
Aortic Arch — A Guide to the Perplexed
Certainly, the World does not need another pictorial essay of aortic arch variants. However, what the world may need is a practical guide of how to go about catheterizing them quickly and safely. So, how about printing the picture below to hang it in your angio suite? I promise it will be more useful than another company poster of their aspiration catheter family. So, below is a picture of what your really need to see — not the usual bovine arches, but something common enough to see and not be perplexed about.
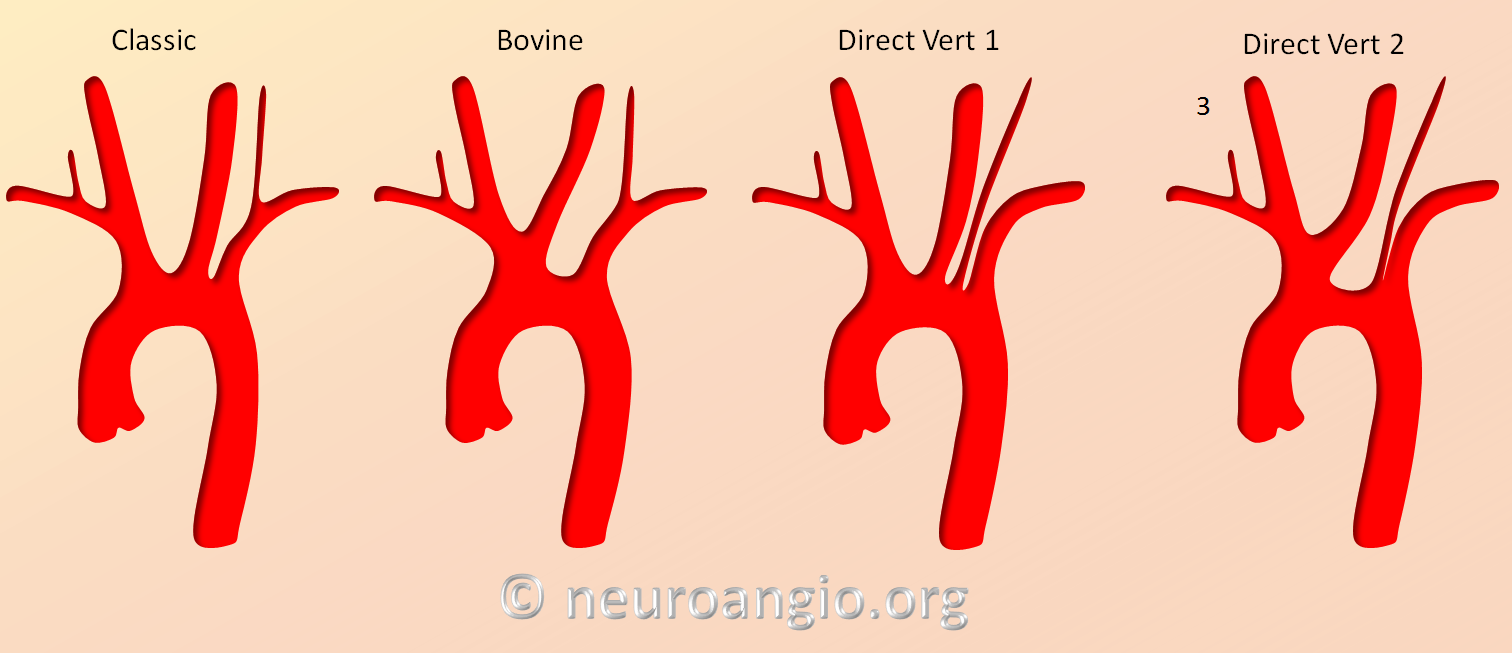
Of course, if you want to see the really common stuff, below is a picture of the usual suspects on top and the unusual ones on the bottom:
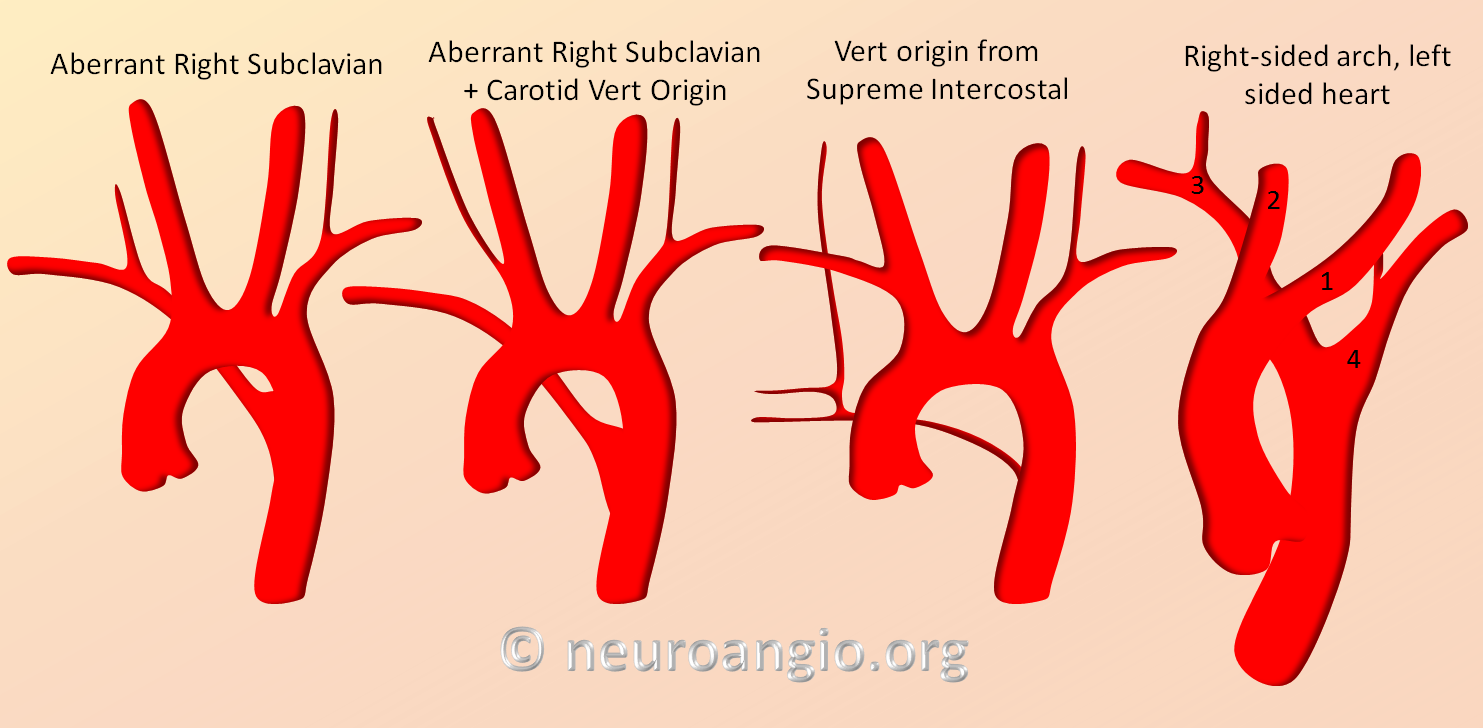
Now, for the specific variants
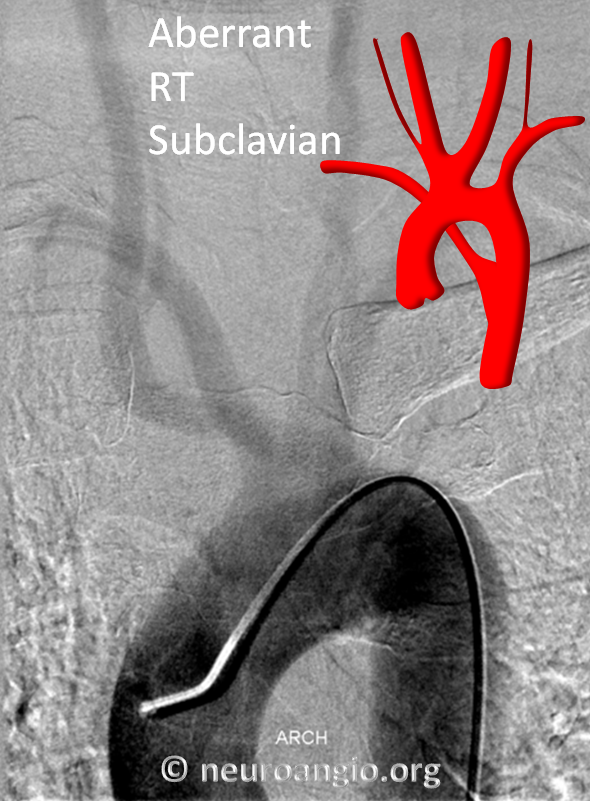
ABERRANT RIGHT SUBCLAVIAN ARTERY
