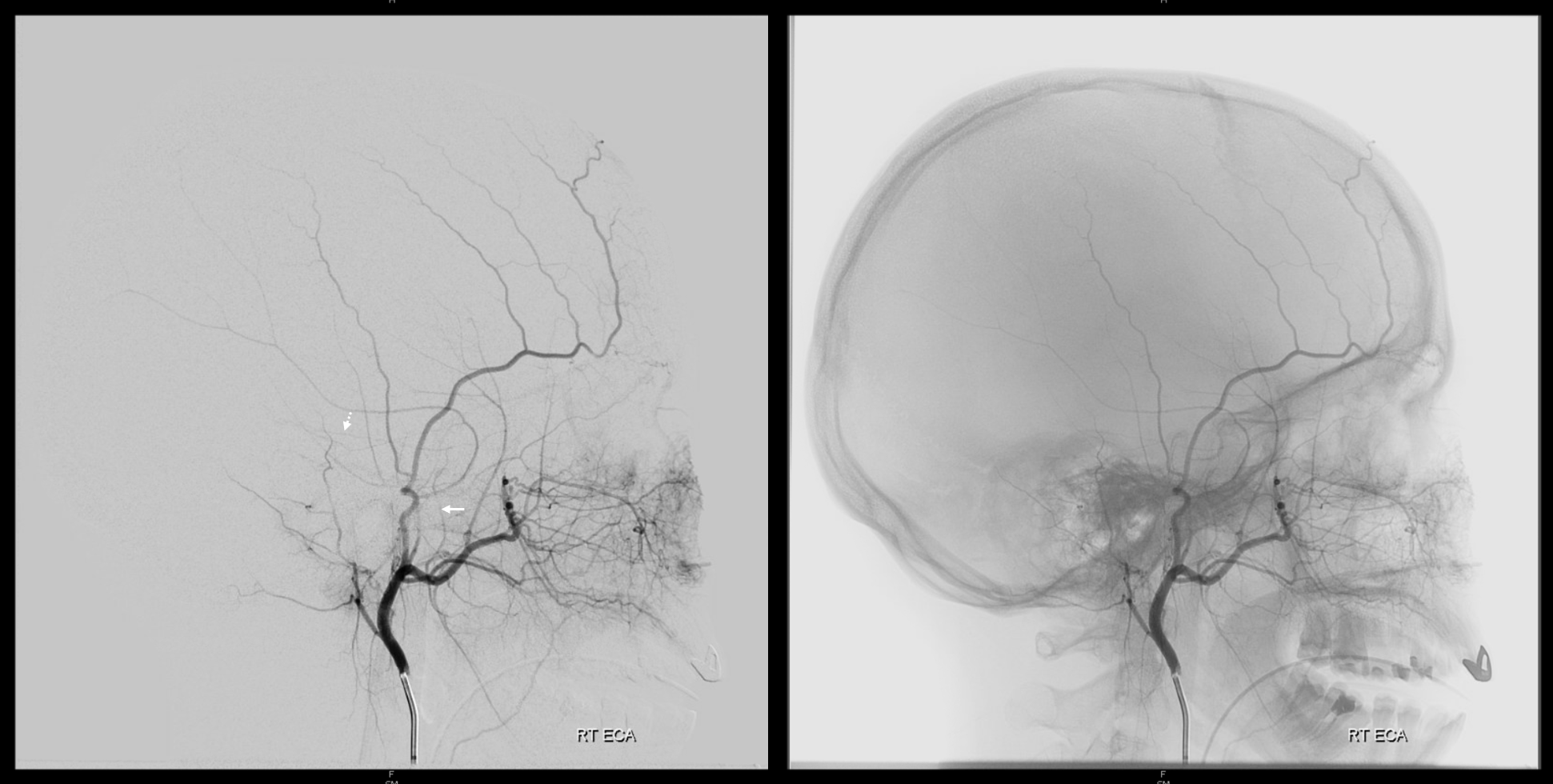
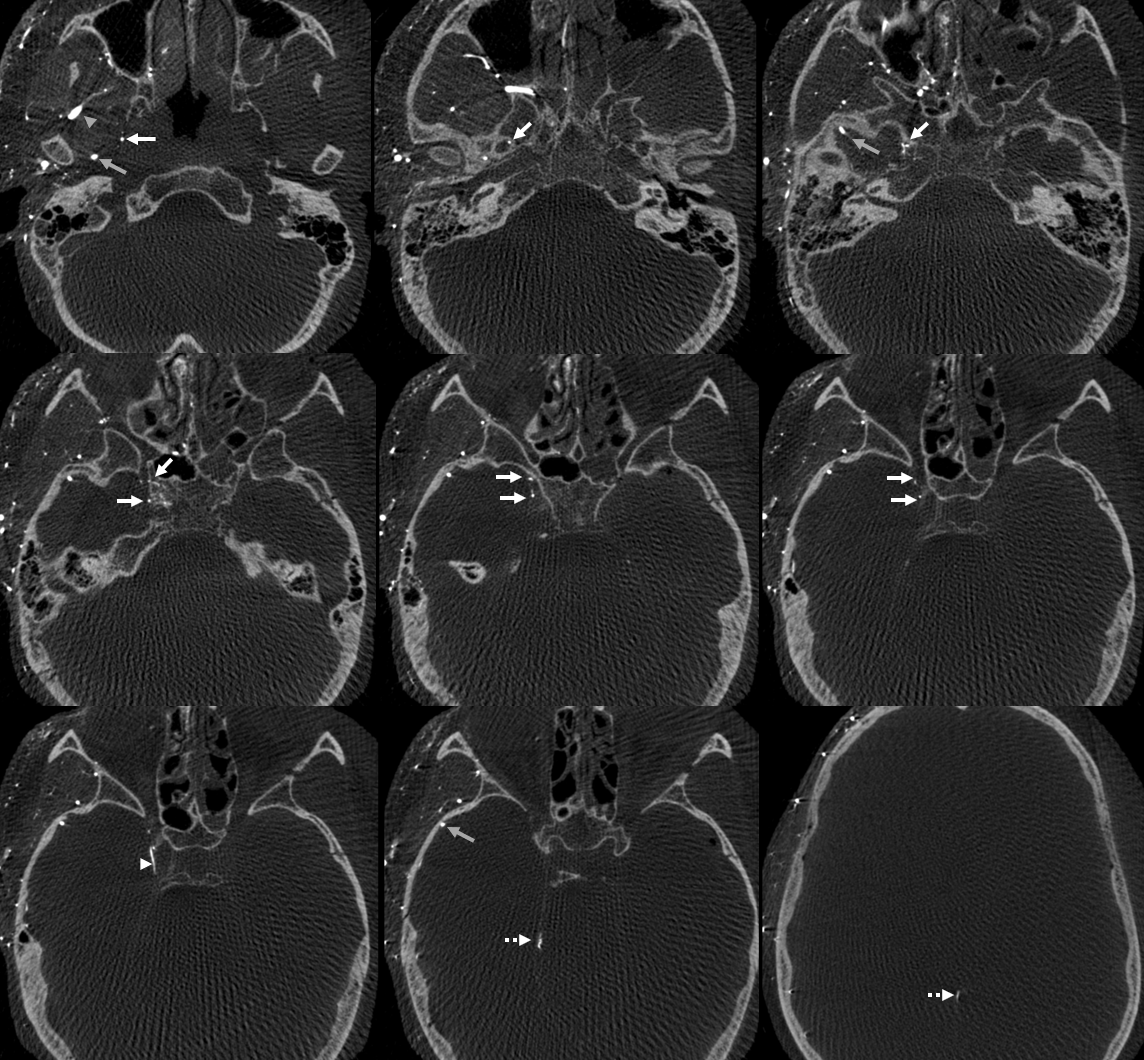
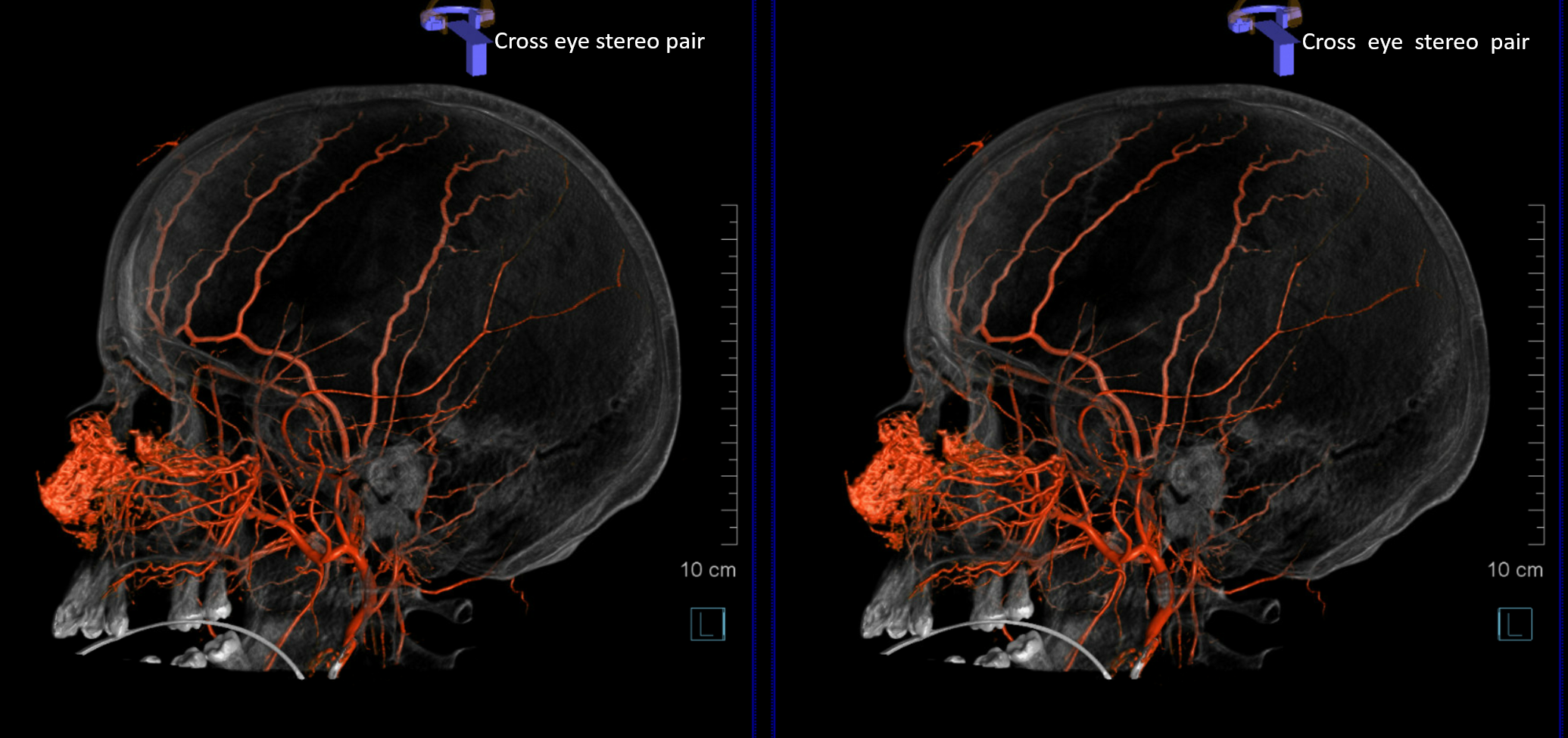
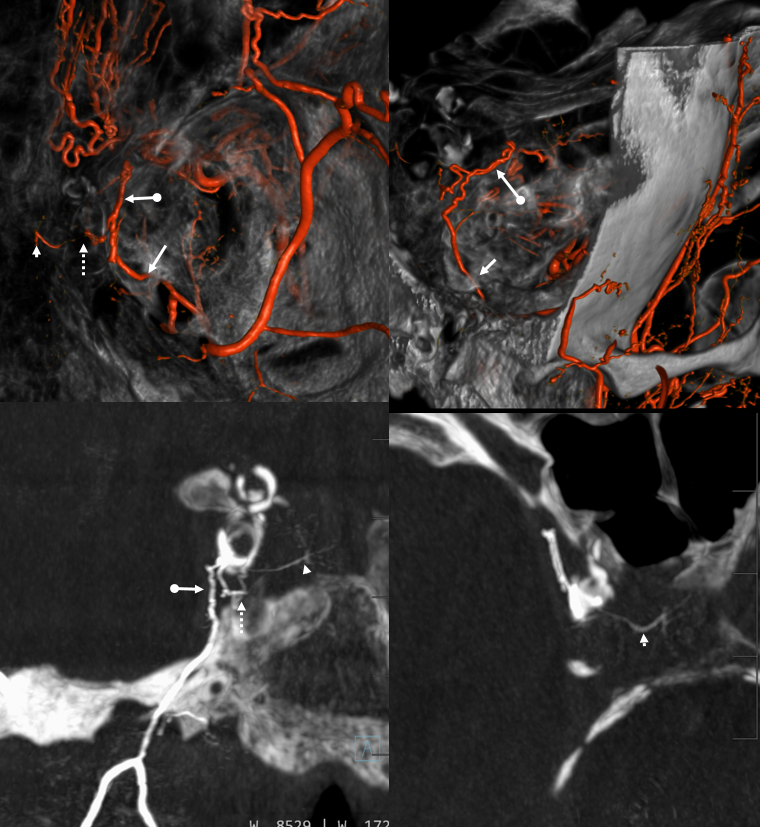
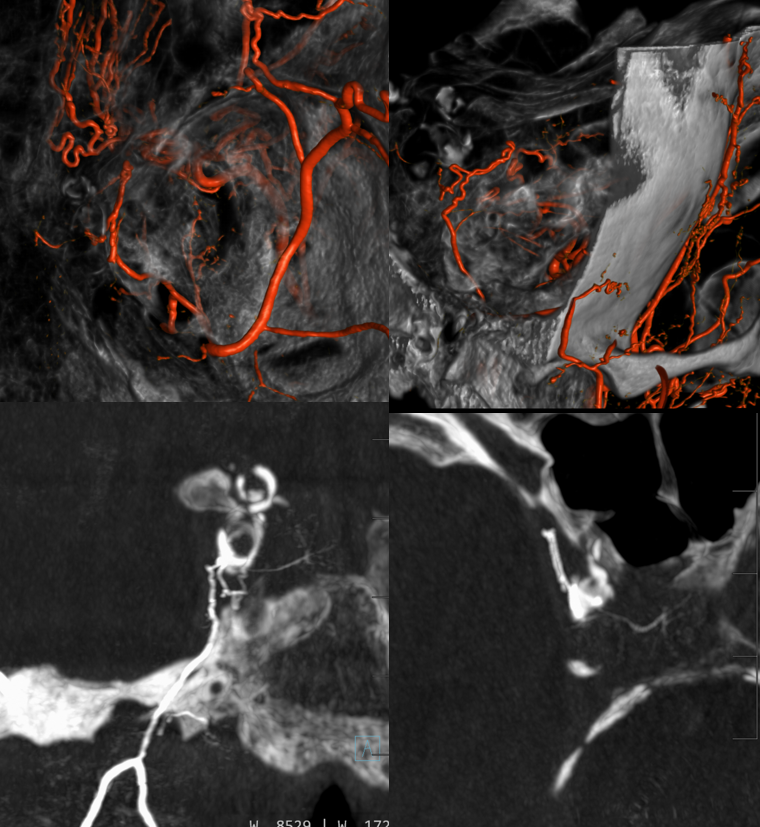
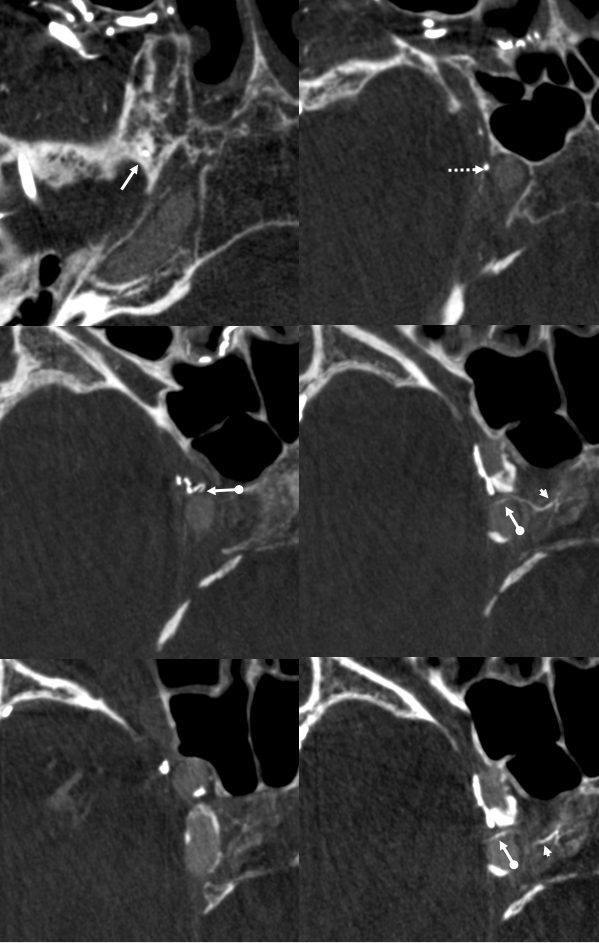
Below is a DYNA example of a large accessory meningeal. 1-9 is bottom to top. Common origin (yellow arrows) of MMA (black arrowhead) and AMA (white arrowhead) — as expected IMAX course is superficial. The large soft tissue branch breaks into multiple twigs that supply the soft palate (yellow ovals) — typically palate is lesser palatine or ascending pharyngeal territory.
