
Number 37 above. Another EC-IC anastomosis. Usually connects the distal IMAX with the ILT system. Occasionally does a lot for revascularization of ICA in cervical occlusive disease. More commonly, participates in supply of shunts, such as cavernous dural fistulas. Embolization carries risk of injury to V2. We had one case (Onyx closure of cavernous dural fistula) that recovered after some months. Can’t find it.
Usually, the branch is small. Supply is a spectrum like everything else — can come predominantly from IMAX, ILT , MMA, or all/either.
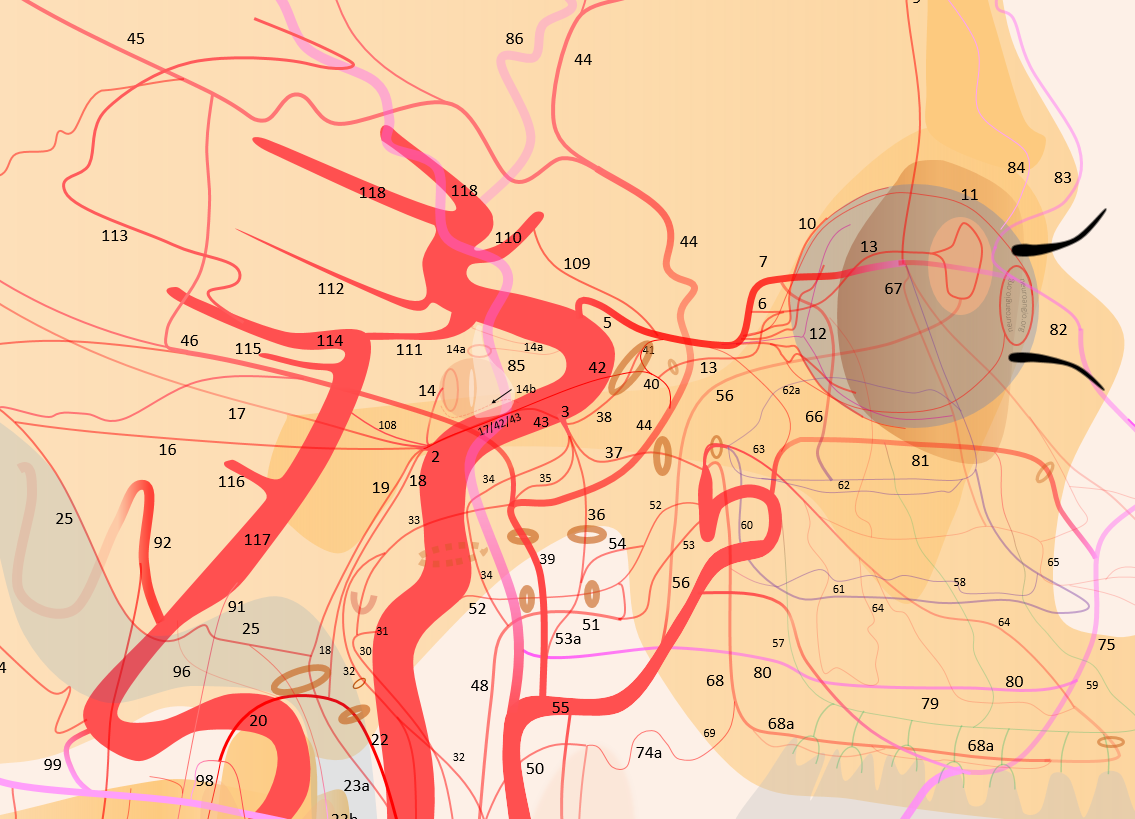
Mostly importance is in diseased states — reconstituting diseased ICA, supply of meningiomas, fistulas, etc. The two main issues with using it for treatment are, of course, that it is a potential EC-IC anastomosis, and that there is V2 going through rotundum. Damage to V2 with liquid embolics especially is likely if embo through rotundum is performed.