This is the most common variant after the well-known bovine arch and direct origin vert. Here is a picture:
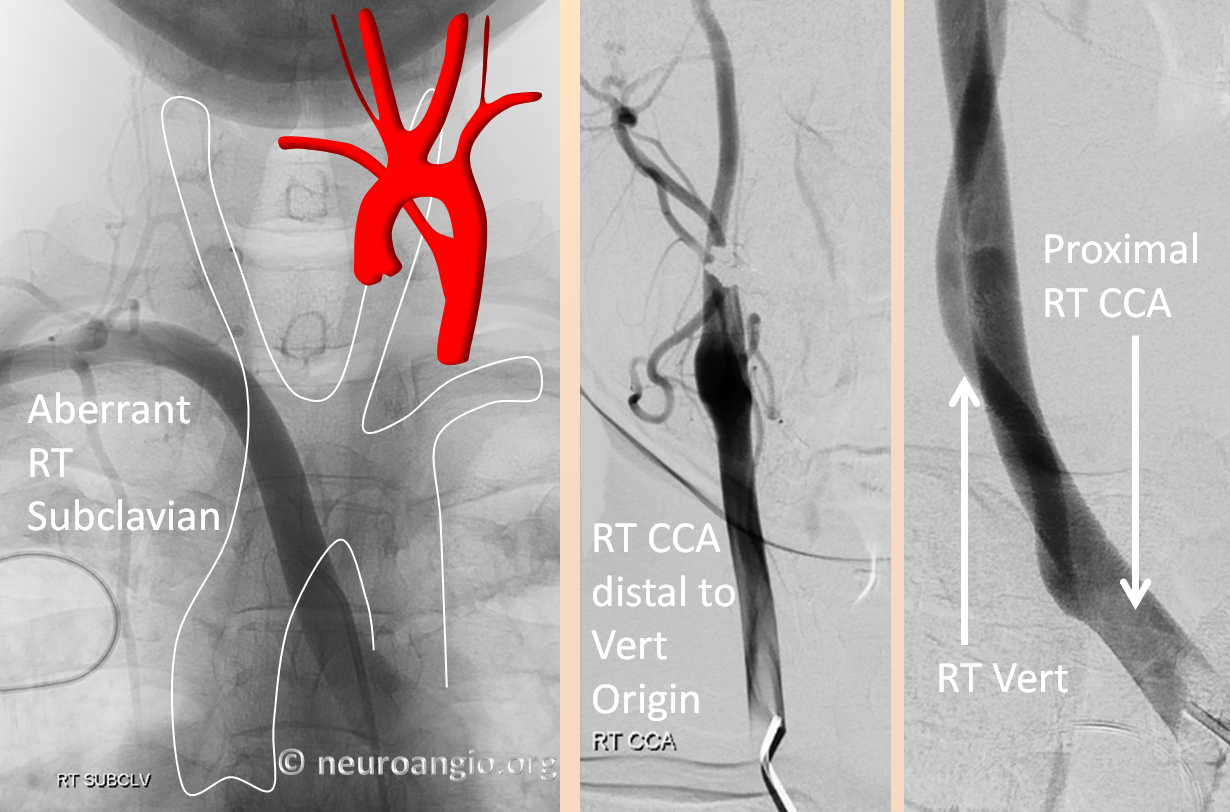
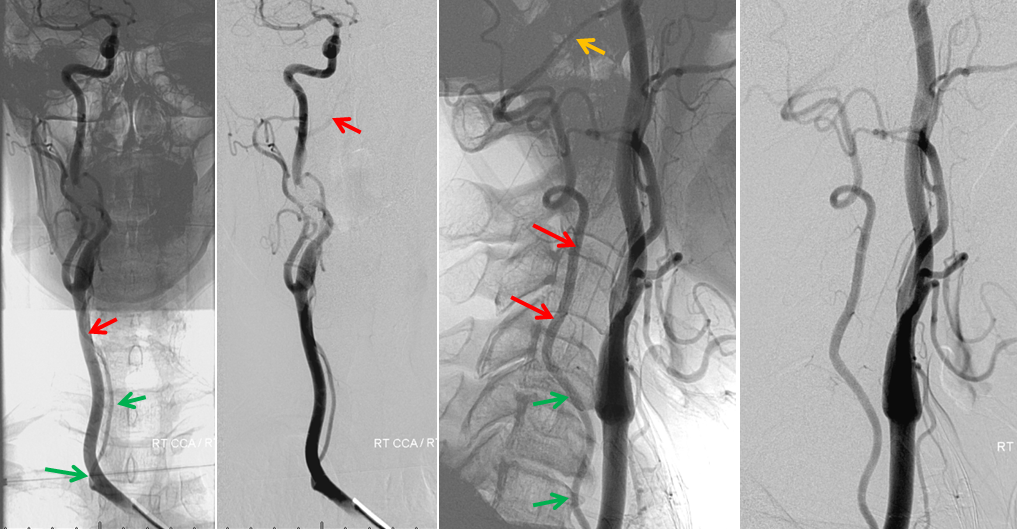
The key thing to remember is that the aberrant subclavian will be coming off FIRST and LOWEST as you come up from below (femoral puncture). Often the wire will find the aberrant subclavian first. It will look like brachiocephalic artery, but without a common carotid (left-sided picture, above). To get to the carotids, you have to go higher up the arch, past the aberrant subclavian. There you will find the right CCA, left CCA, and left Subclavian. Sometimes, the carotids will come off together, in a bovine trunk (image below). The right vertebral artery may come off the right subclavian, or more commonly from the proximal right common carotid, as you can see above and below. Don’t forget that. The picture below shows injections of all great vessels, from proximal to distal.