The meningeal branch (white arrow) enters the skull via foramen of Vesalius (cool — at 10 o’clock relative to Ovale) and, not to be outdone by the large cutaneous branch, is also of possessive character — multiple branches to the Meckel cave region (white oval) are present — embo would endanger all those nerves. Specifically seen are artery of foramen rotundum (purple) and the anteromedial branch (blue) — typically this comes off the ILT as “dorsal ophthalmic artery” remnant — and an important “dangerous” anastomosis with the ophthalmic artery. Explanation — ILT is hypoplastic — hence supply to area comes from AMA. Remember, its all about balance. Here, the situation is not balanced, with an oversized AMA
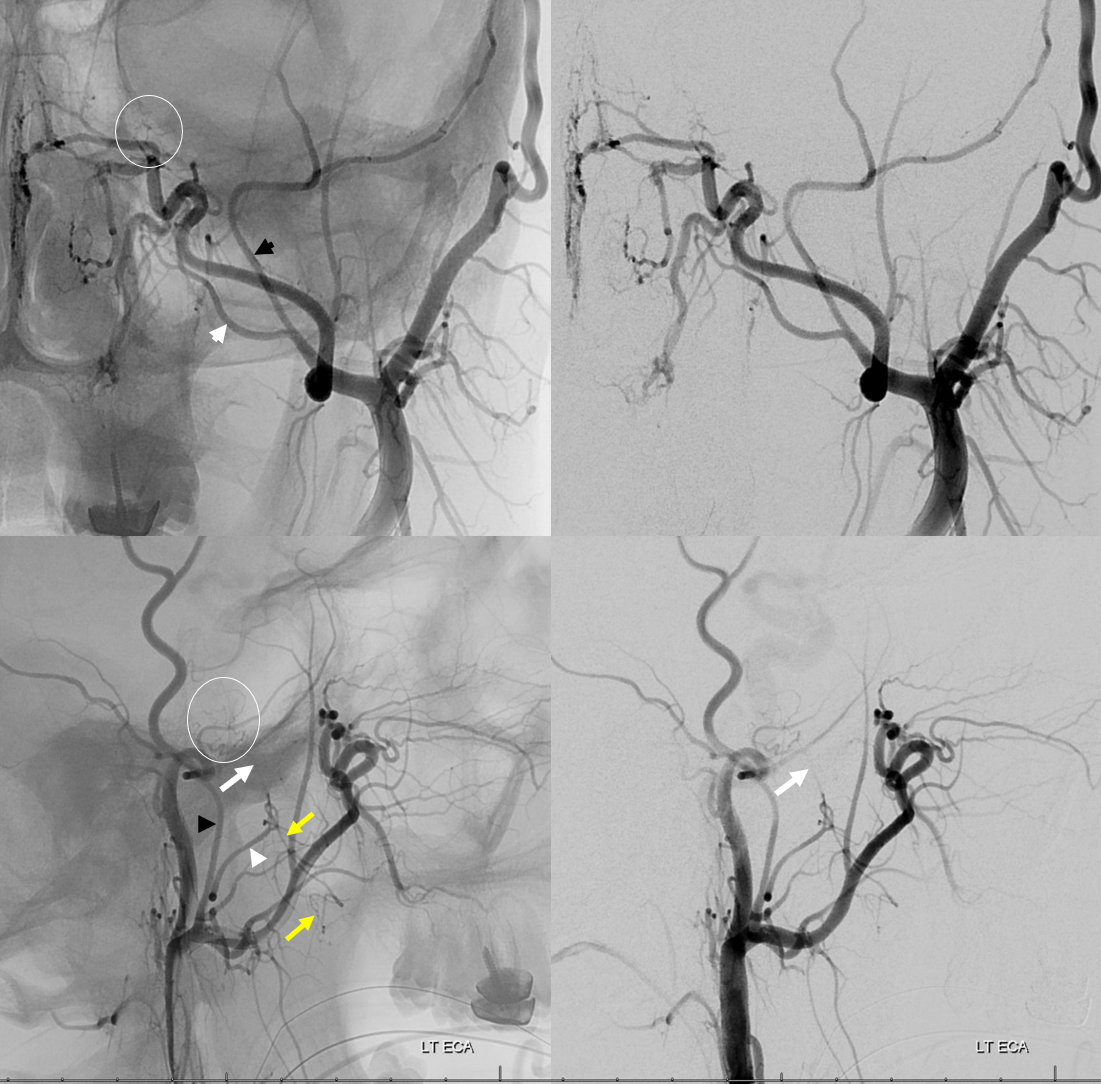
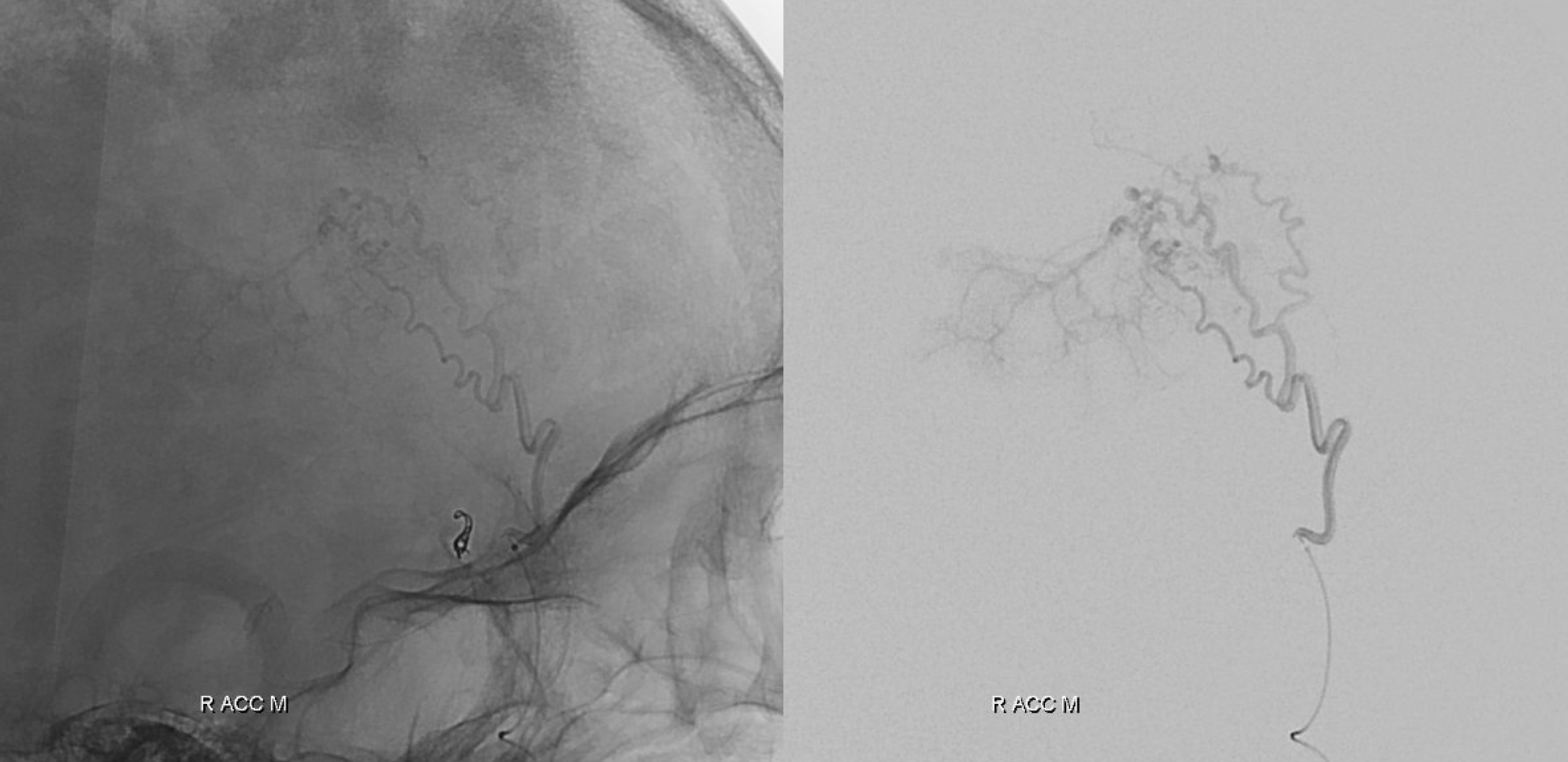
Angio views — same arrows as above — except that yellow arrows point to the soft tissue branches of the AMA, and not to the common AMA/MMA trunk, which is unlabeled
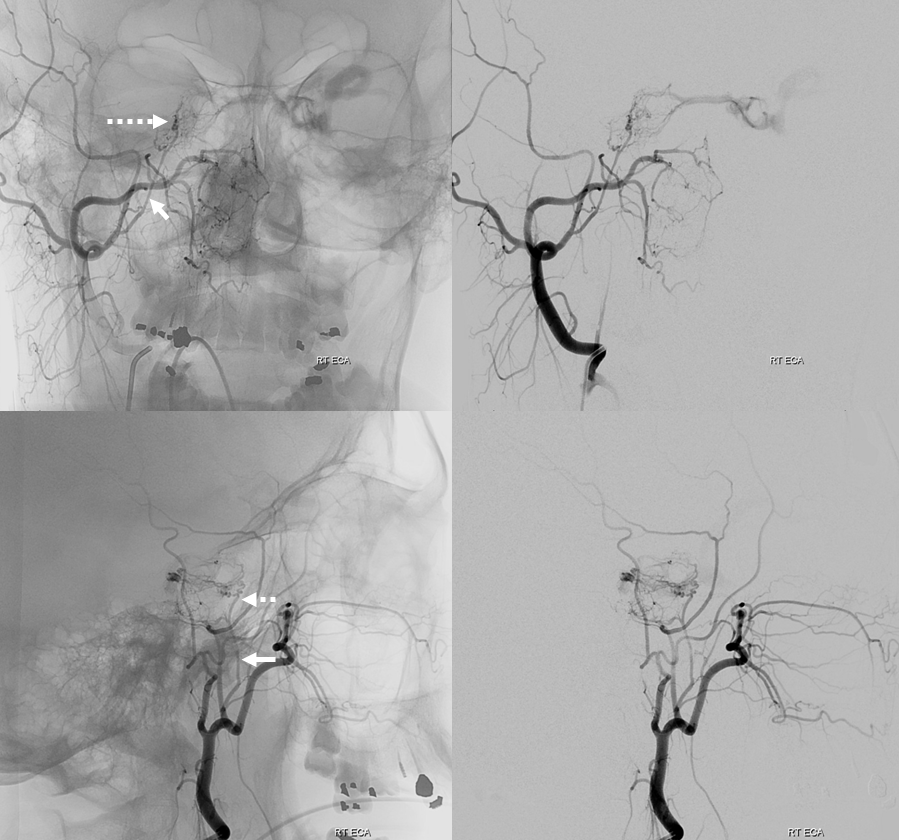
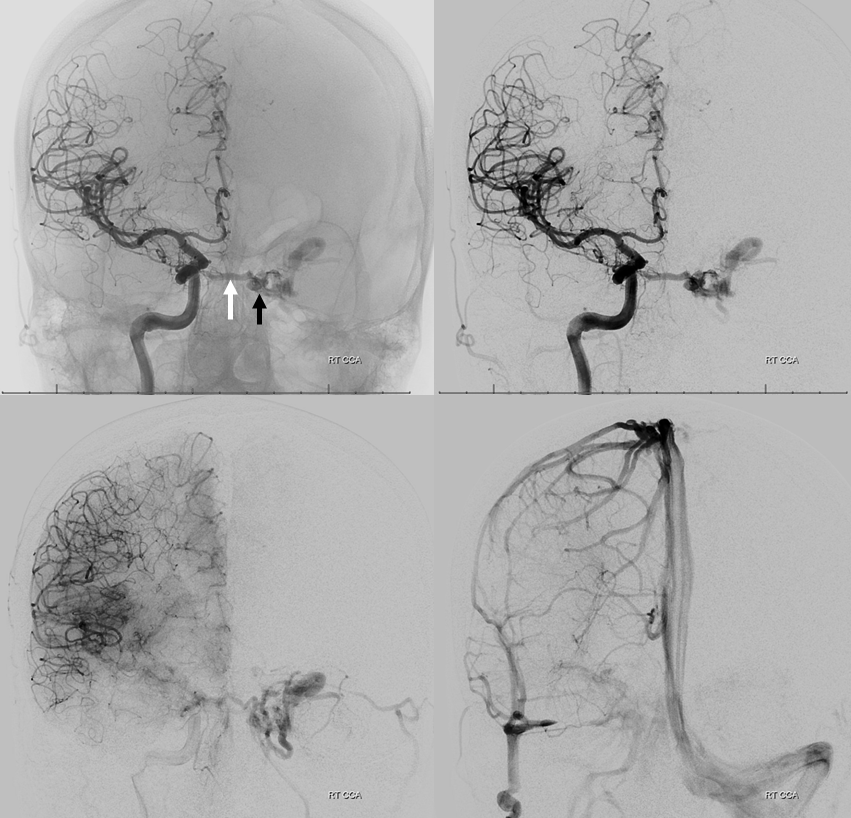
AMA supply of cavernous dural fistula
Full case is here.
Although the AMA might seem like some distance away from the posterior cavernous sinus (the most common site of cavernous dural fistula venous pouch), its propensity to participate in fistula supply highlights role of the cavernous branch of the AMA as a potential ILT/ MHT collateral.