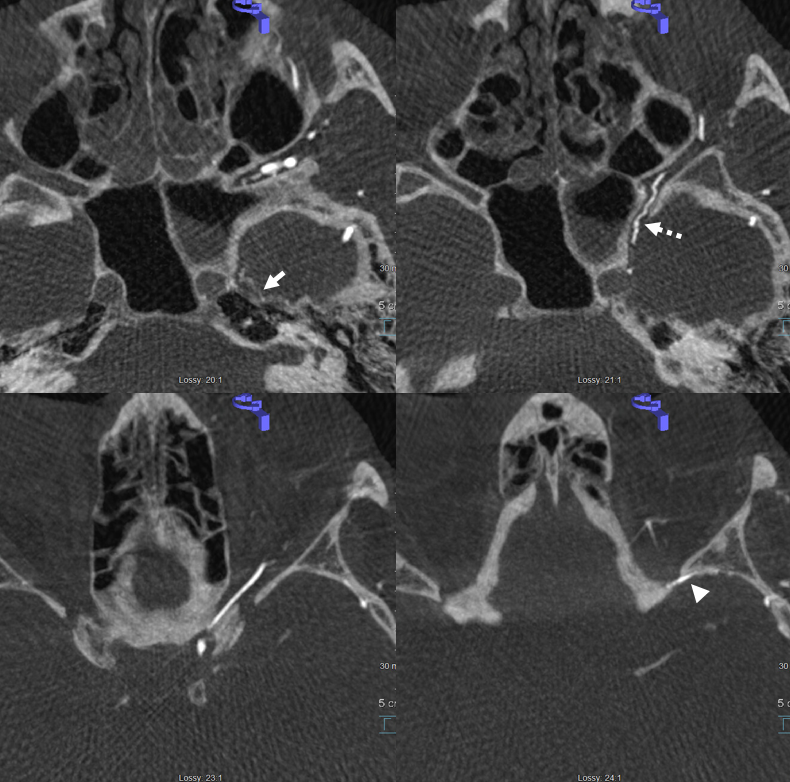
Below is a normal example. Supply from ILT. To see the artery in normal state, Cone Beam CT is usually needed as it is quite small. Coronal is marked by white arrow
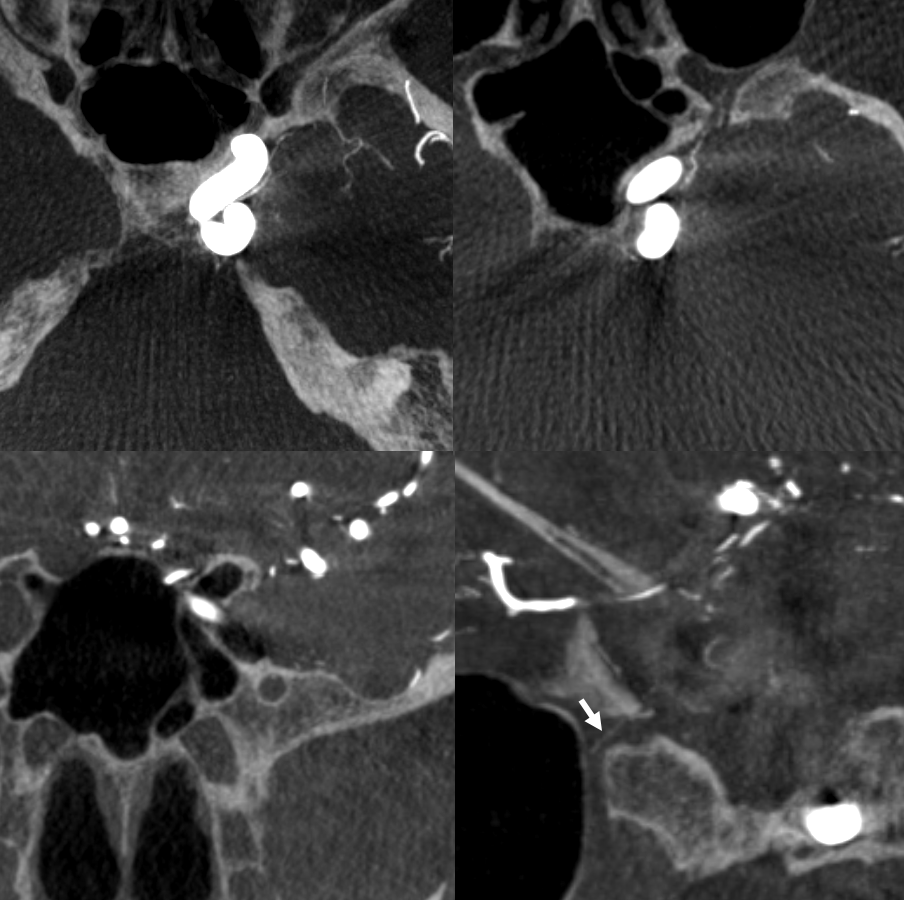