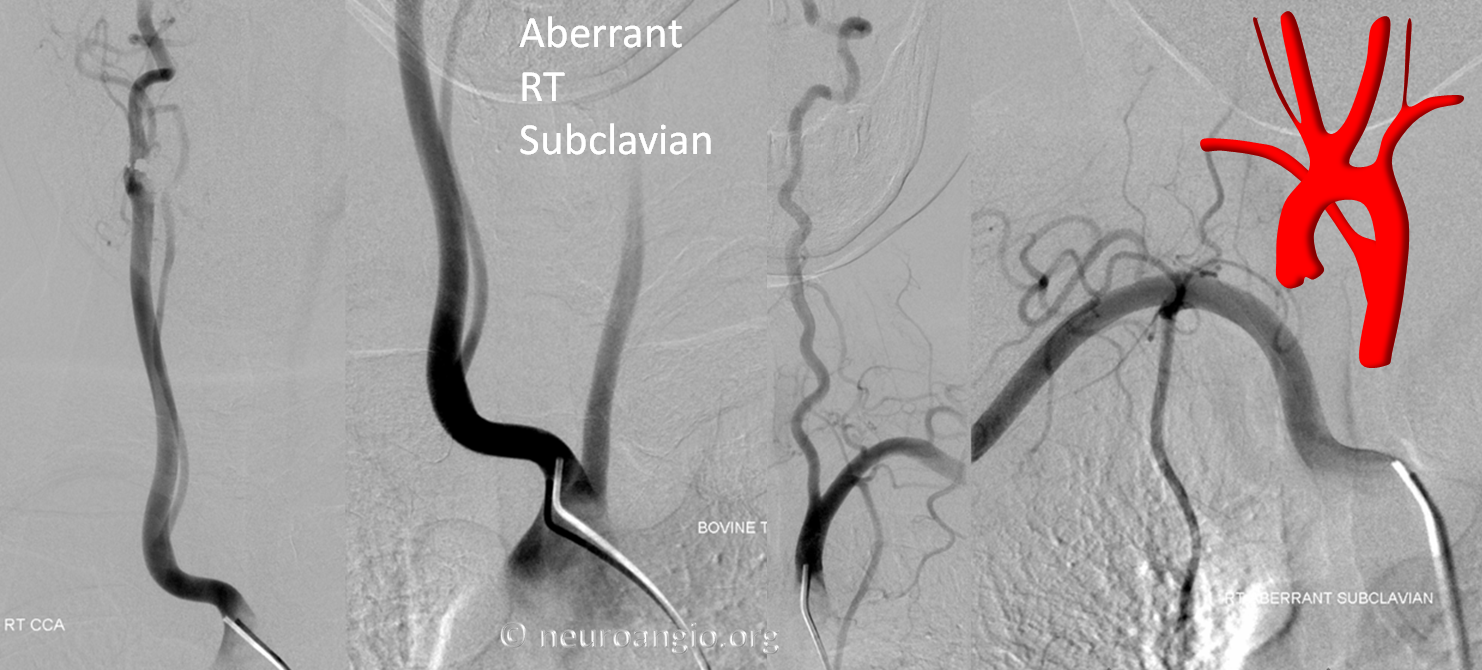
Again, the right vertebral artery will often originate from the common carotid trunk in this variant. In fact, this suggests that embryonically the brachiocephalic strunk and the proximal subclavian artery can be regarded as a single unit, so that in the aberrant subclavian variant the very proximal common carotid trunk is in fact the brachiocephalic equivalent. The segment distal to the vertebral artery is the proper subclavian segment. Here is an arch injection of the aberrant subclavian
Another example of right vertebral artery origin from right common carotid trunk
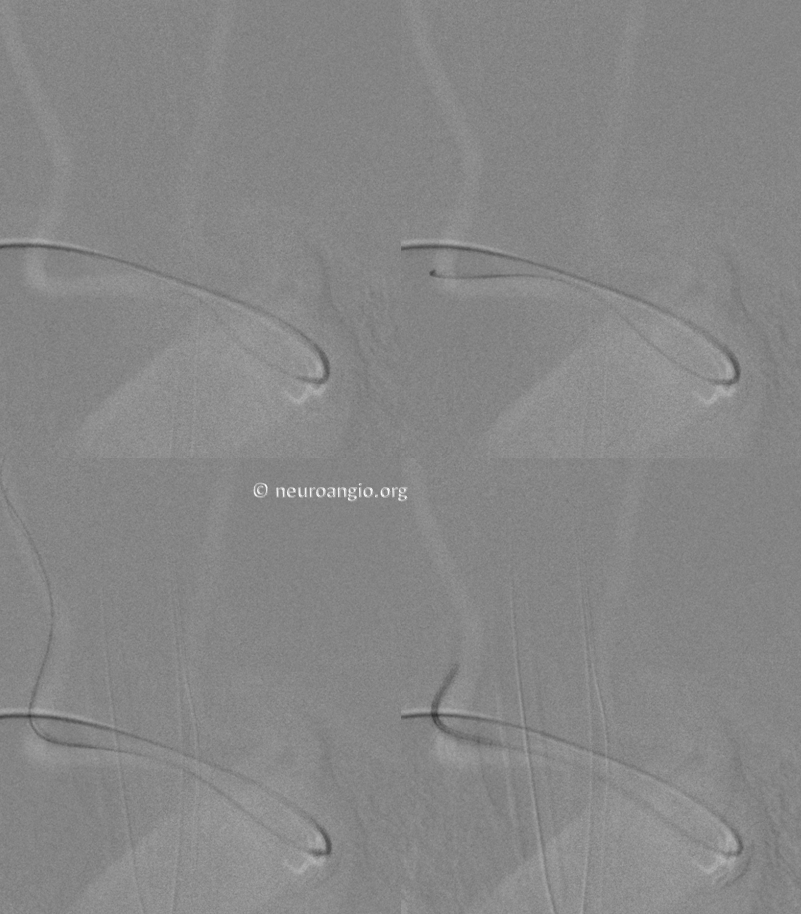
Radial Access to right vert and right CCA in case of Aberrant Right Subclavian (see full case here)
Here is a right radial access to right vertebral artery, in this case coming off the subclavian rather than CCA

However, had it come off the CCA Dr. Raz would have been able to access it anyway