Here, the fistulas is in LEFT posterior cavernous sinus (black arrow — venous pouch). Supply from right ascending pharyngeal opacifies the posterior clival branch of the MHT (white arrow) — principal contributor to fistula
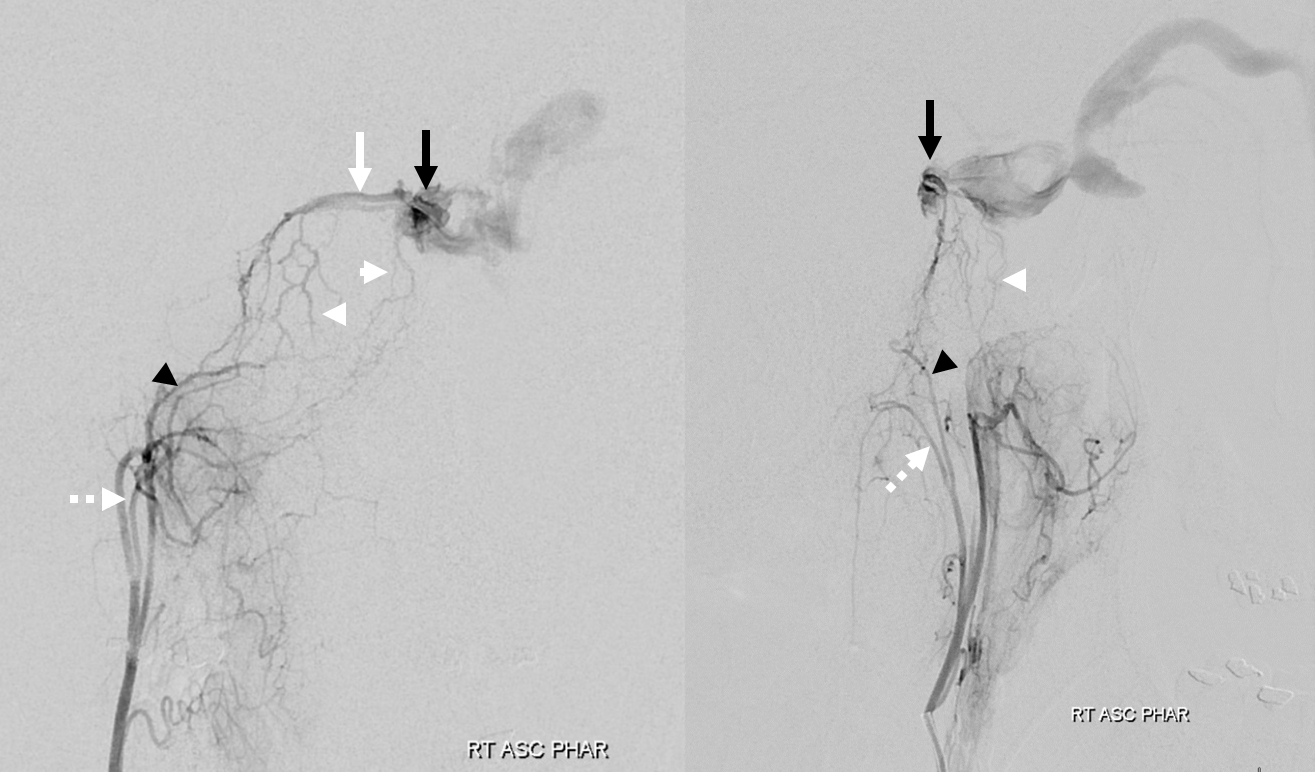
The right AMA (white arrows) also supplies it, via cavernous branches (dashed arrows)
DYNA CT of same
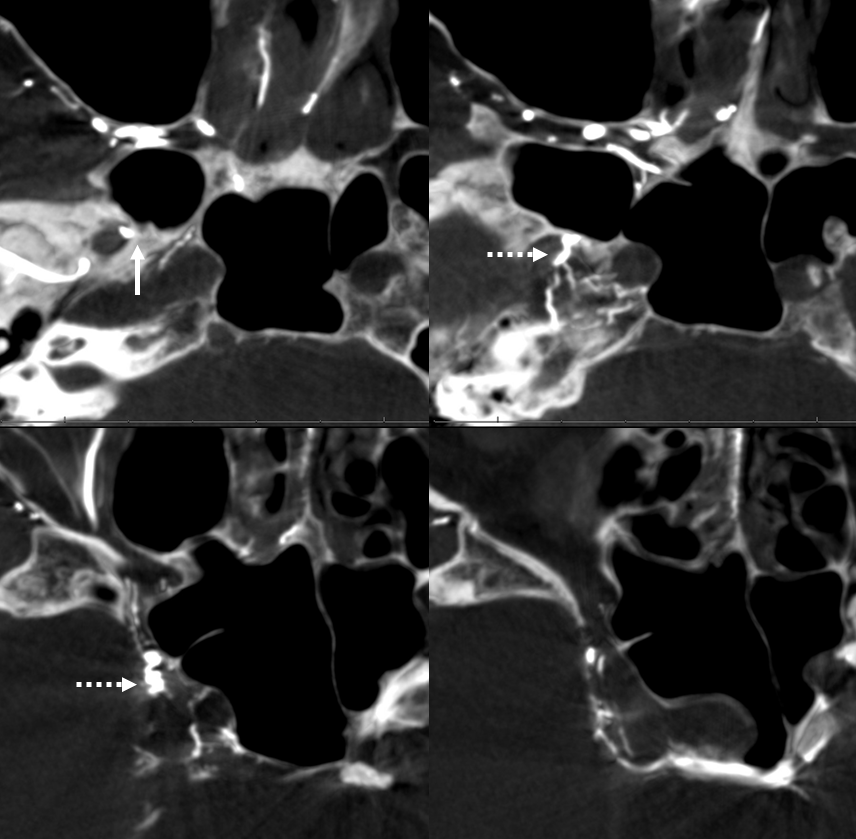
The same fistula is supplied by left AMA as well (same arrows), but to lesser extent — as sometimes happens in cavernous fistulas, the ipsilateral side might not be the dominant supplier.
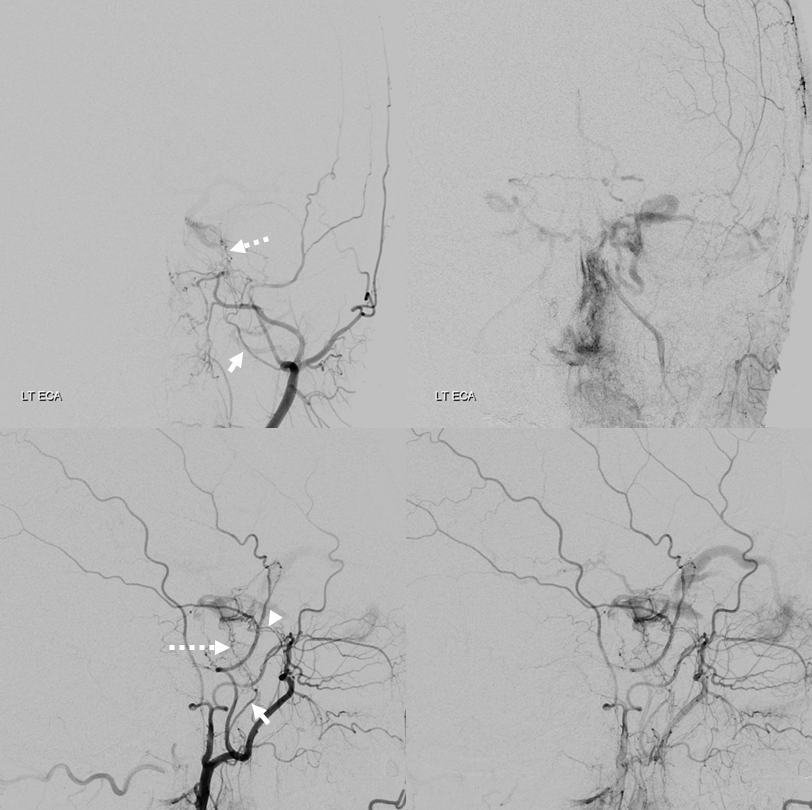
DYNA
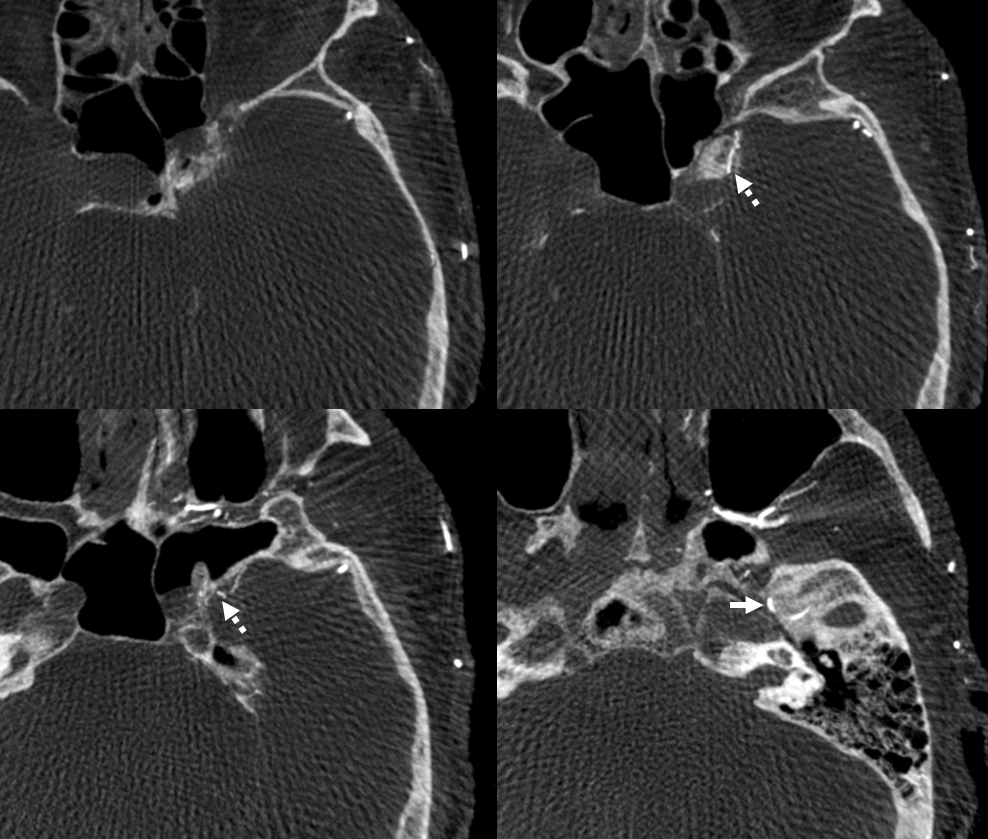
For completeness sake, supply from right ICA via the MHT — the white arrow is on an artery (intercavernous / medial clival), not vein
Accessory Meningeal ICA Reconstitution
Left ICA — chronic occlusion. Accessory Meningeal and Foramen Rotundum reconstitution of the carotid via the ILT — look ’em up! Full case — great revascularization of the left M2 via the PCOM is here

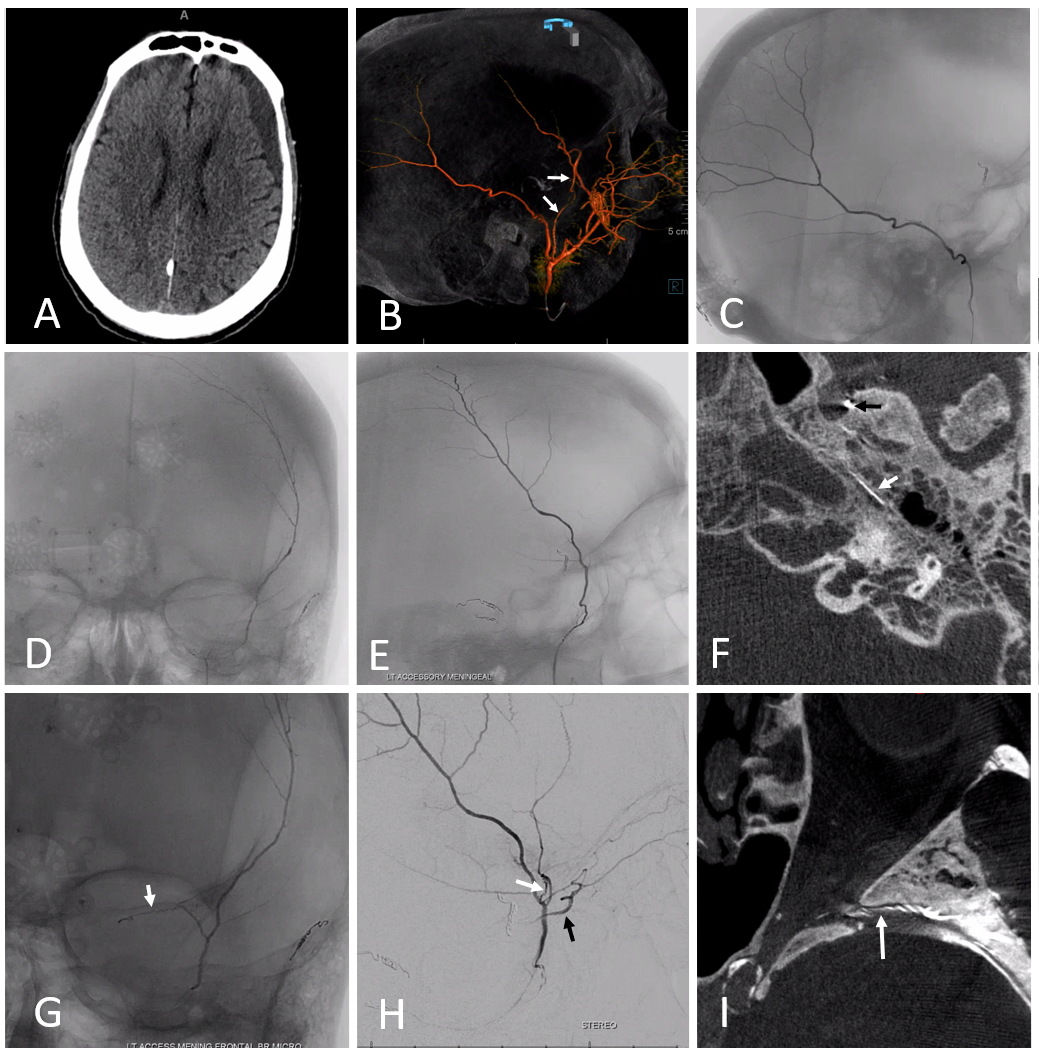
Variant — Accessory Meningeal Supply of Frontal Branch and Petrous branches of MMA
The frontal branch variant is rare. The petrous one might not be so rare after all. Just because ovale is more anterior than spinosum doesn’t mean it wont do the job.