Below, the enlarged Foramen Rotundum artery (dashed arrows) reconstitutes a proximally dissected ICA, along with cavernous branch of MMAand sphenoid branch (arrowhead, connecting to ophthalmic artery) of MMA
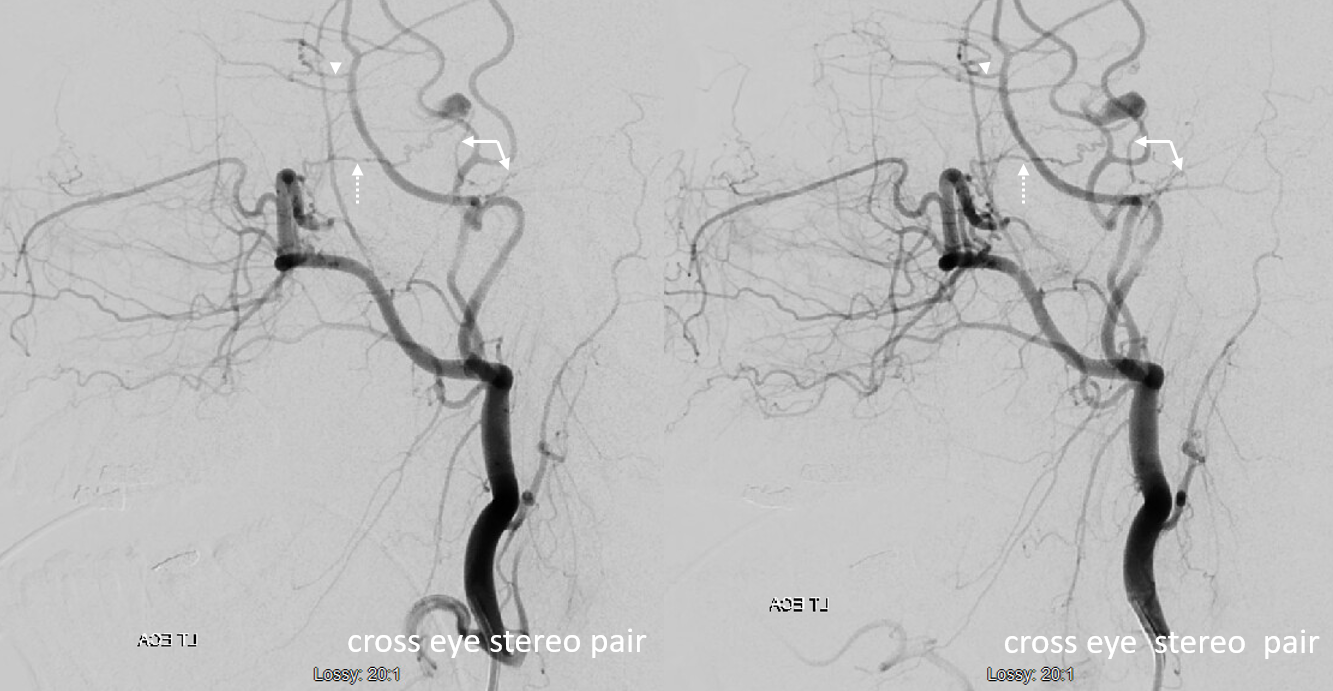
Another view