Pretty neat, huh
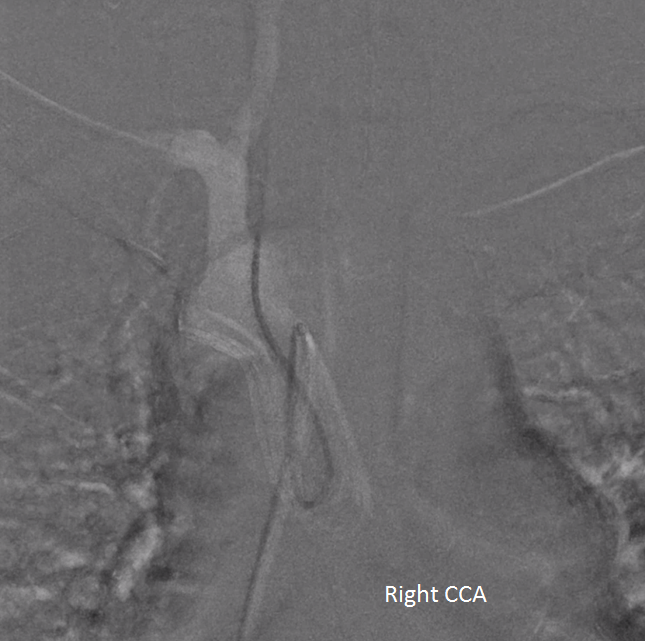
Right CCA injection shows a Carotid Artery Web (white arrow) with contrast stagnation in late arterial phase (black arrow)

Nice resource, including a really user-friendly embryology section, courtesy Dr. Vincent Tatco
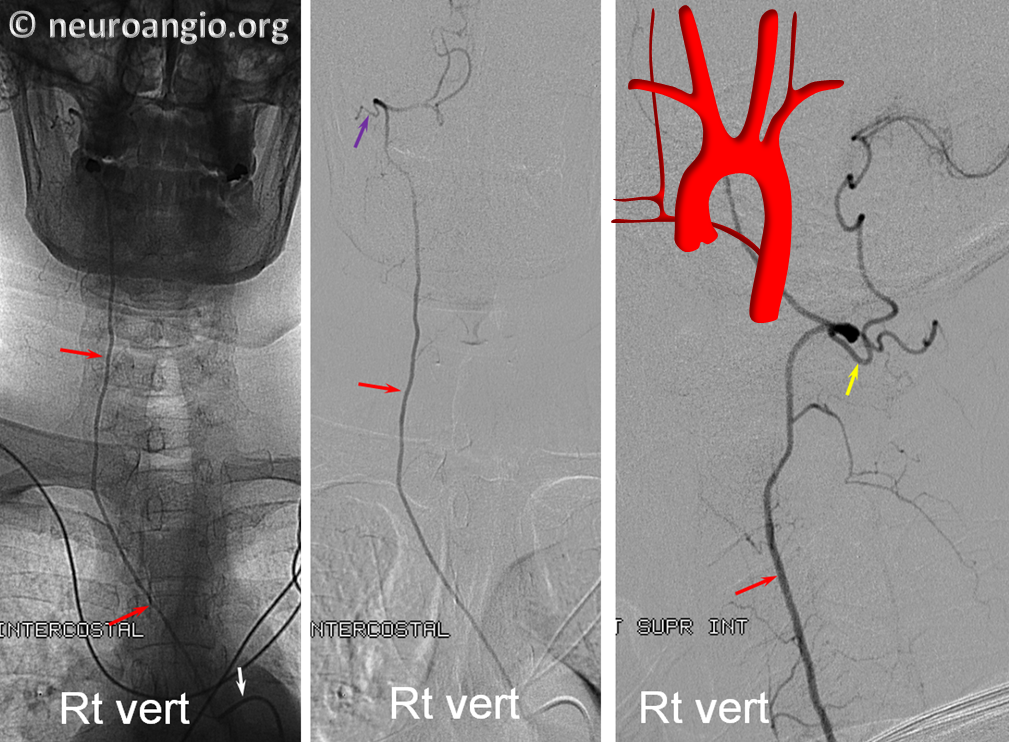
SUPREME INTERCOSTAL ORIGIN OF RIGHT VERT
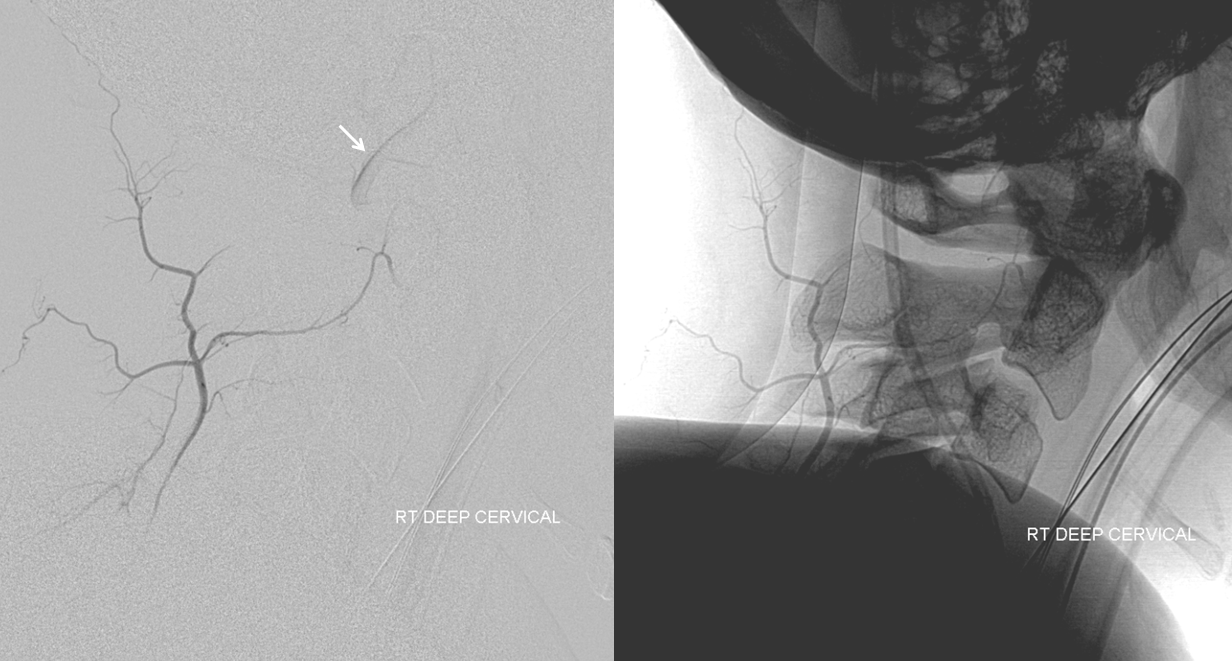
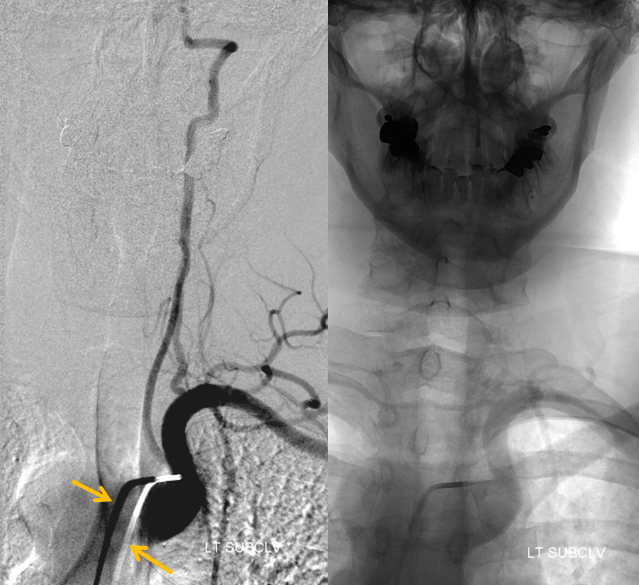
This is not the usual vessel to look for. Yet, it is imporatant to know where you might find it. Here is a rare but important variant of right vert origin from the position of right supreme intercostal. You might need to use your favorite spinal angio catheter (like RDC) to find it.
Another Example of the same. The vert is not found in its usual location

An injection of the right deep cervical artery shows transient opacification of the vert (arrow) via the C2 muscular anastomosis; we know the vert is there