In the case below, a variation is present with frontal MMA branch (B, white arrows) supply from the accessory meningeal artery, which also supplies the petrous branch (F, white arrows. Black arrow is on catheter tip in foramen ovale). Images G, H, and I show sphenoid ridge branch (white arrows) opacifying the ophthalmic artery (black arrow) during superselective catheterization of the frontal branch (in this case of AMA origin) — this connection was not visible on a nonselective injection (B) So, be careful…
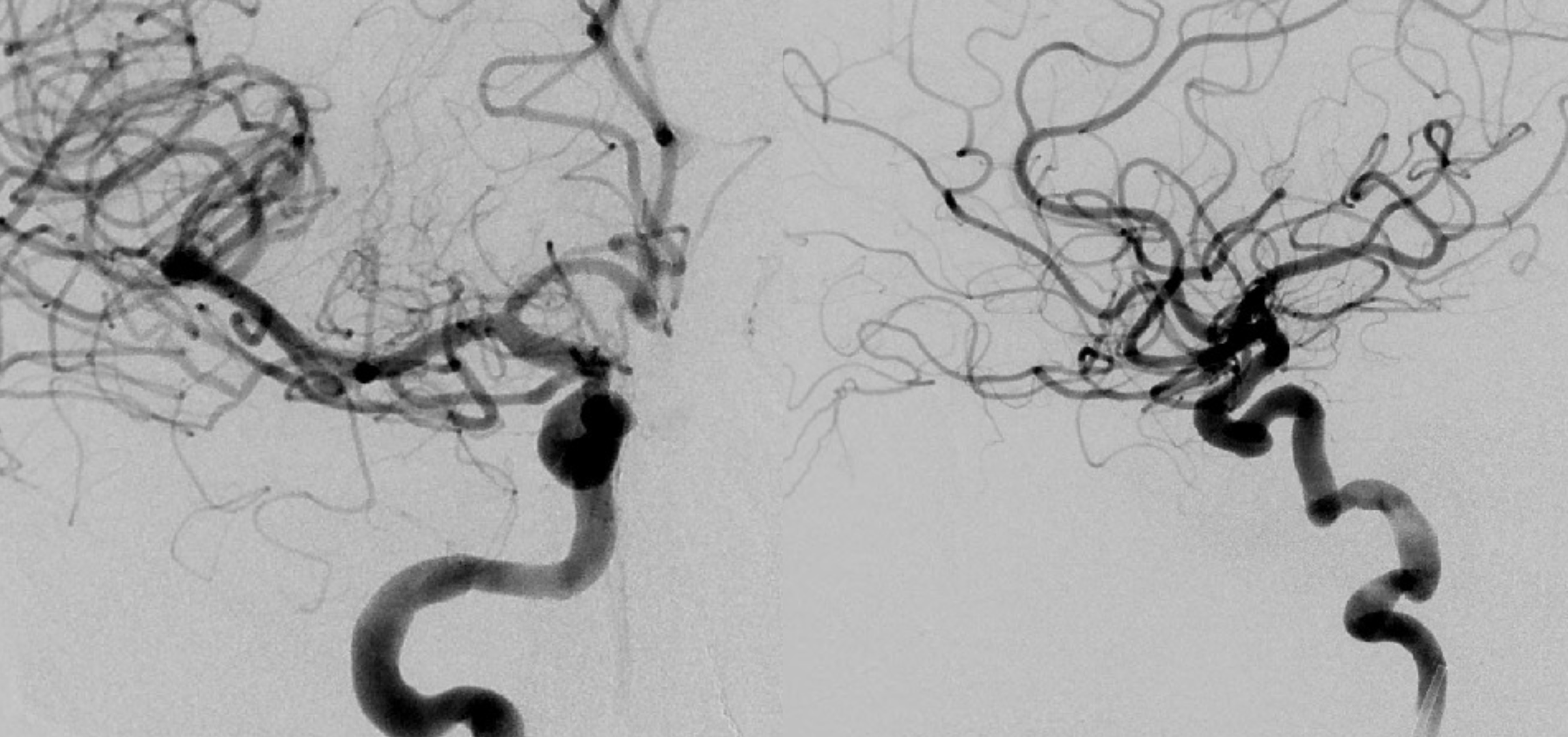
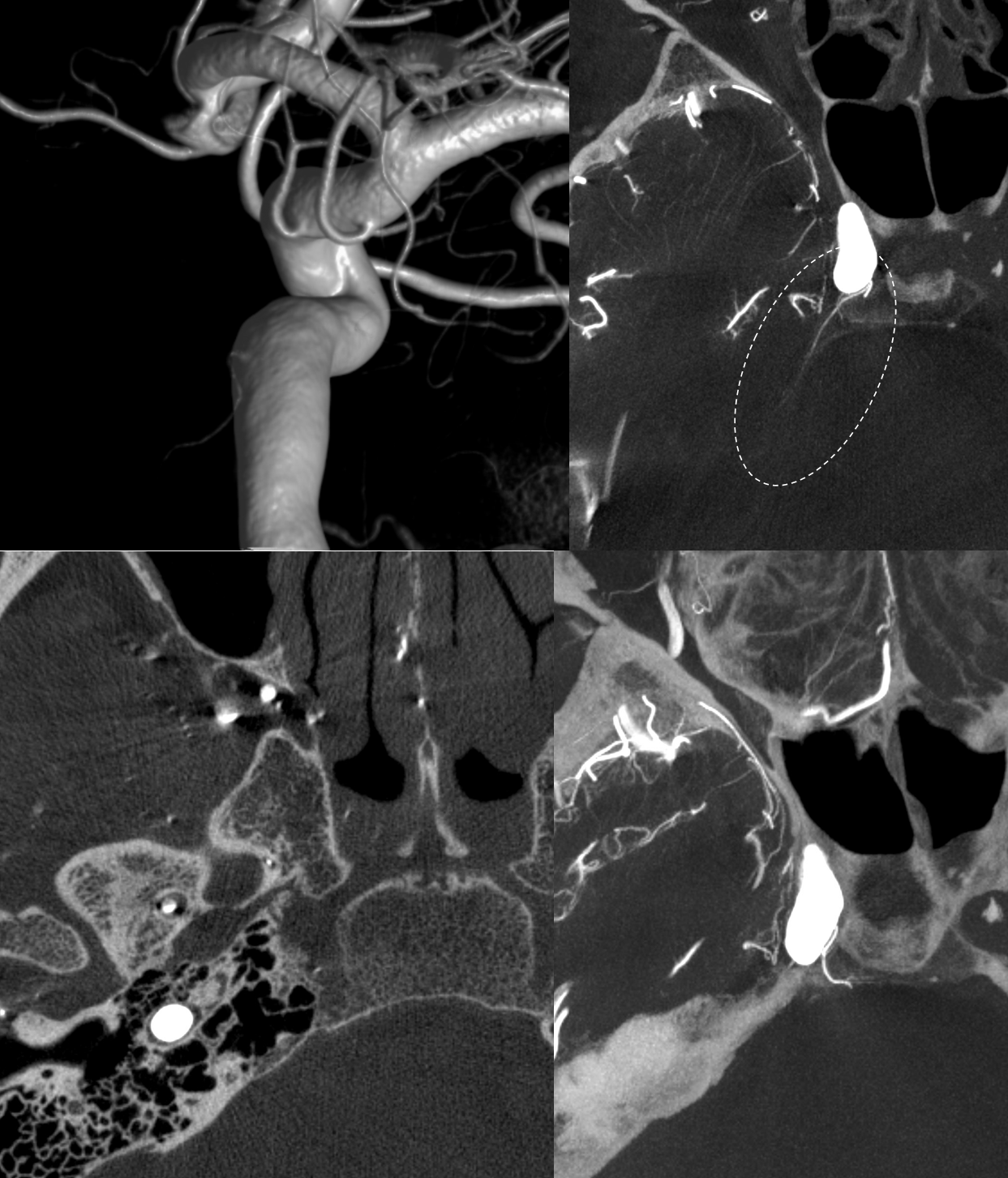
Complete Middle Meningeal Artery Supply by the Accessory Meningeal Artery — Extremely Rare
Again, we return to the idea of the spectrum — central notion of the neuroangio approach to anatomy. Basically, the most “balanced” arrangement between two or more territories is most common and by definition “classic”. Progressively greater takeover of one territory by another is correspondingly rarer. In other words, the more completely one territory supplies the classic distribution of another, the rarer that is seen. This extremely rare variant of complete MMA supply by the accessory meningeal was seen by Dr. Raz in context of MMA embolization.
Distal ECA — see the unusual origin and course of vessel supplying the MMA territory — more distal origin along IMAX and a posterior course along the floor of middle cranial fossa?