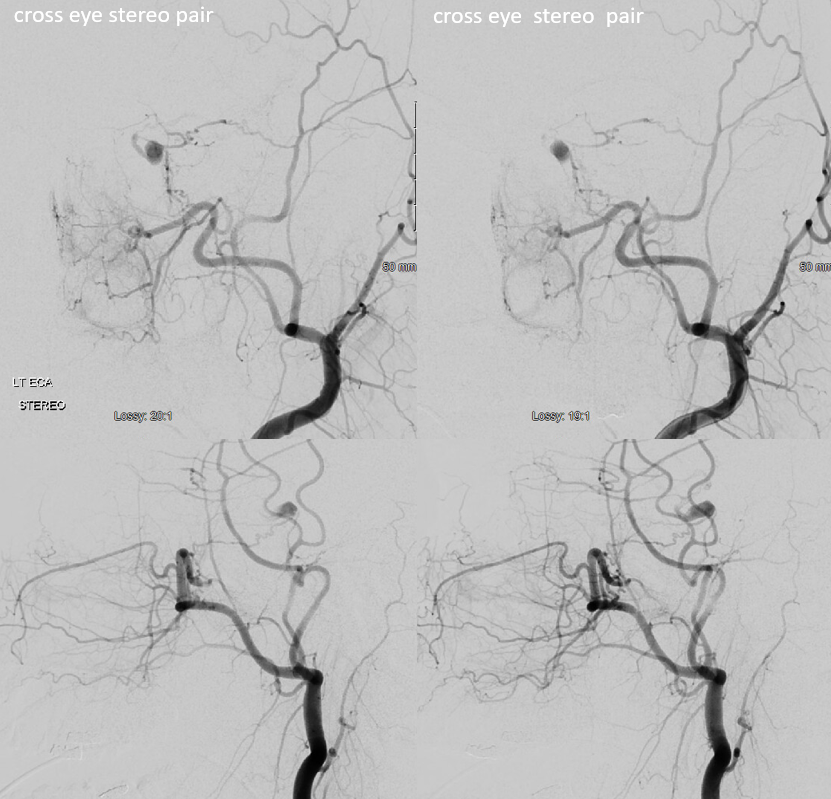
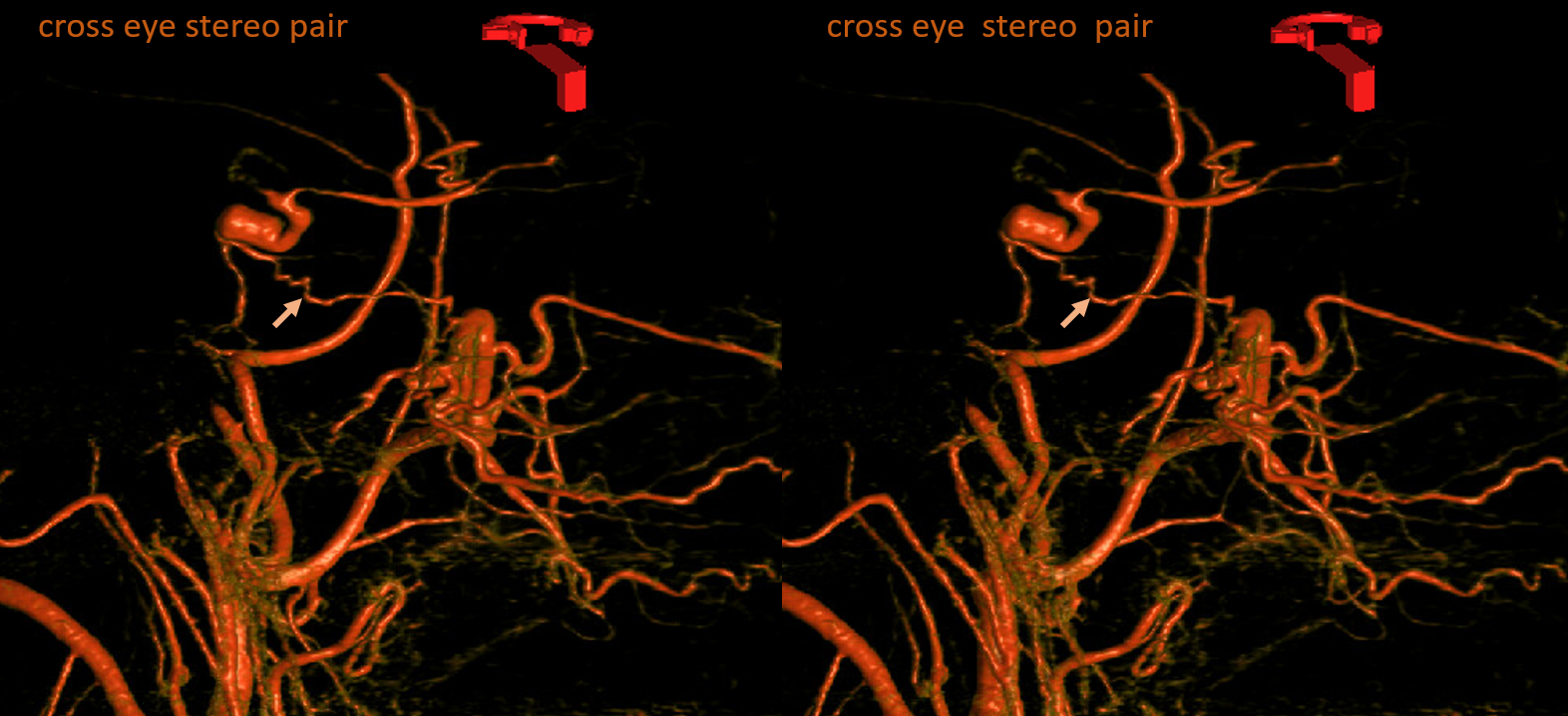
VR images
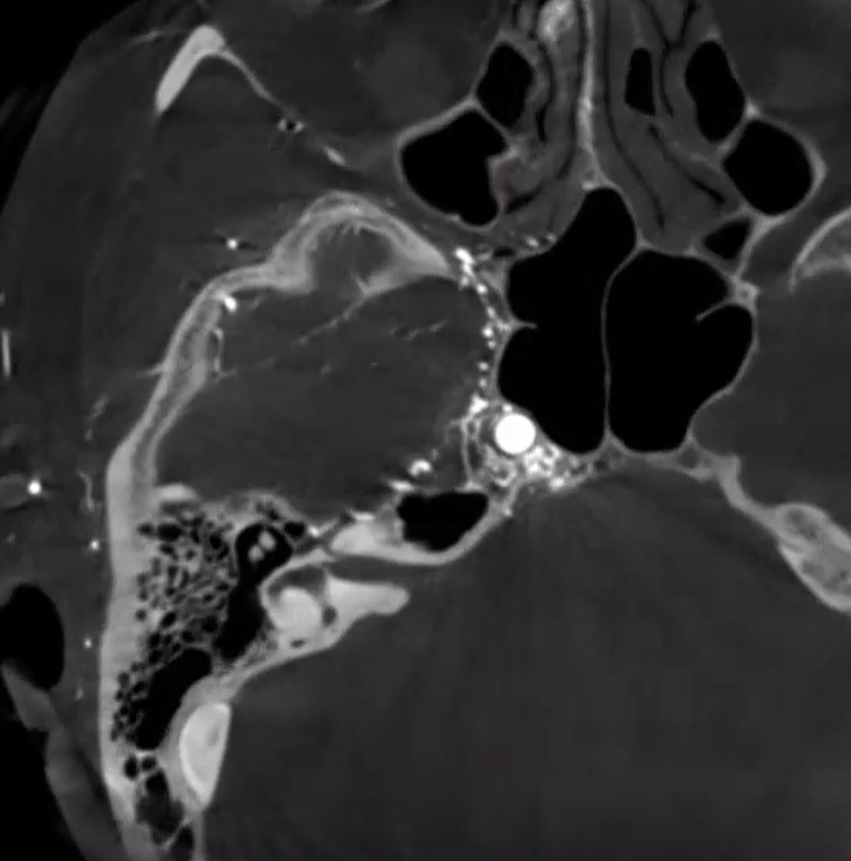
Axial source recons — same arrows
Another Reconstitution Example
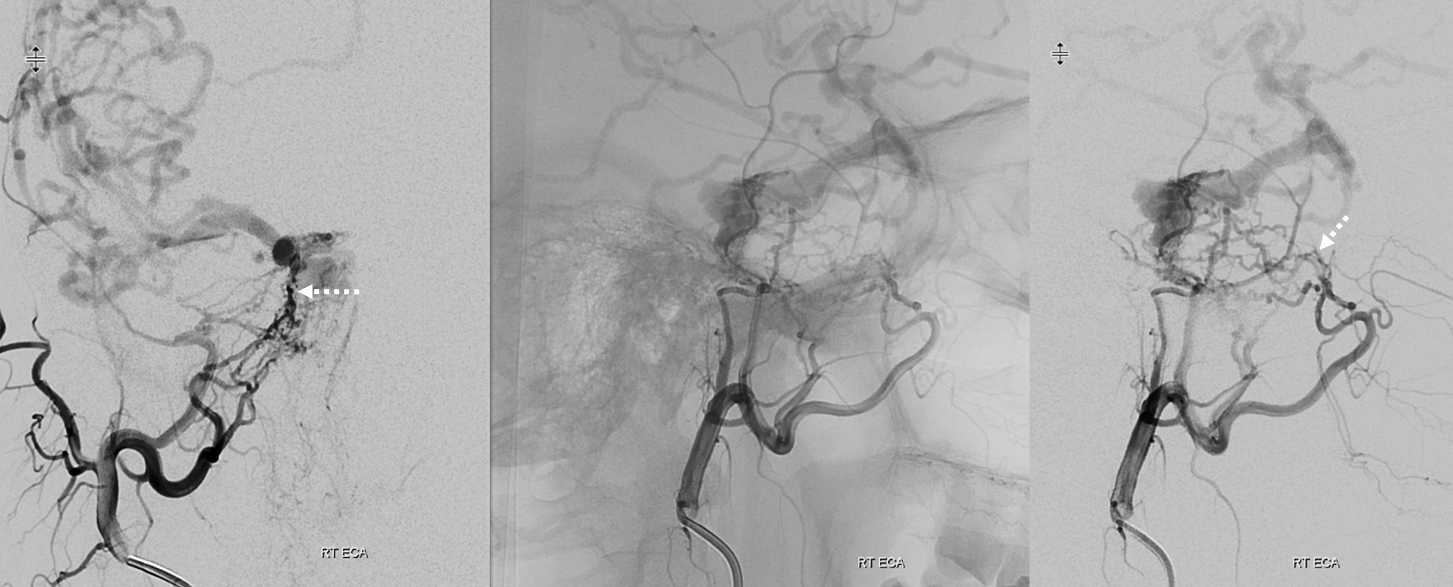
Left ICA — chronic occlusion. Accessory Meningeal and Rotundum reconstitution of the carotid via the ILT — look ’em up! Full case — great revascularization of the left M2 via the PCOM is here

Cavernous Fistula
Here, a large network of multiple vessels supplies a cavernous sinus dural fistula — see full case here. The foramen rotundum arterial network is one of them. Again, this shows how these nice vessel lines we draw in diagrams are really silly. There is a network everywhere. Look at these..
Video — pause and scroll through individual images