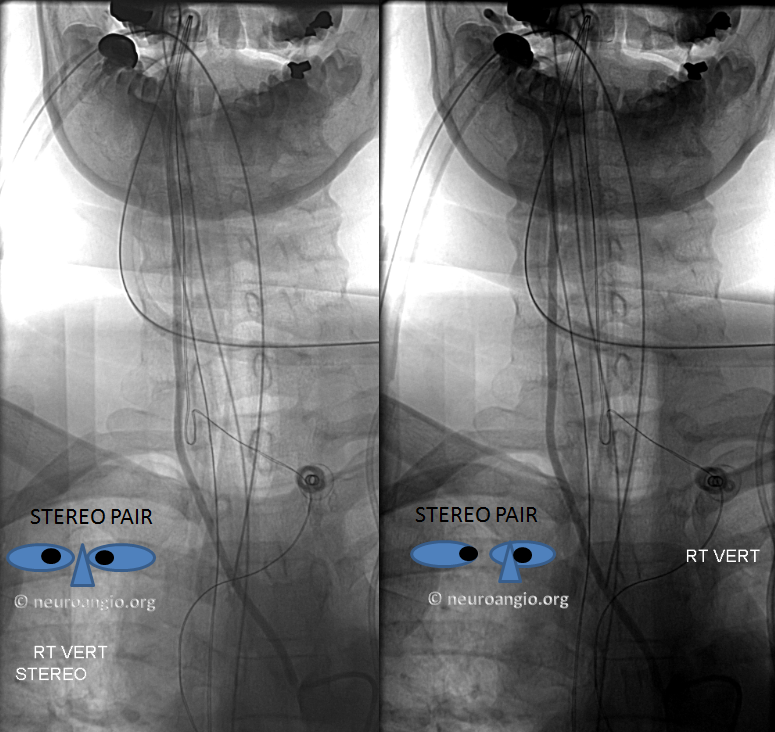
Where is it? The answer is aortic arch. When the right vert is apparently missing in action, the origin is usually in the upper thoracic descending aorta — at the supreme intercostal artery

Stereo views are below
RIGHT SIDED ARCH, LEFT SIDED HEART
This is the really nasty one. Important to know. It can be very difficult to catheterize the carotids here. A recurved catheter with a short curve like Simmons 1 or Vitek could be useful here if your favorite first choice is no good. If you are not sure what’s going on, take a pigtail, put it down at the aotic valve, and shoot a 20 cc/sec for 40 ccs injector run. Don’t tilt the frontal plane — keep it straight. This should clarify things a bit. Take your time. A few minutes of thinking can save a lot in frustration. The numbers correspond to order in which the vessels come off the arch. The LEFT carotid usually comes off first.