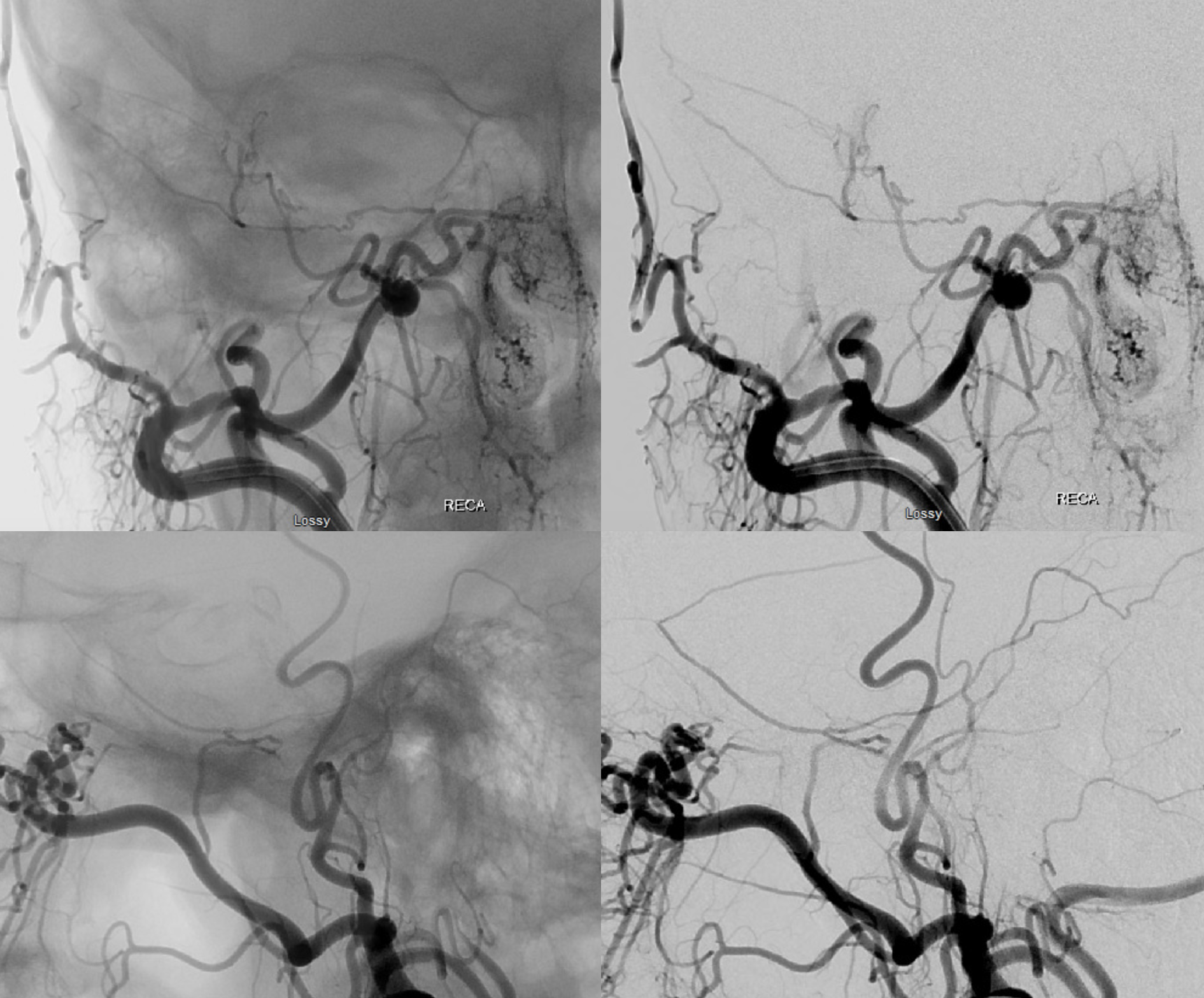
Stereos!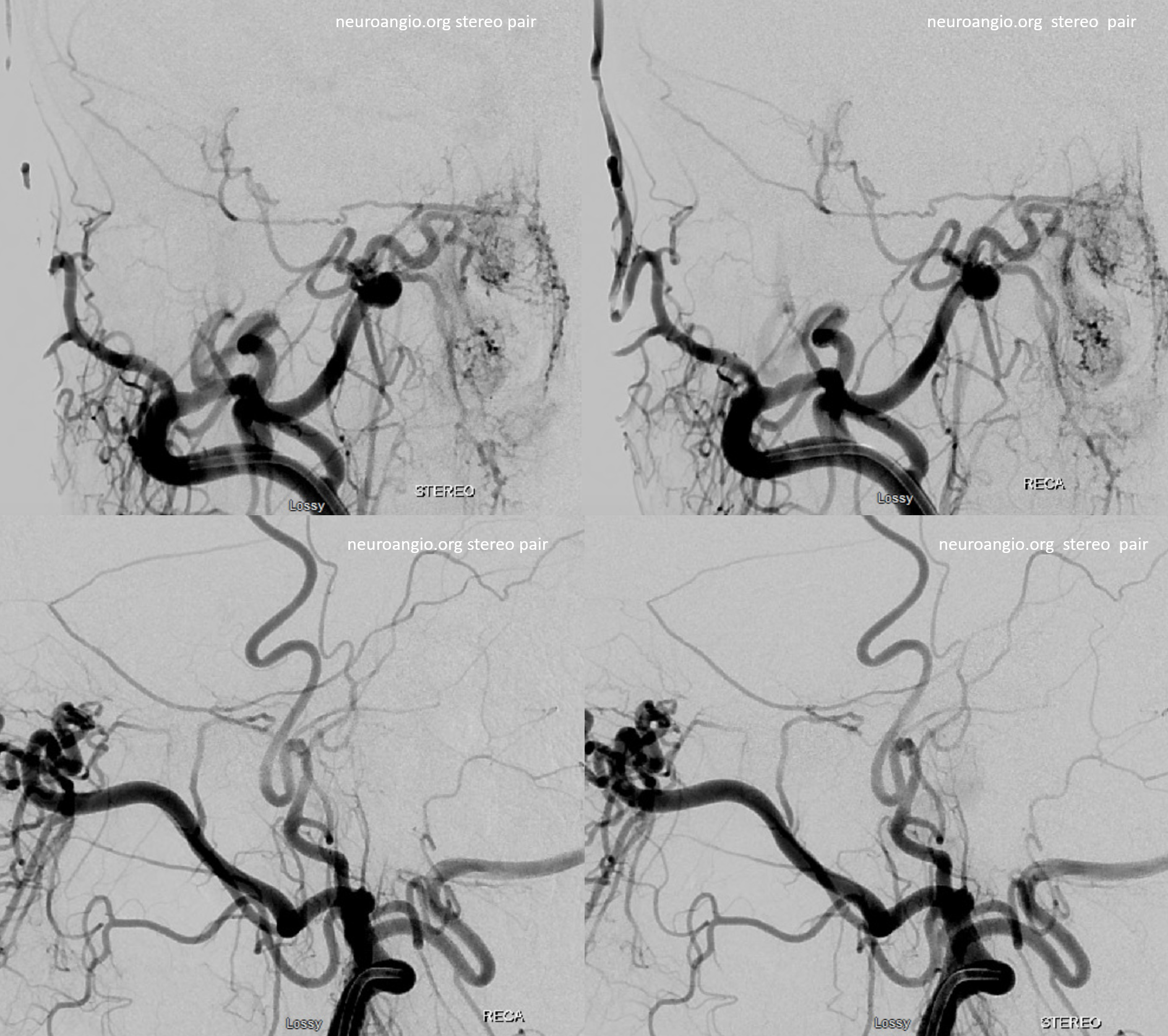
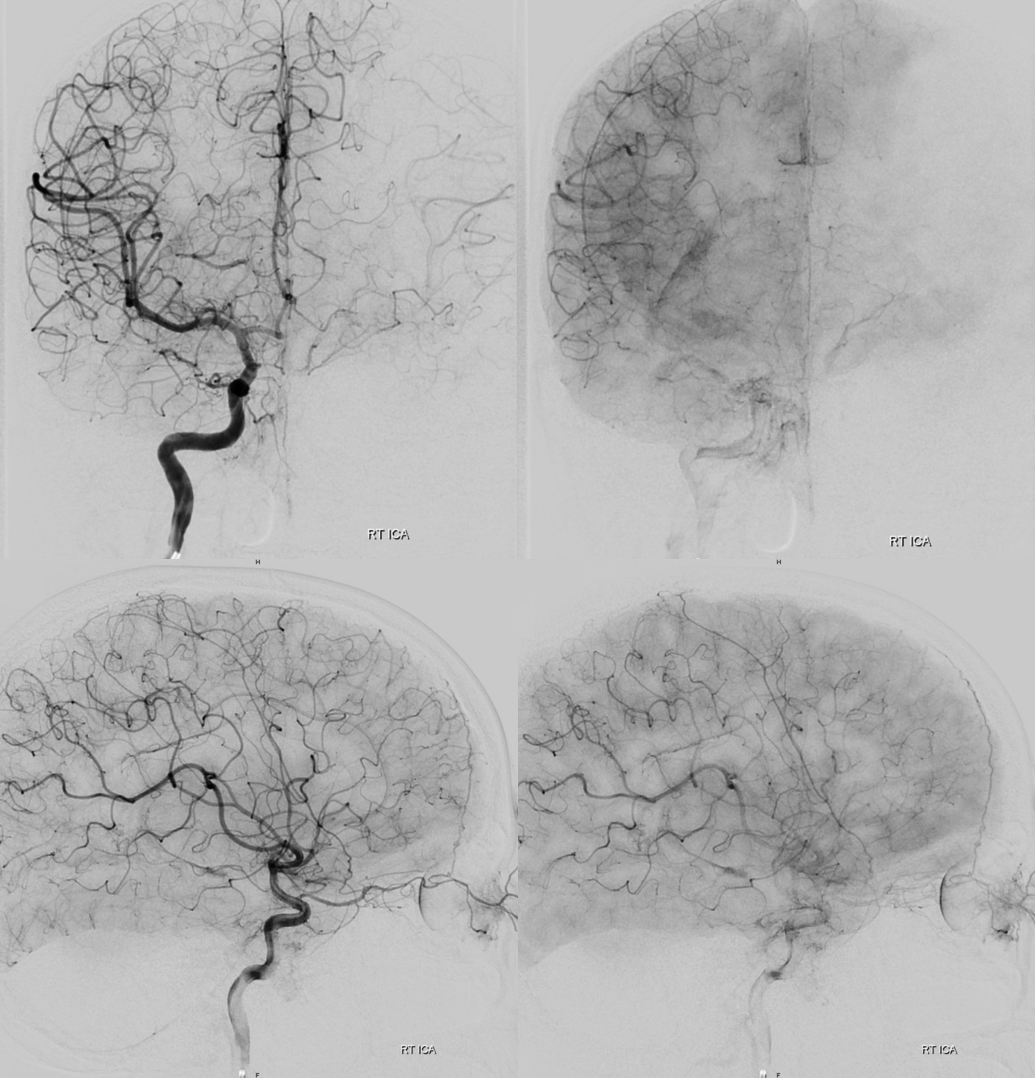
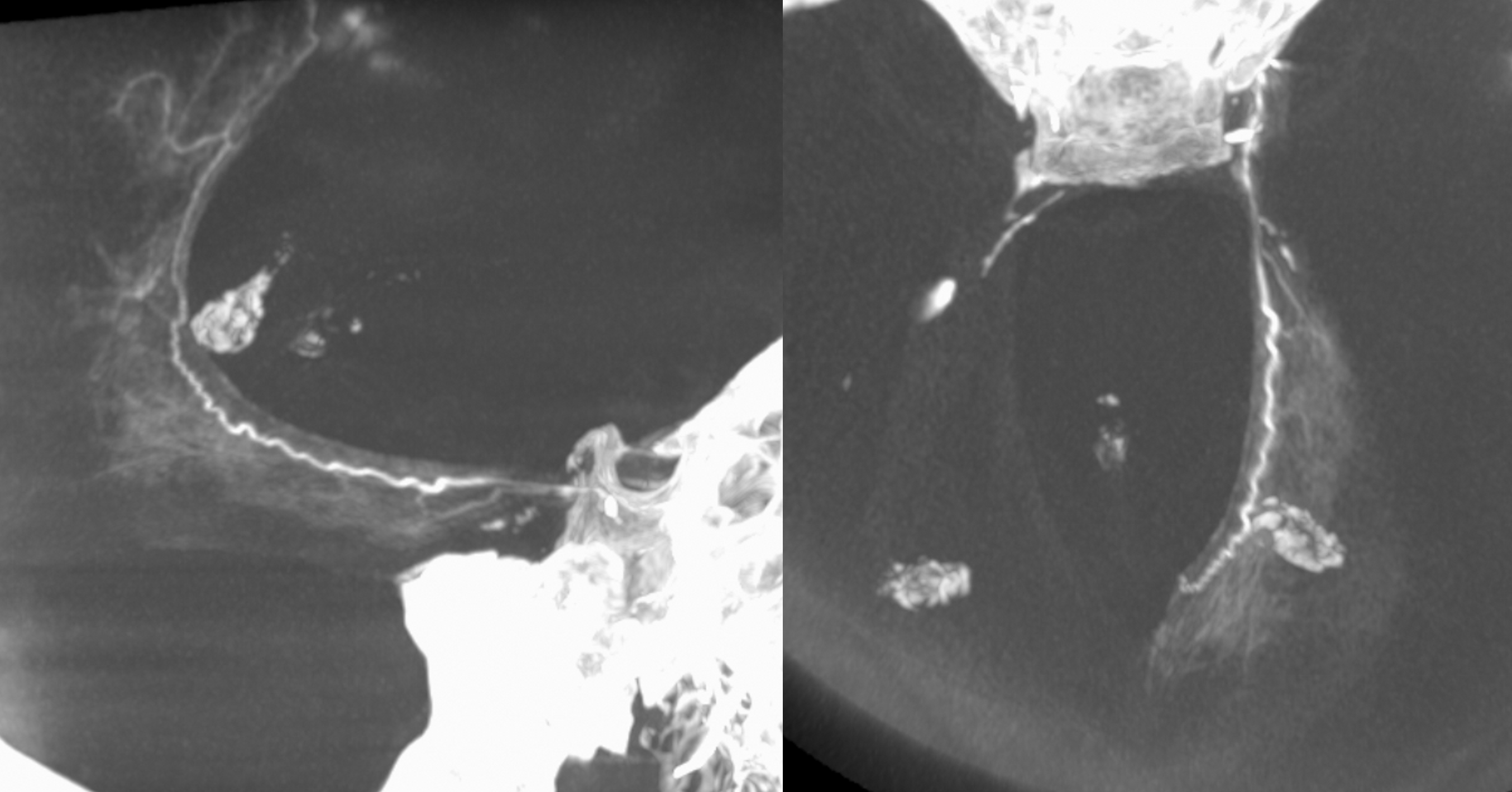
Extremely important technique point. Images on the left show proximal accessory meningeal injections — nothing to worry about right? Images on the right are “wedged” or “flow control” position — see the ophthalmic artery now? Forewarned is forearmed… Particle embo from proximal Accessory position would be a bad idea — but not half as bad as any embolization from the wedge position.
One has to be very careful — see the ICA images below — looks like no problems huh? The connections are always there — its just a matter of how big and how to visualize them.
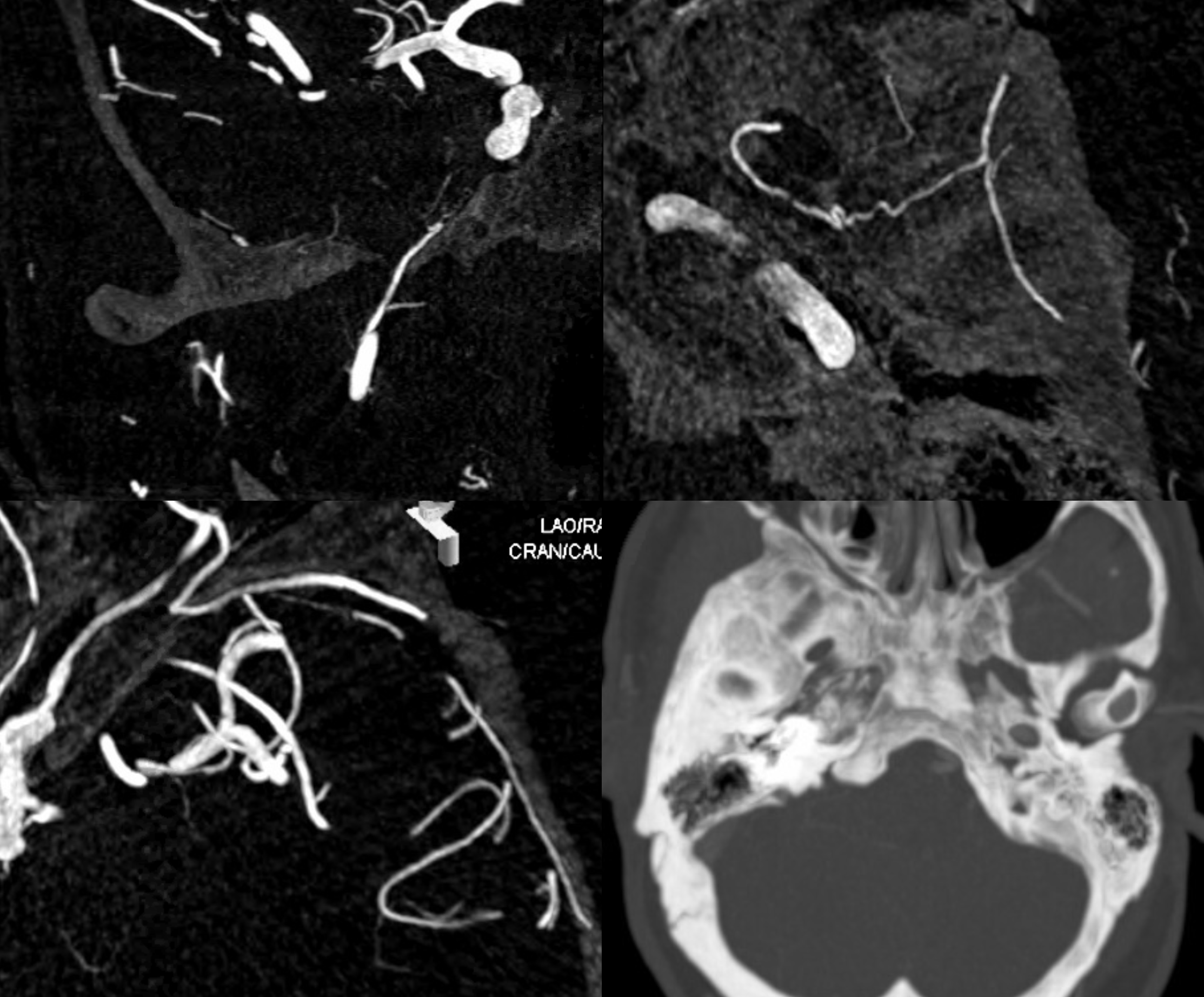
DYNAS — top left is coronal MIP through ovale. Top right is axial MIP through same — the accessory meningeal courses backwards — utilizing the “cavernous” branch of the MMA or the meningeal branch of the ILT — same thing — to reconstitute the MMA. Bottom left is view of ophthalmic artery connection with the MMA via the sphenoid ridge branch. Bottom right is thick MIP showing absence of foramen spinosum.
Accessory Meningeal Supply of Cavernous Sinus and Marginal Tentorial Arcade (Bernasconi-Cassinari) via the clinoid tentorial arcade (deep recurrent meningeal artery)
Variations are endless — here is one where recurrent meningeal from ophthalmic supplies frontal MMA territory (below)
Posterior MMA territory is via classic MMA . However, a very large accessory meningeal (solid arrow) directly supplies the cavernous / ILT region (the ILT is thus hypoplastic) and, via large deep recurrent meningeal artery along the free edge, continues as prominent marginal tentorial arcade (dashed arrow) way above the falcotentorial junction — to the inferior sagittal sinus region
Note how separate origin of MMA (grey arrow) and Accessory Meningeal (white arrows) is associated with the superficial course of the IMAX (grey arrowhead). The marginal tentorial is dashed arrows
Movie — everything is there — stop and scroll thru individual images
Another example of the same — notice also contrast blush of the Meckel cave on DSA images
DYNA MIPs show why the mesial tentorial arcade is so large — because it supplies the tentorium and falx dura. Super, huh.
Movie
Foramen of Vesalius — ILT Territory Supply
Again, balance. Here, we have a hypoplastic ILT and a smallish MHT supplying the lateral tentorial arcade (oval). The ILT area is supplied by the Accessory meningeal (entring skull via foramen of Vesalius)
Pituitary Supply
This is vanishingly rare. The cavernous branch (ball arrow, to the ILT region) is supplied by the accessory meningeal artery (entering via the foramen of Visalius — arrow). That is unusual enough. However, in this case, a very unusual branch courses below the horizontal segment of the cavernous carotid artery (dashed arrow — maybe related to capsular arteries of McConnell, which are tiny and arise from the medial aspect of the horizontal segment, supplying dura and bone of the hypophysis), and supplies the pituitary (arrowhead).