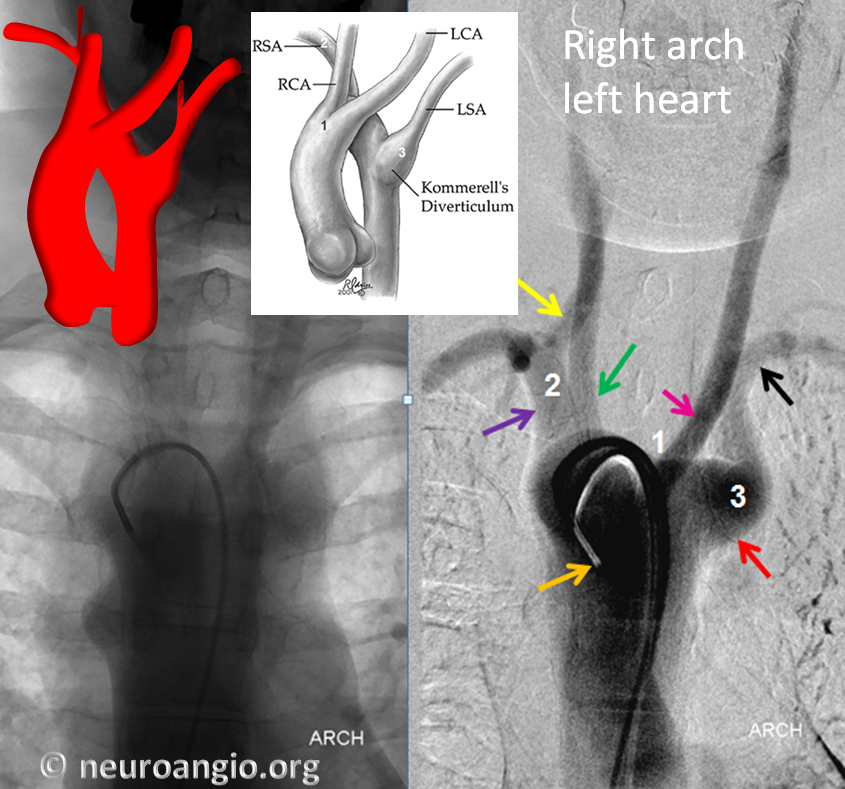
Drawing: Backer CL, et al: Resection of Kommerell’s diverticulum and left subclavian artery: transfer for recurrent symptoms after vascular ring division. Eur J Cardiothorac Surg22:64, 2002 http://www.ncbi.nlm.nih.gov/pubmed/12103375
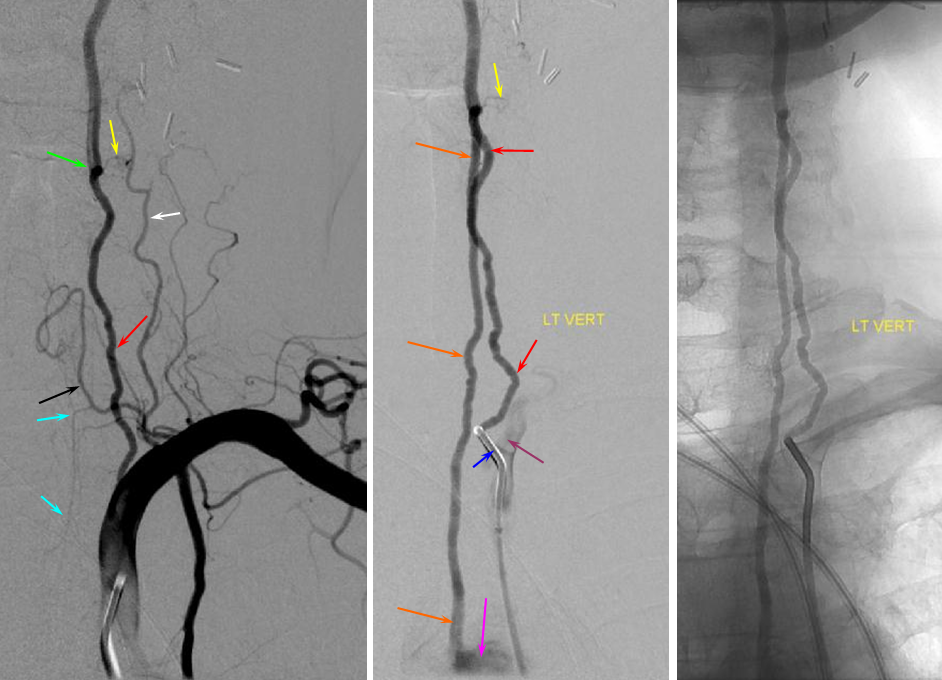
Thus, the diagnostic catheter will encounter these vessels in reverse order: 3,2,1 (unless you are coming from radial artery, in which case you deserve it for not looking at the chest x-ray first). Once you know this, you understand that in order to get into the carotids one must pass both subclavians and come over the arch. The position of the catheter to engage the carotids will look something like this:
The standard 5F VERT (135 degree) catheter (orange arrow) is curved over the arch and is positioned in its proximal portion. Yellow arrow is right vert, purple is right subclavian, green is right CCA, pink is left CCA, red is diverticulum of Kommerell (left aortic arch remnant), and black is left subclavian.
The left subclavian is easy — it is the first vessel to be encountered. Notice how the unsupported catheter (orange) kicks back on injection within the arch.