Same without arrows
MIPS — same arrows
Movie
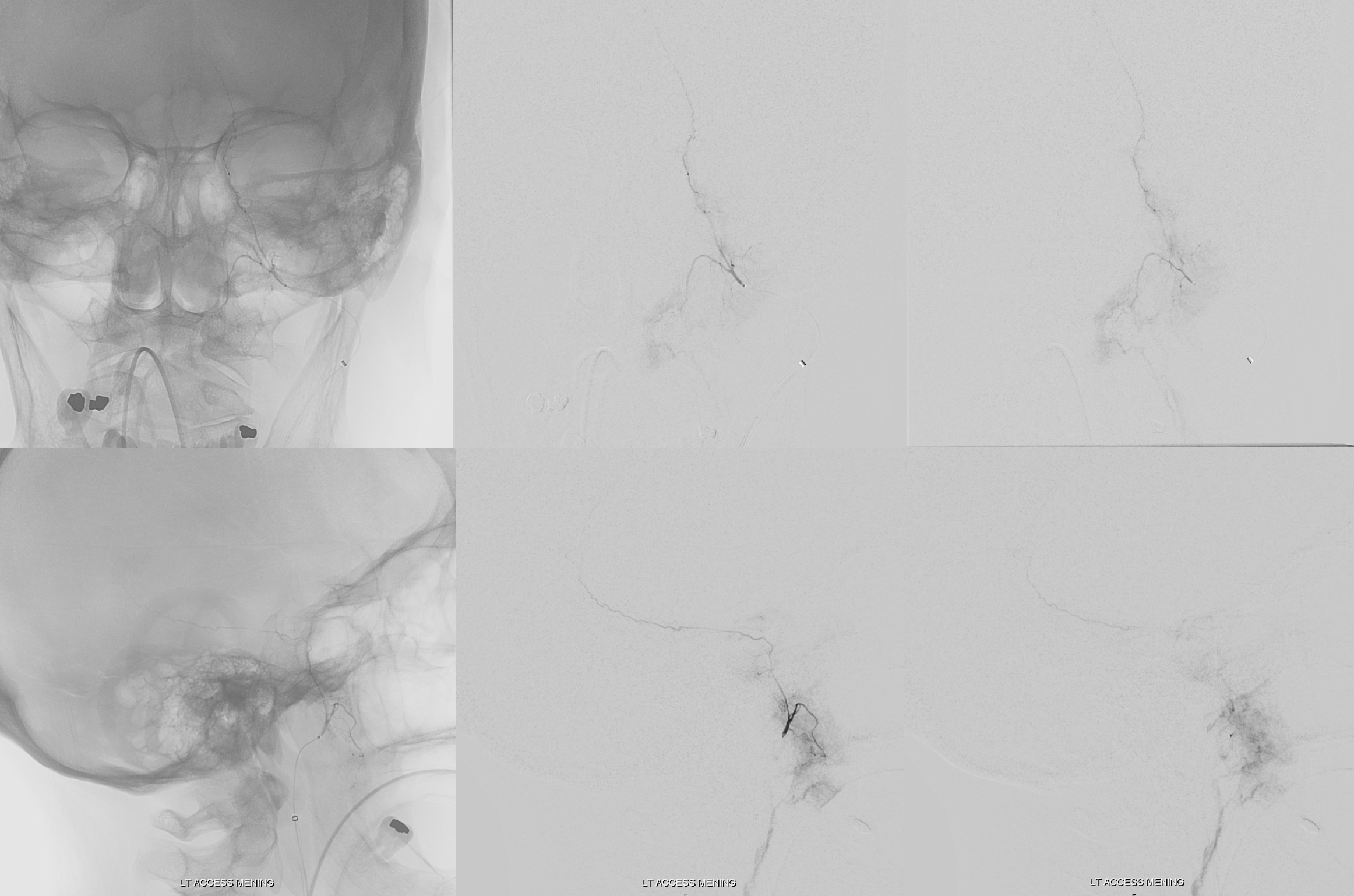
Meningioma Supply
Easy to get confused and think its all MMA . With great DYNAs everyone is smart — look for foramen ovale and you see the accessory MMA . No, its not all MMA . Here is a bad mening — could be a met, but it was a mening
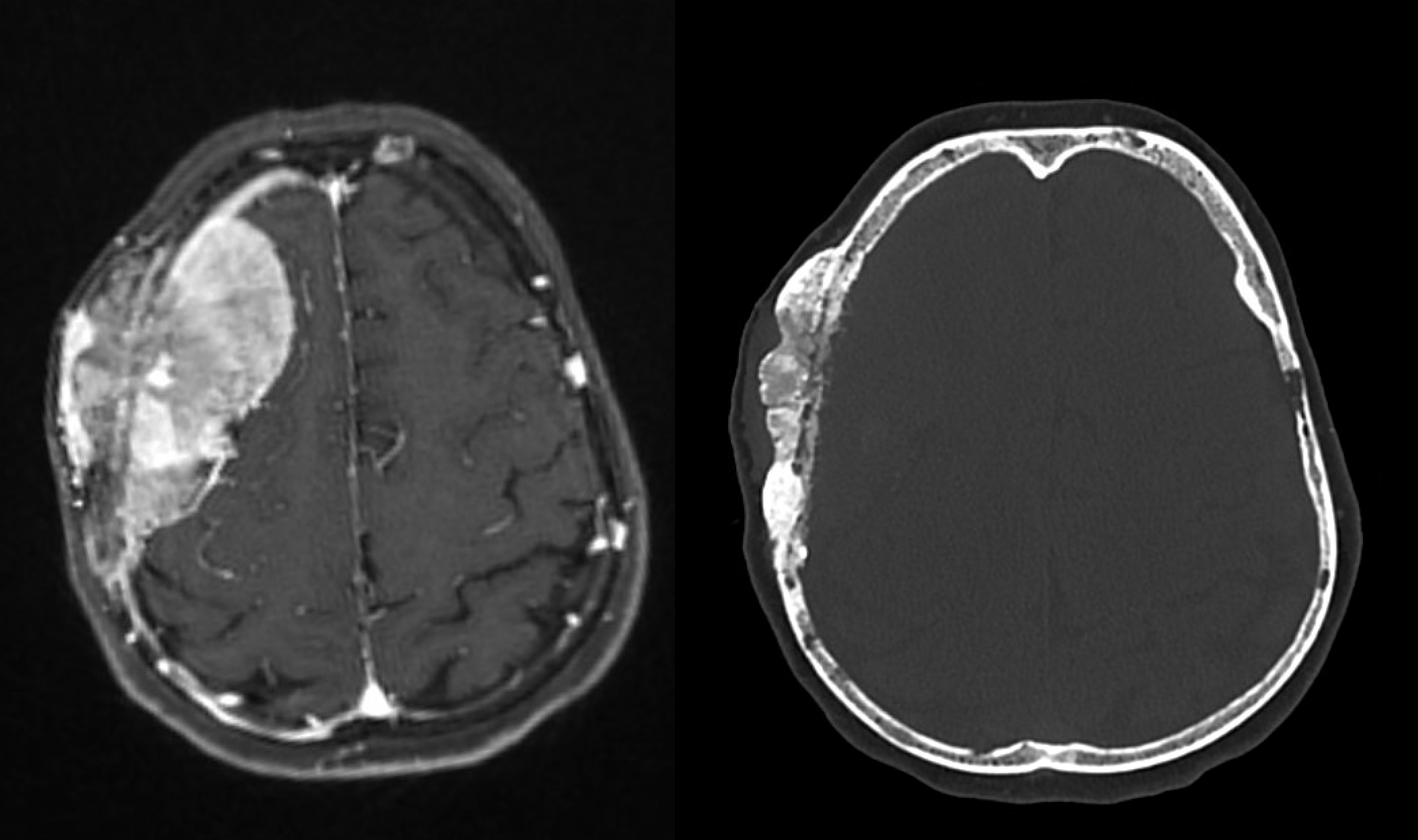
The accessory MMA is dashed arrow — note common origin with MMA , and a prominent anterior deep temporal (arrows) as well — supplying the inferior skull eroding part of mening
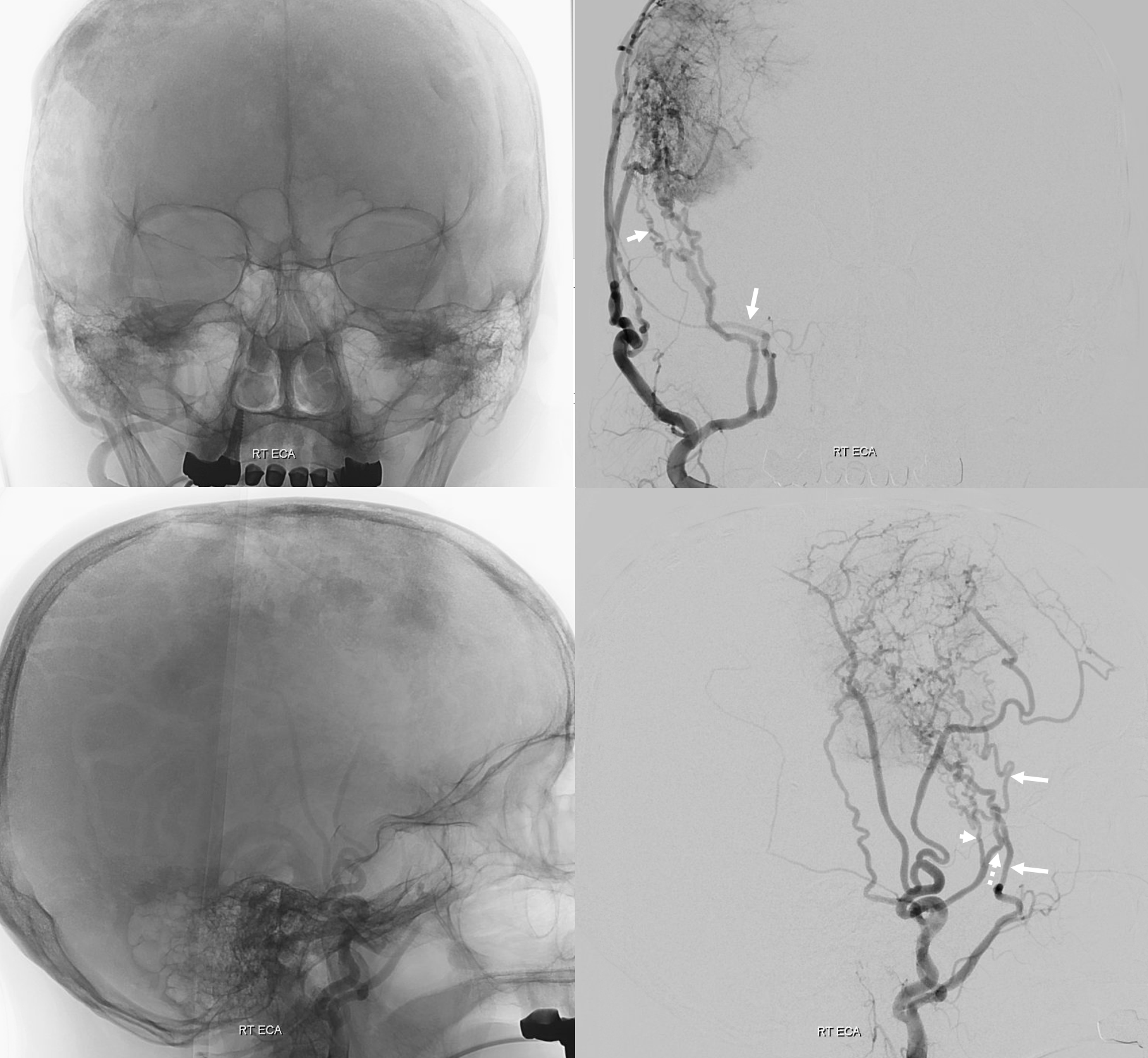
Microcatheter injection of accessory meningeal following MMA embo (coils) — tip is just beyond the Ovale. We embo with particles from here.
This case illustrates the important concept that whatever is close to skull is what supplies skull. From inside its meningeal vessels. From outside is STA, Occipital, deep temporal, facial, skull base vessels (vert, ascending pharyngeal) — get the point right?
See intrinsic dural arterial vasculature page for more info
Back to Diagrams and Drawings Umbrella Page