The right subclavian is generally straighforward also — it will be pointing to the right from the upper arch. The carotids are a problem, because the ostium or ostia may point away from the direction of the catheter — akin to the left CCA in a bovine arch, except worse. It is essential that one have an understanding of the anatomy in this case if one were to use the Simmons! Otherwise, things can evolve from frustrating to dangerous rather quickly. If the vert or Berenstein looks unhelpful, switch to a Vitek or SImmons before wasting too much time. SImmons 2 may be tricky to form and use so if you are not sure start with a Vitek or Simmons 1
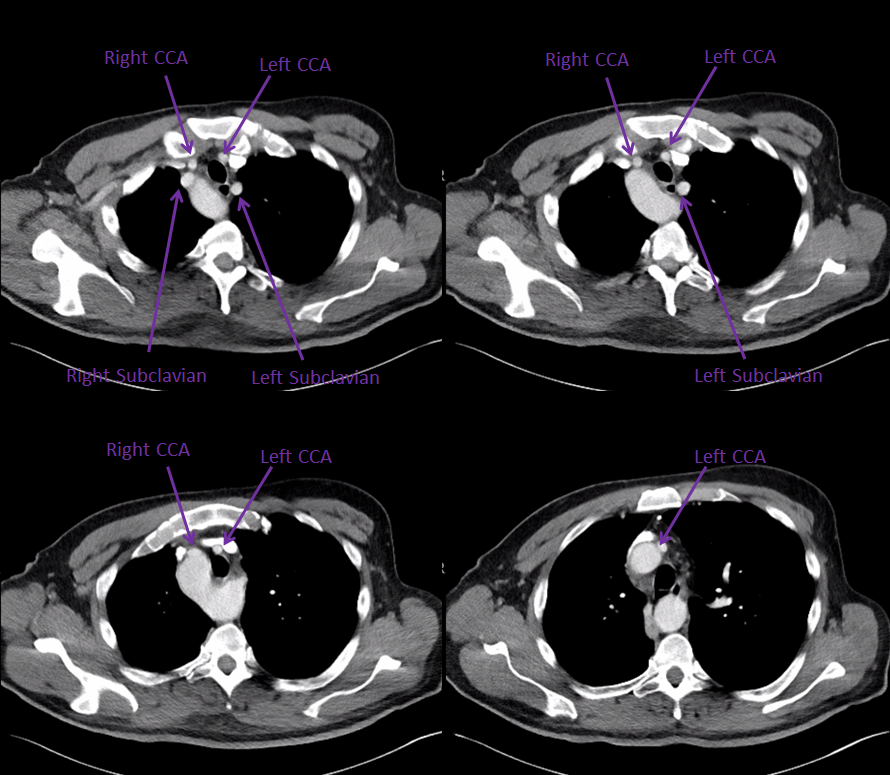
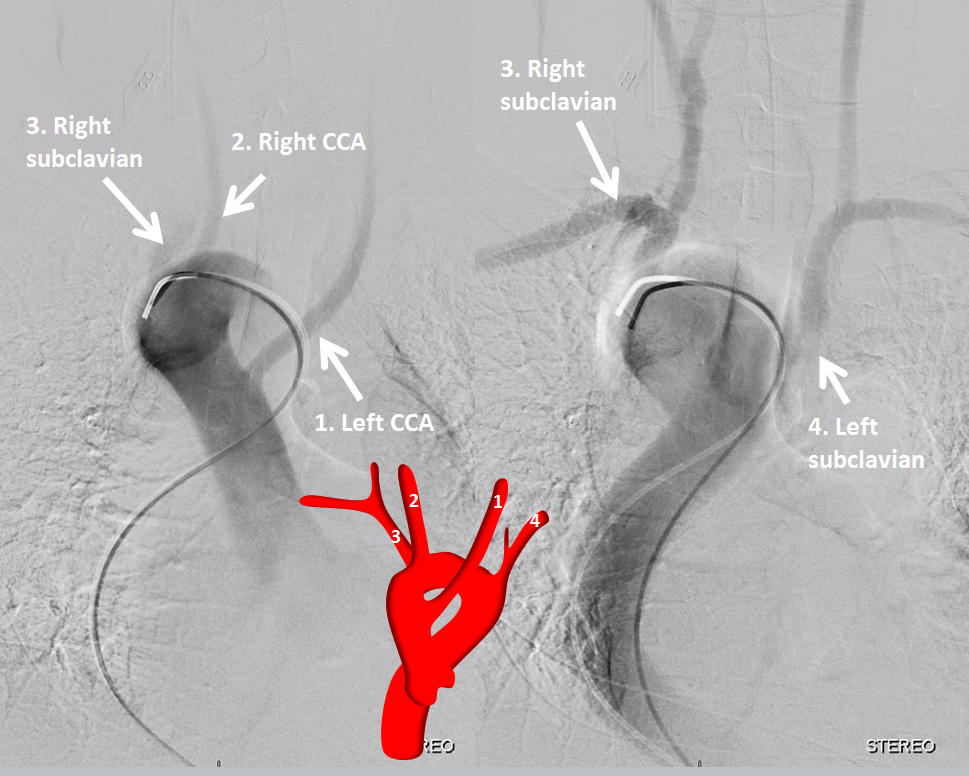
Another example, probably better one, of the right arch left heart variant, also incidental. CT scan, with order of vessel takeoff
1. left CCA (way down ascending aorta, almost at root)
2. right CCA
3. right subclavian
4. left subclavian
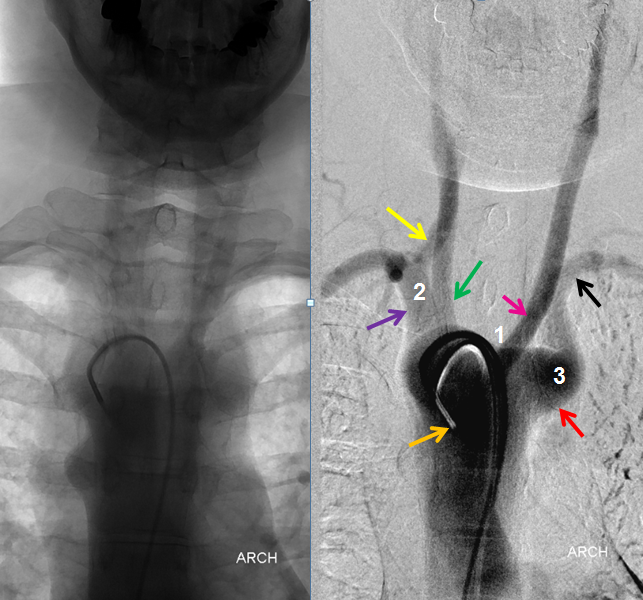
Angio — simple trick is to do a strong injection via your 5F diagnostic catheter in the ascending aorta. It is not as good as a pigtail, but often good enough for a roadmap. Here is the 5F vert in position

Sequential images show order of vessel opacification
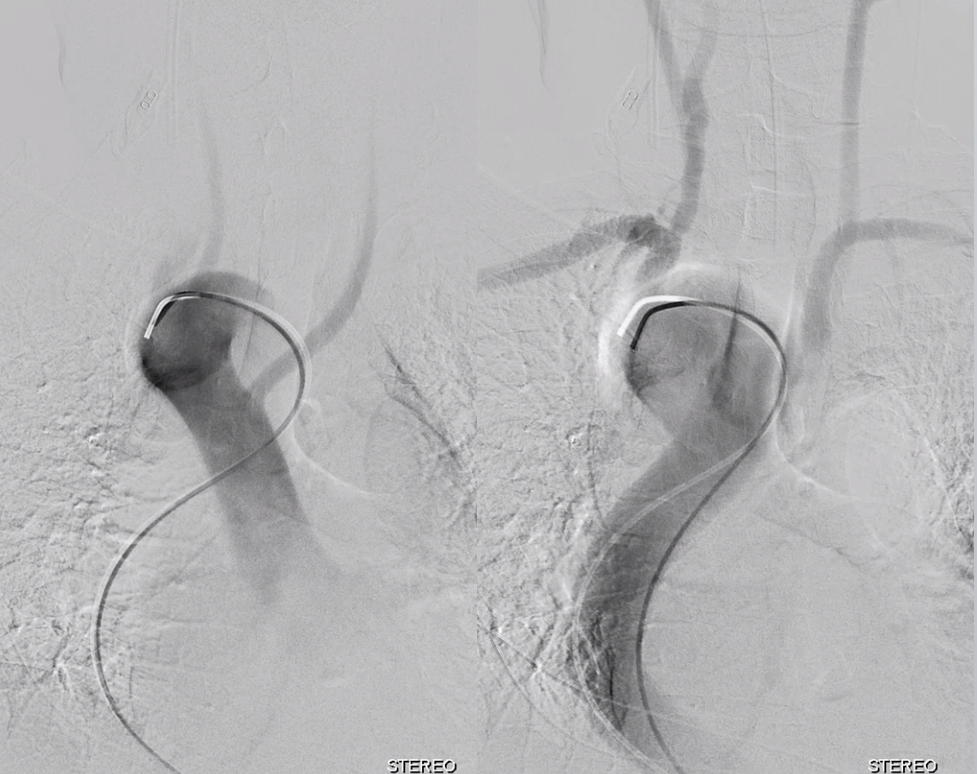
Same image with explanations
First, we catheterize what we can with the vert. Right subclavian is easiest

Next is left subclavian/left vert

Then we exchange for a Simmons 2 (Penumbra Sim to be exact). Whatever Simmons u like.

Right CCA
Left CCA — the proximal-most vessel

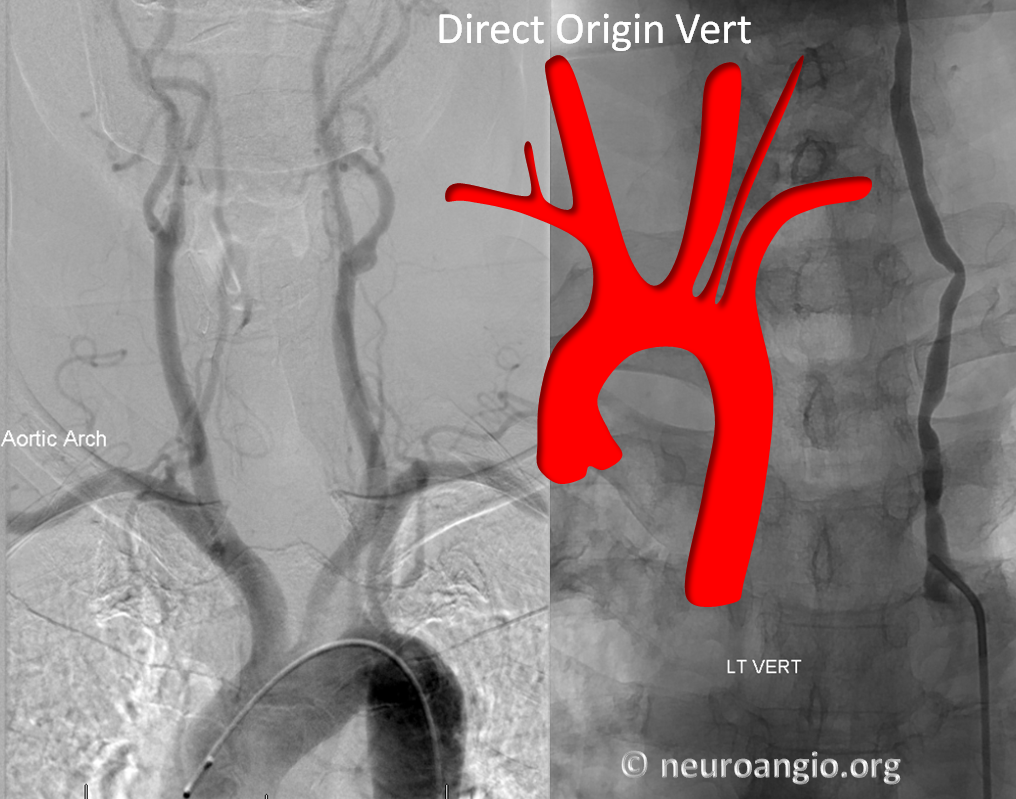
DIRECT ORIGIN LEFT VERTEBRAL ARTERY
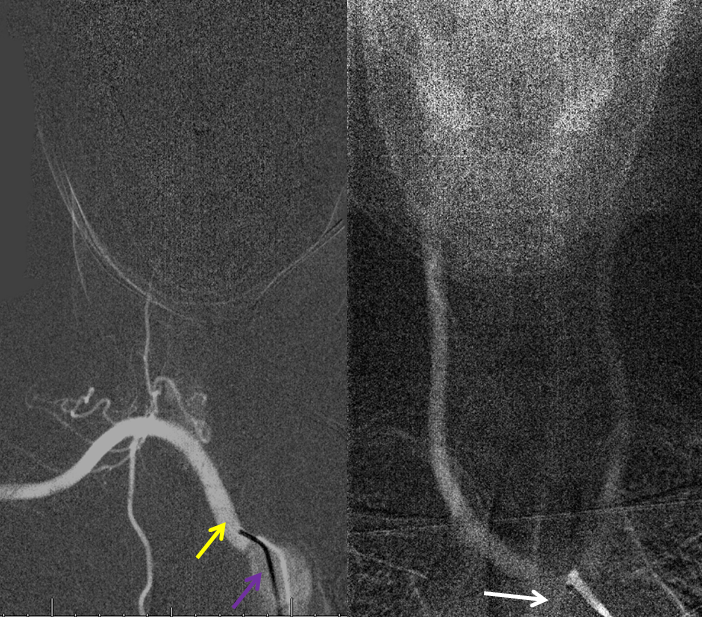
These are a dime a dosen. Everyone knows this. This stereo CTA pair demonstrates direct vert disposition in a patient with cervial vertebral fistula.
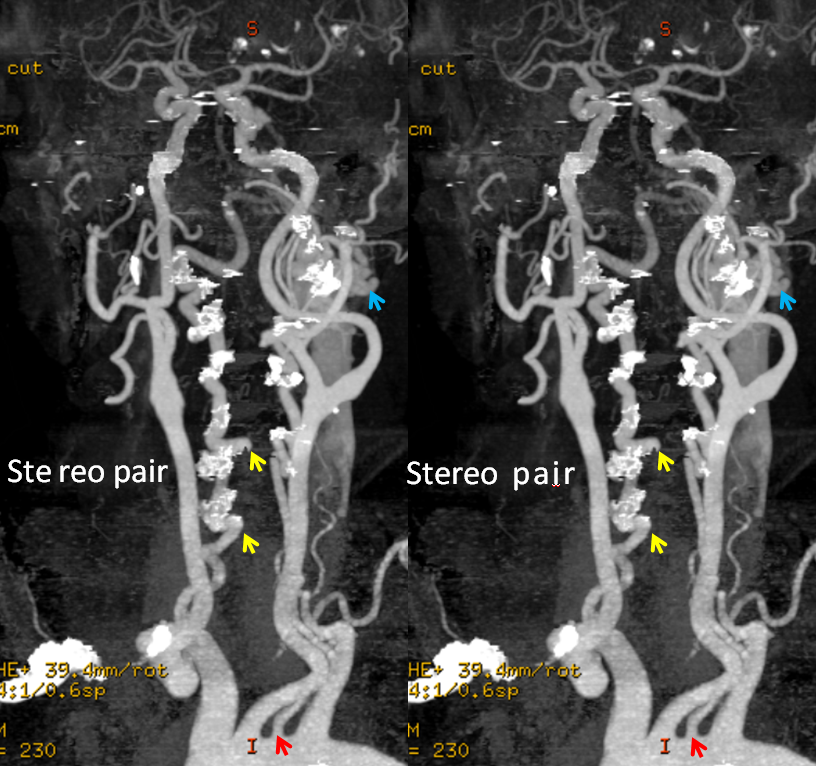
Here is a cool variant of both direct vert and subclavian origins of the vert. The subclavian one is really the ascending cervical, embryologically. Orange arrows point to the direct origin vert coming off the arch (pink arrow). See vertebral artery page for more details
An arch injection of direct origin vert
So, do you have any good angio pictures of variant aches? Send me and get on this page.
Radial Access? Well, its not too handy when it comes to aberrant right subclavian or right-sided arch, certainly not from the right side. How you deal with it is up to you. We prefer to have some kind of idea about arch anatomy before going radial — at least a normal-looking cardiac and arch silhouette on an x-ray.